Introduction
Cancer has been a leading cause of disease-related
deaths worldwide over the past decade (1). Digestive system cancer (DSC) is
responsible for more deaths from cancer than cancer of any other
system. Three out of five of the world's major sources of
cancer-related death are from digestive system tumors (2). Although radiotherapy, chemotherapy,
individualized precision therapy and immunotherapy have been
developed for cancer diagnosis and treatment, the 5-year survival
rate of patients with DSC remains poor (3,4).
Recently, it has been established that numerous biomarkers,
including des-γ-carboxyprothrombin, miR-12 and miR-15b, associated
with tumor screening, diagnosis and prognosis, play significant
roles in the development of DSC (5–7).
However, only a small portion of these biomarkers is well accepted
for clinical usage (8). This may be
due to low specificity, sensitivity or consistency in tumor
development. Therefore, it is clinically necessary and urgent to
develop novel prognostic biomarkers for DSC.
Long non-coding RNAs (lncRNAs) are defined as
non-protein coding RNAs that are >200 nucleotides and do not
contain an open reading frame (9).
Abnormal expression of lncRNAs is observed in various types of
cancer, including breast, colorectal and lung cancer, and these
lncRNAs are involved in tumorigenesis and progression through
interactions with DNA, mRNA, microRNA (miR/miRNA) and proteins
(10–12). In previous years, increasing
evidence has suggested that lncRNAs, such as LINC00645 (13), LINC01133 (14), long non-coding RNA regulating IL-6
transcription (15) and growth
arrest-specific 5 transcript (16),
may serve as novel prognostic biomarkers and potential therapeutic
targets for human cancer.
Colon cancer associated transcript-1 (CCAT1), a
nuclear-restricted lncRNA located on chromosome 8q24.21, was first
identified as an oncogene in colorectal cancer by Nissan (17). Overexpression of CCAT1 was found in
various types of cancer and attracted the attention of a number of
researchers due to its prognostic value (18–20).
You et al (21) found that
CCAT1 was overexpressed in prostate cancer tissue samples and cell
lines, and promoted cell proliferation, which indicated that CCAT1
might suggest an unfavorable outcome for the patient. Similarly, an
investigation by Shen et al (22) suggested that CCAT1 was a key
oncogenic lncRNA correlated with cervical cancer and played an
important role in promoting cervical cancer progression via
regulation of the miR-181a-5p/MMP14 axis. Moreover, Han et
al (23) discovered that CCAT1
was upregulated in triple-negative breast cancer tissues, and
patients with high CCAT1 expression had shorter overall survival
(OS) times compared with those patients with low expression. A
review by Wang et al (24)
summarized that CCAT1 was associated with clinicopathological
features, recurrence-free survival (RFS) and OS rates in patients,
and that CCAT1 could serve as a diagnostic and prognostic marker in
various types of human cancer, including gallbladder cancer,
cholangiocarcinoma and pancreatic cancer. However, due to the
relatively small sample size, these studies on CCAT1 were
moderately limited, and there was no research to systematically
clarify the prognostic value of CCAT1 in DSC. Therefore, the
meta-analysis in the present study aimed to systematically evaluate
the clinicopathological and prognostic role of CCAT1 in patients
with DSC.
Materials and methods
Search strategy and literature
selection
The Preferred Reporting Items for Systematic Reviews
and Meta-Analyses guidelines were strictly followed during the
meta-analysis (25).
A systematic search was performed using PubMed
(https://pubmed.ncbi.nlm.nih.gov/),
Embase (https://www.embase.com), Web of Science
(https://www.webofscience.com), China
National Knowledge Infrastructure (https://en.cnki.com.cn), Cochrane Library (https://www.cochranelibrary.com/), Chinese
Biological Medical Literature database (http://www.sinomed.ac.cn/zh/) and WanFang database
(https://www.wanfangdata.com.cn). The
search terms used for literature retrieval were as follows: ‘colon
cancer associated transcript-1’ or ‘colon cancer associated
transcript 1’ or ‘CCAT1’ or ‘lncRNA CCAT1’ and ‘digestive system’
and ‘cancer’ or ‘tumor’ or ‘neoplasm’ or ‘carcinoma’ or
‘malignancy’. Articles were searched from the creation of each
database to March 31, 2022. Articles eligible for this study were
updated on April 10, 2022.
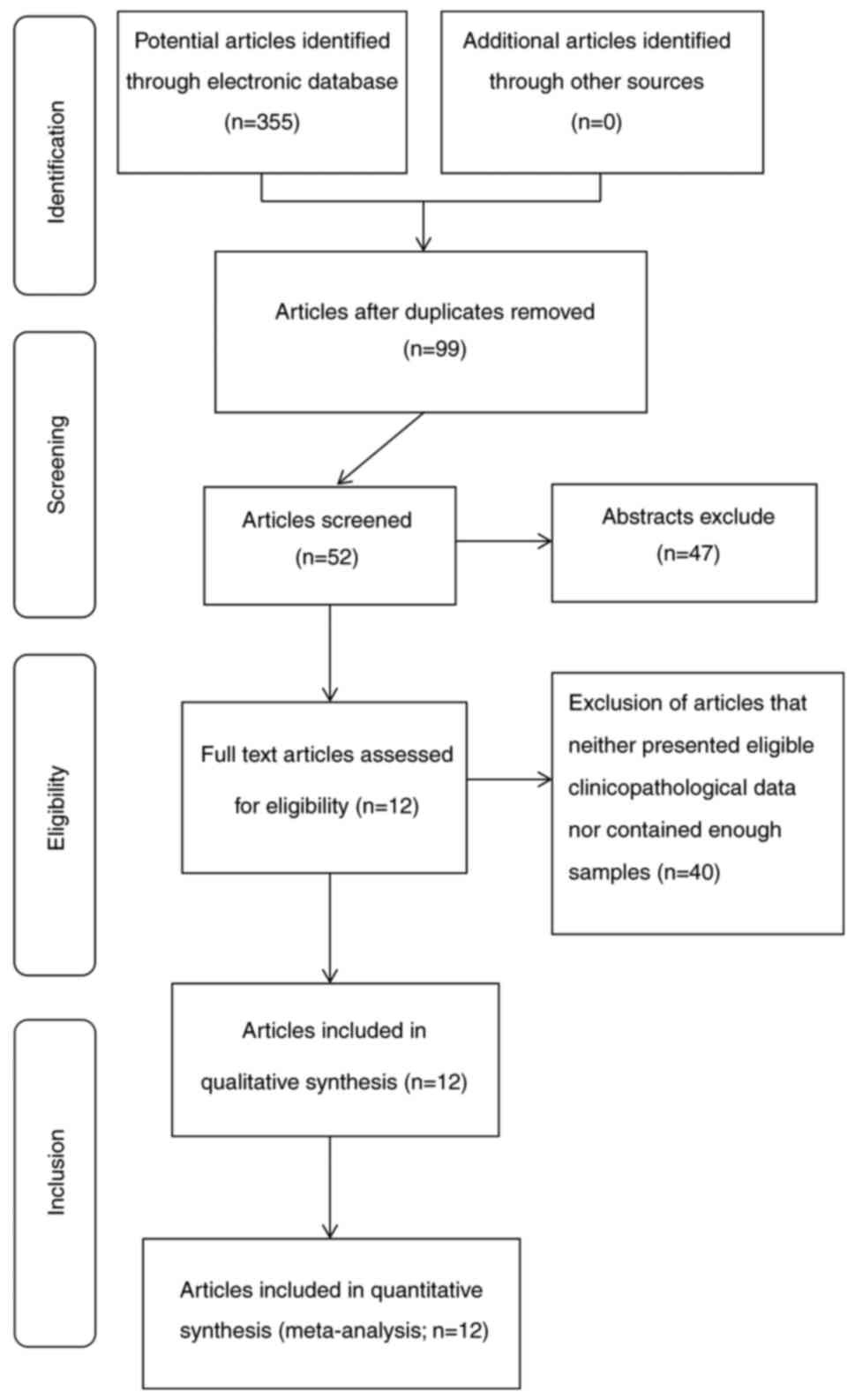
The initial database search yielded 355 articles
according to the search strategy. After screening the titles and
abstracts, 256 literature studies were eliminated due to article
duplication. The remaining 99 articles were quickly browsed, and 47
articles were excluded, as they were reviews, conference summaries
or comments. Following a further assessment of the remaining 52
articles, 40 articles were excluded, as they did not analyze enough
samples or extract data. Finally, 12 articles with a total of 1,719
patients qualified for the present study. Among the 12 included, 1
article was published in 2014, 4 in 2015, 1 in 2016, 5 in 2017 and
1 in 2020. The time range of the studies used for the meta-analysis
was therefore 2014-2020. The details of the screening process are
shown in Fig. 1.
Inclusion and exclusion criteria
Inclusion criteria were as follows: i) Expression
levels of CCAT1 were detected in human DSC; ii) the method of
detecting CCAT1 expression was reverse transcription-quantitative
PCR (RT-qPCR); iii) the hazard ratios (HRs) and corresponding 95%
confidence intervals (CIs) were reported directly or could be
calculated from Kaplan-Meier survival curves; iv) evaluation of a
relationship between high/low CCAT1 expression and clinical
outcomes; v) results included clinicopathological features or
survival rate (OS or RFS); vi) available full-text articles; and
vii) articles were published in English.
Exclusion criteria were as follows: i) Duplicate
publications; ii) studies missing a control group; iii) no data
could be extracted and/or the studies were published as reviews,
abstracts, comments, case reports, expert opinions letters or
editorials; iv) non-human studies; v) articles missing OS or RFS
data; vi) small sample size (total patients <20); vii) articles
not published in English; and viii) HRs could not be calculated
from the published data.
Data extraction and quality
assessment
All data and usable information were screened and
extracted by 2 independent investigators. For all included studies,
the following information was collected: First author, country of
research, publication date, type of cancer, number of patients,
CCAT1 detection method, clinicopathological parameters, survival
analysis and outcome measure. Newcastle-Ottawa Scale (NOS) criteria
were employed to evaluate the quality of each included study
(26). Studies with an NOS score ≥6
were considered to be of high quality; otherwise, they were defined
as low quality. All the studies included in the present
meta-analysis were considered as high quality.
Statistical analysis
The statistical analyses were performed using STATA
14.0 software (StataCorp LP). Statistical analysis with a two-sided
P-value of <0.05 was considered statistically significant. The
original study aims were divided into two categories in the
meta-analysis. The first aim was to assess the correlation of high
CCAT1 expression with clinicopathological characteristics,
including age, sex, depth of infiltration, tumor size, histological
differentiation, lymph node metastasis and TNM stage. The
characteristic standards were based on the latest guidelines by the
publication date (27–29). Pooled odds ratios (ORs) with
corresponding 95% CIs were used to evaluate the association between
CCAT1 expression and clinicopathological parameters. Q test and I2
test were used to assess the statistical heterogeneity.
Heterogeneity was considered present when I2>50% or P<0.05
for the Q test. A random effects model was used to analyze the
data, as heterogeneity was expected for the intervention effects
among multiple studies from different groups and geographical
locations. The second aim was to evaluate the prognostic value of
CCAT1 on OS and RFS with HRs and corresponding 95% CIs. HRs with
corresponding 95% CIs were calculated by the survival data
extracted from Kaplan-Meier curves with Engauge Digitizer version
4.1 (https://markummitchell.github.io/engauge-digitizer/)
when not directly presented in articles. The standard error (SE) of
the HR was computed using lnhr and the upper (lnul) and lower limit
(lnll) of the CIs, taking the mean of the SE of the lnll and lnul,
and selnhr=(lnul-lnll)/(1.96×2). Begg's test was performed to
assess the potential publication bias, and P<0.05 was considered
to indicate a statistically significant difference. The sensitivity
analysis was performed to assess the reliability of the
meta-analysis. STATA 14.0 software (Stata Corp LLC) was used for
the sensitivity analysis, which was performed by excluding studies
one by one and observing whether the heterogeneity changed.
Results
Characteristics of eligible
studies
A total of 12 eligible studies (30–41)
focusing on DSC (1 on colon cancer, 1 on esophageal squamous cell
carcinoma, 2 on cholangiocarcinoma, 2 on gastric cancer, 3 on
colorectal cancer and 3 on hepatocellular carcinoma) were enrolled
in the present meta-analysis. The basic information and
characteristics of each study are summarized in Tables I and II. Among the included studies, 2 came
from the USA and the rest were from China. The expression levels of
CCAT1 were examined by RT-qPCR in all studies. The median
expression levels of CCAT1 in the studies conducted by He et
al (30), Zhu et al
(31) and Deng et al
(33) were regarded as the cut-off
values, while the mean expression levels were set as the cut-off
values in the studies conducted by Zhang et al (38) and Li et al (40). The cut-off value in the study
conducted by Liu and Shangguan (32) was 0.041 and the setting standard was
not introduced. However, the other eligible articles did not report
the cut-off value. Of the 12 studies, 9 provided OS information, 4
presented RFS information and 1 presented DFS information.
Moreover, the included studies were published from 2014 to 2020
with a sample size ranging from 48 to 638.
 | Table I.Basic information of the studies
included in the meta-analysis. |
Table I.
Basic information of the studies
included in the meta-analysis.
| First author,
year | Country | Cancer type | CCAT1 detection
method | Survival
information | Newcastle-Ottawa
Scale score | (Refs.) |
|---|
| He et al,
2014 | China | CC | RT-qPCR | OS | 6 | (30) |
| Zhu et al,
2015 | China | HCC | RT-qPCR | OS, RFS | 7 | (31) |
| Deng et al,
2015 | China | HCC | RT-qPCR | OS, RFS | 7 | (33) |
| McCleland et
al, 2016 | USA | CRC | RT-qPCR | OS | 8 | (37) |
| Wang et al,
2017 | China | HCC | RT-qPCR | OS, DFS | 8 | (36) |
| Zhang E et
al, 2017 | China | ESCC | RT-qPCR | OS | 8 | (38) |
| Jiang et al,
2017 | China | CCA | RT-qPCR | OS | 6 | (34) |
| Ozawa et al,
2017 | USA | CRC | RT-qPCR | OS, RFS | 8 | (35) |
| Liu and Shangguan,
2017 | China | GC | RT-qPCR | OS, RFS | 8 | (32) |
| Zhang et al,
2017 | China | CCA | RT-qPCR | NA | 7 | (39) |
| Li et al,
2017 | China | GC | RT-qPCR | NA | 8 | (40) |
| Shang et al,
2020 | China | CRC | RT-qPCR | NA | 7 | (41) |
| Table II.Characteristics of the studies
included in the meta-analysis. |
Table II.
Characteristics of the studies
included in the meta-analysis.
|
|
Colon
cancer associated transcript-1 expression level |
|
|---|
|
|
|
|
|---|
|
| High | Low |
|
|---|
|
|
|
|
|
|---|
| First author,
year | Total patients,
n | LNM staging, n | Age ≥60 years,
n | T1/2 stage, n | HTS, n | TS>5, n | LD, n | M, n | Total patients,
n | LNM staging, n | Age ≥60 years,
n | T1/2 stage, n | HTS, n | TS>5, n | LD, n | M, n | (Refs.) |
|---|
| He et al,
2014 | 24 | 15 | 10 | NA | 15 | 17 | NA | 14 | 24 | 6 | 13 | NA | 5 | 8 | NA | 9 | (30) |
| Zhu et al,
2015 | 43 | NA | NA | NA | NA | NA | NA | NA | 43 | NA | NA | NA | NA | NA | NA | NA | (31) |
| Deng et al,
2015 | 33 | NA | 8 | NA | NA | 20 | NA | 27 | 33 | NA | 10 | NA | NA | 10 | NA | 25 | (33) |
| McCleland et
al, 2016 | 202 | NA | 107 | NA | 107 | NA | NA | 113 | 436 | NA | 233 | NA | 175 | NA | NA | 213 | (37) |
| Wang et al,
2017 | 60 | NA | 29 | NA | 44 | 36 | NA | 40 | 37 | NA | 16 | NA | 9 | 15 | NA | 18 | (36) |
| Zhang et al,
2017 | 45 | 29 | 26 | 17 | 29 | NA | 27 | 25 | 45 | 19 | 22 | 23 | 15 | NA | 22 | 24 | (38) |
| Jiang et al,
2017 | 47 | 33 | 27 | NA | 34 | NA | 23 | 27 | 44 | 19 | 29 | NA | 19 | NA | 10 | 26 | (34) |
| Ozawa et al,
2017 | 55 | 37 | NA | 11 | 38 | 20 | 3 | 35 | 70 | 32 | NA | 16 | 34 | 27 | 2 | 35 | (35) |
| Liu and Shangguan,
2017 | 121 | 80 | 61 | NA | 73 | 80 | 63 | 45 | 119 | 54 | 70 | NA | 49 | 69 | 36 | 50 | (32) |
| Zhang S et
al, 2017 | 65 | 48 | 35 | 16 | 49 | NA | NA | 27 | 55 | 16 | 35 | 38 | 17 | NA | NA | 27 | (39) |
| Li et al,
2017 | 41 | 31 | 35 | 9 | 19 | 16 | 23 | 17 | 27 | 12 | 25 | 10 | 23 | 11 | 22 | 23 | (40) |
| Shang et al,
2020 | NA | 29 | NA | NA | 14 | NA | NA | 12 | NA | 8 | NA | NA | 7 | NA | NA | 13 | (41) |
Correlation of CCAT1 expression with
clinicopathological characteristics
The association between CCAT1 expression and
clinicopathological characteristics was assessed in 12 studies with
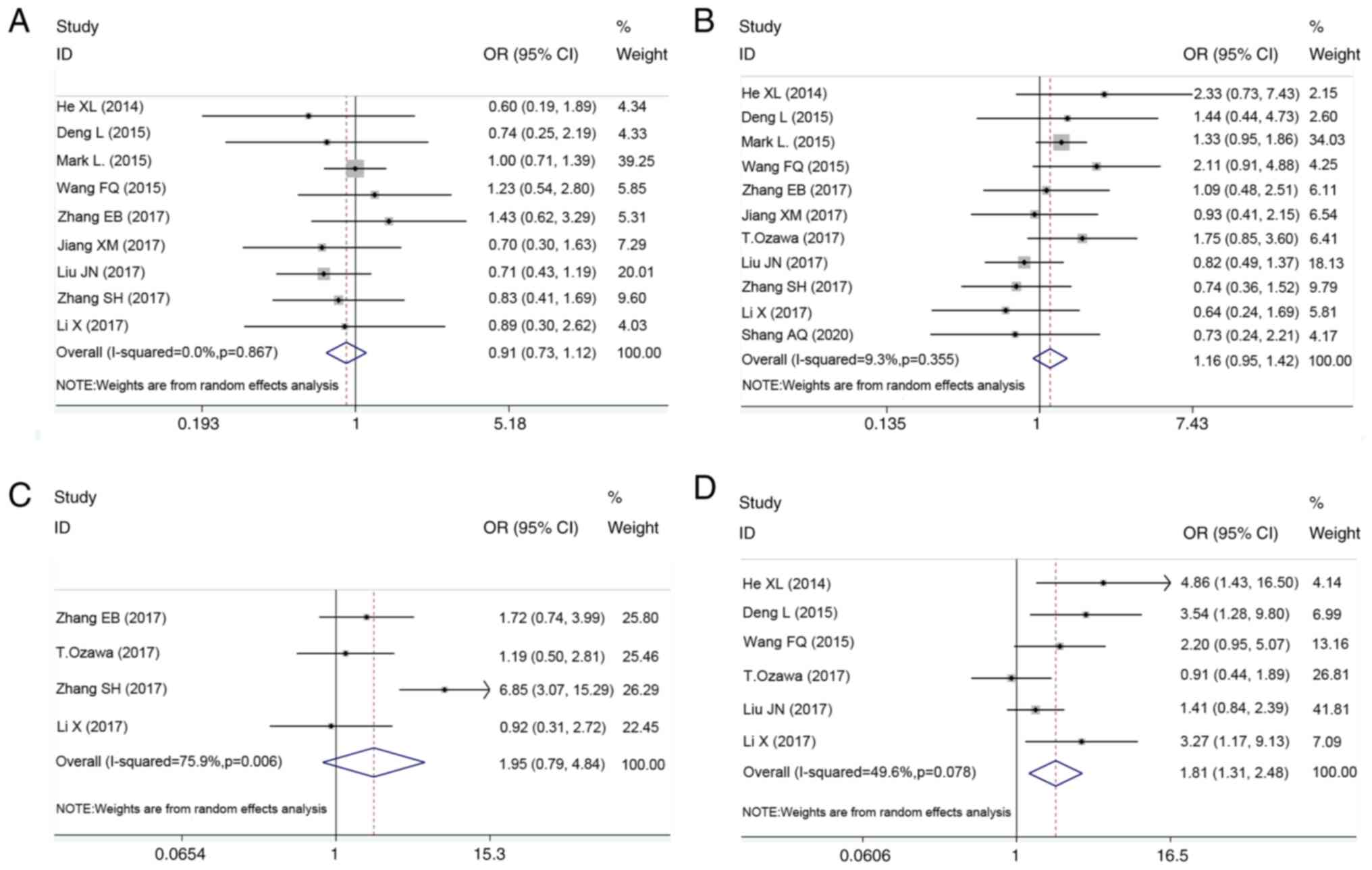
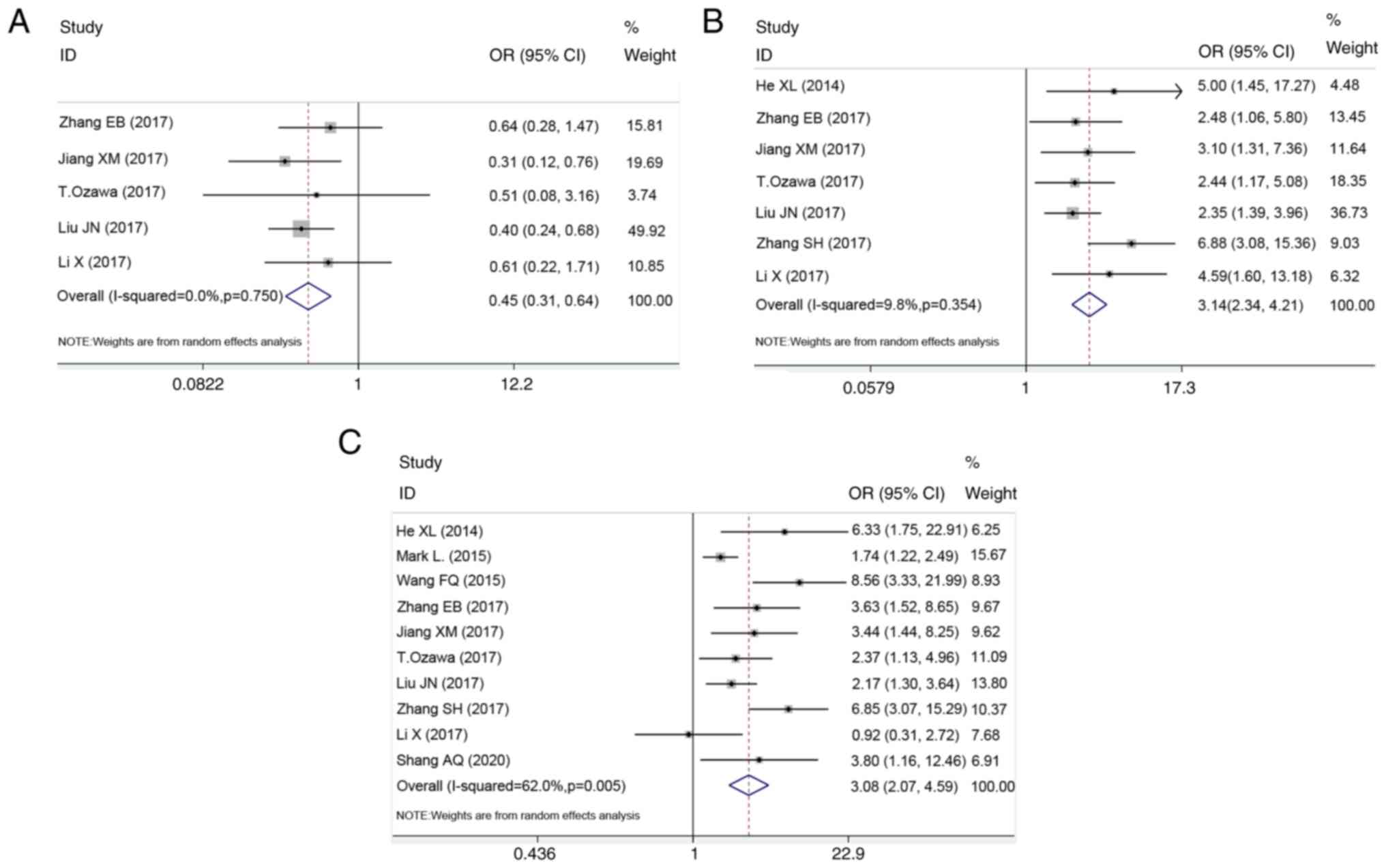
six types of DSC. As shown in Figs.
2 and 3, and Table III, high CCAT1 expression levels
were significantly associated with larger tumor size (>5 cm vs.
≤5 cm; OR, 1.81; 95% CI, 1.31-2.48; P<0.001; Fig. 2D), poorer differentiation (high and
moderate vs. low; OR, 0.45; 95% CI, 0.31-0.64; P<0.001; Fig. 3A), earlier lymph node metastasis
(yes vs. no; OR, 3.14; 95% CI, 2.34-4.22, P<0.001; Fig. 3B) and advanced TNM stage (III+IV vs.
I+II; OR, 3.08; 95% CI, 2.07-4.59, P<0.001, Fig. 3C). However, no significant
association was found with age (≥60 vs. <60; OR, 0.91; 95% CI,
0.73-1.12; P=0.369; Fig. 2A), sex
(male vs. female; OR, 1.16; 95% CI, 0.95-1.42; P=0.156; Fig. 2B) and depth of infiltration (T3+4
vs. T1+2; OR, 1.95; 95% CI, 0.79-4.84; P=0.147; Fig. 2C).
| Table III.Pooled ORs for the association
between colon cancer associated transcript-1 expression levels and
clinicopathological parameters in the meta-analysis. |
Table III.
Pooled ORs for the association
between colon cancer associated transcript-1 expression levels and
clinicopathological parameters in the meta-analysis.
|
|
|
|
|
| Heterogeneity |
|
|---|
|
|
|
|
|
|
|
|
|---|
| Clinicopathological
features | Number of
studies | Number of
patients | Pooled OR (95%
CI) | P-value | I2
(%) | P-value | Model used |
|---|
| Age | 9 | 1,268 | 0.91
(0.73-1.12) | 0.369 | 0.00 | 0.867 | Random |
| Sex | 11 | 1,633 | 1.16
(0.95-1.42) | 0.156 | 9.30 | 0.355 | Random |
| Depth of
infiltration | 4 | 403 | 1.95
(0.79-4.84) | 0.147 | 75.90 | 0.006 | Random |
| Tumor size | 6 | 644 | 1.81
(1.31-2.48) | <0.001 | 49.60 | 0.078 | Random |
|
Differentiation | 5 | 596 | 0.45
(0.31-0.64) | <0.001 | 0.00 | 0.750 | Random |
| Lymph node
metastasis | 7 | 782 | 3.14
(2.34-4.21) | <0.001 | 9.80 | 0.354 | Random |
| TNM stage | 10 | 1,567 | 3.08
(2.07-4.59) | <0.001 | 62.00 | 0.005 | Random |
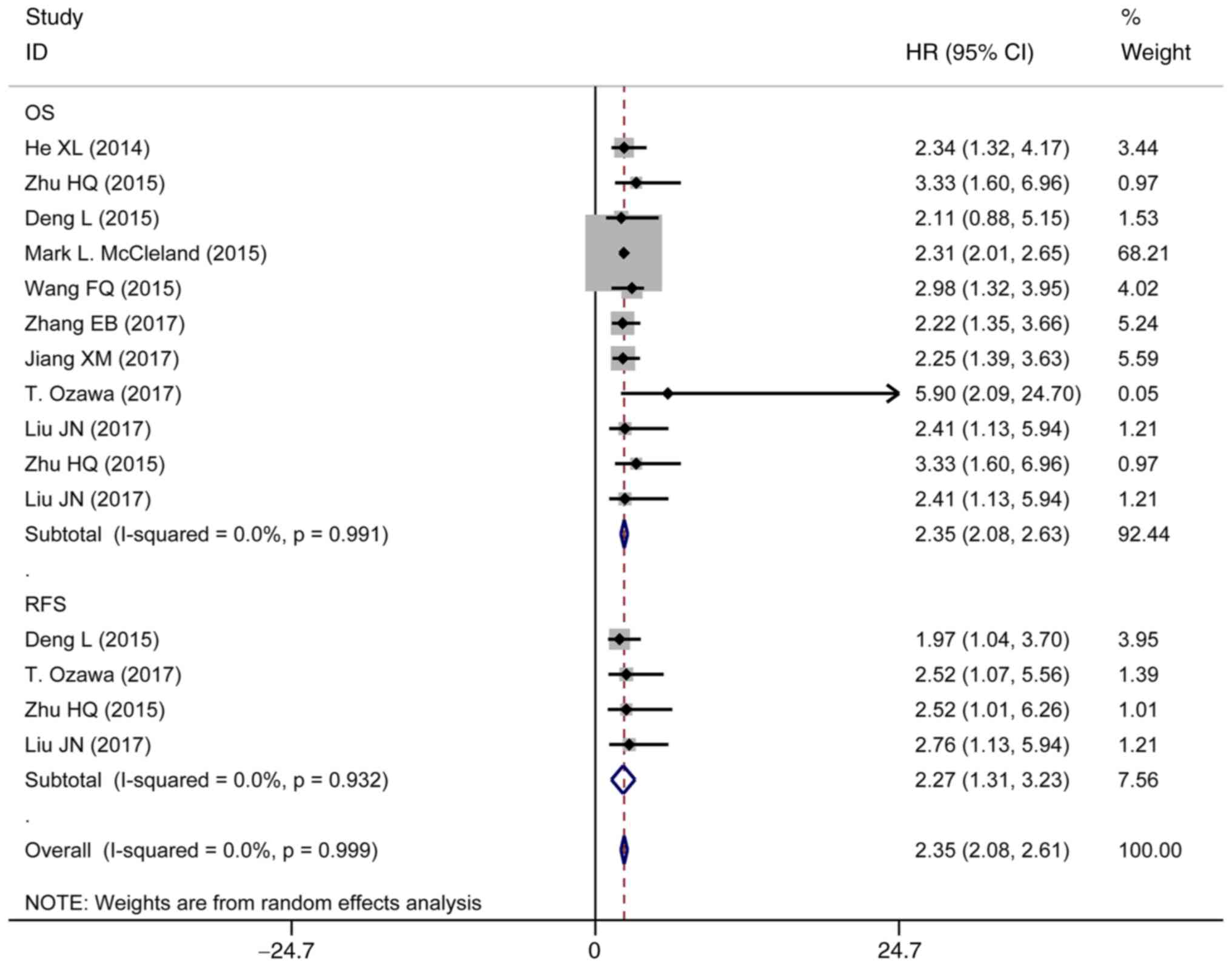
Association between CCAT1 expression
and OS
The studies containing OS rate data covered 1,481
patients. A random effects model was applied to calculate the
pooled HRs and the respective 95% CIs. Subsequently, the result
suggested that CCAT1 expression had a significant effect on OS
(pooled HR, 2.35; 95% CI, 2.08-2.63; Fig. 4 and Table IV), in which higher expression of
CCAT1 was associated with a poorer OS outcome.
| Table IV.Related survival data of enrolled
studies in the meta-analysis. |
Table IV.
Related survival data of enrolled
studies in the meta-analysis.
|
|
|
| Related information
on survival |
|
|
|---|
|
|
|
|
|
|
|
|---|
|
|
|
| Overall
survival | Recurrence-free
survival |
|
|
|---|
| First author,
year | Cancer type | Sample size |
|
| HR estimation
method | (Refs.) |
|---|
| Univariate | Multivariate | Univariate | Multivariate |
|---|
| He et al,
2014 | CC | 48 | 2.34
(1.32-4.17) | NA | NA | NA | KM | (30) |
| Zhu et al,
2015 | HCC | 86 | 3.33
(1.60-6.96) | 3.33
(1.60-6.96) | NA | NA | Rep | (31) |
| Deng et al,
2015 | HCC | 66 | 2.11
(0.88-5.15) | NA |
1.97(1.04-3.70) | NA | KM | (33) |
| McCleland et
al, 2016 | CRC | 638 | 2.31
(2.01-2.65) | NA | NA | NA | KM | (37) |
| Wang et al,
2017 | HCC | 97 | 3.27
(1.62-6.27) | 2.98
(1.32-3.95) | NA | NA | Rep | (36) |
| Zhang et al,
2017 | ESCC | 90 | 2.22
(1.35-3.66) | NA | NA | NA | KM | (38) |
| Jiang et al,
2017 | CCA | 91 | 3.14
(1.97-5.01) | 2.25
(1.40-3.63) | NA | NA | Rep | (34) |
| Ozawa et al,
2017 | CRC | 125 | NA | 5.90
(2.09-24.70) | NA | 2.52
(1.07-5.56) | Rep | (35) |
| Liu and Shangguan,
2017 | GC | 240 | 2.16
(0.98-6.65) | 2.41
(1.13-5.94) | NA | NA | Rep | (32) |
Association between CCAT1 expression
and RFS
A total of 4 studies comprising 191 subjects
reported the RFS based on CCAT1 expression levels in patients with
DSC (Fig. 4 and Table IV). The pooled HR was 2.27 (95% CI,
1.31-3.23) with no significant heterogeneity (I2=0.0%; P=0.932).
This suggested that patients with high CCAT1 expression tended to
have shorter RFS times compared with those patients with low CCAT1
expression.
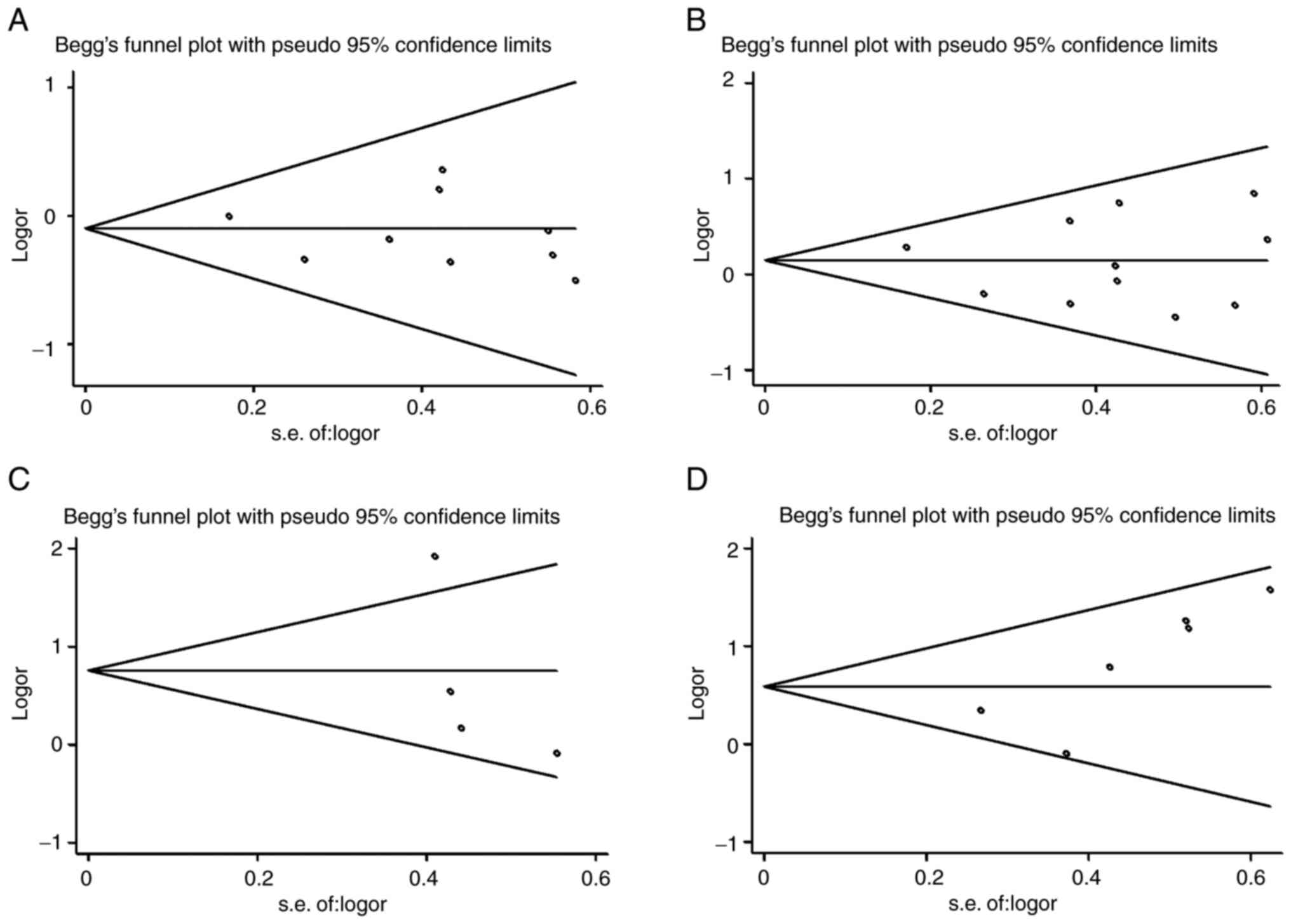
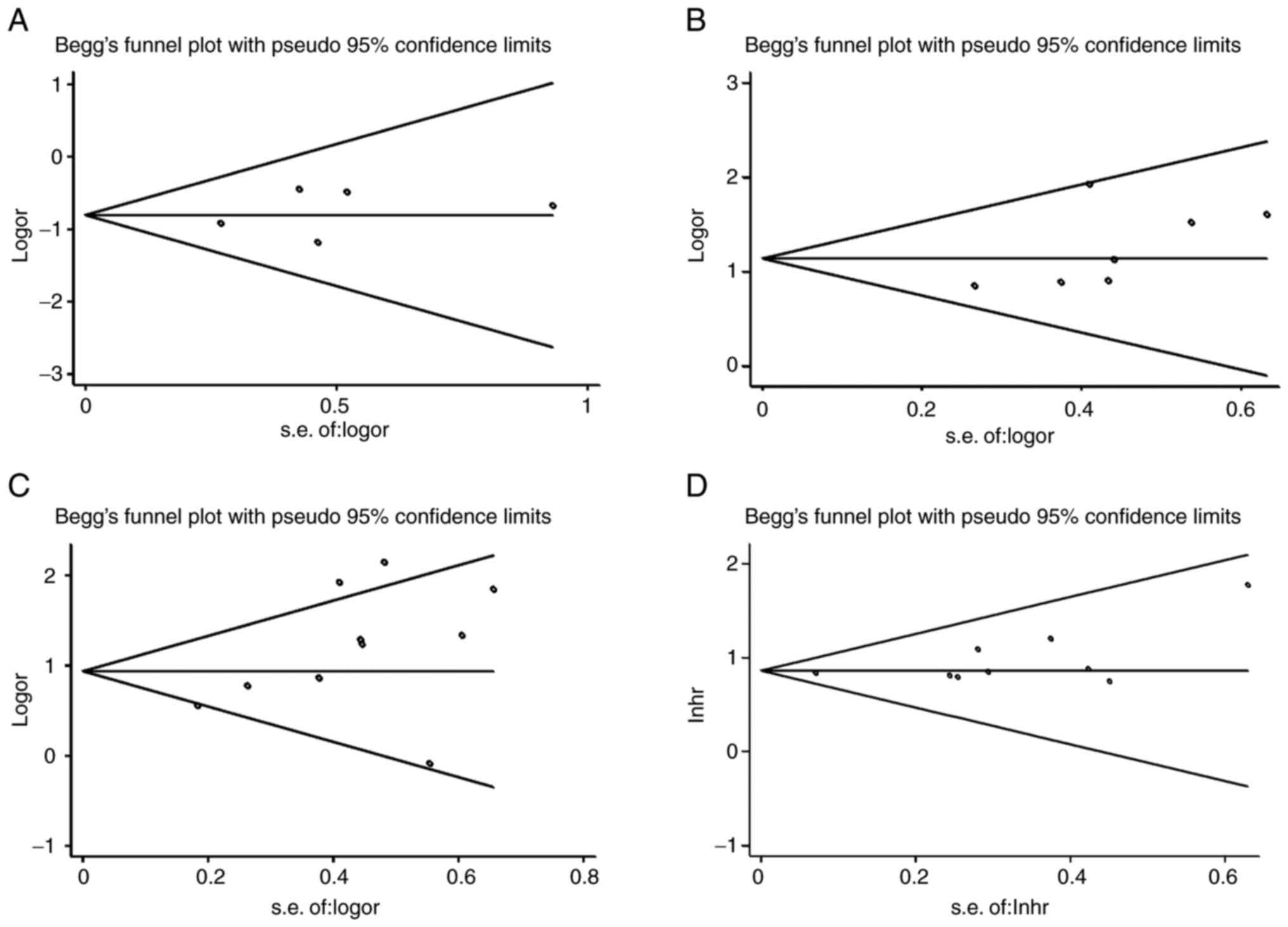
Publication bias
To assess the potential publication bias, Begg's
funnel analysis was performed. As shown in Figs. 5 and 6, there was no publication bias for age
(P=0.602), sex (P=0.533), depth of infiltration (P=0.089), tumor
size (P=0.060), differentiation (P=1.000), lymph node metastasis
(P=0.072), TNM stage (P=0.210) and OS (P=0.076).
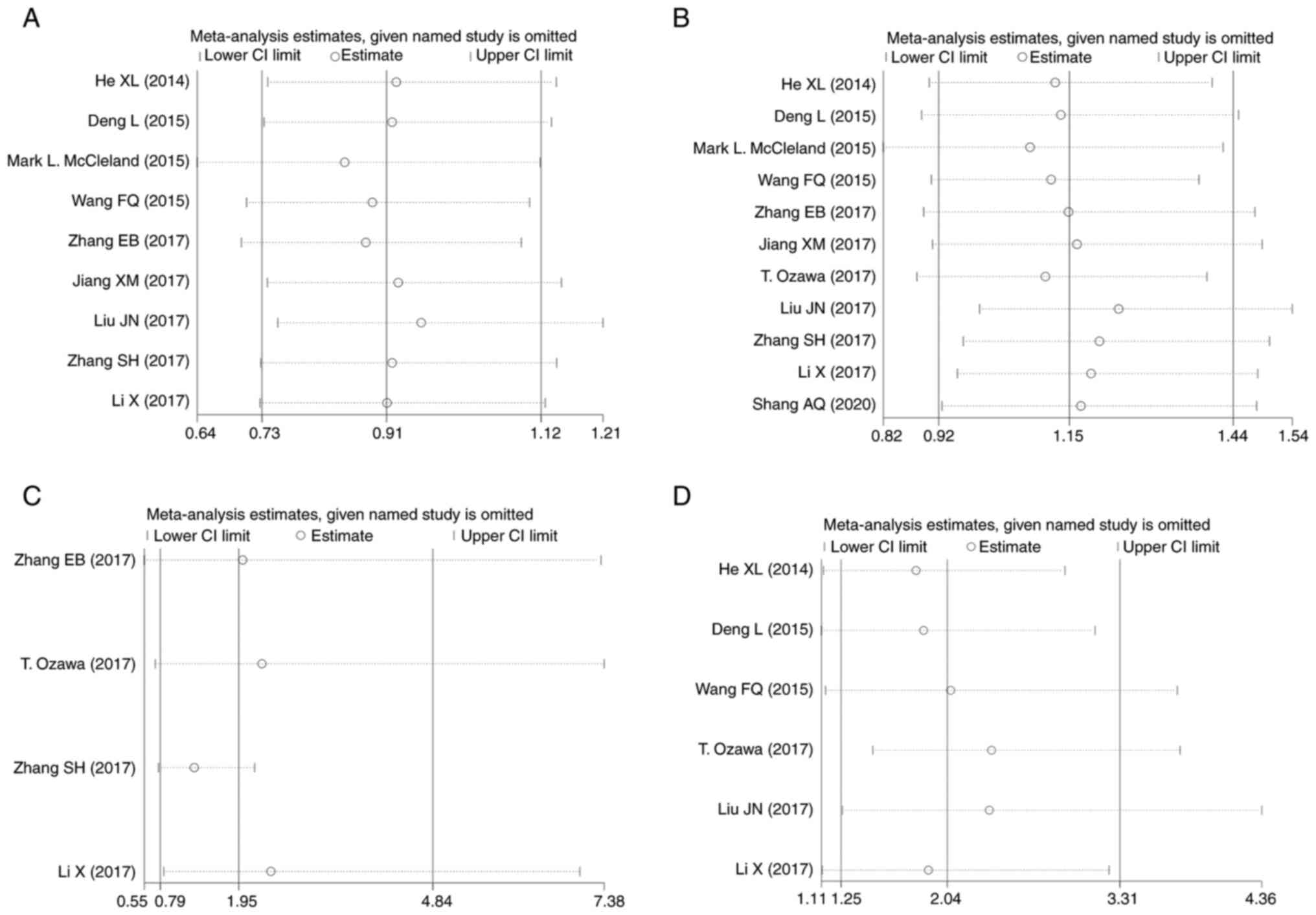
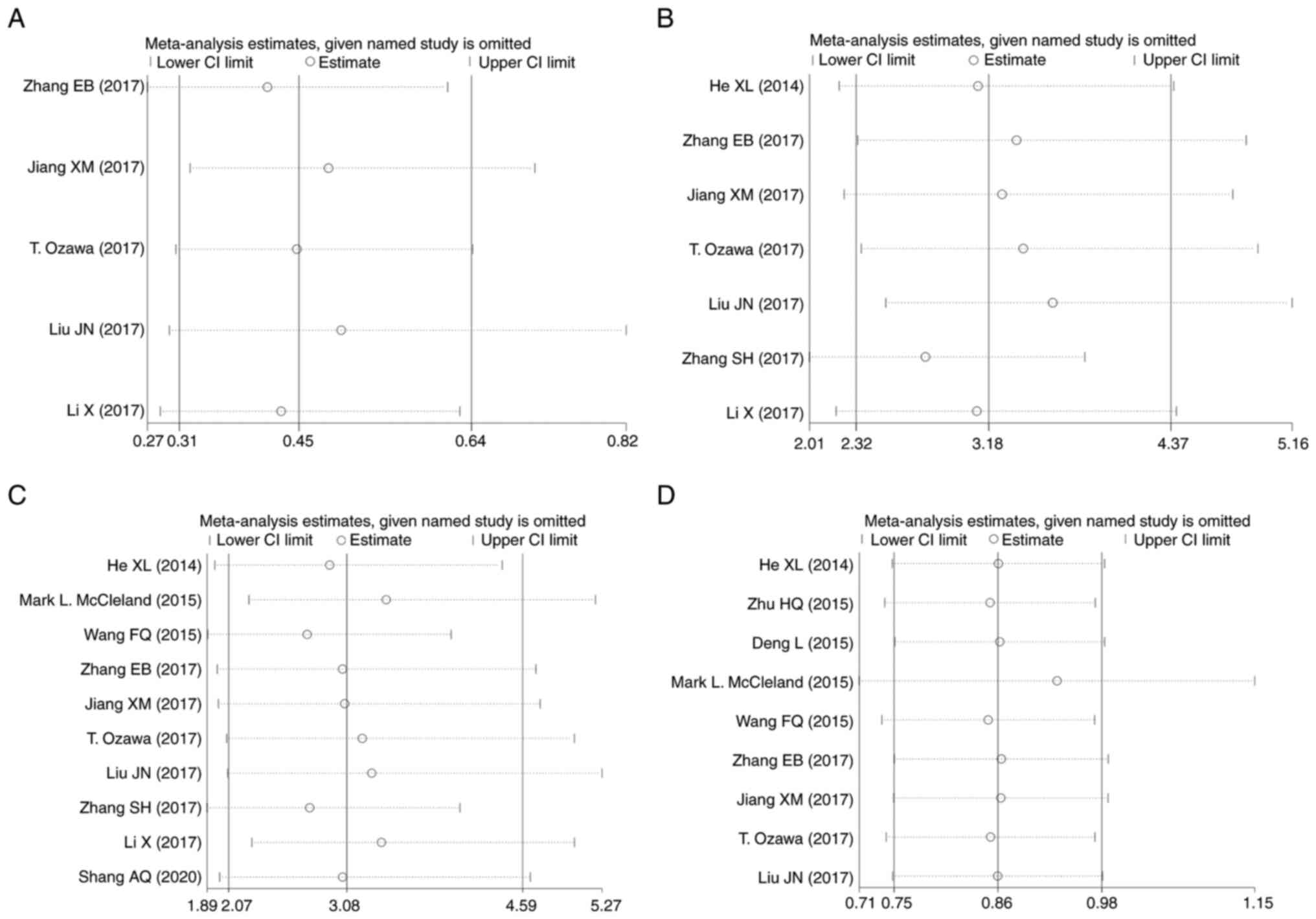
Sensitivity analysis
A sensitivity analysis was conducted to detect the
influence of an individual study on the pooled results by omitting
a single study each time (Figs. 7
and 8). The results verified that
any individual study could not significantly change the pooled
estimates, revealing that the results of the synthetic analysis
were stable and credible.
Discussion
DSC, consisting mainly of esophageal cancer, gastric
cancer, colorectal cancer, hepatocellular carcinoma, gallbladder
cancer and pancreatic cancer, has become a health burden with high
mortality worldwide, and a marked increase in incidence has been
observed (42,43). Traditionally, clinicopathological
variables, such as tumor size, depth of infiltration,
differentiation, lymph node metastasis and TNM stage, are applied
to predict the survival outcome of patients with DSC (7). Early stage DSC has a significantly
improved survival outcome compared with advanced-stage DSC, in
which tumor invasion and metastasis are common pathological
characteristics of a poor prognosis (44). Thus, seeking new tumor biomarkers or
therapeutic targets to increase the survival rate of patients with
DSC has become the key to clinical work (45). Emerging evidence has revealed that
lncRNAs have become a topic of interest due to their functions in a
variety of biological processes, and the alteration of lncRNA
expression could result in abnormal expression of gene products,
cellular differentiation, protein localization and DNA damage
response, leading to the occurrence and development of cancer
(12,46). In a previous study, aberrant
expression of lncRNAs was related to clinical outcomes for patients
with cancer, and could be tracked in numerous malignant biological
behaviors, including proliferation, invasion, migration, the cell
cycle, apoptosis and angiogenesis, which indicated the potential
roles of lncRNAs as biomarkers or therapeutic targets in cancer
(47). Moreover, due to great
specificity, sensitivity and convenient detection in bodily fluids,
lncRNAs have significant potential to be a promising biomarker for
the early detection and accurate survival outcome prediction of
patients with DSC.
The lncRNA CCAT1 has been found to be upregulated in
different types of cancer (17).
Recently, emerging studies suggested that CCAT1 participated in
multiple cellular processes involved in DSC, such as cell
proliferation, invasion and drug resistance, by targeting mRNAs,
regulating miRNAs or competing with endogenous RNAs (48–50).
Zhang et al (51)
demonstrated that CCAT1 could regulate the expression of CCNE1 by
acting as a competing endogenous RNA to sponge miR-30c-2-3p,
thereby regulating the cell proliferation and metastasis of
hepatocellular carcinoma (HCC), indicating that CCAT1 might be a
novel therapeutic target for HCC. An investigation by Fang et
al (52) found that the
expression of CCAT1 in gastric cancer tissues was higher than that
in adjacent tumor tissues, and CCAT1 could promote the metastasis
of gastric cancer by epithelial-mesenchymal transition. Similarly,
a study by Li et al (53)
revealed that CCAT1 upregulation could promote cell proliferation
and migration by affecting Bmi-1 expression in gastric cancer. In
addition, Hu et al (54)
demonstrated that CCAT1 could influence the cell proliferation and
drug resistance of esophageal cancer by inhibiting the
miR-143/PLK1/BUBR1 axis, and that CCAT1 could be a potential
biomarker for esophageal cancer. Together, these studies revealed
that CCAT1 could be a potential prognostic biomarker for DSC.
In order to clarify the association of CCAT1
expression levels with clinicopathological features and patient
survival in DSC, the present meta-analysis was performed. A
previous meta-analysis reported that CCAT1 expression was related
to certain clinicopathological variables (tumor size, lymph node
metastasis, TNM stage, distant metastasis, microvascular invasion
and capsular formation) in all types of cancer, and had a
predictive value for a poor prognosis of cancer (55), which was consistent with the present
study conclusions. In contrast to the previous study, digestive
system tumors were analyzed in the present study rather than all
tumor types. In the present meta-analysis, a total of 1,719
patients from 12 studies were enrolled. The random effects model
was applied for analyzing the relationship between CCAT1 expression
and clinicopathological variables, including age, sex, tumor size,
differentiation and lymph node metastasis. Due to the presence of
moderate heterogeneity among the studies in terms of depth of
infiltration (P=0.006; I2=75.9%) and TNM stage (P=0.005;
I2=62.0%), a random effects model was used to pool data.
It was observed that 4 studies had significant statistical
heterogeneity for depth of infiltration and 10 studies for TNM
stage. This heterogeneity might be the result of design
discrepancies for depth of infiltration among the studies. The
heterogeneity for TNM stage might be due to the different staging
criteria being used by the studies. Most studies did not introduce
the staging criteria they used. The results demonstrated that
increased expression of CCAT1 was significantly related to larger
tumor size (OR, 1.81; 95% CI, 1.31-2.48), poorer differentiation
(OR, 0.45; 95% CI, 0.31-0.64), earlier lymph node metastasis (OR,
3.14; 95% CI, 2.34-4.22) and advanced TNM stage (OR, 3.08; 95% CI,
2.07-4.59). However, no significant association was observed
between the expression of CCAT1 and other clinicopathological
features, including age, sex and depth of infiltration. In
addition, considering the survival rate of patients, the
association between the expression level of CCAT1 and the prognosis
of patients with DSC was clarified. The results showed that
elevated CCAT1 expression was associated with poor OS (HR, 2.37;
95% CI, 2.11-2.67) and RFS (HR, 2.16; 95% CI, 1.31-3.57). Moreover,
Begg's funnel analysis was conducted to estimate the underlying
publication bias. The result indicated that there was no
significant publication bias for age, sex, depth of infiltration,
tumor size, differentiation, lymph node metastasis, TNM stage and
OS. The sensitivity analysis suggested that each individual study
could not influence the conclusions significantly, indicating the
robustness of the results.
Although the association between CCAT1 expression
and the prognosis of patients with DSC was comprehensively
evaluated, there were still some limitations in the present
meta-analysis. Firstly, the lack of further refinement in the
research strategy due to the digestive system tumors being analyzed
as a whole, and not also as separate cancer entities (e.g.,
colorectal, gastric and esophageal cancer), was a major limitation
of the present study. Secondly, most studies were from China, and
only 2 articles were from the USA, which may not fully represent
the conclusions of all countries, and diminished the overall effect
of the results. On the one hand, it might be that through the
inclusion and exclusion criteria, only articles published in
English were used, which led to relevant studies in other countries
not being included. On the other hand, in recent years, the
incidence of DSC in China has gradually increased (56). It is possible that some eating
habits are high-risk factors for the occurrence of DSC, leading to
more articles on DSC in China than in other countries. Thirdly, the
number of patients enrolled in some studies was relatively small,
and the studies could not cover all types of DSC. Fourthly, some of
the HRs were calculated by reconstructing survival curves rather
than being directly obtained from the primary data. Fifthly, most
enrolled studies presented positive results, and those with
negative results were less likely to be published. Sixthly, the
cut-off value of CCAT1 expression levels in each study had its own
criteria (median or mean), which meant that there was no consensus
on the cut-off estimates for differentiating high or low CCAT1
expression. Finally, the biological features and molecular
mechanisms associated with different types of DSC may generate
potentially inconsistent results. However, in the present study,
there was still scope to analyze the existing CCAT1 articles and
explore the clinical significance of CCAT1 in DSC. It is hoped that
there will be more relevant studies of CCAT1 from other countries
and high-quality studies involving large numbers of patients in the
future, which will further strengthen the present findings and will
enhance the understanding of CCAT1 in DSC and its possible
mechanisms.
CCAT1 could serve as a potential biomarker for the
prognosis of patients with DSC and potentially participate in DSC
development and progression. Importantly, the present study sheds
some light on the clinical and molecular mechanisms underlying the
pathogenesis of DSC and facilitates the understanding of novel
therapeutic targets in DSC. Therefore, more relevant studies that
meet the requirements should be included in future studies to
further evaluate the value of CCAT1 in the prognosis of DSC, so as
to provide more sufficient and powerful evidence-based medical
results and guide clinical medical work. A comprehensive prognosis
should be based on a combination of multiple prognostic approaches
to improve the accuracy. Furthermore, more well-designed studies
involving all types of DSC are needed to verify the prognostic
value of CCAT1 in DSC. In future, the mechanism of CCAT1 expression
from the perspective of molecular and epigenetics should be
explored, and the tissue specificity of CCAT1 expression in
different histological types of tumors should be validated.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
ZHX conceived and designed the study. YY collected
and analyzed the data, and drafted the paper. CD and MXJ helped
with the data analysis and manuscript revision. YY and HN analyzed
the data and revised the final paper. ZHX and CD confirm the
authenticity of all the raw data. All authors have read and
approved the final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Hu J, Ni G, Mao L, Xue X, Zhang J, Wu W,
Zhang S, Zhao H, Ding L and Wang L: LINC00565 promotes
proliferation and inhibits apoptosis of gastric cancer by targeting
miR-665/AKT3 axis. Onco Targets Ther. 12:7865–7875. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sung H, Ferlay J, Siegel RL, Laversanne M,
Soerjomataram I, Jemal A and Bray F: Global cancer statistics 2020:
GLOBOCAN estimates of incidence and mortality worldwide for 36
cancers in 185 countries. CA Cancer J Clin. 71:209–249. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Jiang J, Ma T, Xi W, Yang C, Wu J, Zhou C,
Wang N, Zhu Z and Zhang J: Pre-treatment inflammatory biomarkers
predict early treatment response and favorable survival in patients
with metastatic colorectal cancer who underwent first line
cetuximab plus chemotherapy. Cancer Manag Res. 11:8657–8668. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fiorillo C, Quero G and Alfieri S:
Resection margin status in pancreatic cancer surgery: Is it really
less important than the N status? Br J Surg. 106:15592019.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ayoub WS, Steggerda J, Yang JD, Kuo A,
Sundaram V and Lu SC: Current status of hepatocellular carcinoma
detection: Screening strategies and novel biomarkers. Ther Adv Med
Oncol. 11:17588359198691202019. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Salati M, Orsi G, Smyth E, Aprile G,
Beretta G, De Vita F, Di Bartolomeo M, Fanotto V, Lonardi S, Morano
F, et al: Gastric cancer: Translating novels concepts into clinical
practice. Cancer Treat Rev. 79:1018892019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Serra O, Galán M, Ginesta MM, Calvo M,
Sala N and Salazar R: Comparison and applicability of molecular
classifications for gastric cancer. Cancer Treat Rev. 77:29–34.
2019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Necula L, Matei L, Dragu D, Neagu AI,
Mambet C, Nedeianu S, Bleotu C, Diaconu CC and Chivu-Economescu M:
Recent advances in gastric cancer early diagnosis. World J
Gastroenterol. 25:2029–2044. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
López-Urrutia E, Bustamante Montes LP,
Ladrón de Guevara Cervantes D, Pérez-Plasencia C and Campos-Parra
AD: Crosstalk between long non-coding RNAs, Micro-RNAs and mRNAs:
Deciphering molecular mechanisms of master regulators in cancer.
Front Oncol. 9:6692019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Shang W, Adzika GK, Li Y, Huang Q, Ding N,
Chinembiri B, Rashid MS and Machuki JO: Molecular mechanisms of
circular RNAs, transforming growth factor-β, and long noncoding
RNAs in hepatocellular carcinoma. Cancer Med. 8:6684–6699. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Li MY, Tang XH, Fu Y, Wang TJ and Zhu JM:
Regulatory mechanisms and clinical applications of the long
non-coding RNA PVT1 in cancer treatment. Front Oncol. 9:7872019.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chi Y, Wang D, Wang J, Yu W and Yang J:
Long non-coding RNA in the pathogenesis of cancers. Cells.
8:10152019. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li C, Zheng H, Hou W, Bao H, Xiong J, Che
W, Gu Y, Sun H and Liang P: Long non-coding RNA linc00645 promotes
TGF-β-induced epithelial-mesenchymal transition by regulating
miR-205-3p-ZEB1 axis in glioma. Cell Death Dis. 10:7172019.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Song Z, Zhang X, Lin Y, Wei Y, Liang S and
Dong C: LINC01133 inhibits breast cancer invasion and metastasis by
negatively regulating SOX4 expression through EZH2. J Cell Mol Med.
23:7554–7565. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang J, Zhou J, Jiang C, Zheng J, Namba H,
Chi P and Asakawa T: LNRRIL6, a novel long noncoding RNA, protects
colorectal cancer cells by activating the IL-6-STAT3 pathway. Mol
Oncol. 13:2344–2360. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Li W, Li N, Shi K and Chen Q: Systematic
review and meta-analysis of the utility of long non-coding RNA GAS5
as a diagnostic and prognostic cancer biomarker. Oncotarget.
8:66414–66425. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nissan A, Stojadinovic A,
Mitrani-Rosenbaum S, Halle D, Grinbaum R, Roistacher M, Bochem A,
Dayanc BE, Ritter G, Gomceli I, et al: Colon cancer associated
transcript-1: A novel RNA expressed in malignant and pre-malignant
human tissues. Int J Cancer. 130:1598–1606. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ghafouri-Fard S and Taheri M: Colon
cancer-associated transcripts 1 and 2: Roles and functions in human
cancers. J Cell Physiol. Jan 28–2019.(Epub ahead of print).
View Article : Google Scholar
|
|
19
|
Guo X and Hua Y: CCAT1: An oncogenic long
noncoding RNA in human cancers. J Cancer Res Clin Oncol.
143:555–562. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang C, Wang W, Lin J, Xiao J and Tian Y:
lncRNA CCAT1 promotes bladder cancer cell proliferation, migration
and invasion. Int Braz J Urol. 45:549–559. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
You Z, Liu C, Wang C, Ling Z, Wang Y, Wang
Y, Zhang M, Chen S, Xu B, Guan H and Chen M: LncRNA CCAT1 promotes
prostate cancer cell proliferation by interacting with DDX5 and
MIR-28-5P. Mol Cancer Ther. 18:2469–2479. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shen H, Wang L, Xiong J, Ren C, Gao C,
Ding W, Zhu D, Ma D and Wang H: Long non-coding RNA CCAT1 promotes
cervical cancer cell proliferation and invasion by regulating the
miR-181a-5p/MMP14 axis. Cell Cycle. 18:1110–1121. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Han C, Li X, Fan Q, Liu G and Yin J: CCAT1
promotes triple-negative breast cancer progression by suppressing
miR-218/ZFX signaling. Aging (Albany NY). 11:4858–4875. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang N, Yu Y, Xu B, Zhang M, Li Q and Miao
L: Pivotal prognostic and diagnostic role of the long non-coding
RNA colon cancer-associated transcript 1 expression in human cancer
(review). Mol Med Rep. 19:771–782. 2019.PubMed/NCBI
|
|
25
|
Moher D, Liberati A, Tetzlaff J and Altman
DG; PRISMA Group, : Preferred reporting items for systematic
reviews and meta-analyses: The PRISMA statement. J Clin Epidemiol.
62:1006–1012. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Seitz AK, Christensen LL, Christensen E,
Faarkrog K, Ostenfeld MS, Hedegaard J, Nordentoft I, Nielsen MM,
Palmfeldt J, Thomson M, et al: Profiling of long non-coding RNAs
identifies LINC00958 and LINC01296 as candidate oncogenes in
bladder cancer. Sci Rep. 7:3952017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Weiser MR: AJCC 8th edition: Colorectal
cancer. Ann Surg Oncol. 25:1454–1455. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Chun YS, Pawlik TM and Vauthey JN: 8th
Edition of the AJCC cancer staging manual: Pancreas and
hepatobiliary cancers. Ann Surg Oncol. 25:845–847. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tsoukalas N, Tsapakidis K and Kamposioras
K: AJCC-8 TNM staging system for gastric cancer. Is there a scope
for improvement? J Invest Surg. 33:939–940. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
He X, Tan X, Wang X, Jin H, Liu L, Ma L,
Yu H and Fan Z: C-Myc-activated long noncoding RNA CCAT1 promotes
colon cancer cell proliferation and invasion. Tumour Biol.
35:12181–12188. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Zhu HQ, Zhou X, Chang H, Li HG, Liu FF, Ma
CQ and Lu J: Aberrant expression of CCAT1 regulated by c-Myc
predicts the prognosis of hepatocellular carcinoma. Asian Pac J
Cancer Prev. 16:5181–5185. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Liu JN and Shangguan YM: Long non-coding
RNA CARLo-5 upregulation associates with poor prognosis in patients
suffering gastric cancer. Eur Rev Med Pharmacol Sci. 21:530–534.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Deng L, Yang SB, Xu FF and Zhang JH: Long
noncoding RNA CCAT1 promotes hepatocellular carcinoma progression
by functioning as let-7 sponge. J Exp Clin Cancer Res. 34:182015.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Jiang XM, Li ZL, Li JL, Zheng WY, Li XH,
Cui YF and Sun DJ: LncRNA CCAT1 as the unfavorable prognostic
biomarker for cholangiocarcinoma. Eur Rev Med Pharmacol Sci.
21:1242–1247. 2017.PubMed/NCBI
|
|
35
|
Ozawa T, Matsuyama T, Toiyama Y, Takahashi
N, Ishikawa T, Uetake H, Yamada Y, Kusunoki M, Calin G and Goel A:
CCAT1 and CCAT2 long noncoding RNAs, located within the 8q.24.21
‘gene desert’, serve as important prognostic biomarkers in
colorectal cancer. Ann Oncol. 28:1882–1888. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wang F, Xie C, Zhao W, Deng Z, Yang H and
Fang Q: Long non-coding RNA CARLo-5 expression is associated with
disease progression and predicts outcome in hepatocellular
carcinoma patients. Clin Exp Med. 17:33–43. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
McCleland ML, Mesh K, Lorenzana E, Chopra
VS, Segal E, Watanabe C, Haley B, Mayba O, Yaylaoglu M, Gnad F and
Firestein R: CCAT1 is an enhancer-templated RNA that predicts BET
sensitivity in colorectal cancer. J Clin Invest. 126:639–652. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Zhang E, Han L, Yin D, He X, Hong L, Si X,
Qiu M, Xu T, De W, Xu L, et al: H3K27 acetylation activated-long
non-coding RNA CCAT1 affects cell proliferation and migration by
regulating SPRY4 and HOXB13 expression in esophageal squamous cell
carcinoma. Nucleic Acids Res. 45:3086–3101. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Zhang S, Xiao J, Chai Y, Du YY, Liu Z,
Huang K, Zhou X and Zhou W: LncRNA-CCAT1 promotes migration,
invasion, and EMT in intrahepatic cholangiocarcinoma through
suppressing miR-152. Dig Dis Sci. 62:3050–3058. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Li X, Zhou Y and Qian H: CCAT1 expressed
in malignant and pre-malignant human gastric tissues. Cell Mol Biol
(Noisy-le-grand). 63:89–93. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Shang A, Wang W, Gu C, Chen W, Lu W, Sun Z
and Li D: Long non-coding RNA CCAT1 promotes colorectal cancer
progression by regulating miR-181a-5p expression. Aging (Albany
NY). 12:8301–8320. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Guglielmi S, D'Angelo F, Bichard P,
Lepilliez V and Frossard JL: Gastric intestinal metaplasia and
cancer risk: How to follow? Rev Med Suisse. 15:1502–1505. 2019.(In
French). PubMed/NCBI
|
|
43
|
Song Y, Yang H, Lin R, Jiang K and Wang
BM: The role of ferroptosis in digestive system cancer. Oncol Lett.
18:2159–2164. 2019.PubMed/NCBI
|
|
44
|
Song Y, Ye M, Zhou J, Wang Z and Zhu X:
Targeting E-cadherin expression with small molecules for digestive
cancer treatment. Am J Transl Res. 11:3932–3944. 2019.PubMed/NCBI
|
|
45
|
Montalvo-Jave EE, Rahnemai-Azar AA,
Papaconstantinou D, Deloiza ME, Tsilimigras DI, Moris D,
Mendoza-Barrera GE, Weber SM and Pawlik TM: Molecular pathways and
potential biomarkers in gallbladder cancer: A comprehensive review.
Surg Oncol. 31:83–89. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ramnarine VR, Kobelev M, Gibb EA, Nouri M,
Lin D, Wang Y, Buttyan R, Davicioni E, Zoubeidi A and Collins CC:
The evolution of long noncoding RNA acceptance in prostate cancer
initiation, progression, and its clinical utility in disease
management. Eur Urol. 76:546–559. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Zhou DD, Liu XF, Lu CW, Pant OP and Liu
XD: Long non-coding RNA PVT1: Emerging biomarker in digestive
system cancer. Cell Prolif. 50:e123982017. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Guo J, Ma Y, Peng X, Jin H and Liu J:
LncRNA CCAT1 promotes autophagy via regulating ATG7 by sponging
miR-181 in hepatocellular carcinoma. J Cell Biochem.
120:17975–17983. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Abedini P, Fattahi A, Agah S, Talebi A,
Beygi AH, Amini SM, Mirzaei A and Akbari A: Expression analysis of
circulating plasma long noncoding RNAs in colorectal cancer: The
relevance of lncRNAs ATB and CCAT1 as potential clinical hallmarks.
J Cell Physiol. 234:22028–22033. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Yang C, Pan Y and Deng SP: Downregulation
of lncRNA CCAT1 enhances 5-fluorouracil sensitivity in human colon
cancer cells. BMC Mol Cell Biol. 20:92019. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Zhang J, Cai M, Jiang D and Xu L:
Upregulated LncRNA-CCAT1 promotes hepatocellular carcinoma
progression by functioning as miR-30c-2-3p sponge. Cell Biochem
Funct. 37:84–92. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Fang H, Liu HM, Wu WH, Liu H, Pan Y and Li
WJ: Upregulation of long noncoding RNA CCAT1-L promotes
epithelial-mesenchymal transition in gastric adenocarcinoma. Onco
Targets Ther. 11:5647–5655. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Li N, Jiang K, Fang LP, Yao LL and Yu Z:
Knockdown of long noncoding RNA CCAT1 inhibits cell growth,
invasion and peritoneal metastasis via downregulation of Bmi-1 in
gastric cancer. Neoplasma. 65:736–744. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Hu M, Zhang Q, Tian XH, Wang JL, Niu YX
and Li G: lncRNA CCAT1 is a biomarker for the proliferation and
drug resistance of esophageal cancer via the miR-143/PLK1/BUBR1
axis. Mol Carcinog. 58:2207–2217. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Shi D, Wu F, Gao F, Qing X and Shao Z:
Prognostic value of long non-coding RNA CCAT1 expression in
patients with cancer: A meta-analysis. PLoS One. 12:e01793462017.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Cao W, Chen HD, Yu YW, Li N and Chen WQ:
Changing profiles of cancer burden worldwide and in China: A
secondary analysis of the global cancer statistics 2020. Chin Med J
(Engl). 134:783–791. 2021. View Article : Google Scholar : PubMed/NCBI
|