Introduction
Hepatocellular carcinoma (HCC) is one of the most
common types of cancer diagnosed worldwide (1). For several years, the only treatment
option for patients with advanced disease was sorafenib (2,3).
However, more recently, promising results have been obtained from
trials with immunotherapy. For example, the use of atezolizumab
with bevacizumab provided better outcomes than sorafenib (4). Since immunotherapy may be associated
with clinical benefits in certain patients, it is essential to
identify reliable predictive biomarkers of treatment response.
Therefore it is crucial to better understand the molecular and
microenvironmental characteristics of the tumor.
Carcinogenesis is associated with cirrhosis, chronic
inflammation, injuries, and regeneration of hepatocytes (5). The interplay between hepatocytes and
immune cells depends on the tumor microenvironment which forms the
complex network involved in hepatocarcinogenesis. Within this
network most of the cells are hepatocytes, but fibroblasts,
endothelial cells and immune cells [such as tumor-associated
macrophages, T lymphocytes] also play a critical role. The
microenvironment also includes growth factors, enzymes, and
extracellular matrix proteins, and cytokines may also contribute to
carcinogenesis (6). Due to the
association between the gut and liver, the microbiome may also play
a role in forming the tumor microenvironment (7).
In this review, we have summarized the basic data
regarding immune cells and their role in hepatocarcinogenesis.
Tumor-infiltrating leukocytes (TILs) include several populations of
cells with different roles. Some of these may have antitumor
effects, while others may be associated with the progression of the
disease. The most important subsets include tumor-associated
macrophages (TAMs), tumor-associated neutrophils (TANs), and T
lymphocytes, and are briefly described in Table I. Furthermore, we briefly focused
on the prognostic and predictive factors associated with outcomes
of immunotherapy.
 | Table I.Summary of immune cells and their
potential impact on the treatment and prognosis of HCC. |
Table I.
Summary of immune cells and their
potential impact on the treatment and prognosis of HCC.
| Cell type | Impact | Potential
prognostic/predictive factor | (Refs.) |
|---|
| MDSCs | Negative impact on
immunoregulation | Yes | (10–14) |
|
| Increased
neoangiogenesis |
|
|
|
| M2
polarization |
|
|
|
| Targeting MDSCs are
associated with increased response to sorafenib |
|
|
|
| Higher MDSC levels
are inversely correlated with overall and relapse-free
survival |
|
|
| TAMs |
|
|
|
| M1
macrophages (pro-inflammatory) | Antitumor response,
but CD68+ M1 | Yes | (16,17,26) |
|
| TAMs may be
associated with the induction of PD-L1 in HCC cells (pro-tumor
role) |
|
|
| M2
macrophages (anti-inflammatory) | Promotion of tumor
progression | Yes | (18,19,23,24,30) |
|
| Enhanced
angiogenesis and metastasis |
|
|
|
| Poorer
prognosis |
|
|
|
| Resistance to
sorafenib |
|
|
| TILs |
|
|
|
| NK
cells | Targets tumor cells
to prevent tumor | Yes | (38) |
| Cytotoxic T
lymphocytes (CD8+) | progression | Yes | (38,43) |
| Regulatory T
lymphocytes (CD4+) | May promote immune
tolerance and inhibit the anti-tumor-promoting roles of other
cells | Yes | (36,39) |
|
| Promotes disease
progression by promoting angiogenesis |
|
|
| TANs | Able to promote or
inhibit the progression of the disease | Yes | (51,52) |
|
| Resistance to
sorafenib |
|
|
Myeloid-derived suppressor cells
(MDSCs)
MDSCs are a heterogeneous subset of myeloid cells
that play an essential role in the immunosuppressive network. MDSCs
may differentiate into granulocytes, dendritic cells, and
macrophages. Due to the hypoxic microenvironment, the process of
differentiation can be prevented in HCC (8,9). It
was observed that in patients with HCC, MDSCs inhibit T-cell
proliferation and induce T-regulatory cells (10). The proliferation of T cells is
inhibited through the depletion of arginine due to increased
arginase activity. Furthermore, the production of matrix
metallopeptidase 9 (MMP-9) by MDSCs contributes to increased
neoangiogenesis through increasing vascular endothelial growth
factor (VEGF) bioavailability (11). MDSCs can secrete IL-10, which
results in M2 polarization as well as inhibition of natural killer
(NK) cells, CD4+ and CD8+ lymphocytes through
the expression of transforming growth factor β (TGF-β) (12,13).
In a mouse model, targeting MDSCs was associated with a better
response to sorafenib (14). A
recent meta-analysis highlighted several observations. Firstly, the
percentage of MDSCs in HCC patients was higher than in healthy
individuals or patients with other chronic liver diseases.
Moreover, higher quantities of MDSCs were inversely correlated with
overall survival (OS) and relapse-free survival (RFS).
Tumor-associated macrophages (TAMs)
The population of liver macrophages includes Kupffer
cells that reside within the liver and originate from the yolk sack
and infiltrating hematopoietic stem cells/bone marrow-derived
monocytes. TAMs are derived from monocytes recruited at the tumor
site by molecules produced by neoplastic or stromal cells (15). However, they may be associated with
a poorer prognosis, as some TAMs exhibit antitumor properties.
There are two subsets of TAMs.
M1 macrophages are activated by cytokines such as
interferon (IFN)-γ, tumor necrosis factor (TNF)-α, and
granulocyte-macrophage colony-stimulating factor (GM-CSF), or in
response to microbial infection. This mechanism is vital for
pro-inflammatory and antitumor responses. Production of interleukin
(IL)-12 and other pro-inflammatory cytokines leads to the
initiation of a Th-1 dependent immune response. They are also
capable of cytotoxic activity against cancer cells (16,17).
Conversely, M2 macrophages play an anti-inflammatory
role and are associated with the promotion of tumor progression.
They may be alternatively activated by IL-4, IL-10, IL-13, or
macrophage colony-stimulating factor (M-CSF), and glucocorticoid
hormones. M2-like macrophages are further sub-divided into four
subtypes, with different roles (18,19).
M2a macrophages are involved in tissue repair as well as cell
growth and endocytic processes. M2b cells regulate the immune
response. M2c cells are responsible for apoptosis. Finally, M2d
macrophages enhance tumor growth and angiogenesis (20). TAMs may secrete pro-angiogenic
cytokines such as VEGF, TGF-β, or platelet-derived growth factor
(PDGF) which contributes to the progression of cancer (21). Promoting tumor progression by M2
macrophages is associated with increased recruitment of regulatory
T cells leading to the suppression of T effector cells. This
mechanism results from the secretion of cytokines such as IL-10,
TGF-β, or chemokines such as C-C motif chemokine ligand (CCL)17,
CCL18, CCL22, and CCL24 (22).
A high count of M2 cells is associated with enhanced
angiogenesis and metastasis, which leads to a poorer prognosis.
Moreover, the production of IL-17 by M2 TAMs has been shown to
suppress oxaliplatin-induced apoptosis in HCC (23,24).
It was suggested that CD206+ M2, but not
CD68+ TAMs may be used as a prognostic biomarker in HCC
(25). A recently published study
indicated that CD68+ M1 TAMs are associated with the
induction of programmed death-ligand 1 (PD-L1) in HCC cells, which
suggest they possessed a pro-tumor role (26). Another analysis showed that
CD68+ TAMs were associated with a poor prognosis
(27). These results highlight the
need for further investigations.
There are several mechanisms involved in immune
suppression associated with TAMs. One of these is the interaction
with PD-L1, which was confirmed in vivo in mouse models
where TAM-derived PD-L1 contributed more significantly to
suppressing antitumor immunity than the host-derived PD-L1
(28). PD-L2 expressed by TAMs is
also involved in suppressing the host antitumor response in the
murine microenvironment (29).
It is suggested that TAMs are involved in resistance
to sorafenib through sustaining tumor growth and metastasis by
secreting hepatocyte growth factor (HGF). This in turn may activate
the HGF/c-Met, ERK1/2/MAPK, and PI3K/AKT pathways in tumor cells.
An interesting concept would be combining sorafenib with HGF
inhibitors such as cabozantinib to improve treatment outcomes
(30).
Most of the TAMs within the tumor microenvironment
are M2 macrophages. Since M2 cells promote tumor development,
downregulate M1 functions and adaptive immunity, and favor
angiogenesis and regeneration of tissues, they could be a potential
target for novel therapies. In a rat model, zoledronic acid
treatment enhanced the effects of transarterial chemoembolization
by inhibiting TAM infiltration and tumor angiogenesis (31).
As TAMs may influence tumor progression, several
studies have attempted to neutralize their role. One of the
approaches is to re-educate TAMs using the M-CSF receptor with
pexidartinib (PLX3397), which inhibited tumor growth and increased
the CD8+ lymphocyte count (32). In a preclinical setting, another
agent that proved efficacious was baicalin
(8-bromo-7-methoxychrysin) (33).
Tocilizumab inhibits IL-6 produced by TAMs, which may contribute to
the suppression of tumorigenesis (34). Inhibition of TAM recruitment was
also suggested as a therapeutic option; this has been tested in
studies targeting chemokine receptor type 2 (CCR2) antagonists and
showed promising results (35,36).
Tumor-infiltrating leukocytes (TILs)
TILs may be involved in the antitumor responses
through the direct mechanisms of the adaptive immune system and
modulation of the innate response or angiogenesis (37). Various cell subsets play different
roles. First, NK cells and cytotoxic T lymphocytes are able to
target tumor cells and thus prevent their progression, especially
in the early stages. Later, the antitumor response is less
pronounced, which correlates with patient prognosis (38).
Another subset of cells, regulatory T lymphocytes
(Tregs, CD4+), may promote immune tolerance and inhibit
the antitumor roles of other cells. One of these mechanisms is the
secretion of TGF-β and IL-10, which inhibits CD8+
T-cells (39). One subset, Th-17
cells, secrete IL-17 and this promotes disease progression by
inducing angiogenesis, which is associated with poorer outcomes
(36).
One of the roles of cytotoxic CD8+
lymphocytes is to prevent tumor progression by killing cancer
cells. However, in the case of prolonged exposure to antigens,
CD8+ lymphocytes differentiate into so-called exhausted
CD8+ cells with impaired cytotoxic functions (40). These exhausted CD8+
cells may be associated with decreased expression of cytokines, but
also with increased expression of inhibitory receptors, including
programmed cell death 1 (PD-1), lymphocyte-activation gene 3,
cytotoxic T lymphocyte-associated antigen (CTLA-4), and T cell
immunoglobulin domain (41,42).
TILs with high levels of PD-1 expression exhibit higher expression
levels of genes regulating T-cell exhaustion (43).
The low presence of intratumoral Tregs with high
intratumoral activated CD8+ cytotoxic cells (CTLs) was
found to be associated with improved disease-free survival (DFS)
and OS (44). This is supported by
the observation, that increased levels of regulatory T cells were
correlated with CD8+ T-cell impairment and poor survival
in HCC patients (45). Low
CD8+ cell counts were found to be associated with poorer
survival in another study (46).
It was also observed, that CD8+ infiltration was
associated with a so-called ‘immune cell stroma’ HCC type, which in
comparison with ‘conventional stroma’, is characterized by the lack
of catenin β1 (CTNNB1) mutations, global hypermethylation,
expression of PD-1 and PD-L1 in TILs, and expression of PD-L1 in
tumors. This type was also associated with an improved prognosis
(47). The results of several
studies indicate that the inhibition of Treg-induced suppression
may be effective in restoring antitumor immune responses in several
types of cancer (48–50).
Tumor-associated neutrophils (TANs)
The role of TANs in carcinogenesis is complex. TANs
can promote as well as inhibit the progression of the disease,
dependent on the cytokines released. The secretion of CCL-2 or
CCL17 is associated with poorer outcomes. Those cytokines may also
promote the infiltration of Tregs and macrophages. This
infiltration negatively correlates with survival. It is suggested
that TANs are involved in sorafenib resistance (49). In vitro, when HCC cell lines
were cocultured with TANs, colony formation, cell migration,
invasion, and sphere formation were enhanced, while apoptosis was
inhibited.
There is growing evidence, that miRNAs may regulate
tumor progression in HCC. For example, miR-301b-3p was correlated
with the tumor size and advanced stages of the disease. Knockdown
of miR-301b-3p reduced proliferation, induced cell cycle arrest in
the G2/M phase, and induced apoptosis. Furthermore, TANs secrete
bone morphogenetic protein 2 and TGF-β2 and increased miR-301-3p
expression in HCC cells, which subsequently suppressed gene
expression of limbic system-associated membrane protein (LSAMP) and
CYLD lysine 63 deubiquitinase (CYLD), and increased the acquisition
of stem cell characteristics in HCC cells. TAN-induced HCC
stem-like cells were hyperactive and further increased TAN
infiltration, suggesting a positive feedback loop. In clinical HCC
samples, increased quantities of TANs were correlated with elevated
miR-301b-3p levels, decreased LSAMP and CYLD expression, and
increased nuclear p65 accumulation and C-X-C motif chemokine ligand
5 (CXCL5) expression, all of which were associated with patient
outcomes (50).
Tumor microenvironment and the response to
systemic treatment
Sorafenib has been the standard of care for advanced
HCC for several years. However, there are several challenges
associated with sorafenib treatment, including low response rates,
toxicity, and acquisition of drug resistance. The tumor
microenvironment plays an essential role in mechanisms associated
with resistance. Several studies have demonstrated that the
infiltration of TANs and TAMs may be correlated with the
sensitivity to sorafenib (51).
Furthermore, treatment with sorafenib results in hypoxia related to
the depletion of pericytes and a decreased number of vessels. It is
suggested that sorafenib-induced hypoxia may be associated with
subsequent exosome-mediated resistance to sorafenib (52). Characterization of the tumor
microenvironment has led to the division of HCC into four immune
subclasses. About 20% of patients present with an immunogenic
subclass characterized by massive T cell infiltration and
activation of the immune checkpoint pathway. These patients exhibit
the best response not only to immunotherapy, but also to sorafenib
(53).
In 2018, the results of a phase III trial with
lenvatinib showed it to be effective in the first-line treatment of
HCC. It was also evaluated in combination with immunotherapy.
Lenvatinib reduced the number of TAMs and increased the percentage
of activated CD8+ T cells secreting IFN-γ+
and granzyme B. It is worth noting that the exhaustion of
CD8+ lymphocytes is one of the mechanisms involved in
immune escape and cancer development. On the other hand, it is
regulated by the PD-1 signaling (54). These findings provide a scientific
rationale for the combination therapy of lenvatinib with PD-1
blockade (55). In a mouse model
of HCC, the immunomodulatory activity of lenvatinib led to an
enhanced response to anti-PD-1 treatment. In 2021, it was also
suggested in a small retrospective study in which patients with HCC
received lenvatinib with pembrolizumab or nivolumab (56,57).
Immune checkpoint inhibition
Immune checkpoint molecules control the immune
response. One of the most important seems to be the PD-1 receptor,
which typically is induced on activated T cells, NK cells, B cells,
and antigen-presenting cells. Conversely, PD-L1 is expressed by
tumor cells, hepatocytes, hepatic stellate cells, and Kupffer cells
or liver sinusoidal cells (58).
PD-L2 is another known ligand for PD-1, and it is present on
dendritic cells. Complex interactions between ligands and receptors
dependent on the signals from the microenvironment lead to either
cancer development or apoptosis.
Evidence from several studies indicates that
patients with higher expression of PD-L1 on tumor cells or immune
cells are more likely to achieve benefits from treatment with
checkpoint blockade (59,60).
The impact of PD-1/PD-L1 on the prognosis and
treatment outcomes in HCC has been studied in several studies.
However, the results have proven to be conflicting, and the
underlying mechanism is not fully understood. It has been shown
that patients with high expression of PD-L1 and a high TIL presence
tend to have better prognoses, whereas low expression of PD-L1 and
galectin-9 and low CD8+ TIL counts are associated with
poor HCC-specific survival (46).
On the other hand, the results of another study, where the PD-L1
expression was correlated with clinical and pathological features
suggested that PD-L1 expression by either neoplastic or
intratumoral inflammatory cells was associated with tumor
aggressiveness (61). These
conflicting results clearly show the need for further investigation
of the immune landscape of the HCC microenvironment.
Of note, it has been suggested that stratifying
tumors according to the expression of PD-L1 and TILs could be
helpful for predicting the response to treatment. Type 1 cancers
are characterized by PD-L1+TILs+, and benefit
from the single-agent anti-PD-1/L1 blockade. Type 2 cancers
(PD-L1−TIL−) have been predicted to have poor
responses to single-agent immunotherapy and poorer prognoses. In
type 3 cancers (PD-L1+TIL−), PD-L1 positivity
is not a single predictive factor for determining the response to
anti-PD-1/PD-L1 treatment, as without TILs, a reaction to blocking
PD1/L1 is unlikely. Finally, other suppressive mechanisms may be
dominant for type 4 cancers (PD-L1−TIL+)
(62). Thus, a simple distinction
between the presence or absence of TILs or PD-L1 may not be
sufficient. It is well established that other immune checkpoint
molecules may be co-expressed on T cells. For example, lymphocyte
activation gene-3 (LAG-3), a negative regulator of T cells is also
expressed on T cells and its inhibition increases the antitumor
response (63). It has been shown
that HCCs may contain CD8+ T cells that express
different levels of PD-1. Those cells with a discrete population of
PD-1 high CD8+ T cells express T cell immunoglobulin and
mucin-domain-containing protein-3 (TIM-3) or LAG-3 and can produce
low levels of IFN-γ or TNF in response to anti-CD3. Incubation of
these cells with antibodies against PD1 and TIM-3 or LAG-3 further
restored proliferation and production of cytokines. The results of
this study indicate that HCCs with a discrete population of
PD1-high CD8+ T cells may be more susceptible to
combined immune checkpoint blockade-based therapies (43).
Kurebayashi et al suggested that the tumor
microenvironment can be classified into three subtypes based on
immunohistochemical analyses of the immune regulatory molecules;
namely, Immune-high, Immune-mid, and Immune-low. The Immune-high
subtype is characterized by increased B-/plasma-cell and T-cell
infiltration. The Immune-high subtype and B-cell infiltration were
identified as independent positive prognostic factors. Furthermore,
the Immune-high subtype was found to be associated with poorly
differentiated HCC, cytokeratin 19 (CK19)+, or Sal-like
protein 4 (SALL4)+ high-grade HCC, and Hoshida's
S1/Boyault's G2 subclasses. Finally, patients with high-grade HCC
of the predominant Immune-high subtype had significantly better
prognoses. The Immune-mid subtype is characterized by moderately
increased T-cell and other immune cell infiltration with lesser B-
and plasma-cell infiltration, while the Immune-low subtype is
associated with even lower levels of infiltration. Depending on the
Treg/CD4+ ratio, the Immune-low type was subdivided into
2 classes (1-lower Treg/CD4+ ratio; 2-higher) (64).
As mentioned above, TIM-3 is another regulatory
molecule that plays a role in tumor progression. Its levels may be
increased in CD4+ and CD8+ cells or TAMs, and
this is correlated with a poorer prognosis. On the other hand, its
suppression resulted in an increased antitumor response (13).
Immune checkpoint inhibitors assessed for
treatment of HCC
Recently several immune checkpoint inhibitors have
been evaluated as treatments for HCC. Most of the studies have
focused on PD-1/PD-L1 inhibitors and CTLA-4 inhibitors. Anti-PD-1
treatment with monoclonal antibodies was found to result in the
blockade of PD-1 interaction with PD-L1 or PD-L2 expressed in
antigen-presenting cells, which is involved in the T-cell
antitumoral response. Checkpoint inhibition enhances T-cell
response and normalizes the immune response within the
microenvironment (65).
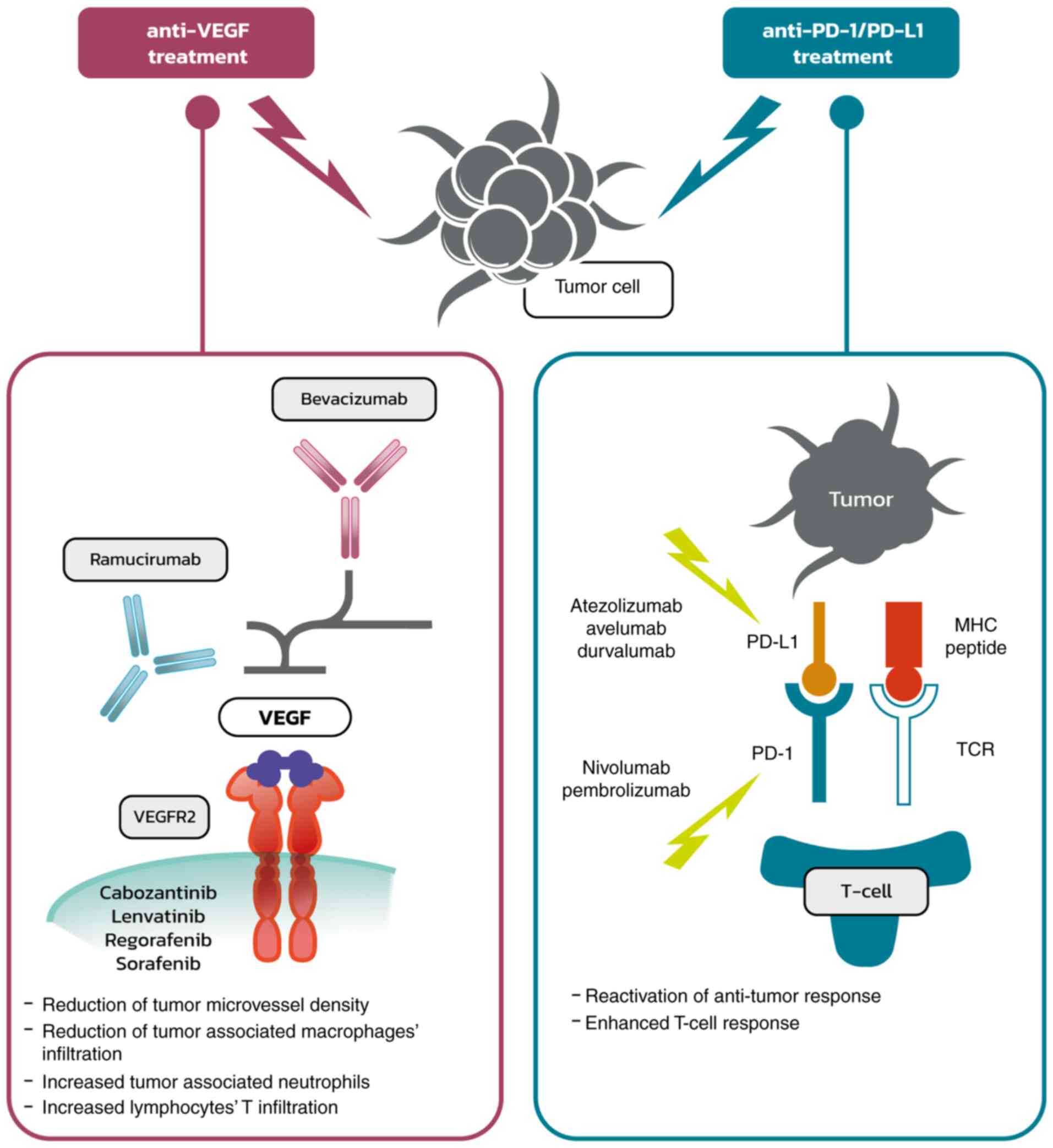
From a clinical point of view, the most important
inhibitors assessed were atezolizumab (anti-PD-L1) and bevacizumab
(anti-VEGF) in the ImBrave150 trial, which showed a significant
response to the combined treatment, and has since become the
recommended standard of care (66,67).
Bevacizumab was shown to reduce tumor microvessel density and
modulate the immune microenvironment through the reduction of
infiltration of tumor-associated macrophages and the increase in
tumor-associated neutrophils (68). VEGF-A produced in the tumor
microenvironment enhances the expression of PD-1 and other
inhibitory checkpoints involved in CD8+ T-cell
exhaustion, and this could be inhibited using anti-angiogenic
agents targeting VEGF-A and/or VEGFR (69). Thus, anti-VEGF therapy leads to the
reduction of immunosuppressive factors within the tumor and its
microenvironment and is associated with increased T-cell
infiltration, which together enhances the response to
immunotherapy. Atezolizumab is a monoclonal antibody that directly
binds to PD-L1 and provides a dual blockade of the PD-1 and B7.1
receptors, releasing PD-L1/PD-1 mediated inhibition of the immune
response, including the reactivation of the antitumor immune
response without inducing antibody-dependent cellular cytotoxicity.
The effect of anti-VEGF and anti-PD-1/PD-L1 treatment is
illustrated in Fig. 1.
Of note, combined treatment with bevacizumab and
atezolizumab was associated not only with improved survival [median
progression-free survival (PFS) was 6.8 months vs. 4.3 months in
the sorafenib group; hazard ratio (HR) 0.59; 95% confidence
interval (CI), 0.47-0.76; P<0.001], but also with the
maintenance of the quality of life (11.2 months vs. 3.6 months in
patients treated with sorafenib; HR 0.63; 95% CI, 0.46-0.85)
(70).
The Check-Mate 459 trial compared nivolumab
(anti-PD-1) with sorafenib as a first-line treatment for HCC.
Although the objective response rate was higher in the
investigational arm, the increase in OS was not significant
(71). Nivolumab was also
evaluated in combination with ipilimumab (anti-CTLA-4) in the phase
1/2 trial CheckMate 040, where manageable safety, promising
objective response rates, and durable responses were shown
(72).
Pembrolizumab is a humanized monoclonal antibody
that blocks the interaction of the PD-1 receptor with PD-L1 and
PD-L2, which results in the enhancement of the antitumor effect of
the immune system associated with T-cell responses (73). Based on the promising results of
the phase II trial Keynote 224 (74), pembrolizumab was evaluated as a
second-line treatment for HCC in the Keynote 240 trial. However,
the results did not show a notable clinical benefit (75).
Combined treatment with tremelimumab, an anti-CTLA4
antibody, and durvalumab showed promising results in patients with
advanced HCC in a phase I/II trial (76). It is also being investigated in the
phase III HIMALAYA trial (77).
Several other immunotherapeutic agents are under
evaluation in various combinations with tyrosine kinase inhibitors
or other immunotherapeutic drugs. Select phase III trials are
summarized in Table II (78–91).
The results of the already published trials suggest that there are
groups of patients that may benefit more from immunotherapy
compared with others. Currently, it seems to be crucial to identify
predictive factors for the response to targeted therapy. It is
suggested that the microenvironment may play an important role in
the response to the treatment.
| Table II.Selected phase III trials with
various immunotherapy approach for HCC. |
Table II.
Selected phase III trials with
various immunotherapy approach for HCC.
| Clinicaltrials.gov
number | Design | Status | (Refs.) |
|---|
| NCT02851784 | Combination therapy
of microwave ablation and expanding activated autologous
lymphocytes | Completed | (78) |
| NCT02562755 | Vaccinia
virus-based immunotherapy (Pexa-Vec) followed by sorafenib vs.
sorafenib | Completed | (79) |
| NCT05033522 | Living allogeneic
Th1-like cells with anti-CD3/CD28 microbeads attached derived from
precursors purified from healthy blood donors that are
differentiated and expanded ex-vivo vs. FOLFOX regimen | Not yet
recruiting | (80) |
| NCT02576509 | Nivolumab vs.
sorafenib as first-line treatment | Active, not
recruiting | (81) |
| NCT02678013 | RFA+highly-purified
CTL vs. RFA alone for recurrent HCC | Active, not
recruiting | (82) |
| NCT04167293 | Combination of
sintilimab and stereotactic body radiotherapy | Recruiting | (83) |
| NCT03949231 | Infusion of
PD-1/PDL-1 inhibitor via hepatic arterial vs. vein | Recruiting | (84) |
| NCT04229355 | DEB-TACE plus
lenvatinib or sorafenib or PD-1 inhibitor for unresectable HCC | Recruiting | (85) |
| NCT00699816 | Adjuvant adoptive
immune therapy using a CIK cell agent (Immuncell-LC) vs.
non-treatment group in HCC | Completed | (86) |
| NCT02709070 | Resection+highly
purified cytotoxic T lymphocytes vs. resection alone | Active | (87) |
| NCT04268888 | Nivolumab in
combination with TACE/TAE | Recruiting | (88) |
| NCT03867084 | Adjuvant
pembrolizumab vs. placebo in HCC with complete radiological
response after surgical resection or local ablation | Recruiting | (89) |
| NCT04682210 | Adjuvant sintilimab
plus bevacizumab in HCC after resection | Not yet
recruiting | (90) |
| NCT01749865 | Adjuvant
cytokine-induced killer cell treatment in HCC after resection | Completed | (91) |
A very interesting topic is the use of immunotherapy
in patients that qualify for liver transplants. There are limited
data regarding the use of immunotherapy for downstaging or bridging
therapy from clinical case reports (92,93).
The use of adoptive immunotherapy with liver allograft-derived NK
cells was evaluated in a study presented during the 2015 American
Transplant Congress, and it was suggested that this approach may
improve RFS (94). Immunotherapy
was also used for recurrent HCC treatment after liver
transplantation. Interestingly, a case report where ipilimumab was
used in a patient with recurrent HCC after liver transplantation
described a durable response and no rejection of the organ
(95). However, it should be noted
that immunotherapy may increase the risk of liver rejection and
therefore should be considered rather as a salvage therapy rather
than a first-line approach (96).
Clearly, there is a need for additional data.
Immune microenvironment factors associated
with the response to immunotherapy
The response to treatments depends on several
mechanisms and the specific characteristics of the tumor, the local
microenvironment, as well as the host itself. Firstly, since most
of the immunotherapeutics that showed clinical efficacy are
checkpoint inhibitors, it has been suggested that the expression of
PD-1 may be a reliable predictive factor. It has been shown that in
patients with head and neck cancers (97), melanoma (98), or lung cancer (99), increased PD-1 expression was
associated with better treatment outcomes.
Interestingly, in the Check-Mate 040 trial,
expression of PD-L1 in >1% of the tumor cells was detected in
20% of patients. However, the objective response between patients
with higher expression of PD-L1 in comparison to those with low
expression did not differ significantly: 26 vs. 19% (95% CI 13–26).
This suggests that other mechanisms may be involved in the response
to immunotherapy (66).
Potentially, this could be related to the expression of PD-1 and
PD-L1 on tumor-infiltrating lymphocytes.
Furthermore, in a small phase II trial where
patients with advanced HCC were treated with pembrolizumab after
sorafenib failure, the response was not correlated with either
PD-L1 tumor staining, prior sorafenib therapy or a history of
hepatitis. Correlative studies revealed high baseline plasma TGF-β
levels (≥200 pg/ml) were significantly correlated with poor
treatment outcomes after pembrolizumab. Tumor PD-L1 and plasma
PD-L1/PD-1 levels were associated with plasma IFN-γ or IL-10.
However, those results need caution due to the low number of
patients (n=28) (100).
Recently it was demonstrated that androgen receptors
may inhibit the expression of PD-L1 in HCC. It was found that the
androgen receptor is overexpressed in the nucleus of ~37% of HCC
tumors, which is significantly associated with an advanced disease
stage and poorer survival rates. It has also been suggested that
the overexpression of androgen receptors may be related to a worse
response to PD-L1 inhibitors (101).
Studies conducted in non-small cell lung cancer
highlighted the role of EGFR signaling in the regulation of the
host immunity and tumor microenvironment. Cell lines with mutant
EGFR exhibit increased expression of PD-L1 compared to wild-type
EGFR cells (102).
There are several questions regarding the potential
use of PD1/PD-L1 expression as a predictive factor. Firstly, the
expression of PD-L1 could be present on tumor cells or on immune
cells, which may play an essential role in the response to
immunotherapy (103). In patients
with HCC, a low baseline intratumoral
CD4+/CD8+ T-cell ratio was associated with a
better OS. Response to PD-1/PD-L1 therapy showed a trend of high
baseline frequency of intratumoral PD-1 CD8+ T cells.
However, LAG-3 and TIM-3 upregulation was also observed in
circulating T cells in patients who did not respond to PD-1/PD-L1
pathway blockade (103).
Furthermore, currently, there is no standard for
assessing the cut-off value for PD-L1 positivity and there are
various kits used, which makes the comparison between studies more
difficult. It was also shown that the expression of PD-L1 may
change during the disease (104,105). On the other hand, it has been
suggested that other factors associated with the tumor
microenvironment may be necessary for predicting the response to
immunotherapy. Recently, a classification of tumor
microenvironments based on TILs and PD-L1 expression was described.
Furthermore, it is suggested, that there is an immune class of HCC
tumors which may be further divided into two subtypes,
characterized by markers of an adaptive T-cell response or
exhausted immune response. The exhausted immune response subclass
expresses several genes regulated by TGF-β1 that mediate
immunosuppression. According to the authors, these findings
indicate that some HCCs may be susceptible to therapeutic agents
designed to block the regulatory pathways in T cells, such as
PD-L1, PD-1, or TGF-β1 inhibitors (106). In another study, a high number of
PD-1+ TILs was shown to be associated with prolonged OS
and DFS in patients with HCC who received surgery and adjuvant
cytokine-induced killer cells treatment (107).
Of note, it was suggested that the response to
immunotherapy may depend on the specific liver disease background,
such as a viral infection. However, a recently published
meta-analysis of 8 studies suggested that there was no significant
difference in objective response rate between virally infected HCC
and non-viral HCC patients [OR=1.03 (95% CI, 0.77-1.37;
I2=30.9%, pH=0.152)]. Similarly, there was no difference
between HBV-HCC and HCV-HCC patients in terms of objective response
rate [OR=0.74 (95% CI, 0.52-1.06; I2=7.4%, pH=0.374)].
The infiltration of immune cells in the tumor microenvironment did
not differ by etiology except for M0 macrophages, M2 macrophages,
regulatory T cells, naive B cells, follicular helper T cells,
activated dendritic cells, activated mast cells, and plasma cells.
Despite differences in infiltration observed in specific cell
types, the immune score and stromal score were generally comparable
among the different etiological groups (108).
Interestingly, it was suggested that immune
checkpoint inhibitors may be ineffective in non-alcoholic
steatohepatitis (NASH)-related HCC. This was observed in a
preclinical model as well as in a meta-analysis of three randomized
phase III clinical trials that tested inhibitors of PD-L1 or PD-1
in >1,600 patients with advanced HCC. According to the results,
immunotherapy did not improve survival in patients with non-viral
HCC. In two additional cohorts, patients with NASH-driven HCC who
received anti-PD-1 or anti-PD-L1 treatment showed reduced OS
compared with patients with other aetiologias (109).
Additional potential biomarkers and
predictive factors for the response to immunotherapy
Since radical treatment options are limited, and the
prognosis for patients with advanced HCC remains poor, there is a
need to identify reliable biomarkers of HCC to better tailor
patient therapy. Several potential biomarkers for the response to
immunotherapy have been investigated in HCC.
Several other mechanisms may be involved in the
response to immunotherapy. The gut-liver axis and the colon
microbiome are some of the suggested factors associated with the
response to immunotherapy. In a small study, where 8 patients with
progressive disease after sorafenib failure were treated with
nivolumab, fecal samples were collected and analyzed at baseline,
after 1 week, and every 3 weeks after that. Variations in the gut
bacteria were analyzed by metagenomic sequencing. It was observed
that fecal samples from patients responding to immunotherapy showed
higher taxa richness and increased gene counts than non-responders
(110). Another mechanism
potentially involved in the response to immunotherapy includes
exosomes due to their role in the communication between host and
tumor cells. Exosomes are involved in the transfer of proteins,
DNA, and RNA. Exosomes could serve as biomarkers for early-stage
HCC and as a possible target for therapy (111). There are several exosomal
biomarkers for the prediction of survival in HCC, i.e. proteins
involved in angiogenesis (S100A11, S100 calcium-binding protein
A11) and numerous microRNAs such as miR-29b-3p, miR-30d-5p which
are involved in cell migration, or miR-210 which is associated with
angiogenesis (112,113). Another example may be exosomal
circulating RNA (circPTGR1) which was suggested to promote HCC
metastasis. Finally, exosome-based strategies to deliver drugs into
tumors and the microenvironment showed promising results in
preclinical and clinical trials (114–116). The complexity of the interplay
between host and tumor requires further studies to identify
reliable predictive factors. Other factors include tumor mutational
burden (TMB), defined as the total number of mutations in the tumor
exome. However, it seems to be relatively rare in HCC; in a
recently published report median TMB was 4 mutations/Mb and only 6
tumors (0.8%) were classed as TMB-high. Out of 542 cases assessed
for microsatellite instability (MSI), one (0.2%) was MSI-high and
TMB-high. TMB may be associated with MSI or DNA mismatch repair
gene deficiency. In a recently published analysis, the most
commonly altered genes were TERT (44%), TP53 (35%), CTNNB1 (31%),
ARID1A (12%), and MYC (12%) (117).
Currently, there are a vast group of biomarkers
being investigated for HCC. They include post-translational
modifications such as phosphorylation, glycosylation,
ubiquitination, or acetylation. These changes are involved in
various physiological processes, but also in disease progression
(118). Next, generation
sequencing techniques (NGS) are proving to be very powerful and
valuable methods. Potentially, thanks to NGS profiling, patient
responses to treatments may be predictable. An analysis showed that
in patients with HCC, the WNT/β-catenin pathway (45%) and TP53
(33%) alterations were frequent and represented mutually exclusive
molecular subsets. In sorafenib-treated patients (n=81), oncogenic
PI3K-mTOR pathway alterations were associated with lower disease
control rates (DCR, 8.3 vs. 40.2%), shorter median PFS (1.9 vs. 5.3
months), and shorter median OS (10.4 vs. 17.9 months). Conversely,
patients treated with immune checkpoint inhibitors (n=31)
activating altered WNT/β-catenin signaling had lower DCR (0% vs.
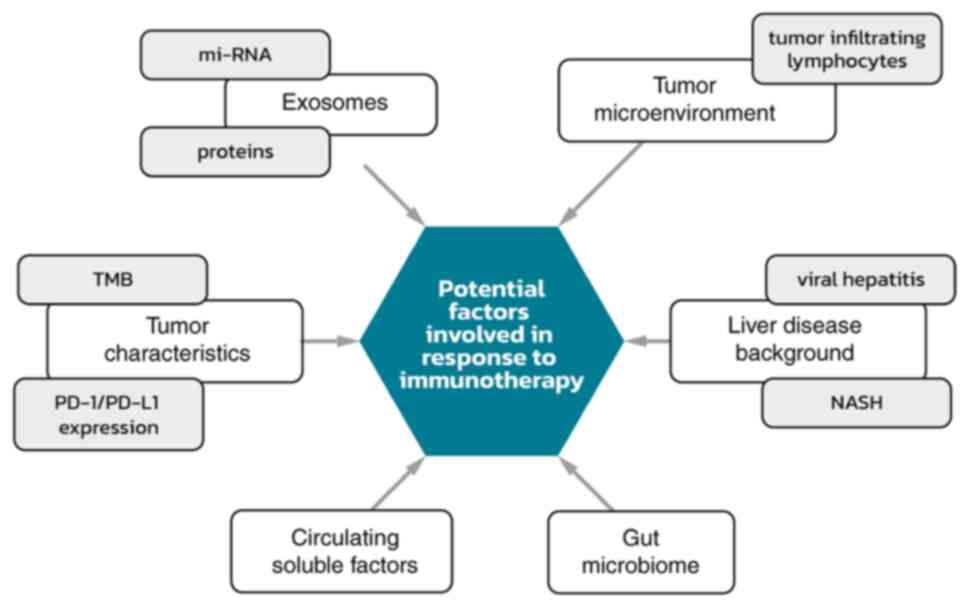
53%), shorter median PFS (2.0 vs. 7.4 months), and shorter median
OS (9.1 vs. 15.2 months) (119,120). Potential factors involved in
response to immunotherapy are summarized in Fig. 2.
Since histological specimens may not always be
available in HCC, factors that could be assessed from blood
examinations would be of value. A number of soluble factors such as
cytokines are of interest. In a phase II study, where several
circulating biomarkers were evaluated, low baseline levels of TGF-β
were significantly associated with improved OS and PFS after
treatment with pembrolizumab in advanced, unresectable HCC
(100,120). However, a detailed analysis is
beyond the scope of this review. A recently published analysis
showed that in patients with unresectable HCC, treated with
nivolumab or pembrolizumab, an early decrease in α-fetoprotein
levels was associated with an increased objective response and
increased survival. Moreover, albumin/bilirubin grade and
Child-Pugh classification determined survival based on
immunotherapy treatment (121).
Conclusions
This review briefly summarizes the current body of
knowledge regarding immune cells within the tumor microenvironment
in HCC. However, other factors may play important roles, such as
tumor mutational burden or microsatellite instability (122). The changing landscape of the
treatment possibilities in advanced HCC makes the role of
predictive factors rise. Thus, there is a need to identify reliable
factors that may help tailor treatments to the specific disease
characteristics presented.
Acknowledgements
The authors would like to thank Mr. Jakub Jaworski
for their assistance with the images used in this review.
Funding
Funding: No funding was received.
Availability of data and materials
Data sharing is not applicable to this article, as
no datasets were generated or analyzed during the current
study.
Authors' contributions
MG was responsible for conception and the design,
data analysis and interpretation of the data as well as draft
preparation of this review. KW conducted the draft preparation,
critical revisions and approved the final manuscript version to be
published; and agrees to be accountable for all aspects of the
work. LK was responsible for draft preparing, critical revisions;
approved of the final manuscript version to be published; and
agrees to be accountable for all aspects of the work. LR conducted
the draft preparation, critical revisions; approved of the final
manuscript version to be published; and agrees to be accountable
for all aspects of the work. RS conducted the draft preparing,
critical revisions; approved of the final manuscript version to be
published; and agrees to be accountable for all aspects of the
work. All authors have read and approved the final manuscript. Data
authentication is not applicable..
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Authors' information
MG (ORCID: 0000-0003-1344-5001) is a medical
oncologist, who graduated at the Medical University of Warsaw, and
has worked for several years at the Maria Curie-Sklodowska Cancer
Center-Institute in Warsaw. He is currently preparing a PhD
programme at the University Clinical Center, Warsaw. His focus is
on gastrointestinal cancers, particularly hepatobiliary cancer and
he is involved in several scientific projects, such as MentorEye
Project (development of Polish complementary system of molecular
surgical navigation for the purposes of cancer treatment); attendee
of several international trainings led by ESMO and ESDO; member of
the Polish Society of Clinical Oncology, ESMO (European Society for
Medical Oncology) and ESDO (European Society of Digestive
Oncology). KW is a medical oncologist and lecturer who graduated at
the Medical University of Warsaw, and is an assistant at the
Central Clinical Hospital, Oncology. His focus is on hepatobiliary
and pancreatic cancer. He was born in 1984 in Czestochowa, Poland.
He completed specialization in medical oncology in October 2016. In
clinical practice he takes care mostly of patients suffering from
gastrointestinal neoplasms. He is an author of more than 10
publications in medical journals and conferences reports. LK
(ORCID: 0000-0001-6509-5993) is a medical oncologist, researcher
and lecturer who graduated at the Medical University of Warsaw
(PhD) and is mainly focused on pancreatic and hepatobiliary
cancers. LK is the winner of several domestic grants and awards for
young researchers. LR is a medical oncology resident, involved in
several scientific projects, and an academic teacher at the Medical
University of Warsaw. Professor Rafal Stec (ORCID:
0000-0002-3291-6422) is a graduate of the Medical University of
Lublin and conducted post-graduate study ‘Innovation Management in
the Health Sector’ of the Academy of Leon Koźmiński in Warsaw. He
has been associated with oncology since 2000, initially at the
Maria Curie-Sklodowska Cancer Center-Institute in Warsaw, and then
at the Department of Oncology at the Military Medical Institute in
Warsaw. From September 2018, he was head of the Oncology Clinic of
the Medical University of Warsaw. He is also editor-in-chief of the
journal ‘Personalized Oncology’. He is co-author of over 100
publications in Polish and foreign journals as well as books and
textbooks, and is a member of the Polish Society of Clinical
Oncology and ESMO (European Society for Medical Oncology). He was a
winner of the awards of the Polish Society of Clinical Oncology and
is the Director of the Military Medical Institute in Warsaw. His
area of particular interest remains molecular and precise oncology
as well as personalized (individual) and interdisciplinary oncology
treatment. He is head of the Oncology Department at the Medical
University of Warsaw.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global Cancer Statistics 2020:
GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36
Cancers in 185 Countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Cheng AL, Kang YK, Chen Z, Tsao CJ, Qin S,
Kim JS, Luo R, Feng J, Ye S, Yang TS, et al: Efficacy and safety of
sorafenib in patients in the Asia-Pacific region with advanced
hepatocellular carcinoma: A phase III randomised, double-blind,
placebo-controlled trial. Lancet Oncol. 10:25–34. 2009. View Article : Google Scholar
|
|
3
|
Llovet JM, Ricci S, Mazzaferro V, Hilgard
P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A,
et al: Sorafenib in advanced hepatocellular carcinoma. N Engl J
Med. 359:378–390. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Cheng A, Qin S, Ikeda M, Galle PR, Ducreux
MP, Zhu AX, Kim T, Kudo M, Breder V, Merle P, et al: Imbrave150:
Efficacy and safety results from a ph III study evaluating
atezolizumab (atezo) + bevacizumab (bev) vs sorafenib (Sor) as
first treatment (tx) for patients (pts) with unresectable
hepatocellular carcinoma (HCC)'. Ann Oncol. 30 (Suppl
9):ix183–ix202. 2019. View Article : Google Scholar
|
|
5
|
Ghouri YA, Mian I and Rowe JH: Review of
hepatocellular carcinoma: Epidemiology, etiology, and
carcinogenesis. J Carcinog. 16:12017. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Novikova MV, Khromova NV and Kopnin PB:
Components of the hepatocellular carcinoma microenvironment and
their role in tumor progression. Biochemistry (Mosc). 82:861–873.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jia W, Rajani C, Xu H and Zheng X: Gut
microbiota alterations are distinct for primary colorectal cancer
and hepatocellular carcinoma. Protein Cell. 12:374–393. 2021.
View Article : Google Scholar
|
|
8
|
Kumar V, Patel S, Tcyganov E and
Gabrilovich DI: The nature of myeloid-derived suppressor cells in
the tumor microenvironment. Trends Immunol. 37:208–220. 2016.
View Article : Google Scholar
|
|
9
|
Chiu DK, Tse AP, Xu IM, Di Cui J, Lai RK,
Li LL, Koh HY, Tsang FH, Wei LL, Wong CM, et al: Hypoxia inducible
factor HIF-1 promotes myeloid-derived suppressor cells accumulation
through ENTPD2/CD39L1 in hepatocellular carcinoma. Nat Commun.
8:5172017. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hoechst B, Ormandy LA, Ballmaier M, Lehner
F, Krüger C, Manns MP, Greten TF and Korangy F: A new population of
myeloid-derived suppressor cells in hepatocellular carcinoma
patients induces CD4(+)CD25(+)Foxp3(+) T cells. Gastroenterology.
135:234–243. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yang L, DeBusk LM, Fukuda K, Fingleton B,
Green-Jarvis B, Shyr Y, Matrisian LM, Carbone DP and Lin PC:
Expansion of myeloid immune suppressor Gr+CD11b+ cells in
tumor-bearing host directly promotes tumor angiogenesis. Cancer
Cell. 6:409–421. 2004. View Article : Google Scholar
|
|
12
|
Li H, Han Y, Guo Q, Zhang M and Cao X:
Cancer-expanded myeloid-derived suppressor cells induce anergy of
NK cells through membrane-bound TGF-beta 1. J Immunol. 182:240–249.
2009. View Article : Google Scholar
|
|
13
|
Yan W, Liu X, Ma H, Zhang H, Song X, Gao
L, Liang X and Ma C: Tim-3 fosters HCC development by enhancing
TGF-β-mediated alternative activation of macrophages. Gut.
64:1593–1604. 2015. View Article : Google Scholar
|
|
14
|
Chang CJ, Yang YH, Chiu CJ, Lu LC, Liao
CC, Liang CW, Hsu CH and Cheng AL: Targeting tumor-infiltrating
Ly6G+ myeloid cells improves sorafenib efficacy in mouse
orthotopic hepatocellular carcinoma. Int J Cancer. 142:1878–1889.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Mantovani A, Bottazzi B, Colotta F,
Sozzani S and Ruco L: The origin and function of tumor-associated
macrophages. Immunol Today. 13:265–270. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Gordon S and Taylor PR: Monocyte and
macrophage heterogeneity. Nat Rev Immunol. 5:953–964. 2005.
View Article : Google Scholar
|
|
17
|
Martinez FO and Gordon S: The M1 and M2
paradigm of macrophage activation: Time for reassessment.
F1000Prime Rep. 6:132014. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zhou D, Huang C, Lin Z, Zhan S, Kong L,
Fang C and Li J: Macrophage polarization and function with emphasis
on the evolving roles of coordinated regulation of cellular
signaling pathways. Cell Signal. 26:192–197. 2014. View Article : Google Scholar
|
|
19
|
Solinas G, Germano G, Mantovani A and
Allavena P: Tumor-associated macrophages (TAM) as major players of
the cancer-related inflammation. J Leukoc Biol. 86:1065–1073. 2009.
View Article : Google Scholar
|
|
20
|
Yao Y, Xu XH and Jin L: Macrophage
polarization in physiological and pathological pregnancy. Front
Immunol. 10:7922019. View Article : Google Scholar
|
|
21
|
Wan S, Kuo N, Kryczek I, Zou W and Welling
TH: Myeloid cells in hepatocellular carcinoma. Hepatology.
62:1304–1312. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wang J, Li D, Cang H and Guo B: Crosstalk
between cancer and immune cells: Role of tumor-associated
macrophages in the tumor microenvironment. Cancer Med. 8:4709–4721.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Guo B, Li L, Guo J, Liu A, Wu J, Wang H,
Shi J, Pang D and Cao Q: M2 tumor-associated macrophages produce
interleukin-17 to suppress oxaliplatin-induced apoptosis in
hepatocellular carcinoma. Oncotarget. 8:44465–44476. 2017.
View Article : Google Scholar
|
|
24
|
Fu XT, Song K, Zhou J, Shi YH, Liu WR, Shi
GM, Gao Q, Wang XY, Ding ZB and Fan J: Tumor-associated macrophages
modulate resistance to oxaliplatin via inducing autophagy in
hepatocellular carcinoma. Cancer Cell Int. 19:712019. View Article : Google Scholar
|
|
25
|
Zhang J, Chang L, Zhang X, Zhou Z and Gao
Y: Meta-analysis of the prognostic and clinical value of
tumor-associated macrophages in hepatocellular carcinoma. J Invest
Surg. 34:297–306. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zong Z, Zou J, Mao R, Ma C, Li N, Wang J,
Wang X, Zhou H, Zhang L and Shi Y: M1 macrophages induce PD-L1
expression in hepatocellular carcinoma cells through IL-1β
signaling. Front Immunol. 10:16432019. View Article : Google Scholar
|
|
27
|
Ding W, Tan Y, Qian Y, Xue W, Wang Y,
Jiang P and Xu X: Clinicopathologic and prognostic significance of
tumor-associated macrophages in patients with hepatocellular
carcinoma: A meta-analysis. PLoS One. 14:e02239712019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Lau J, Cheung J, Navarro A, Lianoglou S,
Haley B, Totpal K, Sanders L, Koeppen H, Caplazi P, McBride J, et
al: Tumour and host cell PD-L1 is required to mediate suppression
of anti-tumour immunity in mice. Nat Commun. 8:145722017.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Umezu D, Okada N, Sakoda Y, Adachi K,
Ojima T, Yamaue H, Eto M and Tamada K: Inhibitory functions of
PD-L1 and PD-L2 in the regulation of anti-tumor immunity in murine
tumor microenvironment. Cancer Immunol Immunother. 68:201–211.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dong N, Shi X, Wang S, Gao Y, Kuang Z, Xie
Q, Li Y, Deng H, Wu Y, Li M and Li JL: M2 macrophages mediate
sorafenib resistance by secreting HGF in a feed-forward manner in
hepatocellular carcinoma. Br J Cancer. 121:22–33. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhou DY, Qin J, Huang J, Wang F, Xu GP, Lv
YT, Zhang JB and Shen LM: Zoledronic acid inhibits infiltration of
tumor-associated macrophages and angiogenesis following
transcatheter arterial chemoembolization in rat hepatocellular
carcinoma models. Oncol Lett. 14:4078–4084. 2017. View Article : Google Scholar
|
|
32
|
Ao JY, Zhu XD, Chai ZT, Cai H, Zhang YY,
Zhang KZ, Kong LQ, Zhang N, Ye BG, Ma DN and Sun HC:
Colony-stimulating factor 1 receptor blockade inhibits tumour
growth by altering the polarization of tumour-associated
macrophages in hepatocellular carcinoma. Mol Cancer Ther.
16:1544–1554. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sun S, Cui Y, Ren K, Quan M, Song Z, Zou
H, Li D, Zheng Y and Cao J: 8-bromo-7-methoxychrysin reversed M2
polarization of tumour-associated macrophages induced by liver
cancer stem-like cells. Anticancer Agents Med Chem. 17:286–293.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Wan S, Zhao E, Kryczek I, Vatan L,
Sadovskaya A, Ludema G, Simeone DM, Zou W and Welling TH:
Tumor-associated macrophages produce interleukin 6 and signal via
STAT3 to promote expansion of human hepatocellular carcinoma stem
cells. Gastroenterology. 147:1393–1404. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li X, Yao W, Yuan Y, Chen P, Li B, Li J,
Chu R, Song H, Xie D, Jiang X and Wang H: Targeting of
tumour-infiltrating macrophages via CCL2/CCR2 signalling as a
therapeutic strategy against hepatocellular carcinoma. Gut.
66:157–167. 2017. View Article : Google Scholar
|
|
36
|
Yao W, Ba Q, Li X, Li H, Zhang S, Yuan Y,
Wang F, Duan X, Li J, Zhang W and Wang H: A natural CCR93
antagonist relieves tumour-associated macrophage-mediated
immunosuppression to produce a therapeutic effect for liver cancer.
EBioMedicine. 22:58–67. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zhang JP, Yan J, Xu J, Pang XH, Chen MS,
Li L, Wu C, Li SP and Zheng L: Increased intratumoral
IL-17-producing cells correlate with poor survival in
hepatocellular carcinoma patients. J Hepatol. 50:980–989. 2009.
View Article : Google Scholar
|
|
38
|
Flecken T, Schmidt N, Hild S, Gostick E,
Drognitz O, Zeiser R, Schemmer P, Bruns H, Eiermann T, Price DA, et
al: Immunodominance and functional alterations of tumor-associated
antigen-specific CD8+ T-cell responses in hepatocellular carcinoma.
Hepatology. 59:1415–1426. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ringelhan M, Pfister D, O'Connor T,
Pikarsky E and Heikenwalder M: The immunology of hepatocellular
carcinoma. Nat Immunol. 19:222–232. 2018. View Article : Google Scholar
|
|
40
|
Khan O, Giles JR, McDonald S, Manne S,
Ngiow SF, Patel KP, Werner MT, Huang AC, Alexander KA, Wu JE, et
al: TOX transcriptionally and epigenetically programs
CD8+ T cell exhaustion. Nature. 571:211–218. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Blackburn SD, Shin H, Haining WN, Zou T,
Workman CJ, Polley A, Betts MR, Freeman GJ, Vignali DA and Wherry
EJ: Coregulation of CD8+ T cell exhaustion by multiple inhibitory
receptors during chronic viral infection. Nat Immunol. 10:29–37.
2009. View Article : Google Scholar
|
|
42
|
Wherry EJ and Kurachi M: Molecular and
cellular insights into T cell exhaustion. Nat Rev Immunol.
15:486–499. 2015. View Article : Google Scholar
|
|
43
|
Kim HD, Song GW, Park S, Jung MK, Kim MH,
Kang HJ, Yoo C, Yi K, Kim KH, Eo S, et al: Association between
expression level of PD1 by tumor-infiltrating CD8(+) T cells and
features of hepatocellular carcinoma. Gastroenterology.
155:1936–1950.e17. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Gao Q, Qiu SJ, Fan J, Zhou J, Wang XY,
Xiao YS, Xu Y, Li YW and Tang ZY: Intratumoral balance of
regulatory and cytotoxic T cells is associated with prognosis of
hepatocellular carcinoma after resection. J Clin Oncol.
25:2586–2593. 2007. View Article : Google Scholar
|
|
45
|
Fu J, Xu D, Liu Z, Shi M, Zhao P, Fu B,
Zhang Z, Yang H, Zhang H, Zhou C, et al: Increased regulatory T
cells correlate with CD8 T-cell impairment and poor survival in
hepatocellular carcinoma patients. Gastroenterology. 132:2328–2339.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Sideras K, Biermann K, Verheij J,
Takkenberg BR, Mancham S, Hansen BE, Schutz HM, de Man RA,
Sprengers D, Buschow SI, et al: PD-L1, Galectin-9 and
CD8+ tumor-infiltrating lymphocytes are associated with
survival in hepatocellular carcinoma. OncoImmunology.
6:e12733092017. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Kang HJ, Oh JH, Chun SM, Kim D, Ryu YM,
Hwang HS, Kim SY, An J, Cho EJ, Lee H, et al: Immunogenomic
landscape of hepatocellular carcinoma with immune cell stroma and
EBV-positive tumor-infiltrating lymphocytes. J Hepatol. 71:91–103.
2019. View Article : Google Scholar
|
|
48
|
Cariani E and Missale G: Immune landscape
of hepatocellular carcinoma microenvironment: Implications for
prognosis and therapeutic applications. Liver Int. 39:1608–1621.
2019. View Article : Google Scholar
|
|
49
|
Zhou SL, Zhou ZJ, Hu ZQ, Huang XW, Wang Z,
Chen EB, Fan J, Cao Y, Dai Z and Zhou J: Tumor-Associated
Neutrophils Recruit Macrophages and T-Regulatory Cells to Promote
Progression of Hepatocellular Carcinoma and Resistance to
Sorafenib. Gastroenterology. 150:1646–1658.e17. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Zhou SL, Yin D, Hu ZQ, Luo CB, Zhou ZJ,
Xin HY, Yang XR, Shi YH, Wang Z, Huang XW, et al: A positive
feedback loop between cancer stem-like cells and tumor-associated
neutrophils controls hepatocellular carcinoma progression.
Hepatology. 70:1214–1230. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Zhang W, Zhu XD, Sun HC, Xiong YQ, Zhuang
PY, Xu HX, Kong LQ, Wang L, Wu WZ and Tang ZY: Depletion of
tumor-associated macrophages enhances the effect of sorafenib in
metastatic liver cancer models by antimetastatic and antiangiogenic
effects. Clin Cancer Res. 16:3420–3430. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Tian XP, Wang CY, Jin XH, Li M, Wang FW,
Huang WJ, Yun JP, Xu RH, Cai QQ and Xie D: Acidic microenvironment
up-regulates exosomal miR-21 and miR-10b in early-stage
hepatocellular carcinoma to promote cancer cell proliferation and
metastasis. Theranostics. 9:1965–1979. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Gao X, Huang H, Wang Y, Pan C, Yin S, Zhou
L and Zheng S: Tumor immune microenvironment characterization in
hepatocellular carcinoma identifies four prognostic and
immunotherapeutically relevant subclasses. Front Oncol.
10:6105132021. View Article : Google Scholar
|
|
54
|
Budimir N, Thomas GD, Dolina JS and
Salek-Ardakani S: Reversing T-cell exhaustion in cancer: Lessons
learned from PD-1/PD-L1 immune checkpoint blockade. Cancer Immunol
Res. 10:146–153. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Kato Y, Tabata K, Kimura T,
Yachie-Kinoshita A, Ozawa Y, Yamada K, Ito J, Tachino S, Hori Y,
Matsuki M, et al: Lenvatinib plus anti-PD-1 antibody combination
treatment activates CD8+ T cells through reduction of
tumor-associated macrophage and activation of the interferon
pathway. PLoS One. 14:e02125132019. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Lu M, Zhang X, Gao X, Sun S, Wei X, Hu X,
Huang C, Xu H, Wang B, Zhang W, et al: Lenvatinib enhances T cell
immunity and the efficacy of adoptive chimeric antigen
receptor-modified T cells by decreasing myeloid-derived suppressor
cells in cancer. Pharmacol Res. 174:1058292021. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Huang X, Xu L, Ma T, Yin X, Huang Z, Ran
Y, Ni Y, Bi X and Che X: Lenvatinib plus immune checkpoint
inhibitors improve survival in advanced hepatocellular carcinoma: A
Retrospective Study. Front Oncol. 11:7511592021. View Article : Google Scholar
|
|
58
|
Wang BJ, Bao JJ, Wang JZ, Wang Y, Jiang M,
Xing MY, Zhang WG, Qi JY, Roggendorf M, Lu MJ and Yang DL:
Immunostaining of PD-1/PD-Ls in liver tissues of patients with
hepatitis and hepatocellular carcinoma. World J Gastroenterol.
17:3322–3329. 2011. View Article : Google Scholar
|
|
59
|
Garon EB, Rizvi NA, Hui R, Leighl N,
Balmanoukian AS, Eder JP, Patnaik A, Aggarwal C, Gubens M, Horn L,
et al: Pembrolizumab for the treatment of non-small-cell lung
cancer. N Engl J Med. 372:2018–2028. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Lin H, Wei S, Hurt EM, Green MD, Zhao L,
Vatan L, Szeliga W, Herbst R, Harms PW, Fecher LA, et al: Host
expression of PD-L1 determines efficacy of PD-L1 pathway
blockade-mediated tumor regression. J Clin Invest. 128:805–815.
2018. View Article : Google Scholar
|
|
61
|
Calderaro J, Rousseau B, Amaddeo G, Mercey
M, Charpy C, Costentin C, Luciani A, Zafrani ES, Laurent A, Azoulay
D, et al: Programmed death ligand 1 expression in hepatocellular
carcinoma: Relationship With clinical and pathological features.
Hepatology. 64:2038–2046. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Teng MW, Ngiow SF, Ribas A and Smyth MJ:
Classifying cancers based on T-cell infiltration and PD-L1. Cancer
Res. 75:2139–2145. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Woo SR, Turnis ME, Goldberg MV, Bankoti J,
Selby M, Nirschl CJ, Bettini ML, Gravano DM, Vogel P, Liu CL, et
al: Immune inhibitory molecules LAG-3 and PD-1 synergistically
regulate T-cell function to promote tumoral immune escape. Cancer
Res. 72:917–927. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Kurebayashi Y, Ojima H, Tsujikawa H,
Kubota N, Maehara J, Abe Y, Kitago M, Shinoda M, Kitagawa Y and
Sakamoto M: Landscape of immune microenvironment in hepatocellular
carcinoma and its additional impact on histological and molecular
classification. Hepatology. 68:1025–1041. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Abdou Y, Pandey M, Sarma M, Shah S, Baron
J and Ernstoff MS: Mechanism-based treatment of cancer with immune
checkpoint inhibitor therapies. Br J Clin Pharmacol. 86:1690–1702.
2020. View Article : Google Scholar
|
|
66
|
European Medicine Agency, . Bevacizumab,
Avastin Summary of Product Characteristics. https://www.ema.europa.eu/en/documents/product-information/avastin-epar-product-information_en.pdfJune
12–2022
|
|
67
|
European Medicine Agency, . Atezolizumab
Summary of Product Characteristics. June 12–2022
|
|
68
|
Roland CL, Dineen SP, Lynn KD, Sullivan
LA, Dellinger MT, Sadegh L, Sullivan JP, Shames DS and Brekken RA:
Inhibition of vascular endothelial growth factor reduces
angiogenesis and modulates immune cell infiltration of orthotopic
breast cancer xenografts. Mol Cancer Ther. 8:1761–1771. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Voron T, Colussi O, Marcheteau E, Pernot
S, Nizard M, Pointet AL, Latreche S, Bergaya S, Benhamouda N,
Tanchot C, et al: VEGF-A modulates expression of inhibitory
checkpoints on CD8+ T cells in tumors. J Exp Med. 212:139–148.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux
M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, et al: Atezolizumab
plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J
Med. 382:1894–1905. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Yau T, Park JW, Finn RS, Cheng AL,
Mathurin P, Edeline J, Kudo M, Harding JJ, Merle P, Rosmorduc O, et
al: Nivolumab versus sorafenib in advanced hepatocellular carcinoma
(CheckMate 459): a randomised, multicentre, open-label, phase 3
trial. Lancet Oncol. 23:77–90. 2022. View Article : Google Scholar
|
|
72
|
Yau T, Kang YK, Kim TY, El-Khoueiry AB,
Santoro A, Sangro B, Melero I, Kudo M, Hou MM, Matilla A, et al:
Efficacy and safety of nivolumab plus ipilimumab in patients with
advanced hepatocellular carcinoma previously treated with
sorafenib: The checkmate 040 randomized clinical trial. JAMA Oncol.
6:e2045642020. View Article : Google Scholar
|
|
73
|
European Medicine Agency, . Pembrolizumab
Summary of Product Characteristics. https://www.ema.europa.eu/en/documents/product-information/keytruda-epar-product-information_en.pdfJune
12–2022
|
|
74
|
Zhu AX, Finn RS, Edeline J, Cattan S,
Ogasawara S, Palmer D, Verslype C, Zagonel V, Fartoux L, Vogel A,
et al: Pembrolizumab in patients with advanced hepatocellular
carcinoma previously treated with sorafenib (KEYNOTE-224): A
non-randomised, open-label phase 2 trial. Lancet Oncol. 19:940–952.
2018. View Article : Google Scholar
|
|
75
|
Finn RS, Ryoo BY, Merle P, Kudo M,
Bouattour M, Lim HY, Breder V, Edeline J, Chao Y, Ogasawara S, et
al: Pembrolizumab as second-line therapy in patients with advanced
hepatocellular carcinoma in KEYNOTE-240: A randomized,
double-blind, phase III trial. J Clin Oncol. 38:193–202. 2020.
View Article : Google Scholar
|
|
76
|
Kelley RK, Sangro B, Harris W, Ikeda M,
Okusaka T, Kang YK, Qin S, Tai DW, Lim HY, Yau T, et al: Safety,
efficacy, and pharmacodynamics of tremelimumab plus durvalumab for
patients with unresectable hepatocellular carcinoma: Randomized
expansion of a phase I/II study. J Clin Oncol. 39:2991–3001. 2021.
View Article : Google Scholar
|
|
77
|
U.S. National Library of Medicine (NIH), .
Study of Durvalumab and Tremelimumab as First-line Treatment in
Patients With Advanced Hepatocellular Carcinoma (HIMALAYA).
ClinicalTrials.gov Identifier: NCT03298451. NIH; Bethesda, MD:
2017, https://clinicaltrials.gov/ct2/show/NCT03298451April
19–2021
|
|
78
|
U.S. National Library of Medicine (NIH), .
Combination Therapy of Microwave Ablation and Cellular
Immunotherapy for Hepatocellular Carcinoma. ClinicalTrials.gov
Identifier: NCT02851784. NIH; Bethesda, MD: 2016, https://clinicaltrials.gov/ct2/show/NCT02851784November
20–2021
|
|
79
|
U.S. National Library of Medicine (NIH), .
Hepatocellular Carcinoma Study Comparing Vaccinia Virus Based
Immunotherapy Plus Sorafenib vs Sorafenib Alone (PHOCUS).
ClinicalTrials.gov Identifier: NCT02562755. NIH; Bethesda, MD:
2015, https://clinicaltrials.gov/ct2/show/NCT02562755November
20–2021
|
|
80
|
U.S. National Library of Medicine (NIH), .
FImmunotherapy for Advanced Liver Cancer (ALIVE).
ClinicalTrials.gov Identifier: NCT05033522. NIH; Bethesda, MD:
2021, https://clinicaltrials.gov/ct2/show/NCT05033522November
20–2021
|
|
81
|
U.S. National Library of Medicine (NIH), .
An Investigational Immuno-therapy Study of Nivolumab Compared to
Sorafenib as a First Treatment in Patients With Advanced
Hepatocellular Carcinoma. ClinicalTrials.gov Identifier:
NCT02576509. NIH; Bethesda, MD: 2015, https://clinicaltrials.gov/ct2/show/NCT02576509November
20–2021
|
|
82
|
U.S. National Library of Medicine (NIH), .
RRFA+Highly-purified CTL vs. RFA Alone for Recurrent HCC.
ClinicalTrials.gov Identifier: NCT02678013. NIH; Bethesda, MD:
2016, https://clinicaltrials.gov/ct2/show/NCT02678013November
20–2021
|
|
83
|
U.S. National Library of Medicine (NIH), .
Combination of Sintilimab and Stereotactic Body Radiotherapy in
Hepatocellular Carcinoma (ISBRT01) (ISBRT01). ClinicalTrials.gov
Identifier: NCT04167293. NIH; Bethesda, MD: 2019, https://clinicaltrials.gov/ct2/show/NCT04167293November
20–2021
|
|
84
|
U.S. National Library of Medicine (NIH), .
Infusion of PD1/PDL1 Inhibitor Via Hepatic Arterial Versus Vein for
Immunotherapy of Advanced Hepatocellular Carcinoma.
ClinicalTrials.gov Identifier: NCT03949231. NIH; Bethesda, MD:
2019, https://clinicaltrials.gov/ct2/show/NCT03949231November
20–2021
|
|
85
|
U.S. National Library of Medicine (NIH), .
DEB-TACE Plus Lenvatinib or Sorafenib or PD-1 Inhibitor for
Unresectable Hepatocellular Carcinoma. ClinicalTrials.gov
Identifier: NCT04229355. NIH; Bethesda, MD: 2020, https://clinicaltrials.gov/ct2/show/NCT04229355November
20–2021
|
|
86
|
U.S. National Library of Medicine (NIH), .
Efficacy and Safety of Immuncell-LC Group and Non-treatment Group
in Hepatocelluar Carcinoma Patients. ClinicalTrials.gov Identifier:
NCT00699816. NIH; Bethesda, MD: 2008, https://clinicaltrials.gov/ct2/show/NCT00699816November
20–2021
|
|
87
|
U.S. National Library of Medicine (NIH), .
Resection+Highly Purified CTL Versus Resection Alone for HCC.
ClinicalTrials.gov Identifier: NCT02709070. NIH; Bethesda, MD:
2016, https://clinicaltrials.gov/ct2/show/NCT02709070November
20–2021
|
|
88
|
U.S. National Library of Medicine (NIH), .
Nivolumab in Combination With TACE/TAE for Patients With
Intermediate Stage HCC (TACE-3). ClinicalTrials.gov Identifier:
NCT04268888. NIH; Bethesda, MD: 2020, https://clinicaltrials.gov/ct2/show/NCT04268888November
20–2021
|
|
89
|
U.S. National Library of Medicine (NIH), .
Safety and Efficacy of Pembrolizumab (MK-3475) Versus Placebo as
Adjuvant Therapy in Participants With Hepatocellular Carcinoma
(HCC) and Complete Radiological Response After Surgical Resection
or Local Ablation (MK-3475-937 / KEYNOTE-937). ClinicalTrials.gov
Identifier: NCT03867084. NIH; Bethesda, MD: 2019, https://clinicaltrials.gov/ct2/show/NCT03867084November
20–2021
|
|
90
|
U.S. National Library of Medicine (NIH), .
Sintilimab Plus Bevacizumab as Adjuvant Therapy in HCC Patients at
High Risk of Recurrence After Curative Resection (DaDaLi).
ClinicalTrials.gov Identifier: NCT04682210. NIH; Bethesda, MD:
2020, https://www.clinicaltrials.gov/ct2/show/NCT04682210November
20–2021
|
|
91
|
U.S. National Library of Medicine
(NIH):CIK Treatment for HCC Patient Underwent Radical Resection, .
ClinicalTrials.gov Identifier NCT01749865. NIH; Bethesda, MD: 2012,
https://clinicaltrials.gov/ct2/show/NCT01749865November
20–2021
|
|
92
|
Schwacha-Eipper B, Minciuna I, Banz V and
Dufour JF: Immunotherapy as a downstaging therapy for liver
transplantation. Hepatology. 72:1488–1490. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Tabrizian P, Florman SS and Schwartz ME:
PD-1 inhibitor as bridge therapy to liver transplantation? Am J
Transplant. 21:1979–1980. 2021. View Article : Google Scholar
|
|
94
|
Tanimine N, Tanaka Y, Ishiyama K, Ohira M,
Shimizu S, Yano T and Ohdan H: Adoptive Immunotherapy with Liver
allograft-derived NK Cells Improves Recurrence-free Survival after
Living-donor Liver Transplantation in Patients with Hepatocellular
Carcinoma. Am J Transplant. 15 (Suppl 3):3172015.
|
|
95
|
Pandey A and Cohen DJ: Ipilumumab for
hepatocellular cancer in a liver transplant recipient, with durable
response, tolerance and without allograft rejection. Immunotherapy.
12:287–292. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Luo Y, Teng F, Fu H and Ding GS:
Immunotherapy in liver transplantation for hepatocellular
carcinoma: Pros and cons. World J Gastrointest Oncol. 14:163–180.
2022. View Article : Google Scholar
|
|
97
|
Burtness B, Harrington KJ, Greil R,
Soulières D, Tahara M, de Castro G Jr, Psyrri A, Basté N, Neupane
P, Bratland Å, et al: Pembrolizumab alone or with chemotherapy
versus cetuximab with chemotherapy for recurrent or metastatic
squamous cell carcinoma of the head and neck (KEYNOTE-048): A
randomised, open-label, phase 3 study. Lancet. 394:1915–1928. 2019.
View Article : Google Scholar
|
|
98
|
Daud AI, Wolchok JD, Robert C, Hwu WJ,
Weber JS, Ribas A, Hodi FS, Joshua AM, Kefford R, Hersey P, et al:
Programmed Death-Ligand 1 expression and response to the
anti-programmed death 1 antibody pembrolizumab in melanoma. J Clin
Oncol. 34:4102–4109. 2016. View Article : Google Scholar
|
|
99
|
Tian P, He B, Mu W, Liu K, Liu L, Zeng H,
Liu Y, Jiang L, Zhou P, Huang Z, et al: Assessing PD-L1 expression
in non-small cell lung cancer and predicting responses to immune
checkpoint inhibitors using deep learning on computed tomography
images. Theranostics. 11:2098–2107. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Feun LG, Li YY, Wu C, Wangpaichitr M,
Jones PD, Richman SP, Madrazo B, Kwon D, Garcia-Buitrago M, Martin
P, et al: Phase 2 study of pembrolizumab and circulating biomarkers
to predict anticancer response in advanced, unresectable
hepatocellular carcinoma. Cancer. 125:3603–3614. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Zhang H, Li XX, Yang Y, Zhang Y, Wang HY
and Zheng XFS: Significance and mechanism of androgen receptor
overexpression and androgen receptor/mechanistic target of
rapamycin cross-talk in hepatocellular carcinoma. Hepatology.
67:2271–2286. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Azuma K, Ota K, Kawahara A, Hattori S,
Iwama E, Harada T, Matsumoto K, Takayama K, Takamori S, Kage M, et
al: Association of PD-L1 overexpression with activating EGFR
mutations in surgically resected nonsmall-cell lung cancer. Ann
Oncol. 25:1935–1940. 2014. View Article : Google Scholar
|
|
103
|
Taube JM, Klein A, Brahmer JR, Xu H, Pan
X, Kim JH, Chen L, Pardoll DM, Topalian SL and Anders RA:
Association of PD-1, PD-1 ligands, and other features of the tumour
immune microenvironment with response to anti-PD-1 therapy. Clin
Cancer Res. 20:5064–5074. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Macek Jilkova Z, Aspord C, Kurma K, Granon
A, Sengel C, Sturm N, Marche PN and Decaens T: Immunologic features
of patients with advanced hepatocellular carcinoma before and
during sorafenib or anti-programmed death-1/programmed death-L1
treatment. Clin Transl Gastroenterol. 10:e000582019. View Article : Google Scholar
|
|
105
|
Kleinovink JW, van Hall T, Ossendorp F and
Fransen MF: PD-L1 immune suppression in cancer: Tumor cells or host
cells? OncoImmunology. 6:e13259822017. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Vilain RE, Menzies AM, Wilmott JS,
Kakavand H, Madore J, Guminski A, Liniker E, Kong BY, Cooper AJ,
Howle JR, et al: Dynamic changes in PD-L1 expression and immune
infiltrates early during treatment predict response to PD-1
blockade in melanoma. Clin Cancer Res. 23:5024–5033. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Sia D, Jiao Y, Martinez-Quetglas I, Kuchuk
O, Villacorta-Martin C, Castro de Moura M, Putra J, Camprecios G,
Bassaganyas L, Akers N, et al: Identification of an immune-specific
class of hepatocellular carcinoma, based on molecular features.
Gastroenterology. 153:812–826. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Chang B, Shen L, Wang K, Jin J, Huang T,
Chen Q, Li W and Wu P: High number of PD-1 positive intratumoural
lymphocytes predicts survival benefit of cytokine-induced killer
cells for hepatocellular carcinoma patients. Liver Int.
38:1449–1458. 2018. View Article : Google Scholar
|
|
109
|
Ding Z, Dong Z, Chen Z, Hong J, Yan L, Li
H, Yao S, Yan Y, Yang Y, Yang C and Li T: Viral status and efficacy
of immunotherapy in hepatocellular carcinoma: A systematic review
with meta-analysis. Front Immunol. 12:7335302021. View Article : Google Scholar
|
|
110
|
Pfister D, Núñez NG, Pinyol R, Govaere O,
Pinter M, Szydlowska M, Gupta R, Qiu M, Deczkowska A, Weiner A, et
al: NASH limits anti-tumour surveillance in immunotherapy-treated
HCC. Nature. 592:450–456. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
111
|
Zheng Y, Wang T, Tu X, Huang Y, Zhang H,
Tan D, Jiang W, Cai S, Zhao P, Song R, et al: Gut microbiome
affects the response to anti-PD-1 immunotherapy in patients with
hepatocellular carcinoma. J Immunother Cancer. 7:1932019.
View Article : Google Scholar : PubMed/NCBI
|
|
112
|
Sasaki R, Kanda T, Yokosuka O, Kato N,
Matsuoka S and Moriyama M: Exosomes and hepatocellular carcinoma:
From bench to bedside. Int J Mol Sci. 20:14062019. View Article : Google Scholar
|
|
113
|
Hao J, Liang C and Jiao B: Eukaryotic
translation initiation factor 3, subunit C is overexpressed and
promotes cell proliferation in human glioma U-87 MG cells. Oncol
Lett. 9:2525–2533. 2015. View Article : Google Scholar
|
|
114
|
Lin XJ, Fang JH, Yang XJ, Zhang C, Yuan Y,
Zheng L and Zhuang SM: Hepatocellular carcinoma cell-secreted
exosomal MicroRNA-210 promotes angiogenesis in vitro and in vivo.
Mol Ther Nucleic Acids. 11:243–252. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
115
|
Tai YL, Chen KC, Hsieh JT and Shen TL:
Exosomes in cancer development and clinical applications. Cancer
Sci. 109:2364–2374. 2018. View Article : Google Scholar
|
|
116
|
Wang G, Liu W, Zou Y, Wang G, Deng Y, Luo
J, Zhang Y, Li H, Zhang Q, Yang Y and Chen G: Three isoforms of
exosomal circPTGR1 promote hepatocellular carcinoma metastasis via
the miR449a-MET pathway. EBioMedicine. 40:432–445. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
117
|
Ang C, Klempner SJ, Ali SM, Madison R,
Ross JS, Severson EA, Fabrizio D, Goodman A, Kurzrock R, Suh J and
Millis SZ: Prevalence of established and emerging biomarkers of
immune checkpoint inhibitor response in advanced hepatocellular
carcinoma. Oncotarget. 10:4018–4025. 2019. View Article : Google Scholar
|
|
118
|
Chen F, Wang J, Wu Y, Gao Q and Zhang S:
Potential biomarkers for liver cancer diagnosis based on
multi-omics strategy. Front Oncol. 12:8224492022. View Article : Google Scholar
|
|
119
|
Dominguez DA and Wang XW: Impact of
next-generation sequencing on outcomes in hepatocellular carcinoma:
How precise are we really? J Hepatocell Carcinoma. 7:33–37. 2020.
View Article : Google Scholar
|
|
120
|
Harding JJ, Nandakumar S, Armenia J,
Khalil DN, Albano M, Ly M, Shia J, Hechtman JF, Kundra R, El Dika
I, et al: Prospective genotyping of hepatocellular carcinoma:
Clinical Implications of next-generation sequencing for matching
patients to targeted and immune therapies. Clin Cancer Res.
25:2116–2126. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
121
|
Lee PC, Chao Y, Chen MH, Lan KH, Lee CJ,
Lee IC, Chen SC, Hou MC and Huang YH: Predictors of response and
survival in immune checkpoint inhibitor-treated unresectable
hepatocellular carcinoma. Cancers (Basel). 12:1822020. View Article : Google Scholar
|
|
122
|
Kim JY, Kronbichler A, Eisenhut M, Hong
SH, van der Vliet HJ, Kang J, Shin JI and Gamerith G: Tumour
mutational burden and efficacy of immune checkpoint inhibitors: A
systematic review and meta-analysis. Cancers (Basel). 11:17982019.
View Article : Google Scholar
|