Introduction
Breast cancer (BC) is one of the most common
malignant tumors. There are ~2.2 million new cases of BC and
>680,000 deaths due to BC in the world every year (1). In China, 420,000 new cases of BC and
120,000 deaths from BC are registered per year (2,3).
Recently, the survival rate of patients with BC has been
significantly improved, with the cancer becoming one of the solid
tumors with the best curative effect following the development of
comprehensive BC treatments. However, there are still >100,000
BC-associated deaths in China annually, mainly due to recurrence
and distant metastasis (4,5).
Axillary lymph nodes (ALNs) are an important
prognostic factor for patients with BC, and ALN dissection (ALND)
has been widely used in clinical practice as a diagnostic criterion
to determine whether the ALNs are involved (6,7).
However, its large surgical range can easily cause complications,
such as lymphedema, hematoma formation, and restricted mobility
(8,9). The sentinel lymph nodes (SLNs) are
the first station or group of lymph nodes for drainage. As a
barrier to prevent tumor cells from spreading from the lymphatic
tract, the clinical significance of SLN has attracted increasing
attention (10). Moreover, SLN
biopsy (SLNB) is the standard procedure for axillary staging in
patients with clinically node-negative (cN0) BC. However, the
positive rate of cancer detection in SLNs in patients with cN0
stage BC receiving SLNB is between 20.5 and 25.5% (11,12).
Nevertheless, identifying non-invasive and suitable SLNB candidates
can be challenging. Although some studies have proposed
non-invasive or minimally invasive methods to determine SLN
metastasis in patients with BC, such as MRI (13,14),
cytokeratin 19 mRNA detection in peripheral blood (15) and Ras association domain family 1
isoform A methylation detection in tissues (16), there is no consensus on the use or
recommendation of these approaches in the National Comprehensive
Cancer Network guidelines due to lack of evidence (17).
Contrast-enhanced ultrasound (CEUS) is a technology
that enhances the echo of the backscatter using a contrast agent to
improve the resolution, sensitivity and specificity of ultrasound
diagnosis. CEUS can directly reflect the blood perfusion of
diseased and normal tissues, show the new abnormal blood vessels
that appear when the tumor rapidly progresses and play an important
role in the qualitative diagnosis of tumors (18,19).
Recently, a number of studies demonstrated that CEUS could be used
to non-invasively predict SLN metastasis in patients with early
stage BC (20,21), but it was rarely included in
previous SLN metastasis prediction models (22). Hence, in the present study, a model
was built to predict SLN metastasis based on CEUS and the basic
clinical features of patients with BC.
Patients and methods
Patients
First, the data of 365 patients with BC (all female)
hospitalized in the Cangzhou Central Hospital (Cangzhou, China)
between January 2017 and December 2018 were retrospectively
collected. These 365 patients comprised the training set (the
population used to build the model; age range, 24–83 years; mean
age, 52.07 years) and were divided into the SLN-negative
(no-metastasis; n=255) and SLN-positive (metastasis; n=110) groups
based on pathological results. Next, the data of 402 patients with
BC (all female) hospitalized in the Cangzhou Central Hospital
between January 2019 and April 2021 were prospectively collected
(age range, 23–79 years; mean age, 51.43 years). These 402 patients
were used as the prospective validation set to verify the SLN
status predictive model established using the training set.
Similarly, they were divided into SLN-negative (no-metastasis;
n=287) and SLN-positive (metastasis; n=115) groups based on
pathological results.
All recruited patients with BC (including patients
in the validation and training sets) met the following criteria.
The inclusion criteria were: i) Female sex; ii) no previous history
of other malignancies; iii) a pathological diagnosis of BC; iv)
cancer cells that have not metastasized to distant organs; v) the
first diagnosis of BC; and vi) a clear SLN status. The exclusion
criteria were: i) male sex; ii) radiotherapy and chemotherapy
received before surgery; iii) allergy to ultrasound contrast
agents; iv) pregnancy or breastfeeding; v) a previous history of
axillary surgery; and vi) severe heart or lung disease. This study
was approved by the Ethics Committee of the Cangzhou Central
Hospital, and clinical diagnoses and treatments complied with the
Helsinki Declaration.
Data collection
The age and menopause data of the patients with BC
were extracted from electronic medical records. Laboratory tests
included those for pathological type, tumor diameter, histological
grade, CEUS detection, and expression of estrogen receptor (ER),
progesterone receptor (PR), human epidermal growth factor receptor
2 (HER2) and Ki-67. SLNB was used to identify SLN+/- status.
Establishment of CEUS scoring
system
According to the CEUS performance, the patients with
BC were divided into four categories: Complete uniform enhancement
(type I), uniform enhancement of the periphery and medulla (type
II), uneven enhancement (type III) and no enhancement of the
periphery and/or medulla (type IV). In the training and prospective
validation sets, most patients with SLN-negative BC were type I,
followed by type II. By contrast, most patients with SLN-positive
BC were type IV, followed by type III.
Statistical analysis
In the present study, SPSS19.0 software (IBM Corp.)
was used for statistical analysis. Univariate binary regression
analysis was used for univariate analysis of categorical data, and
unconditional logistic regression was used for the multivariate
analysis, and the relative risk is expressed as odds ratio (OR) and
95% confidence intervals (CIs). Additionally, receiver operating
characteristic (ROC) curves were used to evaluate the predictive
value of the SLN status predictive model in the patients with BC.
The areas under the ROC curves (AUCs) were used to estimate the
predictive accuracy. The cut-off value was defined at the maximum
of the sum of sensitivity and specificity. P<0.05 was considered
to indicate a statistically significant difference.
Results
Baseline characteristics of patients
with BC in the training set
The baseline characteristics of the patients with BC
in the training set are presented in Table I. Patients with SLN-negative and
-positive BC significantly differed regarding the pathological
type, tumor diameter, menopause, ER expression, PR expression and
CEUS type. Namely, compared with the SLN-negative BC group, the
SLN-positive BC group had a higher proportion of infiltration, a
larger tumor diameter, a higher proportion of postmenopausal
patients, a higher proportion of ER-positive patients and a higher
proportion of PR-positive patients. Meanwhile, they did not differ
in age, histological grade, HER2 expression and Ki-67 expression
(P>0.05).
 | Table I.Baseline characteristics of
SLN-negative (n=255) and -positive (n=110) patients with breast
cancer in the training set (n=365). |
Table I.
Baseline characteristics of
SLN-negative (n=255) and -positive (n=110) patients with breast
cancer in the training set (n=365).
|
|
| SLN, n (%) |
|
|
|
|---|
|
|
|
|
|
|
|
|---|
| Characteristics | Total patients,
n | Negative | Positive | OR | 95% CI | P-valuea |
|---|
| Pathological
type |
|
|
|
|
|
|
|
Non-infiltration | 58 | 54 (93.10) | 4 (6.90) | 7.199 | 2.510-20.193 | <0.001 |
|
Infiltration | 307 | 201 (65.47) | 106 (34.53) |
|
|
|
| Tumor diameter,
cm |
|
|
|
|
|
|
| ≤2 | 133 | 107 (80.45) | 26 (19.55) | 2.336 | 1.409-3.872 | 0.001 |
|
>2 | 232 | 148 (63.79) | 84 (36.21) |
|
|
|
| Age, years |
|
|
|
|
|
|
| ≤50 | 230 | 158 (68.70) | 72 (31.30) | 0.860 | 0.539-1.372 | 0.526 |
|
>50 | 135 | 97 (71.85) | 38 (28.15) |
|
|
|
| Menopause |
|
|
|
|
|
|
| Yes | 228 | 146 (64.03) | 82 (35.97) | 0.457 | 0.279-0.751 | 0.002 |
| No | 137 | 109 (79.56) | 28 (20.44) |
|
|
|
| Histological
grade |
|
|
|
|
|
|
|
I+II | 288 | 202 (70.14) | 86 (29.86) | 1.064 | 0.617-1.833 | 0.824 |
|
III | 77 | 53 (68.83) | 24 (31.17) |
|
|
|
| ER |
|
|
|
|
|
|
|
Negative | 113 | 92 (81.42) | 21 (18.58) | 2.009 | 1.167-3.458 | 0.012 |
|
Positive | 252 | 163 (64.68) | 89 (35.32) |
|
|
|
| PR |
|
|
|
|
|
|
|
Negative | 136 | 108 (79.41) | 28 (20.59) | 2.152 | 1.311-3.532 | 0.002 |
|
Positive | 229 | 147 (64.19) | 82 (35.81) |
|
|
|
| HER2 |
|
|
|
|
|
|
|
Negative | 257 | 185 (71.98) | 72 (28.02) | 1.395 | 0.863-2.253 | 0.174 |
|
Positive | 108 | 70 (64.81) | 38 (35.19) |
|
|
|
| Ki-67 |
|
|
|
|
|
|
|
Negative | 71 | 55 (77.46) | 16 (22.54) | 1.616 | 0.879-2.968 | 0.122 |
|
Positive | 294 | 200 (68.03) | 94 (31.97) |
|
|
|
| CEUS type |
|
|
|
|
|
|
|
I+II | 223 | 213 (95.52) | 10 (4.48) | 50.714 | 24.454-105.176 | <0.001 |
|
III+IV | 142 | 42 (29.58) | 100 (70.42) |
|
|
|
Baseline characteristics of patients
with BC in the prospective validation set
The baseline characteristics of patients with BC in
the prospective validation set are shown in Table II. Similar to the training set,
patients with SLN-negative and -positive BC were significantly
different regarding the pathological type, tumor diameter,
menopause, ER expression, PR expression, Ki-67 expression, and CEUS
type (P<0.05). Namely, compared with the SLN-negative BC group,
the SLN-positive BC group had a higher proportion of infiltration,
a larger tumor diameter, a higher proportion of postmenopausal
patients, a higher proportion of ER-positive patients, a higher
proportion of PR-positive patients and a higher proportion of
Ki-67-positive patients. Meanwhile, they did not differ in age,
histological grade or HER2 expression (P>0.05).
| Table II.Baseline characteristics of
SLN-negative (n=287) and -positive (n=115) patients with breast
cancer in the prospective validation set (n=402). |
Table II.
Baseline characteristics of
SLN-negative (n=287) and -positive (n=115) patients with breast
cancer in the prospective validation set (n=402).
|
|
| SLN, n (%) |
|
|
|
|---|
|
|
|
|
|
|
|
|---|
|
Characteristics | Total patients,
n | Negative | Positive | OR | 95% CI |
P-valuea |
|---|
| Pathological
type |
|
|
|
|
|
|
|
Non-infiltration | 69 | 63 (91.30) | 6 (8.70) | 4.514 | 2.016-10.104 | <0.001 |
|
Infiltration | 333 | 224 (67.27) | 109 (32.73) |
|
|
|
| Tumor diameter,
cm |
|
|
|
|
|
|
| ≤2 | 150 | 123 (82.00) | 27 (18.00) | 1.825 | 1.279-2.606 | 0.001 |
| >2
to <3 | 165 | 108 (65.45) | 57 (34.55) |
|
|
|
| ≥3 | 87 | 56 (64.37) | 31 (35.63) |
|
|
|
| Age, years |
|
|
|
|
|
|
|
≤40 | 80 | 58 (72.50) | 22 (27.50) | 1.084 | 0.910-1.291 | 0.804 |
|
40-50 | 172 | 126 (73.26) | 46 (26.74) |
|
|
|
|
50-60 | 93 | 63 (67.74) | 30 (32.26) |
|
|
|
|
≥60 | 57 | 40 (70.18) | 17 (29.82) |
|
|
|
| Menopause |
|
|
|
|
|
|
|
Yes | 254 | 167 (65.75) | 87 (34.25) | 0.769 | 0.667-0.887 | 0.001 |
| No | 148 | 120 (81.08) | 28 (18.92) |
|
|
|
| Histological
grade |
|
|
|
|
|
|
| I | 13 | 10 (76.92) | 3 (23.08) | 0.929 | 0.836-1.033 | 0.768 |
| II | 300 | 211 (70.33) | 89 (29.67) |
|
|
|
|
III | 89 | 66 (74.16) | 23 (25.84) |
|
|
|
| ER |
|
|
|
|
|
|
|
Negative | 126 | 105 (83.33) | 21 (16.67) | 2.003 | 1.322-3.036 | <0.001 |
|
Positive | 276 | 182 (65.94) | 94 (34.06) |
|
|
|
| PR |
|
|
|
|
|
|
|
Negative | 150 | 121 (80.67) | 29 (19.33) | 1.672 | 1.187-2.355 | 0.002 |
|
Positive | 252 | 166 (65.87) | 86 (34.13) |
|
|
|
| HER2 |
|
|
|
|
|
|
|
Negative | 263 | 190 (72.24) | 73 (27.76) | 1.043 | 0.887-1.226 | 0.604 |
|
Positive | 139 | 97 (69.78) | 42 (30.22) |
|
|
|
| Ki-67 |
|
|
|
|
|
|
|
Negative | 79 | 63 (79.75) | 16 (20.25) | 1.578 | 0.953-2.612 | 0.043 |
|
Positive | 323 | 224 (69.35) | 99 (30.65) |
|
|
|
| CEUS type |
|
|
|
|
|
|
| I | 163 | 159 (97.55) | 4 (2.45) | 3.531 | 2.534-4.920 | <0.001 |
| II | 82 | 68 (82.93) | 14 (17.07) |
|
|
|
|
III | 102 | 45 (44.12) | 57 (55.88) |
|
|
|
| IV | 55 | 15 (27.27) | 40 (72.73) |
|
|
|
Establishment of the SLN status
predictive model
According to the results in Tables I and II, pathological type, tumor diameter
(≤2, 2–3, and ≥3 were assigned as 1, 2, and 3, respectively), age
(≤40, 40–50, 50–60 and ≥60 years were assigned as 1, 2, 3, and 4,
respectively), ER (negative and positive were assigned as 1 and 2,
respectively), PR (negative and positive were assigned as 1 and 2,
respectively), Ki-67 (negative and positive were assigned as 1 and
2, respectively) and CEUS type (types I, II, III and IV were
assigned as 1, 2, 3 and 4, respectively) were included into the
multivariate analysis to establish the predictive model for SLN
status. The model was as follows: (0.173 × tumor diameter)-(4.490 ×
menopause) + (2.322 × ER) + (5.445 × CEUS type). Moreover, the
independent predictors of SLN status in patients with BC included
tumor diameter (OR, 1.189; 95% CI, 1.124-1.257; P<0.001),
menopause (OR, 1.011; 95% CI, 0.603-1.436; P<0.001), ER
expression (OR, 3.199; 95% CI, 1.077-6.567; P=0.043) and CEUS type
(OR, 10.563; 95% CI, 6.890-28.372; P<0.001) (Table III). Overall, the model could be
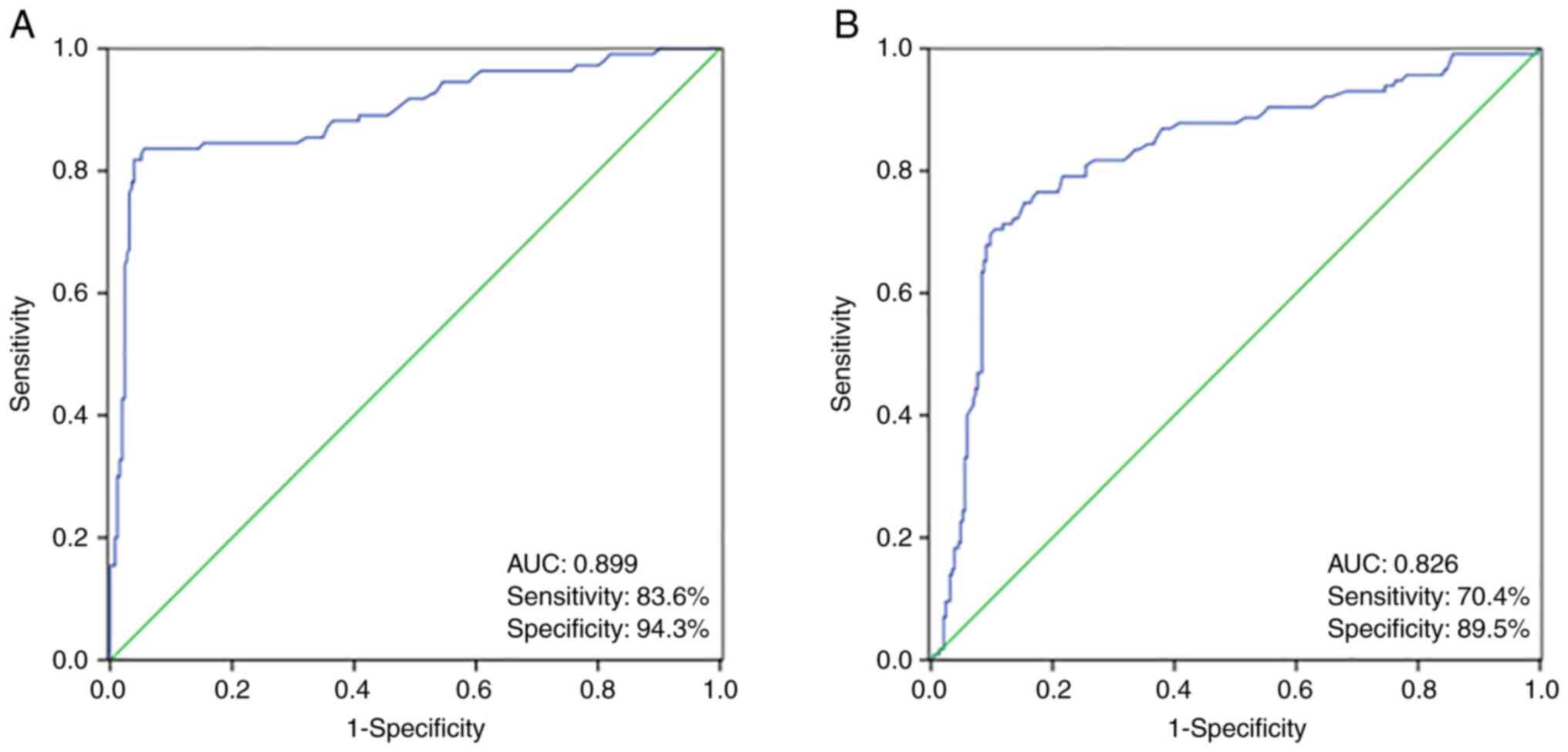
used to predict the SLN status of patients with BC. According to
SLN status using SLNB, the sensitivity and specificity of the model
for diagnosing SLN status could then be calculated (Fig. 1). The clinical data (tumor
diameter, menopause, ER and CEUS type) of one patient with BC were
substituted into the aforementioned formula (model) to obtain a
value, and if the value was >0, SLN positivity was predicted,
otherwise an SLN-negative status was predicted. In the training
set, the AUC, sensitivity and specificity were 0.899, 83.6 and
94.3%, respectively (Fig. 1A). In
the prospective validation set, the AUC, sensitivity and
specificity were 0.826, 70.4 and 89.5%, respectively (Fig. 1B).
| Table III.Multivariate analysis of CEUS,
clinical features and sentinel lymph node status. |
Table III.
Multivariate analysis of CEUS,
clinical features and sentinel lymph node status.
| Variables | Coefficient | S.E. | Wals | P-value | OR | 95% CI |
|---|
| Pathological
type | 1.048 | 0.568 | 3.402 | 0.065 | 2.851 | 0.936-8.677 |
| Tumor diameter | 0.173 | 0.028 | 36.805 | <0.001 | 1.189 | 1.124-1.257 |
| Age | −0.062 | 0.022 | 2.650 | 0.056 | 0.940 | 0.900-0.982 |
| Menopause | −4.490 | 0.599 | 56.287 | <0.001 | 1.011 | 0.603-1.436 |
| ER | 2.322 | 1.147 | 4.099 | 0.043 | 3.199 | 1.077-6.567 |
| PR | −4.845 | 1.545 | 3.838 | 0.062 | 0.008 | 0.000-0.162 |
| Ki-67 | −1.289 | 1.093 | 1.390 | 0.238 | 0.276 | 0.032-2.348 |
| CEUS type | 5.445 | 0.619 | 77.484 | <0.001 | 10.563 | 6.890-28.372 |
| Constant value | −1.952 | 0.948 | 1.009 | 0.315 | 0.386 |
|
Discussion
SLNB is a minimally invasive detection method that
can accurately determine the pathological status of the ALNs in
patients with early stage BC, preventing ALN-negative patients from
undergoing ALND, thereby reducing the incidence of postoperative
complications and improving the quality of life of patients after
surgery (23,24). Nevertheless, SLNB still has
postoperative complications, such as a 0–7% incidence of lymphedema
and a 20% incidence of upper limb numbness (25,26).
Furthermore, the radionuclide labeling, blue dye injection and
fluorescent dye methods used in SLNB are not only invasive, but
also have a low diagnostic accuracy rate due to the difficulty of
lymph node puncture (27,28). Moreover, performing SLNB for all
patients with wastes limited medical resources and increases the
financial burden on the patients. By contrast, SLN status is not
only necessary for the staging of patients with BC, but SLN burden
also has a strong effect on the outcome of invasive patients with
BC (29). Therefore, the
establishment of a model that can predict SLN metastasis is of
great significance to patients with BC. However, the
clinicopathological characteristics of SLN-positive patients are
similar to those of SLN-negative patients, which limits the ability
to predict lymph node metastasis before surgery (30).
In the present study, besides the
clinicopathological characteristics of BC patients, CEUS was
introduced to establish an SLN metastasis prediction model for
patients with BC. In CEUS detection, the contrast agent is
percutaneously injected and can conveniently pass through the
lymphatic endothelial cell space and enter lymphatic vessels
through a series of related processes, such as endocytosis and
exocytosis, and finally gathers in the lymph nodes of the drainage
area. Moreover, CEUS has proved to be helpful for the diagnosis of
SLN metastasis (31,32). Previous studies have divided the
mode of SLN transcutaneous CEUS enhancement into uniform, uneven
and no enhancement (32,33). The uniform enhancement is
characterized as benign, and the uneven and non-enhancement as
malignant. However, this classification method has very low
specificity in the diagnosis of SLN metastasis (52–78%) (32,33).
This might be related to the fact that some benign lymph nodes can
also show uneven enhancement. Therefore, uneven enhancement cannot
be simply diagnosed as a metastatic lymph node. The present study
first established the CEUS classification standard based on the
CEUS performance of 365 patients with BC in the training set:
Completely uniform enhancement (type I), uniform enhancement of the
periphery and medulla (type II), uneven enhancement (type III), and
no enhancement of the periphery and (or) medulla (type IV).
In both the retrospective training and prospective
validation sets, it was found that most patients with SLN-negative
BC were classified as type I, followed by type II, and that most
patients with SLN-positive BC were classified as type IV, followed
by type III. Considering the associations between SLN metastasis
and clinical characteristics, pathological type, tumor diameter,
age, ER expression, PR expression, Ki-67 expression and CEUS type
were included into the multiple regression analysis. Hence, a
simple model was established to predict SLN metastasis in patients
with BC, including tumor diameter, menopause, ER expression and
CEUS type. In the training and validation sets, the AUCs were 0.899
and 0.826, respectively, which suggested that this model had high
accuracy in predicting SLN metastasis in patients with BC (34,35).
At the same time, the model also had high sensitivity and
specificity in diagnosing SLN metastasis in training and validation
sets.
However, since the clinical data of the training set
was retrospectively analyzed when building the model, invasive
tests (CEUS) were included, indicating that the model can not work
under non-invasive conditions. Meanwhile, in the retrospective and
prospective validation sets, the sensitivity of the model was not
high (83.6 and 70.4%, respectively). Nevertheless, a predictive
model can be gradually revised as the sample size increases in the
future. Overall, in the present study, a model was established to
predict SLN metastasis in patients with BC based on tumor diameter,
menopausal status, ER expression and CEUS detection. However, one
limitation of the present study was that it did not have a test
set. In the future, larger scale clinical data in patients with BC,
including tumor diameter, menopausal status, ER expression and CEUS
detection, could be applied from other studies to evaluate the
model. In addition, a nomogram was not constructed for relapse in
the patients with BC (36), which
makes the results of this study difficult to understand for
non-specialists.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JX was responsible for the conception and design of
the study. JX and JL performed the experiments, analyzed the data
and confirm the authenticity of all the raw data. Both authors have
read and approved the final version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Cangzhou
Central Hospital Ethics Committee (Cangzhou, China). All patients
provided written informed consent.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2020. CA Cancer J Clin. 70:7–30. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Wong IO, Schooling CM, Cowling BJ and
Leung GM: Breast cancer incidence and mortality in a transitioning
Chinese population: Current and future trends. Br J Cancer.
112:167–170. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jian W, Shao K, Qin Q and Wang X, Song S
and Wang X: Clinical and genetic characterization of hereditary
breast cancer in a Chinese population. Hered Cancer Clin Pract.
15:192017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liao Y, Li D, Zhang N, Xia C, Zheng R,
Zeng H, Zhang S, Wang J and Chen W: Application of sandwich spatial
estimation method in cancer mapping: A case study for breast cancer
mortality in the Chinese mainland, 2005. Stat Methods Med Res.
28:3609–3626. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang Z, Bao J, Yu C, Wang J and Li C:
Secular trends of breast cancer in China, South Korea, Japan and
the United States: Application of the age-period-cohort analysis.
Int J Environ Res Public Health. 12:15409–15418. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Zhang Y, Li J, Fan Y, Li X, Qiu J, Zhu M
and Li H: Risk factors for axillary lymph node metastases in
clinical stage T1-2N0M0 breast cancer patients. Medicine
(Baltimore). 98:e174812019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hennigs A, Riedel F, Feißt M, Köpke M,
Rezai M, Nitz U, Moderow M, Golatta M, Sohn C and Heil J: Evolution
of the use of completion axillary lymph node dissection in patients
with T1/2N0M0 breast cancer and tumour-involved sentinel lymph
nodes undergoing mastectomy: A cohort study. Ann Surg Oncol.
26:2435–2443. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Taflampas P, Sanidas E, Christodoulakis M,
Askoxylakis J, Melissas J and Tsiftsis DD: Sealants after axillary
lymph node dissection for breast cancer: Good intentions but bad
results. Am J Surg. 198:55–58. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Madsen RJ, Esmonde NO, Ramsey KL and
Hansen JE: Axillary lymph node dissection is a risk factor for
major complications after immediate breast reconstruction. Ann
Plast Surg. 77:513–516. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Euscher E: Pathology of sentinel lymph
nodes: Historical perspective and current applications in
gynecologic cancer. Int J Gynecol Cancer. 30:394–401. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Malter W, Hellmich M, Badian M, Kirn V,
Mallmann P and Krämer S: Factors predictive of sentinel lymph node
involvement in primary breast cancer. Anticancer Res. 38:3657–3662.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen X, He Y, Wang J, Huo L, Fan Z, Li J,
Xie Y, Wang T and Ouyang T: Feasibility of using negative
ultrasonography results of axillary lymph nodes to predict sentinel
lymph node metastasis in breast cancer patients. Cancer Med.
7:3066–3072. 2018.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Liu C, Ding J, Spuhler K, Gao Y, Serrano
Sosa M, Moriarty M, Hussain S, He X, Liang C and Huang C:
Preoperative prediction of sentinel lymph node metastasis in breast
cancer by radiomic signatures from dynamic contrast-enhanced MRI. J
Magn Reson Imaging. 49:131–140. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dong Y, Feng Q, Yang W, Lu Z, Deng C,
Zhang L, Lian Z, Liu J, Luo X, Pei S, et al: Preoperative
prediction of sentinel lymph node metastasis in breast cancer based
on radiomics of T2-weighted fat-suppression and diffusion-weighted
MRI. Eur Radiol. 28:582–591. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Visser M, Jiwa M, Horstman A, Brink AA,
Pol RP, van Diest P, Snijders PJ and Meijer CJ: Intra-operative
rapid diagnostic method based on CK19 mRNA expression for the
detection of lymph node metastases in breast cancer. Int J Cancer.
122:2562–2567. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Abe M, Kagara N, Miyake T, Tanei T, Naoi
Y, Shimoda M, Shimazu K, Kim SJ and Noguchi S: Highly sensitive
detection of sentinel lymph node metastasis of breast cancer by
digital PCR for RASSF1A methylation. Oncol Rep. 42:2382–2389.
2019.PubMed/NCBI
|
|
17
|
Gradishar WJ, Anderson BO, Abraham J, Aft
R, Agnese D, Allison KH, Blair SL, Burstein HJ, Dang C, Elias AD,
et al: Breast cancer, version 3.2020, NCCN clinical practice
guidelines in oncology. J Natl Compr Canc Netw. 18:452–478. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Buchtele N, Staudinger T, Schwameis M,
Schörgenhofer C, Herkner H and Hermann A; UltraECMO investigators,
: Feasibility and safety of watershed detection by
contrast-enhanced ultrasound in patients receiving peripheral
venoarterial extracorporeal membrane oxygenation: A prospective
observational study. Crit Care. 24:1262020. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Spiesecke P, Fischer T, Maxeiner A, Hamm B
and Lerchbaumer MH: Contrast-enhanced ultrasound (CEUS) reliably
rules out neoplasm in developmental renal pseudotumor. Acta Radiol.
62:821–829. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Li C, Yao M, Shao S, Li X, Li G and Wu R:
Diagnostic efficacy of contrast-enhanced ultrasound for breast
lesions of different sizes: A comparative study with magnetic
resonance imaging. Br J Radiol. 93:201909322020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen C, Wang Y, Niu J, Liu X, Li Q and
Gong X: Domain knowledge powered deep learning for breast cancer
diagnosis based on contrast-enhanced ultrasound videos. IEEE Trans
Med Imaging. 40:2439–2451. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang L, Li J, Qiao J, Guo X, Bian X, Guo
L, Liu Z and Lu Z: Establishment of a model for predicting sentinel
lymph node metastasis in early breast cancer based on
contrast-enhanced ultrasound and clinicopathological features.
Gland Surg. 10:1701–1712. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Poodt IGM, Walstra CJEF, Vugts G,
Maaskant-Braat AJG, Voogd AC, Schipper RJ and Nieuwenhuijzen GAP;
Sentinel Node and Recurrent Breast Cancer (SNARB) study Group, :
Low risk of development of a regional recurrence after an
unsuccessful repeat sentinel lymph node biopsy in patients with
ipsilateral breast tumor recurrence. Ann Surg Oncol. 26:2417–2427.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Oaks ZA, Goyal S, Liu Y, Hayes KR, Gupta
GP, Patel SA and Royce TJ: Sentinel lymph node biopsy (SLNB) versus
axillary lymph node dissection in US women with breast cancer and
persistently positive lymph nodes following neoadjuvant
chemotherapy. Int J Radiat Oncol Biol Phys. 108 (Suppl):e24–e25.
2020. View Article : Google Scholar
|
|
25
|
Qiu PF, Liu YB and Wang YS: Internal
mammary sentinel lymph node biopsy: Abandon or persist? Onco
Targets Ther. 9:3879–3882. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ugras S, Matsen C, Eaton A, Stempel M,
Morrow M and Cody HS III: Reoperative sentinel lymph node biopsy is
feasible for locally recurrent breast cancer, but is it worthwhile?
Ann Surg Oncol. 23:744–748. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Dasgupta P, Youl PH, Pyke C, Aitken JF and
Baade PD: Sentinel node biopsy for early breast cancer in
Queensland, Australia, during 2008–2012. ANZ J Surg. 88:E400–E405.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Goonawardena J, Yong C and Law M: Use of
indocyanine green fluorescence compared to radioisotope for
sentinel lymph node biopsy in early-stage breast cancer: Systematic
review and meta-analysis. Am J Surg. 220:665–676. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Meattini I, Desideri I, Saieva C,
Francolini G, Scotti V, Bonomo P, Greto D, Mangoni M, Nori J,
Orzalesi L, et al: Impact of sentinel node tumor burden on outcome
of invasive breast cancer patients. Eur J Surg Oncol. 40:1195–1202.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Caudle AS, Yi M, Hoffman KE, Mittendorf
EA, Babiera GV, Hwang RF, Meric-Bernstam F, Sahin AA and Hunt KK:
Impact of identification of internal mammary sentinel lymph node
metastasis in breast cancer patients. Ann Surg Oncol. 21:60–65.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Gkegkes ID and Lavazzo C: Contrast
enhanced ultrasound (CEU) using microbubbles for sentinel lymph
node biopsy in breast cancer: A systematic review. Acta Chir Belg.
115:212–218. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhao J, Zhang J, Zhu QL, Jiang YX, Sun Q,
Zhou YD, Wang MQ, Meng ZL and Mao XX: The value of
contrast-enhanced ultrasound for sentinel lymph node identification
and characterisation in pre-operative breast cancer patients: A
prospective study. Eur Radiol. 28:1654–1661. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Xie F, Zhang D, Cheng L, Yu L, Yang L,
Tong F, Liu H and Wang S and Wang S: Intradermal microbubbles and
contrast-enhanced ultrasound (CEUS) is a feasible approach for
sentinel lymph node identification in early-stage breast cancer.
World J Surg Oncol. 13:3192015. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cook NR: Use and misuse of the receiver
operating characteristic curve in risk prediction. Circulation.
115:928–935. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Hajian-Tilaki K: Receiver operating
characteristic (ROC) curve analysis for medical diagnostic test
evaluation. Caspian J Intern Med. 4:627–635. 2013.PubMed/NCBI
|
|
36
|
Iasonos A, Schrag D, Raj GV and Panageas
KS: How to build and interpret a nomogram for cancer prognosis. J
Clin Oncol. 26:1364–1370. 2008. View Article : Google Scholar : PubMed/NCBI
|