Introduction
Cancer is a global health problem and the second
leading cause of death in developed countries (1). A significant part of that problem is
gastric cancer, being the fifth most common cancer worldwide
(2). Despite numerous improvements
in systemic treatment, patients diagnosed at an advanced stage have
poor prognosis (3), and in such
cases, medical procedures may be more of a palliative nature
(4). For some patients with
metastatic, unresectable, microsatellite instability-high (MSI-H),
or mismatch repair-deficiency solid tumors, the US Food and Drug
Administration (FDA) has approved treatment with immune checkpoint
inhibitors such as pembrolizumab (5).
Primary squamous cell carcinoma of the stomach
(GSCC) is an extremely rare condition, described for the first time
in 1895 (6,7). The first guidelines for GSCC
histopathological diagnosis were published in 1965 (8). The current incidence of GSCC is
described as 0.04 to 0.07% of all gastric carcinomas (9–13).
GSCC is more common in men, with a male-to-female ratio of 5 to 1
(14). GSCC patients are usually
diagnosed in the sixth decade of life (13,15),
in an advanced stage of the disease. The tumor stage is recognized
to be the most important prognostic factor (15). Most commonly, a GSCC tumor is
located in the upper third of the stomach (16). Although the chemotherapeutic options
continue to develop, surgery remains the most effective therapeutic
option (12,13). Even so, the prognosis for GSCC
patients, especially those in advanced stages, is poor (17).
Case report
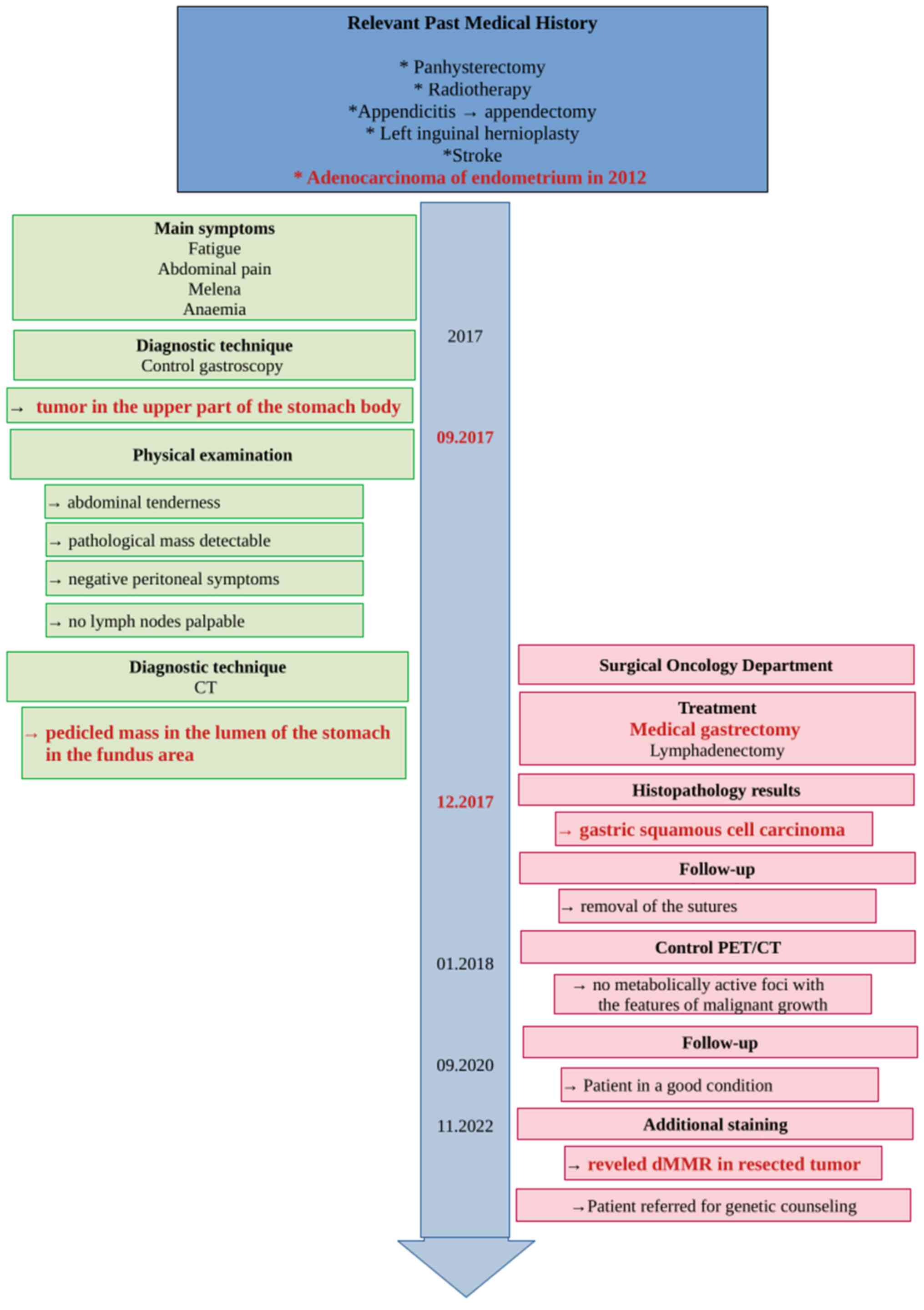
In December 2017, a 79-year-old Polish woman
suffering from fatigue, abdominal pain, melena, and anemia was
admitted to Surgical Oncology Outpatient Clinic (Medical University
of Lodz, Copernicus Memorial Hospital, Lodz, Poland). She denied
chronic diseases and ongoing pharmacological treatment. Her past
medical history included adenocarcinoma of the endometrium (treated
with panhysterectomy and radiotherapy in 2012), appendectomy due to
appendicitis, left inguinal hernioplasty, and stroke. Physical
examination revealed abdominal tenderness without any pathological
mass detectable, with negative peritoneal symptoms and no lymph
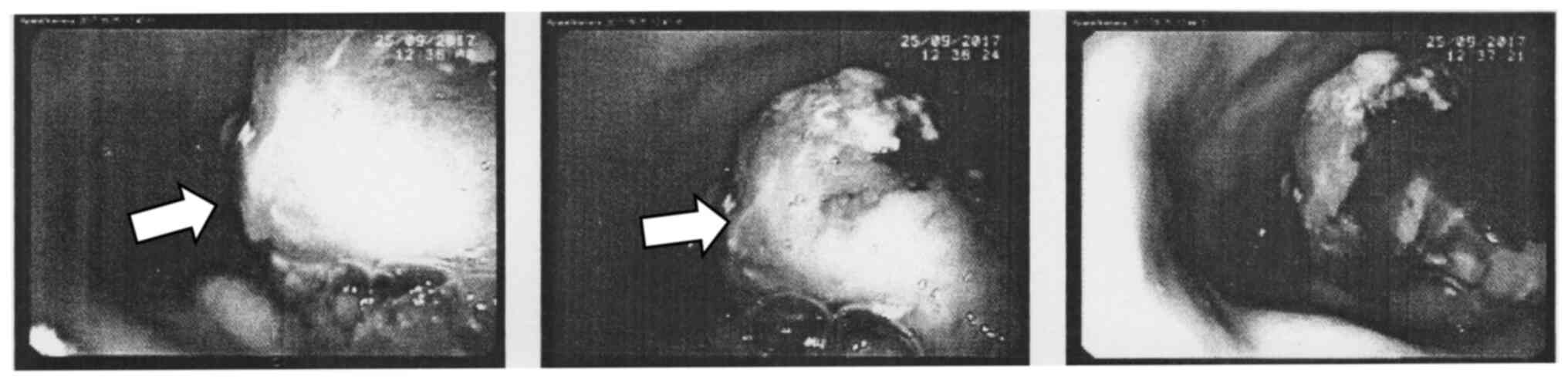
nodes palpable. A diagnostic gastroscopy (Fig. 1) was performed. A large, exophytic,
bleeding tumor was found in the upper part of the stomach body.
Abdominal ultrasonography did not reveal any
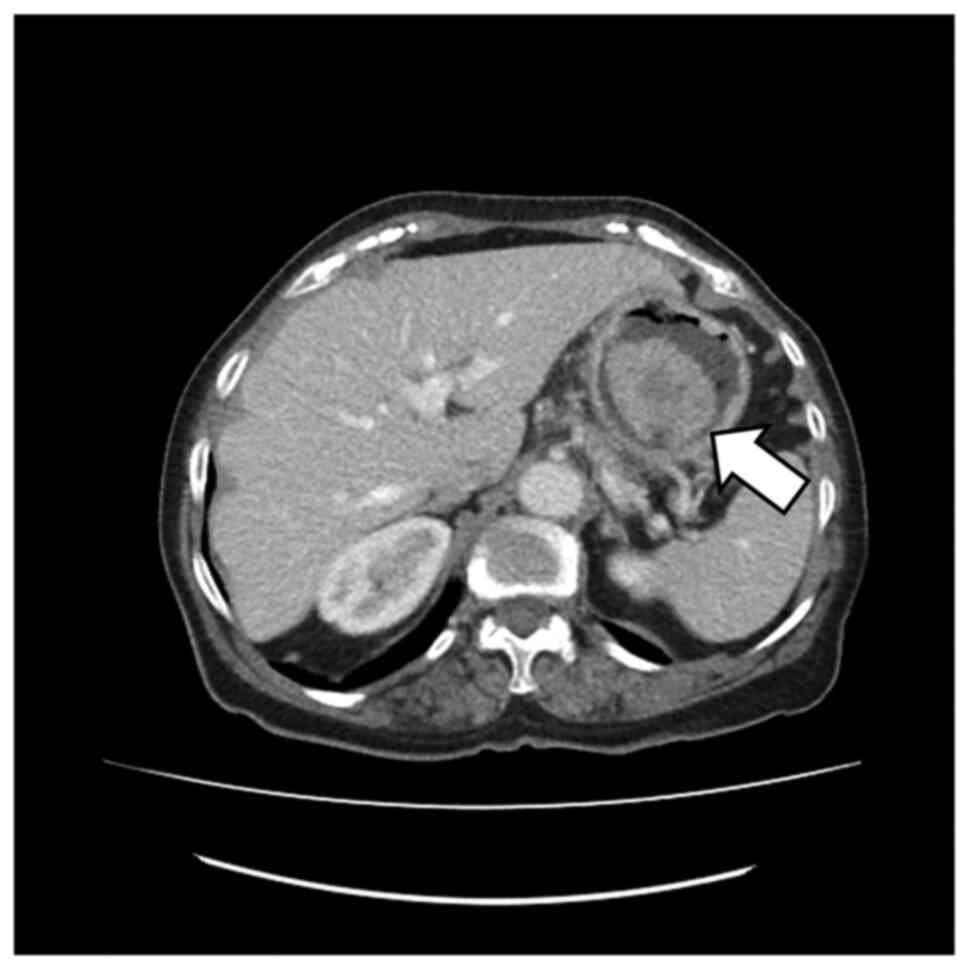
pathology. An abdominal Computer Tomography (CT) (Fig. 2) scan showed a pedicled mass
(49×40×42 mm) in the lumen of the stomach in the fundus area,
without features of surrounding fatty tissue invasion, and no
pathological abdominal lymph nodes. There were no signs of disease
spread in medical imaging.
Taking into consideration the patient's condition
and test results, particularly the signs of active gastrointestinal
bleeding, a strong suspicion of gastric cancer arose. The patient
was informed about the clinical diagnosis and surgical treatment
was proposed. The patient initially declined, but changed her mind
after one month and was immediately admitted to the Surgical
Oncology Department. Radical gastrectomy with Roux-en-Y loop and D2
lymphadenectomy was performed without complications. The patient
was discharged home in good general condition 10 days later,
without any clinically-significant blood morphology deviations.
The tumor specimen used for histopathological
analysis were taken by surgery. The histopathological analysis of
post-operational material (Fig. 3)
revealed a large tumor (5×6×4 cm) with central ulceration and
bleeding signs in the lumen of the stomach, located 10 cm from the
proximal end of the specimen. The tumor had invaded the mucosa,
submucosa and muscle layer. The radial margin was assessed as 0.2
cm. Immunostaining was positive for p63 (Fig. 3F), and negative for CK7 (Fig. 3E), CK19, CK20, and CDX2.
Histochemical staining with AB/PAS was negative (Fig. 3C). Additionally, no vascular
invasion was apparent in the tumor (anti-CD31 staining) (Fig. 3D). This all favored a diagnosis of
squamous cell carcinoma G2. All 32 removed regional lymph nodes
were free from cancer cells.
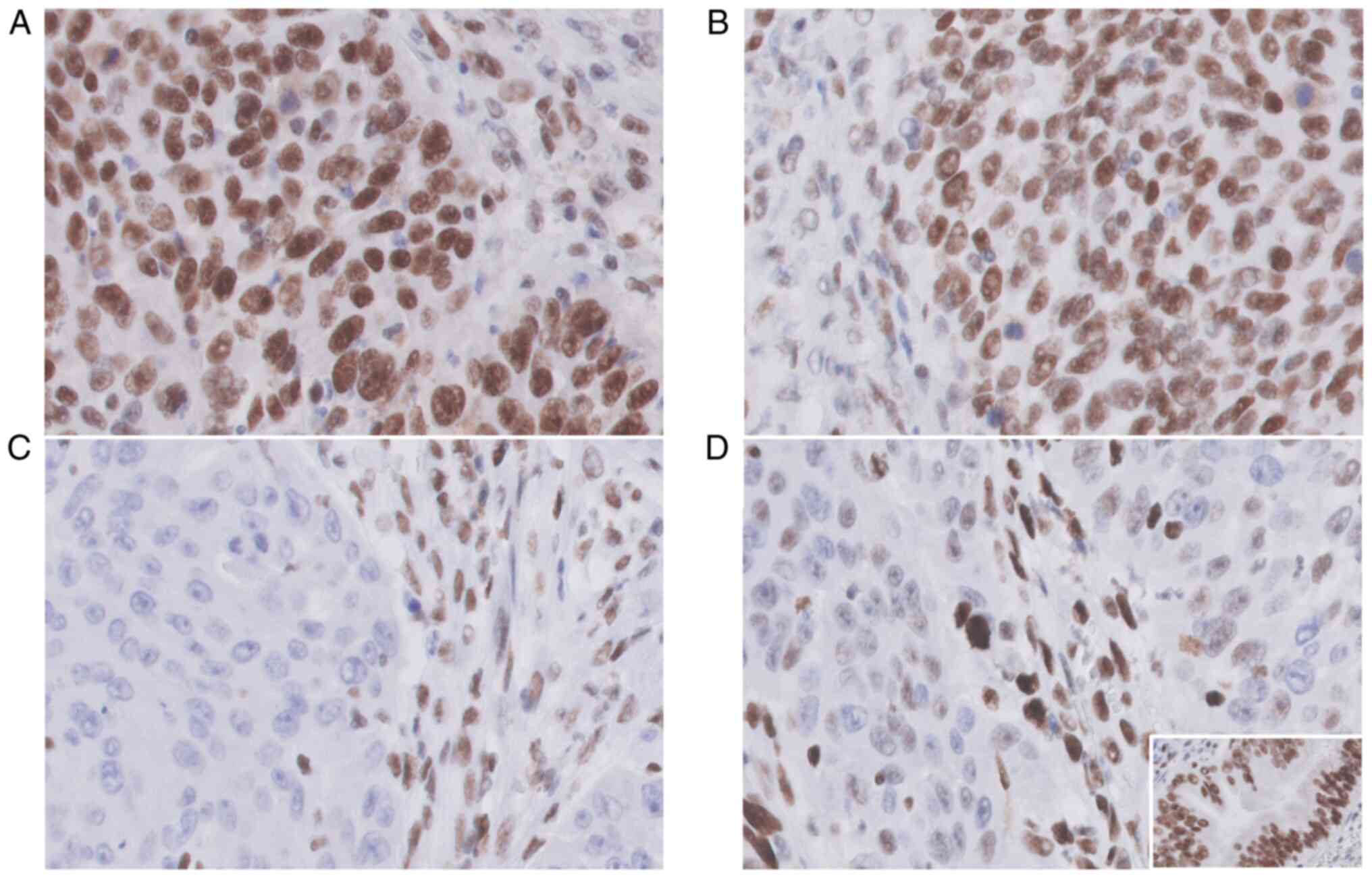
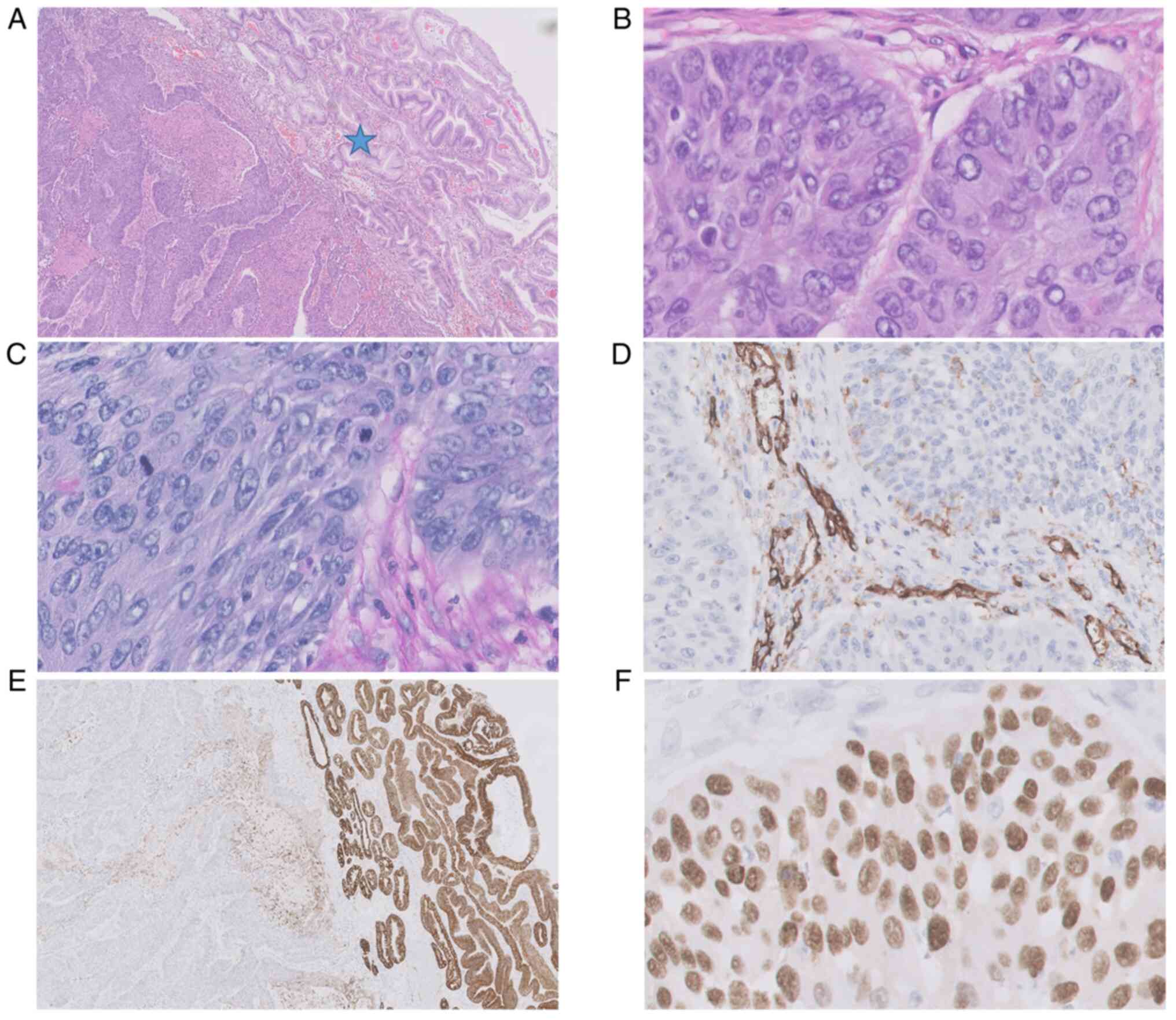 | Figure 3.Histopathological picture of primary
gastric squamous cell carcinoma in the antrum. (A and B) Tumor
cells showed only squamous cell differentiation without any
formation of glands with central necrosis (HE 20×, 400×); (C)
AB/PAS histochemical staining was completely negative in tumor
cells (AB/PAS, 400×); (D) no vascular invasion was seen in the
tumor, CD31 was positive in the endothelial cells of stromal
vessels [IHC reaction with anti-CD31 antibody (DAKO), 400×]; the
pre-existent prepyloric mucosa was intact, (A) with no infiltration
by carcinoma (asterisk) and was (E) positive in anti-CK7 staining
(IHC reaction with anti-CK7 antibody (DAKO), 20×); (F) p63 IHC
positive expression in squamous cell carcinoma (IHC reaction with
anti-p63 antibody (DAKO), 400×). AB/PAS, alcian blue/periodic
acid-Schiff; HE, hematoxylin and eosin; IHC,
immunohistochemical. |
A selected representative block of tumor tissue was
stained immunohistochemically (IHC) with MSH2 (Monoclonal Mouse
Anti-Human antibody, Clone FE11), MSH6 (Monoclonal Rabbit
Anti-Human antibody, Clone EP49), MLH1 (Monoclonal Mouse Anti-Human
antibody, Clone ES05), and PMS2 (Monoclonal Rabbit Anti-Human
antibody, Clone EP51) (Agilent Dako, Glostrup, Denmark) to
characterize DNA-mismatch repair (MMR) protein expression patterns.
Immunohistochemistry (IHC) was performed in tissue sections of
formalin-fixed, paraffin-embedded (FFPE). We used EnVision FLEX+,
Mouse, High pH (Link) (Dako) in Autostainer Link 48 with the HIER
(heat-induced epitope retrieval) method using the panel of
following antibodies: CK-7 (Clone OV-TL 12/30, Mouse monoclonal,
Catalog No. IR619), CK19 (Clone RCK108, Mouse monoclonal, Catalog
No. IR615), CK20 (Clone Ks20.8, Mouse monoclonal, Catalog No.
IR777), CDX2 (Clone DAK-CDX2, Mouse monoclonal, Catalog No. IR080),
CD31 (Clone JC70A, Mouse monoclonal, Catalog No. IR610), p63 (Clone
DAK-P63, Mouse monoclonal, Catalog No. IR662), MLH1 (Clone ES05,
Mouse monoclonal, Catalog No. IR076), PSM2 (Clone EP51, Rabbit
monoclonal, Catalog No. IR087), MSH2 (Clone FE11, Mouse monoclonal,
Catalog No. IR085), MSH6 (Clone EP49, Rabbit monoclonal, Catalog
No. IR086), all provided by DAKO, Agilent. All primary antibodies
were ready-to-use (RTU), and the incubation time was 20 min at room
temperature. To distinguish mucins in tissue sections, we used
Alcian Blue/PAS Stain Kit, Artisan, Ready-to-use (Catalog No.
AR178, DAKO, Agilent), which is intended to identify acidic and
neutral mucins in tissue sections on the Artisan Link Staining
Systems.
A positive external control was performed on normal
gastric tissue (Fig. 4D, inset).
Positive nuclear staining was performed for each MMR protein in
lymphocytes, stroma and endothelial cells as a positive internal
control (Fig. 4A-D) (18).
A lack of nuclear reactivity was considered as loss
of expression (negative in 100% of tumor cells) (MMR-deficient). At
least 1% nuclear staining of each antibody in tumor cells was
considered as retained expression (positive in tumor cells)
(MMR-proficient) (19). As the IHC
indicated MSH2 loss of expression, the tumor was diagnosed as
mismatch-repair deficient.
The existence of metabolically-active malignant-type
lesions was excluded by whole-body PET-CT scan (Fig. 5), and the diagnosis of GSCC was
maintained.
In 2018, a routine CT scan failed to find any sign
of disease recurrence. Interestingly, five years after surgery (in
2022), the patient is in good health condition and remains under
the supervision of the Outpatient Clinic. Due to a past history of
endometrial cancer (in 2012) and diagnosed dMMR in GSCC tissue, the
patient was referred for genetic counseling (Fig. 6).
Discussion
Almost 100 cases of primary gastric squamous cell
carcinoma had been published by the year 2016 (20). The most frequent localization of
GSCC is the proximal 1/3 of the gastric wall (11,17).
Diagnosis of GSCC can be excluded by esophagus invasion and
localization in gastric cardia (21). Pathogenetic differences between GSCC
and gastric adenocarcinoma are still unclear. One metastatic theory
suggests that basal cells in the gastric mucosa can transform into
squamous cells, then into squamous cell carcinoma cells (7). One study proposes that squamous
differentiation may occur in previously-existing adenocarcinoma
(9), while Takita et al
suggest that the Epstein-Barr virus may play a part in this
process: they confirmed the presence of the Epstein-Barr in
surgically removed GSCC (22).
However, there is no information about previous stomach
malignancies or Epstein-Barr infection in records of the
currently-described patient.
Generally, the established risk factors for GSCC
include male sex, with a male-to-female incidence ratio ranging
from 5: 1 (11,15,23) to
2.3: 1 (17), African/Caribbean
ethnicity (17), presence of
squamous cell metaplasia and tobacco use (24,25).
In addition, five-year survival depends on the stage at which the
treatment was started. At stages I and IV, survival rates do not
differ significantly between GSCC and gastric adenocarcinoma (I-80%
vs. 79%, II-67.5% vs. 43.2%, III-39.7% vs. 28.7%, IV-6% vs. 5%);
however, GSCC patients are rarely diagnosed in early stage (stage
I-7.4% vs. 22.8% in gastric adenocarcinoma). Results of the
treatment depend strongly on initial qualification for surgical
treatment (yes-5-year OS 59.2%, no-17.4%) (17). The patient described herein was
diagnosed in stage IB (pT2pN0cM0), which gives her an 80%
possibility of 5-year survival according to Dong et al
(17).
Surprisingly, the pathological report revealed a
deficiency in mismatch repair mechanisms, with negative staining
for MSH2. Given her past medical history of endometrial cancer, the
patient was referred to genetic counseling to revise the hereditary
dMMR background and perform differentiation diagnostics of Lynch
Syndrome type II OMIM#120435 and Muir-Torre Syndrome OMIM#158320. A
literature search using EMBASE, MEDLINE, PubMed and Cochrane
databases with the terms gastric cancer, squamous cell
carcinoma and mismatch repair deficiency did not reveal
any other case of mismatch repair deficient, primary gastric
squamous cell carcinoma ever published.
Although chemotherapy and radiotherapy have
well-established places in the algorithms of gastric adenocarcinoma
treatment (26,27), no indications exist for GSCC, since
the outcome of chemotherapy in these patients is unknown. Data on
GSCC treatment is only available from case reports or series with
the largest cohorts reaching 56 patients. Based on existing
literature, GSCC treatment in Europe is based around cisplatin,
5-fluorouracil, oxaliplatin, capecitabine, docetaxel, gemcitabine
and S1; however, a Japanese publication (11) notes that mitomycin, epirubicin and
bleomycin can also be applied in both systemic and intrahepatic
infusions.
Although the majority of publications describe
chemotherapy in a palliative setting (28), a few radical resections with
adjuvant chemotherapy (29) and
radiation were noted (11,25,30).
Only one patient was reported to undergo neoadjuvant treatment,
which resulted in partial response to 5-FU/cisplatin systemic
treatment (11); nevertheless,
5-FU/cisplatin seems to be chosen most often in the reviewed
publications. Unfortunately, as no randomized clinical trials have
been conducted on GSCC patients, decisions on chemotherapy should
be made individually by the multidisciplinary team. In the present
case, adjuvant chemotherapy was not advised by the medical
oncologist, based on the presence of upper gastrointestinal
bleeding prior to the surgery and the poor performance status of
the patient post gastrectomy (according to Eastern Cooperative
Oncology Group-ECOG 2). The patient's treatment was standard and
included only surgical intervention.
In our case, negative IHC nuclear staining of MSH2
indicates possible microsatellite instability (MSI). Furthermore,
based on recent reports, weak, heterogeneous nuclear expression of
MSH2 protein requires testing for MSI mutations; in our case, the
MSH6 protein showed only focally weak nuclear expression in a few
cells. It should be emphasized that molecular testing is mandatory
in cases with loss/patchy MMR-IHC in daily clinical practice, to
avoid misdiagnosis and consequently inadequate therapeutic choices
(31).
Immune checkpoint inhibitors have been approved by
the FDA and they have demonstrated survival benefits among patients
with MSI-H/dMMR diagnosis (3).
Hence, pembrolizumab appears an attractive potential treatment
option in the case of GSCC relapse or dissemination.
It is important to emphasize the major limitations
of our case report. Firstly, diagnostic MMR analysis was not
initially performed, as the patient did not have metastatic cancer,
which would have required other treatment options and the
aforementioned MMR testing. Upon additional diagnostics, we
detected IHC MSH2 negative nuclear staining, indicating possible
microsatellite instability (MSI). Secondly, the limitation of our
study is also the lack of assessment of the microvessel density
with CD31 expression, which may be a potential prognostic
biomarker. CD31 immunohistochemical staining was performed to
assess tumor angioinvasion.
As a particularly rare malignancy, GSCC presents a
challenging problem in setting a correct diagnosis and in planning
optimal treatment. Nevertheless, despite its generally serious
prognosis and poor treatment outcomes, early diagnosis and
effective treatment are possible. There is a need for further
research in the field of GSCC, especially for developing diagnostic
methods and new systemic treatment options.
The presented case report adds to the limited amount
of data available on GSCC. More importantly, it serves as an
important reminder that despite being a very rare condition, it
should still be a consideration when diagnosing patients with
gastric tumors.
This is the first reported case of dMMR primary
gastric squamous cell cancer. Based on the reviewed literature, the
MSI/MMR status of previously published GSCC cases remains unknown.
Therefore, in the event of a diagnosis of GSCC, we encourage
clinicians to consider MSI/MMR testing. This could directly benefit
the patients by indicating the need for immune checkpoint
inhibition implementation in cases with disseminated disease.
Acknowledgements
The Department of Surgical Oncology is the
scientific, structural part of the Medical University of Lodz,
located in the Copernicus Memorial Hospital in Lodz. The Surgical
Oncology Outpatient Clinic is the medical, structural part of the
Copernicus Memorial Hospital in Lodz.
Funding
Funding: No funding was received.
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
JarJ, AM, JagJ and KLG conceptualized the study;
JarJ, DJK and AM performed an operation or performed
histopathological examination of the patient's cancer tissue; JagJ,
AM, EW and KLG wrote and prepared the original draft; EW reviewed
the literature and treatment methods; JagJ, AM, EW, JarJ, AKS and
KLG analyzed the data; JagJ, AM, EW, JarJ, KLG, DJK and AKS
reviewed and edited the manuscript. JagJ, KLG and JarJ confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of any data and/or accompanying images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2021. CA Cancer J Clin. 71:7–33. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Yu H, Xu L, Yin S, Jiang J, Hong C, He Y
and Zhang C: Risk factors and prognostic impact of postoperative
complications in patients with advanced gastric cancer receiving
neoadjuvant chemotherapy. Curr Oncol. 29:6496–6507. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Rihawi K, Ricci AD, Rizzo A, Brocchi S,
Marasco G, Pastore LV, Llimpe FLR, Golfieri R and Renzulli M:
Tumor-associated macrophages and inflammatory microenvironment in
gastric cancer: Novel translational implications. Int J Mol Sci.
22:38052021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ricci AD, Rizzo A, Rojas Llimpe FL, Di
Fabio F, De Biase D and Rihawi K: Novel HER2-directed treatments in
advanced gastric carcinoma: AnotHER paradigm shift? Cancers
(Basel). 13:16642021. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Ricci AD, Rizzo A and Brandi G: DNA damage
response alterations in gastric cancer: Knocking down a new wall.
Future Oncol. 17:865–868. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Segura S, Pender J, Dodge J, Brandwein SL
and El-Fanek H: Primary squamous cell carcinoma of the stomach: A
case report and review of the literature. Conn Med. 80:209–212.
2016.PubMed/NCBI
|
|
7
|
Altshuler JH and Shaka JA: Squamous cell
carcinoma of the stomach. Review of the literature and report of a
case. Cancer. 19:831–838. 1966. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Boswell JT and Helwig EB: Squamous cell
carcinoma and adenoacanthoma of the stomach. A clinicopathologic
study. Cancer. 18:181–192. 1965. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Straus R, Heschel S and Fortmann DJ:
Primary adenosquamous carcinoma of the stomach. A case report and
review. Cancer. 24:985–995. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Muto M, Hasebe T, Muro K, Boku N, Ohtsu A,
Fujii T, Ono M, Taijiri H, Mukai K and Yoshida S: Primary squamous
cell carcinoma of the stomach: A case report with a review of
Japanese and Western literature. Hepatogastroenterology.
46:3015–3018. 1999.PubMed/NCBI
|
|
11
|
Amuluru K and Gupta H: Primary squamous
cell carcinoma of the stomach: A case report. J Gastrointest
Cancer. 41:24–26. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bonnheim DC, Sarac OK and Fett W: Primary
squamous cell carcinoma of the stomach. Am J Gastroenterol.
80:91–94. 1985.PubMed/NCBI
|
|
13
|
Schmidt C, Schmid A, Lüttges JE, Kremer B
and Henne-Bruns D: Primary squamous cell carcinoma of the stomach.
Report of a case and review of literature. Hepatogastroenterology.
48:1033–1036. 2001.PubMed/NCBI
|
|
14
|
González-Sánchez JA, Vitón R, Collantes E
and Rodríguez-Montes JA: Primary squamous cell carcinoma of the
stomach. Clin Med Insights Oncol. 11:11795549166860762017.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hwang SH, Lee JH, Kim K, Shin DH, Kim JY,
Sol MY and Choi KU: Primary squamous cell carcinoma of the stomach:
A case report. Oncol Lett. 8:2122–2124. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wakabayashi H, Matsutani T, Fujita I,
Kanazawa Y, Nomura T, Hagiwara N, Hosone M, Katayama H and Uchida
E: A rare case of primary squamous cell carcinoma of the stomach
and a review of the 56 cases reported in Japan. J Gastric Cancer.
14:58–62. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Dong C, Jiang M, Tan Y, Kong Y, Yang Z,
Zhong C, Li D and Yuan Y: The clinicopathological features and
prognostic factors of gastric squamous cell carcinoma. Medicine
(Baltimore). 95:e47202016. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kato A, Sato N, Sugawara T, Takahashi K,
Kito M, Makino K, Sato T, Shimizu D, Shirasawa H, Miura H, et al:
Isolated loss of PMS2 immunohistochemical expression is frequently
caused by heterogenous MLH1 promoter hypermethylation in Lynch
syndrome screening for endometrial cancer patients. Am J Surg
Pathol. 40:770–776. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sharma M, Yang Z and Miyamoto H: Loss of
DNA mismatch repair proteins in prostate cancer. Medicine
(Baltimore). 99:e201242020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Callacondo D, Ganoza-Salas A, Anicama-Lima
W, Quispe-Mauricio A and Longacre TA: Primary squamous cell
carcinoma of the stomach with paraneoplastic leukocytosis: A case
report and review of literature. Hum Pathol. 40:1494–1498. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Parks RE: Squamous neoplasms of the
stomach. Am J Roentgenol Radium Ther Nucl Med. 101:447–449. 1967.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Takita J, Kato H, Miyazaki T, Nakajima M,
Fukai Y, Masuda N, Manda R, Fukuchi M and Kuwano H: Primary
squamous cell carcinoma of the stomach: A case report with
immunohistochemical and molecular biologic studies.
Hepatogastroenterology. 52:969–974. 2005.PubMed/NCBI
|
|
23
|
Volpe CM, Hameer HR, Masetti P, Pell M,
Shaposhnikov YD and Doerr RJ: Squamous cell carcinoma of the
stomach. Am Surg. 61:1076–1078. 1995.PubMed/NCBI
|
|
24
|
Chen Y, Zhu H, Xu F, Cao Y, Gu X, Wan Y
and Gou H: Clinicopathological characteristics, treatment, and
prognosis of 21 patients with primary gastric squamous cell
carcinoma. Gastroenterol Res Pract. 2016:3062542016. View Article : Google Scholar
|
|
25
|
von Waagner W, Wang Z and Picon AI: A rare
case of a primary squamous cell carcinoma of the stomach presenting
as a submucosal mas. Case Rep Surg. 2015:4823422015.PubMed/NCBI
|
|
26
|
Karaca M, Tural D, Kocoglu H,
Selcukbiricik F, Bilgetekin I and Özet A: Adjuvant chemotherapy for
gastric cancer in elderly patients has same benefits as in younger
patients. J Cancer Res Ther. 14:593–596. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Yang J, Liu J, Gao S, Yang Y, Kong W, Ren
W, Zhu L, Yang M, Wei J, Zou Z, et al: Use of simultaneous
radiation boost achieves high treatment response rate in patients
with metastatic gastric cancer. J Cancer Res Ther. 14:36–39. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Meng Y, Zhang J, Wang H, Zhang Y, Sun R,
Zhang Z, Gao F, Huang C and Zhang S: Poorer prognosis in patients
with advanced gastric squamous cell carcinoma compared with
adenocarcinoma of the stomach: Case report. Medicine (Baltimore).
96:e92242017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Guzman Rojas P, Parikh J, Vishnubhotla P
and Oharriz JJ: Primary gastric squamous cell carcinoma. Cureus.
10:e23892018.PubMed/NCBI
|
|
30
|
Gülçiçek OB, Solmaz A, Özdoğan K, Erçetin
C, Yavuz E, Yiğitbaş H, Çelebi F and Altınay S: Primary squamous
cell carcinoma of the stomach. Ulus Cerrahi Derg. 32:221–223.
2015.PubMed/NCBI
|
|
31
|
Zito Marino F, Amato M, Ronchi A, Panarese
I, Ferraraccio F, De Vita F, Tirino G, Martinelli E, Troiani T,
Facchini G, et al: Microsatellite status detection in
gastrointestinal cancers: PCR/NGS is mandatory in negative/patchy
MMR immunohistochemistry. Cancers (Basel). 14:22042022. View Article : Google Scholar : PubMed/NCBI
|