Introduction
Colorectal cancer (CRC) is a disease with an
increasing global incidence rate; it is currently the third most
frequently diagnosed and the second leading cause of mortality
among types of cancer worldwide (1). It has therefore spurred numerous
efforts to improve treatment strategies, but also to develop new
diagnostic approaches for an early and accurate detection. CRC is
one of the types of cancer with a dominant inflammatory component
and it frequently occurs against an inflammatory background
(2). Cytokines, cell adhesion
molecules and other molecules change their expression during the
inflammatory process and this finally leads to alterations in their
serum levels (3,4). At present, the diagnosis of CRC is
based on non-invasive screening methods like guaiac-based fecal
occult blood test (gFOBT) or the newer fecal DNA test, or on the
more precise and accurate flexible sigmoidoscopy and colonoscopy.
However, these methods are invasive, expensive or less sensitive in
the diagnosis of CRC; consequently, alternative methods were tested
for their diagnostic value in colorectal tumors (4,5).
One of these methods takes advantage of the
increased serum levels of cytokines that accompanies inflammation
in tumors (4). There have been
numerous studies that have evaluated the potential diagnostic
contribution of cytokines and other molecules to the diagnosis of
CRC; the results were often inconsistent or inconclusive (4–7).
Thus, the present study aimed to investigate whether serum levels
of cytokines, cell adhesion molecules or matrix metalloproteinases
(MMPs), alone or in combinations, could contribute to the
non-invasive diagnostic of CRC.
The present study evaluated the serum level of nine
cytokines (ILs; IL-1β, IL-4, IL-6, IL-8, IL-10, IL-17A, IL-22 and
IL-33, and interferon (IFN)-γ), two cell adhesion molecules
[intercellular adhesion molecule-1 (ICAM-1) and P-selectin (P-sel)]
and MMP-7. The cytokines were selected to represent the main immune
networks in tumors, allowing not only their use as potential
diagnostic tools, but also a global characterization of the immune
response in colorectal cancer.
Materials and methods
Patients
The present study was a prospective, case-control
study, in which 33 patients with colorectal malignant tumors and 35
age and sex-matched healthy controls were enrolled (Table I). The patients were treated in the
Surgical Clinic of the Regional Institute of Gastroenterology and
Hepatology (Cluj-Napoca, Romania), between March 2019 and March
2020.
 | Table I.Clinicopathological characteristics
of patients with CRC and healthy control patients. |
Table I.
Clinicopathological characteristics
of patients with CRC and healthy control patients.
| Clinicopathological
characteristic | CRC patients,
n=33 | Healthy controls,
n=35 |
|---|
| Sex, n (%) |
|
|
|
Male | 16 (48.5) | 14 (40.0) |
|
Female | 17 (51.5) | 21 (60.0) |
| Mean age,
years | 66.24 | 66.02 |
| Tumor stage, n
(%) |
|
|
| I | 7 (21.2) |
|
| II | 15 (45.5) |
|
|
III–IV | 11 (33.3) |
|
| Tumor WHO grade, n
(%) |
|
|
| 1 | 10 (30.3) |
|
| 2 | 21 (63.6) |
|
| 3 | 2 (6.1) |
|
| Tumor location, n
(%) |
|
|
| Right
colon | 10 (30.3) |
|
| Left
colon (including rectum) | 23 (69.7) |
|
| Tumor histology, n
(%) |
|
|
|
Adenocarcinoma | 33 (100.0) |
|
| Comorbidity, n
(%) |
|
|
|
Diabetes | 6 (18.18) | 7 (20.0) |
| Chronic
cardiovascular disease | 8 (24.24) | 7 (20.0) |
| (CAD,
atrial fibrillation) |
|
|
|
Cirrhosis | 1 (3.03) | 0 (0.0) |
|
Ascites | 1 (3.03) | 0 (0.0) |
|
Hypothyroidism | 1 (3.03) | 2 (5.71) |
| Chronic
kidney disease | 1 (3.03) | 0 (0.0) |
| Adrenal
adenoma | 1 (3.03) | 0 (0.0) |
|
Obesity | 1 (3.03) | 1 (2.85) |
The present study included patients with colorectal
adenocarcinoma confirmed by biopsy and pathologic examination. The
following subjects were excluded from the study: Patients and
controls suffering from inflammatory diseases that may affect the
serum levels of cytokines (such as collagen diseases, active
rheumatoid arthritis or inflammatory bowel disease), active
infections, active neoplasms in other locations; surgery, trauma or
vascular events in the previous four months, severe organic
deficiencies and patients with concomitant treatments that could
alter the immune response (including chemotherapy or cortisol). The
alcohol consumption and smoking status was comparable between the
two groups.
The present study was approved by the Ethics
Committee of the Iuliu Hațieganu University of Medicine and
Pharmacy (Cluj-Napoca; approval no. 40/02.04.2018) and of the
Regional Institute of Gastroenterology and Hepatology from
Cluj-Napoca (approval no. 2769/1.03.2018). Written informed consent
was obtained from each patient and healthy control.
ELISA analysis
A total of 10 ml serum was obtained from each
patient and healthy control by venous puncture of the median
cubital vein, followed by centrifugation for 10 min at 3,175 × g at
room temperature. The serum was stored at −80°C before testing.
ELISA kits (from Elabscience Biotechnology Inc.) with appropriate
working ranges for the cytokines were used, including for IL-6
(cat. no. E-EL-H0102), IL-8 (cat. no. E-EL-H0048), IL-10 (cat. no.
E-EL-H0103), IL-17A (cat. no. E-EL-H0105), IL-33 (cat. no.
E-EL-H2402), IFN-γ (cat. no. E-EL-H0108), ICAM-1 (cat. no.
E-EL-H2585) and P-sel (cat. no. E-EL-H0917). ELISA kits were also
purchased from Biolegend, Inc., including IL1β (cat. no. BZ-437007)
and IL-4 (cat. no. BZ-430307), and from R&D Systems Inc.,
including IL-22 (cat. no. RD-D2200) and MMP-7 (cat. no. RD-DMP700).
Each cytokine was tested individually and not through multiplexed
analysis, thus avoiding interactions between analytes in the
testing process and also allowing to choose the range of each kit.
All cytokines were analyzed in the present study, since they had
values inside the assay working range and 100 µl serum was used for
each cytokine assay. Standard curves for molecules were generated,
using the reference concentrations provided by the manufacturers.
The results were read on a Biotek Synergy H1 Hybrid microplate
reader (BioTek Instruments, Inc.). GraphPad Prism 6 (GraphPad
Software, Inc.) was used for analysis.
Statistical analysis
The analysis of the statistical significance of
differences in serum levels was performed either with the unpaired
t-test for normally-distributed data, or with the Mann-Whitney U
test for non-normally distributed data. Differences in cytokine
levels between stages or tumor grades were analyzed with either
one-way analysis of variance (ANOVA) with Games-Howell post hoc
test for data with normal distribution, or Kruskal-Wallis test with
Dunn's post hoc test for other continuous data. Shapiro-Wilk test
was used to test data normality.
To summarize the potential of all molecules to
discriminate between patients with CRC and healthy individuals,
logistic regression was performed; a stepwise approach was
followed, excluding molecules with no significant influence on the
dependent variable; different combinations of the remaining
molecules were tested for their ability to discriminate between CRC
and control samples. Logistic regression was used to check for
confounding factors. Correlational analysis of Spearman
coefficients was performed on all molecules; none of the molecules
analyzed together in logistic regression had correlation
coefficients above 0.7.
Receiver operating characteristics (ROC) curves for
each molecule and for the logistic regressions were generated using
XLstat software version 2021.3.1 (Addinsoft). All other statistical
analyzes were performed with R software version 4.1.0 (8). P<0.05 was considered to indicate a
statistically significant difference.
Results
The biological background and the
clinicopathological characteristics of the patients with CRC and
those in the control group are summarized in Table I. The differences in the serum
levels of molecules between patients and control groups are
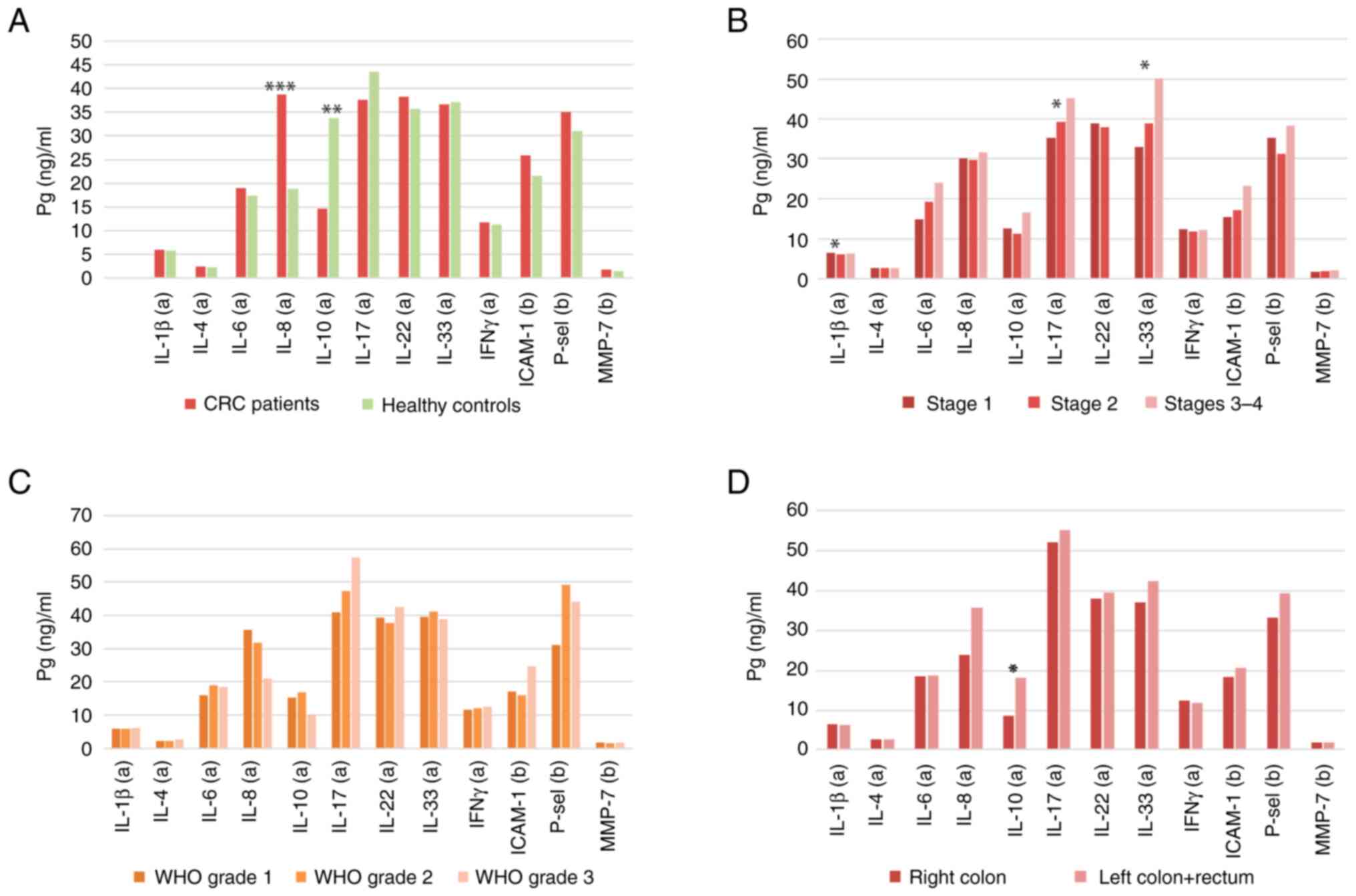
presented in Fig. 1A. A
significant increase was observed for IL-8 serum levels in CRC
compared with the control, whereas IL-10 was found significantly
decreased. IL-1β, IL-4, IL-6, IFN-γ, ICAM-1, MMP-7 and P-sel levels
were increased, but not significantly. IL-17 and IL-33 were found
slightly reduced in CRC patients, but with no statistical
significance.
The modifications in the serum levels of molecules
linked to the tumor TNM stage, WHO grade and location are presented
in Fig. 1B-D. Significant
increases with the tumor TNM stage were observed in IL-17 and IL-33
levels; IL-1β also had significant modifications but exhibited a
particular behavior, decreasing between stages I and II, and
increasing in the later stages (Fig.
1B). IL-6, ICAM-1 and MMP-7 increased with stage, but without
statistical significance. No stage-related modifications in the
serum levels of IL-4, IL-8 IL-22, IFN-γ and P-sel were observed.
The present study did not find any significant modification linked
to the tumor WHO grade; however, some trends were observed. For
example, IL-8, MMP-7 and ICAM-1 levels were increased in grade 1
compared with grade 2 tumors, whereas IL-6, IL-17 and P-sel levels
were increased in grade 2 compared with grade 1 tumors (Fig. 1C). Only 2 patients had grade 3, so
no significant comparisons were found.
Concerning the levels in the right and left colon
(which included the left colon distally from the splenic flexure
and the rectum) of the tumoral process, there were significant
increases in the levels of IL-10 in the left locations; the
adhesion molecules IL-8, ICAM-1 and P-sel as well as IL-33 were
also increased on the left, but not significantly (Fig. 1D). IFN-γ was increased in the right
colon tumors, without statistical significance. Finally, IL-1β,
IL-6, IL-17 and IL-22 and MMP-7 were not significantly modified in
right compared with left tumor locations.
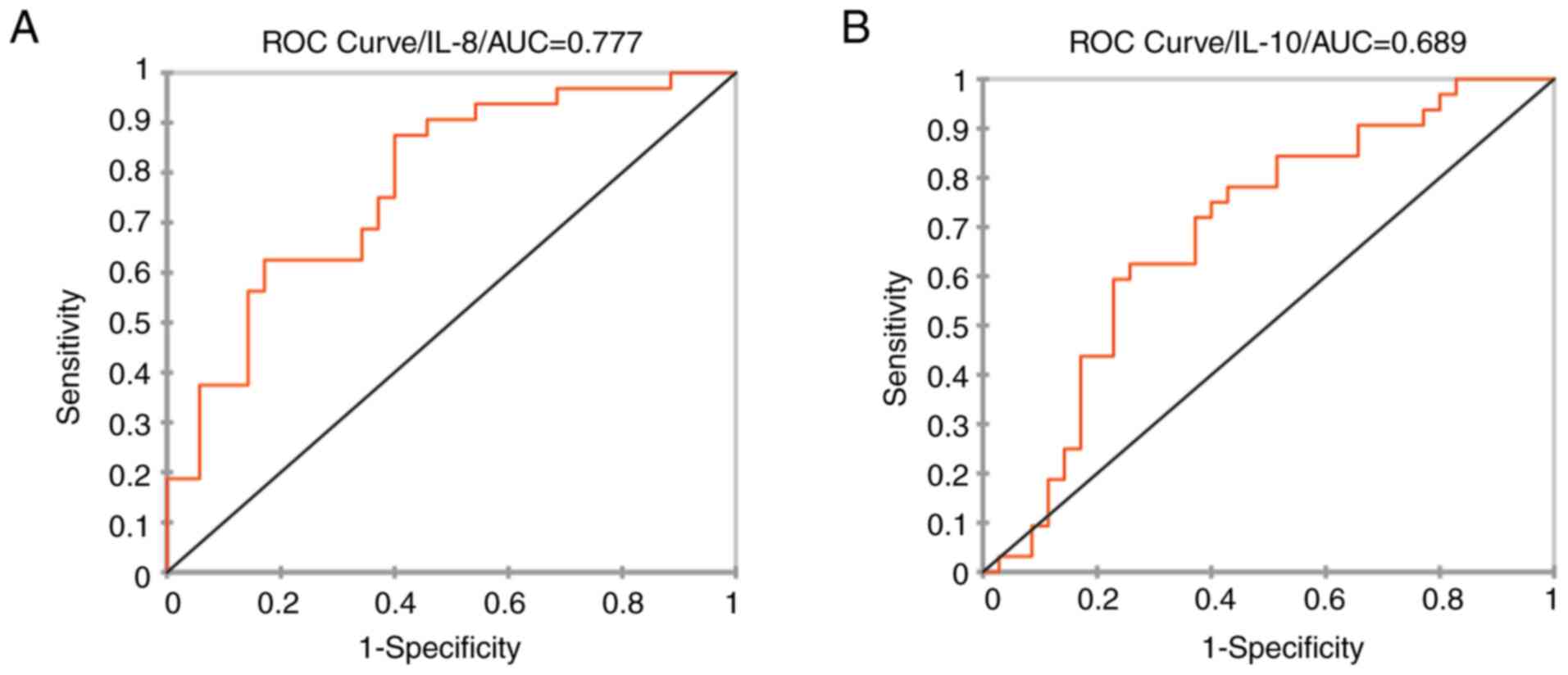
The biomarker potential of each significantly
modified molecule was tested. The ROC curves are presented in
Fig. 2. IL-8 had a sensitivity of
0.865, a specificity of 0.600 at a cutoff value of 20.741 pg/ml and
an AUC of 0.777; for IL-10 sensitivity was 0.65, specificity was
0.69, with an AUC of 0.689.
Investigation of the differences between patients
and controls linked to stage, tumor differentiation or locations
showed significant increases in ICAM-1 for stage II in patients
(P=0.0127; Fig. S1); for the rest
of the molecules, there were no distinctive elements in different
tumor stages compared with CRC in general. ICAM-1 showed some
biomarker potential for stage II, with a sensitivity of 0.86, a
specificity of 0.63 and an AUC of 0.724 (Fig. S1).
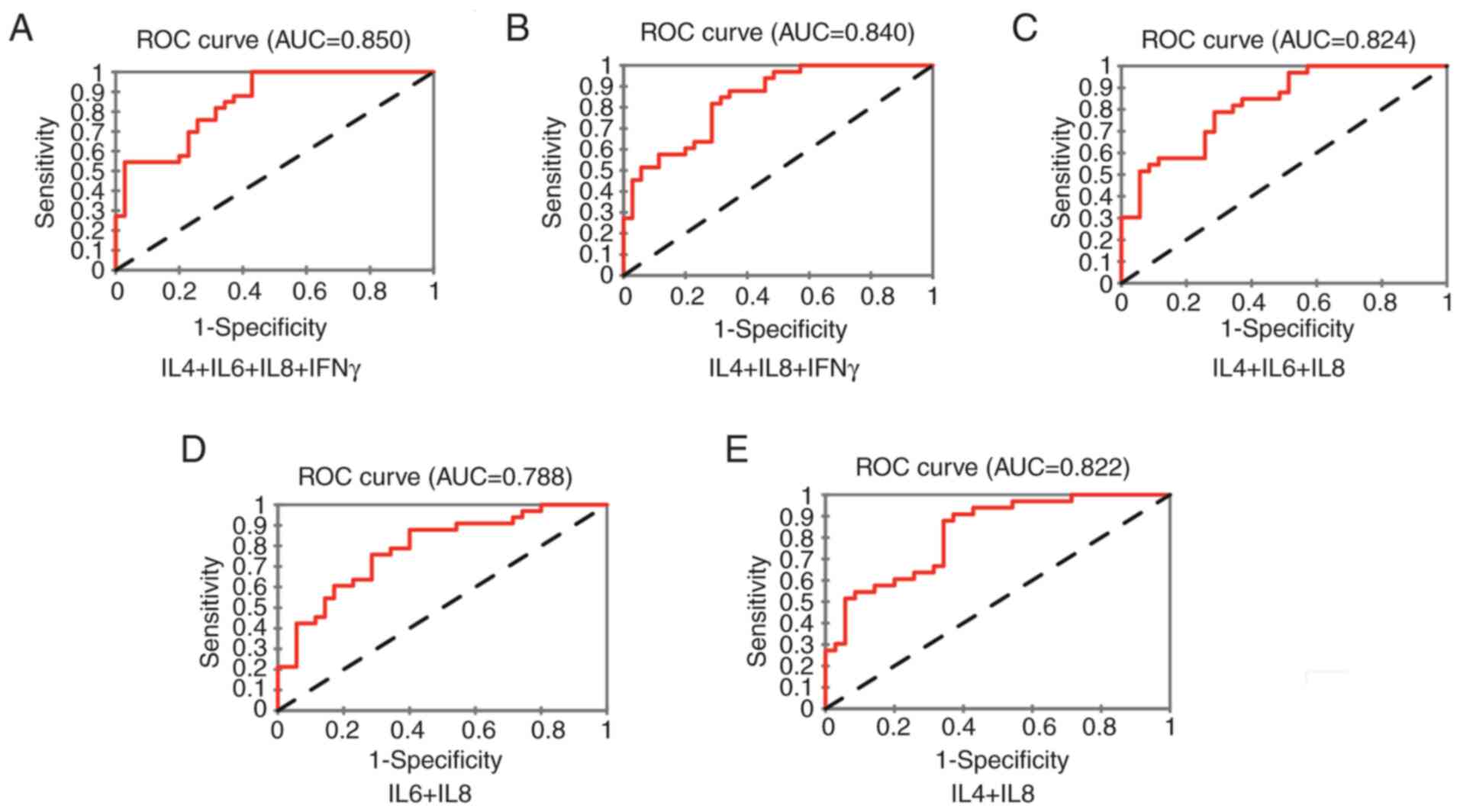
Correlation between molecules were tested prior to
logistic regression analyses (Table
SI). None of the molecules that had a correlation coefficient
>0.7 were assessed together in logistic regression. For the
combinations of molecules that were used (Fig. 3), IL4 + IL6 + IL8 + IFN-γ had a
sensitivity of 0.97, a specificity of 0.58 and an AUC of 0.85; for
IL4 + IL8 + IFN-γ, the sensitivity was 0.87, the specificity was
0.63 specificity and the AUC was 0.840; for IL4 + IL6 + IL8, there
was 0.84 sensitivity and 0.63 specificity, with an AUC of 0.824;
for IL6 + IL8, sensitivity was 0.84, specificity was 0.60 and AUC
was 0.788; finally, for IL4 + IL8, there was a sensitivity of 0.84,
a specificity of 0.66 and an AUC of 0.822.
The model with four cytokines had the best
sensitivity (0.97) at the optimal cutoff point of 0.71. The
equation of the model was: Z=−7.77 + (3.297×IL4)-(0.03×IL6) +
(0.086×IL8)-(0.103×IFNγ), where Z is the log(odds) for the positive
diagnosis of CRC, −7.77 is the intercept of the y-axis, and 3.297,
0.03, 0.086 and 0.103 are the regression coefficients for each
molecule. To test the potential of molecules for an early diagnosis
in CRC, the present study performed logistic regression on stage I
patients and controls. Table SII
presents the logistic regressions and Fig. S2 presents the most significant of
these. Some of the combinations tested for stage I had good
discriminative potential, in particular, the combination IL6 + IL8
+ IL22, with an AUC of 0.927, 0.85 sensitivity and 0.89 specificity
(Fig. S2E). The same combination
tested on all patients with CRC did not perform well (Fig. S2F).
Discussion
There are a number of studies which address the
serum levels of cytokines and their possible diagnostic
applications, many of which show increased levels of IL-8 in
colorectal cancer patients (4–6).
IL-1 exhibited no significant changes in a number of studies
(4–7). IL-6 level is found increased
(9), including two meta-analyses
(10,11), whereas another found no differences
or even a decrease compared with healthy subjects (4). IL-4 and IFN γ were evaluated in two
studies (4,5); one study showed significant
differences (4), while the other
found non-significant changes in these two cytokines (5). IL-17 was found increased in some
studies (4,12), but the majority reported no
difference or even decrease in CRC patients (13–15).
Two studies (10,12), one of them a meta-analysis
(10), showed a high level of
IL-22 in CRC patients. IL-10 is generally found increased in CRC
patients (13,16); however, Abtahi et al
(17) show decreased levels
compared with healthy patients, whereas Yamaguchi et al
(4) found no difference.
The adhesion molecules ICAM-1 and P-sel are
generally increased in CRC patients (18,19).
The same is true of MMP-7, which correlates with the tumor stage
(20). Some studies report low
levels of ICAM-1 or P-sel as the disease progresses (21,22).
Concerning the studies with multiple cytokines, Yamaguchi et
al (4) show a profile with
moderate increase in proinflammatory cytokines, IL-8, IL-12,
IL-17A, TNF-α and IFN-γ, as well as increases in IL-4, IL-9 and
some proinflammatory chemokines (such as CXCL-10 and CCL-3 and 4).
Kantola et al (5) found a
profile with significant increases of IL-6, IL-7 and IL-8, as well
as non-significant increases in IL-12, IFN γ and CXCL-10. Pengjun
et al (23) found IL-8,
TNF-α and MMP-7 as potential serum biomarkers, while IFN γ, IL-6
and IL-10 were not significant in discriminating between CRC and
normal serum.
The potential value as biomarkers for diagnosis and
prognosis was tested for the following molecules: IL-4, IL-6, IL-8
and IL-10, P-sel and MMP-7 (4–6,9,16,18,24),
as well as for multi-cytokine profiles (4,5,23),
highlighting the potential of all these molecules for being such
biomarkers. Other biomarker molecules for CRC were found to be
IL-7, IL-9, CCL-11 and CXCL-10 (4,5).
However, there was an inconsistency in the aforementioned studies
concerning cytokine levels, some showing increased and others
showing decreased levels for the same molecule. This inconsistency
was also observed concerning the biomarker potential of these
cytokines, neither molecule being found as universal biomarker for
CRC (5,23).
In this context, the present study selected
molecules representing the main immune networks that are present in
colorectal tumors: IL-1β, IL-6, IL-8 and IL-33 for the inflammatory
network, IFN-γ for the T helper (Th)1 and IFN-γ-secreting network,
IL-4 for the Th2 network, IL-17A and IL-22 for the Th17 and Th22
networks, and IL-10 for the suppressive network. Two adhesion
molecules, ICAM-1 and P-sel, were also tested, as was MMP-7, which
is produced as a consequence of the tumor development process. In
addition to its diagnostic utility, such a profile may allow a
global characterization of the immune response in colorectal
tumors. The profile that was obtained suggested a moderate increase
in the inflammatory compartment (mainly IL-1β and IL-8) and in the
Th1 and Th2 networks, no difference in the Th17 response and a
reduction in the suppressive network, reflected in the
significantly low levels of IL-10 level. However, the increases are
not notable, some of them being even not significant, the most
likely causes being the low immunogenicity of colorectal cancer and
the generally weak response that the organism mounts against
tumors.
Not all the significantly modified molecules showed
biomarker potential. The present study highlighted that increased
IL-8 had the capacity to discriminate between CRC and normal serum
(Fig. 2).
Combinations of molecules were tested by logistic
regression; all showed discriminative potential for CRC, providing
possible diagnostic approaches for the clinician (Fig. 3). Concerning the potential of these
molecules, alone or in combinations, to detect the early stages of
the tumoral process, the combination IL-6 + IL-8 + IL-22 showed a
good discriminative potential for this stage (Fig. S2E). The same combination, tested
in all CRC patients, did not have notable performances (Fig. S2F). However, this result should be
considered cautiously, given the small number of subjects in stage
I that were tested in the present study. The results should be
interpreted in the context of the variability of the results in IL
testing in CRC, highlighted in the aforementioned studies. Within
this variability, certain patterns can be observed. For example,
from the few studies with multi-cytokine analysis aforementioned,
including the present study, the main patterns that emerge are
those with increased IFN-γ, IL-12 and CXCL-10, along with a
moderate increase in Th2 and Th17 cytokines (4), and patterns with non-significant
increases of these cytokines (5,23).
Inflammation was found increased by all studies, through its
representative molecules (IL-6, IL-8, ICAM-1 and P-sel) (4,5,18,19,23).
The most constantly increased cytokines that all studies, including
the present study, have found significantly increased is IL-8,
followed by IL-6.
This behavior of ILs and adhesion molecules in CRC
may be explained by the heterogeneity of colorectal cancer in
histological structure and molecular mechanisms, which leads to
different immune infiltration and, by consequence, to different
cytokine production patterns (25).
The heterogeneity of the immune infiltration in
tumors and its consequence, the variability of the seric cytokine
profiles, makes it difficult to find reliable biomarkers in
colorectal cancer; a good strategy may be to choose cytokine
combinations that cover all possible patterns, such as IL6 + IL8 +
IL4 + IFN-γ, or IL-6 + IL-8 for the patterns with only
inflammation. An alternative is to use molecules that have been
found constantly elevated in CRC, such as IL-8 and IL-6 or, in
other studies, IL-7 and IL-9 (4,5).
The results of the present study were generally in
line with other studies on this topic (4,5,18,19,23);
however, owing to the small sample size, these results should be
validated on larger population samples before translation into the
clinic. An area that the study did not cover is represented by
cytokine level increases in precancerous lesions, such as polyps,
familial polyps or adenomas; some of the molecules studied, such as
IL-4 and IL-17, increased in expression along the adenoma-carcinoma
sequence (26). Such an approach
would be useful as a non-invasive method of differentiating between
malignant and non-malignant lesions.
Compared with the gFOBT test, which has a
sensitivity of 31% and a specificity of 87% (27), the combinations of ILs used in the
present study have sensitivities that range between 84 and 97% and
specificities ranging between 58 and 66%. Cytokine testing is
superior in terms of sensitivity but less specific compared with
the gFOBT test; cytokine testing is also more expensive. However,
since a cancer has to be diagnosed, high sensitivities are
preferable; the combined use of cytokine testing and gFOBT test
would provide a combination of high sensitivity and
specificity.
A significant challenge is that serum cytokines
levels also increase in inflammatory diseases. However, these
increases are much more prominent in inflammation than in cancer,
which could help to differentiate between the two (28–30);
the pattern of these increases could also be helpful, as it has
been shown that there is a complex pattern of these increases in
CRC (4,5,23),
whereas the immune response in inflammatory diseases is not as
complex, being usually Th1, Th2 or Th17-driven.
Using the right strategy, cytokines may have a role
in the diagnosis of colorectal neoplasias, along with their
emerging role as a prerequisite for future personalized
immuno-therapies in cancer (31).
It is a non-invasive and inexpensive method, which proved to be
accurate in terms of results, and may be considered to have its
place in the diagnostic strategies in colorectal cancer.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
The study was supported partially through a grant from The Iuliu
Hatieganu Medicine and Pharmacy University of Cluj-Napoca, Romania;
(grant no. 2462/19/17.01.2020).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
OF conceived the study and wrote the manuscript;
IBN, LB and OZ made substantial contributions to analysis and
interpretation of data; FZ made substantial contributions to
acquisition of data; VC made important contributions to the
conception and design of the work, being also involved in drafting
the manuscript and revising it critically for important
intellectual content. All authors read and approved the final
manuscript. LB and OZ confirm the authenticity of all the raw
data.
Ethics approval and consent to
participate
The study obtained the approvals of the Ethics
Committee of the Iuliu Hatieganu Medicine and Pharmacy University
(Cluj-Napoca, Romania; approval no. 40/02.04.2018) and of the
Regional Gastroenterology and Hepatology Institute (Cluj-Napoca,
Romania; approval no 2769/1.03.2018) and the written informed
consent from each patient and healthy control.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AUC
|
area under the curve
|
|
CRC
|
colorectal cancer
|
|
ICAM-1
|
intercellular adhesion molecule-1
|
|
IFN
|
interferon
|
|
IL
|
interleukin
|
|
MMP
|
matrix metalloproteinase
|
|
P-sel
|
P-selectin
|
|
ROC
|
receiver operating characteristic
|
|
Th
|
T helper
|
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
types of cancer in 185 countries. CA Cancer J Clin. 71:209–249.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Long AG, Lundsmith ET and Hamilton KE:
Inflammation and colorectal cancer. Curr Colorectal Cancer Rep.
13:341–351. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wei X, Zhang Y, Yang Z, Sha Y, Pan Y, Chen
Y and Cai L: Analysis of the role of the interleukins in colon
cancer. Biol Res. 53:202020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yamaguchi M, Okamura S, Yamaji T, Iwasaki
M, Tsugane S, Shetty V and Koizumi T: Plasma cytokine levels and
the presence of colorectal cancer. PLoS One. 14:e02136022019.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Kantola T, Klintrup K, Väyrynen JP,
Vornanen J, Bloigu R, Karhu T, Herzig KH. Näpänkangas J, Mäkelä J,
Karttunen TJ, et al: Stage-dependent alterations of the serum
cytokine pattern in colorectal carcinoma. Br J Cancer.
107:1729–1736. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bünger S, Haug U, Kelly M, Posorski N,
Klempt-Giessing K, Cartwright A, Fitzgerald SP, Toner V, McAleer D,
Gemoll T, et al: A novel multiplex-protein array for serum
diagnostics of colon cancer: A case-control study. BMC Cancer.
12:3932012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ueda T, Shimada E and Urakawa T: Serum
levels of cytokines in patients with colorectal cancer: Possible
involvement of interleukin-6 and interleukin-8 in hematogenous
metastasis. J Gastroenterol. 29:423–429. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
R Core Team R, . A language and
environment for statistical computing. R foundation for statistical
computing; Vienna: 2021, https://www.r-project.org/
|
|
9
|
Chung YC and Chang YF: Serum interleukin-6
levels reflect the disease status of colorectal cancer. J Surg
Oncol. 83:222–226. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Yan G, Liu T, Yin L, Kang Z and Wang L:
Levels of peripheral Th17 cells and serum Th17-related cytokines in
patients with colorectal cancer: A meta-analysis. Cell Mol Biol
(Noisy-le-grand). 64:94–102. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Xu J, Ye Y, Zhang H, Szmitkowski M,
Mäkinen MJ, Li P, Xia D, Yang J, Wu Y and Wu H: Diagnostic and
prognostic value of serum interleukin-6 in colorectal cancer.
Medicine (Baltimore). 95:e25022016. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Doulabi H, Rastin M, Shabahangh H, Maddah
G, Abdollahi A, Nosratabadi R, Esmaeili SA and Mahmoudi M: Analysis
of Th22, Th17 and CD4+ cells co-producing IL-17/IL-22 at
different stages of human colon cancer. Biomed Pharmacother.
103:1101–1106. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Stanilov N, Miteva L, Deliysky T, Jovchev
J and Stanilova S: Advanced colorectal cancer is associated with
enhanced IL-23 and IL-10 serum levels. Lab Med. 41:159–163. 2010.
View Article : Google Scholar
|
|
14
|
Karabulut S, Usul Afsar C, Karabulut M,
Kilic L, Alis H, Kones O, Bilgin E and Faruk Aykan N: Clinical
significance of serum interleukin-17 levels in colorectal cancer
patients. J Buon. 21:1137–1145. 2016.PubMed/NCBI
|
|
15
|
Wägsäter D, Löfgren S, Hugander A and
Dimberg J: Expression of interleukin-17 in human colorectal cancer.
Anticancer Res. 26:4213–4216. 2006.PubMed/NCBI
|
|
16
|
Li B, Wang F, Ma C, Hao T, Geng L and
Jiang H: Predictive value of IL-18 and IL-10 in the prognosis of
patients with colorectal cancer. Oncol Lett. 18:713–719.
2019.PubMed/NCBI
|
|
17
|
Abtahi S, Davani F, Mojtahedi Z, Hosseini
SV, Bananzadeh A and Ghaderi A: Dual association of serum
interleukin-10 levels with colorectal cancer. J Cancer Res Ther.
13:252–256. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Alexiou D, Karayiannakis AJ, Syrigos KN,
Zbar A, Kremmyda A, Bramis I and Tsigris C: Serum levels of
E-selectin, ICAM-1 and VCAM-1 in colorectal cancer patients:
Correlations with clinico-pathological features, patient survival
and tumour surgery. Eur J Cancer. 37:2392–2397. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Korniluk A, Kamińska J, Kiszło P, Kemona H
and Dymicka-Piekarska V: Lectin adhesion proteins (P-, L- and
E-selectins) as biomarkers in colorectal cancer. Biomarkers.
22:629–634. 2017.PubMed/NCBI
|
|
20
|
Polistena A, Cucina A, Dinicola S, Stene
C, Cavallaro G, Ciardi A, Orlando G, Arena R, D'Ermo G, Cavallaro
A, et al: MMP7 expression in colorectal tumours of different
stages. In Vivo. 28:105–110. 2014.PubMed/NCBI
|
|
21
|
Peeters C, Ruers T, Westphal J and de Waal
RMW: Progressive loss of endothelial P-selectin expression with
increasing malignancy in colorectal cancer. Lab Invest. 85:248–256.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shibata M, Ando K, Amano S and Kurosu Y:
Local expression and circulating form of ICAM-1 in colorectal
cancer. Ann Cancer Res Ther. 5:29–33. 1996. View Article : Google Scholar
|
|
23
|
Pengjun Z, Xinyu W, Feng G, Xinxin D,
Yulan L, Juan L, Xingwang J, Zhennan D and Yaping T: Multiplexed
cytokine profiling of serum for detection of colorectal cancer.
Future Oncol. 9:1017–1027. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang D, Yuan W, Wang Y, Wu Q, Yang L, Li
F, Chen X, Zhang Z, Yu W, Maimela NR, et al: Serum CCL20 combined
with IL-17A as early diagnostic and prognostic biomarkers for human
colorectal cancer. J Transl Med. 17:2532019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Karpinski P, Rossowska J and Sasiadek MM:
Immunological landscape of consensus clusters in colorectal cancer.
Oncotarget. 8:105299–105311. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mager LF, Wasmer MH, Rau TT and Krebs P:
Cytokine-induced modulation of colorectal cancer. Front Oncol.
6:962016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ramdzan AR, Abd Rahim MA, Mohamad Zaki A,
Zaidun Z and Mohammed Nawi A: Diagnostic accuracy of FOBT and
colorectal cancer genetic testing: A systematic review &
meta-analysis. Ann Glob Health. 85:702019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Yang M, Cen X, Xie Q, Zuo C, Shi G and Yin
G: Serum interleukin-6 expression level and its clinical
significance in patients with dermatomyositis. Clin Dev Immunol.
2013:7178082013. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Pavlovic V, Dimic A, Milenkovic S and
Krtinic D: Serum levels of IL-17, IL-4 and IFNγ in Serbian patients
with early rheumatoid arthritis. J Res Med Sci. 19:18–22.
2014.PubMed/NCBI
|
|
30
|
Jafarzadeh A, Mahdavi R, Jamali M,
Hajghani H, Nemati M and Ebrahimi HA: Increased concentrations of
interleukin-33 in the serum and cerebrospinal fluid of patients
with multiple sclerosis. Oman Med J. 31:40–45. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Palucka AK and Coussens LM: The basis of
oncoimmunology. Cell. 164:1233–1247. 2016. View Article : Google Scholar : PubMed/NCBI
|