Chimeric antigen receptor (CAR) T-cell therapy is a
successful adoptive cell therapy strategy that has significantly
improved the treatment and prognosis of hematological malignancies.
So far, the Food and Drug Administration (FDA) has approved seven
CAR-T cell products to treat hematological malignancies (1–3). CAR-T
cells can have a single chain variable fragment (scFv) on their
surface that recognizes tumor-related surface antigens after
genetic engineering modification and pass through CD3ξ, 4-1BB (a
costimulatory protein, a component of CAR intracellular modules),
CD28 and other intracellular signal domains to initiate an
anti-tumor immune response and release INF-γ, TNF-α, perforin and
granzyme can kill tumor cells (4–7).
Compared with traditional T-cell receptors (TCRs), CARs can
independently recognize tumor antigens and do not rely on
antigen-derived peptides presented by class I molecules of the
major histocompatibility complex (MHC). Moreover, when CARs are
added to T-cells, they can be designed to specifically recognize
and bind to these proteins or gangliosides on the surface of cancer
cells (8). This recognition
triggers the activation of the T-cells and leads to the destruction
of the cancer cells; to date, four generations of CARs have been
created (9). The first-generation
CARs only possess an intracellular signaling domain of CD3ξ to
activate T cells (10). In the
second-generation CARs, the intracellular signaling domain added a
co-stimulatory domain to CD3ξ, usually 4-1BB (CD137) or CD28, to
enhance T cell activation and proliferation (11). CD3ζ is a T-cell-activated switch in
CARs, and the co-stimulatory domain increases the effectiveness and
durability of the CAR (12). The
third-generation CARs have three intracellular signaling domains,
with two co-stimulatory signaling domains [4-1BB (CD137) and CD28]
used in conjunction with the CD3ξ domain. The fourth-generation
CARs are referred to as T cells redirected for universal
cytokine-mediated killing. Here, the addition of cytokine
expression cassettes to the second-generation CARs enables the
secretion of proteins, including interleukin (IL)-2, IL-12, IL-10,
IL-17 and IL-15, and promotes enhanced T cell activation, while
recruiting a patient's immune cells (4,13).
CAR-T cell therapy is an up-and-coming adoptive
immunotherapy technique with remarkable efficacy in the treatment
of hematological tumors. However, despite its potential, several
obstacles still limit its effectiveness in hematological and solid
tumors (14,15). There is a need for continued
research to address these challenges and optimize the use of CAR-T
cell therapy in the treatment of hematological and solid tumors.
This includes developing strategies to overcome antigen escape,
reducing the toxicity associated with CAR-T cell therapy, improving
the penetration of CAR-T cells into solid tumors, and enhancing the
long-term efficacy of CAR-T cell therapy. By addressing these
challenges, CAR-T cell therapy has the potential to become an even
more effective and widely used therapy for cancer treatment.
CAR-T cell therapy is a promising cancer treatment
that genetically modifies a patient's T cells to recognize and
attack cancer cells. While CAR-T cell therapy has been reported to
show great success in treating certain types of cancer, such as
lymphoma, this approach has certain limitations and challenges
(16). Reportedly, the main
limitations of CAR-T cell therapy for hematological malignancies
are antigen escape, CAR-T cell associated toxicities (17). There are also challenges such as
insufficient CAR-T cell infiltration and immunosuppression when it
is used to treat solid tumors (18).
Antigen escape and toxicity are significant
challenges associated with CAR-T cell therapy when used alone or in
combination with radiotherapy (19). One approach to reducing antigen
escape is to develop dual-targeting CAR-T cells that target
multiple antigens on tumor cells, which increase the breadth of the
CAR-T cell response and reduce the likelihood of antigen escape.
CAR-T cell therapy can also target antigens which are essential for
cancer cells, which reduces the risk of antigen escape, and
controlled expression of the target antigen, such as through
inducible promoters or RNA interference, helps to reduce off-target
effects and toxicity (20).
Optimizing toe dose of CAR-T cells also helps to reduce toxicity
and the risk of antigen escape. Previous studies have reported that
lower doses of CAR-T cells were more effective than higher doses,
as higher doses caused more severe toxicity and increased the risk
of off-target effects (21).
Reducing the risk of antigen escape and toxicity associated with
CAR-T cell therapy when used alone or in combination with
radiotherapy is a critical area of research. These strategies can
help improve CAR-T cell therapy's safety and efficacy and reduce
the risk of treatment-related side effects (22).
The key obstacle affecting the effectiveness of
CAR-T cell therapy is antigen escape. During follow-up of a
clinical trial on the treatment of recurrent and/or refractory
acute lymphocytic leukemia with CD19 targeted CAR-T cells, CD19
antigen was reported to be downregulated in tumor cells, which led
to therapy resistance (23,24). Although CAR-T cells targeting a
single antigen have shown good anti-tumor efficacy in the early
stage of hematological malignancies, the recurrence rate is high
due to the tumor cells partially or completely losing the
expression of target antigen in the late stages (15,25).
However, the mechanism of antigen escape is still unclear. It may
be that the CAR induces antigen loss upon the activation of T cells
through phagocytosis of target antigens and promoter DNA
hypermethylation (26–28). During antigen escape, the density of
target antigen on the surface of tumor cells decreases below the
threshold required for CAR-T lymphocyte activity, and tumor cells
develop resistance to CAR-T cell therapy (29). Solid tumors are more prone to
antigen escape and therapy resistance because of their low
expression level of tumor antigens and obvious tumor heterogeneity
(30). It has been previously
suggested that CAR-T cells combined with radiotherapy may cause
epitope diffusion to overcome immune escape (31).
The main toxic reactions to CAR-T cell therapy are
on target/on tumor toxicity and on target/off-tumor toxicity.
Cytokine release syndrome (CRS) is one of the side effects of CAR-T
cell therapy with high incidence and lethality (32). CRS is characterized by the release
of a great quantity of inflammatory cytokines, which are closely
related to CAR-T cells and bystander cells (such as
monocytes/macrophages) that have recognized the antigens on target
tumor cells. The occurrence and severity of CRS depend on the tumor
load, CAR structure, CAR-T cell number and other factors (33,34).
Controlled CRS can improve the remission rate and progression free
survival (PFS) of cancer patients and improve the effectiveness of
CAR-T cell treatment. In addition, the severity of CRS is reported
to be positively correlated with the tumor load of patients
(35). Bridging therapy can reduce
the tumor burden before CAR-T cells are used to reduce the
occurrence of lethal CRS (36). CRS
is mainly mediated by the cytokine IL-6 (37,38).
The use of tocilizumab, an IL-6 receptor antagonist, blocks IL-6
and relieves the clinical symptoms of CRS. In addition, the use of
IL-1 receptor antagonists, such as anakinra and
granulocyte-macrophage colony-stimulating factor, have been
reported to alleviate the symptoms of CRS (39). Differently to hematological tumors,
target antigens in patients with solid tumors are often delivered
to different levels by normal tissues (40). Targeting of antigens expressed on
normal cells by CAR-T cells causes harm to normal tissues and
organs. Therefore, the specificity of CAR-T cells for the target
antigen is the key to reduce its toxicity (41). The on-target/off-tumor toxicity can
also be reduced by adjusting the affinity of the scFv (42).
The number of CAR-T cells transported to solid tumor
tissue determines whether the treatment of CAR-T cells is
successful. Firstly, local tissue hypoxia develops in solid tumors
on account of the hyperproliferation of tumor cells, abnormal
vascularization and insufficient blood supply in the expanded tumor
tissue (43). The conveyance and
activation of CAR-T cells depend on tumor blood vessels; therefore,
CAR-T cells have difficulty in reaching tumor tissues far away from
blood vessels, which results in therapy resistance (44). At the same time, in the hypoxic
tumor microenvironment (TME), tumor cells produce cytokines, which
are recruited to immunosuppressive cells to deplete CAR-T cells
(45). Hypoxia promotes the
expression of HIF-1α, which activates the secretion of
pro-angiogenic factors such as VEGF-A. VEGF-A inhibits the release
of inter-endothelial cell adhesion molecule (ICAM)-1 and vascular
cell adhesion protein (VCAM)-1, and inhibits the migration of CAR-T
cells across the vascular endothelial cell barrier into the tumor
tissue (46,47).
After CAR-T cells surmount obstacles and
successfully arrive at the tumor tissue, suppressive immune cell
subsets in the TME can deplete and render the CAR-T cells
dysfunctional. Suppressive immune cell subsets are mainly recruited
by cytokines secreted by tumor cells (48). Regulatory T cells (Tregs), an
important subgroup of suppressive immune cells, are recruited to
tumor tissue by the chemokines CXCL12 or SDF1α, which inhibit the
activity of effector T cells and CAR-T cells (49). Myeloid-derived suppressor cells
(MDSCs) and tumor-associated macrophages (TAMs) have been reported
to be immunosuppressive subsets that affect CAR-T cell function
(50). MDSCs produce and secrete
cytokines and metabolic factors, such as IL-10, IL-1 receptor
antagonist, TGF-β and nitric oxide, which hinder the anti-tumor
immune response. MDSCs also express immune checkpoint molecules
that promote T cell and CAR-T cell exhaustion (51,52).
TAMs can be taken up by tumor cells and polarized
into an anti-inflammatory M2-subtype by secreting TGF-β,
prostaglandin E2, IL-10, indoleamine 2,3-dioxygenase IDO, and
chemokines such as CCL17, CCL18 and CCL22, which lead to the
inhibition of T cell responses and infiltration of Tregs (53–55).
To overcome the factors which hinder the application of CAR-T cell
therapy in solid tumors, a combination therapy strategy has been
proposed, in which CAR-T cells are administered alongside
radiotherapy.
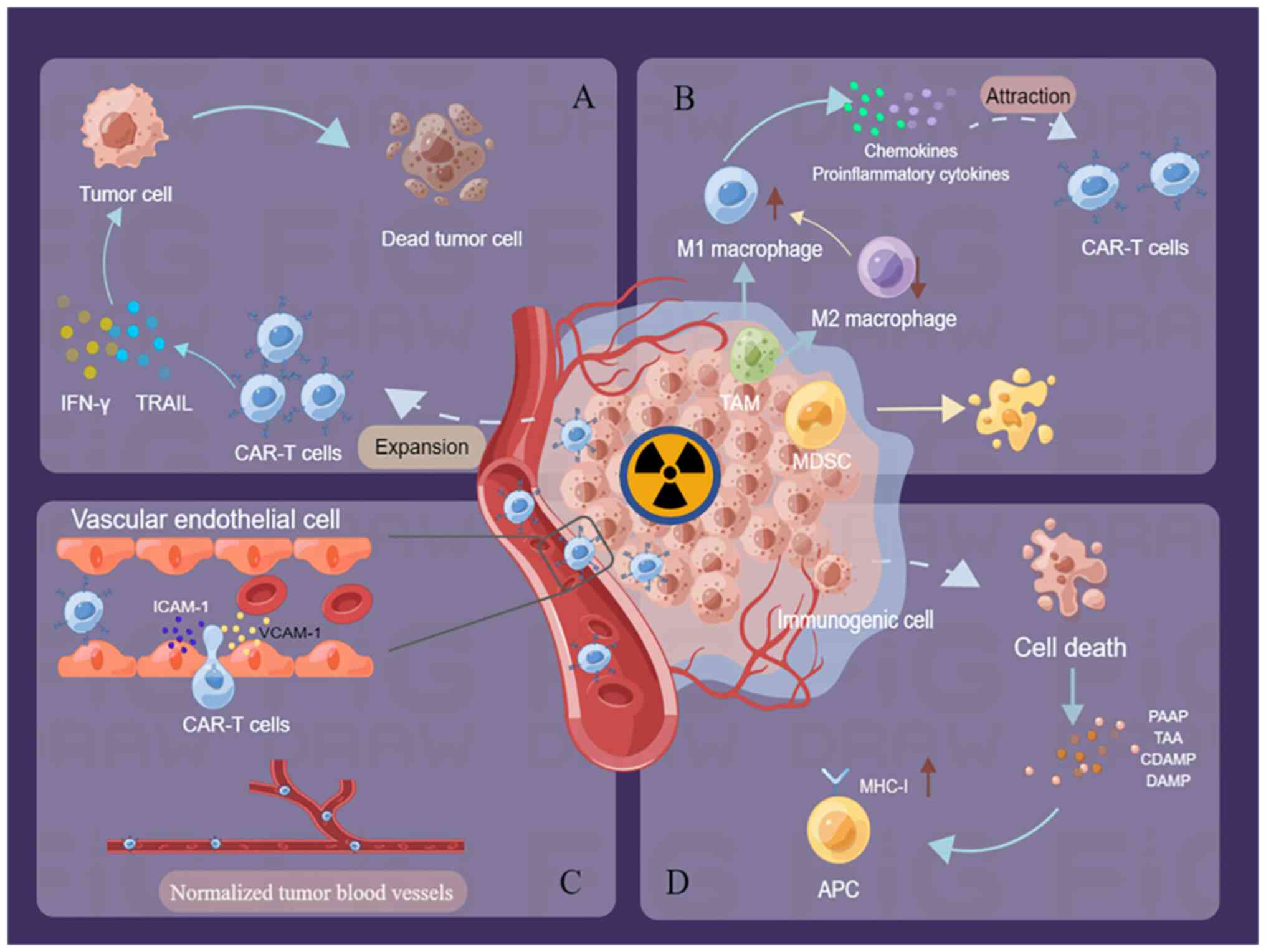
Radiotherapy (RT) is a traditional first-line
anti-tumor therapy. In addition to directly killing the tumor
cells, radiotherapy also activates immune responses in the TME
(56) (Fig. 1D). Dying immunogenic cells secrete
radiation-associated antigen proteins, tumor-associated antigens,
and cell death-associated molecular patterns that increase target
antigen expression, which leads to the activation of immune
surveillance (6,57). Radiotherapy also increases the
number of MHC molecules on antigen-presenting cells (APCs), which
leads to the translocation of calreticulin (CRT), which releases
high mobility group box 1 protein as well as ATP and heat shock
protein, which activated dendritic cells, APCs, etc., and enhanced
endogenous target antigen-specific immunity (13,58).
In addition, radiation converts immunosuppressive
cells in the TME into immune-promoting cells, which strengthens the
anti-tumor behavior of CAR-T cells (59) (Fig.
1B). Radiotherapy increases the number of M1-like macrophages
and decreases M2-like macrophages and MDSCs in the TME (6). Although radiotherapy offers strong
advantages in tumor treatment, it also promotes radio resistance in
tumor cells, which results in the failure of local cancer treatment
(60). However, radioresistant
tumor cells are sensitive to T-cell retargeting, therefore,
combining radiation with CAR-T cell immunotherapy can achieve the
greatest efficacy. According to previous reports, radiotherapy
boosts the efficacy of CAR-T cells through multiple mechanisms
(61,62).
In the TME, radiotherapy triggers M1-type
macrophages to secrete more chemokines, such as CXCR3, CXCL9-11 or
CXCL16, in response to IFN-γ, which promotes CAR-T cell recruitment
(63). Irradiation also induces an
increase in the production of the integrins ICAM-1 and VCAM-1 in
vascular endothelial cells, which facilitates the movement of CAR-T
cells across the vascular endothelium into the tumor tissue
(64,65) (Fig.
1C). In addition, radiotherapy normalizes tumor blood vessels
and improves tumor reoxygenation, which improves hypoxia-induced
therapy resistance (60).
Radiotherapy also promotes the local expansion of CAR-T cells in
tumors (Fig. 1A). In conclusion,
radiotherapy may improve the effectiveness of CAR-T cell therapy by
activating and enhancing endogenous target antigen-specific immune
responses, which promotes CAR-T cell recruitment and expansion, and
modulates the inflammatory TME (66,67).
Although there is ample evidence that the
combination of radiotherapy and CAR-T cell therapy exerts
synergistic antitumor effects, radiation therapy can cause
immunosuppression and CAR-T cell death, which reduces the efficacy
of the combination therapy. Radiotherapy induces the transformation
of immune cells to immunosuppressive cells, such as Tregs, and
enhances the effect of immunosuppressive molecules, such as IL-10,
TGF-β and adenosine in the TME (68–70).
Tregs are key cells that promote immunosuppression in the tumor
immune microenvironment. Radiotherapy causes increased Tregs
infiltration in irradiated tumor areas, and Tregs show increased
Akt expression, which makes them more radioresistant than other T
cell subsets (71). A preclinical
study reported that targeted depletion of Tregs after radiotherapy
promoted long-lasting antitumor effects (72). Notably, it has been reported that
the infiltration efficiency of Tregs depends on the dose at each
administration rather than the total dose and that this is
positively correlated with each radiation dose (73). Therefore, when combining
radiotherapy with CAR-T cell therapy, the optimal fractionation and
radiation dose should be evaluated to maximize the efficacy and
minimize the toxic side effects (74).
In addition, radiotherapy also directly damages
CAR-T cells. Although there are few reports on the direct damaging
effects of radiotherapy on CAR-T cells, high-dose radiotherapy
administration immediately after the infusion of CAR T cells needs
to be carefully evaluated for its effects on the health of the
CAR-T cells (75). Notably, in a
clinical study, it was shown that administration of 2 Gy of
radiotherapy per dose induced in vivo expansion of CAR-T
cells (76).
Radiotherapy is a double-edged sword, with
differences in dose and fractionation times resulting in different
immunomodulatory responses. On the one hand, it synergistically
promotes anti-tumor effects when used in combination with CAR-T
cell treatment (77). On the other
hand, radiotherapy promotes an immunosuppressive microenvironment
and reduces the anti-tumor effects of CAR-T cells (78). Therefore, the timing, total
radiation dose and the number of fractions of radiation therapy
during CAR-T cell treatment are critical for the success of the
combination therapy (67). When
CAR-T-cell therapy is used in union with radiotherapy, the standard
total radiation dose and fractionations need to be optimized
(56,79). Few previous studies have explored
this, but the conclusions of studies on other immunotherapies such
as immune checkpoint blockage and their combination with
radiotherapy can be used for reference. Existing research indicates
that the dose-fraction regimen of 8 Gy ×3 is the best standard
fractionation regimen for immunotherapy combinations (80,81).
However, certain studies have suggested that low-dose radiotherapy
(<2-4 Gy) may be a better complement to CAR-T cell treatment
based on the radioimmunological effects (82).
Substantial evidence suggests that hypo-fractionated
RT (>2 Gy/fraction) or standard fractionated RT (1.8-2
Gy/fraction) enhances the ability of radiation to promote
anti-tumor immune response by the mechanisms described above
(18,83). Hypo-fractionated irradiation has
been reported to be the best radiotherapy method for extending the
benefits of immunotherapy (84).
CAR-T cell treatment combined with photon radiation is the type of
combination therapy that has reported to demonstrate the best
anti-tumor effects and minimal side effects (85). However, other types of radiation
therapy such as iodine 125 seed brachytherapy combined with Robo1
(a member of the axon guidance receptor family that has also been
reported to play a role in modulating chemotaxis of T cells and
tumor angiogenesis) dimeric antigen receptor-natural killer cells
has also been reported to suppress human pancreatic tumor growth in
mice (39,86). Minimizing immunosuppression and
CAR-T cell death due to radiotherapy and optimizing the dose and
fractionation of radiotherapy when combined with CAR-T cell therapy
are essential considerations for enhancing treatment efficacy and
reducing toxicity (87). These
strategies are still being studied, and more research is needed to
fully understand the optimal parameters for combining radiotherapy
and CAR-T cell therapy (88).
The implementation and feasibility of combined
radiotherapy and CAR-T cell therapy is an area of active research
and clinical investigation. The combination of these two therapies
has the potential to enhance treatment efficacy; however, certain
challenges and considerations need to be addressed (89). One potential benefit of combining
radiotherapy and CAR-T cell therapy is that radiotherapy can help
to create a more favorable TME for CAR-T cells to function.
Radiation can cause DNA damage in cancer cells, which leads to the
release of tumor-associated antigens and the activation of immune
cells (90). One concern is that
radiation can cause damage to CAR-T cells, which may compromise
their function and reduce treatment efficacy. Several clinical
trials to investigate the feasibility and efficacy of combining
radiotherapy and CAR-T cell therapy to treat various types of
cancer are understood to be currently underway (60,91,92).
These studies are reported to be evaluating dosing schedules,
radiation techniques and CAR-T cell products. The combination of
radiotherapy and CAR-T cell therapy has the potential to be a
powerful treatment option for certain types of cancer such as
prostate cancer, pancreatic cancer and glioblastoma (93). The below section enumerates and
summarizes the existing preclinical and clinical studies which have
reported on the combination of CAR-T cell therapy and radiotherapy,
to understand its safety and efficacy and to assess the optimal
timing, total radiation dose and the number of fractionations of
radiotherapy, and CAR-T cell infusion.
In a preclinical study of glioma, GL-261 cells were
intravenously injected with NKG2D CAR T cells 5, 7 days and 10 days
after implantation of the GL-261 cells into the brains of mice, and
local skull radiotherapy was performed on the 7th day after tumor
cell implantation, with a single dose of 4 Gy (31). The NKG2D system serves an
indispensable role in cancer immune surveillance, and NKG2D-ligand
is delivered on the surface of glioblastoma cells and radiotherapy
is known to induce its expression (31,94).
After systemic administration, chNKG2D CAR-T cells moved to the
brain tumor site through the blood brain barrier, and no adverse
events were reported (95). The
results indicated that local tumor irradiation promoted the
movement of CAR-T lymphocytes to the tumor site and increased the
expression of IFN-γ in a NKG2D-based chimeric antigen receptor
construct (chNKG2D) in CAR-T cells. Moreover, the survival of tumor
bearing mice was prolonged and certain of the treated mice
demonstrated complete tumor regression (31).
A preclinical study in glioblastoma compared the
anti-tumor effects of GD2 CAR-T cells combined with a sub-lethal 5
Gy WBI or localized 5 Gy radiotherapy (96). In vitro, the combination
treatment induced substantial cytotoxic effects on
GD2-overexpressing mouse GBM cell lines. In the in vivo
experiments, a single intravenous infusion of GD2 CAR-T cells
within 1–3 h of 5 Gy WBI, significantly improved the anti-tumor
response and survival of tumor bearing mice compared with the other
groups (97). Ten weeks after the
first treatment, the same GD2+ tumor cells were inoculated in the
contralateral tumor hemisphere of mice, and only the group which
received the combination of WBI and GD2 CAR-T cell therapy showed
tumor regression, which indicated antigen-specific T cell memory.
However, treatment with GD2 CAR-T cells 4 days after WBI indicated
no anti-tumor therapeutic effects. Therefore, the timing of
radiotherapy and CAR-T cell injection may be critical. The
combination of localized 5 Gy RT and GD2 CAR-T cells indicated
significant complete anti-tumor responses only in mice that
received the combined treatment compared with the single-arm
control group (98).
Imaging with intravital microscopy indicated that
WBI enabled rapid extravasation of GD2 CAR-T-cells from the
vasculature, which promoted their local expansion and durable
immune responses in the TME. In the two aforementioned preclinical
studies on GD2 CAR-T cells joined with large fraction radiotherapy
for glioma bearing mice, local treatment joined with CAR-T cells
was confirmed to promote tumor regression, and no serious toxic
effects were observed. However, when combining systemic
radiotherapy and CAR-T cells, the anti-tumor effects and treatment
timing were crucial owing to the impact of the timeliness of
radiotherapy in promoting local infiltration and migration of CAR-T
cells (99).
In a study with sLeA-expressing pancreatic cancer
tumor-bearing mice, a strategy which combined sLeA-targeted CAR-T
cells with 2 Gy single low-dose radiotherapy was used. The study
reported that local radiation sensitized tumor cells to activated
CAR-T cells, and that combination therapy upregulated the
sensitivity of sLeA- and sLeA+ tumor cells to TRAIL-mediated cell
death (80). Pancreatic cancer is
considered as a cold tumor, having the characteristics of low
mutation load and low response to T cell infiltration, which
indicate its low response to immunotherapy. The combination of
low-dose radiotherapy with CAR-T cells increased the sensitivity of
pancreatic cancer cells to the immune response. The potential
mechanism may involve the activation of the innate and adaptive
immunity (mainly CD4+effector T cells), which enable NKG2D
dependent tumor growth control and reprogramming of the
immunosuppressive tumor immune microenvironment (100). However, evidence for the
immunogenicity of 1.8-2 Gy conventional radiotherapy in the TME is
insufficient. The complex TME of solid tumors is a serious obstacle
to CAR-T cell treatment, which necessitates its combination with
other anti-tumor therapies to achieve improved therapeutic efficacy
(91). Although the combination
therapy with radiotherapy and CAR-T cells has been evaluated in
animal tumor models, none of the CAR-T cell products have been
approved for treating for solid tumors in the clinic.
To achieve improved anti-tumor effects between the
time when autologous T cells were collected and final CD19
CAR-T-cell therapy was administered to treat patients with DLBCL,
the use of bridging radiotherapy was proposed (101). Relapsed/refractory (R/R) DLBCL
patients accepted bridging radiation treatment prior to the
administration of Axicabtagene ciloleucel, and all patients
received 2–4 Gy per session, with a median dose of 20 Gy (range,
6.0-36.5 Gy). A subset of patients received concurrent chemotherapy
(fludarabine/cyclophosphamide). The results of the study indicated
that patients did not experience disease progression prior to CAR-T
cells treatment. Therefore, these results indicated that bridging
radiation treatment provided adequate local disease control prior
to CAR-T cell injection. In addition, no obvious toxicity was
observed during the bridging treatment and 27% of the patients
developed CRS after the infusion of Axicabtagene ciloleucel
(61).
In a study which evaluated the targeting of CAR-T
cells by autologous BCMA, it was reported that radiotherapy
combined with CAR-T cells, unexpectedly, exerted synergistic
anti-tumor effects through an abscopal-like response (102). In this clinical trial, a patient
with multiple relapsed refractory myeloma received BCMA CAR-T cell
therapy. Shortly after the treatment, emergency high-dose steroids
and palliative radiotherapy (total dose, 20 Gy, 5 times, per site)
were given to the affected thoracic vertebrae and whole brain due
to spinal cord compression. The authors reported that after the use
of a high dose of steroids, there was no decline in the therapeutic
efficacy of CAR-T cells. Moreover, compared with other patients
with multiple relapsed refractory myeloma who only received BCMA
CAR-T cells, this patient presented with a specific delayed CRS.
The time of onset for CRS-like clinical symptoms and inflammatory
markers was consistent with the expansion of new TCR clones after
radiotherapy (103). Therefore,
this combination treatment showed synergistic effects, which lead
to an abscopal-like response.
In a phase II clinical trial which evaluated the
safety and efficacy of CAR-T cells, the investigators enrolled ten
patients with R/R DLBCL, who had high tumor burden and received
bridging radiotherapy (2 Gy ×20) and bridging chemotherapy
(104). CAR-T cells have three
types of targets, namely, CD19, CD20 and CD22. Dual-targeted CAR-T
cells are selected according to the two antigens with higher
expression at relapse. Patients who underwent radiotherapy showed a
higher overall response rate and the toxicity was lower than in
patients who underwent chemotherapy (89). This suggested that radiation
treatment was an effective and safe treatment for tumor reduction
prior to CAR-T cell therapy. These findings indicated that bridging
radiotherapy was an effective and safe option prior to CAR-T cell
therapy. In addition, in patients with R/R DLBCL and a high tumor
burden, radiotherapy prior to CAR-T cell treatment may reduce the
severity of CRS and neurotoxicity associated with the
treatment.
In a retrospective analysis of CD19 CAR-T cells, the
leading cause of treatment failure after CAR-T cell infusion in
patients with non-Hodgkin lymphoma was reported to be the
progression of the primary tumor site. Patients who accepted CAR-T
cell infusion after bridging radiotherapy had higher rates of local
tumor control and durable responses. Thus, higher doses of bridging
radiotherapy may be beneficial in patients with a high risk of
recurrence (105). In a clinical
study on radiotherapy and CAR-T cells, radiotherapy, as a bridge
treatment, was reported to reduce the tumor load, improve the
curative effect of CAR-T cell therapy, and reduce the occurrence of
CAR-T cell related serious toxic reactions (106) (Table
I). Fortunately, abscopal effects were also observed, which
together with CAR-T cells could have promoted the anti-tumor immune
effects. The combination of bridging radiation treatment and CAR-T
cell treatment was a clinically relevant treatment strategy, but
there were few relevant clinical studies exploring this at present
(96). Further clinical studies
which evaluated the efficacy of the above combination treatment
strategy are required to validate its safety and therapeutic
efficacy in the clinic (107).
CAR-T cell therapy is a revolutionary and promising
immunotherapy technology. Mature CAR-T cell products have been
approved for treating hematological tumors and have demonstrated
promising results in the clinic. However, its application in
hematological and solid tumors faces many unexpected difficulties
and reduces the therapeutic effect. As a conventional anti-tumor
therapy, radiotherapy can overcome certain obstacles by enhancing
the specific immunity against endogenous tumor antigens, which
promotes the amplification and expansion of CAR-T cells and
improves the hypoxic TME (108).
However, radiotherapy has advantages and disadvantages, and
differences in dose and the number of divisions generates different
immune regulatory responses. Therefore, the timing of radiotherapy,
the total radiation dose and the number of fractionations, and the
type of radiation are critical parameters that influence the
success of the combination therapy (107).
In preclinical and clinical studies on the
combination of CAR-T cells and radiotherapy, radiotherapy has been
reported to promote the rapid exosmosis and migration of CAR-T
cells from the vascular system into the tumor site, activate
anti-tumor immunity, reduce tumor load, improve the therapeutic
effect and reduce the occurrence of CAR-T cell related severe toxic
reactions. Although the antitumor effects of this combined
treatment strategy are definite, there is still a long way to go
before a standard treatment plan is put forward, and more research
is needed to fully understand the optimal parameters for combining
therapies to address the associated challenges for clinical
translation.
Not applicable.
Funding: No funding was received.
Not applicable.
LZ was responsible for conceptualization and the
writing of the original draft. YL wrote and revised the manuscript.
TAM was responsible for visualization, generation of the figures,
and was involved in drafting and revising the intellectual content
of the manuscript. YW was responsible for revising the manuscript,
and for project administration and supervision. Data authentication
is not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Xiao X, Wang Y, Zou Z, Yang Y, Wang X, Xin
X, Tu S and Li Y: Combination strategies to optimize the efficacy
of chimeric antigen receptor T cell therapy in haematological
malignancies. Front Immunol. 13:9542352022. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen W, Yuan Y and Jiang X: Antibody and
antibody fragments for cancer immunotherapy. J Control Release.
328:395–406. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Long AH, Haso WM, Shern JF, Wanhainen KM,
Murgai M, Ingaramo M, Smith JP, Walker AJ, Kohler ME, Venkateshwara
VR, et al: 4-1BB costimulation ameliorates T cell exhaustion
induced by tonic signaling of chimeric antigen receptors. Nat Med.
21:581–590. 2015. View
Article : Google Scholar : PubMed/NCBI
|
|
4
|
Breuning J, Philip B and Brown MH:
Addition of the C-terminus of CD6 to a chimeric antigen receptor
enhances cytotoxicity and does not compromise expression.
Immunology. 156:130–135. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Haddadi MH, Hajizadeh-Saffar E,
Khosravi-Maharlooei M, Basiri M, Negahdari B and Baharvand H:
Autoimmunity as a target for chimeric immune receptor therapy: A
new vision to therapeutic potential. Blood Rev. 41:1006452020.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Jarosz-Biej M, Smolarczyk R, Cichoń T and
Kułach N: Tumor Microenvironment as A ‘Game Changer’ in cancer
radiotherapy. Int J Mol Sci. 20:32122019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Mansouri V, Yazdanpanah N and Rezaei N:
The immunologic aspects of cytokine release syndrome and graft
versus host disease following CAR T cell therapy. Int Rev Immunol.
41:649–668. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bashiri Dezfouli A, Yazdi M, Pockley AG,
Khosravi M, Kobold S, Wagner E and Multhoff G: NK cells armed with
chimeric antigen receptors (CAR): Roadblocks to successful
development. Cells. 10:33902021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Füchsl F and Krackhardt AM: Paving the way
to solid tumors: Challenges and strategies for adoptively
transferred transgenic T cells in the tumor microenvironment.
Cancers (Basel). 14:41922022. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Brandjes BD and Davila ML: Adding chimeric
antigen receptor-induced killer cells to the medical oncology
shelf. J Clin Invest. 129:5077–5078. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Fujiwara K, Kitaura M, Tsunei A, Kusabuka
H, Ogaki E and Okada N: Structure of the signal transduction domain
in second-generation CAR regulates the input efficiency of CAR
signals. Int J Mol Sci. 22:24762021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Krug C, Birkholz K, Paulus A, Schwenkert
M, Schmidt P, Hoffmann N, Fey G, Abken H, Schuler G,
Schuler-Thurner B, et al: Stability and activity of MCSP-specific
chimeric antigen receptors (CARs) depend on the scFv
antigen-binding domain and the protein backbone. Cancer Immunol
Immunother. 64:1623–1635. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Yadollahvandmiandoab R, Jalalizadeh M,
Buosi K, Garcia-Perdomo HA and Reis LO: Immunogenic cell death role
in urothelial cancer therapy. Curr Oncol. 29:6700–6713. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sterner RC and Sterner RM: CAR-T cell
therapy: Current limitations and potential strategies. Blood Cancer
J. 11:692021. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wang L: Clinical determinants of relapse
following CAR-T therapy for hematologic malignancies: Coupling
active strategies to overcome therapeutic limitations. Curr Res
Transl Med. 70:1033202022. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Haslauer T, Greil R, Zaborsky N and
Geisberger R: CAR T-cell therapy in hematological malignancies. Int
J Mol Sci. 22:89962021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhang X, Zhu L, Zhang H, Chen S and Xiao
Y: CAR-T cell therapy in hematological malignancies: Current
opportunities and challenges. Front Immunol. 13:9271532022.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Qin VM, Haynes NM, D'Souza C, Neeson PJ
and Zhu JJ: CAR-T plus radiotherapy: A promising combination for
immunosuppressive tumors. Front Immunol. 12:8138322021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kulczycka M, Derlatka K, Tasior J, Lejman
M and Zawitkowska J: CAR T-Cell therapy in children with solid
tumors. J Clin Med. 2:23262023. View Article : Google Scholar
|
|
20
|
Qu J, Mei Q, Chen L and Zhou J: Chimeric
antigen receptor (CAR)-T-cell therapy in non-small-cell lung cancer
(NSCLC): Current status and future perspectives. Cancer Immunol
Immunother. 70:619–631. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Sun Y, Li F, Sonnemann H, Jackson KR,
Talukder AH, Katailiha AS and Lizee G: Evolution of CD8+
T cell receptor (TCR) engineered therapies for the treatment of
cancer. Cells. 10:23792021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Gu R, Liu F, Zou D, Xu Y, Lu Y, Liu B, Liu
W, Chen X, Liu K, Guo Y, et al: Efficacy and safety of CD19 CAR T
constructed with a new anti-CD19 chimeric antigen receptor in
relapsed or refractory acute lymphoblastic leukemia. J Hematol
Oncol. 13:1222020. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Aldoss I and Forman SJ: How I treat adults
with advanced acute lymphoblastic leukemia eligible for
CD19-targeted immunotherapy. Blood. 135:804–813. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chen YH, Zhang X, Cheng YF, Chen H, Mo XD,
Yan CH, Chen Y, Han W, Sun YQ, Wang Y, et al: Long-term follow-up
of CD19 chimeric antigen receptor T-cell therapy for
relapsed/refractory acute lymphoblastic leukemia after allogeneic
hematopoietic stem cell transplantation. Cytotherapy. 22:755–761.
2020. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Xie D, Jin X, Sun R, Zhang M, Wang J,
Xiong X, Zhang X and Zhao M: Relapse mechanism and treatment
strategy after chimeric antigen receptor T-cell therapy in treating
B-cell hematological malignancies. Technol Cancer Res Treat.
21:153303382211184132022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hamieh M, Dobrin A, Cabriolu A, van der
Stegen SJC, Giavridis T, Mansilla-Soto J, Eyquem J, Zhao Z,
Whitlock BM, Miele MM, et al: CAR T cell trogocytosis and
cooperative killing regulate tumour antigen escape. Nature.
568:112–116. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ledererova A, Dostalova L, Kozlova V,
Peschelova H, Ladungova A, Culen M, Loja T, Verner J, Pospisilova
S, Smida M and Mancikova V: Hypermethylation of CD19 promoter
enables antigen-negative escape to CART-19 in vivo and in vitro. J
Immunother Cancer. 9:e0023522021. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Salter AI, Pont MJ and Riddell SR:
Chimeric antigen receptor-modified T cells: CD19 and the road
beyond. Blood. 131:2621–2629. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sun C, Dotti G and Savoldo B: Utilizing
cell-based therapeutics to overcome immune evasion in hematologic
malignancies. Blood. 127:3350–3359. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Vander Mause ER, Atanackovic D, Lim CS and
Luetkens T: Roadmap to affinity-tuned antibodies for enhanced
chimeric antigen receptor T cell function and selectivity. Trends
Biotechnol. 40:875–890. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Weiss T, Weller M, Guckenberger M, Sentman
CL and Roth P: NKG2D-based CAR T cells and radiotherapy exert
synergistic efficacy in glioblastoma. Cancer Res. 78:1031–1043.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Luan C, Zhou J, Wang H, Ma X, Long Z,
Cheng X, Chen X, Huang Z, Zhang D, Xia R and Ge J: Case report:
Local cytokine release syndrome in an acute lymphoblastic leukemia
patient after treatment with chimeric antigen receptor T-cell
therapy: A possible model, literature review and perspective. Front
Immunol. 12:7071912021. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Dos Santos DMC, Rejeski K, Winkelmann M,
Liu L, Trinkner P, Günther S, Bücklein VL, Blumenberg V, Schmidt C,
Kunz WG, et al: Increased visceral fat distribution and body
composition impact cytokine release syndrome onset and severity
after CD19 chimeric antigen receptor T-cell therapy in advanced
B-cell malignancies. Haematologica. 107:2096–2107. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Yan Z, Zhang H, Cao J, Zhang C, Liu H,
Huang H, Cheng H, Qiao J, Wang Y, Wang Y, et al: Characteristics
and risk factors of cytokine release syndrome in chimeric antigen
receptor T cell treatment. Front Immunol. 12:6113662021. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Giavridis T, van der Stegen SJC, Eyquem J,
Hamieh M, Piersigilli A and Sadelain M: CAR T cell-induced cytokine
release syndrome is mediated by macrophages and abated by IL-1
blockade. Nat Med. 24:731–738. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Wright CM, LaRiviere MJ, Baron JA, Uche C,
Xiao Y, Arscott WT, Anstadt EJ, Barsky AR, Miller D, LaRose MI, et
al: Bridging radiation therapy before commercial chimeric antigen
receptor T-cell therapy for relapsed or refractory aggressive
B-cell lymphoma. Int J Radiat Oncol Biol Phys. 108:178–188. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Dong R, Jiang S, Chen Y, Ma Y, Sun L, Xing
C, Zhang S and Yu K: Prognostic significance of cytokine release
syndrome in B cell hematological malignancies patients after
chimeric antigen receptor T cell therapy. J Interferon Cytokine
Res. 41:469–476. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Strati P, Ahmed S, Kebriaei P, Nastoupil
LJ, Claussen CM, Watson G, Horowitz SB, Brown ART, Do B, Rodriguez
MA, et al: Clinical efficacy of anakinra to mitigate CAR T-cell
therapy-associated toxicity in large B-cell lymphoma. Blood Adv.
4:3123–3127. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Norelli M, Camisa B, Barbiera G, Falcone
L, Purevdorj A, Genua M, Sanvito F, Ponzoni M, Doglioni C,
Cristofori P, et al: Monocyte-derived IL-1 and IL-6 are
differentially required for cytokine-release syndrome and
neurotoxicity due to CAR T cells. Nat Med. 24:739–748. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Li H and Zhao Y: Increasing the safety and
efficacy of chimeric antigen receptor T cell therapy. Protein Cell.
8:573–589. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Sagnella SM, White AL, Yeo D, Saxena P,
van Zandwijk N and Rasko JEJ: Locoregional delivery of CAR-T cells
in the clinic. Pharmacol Res. 182:1063292022. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Duan Y, Chen R, Huang Y, Meng X, Chen J,
Liao C, Liao C, Tang Y, Zhou C, Gao X and Sun J: Tuning the
ignition of CAR: Optimizing the affinity of scFv to improve CAR-T
therapy. Cell Mol Life Sci. 79:142021. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kosti P, Opzoomer JW, Larios-Martinez KI,
Henley-Smith R, Scudamore CL, Okesola M, Taher MYM, Davies DM,
Muliaditan T, Larcombe-Young D, et al: Hypoxia-sensing CAR T cells
provide safety and efficacy in treating solid tumors. Cell Rep Med.
2:1002272021. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Liu G, Rui W, Zhao X and Lin X: Enhancing
CAR-T cell efficacy in solid tumors by targeting the tumor
microenvironment. Cell Mol Immunol. 18:1085–1095. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Rodriguez-Garcia A, Palazon A,
Noguera-Ortega E, Powell DJ and Guedan S: CAR-T cells Hit the tumor
microenvironment: Strategies to overcome tumor escape. Front
Immunol. 11:11092020. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Majidpoor J and Mortezaee K: Angiogenesis
as a hallmark of solid tumors-clinical perspectives. Cell Oncol
(Dordr). 44:715–737. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
He H, Liao Q, Zhao C, Zhu C, Feng M, Liu
Z, Jiang L, Zhang L, Ding X, Yuan M, et al: Conditioned CAR-T cells
by hypoxia-inducible transcription amplification (HiTA) system
significantly enhances systemic safety and retains antitumor
efficacy. J Immunother Cancer. 9:e0027552021. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Ando Y, Siegler EL, Ta HP, Cinay GE, Zhou
H, Gorrell KA, Au H, Jarvis BM, Wang P and Shen K: Evaluating CAR-T
cell therapy in a Hypoxic 3D tumor model. Adv Healthc Mater.
8:e19000012019. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Karin N: The multiple faces of CXCL12
(SDF-1alpha) in the regulation of immunity during health and
disease. J Leukoc Biol. 88:463–473. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Park JA, Wang L and Cheung NV: Modulating
tumor infiltrating myeloid cells to enhance bispecific
antibody-driven T cell infiltration and anti-tumor response. J
Hematol Oncol. 14:1422021. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Jiang A, Qin Y and Springer TA: Loss of
LRRC33-dependent TGFβ1 activation enhances antitumor immunity and
checkpoint blockade therapy. Cancer Immunol Res. 10:453–467. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Siewe N and Friedman A: TGF-β inhibition
can overcome cancer primary resistance to PD-1 blockade: A
mathematical model. PLoS One. 16:e02526202021. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Jorquera-Cordero C, Lara P, Cruz LJ,
Schomann T, van Hofslot A, de Carvalho TG, Guedes PMDM, Creemers L,
Koning RI, Chan AB and de Araujo Junior RF: Extracellular vesicles
from M1-polarized macrophages combined with hyaluronic acid and a
β-blocker potentiate Doxorubicin's antitumor activity by
downregulating tumor-associated macrophages in breast cancer.
Pharmaceutics. 14:10682022. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Kos K, Salvagno C, Wellenstein MD, Aslam
MA, Meijer DA, Hau CS, Vrijland K, Kaldenbach D, Raeven EAM,
Schmittnaegel M, et al: Tumor-associated macrophages promote
intratumoral conversion of conventional CD4+ T cells into
regulatory T cells via PD-1 signalling. Oncoimmunology.
11:20632252022. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Farhood B, Khodamoradi E,
Hoseini-Ghahfarokhi M, Motevaseli E, Mirtavoos-Mahyari H, Eleojo
Musa A, Leojo Musa A and Najafi M: TGF-β in radiotherapy:
Mechanisms of tumor resistance and normal tissues injury. Pharmacol
Res. 155:1047452020. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Donlon NE, Power R, Hayes C, Reynolds JV
and Lysaght J: Radiotherapy, immunotherapy, and the tumour
microenvironment: Turning an immunosuppressive milieu into a
therapeutic opportunity. Cancer Lett. 502:84–96. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Ashrafizadeh M, Farhood B, Eleojo Musa A,
Taeb S and Najafi M: Damage-associated molecular patterns in tumor
radiotherapy. Int Immunopharmacol. 86:1067612020. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Mittal A, Nenwani M, Sarangi I, Achreja A,
Lawrence TS and Nagrath D: Radiotherapy-induced metabolic hallmarks
in the tumor microenvironment. Trends Cancer. 8:855–869. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Olivares-Urbano MA, Griñán-Lisón C,
Marchal JA and Núñez MI: CSC Radioresistance: A therapeutic
challenge to improve radiotherapy effectiveness in cancer. Cells.
9:16512020. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Minn I, Rowe SP and Pomper MG: Enhancing
CAR T-cell therapy through cellular imaging and radiotherapy.
Lancet Oncol. 20:e443–e451. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Sim AJ, Jain MD, Figura NB, Chavez JC,
Shah BD, Khimani F, Lazaryan A, Krivenko G, Davila ML, Liu HD, et
al: Radiation therapy as a bridging strategy for CAR T cell therapy
with axicabtagene ciloleucel in diffuse large B-cell lymphoma. Int
J Radiat Oncol Biol Phys. 105:1012–1021. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Oertel M and Eich HT: Bridging before CAR
T-cell therapy-a new opportunity for radiotherapy? Strahlenther
Onkol. 197:1154–1156. 2021.(In German). View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Shi LZ and Bonner JA: Bridging
radiotherapy to immunotherapy: The IFN-JAK-STAT axis. Int J Mol
Sci. 22:122952021. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Singh AK and McGuirk JP: CAR T cells:
Continuation in a revolution of immunotherapy. Lancet Oncol.
21:e168–e178. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Rodriguez-Ruiz ME, Garasa S, Rodriguez I,
Solorzano JL, Barbes B, Yanguas A, Teijeira A, Etxeberria I, Aristu
JJ, Halin C, et al: Intercellular adhesion Molecule-1 and vascular
cell adhesion molecule are induced by ionizing radiation on
lymphatic endothelium. Int J Radiat Oncol Biol Phys. 97:389–400.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Liu Z, Zhao Q, Zheng Z, Liu S, Meng L,
Dong L and Jiang X: Vascular normalization in immunotherapy: A
promising mechanisms combined with radiotherapy. Biomed
Pharmacother. 139:1116072021. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Hauth F, Ho AY, Ferrone S and Duda DG:
Radiotherapy to enhance chimeric antigen receptor T-cell
therapeutic efficacy in solid tumors: A narrative review. JAMA
Oncol. 7:1051–1059. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Li L, Yue HC, Han YW, Liu W, Xiong LG and
Zhang JW: Relationship between the invasion of lymphocytes and
cytokines in the tumor microenvironment and the interval after
single brachytherapy hypofractionated radiotherapy and conventional
fractionation radiotherapy in non-small cell lung Cancer. BMC
Cancer. 20:8932020. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Lan Y, Moustafa M, Knoll M, Xu C, Furkel
J, Lazorchak A, Yeung TL, Hasheminasab SM, Jenkins MH, Meister S,
et al: Simultaneous targeting of TGF-β/PD-L1 synergizes with
radiotherapy by reprogramming the tumor microenvironment to
overcome immune evasion. Cancer Cell. 39:1388–403.e10. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Prakash H, Klug F, Nadella V, Mazumdar V,
Schmitz-Winnenthal H and Umansky L: Low doses of gamma irradiation
potentially modifies immunosuppressive tumor microenvironment by
retuning tumor-associated macrophages: Lesson from insulinoma.
Carcinogenesis. 37:301–313. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Li CG, He MR, Wu FL, Li YJ and Sun AM: Akt
promotes irradiation-induced regulatory T-cell survival in
hepatocellular carcinoma. Am J Med Sci. 346:123–127. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Ji D, Song C, Li Y, Xia J, Wu Y, Jia J,
Cui X, Yu S and Gu J: Combination of radiotherapy and suppression
of Tregs enhances abscopal antitumor effect and inhibits metastasis
in rectal cancer. J Immunother Cancer. 8:e0008262020. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Zammarchi F, Havenith K, Bertelli F,
Vijayakrishnan B, Chivers S and van Berkel PH: CD25-targeted
antibody-drug conjugate depletes regulatory T cells and eliminates
established syngeneic tumors via antitumor immunity. J Immunother
Cancer. 8:e0008602020. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Sia J, Hagekyriakou J, Chindris I,
Albarakati H, Leong T, Schlenker R, Keam SP, Williams SG, Neeson
PJ, Johnstone RW and Haynes NM: Regulatory T cells shape the
differential impact of radiation dose-fractionation schedules on
host innate and adaptive antitumor immune defenses. Int J Radiat
Oncol Biol Phys. 111:502–514. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Huang Z, Dewanjee S, Chakraborty P, Jha
NK, Dey A, Gangopadhyay M, Chen XY, Wang J and Jha SK: CAR T cells:
Engineered immune cells to treat brain cancers and beyond. Mol
Cancer. 22:222023. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Laurent PA, Morel D, Meziani L, Depil S
and Deutsch E: Radiotherapy as a means to increase the efficacy of
T-cell therapy in solid tumors. Oncoimmunology. 12:21580132023.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Demaria S, Guha C, Schoenfeld J, Morris Z,
Monjazeb A, Sikora A, Crittenden M, Shiao S, Khleif S, Gupta S, et
al: Radiation dose and fraction in immunotherapy: One-size regimen
does not fit all settings, so how does one choose? J Immunother
Cancer. 9:e0020382021. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Pocaterra A, Catucci M and Mondino A:
Adoptive T cell therapy of solid tumors: Time to team up with
immunogenic chemo/radiotherapy. Curr Opin Immunol. 74:53–59. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Ratnayake G, Reinwald S, Edwards J, Wong
N, Yu D, Ward R, Smith R, Haydon A, Au PM, van Zelm MC and Senthi
S: Blood T-cell profiling in metastatic melanoma patients as a
marker for response to immune checkpoint inhibitors combined with
radiotherapy. Radiother Oncol. 173:299–305. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
DeSelm C, Palomba ML, Yahalom J, Hamieh M,
Eyquem J, Rajasekhar VK and Sadelain M: Low-dose radiation
conditioning enables CAR T cells to mitigate antigen escape. Mol
Ther. 26:2542–2552. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Klug F, Prakash H, Huber PE, Seibel T,
Bender N, Halama N, Pfirschke C, Voss RH, Timke C, Umansky L, et
al: Low-dose irradiation programs macrophage differentiation to an
iNOS+/M1 phenotype that orchestrates effective T cell
immunotherapy. Cancer Cell. 24:589–602. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Morris EC, Neelapu SS, Giavridis T and
Sadelain M: Cytokine release syndrome and associated neurotoxicity
in cancer immunotherapy. Nat Rev Immunol. 22:85–96. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Xia N, Haopeng P, Gong JU, Lu J, Chen Z,
Zheng Y, Wang Z, Sun YU, Yang Z, Hoffman RM and Liu F:
Robo1-specific CAR-NK immunotherapy enhances efficacy of 125I seed
brachytherapy in an orthotopic mouse model of human pancreatic
carcinoma. Anticancer Res. 39:5919–5925. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Kulzer L, Rubner Y, Deloch L, Allgäuer A,
Frey B, Fietkau R, Dörrie J, Schaft N and Gaipl US: Norm- and
hypo-fractionated radiotherapy is capable of activating human
dendritic cells. J Immunotoxicol. 11:328–336. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Marcus D, Lieverse RIY, Klein C, Abdollahi
A, Lambin P, Dubois LJ and Yaromina A: Charged particle and
conventional radiotherapy: Current implications as partner for
immunotherapy. Cancers (Basel). 13:14682021. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Kadauke S, Myers RM, Li Y, Aplenc R,
Baniewicz D, Barrett DM, Barz Leahy A, Callahan C, Dolan JG,
Fitzgerald JC, et al: Risk-adapted preemptive tocilizumab to
prevent severe cytokine release syndrome after CTL019 for pediatric
B-cell acute lymphoblastic leukemia: A prospective clinical trial.
J Clin Oncol. 39:920–930. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Wang Z, Chen C, Wang L, Jia Y and Qin Y:
Chimeric antigen receptor T-cell therapy for multiple myeloma.
Front Immunol. 13:10505222022. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Fang PQ, Gunther JR, Wu SY, Dabaja BS,
Nastoupil LJ, Ahmed S, Neelapu SS and Pinnix CC: Radiation and CAR
T-cell therapy in lymphoma: Future frontiers and potential
opportunities for synergy. Front Oncol. 11:6486552021. View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Qu C, Ping N, Kang L, Liu H, Qin S, Wu Q,
Chen X, Zhou M, Xia F, Ye A, et al: Radiation priming chimeric
antigen receptor T-cell therapy in Relapsed/Refractory diffuse
large B-cell lymphoma with high tumor burden. J Immunother.
43:32–37. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Muroyama Y, Nirschl TR, Kochel CM,
Lopez-Bujanda Z, Theodros D, Mao W, Carrera-Haro MA, Ghasemzadeh A,
Marciscano AE, Velarde E, et al: Stereotactic radiotherapy
increases functionally suppressive regulatory T cells in the tumor
microenvironment. Cancer Immunol Res. 5:992–1004. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Guha P, Heatherton KR, O'Connell KP,
Alexander IS and Katz SC: Assessing the future of solid tumor
immunotherapy. Biomedicines. 10:6552022. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Huan T, Li H and Tang B: Radiotherapy plus
CAR-T cell therapy to date: A note for cautions optimism? Front
Immunol. 13:10335122022. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
DeSelm C: The current and future role of
radiation therapy in the era of CAR T-cell salvage. Br J Radiol.
94:202100982021. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Chitadze G and Kabelitz D: Immune
surveillance in glioblastoma: Role of the NKG2D system and novel
cell-based therapeutic approaches. Scand J Immunol. 96:e132012022.
View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Rana PS, Murphy EV, Kort J and Driscoll
JJ: Road testing new CAR design strategies in multiple myeloma.
Front Immunol. 13:9571572022. View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Ashrafizadeh M, Farhood B, Eleojo Musa A,
Taeb S, Rezaeyan A and Najafi M: Abscopal effect in
radioimmunotherapy. Int Immunopharmacol. 85:1066632020. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Mortezaee K: Enriched cancer stem cells,
dense stroma, and cold immunity: Interrelated events in pancreatic
cancer. J Biochem Mol Toxicol. 35:e227082021. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Belkahla S, Brualla JM, Fayd'herbe de
Maudave A, Falvo P, Allende-Vega N, Constantinides M, Khan AUH,
Coenon L, Alexia C, Mitola G, et al: The metabolism of cells
regulates their sensitivity to NK cells depending on p53 status.
Sci Rep. 12:32342022. View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Murty S, Haile ST, Beinat C, Aalipour A,
Alam IS, Murty T, Shaffer TM, Patel CB, Graves EE, Mackall CL and
Gambhir SS: Intravital imaging reveals synergistic effect of CAR
T-cells and radiation therapy in a preclinical immunocompetent
glioblastoma model. Oncoimmunology. 9:17573602020. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Herrera FG, Ronet C, Ochoa de Olza M,
Barras D, Crespo I, Andreatta M, Corria-Osorio J, Spill A,
Benedetti F, Genolet R, et al: Low-dose radiotherapy reverses tumor
immune desertification and resistance to immunotherapy. Cancer
Discov. 12:108–133. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
101
|
Westin JR, Kersten MJ, Salles G, Abramson
JS, Schuster SJ, Locke FL and Andreadis C: Efficacy and safety of
CD19-directed CAR-T cell therapies in patients with
relapsed/refractory aggressive B-cell lymphomas: Observations from
the JULIET, ZUMA-1, and TRANSCEND trials. Am J Hematol.
96:1295–1312. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Raje N, Berdeja J, Lin Y, Siegel D,
Jagannath S, Madduri D, Liedtke M, Rosenblatt J, Maus MV, Turka A,
et al: Anti-BCMA CAR T-cell therapy bb2121 in relapsed or
refractory multiple myeloma. N Engl J Med. 380:1726–1737. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Smith EL, Mailankody S, Staehr M, Wang X,
Senechal B, Purdon TJ, Daniyan AF, Geyer MB, Goldberg AD, Mead E,
et al: BCMA-targeted CAR T-cell therapy plus radiotherapy for the
treatment of refractory myeloma reveals potential synergy. Cancer
Immunol Res. 7:1047–1053. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
104
|
Ababneh HS, Abramson JS, Johnson PC and
Patel CG: Assessing the role of radiotherapy in patients with
refractory or relapsed high-grade B-cell lymphomas treated with CAR
T-cell therapy. Radiother Oncol. 175:65–72. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Saifi O, Breen WG, Lester SC, Rule WG,
Stish B, Rosenthal A, Munoz J, Herchko SM, Murthy HS, Lin Y, et al:
Does bridging radiation therapy affect the pattern of failure after
CAR T-cell therapy in non-Hodgkin lymphoma? Radiother Oncol.
166:171–179. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Fan J, Adams A, Sieg N, Heger JM, Gödel P,
Kutsch N, Kaul D, Teichert M, von Tresckow B, Bücklein V, et al:
Potential synergy between radiotherapy and CAR T-cells-a
multicentric analysis of the role of radiotherapy in the
combination of CAR T cell therapy. Radiother Oncol. 183:1095802023.
View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Abramson JS: Anti-CD19 CAR T-cell therapy
for B-cell Non-Hodgkin lymphoma. Transfus Med Rev. 34:29–33. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Mohanty R, Chowdhury CR, Arega S, Sen P,
Ganguly P and Ganguly N: CAR T cell therapy: A new era for cancer
treatment (Review). Oncol Rep. 42:2183–2195. 2019.PubMed/NCBI
|