Introduction
An estimated 460,000 new pancreatic cancer cases
occur worldwide each year, resulting in 430,000 annual deaths
(1). Pancreatic cancer has several
risk factors, including smoking, age, alcohol abuse, obesity,
genetic factors, diabetes, diet, and lack of exercise, and it is
one of the most intractable carcinomas, with a 5-year survival rate
of approximately 9% (2,3). In Japan, the number of pancreatic
cancer patients has been increasing in recent years; it is
responsible for more than 30,000 deaths every year, making it the
fourth leading cause of cancer death following lung cancer, colon
cancer, and stomach cancer (4).
Gemcitabine plus nab-paclitaxel combination therapy
(GnP) was shown to be superior to gemcitabine monotherapy in terms
of overall survival (OS) as a first-line treatment for patients
with metastatic pancreatic cancer in a phase III trial (5). The treatment guideline of the
National Comprehensive Cancer Network and Japanese Pancreas Society
recommends GnP as a standard treatment for pancreatic cancer in
combination with a FOLFIRINOX (fluorouracil, leucovorin,
irinotecan, and oxaliplatin) regimen (6,7). GnP
and FOLFIRINOX have become the standard treatment for unresectable
pancreatic cancer not only in Japan but also worldwide.
Sarcopenia is a condition in which muscle mass
decreases with age (8). Sarcopenia
can be divided into primary or secondary sarcopenia according to
its origin (i.e., malignant tumors, chronic heart failure, or
chronic kidney disease) (9,10).
In recent years, global interest in sarcopenia has increased, and
diagnostic algorithms were proposed by the European Working Group
on Sarcopenia in Older People (EWGSOP) in 2010 and the Asian
Working Group for Sarcopenia in 2014, respectively (11,12).
In both sets of criteria, sarcopenia is defined as a morbid status
involving loss of muscle mass or loss of physical function.
Because it is defined by a decrease in skeletal
muscle mass, the skeletal muscle index (SMI) is useful for the
evaluation of sarcopenia (13).
The methods of measuring the SMI include measuring the
cross-sectional area of the muscle by examining images, such as
computed tomography (CT) and magnetic resonance imaging (MRI);
bioelectrical impedance analysis (BIA); and dual-energy X-ray
absorptiometry (DEXA) (14,15).
Sarcopenia has been reported to be a prognostic
factor in various cancers, including pancreatic cancer (16–19).
Moreover, in patients receiving cytotoxic chemotherapy, sarcopenia
has been reported to be a predictor of response and to contribute
to increased toxicity (20–22).
Although GnP is the standard chemotherapy for pancreatic cancer and
has been administered to numerous patients, there are no reports on
the relationship between GnP treatment outcomes and sarcopenia in
patients with advanced pancreatic cancer. As the relationship
between sarcopenia and prognosis becomes clear, early nutritional
and exercise interventions may improve the prognosis. Therefore, we
retrospectively analyzed the impact of sarcopenia on OS,
progression-free survival (PFS), response rate, disease control
rate, and adverse events (AEs) by assessing SMI via BIA.
Materials and methods
Ethics
The present study was approved by the Institutional
Review Board of Kanagawa Cancer Center. Informed consent was
obtained in the form of an opt-out form on the website.
Patients
We retrospectively analyzed 121 consecutive patients
with advanced pancreatic cancer who received GnP as the first-line
treatment from January 2015 to December 2017. GnP treatment
included 1,000 mg/m2 of gemcitabine and 125
mg/m2 of nab-paclitaxel administered on days 1, 8, and
15 at four-week-intervals. The dose was reduced or postponed
depending on general condition, laboratory data, and AEs.
The inclusion criteria were as follows: patients
with unresectable pancreatic cancer diagnosed as stage III or IV
according to the 7th edition of the Union for International Cancer
Control TNM classification and an Eastern Cooperative Oncology
Group Performance Status (ECOG PS) of 0 or 1 (23,24).
Adenocarcinoma was diagnosed by tissue biopsy or cytology. These
patients received GnP as first-line chemotherapy. Any patient
unsuitable for InBody 720 measurement due to massive ascites and
pleural effusion was excluded from the study. We also excluded
patients with clinically symptomatic cholangitis or
pancreatitis.
Predictors
Body composition was evaluated using an InBody
720® (InBody, Tokyo, Japan) prior to the initiation of
GnP. SMI was calculated by dividing the skeletal muscle mass of the
extremities by the square of the height. The cutoff values were
based on values measured in healthy adults in Taiwan using BIA. The
SMI cutoff values were below the mean adult skeletal muscle mass
indicated by the EWGSOP, with reference to the value determined as
−2 standard deviations. In this study, the cutoff values were 8.87
kg/m2 for males and 6.42 kg/m2 for females
(25). Cases with an SMI higher
than the cutoff values were allocated to the non-sarcopenia group
and those with an SMI lower than the cutoff values were allocated
to the sarcopenia group. In both groups, sex age, PS, body mass
index (BMI), clinical stage, the modified Glasgow prognostic score
(mGPS), tumor localization (pancreatic head or body tail), and
tumor marker [serum carbohydrate antigen 19-9 (CA19-9)] were
analyzed.
CA19-9 was measured at the start of GnP. We measured
CA19-9 by chemiluminescent immunoassay using an
ARCHITECTi2000SR® (Abbott Japan, Tokyo, Japan). The BMI
was calculated by dividing the weight at the start of GnP by the
square of the height. The standard value was set at 22 (26). The adopted mGPS was based on both
the C-reactive protein (CRP) and albumin levels as sarcopenia
indicators (27). Patients with
both elevated CRP (>1.0 mg/l) and hypoalbuminemia (<3.5 g/l)
were assigned a score of 2; those patients with either elevated CRP
or hypoalbuminemia were assigned a score of 1; and those with
neither elevated CRP nor hypoalbuminemia were assigned a score of
0. The relative dose intensity (RDI) for each chemotherapy regimen
was calculated by dividing the actual dose by the planned dose. We
analyzed the RDI up to 12 weeks after the start of GnP because it
is expected to decrease with long-term treatment, mainly due to
peripheral neuropathy caused by nab-paclitaxel (5). Second-line treatment after GnP
failure was initiated when patients had adequate organ function and
a good PS; otherwise, they received best supportive care.
Follow-up
The follow-up period was until December 2019. The
response and disease control rates were evaluated based on 5-mm
slice CT scans every 6–10 weeks and the (Response Evaluation
Criteria in Solid Tumors version 1.1 (28). GnP was continued until the
appearance of unacceptable AEs or disease progression.
Outcomes
In this study, the primary outcomes were OS, PFS,
disease control rate, and response rate. OS was calculated from the
date of GnP initiation to the date of death by any cause. PFS was
calculated from the date of GnP initiation to the date of disease
progression or death by any cause. Patients lost to follow-up were
treated as censored cases.
The secondary outcomes were AEs. Hematologic
toxicities, such as leukopenia, neutropenia, thrombocytopenia, and
anemia, and non-hematologic toxicities, such as nausea, anorexia,
diarrhea, constipation, fatigue, peripheral neuropathy, and
anorexia were listed as retrospectively evaluable AEs. AEs were
classified into grades 1–5 according to the Common Terminology
Criteria for Adverse Events version 5 (29).
Statistical method
According to previous reports (30), the proportion of sarcopenia was
estimated as 30–65%, and its impact on hazard ratio (HR) of
survival was at least 0.5. We set the duration of accrual and
follow-up as 2 years and 1 year, respectively, and considered that
a sample size of 109 patients was required to detect the impact of
sarcopenia on the survival, with an alpha error of 0.05 and a power
of 90%. JMPPro15.0 (JMP Japan, Toyo, Japan) was used for the
statistical analysis. The unpaired Student's t-test and Fisher's
exact test were used for comparisons of patient backgrounds and
AEs. The comparison of RDI was evaluated by unpaired Student's
t-test for each drug.
PFS and OS were analyzed using the Kaplan-Meier
method and the HR and corresponding 95% confidence interval (CI)
were estimated using the log-rank test and Cox regression analysis.
Multivariate analysis for prognostic factors was performed using
the Cox Proportional Hazards model with the backward selection
method. P<0.05 was considered to indicate a statistically
significant difference.
Results
Patients
Table I shows the
patient backgrounds in each group. There were no differences in
age, tumor location, clinical stage, mGPS, PS, or CA19-9 between
the two groups. There were significantly more males than females in
the sarcopenia group.
 | Table I.Patient backgrounds of the sarcopenia
and non-sarcopenia groups. |
Table I.
Patient backgrounds of the sarcopenia
and non-sarcopenia groups.
| Characteristic | All patients
(n=121) | Non-sarcopenia
(n=81) | Sarcopenia
(n=40) | P-value |
|---|
| Median age, years
(range) | 69 (43–80) | 67 (43–80) | 70 (44–78) | 0.05 |
| Sex, n |
|
|
| <0.01 |
|
Male | 71 | 36 | 35 |
|
|
Female | 50 | 45 | 5 |
|
| Performance status,
n |
|
|
| 0.84 |
| 0 | 43 | 28 | 15 |
|
| 1 | 78 | 53 | 25 |
|
| Mean BMI,
kg/m2 (SD) | 20.6 (3.0) | 21.5 (2.67) | 18.5 (2.45) | <0.01 |
| Mean SMI,
kg/m2 (SD) |
|
|
|
|
|
All | 8.4 (1.15) | 8.7 (1.1) | 7.8 (0.98) | <0.01 |
|
Male | 8.9 (1.04) | 9.7 (0.61) | 8.1 (0.7) | <0.01 |
|
Female | 7.7 (0.94) | 7.9 (0.79) | 5.9 (0.98) | <0.01 |
| UICC clinical
stage, n |
|
|
| 0.83 |
|
III | 33 | 23 | 10 |
|
| IV | 88 | 58 | 30 |
|
| Mean albumin, g/dl
(SD) | 3.7 (0.54) | 3.7 (0.53) | 3.5 (0.50) | 0.07 |
| Median CRP, mg/dl
(IQR) | 1.56
(0.12-1.29) | 0.2
(0.10-1.02) | 0.54
(0.14-2.26) | 0.08 |
| mGPS, n |
|
|
| 0.18 |
| 0 | 59 | 44 | 15 |
|
| 1 | 30 | 19 | 11 |
|
| 2 | 32 | 18 | 14 |
|
| Localization of
tumor, n |
|
|
| 0.44 |
|
Head | 47 | 36 | 11 |
|
| Body or
tail | 74 | 45 | 29 |
|
| Median CA19-9, U/ml
(IQR) | 628.2
(99.4-17,966) | 564.7
(70.0-20,349) | 1,477 (332–16,147) | 0.37 |
Treatment course
In the non-sarcopenia and sarcopenia groups, the
median RDIs at 12 weeks after the start of GnP were 0.84 (range:
0.11-1.0) and 0.73 (range: 0.22-1.0) for gemcitabine, and 0.80
(range: 0.11-1.0) and 0.67 (range: 0.11-1.0) for nab-paclitaxel,
respectively, with corresponding P-values of 0.32 and 0.26 for
gemcitabine and nab-paclitaxel, respectively (Table II). The number of patients with
dose reduction at GnP initiation was significantly higher in the
sarcopenia group (P=0.03, Table
II) than in the non-sarcopenia group. The reasons for
discontinuing chemotherapy were not different between the two
groups.
| Table II.Treatment courses of the sarcopenia
and non-sarcopenia groups. |
Table II.
Treatment courses of the sarcopenia
and non-sarcopenia groups.
| Variable | Non-sarcopenia
(n=81) | Sarcopenia
(n=40) | P-value |
|---|
| Median relative
dose intensity at 12 weeks (range) |
|
|
|
|
Gemcitabine | 0.84
(0.11-1.0) | 0.73
(0.22-1.0) | 0.32 |
|
Nab-paclitaxel | 0.80
(0.11-1.0) | 0.67
(0.11-1.0) | 0.26 |
| Dose reduction at
GnP initiation, n (%) | 5 (6) | 4 (10) | 0.03 |
| Reason for GnP
discontinuation, n (%) |
|
|
|
| Disease
progression | 68 (84) | 30 (75) | 0.28 |
| Adverse
events | 5 (6) | 5 (12.5) | 0.26 |
| Poor
performance status | 2 (2) | 3 (7) | 0.20 |
|
Patient's request | 3 (4) | 2 (5) | 0.77 |
|
Conversion surgery | 3 (4) | 0 (0) | 0.20 |
| Secondary
treatment, n (%) | 60 (74) | 29 (73) | 0.85 |
|
Chemotherapy, n (%) | 54 (67) | 27 (68) |
|
|
Chemoradiotherapy, n (%) | 3 (4) | 1 (3) |
|
|
Conversion surgery, n (%) | 3 (4) | 0 (0) |
|
| Others,
n (%) | 0 (0) | 1 (3) |
|
A total of 60 patients (74%) in the non-sarcopenia
group and 29 patients (73%) in the sarcopenia group received
second-line chemotherapy (P=0.85, Table II). The regimen for the
second-line treatment was at the physician's discretion:
FOLFIRINOX, S-1, or other investigational drugs. Three patients in
the non-sarcopenia group who showed remarkable tumor shrinkage
underwent surgical resection as a conversion surgery.
Efficacy
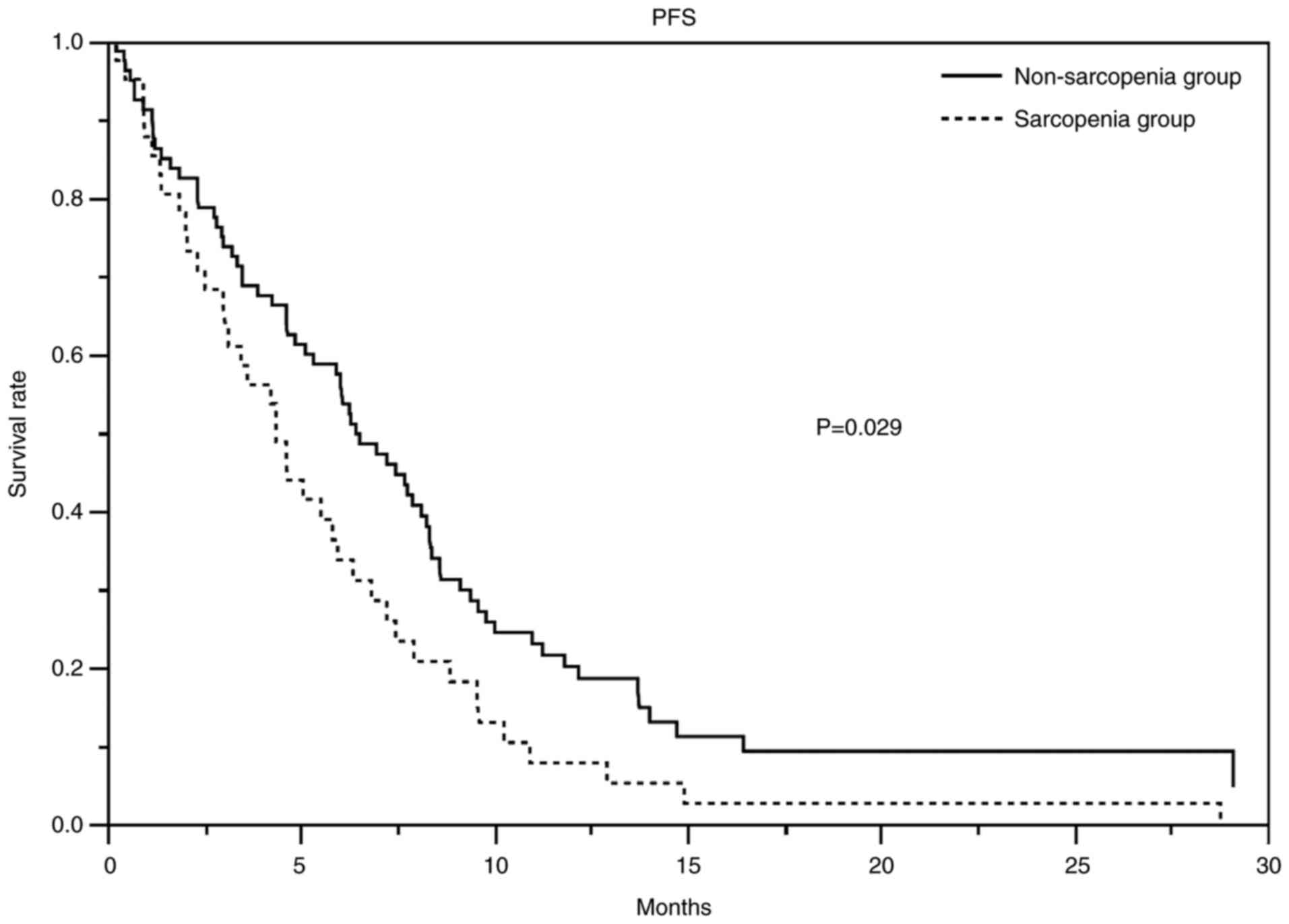
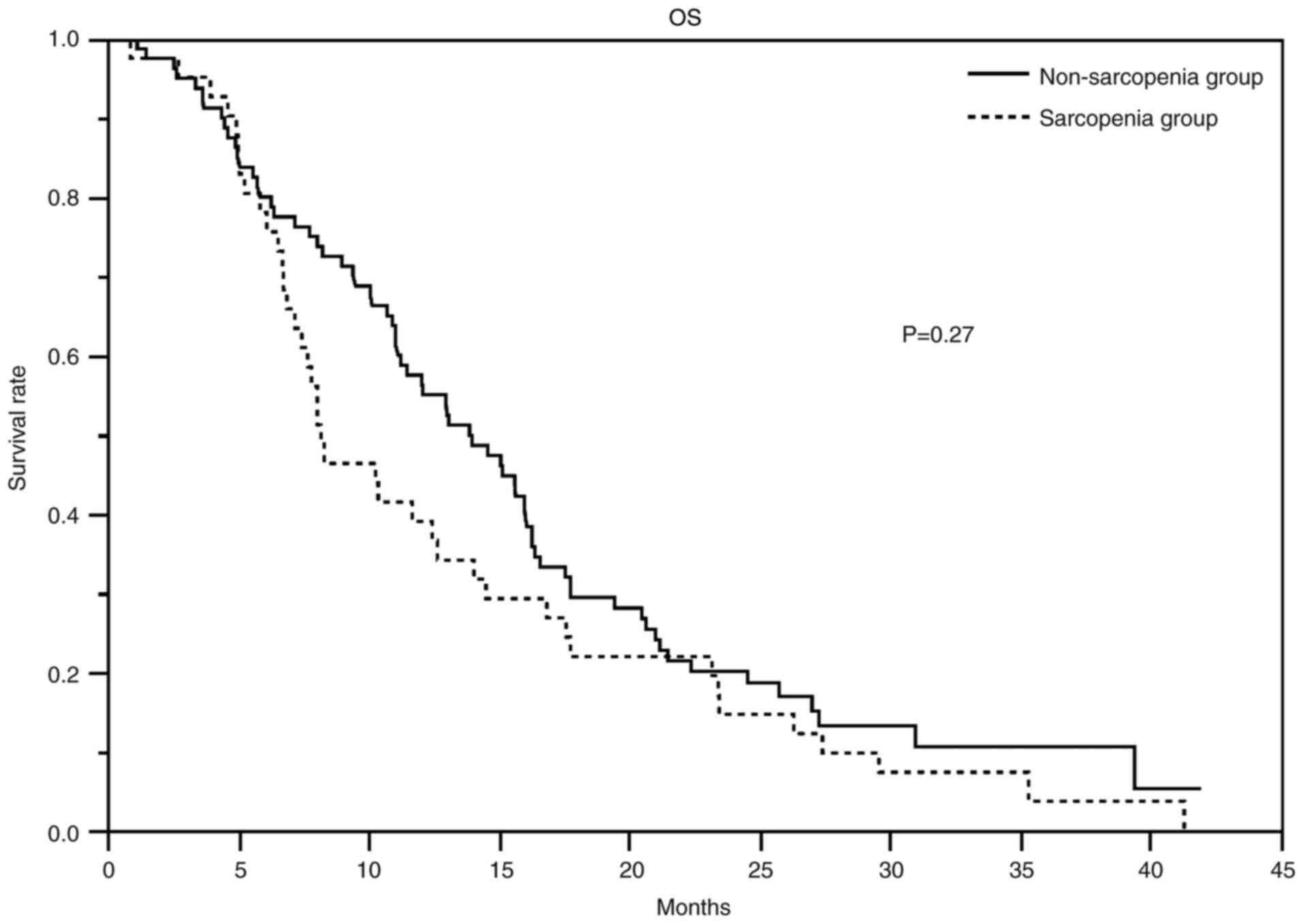
At the time of data cutoff, the median duration of
follow-up for censored cases was 27.4 months. Table III showed the response and
disease control rates, PFS, and OS. The response rates in the
non-sarcopenia and sarcopenia groups were 32 and 20% (P=0.20),
respectively, and the disease control rates were 81 and 80%
(P=1.00), respectively. The non-sarcopenia and sarcopenia groups
had a median PFS of 6.4 months (95% CI 4.9-8.1) and 4.4 months
(range: 3–5.9), respectively, and a median OS of 13.9 months (95%
CI 11.0-16.1) and 8.2 months (95% CI 6.9-12.7), respectively.
Figs. 1 and 2 show the PFS and Kaplan-Meier curves for
OS, respectively. The HR for PFS in the non-sarcopenia group
compared with the sarcopenia group was 0.63 (95% CI 0.42-0.95;
Table IV), whereas that for OS
was 0.79 (95% CI 0.53-1.20; Table
V). We could not reject the null hypothesis for the OS.
| Table III.Treatment efficacy in the sarcopenia
and non-sarcopenia groups. |
Table III.
Treatment efficacy in the sarcopenia
and non-sarcopenia groups.
| Variable | Non-sarcopenia
(n=81) | Sarcopenia
(n=40) | P-value |
|---|
| Objective response,
n (%) |
|
| 0.30 |
| CR | 0 (0) | 1 (3) |
|
| PR | 26 (32) | 7 (18) |
|
| SD | 40 (49) | 24 (60) |
|
| PD | 15 (19) | 8 (20) |
|
| Response rate,
% | 32 | 20 | 0.20 |
| Disease control
rate, % | 81 | 80 | >0.99 |
| Median PFS, months
(95% CI) | 6.4 (95% CI
4.9-8.1) | 4.3 (95% CI
3.0-5.9) | 0.02 |
| Median OS, months
(95% CI) | 13.9 (95% CI
11.0-16.1) | 8.3 (95% CI
6.9-12.7) | 0.18 |
| Table IV.Factors related to progression-free
survival. |
Table IV.
Factors related to progression-free
survival.
|
| Univariate
analysis | Multivariate
analysisa |
|---|
|
|
|
|
|---|
| Characteristic | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Group |
|
| 0.02 |
|
| 0.03 |
|
Non-sarcopenia | 0.62 | 0.42-0.92 |
| 0.63 | 0.42-0.95 |
|
|
Sarcopenia | 1 |
|
| 1 |
|
|
| Sex |
|
| 0.80 |
|
|
|
|
Male | 1.05 | 0.71-1.55 |
|
|
|
|
|
Female | 1 |
|
|
|
|
|
| Performance
status |
|
| 0.45 |
|
|
|
| 0 | 0.85 | 0.57-1.28 |
|
|
|
|
| 1 | 1 |
|
|
|
|
|
| Clinical stage |
|
| 0.02 |
|
| 0.03 |
|
III | 0.59 | 0.38-0.91 |
| 0.62 | 0.39-0.97 |
|
| IV | 1 |
|
| 1 |
|
|
| Age, years |
|
| 0.88 |
|
|
|
|
≤75 | 1.03 | 0.66-1.61 |
|
|
|
|
|
>75 | 1 |
|
|
|
|
|
| BMI,
kg/m2 |
|
| 0.60 |
|
|
|
|
>22 | 1.11 | 0.74-1.69 |
|
|
|
|
|
≤22 | 1 |
|
|
|
|
|
| mGPS |
|
| 0.08 |
|
| 0.56 |
| 0 or
1 | 0.69 | 0.45-1.05 |
| 0.88 | 0.56-1.37 |
|
| 2 | 1 |
|
| 1 |
|
|
| Tumor
localization |
|
| 0.99 |
|
|
|
|
Head | 0.99 | 0.68-1.46 |
|
|
|
|
| Body or
tail | 1 |
|
|
|
|
|
| CA19-9, U/ml |
|
| 0.30 |
|
|
|
|
<628 | 0.82 | 0.56-1.20 |
|
|
|
|
|
≥628 | 1 |
|
|
|
|
|
| Table V.Factors related to overall
survival. |
Table V.
Factors related to overall
survival.
|
| Univariate
analysis | Multivariate
analysisa |
|---|
|
|
|
|
|---|
| Characteristic | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Group |
|
| 0.17 |
|
| 0.27 |
|
Non-sarcopenia | 0.76 | 0.51-1.13 |
| 0.79 | 0.53-1.20 |
|
|
Sarcopenia | 1 |
|
| 1 |
|
|
| Sex |
|
| 0.43 |
|
|
|
|
Male | 1.16 | 0.79-1.72 |
|
|
|
|
|
Female | 1 |
|
|
|
|
|
| Performance
status |
|
| 0.02 |
|
| 0.04 |
| 0 | 0.60 | 0.40-0.91 |
| 0.64 | 0.42-0.98 |
|
| 1 | 1 |
|
| 1 |
|
|
| Clinical stage |
|
| <0.01 |
|
| 0.01 |
|
III | 0.50 | 0.32-0.78 |
| 0.53 | 0.33-0.83 |
|
| IV | 1 |
|
| 1 |
|
|
| Treatment after
GnP |
|
| 0.05 |
|
|
|
|
Secondary treatment | 0.65 | 0.43-1.01 |
|
|
|
|
|
BSC | 1 |
|
|
|
|
|
| Age, years |
|
| 0.94 |
|
|
|
|
≤75 | 1.02 | 0.65-1.59 |
|
|
|
|
|
>75 | 1 |
|
|
|
|
|
| BMI,
kg/m2 |
|
| 0.24 |
|
|
|
|
<22 | 1.29 | 0.85-1.95 |
|
|
|
|
|
≥22 | 1 |
|
|
|
|
|
| mGPS |
|
| <0.01 |
|
| 0.13 |
| 0 or
1 | 0.49 | 0.32-0.76 |
| 0.69 | 0.43-1.11 |
|
| 2 | 1 |
|
| 1 |
|
|
| Tumor
localization |
|
| 0.69 |
|
|
|
|
Head | 0.92 | 0.64-1.35 |
|
|
|
|
| Body or
tail | 1 |
|
|
|
|
|
| CA19-9, U/ml |
|
| 0.19 |
|
|
|
|
<628 | 0.78 | 0.53-1.13 |
|
|
|
|
|
≥628 | 1 |
|
|
|
|
|
AEs
The incidences of AEs are shown in Table VI. The incidences of all grade AEs
and grade 3–4 AEs of hematologic toxicities were not significantly
different between the non-sarcopenia and sarcopenia groups.
| Table VI.Adverse events in the non-sarcopenia
and sarcopenia groups. |
Table VI.
Adverse events in the non-sarcopenia
and sarcopenia groups.
|
| Non-sarcopenia
(n=81) | Sarcopenia
(n=40) | P-value |
|---|
|
|
|
|
|
|---|
| Event | All grades | Grade 3/4 | All grades | Grade 3/4 | All grades | Grade 3/4 |
|---|
| Leukopenia, n
(%) | 73 (90) | 36 (44) | 36 (90) | 13 (33) | 1.0 | 0.24 |
| Neutropenia, n
(%) | 66 (81) | 50 (62) | 29 (73) | 19 (48) | 0.34 | 0.17 |
| Thrombocytopenia, n
(%) | 68 (84) | 5 (6) | 33 (83) | 0 (0) | 1.0 | 0.17 |
| Anemia, n (%) | 78 (96) | 21 (26) | 40 (100) | 5 (12.5) | 0.55 | 0.10 |
| Nausea, n (%) | 11 (14) | 1 (1) | 6 (15) | 0 (0) | >0.99 | >0.99 |
| Diarrhea, n
(%) | 10 (12) | 0 (0) | 6 (15) | 0 (0) | 0.78 | - |
| Constipation, n
(%) | 20 (25) | 0 (0) | 11 (28) | 0 (0) | 0.83 | - |
| Peripheral
neuropathy, n (%) | 55 (68) | 9 (11) | 26 (65) | 6 (15) | 0.84 | 0.57 |
| Anorexia, n
(%) | 22 (27) | 1 (1) | 15 (38) | 0 (0) | 0.30 | 1.0 |
| Malaise, n (%) | 25 (31) | 1 (1) | 11 (28) | 0 (0) | 0.83 | 1.0 |
Discussion
In this study, it was suggested that the evaluation
of SMI by BIA may be an indicator of the prognosis and therapeutic
effect of GnP. It has been reported that sarcopenia and
chemotherapeutic outcomes have relationships in various cancers,
including pancreatic cancer, and various evaluation methods have
been utilized for sarcopenia (30–34).
However, there have been no reports regarding the association of
sarcopenia on the outcomes of GnP for advanced pancreatic cancer
patients.
We noted a statistically significant difference in
the PFS between advanced pancreatic cancer patients with and
without sarcopenia, and a tendency toward a slight prolongation of
OS in the non-sarcopenia group. OS was affected not only by the
first-line treatment but also by the second-line treatment. In this
study, we observed a trend toward longer OS in patients who were
able to receive secondary treatment, although the difference was
not significant (HR 0.65; 95% CI 0.43-1.01). Approximately 74 and
73% of the patients in the sarcopenia and non-sarcopenia groups
received second-line treatment between, which was not significantly
different. Since secondary treatment was not limited, a wide
variety of treatment methods may have affected the OS. In addition,
only the SMI values before the first administration of the
chemotherapy regimen were available, so it was not possible to
evaluate changes in SMI values during the treatment course, which
may impact the prognosis (35).
Patients with advanced pancreatic cancer often have
a poor nutritional status due to cachexia (36). The relationship between cachexia,
malnutrition, and reduced SMI has been reported (37). Approximately one-third of
cancer-related deaths are reportedly due to malnutrition rather
than cancer (38). Cachexia and
malnutrition associated with cancer would reduce SMI and affect
secondary sarcopenia. Recently, a clinical trial focusing on
multimodal exercise, nutrition, and anti-inflammatory medication
for cachexia confirmed the importance of exercise and nutrition
therapy (39). Maintaining or
increasing skeletal muscle mass through nutritional or exercise
interventions may prevent sarcopenia and improve prognosis as well
as quality of life.
The mGPS is widely used as an indicator of
nutritional status (40). CRP and
albumin, the acute proteins that constitute the mGPS, are sensitive
and reliable markers that reflect the systemic inflammatory
response of cancer patients. The mGPS 0 is defined as normal or
symptomatically relieved hypocachexia, 1 as precachexia, and 2 as
cachexia or irreversible cachexia, which may reflect tumor
extension, necrosis, and undernutrition (41). A previous meta-analysis reported an
association between mGPS and OS and PFS in pancreatic cancer
patients (42). However, it was
not a significant prognostic factor in this study. In pancreatic
cancer, the mGPS may not necessarily reflect the disease state due
to increases in CRP from cholangitis or associated pancreatitis.
Hence, this study excluded patients with cholangitis or
pancreatitis showing apparent clinical symptoms, but SMI may be
useful in patients ineligible for evaluation by mGPS.
Regarding the relationship between sarcopenia and
efficacy of chemotherapy for pancreatic cancer, a decrease in
skeletal muscle mass, as measured by CT, was reported to be a
prognostic predictor in patients who received FOLFIRINOX as
second-line chemotherapy (43).
Other studies showed that gemcitabine alone and gemcitabine plus
erlotinib resulted in a significantly worse prognosis in patients
with sarcopenia than in those without (44). The lack of difference in AEs
between groups suggests that GnP was well tolerated and may be
useful for patients with low SMI. GnP may be a tolerable treatment
option for older patients with low SMI.
The optimal method for SMI measurement is
controversial. DEXA has the advantage of being able to measure
skeletal muscle mass throughout the body very accurately, but it
requires special equipment and has the disadvantages of radiation
exposure and excessive cost (45).
Measuring the SMI via CT is commonly used and has been reported to
be a useful method, although it is not completely consistent with
the BIA method. However, we believe that BIA is more effective in
terms of radiation exposure and cost (46,47).
The measurement of skeletal muscle mass by MRI has also been
reported as an effective method, but it has disadvantages such as
excessive cost, limited availability of facilities, long
examination time, and inability to be performed in patients with
claustrophobia (48). We chose BIA
because it is an inexpensive, simple, non-invasive measurement
method with high reproducibility.
BIA can be measured repeatedly, and it is easy to
check changes in SMI with active nutrition and exercise
intervention support as needed. In the future, prevention and
improvement of sarcopenia as well as chemotherapy are expected to
improve the prognosis of patients with pancreatic cancer, and BIA
may enable early detection of sarcopenia and early therapeutic
intervention. Furthermore, chemotherapy may trigger immune
responses mediated by tumor-specific T cells by stimulating
immunogenic cell death, and novel minimal drug nanoplatforms that
can stimulate the immunotherapeutic potential inherent in
gemcitabine could be developed (49). In the future, we will study the
association of SMI with other chemotherapy regimens and novel
agents.
There were some limitations in this study. First it
included only a small number of cases. Second, it was a
retrospective study. In the future, verification in a prospective
study with a larger sample size is desired. However, considering
previous reports, our study tends to correlate sarcopenia with
prognosis, which may be a reliable result. Third, we chose the
cutoff values based on Taiwanese adults without cancer. The cutoff
values were reliable because they study cohort also comprised East
Asians (Japanese individuals) with similar physical
characteristics. However, there may be more appropriate cutoff
values for pancreatic cancer patients. Fourth, some patients
received conversion surgery or radiotherapy as second-line
treatment, so the OS may not reflect the effect of chemotherapy,
and the cases were heterogeneous between the two groups. Fifth, the
cutoff values in this study tended to be less for female patients
with sarcopenia. The low number of females may have led to a lower
estimate of toxicity. Thus, the setting of cutoff values may need
to be examined.
In conclusion, SMI measured by BIA was indicative of
the PFS of patients with advanced pancreatic cancer who received
GnP as first-line treatment, suggesting its importance as a
prognostic factor in these patients. Therefore, it may be one of
the useful diagnostic methods of sarcopenia.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YT, MU and MM conceptualized this study. YT, MU and
SK analyzed the data. YT, MU and SK confirm the authenticity of all
the raw data. YT, TF, YS, KK, AH, ST, HA, SaM, SoM, SO and ShM
validated the results and investigated the data in the present
study. All authors participated in the writing of the manuscript.
All authors discussed the results and commented on the manuscript.
All authors read and approved the final version of the
manuscript.
Ethics approval and consent to
participate
The present study was approved by the Institutional
Review Board of Kanagawa Cancer Center (approval no. 2021-152).
Informed consent was obtained in the form of an opt-out form on the
website.
Patient consent for publication
Patient consent for publication was obtained in the
form of an opt-out form on the website.
Competing interests
Dr Ueno and Dr Kobayashi reports grants and personal
fees from Taiho Pharmaceutical. All the other authors declare that
they have no competing interests.
Glossary
Abbreviations
Abbreviations:
|
GnP
|
gemcitabine plus nab-paclitaxel
combination therapy
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
|
AEs
|
adverse events
|
|
BIA
|
bioimpedance analysis
|
|
HR
|
hazard ratio
|
|
CI
|
confidence interval
|
|
EWGSOP
|
European Working Group on Sarcopenia
in Older People
|
|
SMI
|
skeletal muscle index
|
|
CT
|
computed tomography
|
|
MRI
|
magnetic resonance imaging
|
|
DEXA
|
dual-energy X-ray absorptiometry
|
|
ECOG PS
|
Eastern Cooperative Oncology Group
Performance Status
|
|
BMI
|
body mass index
|
|
mGPS
|
modified Glasgow prognostic score
|
|
CA19-9
|
serum carbohydrate antigen 19-9
|
|
CRP
|
C-reactive protein
|
|
RDI
|
relative dose intensity
|
References
|
1
|
Rawla P, Sunkara T and Gaduputi V:
Epidemiology of pancreatic cancer: Global trends, etiology and risk
factors. World J Oncol. 10:10–27. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Tsai HJ and Chang JS: Environmental risk
factors of pancreatic cancer. J Clin Med. 8:14272019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ilic M and Ilic I: Epidemiology of
pancreatic cancer. World J Gastroenterol. 22:9694–9705. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cancer Statistics, . Cancer Information
Service, National Cancer Center, Japan (Vital Statistics of Japan,
Ministry of Health, Labour and Welfare). https://view.officeapps.live.com/op/view.aspx?src=https%3A%2F%2Fganjoho.jp%2Freg_stat%2Fstatistics%2Fdata%2Fdl%2Fexcel%2Fcancer_mortality(1958–2020).xls&wdOrigin=BROWSELINKMay
9–2022
|
|
5
|
Von Hoff DD, Ervin T, Arena FP, Chiorean
EG, Infante J, Moore M, Seay T, Tjulandin SA, Ma WW, Saleh MN, et
al: Increased survival in pancreatic cancer with nab-paclitaxel
plus gemcitabine. N Engl J Med. 369:1691–1703. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tempero MA, Malafa MP, Al-Hawary M,
Behrman SW, Benson AB, Cardin DB, Chiorean EG, Chung V, Czito B,
Del Chiaro M, et al: Pancreatic adenocarcinoma, version 2.2021,
NCCN clinical practice guidelines in oncology. J Natl Compr Canc
Netw. 19:439–457. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ueno H, Ikeda M, Ueno M, Mizuno N, Ioka
TE, Omuro Y, Nakajima T and Furuse J: Phase I/II study of
nab-paclitaxel plus gemcitabine for chemotherapy-naive Japanese
patients with metastatic pancreatic cancer. Cancer Chemother
Pharmacol. 77:595–603. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rosenberg IH: Sarcopenia: Origins and
clinical relevance. J Nutr. 127 (5 Suppl):990S–991S. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Fearon K, Strasser F, Anker SD, Bosaeus I,
Bruera E, Fainsinger RL, Jatoi A, Loprinzi C, MacDonald N,
Mantovani G, et al: Definition and classification of cancer
cachexia: An international consensus. Lancet Oncol. 12:489–495.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bauer J, Morley JE, Schols AMWJ, Ferrucci
L, Cruz-Jentoft AJ, Dent E, Baracos VE, Crawford JA, Doehner W,
Heymsfield SB, et al: Sarcopenia: A time for action. An SCWD
position paper. J Cachexia Sarcopenia Muscle. 10:956–961. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cruz-Jentoft AJ, Baeyens JP, Bauer JM,
Boirie Y, Cederholm T, Landi F, Martin FC, Michel JP, Rolland Y,
Schneider SM, et al: Sarcopenia: European consensus on definition
and diagnosis: Report of the European working group on sarcopenia
in older people. Age Ageing. 39:412–423. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen LK, Liu LK, Woo J, Assantachai P,
Auyeung TW, Bahyah KS, Chou MY, Chen LY, Hsu PS, Krairit O, et al:
Sarcopenia in Asia: Consensus report of the Asian working group for
sarcopenia. J Am Med Dir Assoc. 15:95–101. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Walowski CO, Braun W, Maisch MJ, Jensen B,
Peine S, Norman K, Müller MJ and Bosy-Westphal A: Reference values
for skeletal muscle mass-current concepts and methodological
considerations. Nutrients. 12:7552020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
González Correa CH, Marulanda Mejía F,
Castaño González PA, Vidarte Claros JA and Castiblanco Arroyabe HD:
Bioelectrical impedance analysis and dual x-ray absorptiometry
agreement for skeletal muscle mass index evaluation in sarcopenia
diagnosis. Physiol Meas. 41:0640052020. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
McSharry V, Glennon K, Mullee A and
Brennan D: The impact of body composition on treatment in ovarian
cancer: A current insight. Expert Rev Clin Pharmacol. 14:1065–1074.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
McSharry V, Mullee A, McCann L, Rogers AC,
McKiernan M and Brennan DJ: The impact of sarcopenia and low muscle
attenuation on overall survival in epithelial ovarian cancer: A
systematic review and meta-analysis. Ann Surg Oncol. 27:3553–3564.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sakamoto T, Yagyu T, Uchinaka E, Miyatani
K, Hanaki T, Kihara K, Matsunaga T, Yamamoto M, Tokuyasu N, Honjo S
and Fujiwara Y: Sarcopenia as a prognostic factor in patients with
recurrent pancreatic cancer: A retrospective study. World J Surg
Oncol. 18:2212020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ubachs J, Ziemons J, Minis-Rutten IJG,
Kruitwagen RFPM, Kleijnen J, Lambrechts S, Olde Damink SWM, Rensen
SS and Van Gorp T: Sarcopenia and ovarian cancer survival: A
systematic review and meta-analysis. J Cachexia Sarcopenia Muscle.
10:1165–1174. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yang M, Shen Y, Tan L and Li W: Prognostic
value of sarcopenia in lung cancer: A systematic review and
meta-analysis. Chest. 156:101–111. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ishida T, Makino T, Yamasaki M, Tanaka K,
Miyazaki Y, Takahashi T, Kurokawa Y, Motoori M, Kimura Y, Nakajima
K, et al: Impact of measurement of skeletal muscle mass on clinical
outcomes in patients with esophageal cancer undergoing
esophagectomy after neoadjuvant chemotherapy. Surgery.
166:1041–1047. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim IH, Choi MH, Lee IS, Hong TH and Lee
MA: Clinical significance of skeletal muscle density and sarcopenia
in patients with pancreatic cancer undergoing first-line
chemotherapy: A retrospective observational study. BMC Cancer.
21:772021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shachar SS, Deal AM, Weinberg M, Nyrop KA,
Williams GR, Nishijima TF, Benbow JM and Muss HB: Skeletal muscle
measures as predictors of toxicity, hospitalization, and survival
in patients with metastatic breast cancer receiving taxane-based
chemotherapy. Clin Cancer Res. 23:658–665. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM classification of malignant tumours. 7th edition.
Chichester, West Sussex, UK: Wiley-Blackwell; 2010
|
|
24
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chien MY, Huang TY and Wu YT: Prevalence
of sarcopenia estimated using a bioelectrical impedance analysis
prediction equation in community-dwelling elderly people in Taiwan.
J Am Geriatr Soc. 56:1710–1715. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Body mass index-BMI. World Health
Organization, regional office for Europe, . https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/body-mass-indexFebruary
13–2022
|
|
27
|
Imaoka H, Mizuno N, Hara K, Hijioka S,
Tajika M, Tanaka T, Ishihara M, Yogi T, Tsutsumi H, Fujiyoshi T, et
al: Evaluation of modified Glasgow prognostic score for pancreatic
cancer: A retrospective cohort study. Pancreas. 45:211–217. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schwartz LH, Litière S, de Vries E, Ford
R, Gwyther S, Mandrekar S, Shankar L, Bogaerts J, Chen A, Dancey J,
et al: RECIST 1.1-update and clarification: From the RECIST
committee. Eur J Cancer. 62:132–137. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Common Terminology Criteria for Adverse
Events (CTCAE) Version 5, . Published: November 27. US Department
of Health and Human Services, National Institutes of Health,
National Cancer Institute;
|
|
30
|
Ozola Zalite I, Zykus R, Francisco
Gonzalez M, Saygili F, Pukitis A, Gaujoux S, Charnley RM and Lyadov
V: Influence of cachexia and sarcopenia on survival in pancreatic
ductal adenocarcinoma: A systematic review. Pancreatology.
15:19–24. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Begini P, Gigante E, Antonelli G,
Carbonetti F, Iannicelli E, Anania G, Imperatrice B, Pellicelli AM,
Fave GD and Marignani M: Sarcopenia predicts reduced survival in
patients with hepatocellular carcinoma at first diagnosis. Ann
Hepatol. 16:107–114. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Vergara-Fernandez O, Trejo-Avila M and
Salgado-Nesme N: Sarcopenia in patients with colorectal cancer: A
comprehensive review. World J Clin Cases. 8:1188–1202. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhang XM, Dou QL, Zeng Y, Yang Y, Cheng
ASK and Zhang WW: Sarcopenia as a predictor of mortality in women
with breast cancer: A meta-analysis and systematic review. BMC
Cancer. 20:1722020. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Bundred J, Kamarajah SK and Roberts KJ:
Body composition assessment and sarcopenia in patients with
pancreatic cancer: A systematic review and meta-analysis. HPB
(Oxford). 21:1603–1612. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Choi Y, Oh DY, Kim TY, Lee KH, Han SW, Im
SA, Kim TY and Bang YJ: Skeletal muscle depletion predicts the
prognosis of patients with advanced pancreatic cancer undergoing
palliative chemotherapy, independent of body mass index. PLoS One.
10:e01397492015. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Vashi P, Popiel B, Lammersfeld C and Gupta
D: Outcomes of systematic nutritional assessment and medical
nutrition therapy in pancreatic cancer. Pancreas. 44:750–755. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lv Y, Ji ML, Feng QY, Zhu DX, Lin SB, Mao
YH, Xu YQ, Zheng P, He GD and Xu JM: Combined test of third lumbar
skeletal muscle index and prognostic nutrition index improve
prognosis prediction power in resected colorectal cancer liver
metastasis. Aging (Albany NY). 11:10301–10315. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
García-Luna PP, Parejo Campos J and
Pereira Cunill JL: Causes and impact of hyponutrition and cachexia
in the oncologic patient. Nutr Hosp. 21 (Suppl 3):S10–S16. 2006.(In
Spanish). PubMed/NCBI
|
|
39
|
Solheim TS, Laird BJA, Balstad TR, Stene
GB, Bye A, Johns N, Pettersen CH, Fallon M, Fayers P, Fearon K and
Kaasa S: A randomized phase II feasibility trial of a multimodal
intervention for the management of cachexia in lung and pancreatic
cancer. J Cachexia Sarcopenia Muscle. 8:778–788. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Proctor MJ, Morrison DS, Talwar D, Balmer
SM, O'Reilly DS, Foulis AK, Horgan PG and McMillan DC: An
inflammation-based prognostic score (mGPS) predicts cancer survival
independent of tumour site: A Glasgow inflammation outcome study.
Br J Cancer. 104:726–734. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Zhang H, Ren D, Jin X and Wu H: The
prognostic value of modified Glasgow prognostic score in pancreatic
cancer: A meta-analysis. Cancer Cell Int. 20:4622020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Fu W, Wang K, Yan S, Wang X, Tang B, Chang
J, Wang R and Wu T: Prognostic significance of the modified Glasgow
prognostic score in patients with pancreatic cancer: A
meta-analysis. Dose Response. 18:15593258209420652020. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Lee HS, Kim SY, Chung MJ, Park JY, Bang S,
Park SW and Song SY: Skeletal muscle mass predicts poor prognosis
in patients with advanced pancreatic cancer undergoing second-line
FOLFIRINOX chemotherapy. Nutr Cancer. 71:1100–1107. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Park I, Choi SJ, Kim YS, Ahn HK, Hong J,
Sym SJ, Park J, Cho EK, Lee JH, Shin YJ and Shin DB: Prognostic
factors for risk stratification of patients with recurrent or
metastatic pancreatic adenocarcinoma who were treated with
gemcitabine-based chemotherapy. Cancer Res Treat. 48:1264–1273.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Antonio J, Kenyon M, Ellerbroek A, Carson
C, Burgess V, Tyler-Palmer D, Mike J, Roberts J, Angeli G and
Peacock C: Comparison of dual-energy X-ray absorptiometry (DXA)
versus a multi-frequency bioelectrical impedance (InBody 770)
device for body composition assessment after a 4-week hypoenergetic
diet. J Funct Morphol Kinesiol. 4:232019. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Jones DJ, Lal S, Strauss BJ, Todd C,
Pilling M and Burden ST: Measurement of muscle mass and sarcopenia
using anthropometry, bioelectrical impedance, and computed
tomography in surgical patients with colorectal malignancy:
Comparison of agreement between methods. Nutr Cancer. 72:1074–1083.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Looijaard WGPM, Stapel SN, Dekker IM,
Rusticus H, Remmelzwaal S, Girbes ARJ, Weijs PJM and Oudemans-van
Straaten HM: Identifying critically ill patients with low muscle
mass: Agreement between bioelectrical impedance analysis and
computed tomography. Clin Nutr. 39:1809–1817. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chang MY, Park Y, Ha JW, Zhang HY and Lee
SH, Hong TH and Lee SH: Paraspinal lean muscle mass measurement
using spine MRI as a predictor of adjacent segment disease after
lumbar fusion: A propensity score-matched case-control analysis.
AJR Am J Roentgenol. 212:1310–1317. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Zhou S, Shang Q, Wang N, Li Q, Song A and
Luan Y: Rational design of a minimalist nanoplatform to maximize
immunotherapeutic efficacy: Four birds with one stone. J Control
Release. 328:617–630. 2020. View Article : Google Scholar : PubMed/NCBI
|