Introduction
Lung cancer is the leading cause of cancer-related
mortality worldwide and non-small cell lung cancer (NSCLC) accounts
for 80–85% of lung cancer cases (1). Among them, lung adenocarcinoma
comprises ~40% of all NSCLC cases. NSCLC has a poor prognosis, with
a 5-year overall survival (OS) rate of <10% (2). Notably, ~50% of patients with NSCLC
are positive for epidermal growth factor receptor (EGFR) mutations,
and benefit from targeted therapy with first- and second-generation
tyrosine kinase inhibitors (TKIs), resulting in disease-free
survival of 10–14 months (3,4).
Third-generation EGFR-TKIs, such as osimertinib, aumolertinib and
furmonertinib, have been reported to achieve a median
progression-free survival (mPFS) time of 18.9-20.8 months (5–7). EGFR
mutations are responsible for 51.4% of cases of advanced lung
adenocarcinoma in patients of Asian origin, and are strictly
concentrated in four exons (exons 18–21) (8). The most common mutations include exon
19 deletion (mutation frequency 45%; DEL) and exon 21 point
mutation (mutation frequency 40–45%; L858R) (8,9); these
two mutations account for 85–90% of all EGFR mutations (8,9). The
National Comprehensive Cancer Network guidelines recommend
first-line EGFR-TKI treatment for patients with NSCLC and EGFR
mutations, such as gefitinib and erlotinib (first-generation
EGFR-TKI), afatinib and dacomitinib (second-generation EGFR-TKI),
or osimertinib (third-generation EGFR-TKI) (2). Although EGFR-TKIs have significantly
prolonged survival in patients with EGFR-mutant NSCLC compared with
traditional chemotherapy (10–12),
acquired EGFR-TKI resistance is inevitable. In addition to the EGFR
T790M mutation (13), a high level
of vascular endothelial growth factor (VEGF) is also involved in
EGFR-TKI resistance (14,15). Activation of the EGFR signaling
pathway can upregulate VEGF production in human cancer cells
(16–18). Conversely, inhibition of EGFR has
been shown to inhibit the secretion of VEGF (16–18).
Notably, the level of VEGF has been shown to increase after
EGFR-TKI resistance (14).
Therefore, the combination of anti-angiogenic therapy with TKI or
chemotherapy after EGFR-TKI failure can theoretically control tumor
proliferation.
Anlotinib is an oral small-molecule multi-targeted
TKI, which not only hinders tumor angiogenesis by inhibiting VEGF
receptor (VEGFR)2/3, platelet-derived growth factor receptor-β,
fibroblast growth factor receptor (FGFR) and other signaling
pathways, but also directly suppresses tumor cell proliferation by
inhibiting c-kit gene expression (19,20).
Compared with other receptor TKIs, such as sorafenib, sunitinib and
pazopanib, anlotinib has more inhibitory targets and better
antitumor effects (21), and it has
been approved for third-line treatment of advanced NSCLC (22).
The present study retrospectively evaluated the
efficacy of anlotinib, alone or in combination with EGFR-TKI, as
second- or third-line treatment for patients with EGFR
mutation-positive advanced lung adenocarcinoma.
Patients and methods
Study population
Between March 1, 2018 and December 31, 2021, 48
patients were enrolled from the First Affiliated Hospital of
Nanjing Medical University. Patients histologically and
cytologically diagnosed with advanced lung adenocarcinoma (stage
III/IV), who experienced disease progression after EGFR-TKI
treatment, were retrospectively screened. Of the 48 patients
enrolled, 64.58% of patients were female, median age was 70 years
(range, 60–85), and 62.5% of patients had never smoked. All
patients enrolled were assessed to be positive for EGFR mutations
(exon 19 deletion or exon 21 L858R mutation), Eastern Cooperative
Oncology Group (ECOG) performance status (PS) (23) of 0–2, and had measurable disease
based on Response Evaluation Criteria in Solid Tumors (RECIST)
version 1.1 (24). After EGFR-TKI
resistance, patients were divided into two groups: One group
received anlotinib monotherapy and the other received treatment
with anlotinib plus EGFR-TKI. Gene mutation status was determined
by next-generation sequencing.
Anlotinib and EGFR-TKI regimens
Low-dose anlotinib (Chia Tai Tianqing Pharmaceutical
Group Co., Ltd.) was taken orally once daily (6 or 8 mg) on days
1–14 of a 21-day cycle. First-generation EGFR-TKIs, such as
gefitinib (250 mg/day) and icotinib (125 mg three times per day),
or third-generation EGFR-TKIs, such as osimertinib (80 mg/day) and
almonertinib (110 mg/day), were combined with low-dose anlotinib.
The choice of different regimens was based on objective factors,
such as the regimens formulated by different doctors, the degree of
TKI side effects, and the physical and economic conditions of the
patient.
Of note, based on clinical trials showing that
anlotinib brings survival benefits to patients with NSCLC in
third-line or further treatment (22), two patients with adencarcinoma and
EGFR mutations chose the trial package of anlotinib for treatment
before anlotinib went on the market in May 2018. These two patients
were also enrolled in the present study.
Ethics approval and patient
consent
The present retrospective study was approved by the
Ethics Committee of First Affiliated Hospital of Nanjing Medical
University (Nanjing, China, approval no. 2020-SR-279) and was
conducted according to the principles of The Declaration of
Helsinki as revised in 2013. The present study is a retrospective
study without intervention in clinical treatment. The study
collected basic information, treatment options, adverse reactions
and follow-up information of patients. Written informed consent was
obtained from the patients for the collection/analysis of their
personal information. If the patient was dead at the time of
signing, the consent form was signed by their immediate family. The
next of kin of the patient whose images are displayed provided
written informed consent for the publication of their data and
images.
Genetic sequencing method
The mutation status of ERFR was obtained from NGS
next-generation sequencing detection. Tissue samples were fixed
with 10% formalin at room temperature for 4 h. DNA was extracted
from paraffin-embedded tissue (FFPE) with QIAamp DNA FFPE Tissue
kit (Qiagen; cat. no. 56404), and the quality of the DNA was
ensured by a NanoDrop DNA analyzer (Thermo Fisher Scientific,
Inc.). The length of the sequencing was 150 bp and paired end. The
sequencing kit was NovaSeq 6000 S4 Rgt Kit v1.5 (300 cycles; cat.
no. 20028312; Illumina Inc.). The loading concentration of the
final library was 200–400pM QPCR. The software used for reference
sequence alignment, post-alignment processing, and variation
detection were BWA v0.7.17 and lofreq v2.1.3a, respectively.
Specific modified primers were used for PCR
amplification to accurately identify the target sequence. The PCR
cycle was completed by Pfu DNA Polymerase (Promega Corporation).
The specific steps included pre-denaturation at 98°C for 1 min,
denaturation at 98°C for 10 sec, annealing at 65°C for 30 sec and
extension at 72°C for 30 sec for 38 cycles then extension at 72°C
for 2 min. The amplified products were purified and enriched by 108
µl magnetic beads (Beckman Coulter, Inc.), followed by DNA fragment
repair and terminal modification, and then DNA fragments ligated to
form a library for sequencing on the Illumina platform (Illumina,
Inc.). Finally, the data software was used to analyze the gene
variation information and obtain the genetic test report. The
primers for EGFR exon 19 were: Forward 5′-CACTGGGCAGCATGTGGCA-3′
and reverse 5′-CAGCTGCCAGACATGAGAA-3′, and the primers for EGFR
exon 21 were: Forward 5′-ATTCGGATGCAGAGCTTCT-3′ and reverse
5′-CTGGTGTCAGGAAAATGCT-3′. The sequencing data are not publicly
available to protect patient privacy.
Efficacy and safety evaluation
EGFR-TKI treatment failure was classified into
dramatic progression (disease control ≥3 months; rapid increase of
tumor burden compared with the previous assessment; symptom score,
2), gradual progression (disease control ≥6 months; minor increase
of tumor burden compared with the previous assessment; symptom
score f1), and local progression (disease control ≥3 months;
isolated extracranial or intracranial progression; symptom score
r1) according to the criteria of Yang et al (25). The primary endpoint of the present
study was PFS, and the secondary endpoints included OS, response
rate and toxicity. PFS was defined as the time from the start of
treatment to disease progression or the last follow-up, and OS was
defined as the time from the start of treatment to death or the
last follow-up. Tumor response was evaluated using RECIST 1.1.
Objective tumor responses included complete response (CR), partial
response (PR), stable disease (SD) and progressive disease (PD).
Objective response rate (ORR) was the sum of CR and PR. Disease
control rate (DCR) is the sum of CR, PR and SD. Adverse events
(AEs) were assessed according to Common Terminology Criteria for
Adverse Events of the National Cancer Institute 4.0 (https://evs.nci.nih.gov/ftp1/CTCAE/CTCAE_4.03/Archive/CTCAE_4.0_2009-05-29_QuickReference_8.5×11.pdf).
Statistical analyses
Statistical analysis was performed using SPSS 23.0
(IBM) and GraphPad Prism 8.3.0 (Dotmatics). To assess the
between-group differences, clinical characteristics and treatment
efficacy were compared using the χ2 test or the Fisher's
exact test when the expected count was ≤5 in >20% of cells in a
contingency table. Survival analyses were performed using the
Kaplan-Meier method and the survival time was compared using the
log-rank test. Both univariate and multivariate analyses were
conducted using the Cox proportional hazards model to analyze
factors associated with treatment response and survival. Covariates
with P<0.05 in univariate analyses were incorporated in the
multivariate model constructed using the enter method. P<0.05
was considered to indicate a statistically significant
difference.
Results
Patients and clinical
characteristics
A total of 48 elderly patients with EGFR
mutation-positive advanced lung adenocarcinoma were enrolled after
first- or second-line EGFR-TKI treatment failure between March 2018
and December 2021. Patients subsequently received anlotinib or
anlotinib combined with EGFR-TKI. Among them, 25 patients received
anlotinib plus EGFR-TKI, whereas the remaining 23 patients received
anlotinib alone. Baseline demographic and clinical characteristics
are listed in Table I, including
age, sex, ECOG PS, smoking history, clinical stage, EGFR mutation
type, brain metastasis status, EGFR-TKI generation resistance, line
of treatment and mode of EGFR-TKI failure. There were 17 men
(35.42%) and 31 women (64.58%) aged 60–85 years, and the median age
was 70 years. A total of 24 patients (50%) were treated with
first-generation EGFR-TKI and the remaining patients were treated
with third-generation EGFR-TKI. There was no significant difference
in the mode of EGFR-TKI failure between the two groups. Second- and
third-line treatments were each given to 50% of patients.
 | Table I.Baseline characteristics of the study
population. |
Table I.
Baseline characteristics of the study
population.
| Characteristic | Anlotinib
(n=23) | Anlotinib +
EGFR-TKI (n=25) | χ2 | P-value |
|---|
| Median age, years
(range) | 69 (63–84) | 71 (60–85) |
|
|
| Sex |
|
| 0.479 | 0.489 |
|
Male | 7 (30.43%) | 10 (40.00%) |
|
|
|
Female | 16 (69.57%) | 15 (60.00%) |
|
|
| ECOG PS |
|
| 0.280 | 0.597 |
|
0-1 | 13 (56.52%) | 16 (64.00%) |
|
|
| 2 | 10 (43.48%) | 9 (36.00%) |
|
|
| Smoking
history |
|
| 0.941 | 0.332 |
|
Yes | 7 (30.43%) | 11 (44.00%) |
|
|
| No | 16 (69.57) | 14 (56.00%) |
|
|
| Clinical stage |
|
| - | 0.407a |
|
III | 4 (17.39%) | 2 (8.00%) |
|
|
| IV | 19 (82.61%) | 23 (92.00%) |
|
|
| Brain
metastases |
|
| 0 | 0.990 |
|
Yes | 11 (47.83%) | 12 (48.00%) |
|
|
| No | 12 (52.17%) | 13 (52.00%) |
|
|
| EGFR mutation
type |
|
| 0.004 | 0.951 |
| Exon 19
deletion | 14 (60.87%) | 15 (60.00%) |
|
|
|
L858R | 9 (39.13%) | 10 (40.00%) |
|
|
| T790M mutation |
|
| 0.117 | 0.732 |
|
Yes | 9 (39.13%) | 11 (44.00%) |
|
|
| No | 14 (60.87%) | 14 (56.00%) |
|
|
| EGFR-TKI generation
resistance |
|
| 0.751 | 0.386 |
|
First-generation | 10 (43.48%) | 14 (56.00%) |
|
|
|
Third-generation | 13 (56.52%) | 11 (44.00%) |
|
|
| Mode of EGFR-TKI
failure |
|
| 0.034 | 0.853 |
|
Gradual/Local progression | 16 (69.57%) | 18 (72.00%) |
|
|
|
Dramatic progression | 7 (30.43%) | 7 (28.00%) |
|
|
| Treatment-line |
|
| 2.087 | 0.149 |
|
Second-line | 9 (39.13%) | 15 (60.00%) |
|
|
|
Third-line | 14 (60.87%) | 10 (40.00%) |
|
|
Efficacy outcomes and subgroup
analysis
After two cycles/2 months of treatment, the response
rate was evaluated. One (4.35%) of the 23 patients in the anlotinib
monotherapy group and three (12.00%) of the 25 patients in the
combination group experienced PR (P=0.663). A total of 13 (56.52%)
of the 23 patients in the anlotinib monotherapy group and 19
(76.00%) of the 25 patients in the combination group experienced
DCR (P=0.153). No statistical difference in ORR and DCR between the
two groups was observed (Table
II).
| Table II.Efficacy evaluation. |
Table II.
Efficacy evaluation.
| Treatment
outcome | Total | Anlotinib
(n=23) | Anlotinib +
EGFR-TKI (n=25) | χ2 | P-value |
|---|
| CR | 0 | 0 | 0 |
|
|
| PR | 4 | 1 (4.35%) | 3 (12%) |
|
|
| SD | 28 | 12 (52.17%) | 16 (64%) |
|
|
| PD | 16 | 10 (43.48%) | 6 (24%) |
|
|
| ORR | 13 | 1 (4.35%) | 3 (12%) | - | 0.610a |
| DCR | 32 | 13 (56.52%) | 19 (76%) | 2.045 | 0.153 |
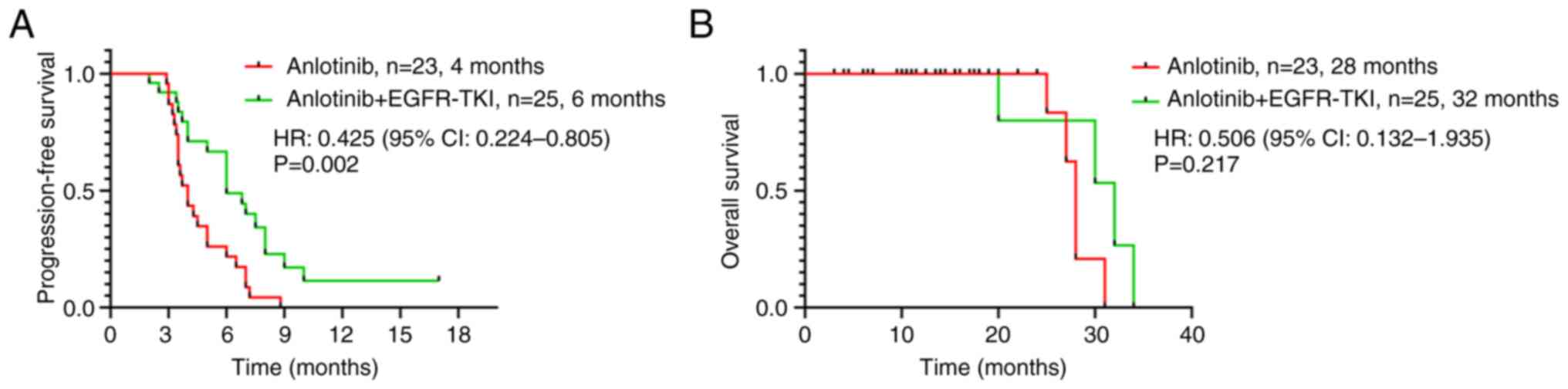
On December 31, 2021, 42 patients (87.50%) had
reached the endpoint of disease progression or death, and the
median follow-up time was 14.75 months. The mPFS was 4.0 months
[95% confidence interval (CI), 3.38-4.62] in the anlotinib
monotherapy group and 6.0 months (95% CI, 4.35-7.65) in the
combination group (HR=0.425; 95% CI, 0.224-0.805; Fig. 1A), and the difference was
statistically significant (P=0.002). The median OS (mOS) was 28
months (95% CI, 27.13-28.87) in the anlotinib monotherapy group and
32 months (95% CI, 22.04-41.96) in the combination group, and there
was no statistically significant difference between the two groups
(HR=0.506; 95% CI, 0.132-1.935; P=0.217; Fig. 1B). However, mOS in the combination
group had a prolonged trend compared with that in the anlotinib
monotherapy group.
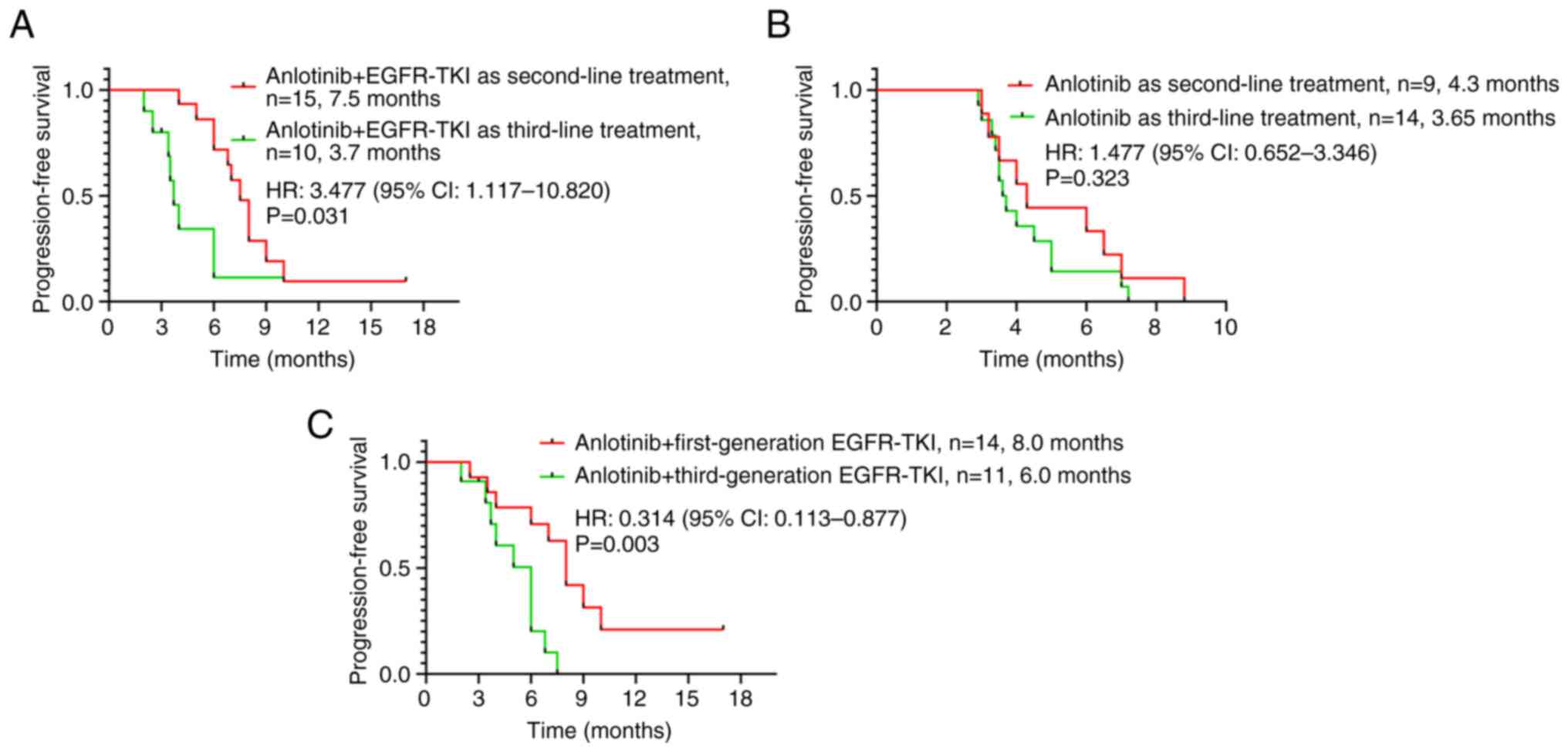
At the time of data cutoff, anlotinib combined with
EGFR-TKI had a significant benefit on mPFS as second-line treatment
compared with as third-line treatment (7.5 vs. 3.7 months;
HR=3.477; 95% CI, 1.117-10.820; P=0.031; Fig. 2A), whereas there was no significant
difference in mPFS between second- and third-line treatment with
anlotinib alone (4.3 vs. 3.65 months; HR=1.477; 95% CI,
0.652-3.346; P=0.323; Fig. 2B).
Moreover, the difference between anlotinib combined with first- or
third-generation TKIs was statistically compared; the results
revealed that anlotinib combined with first-generation TKIs could
more significantly prolong the PFS of TKI-resistant patients (8.0
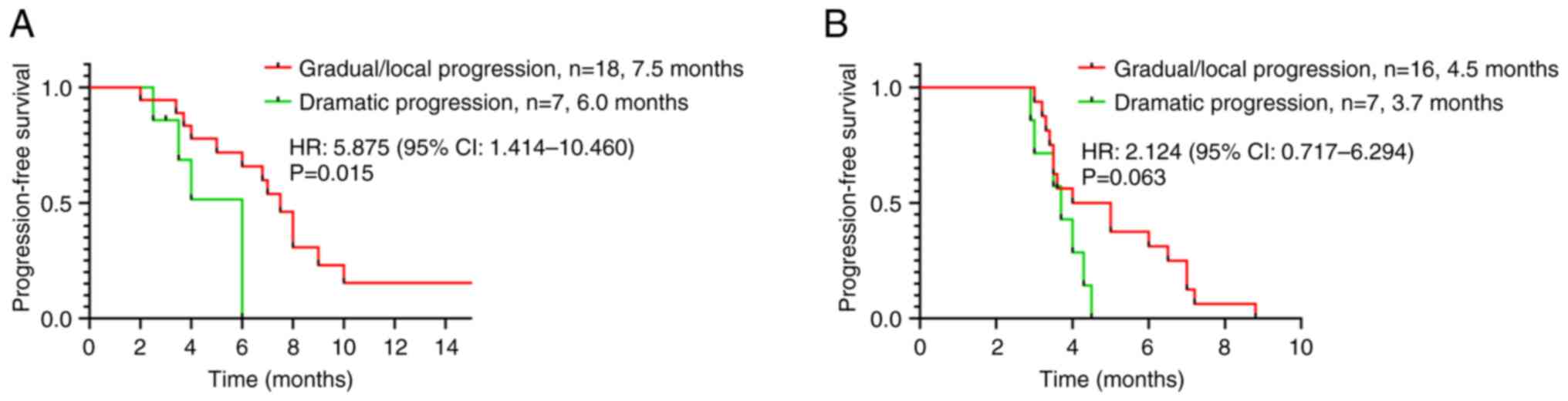
vs. 6.0 months; HR=0.314; 95% CI, 0.113-0.877; P=0.003; Fig. 2C). Further stratification analysis
was performed based on EGFR-TKI failure modes. In the combination
group, patients with gradual/local progression had longer mPFS than
those with dramatic progression (7.5 vs. 6.0 months; HR=5.875; 95%
CI, 1.414-10.460; P=0.015; Fig.
3A). In the anlotinib monotherapy group, mPFS was not
statistically different between patients with gradual/local
progression and those with dramatic progression (4.5 vs. 3.7
months; HR=2.124; 95% CI, 0.717-6.294; P=0.063; Fig. 3B).
The factors in subgroup analysis included age, sex,
smoking history, tumor stage, ECOG PS, brain metastasis status,
EGFR mutation type, EGFR-TKI generation resistance, line of
treatment and mode of EGFR-TKI failure. As shown in Fig. 4 (log-rank test), combination therapy
could markedly reduce the risk of PD in patients ≥70 years old
(HR=0.339; 95% CI, 0.150-0.767; P=0.005), in female patients
(HR=0.386; 95% CI, 0.175-0.853; P=0.009), in patients with an ECOG
PS of 2 (HR=0.218; 95% CI, 0.072-0.655; P=0.001), in patients
without brain metastasis (HR=0.297; 95% CI, 0.115-0.766; P=0.003)
and in patients with EGFR L858R mutation (HR=0.281; 95% CI,
0.092-0.851; P=0.002). Significant differences were also detected
in subgroups of patients with first-generation EGFR-TKI resistance
(HR=0.275; 95% CI, 0.095-0.795; P=0.001) and gradual/local EGFR-TKI
progression (HR=0.376; 95%CI, 0.172-0.822; P=0.012).
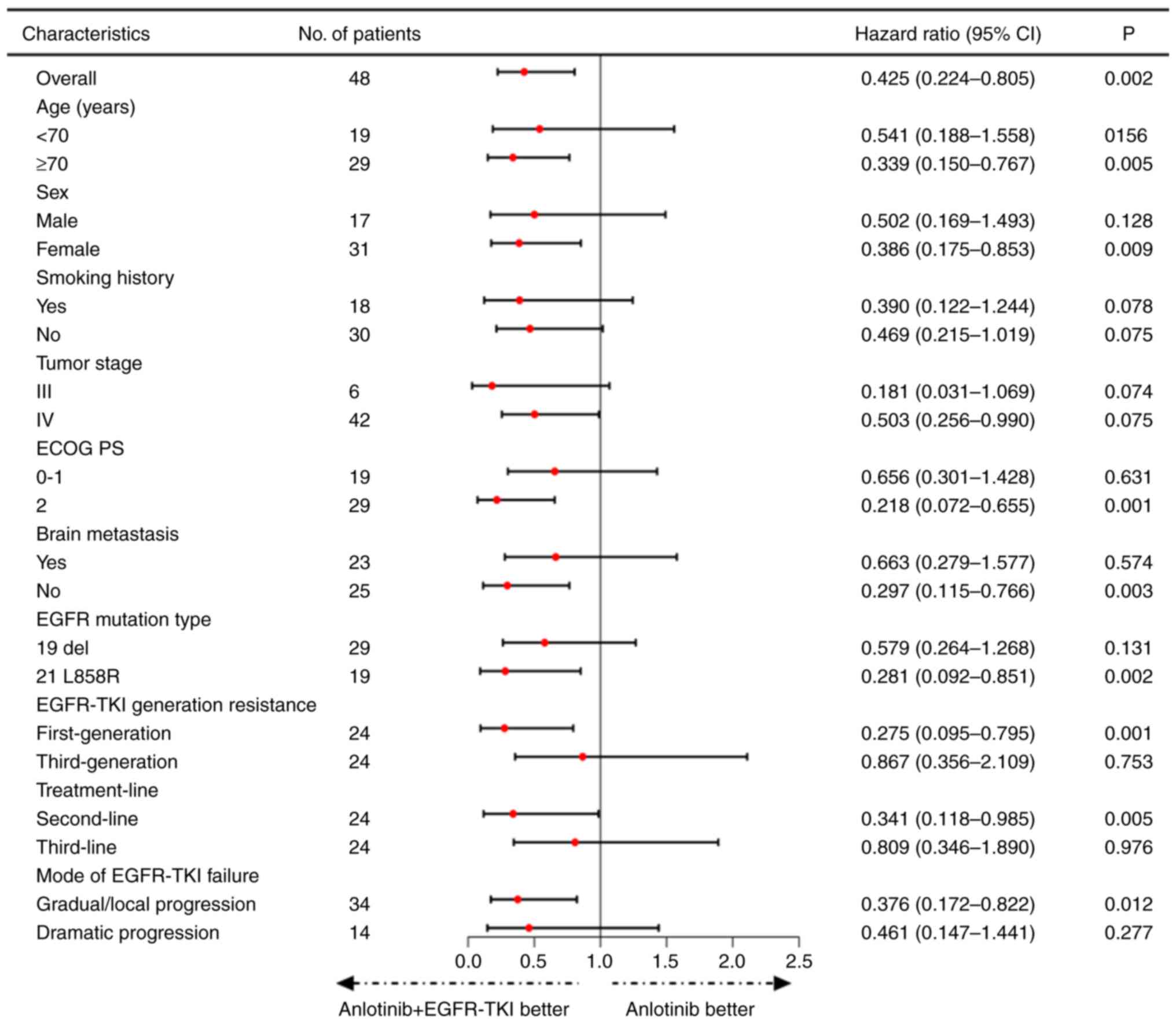 | Figure 4.Effects of different factors on the
prognosis of patients with TKI treatment failure were analyzed in
subgroups, including age, sex, smoking history, tumor stage, ECOG
PS, brain metastasis, EGFR mutation type, EGFR-TKI generation
resistance, treatment-line and mode. CI, confidence interval; ECOG
PS, Eastern Cooperative Oncology Group performance status; EGFR,
epidermal growth factor receptor; TKI, tyrosine kinase
inhibitor. |
Exploratory analyses were also performed to
determine whether any clinical or pathological features were
associated with PFS. In the Cox univariate analysis, EGFR-TKI
generation resistance, mode of EGFR-TKI failure, treatment group
and line of treatment were associated with PFS (P=0.028, P=0.005,
P=0.004 and P=0.005, respectively; Table III). Notably, tumor stage, ECOG
PS, EGFR mutation type and brain metastasis status were not found
to be associated with any predictive effects. In multivariate
analysis, combination therapy of anlotinib and EGFR-TKI was
identified as an independent predictor for better PFS as compared
with anlotinib monotherapy (HR=0.438; 95% CI, 0.220-0.871;
P=0.019). Dramatic progression was also revealed to be an
independent risk factor for poor prognosis (HR=2.637; 95% CI,
1.218-5.706; P=0.014) (Table
III).
| Table III.Univariate and multivariate Cox
regression analyses of factors associated with progression-free
survival. |
Table III.
Univariate and multivariate Cox
regression analyses of factors associated with progression-free
survival.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Characteristic | HR | 95% CI | P-value | HR | 95% CI | P-value |
|---|
| Age (<70 vs. ≥70
years) | 0.390 | 0.406-1.422 | 0.456 |
|
| NI |
| Sex (Male vs.
Female) | 0.786 | 0.417-1.480 | 0.456 |
|
| NI |
| Smoking (No vs.
Yes) | 0.862 | 0.461-1.611 | 0.642 |
|
|
|
| ECOG PS (0–1 vs.
2) | 1.064 | 0.564-2.009 | 0.848 |
|
| NI |
| Tumor stage (III
vs. IV) | 0.794 | 0.306-2.063 | 0.637 |
|
| NI |
| Brain metastases
(No vs. Yes) | 0.849 | 0.578-1.946 | 1.061 |
|
| NI |
| EGFR mutation
type |
|
|
|
|
|
|
| (Exon 19 deletion
vs. L858R) | 1.169 | 0.625-2.186 | 0.624 |
|
| NI |
| EGFR-TKI generation
resistance |
|
|
|
|
|
|
| (First-generation
vs. Third-generation) | 2.060 | 1.083-3.918 | 0.028a | 1.269 | 0.587-2.741 | 0.545 |
| Mode of EGFR-TKI
failure (Gradual/Local | 2.831 | 1.361-5.891 | 0.005a | 2.637 | 1.218-5.706 | 0.014a |
| progression vs.
Dramatic progression) |
|
|
|
|
|
|
| Treatment group
(Anlotinib vs. Anlotinib + | 0.390 | 0.205-0.744 | 0.004a | 0.438 | 0.220-0.871 | 0.019a |
| EGFR-TKI) |
|
|
|
|
|
|
| Treatment-line
(Second-line vs. Third-line) | 2.465 | 1.319-4.607 | 0.005a | 1.512 | 0.697-3.283 | 0.296 |
AEs
None of the patients stopped treatment due to severe
AEs. During the treatment, two patients (8.69%) in the anlotinib
monotherapy group and five patients (20.00%) in the combination
group had their anlotinib dose reduced. The patients experienced
grade 3 adverse reactions after taking anlotinib, including
hypertension, fatigue and mucositis. The elderly patients had poor
tolerance to adverse reactions, so the dosage of anlotinib was
reduced. After the dose reduction, the patient had no adverse
reactions of grade 3 or above. No new or unexpected AEs were
observed in the present study. The most common AEs included
hypertension, fatigue, diarrhea, mucositis, hoarseness, rash,
bleeding, proteinuria, paronychia, leukopenia, thrombocytopenia and
transaminase elevation (Table IV).
AEs of grade 2 were reported in four patients (17.39%) in the
anlotinib monotherapy group and eight patients (32.00%) in the
combination group. Of these, the most common grade 2 AEs were
hypertension, fatigue, diarrhea, paronychia, mucositis and
transaminase elevation. There were no grade 3–5 AEs.
| Table IV.Adverse events. |
Table IV.
Adverse events.
|
| Anlotinib group
(n=23) | Anlotinib +
EGFR-TKI group (n=25) |
|---|
|
|
|
|
|---|
| Toxicity | All grades (%) | Grade 2 | All grades (%) | Grade 2 |
|---|
| Hypertension | 12 (52.17) | 2 (8.70%) | 15 (60.00) | 2 (8.00%) |
| Fatigue | 10 (43.48) | 1 (4.35%) | 11 (44.00) | 3 (12.00%) |
| Diarrhea | 6 (26.09) | 1 (4.35%) | 6 (24.00) | 0 |
| Mucositis | 4 (17.39) | 0 | 4 (16.00) | 1 (4.00%) |
| Hoarseness | 2 (8.70) | 0 | 3 (12.00) | 0 |
| Rash | 7 (30.43) | 0 | 10 (40.00) | 0 |
| Bleeding | 3 (13.04) | 0 | 3 (12.00) | 0 |
| Proteinuria | 5 (21.74) | 0 | 6 (24.00) | 0 |
| Paronychia | 2 (8.70) | 0 | 3 (12.00) | 1 (4.00%) |
| Leukopenia | 1 (4.35) | 0 | 1 (4.00) | 0 |
|
Thrombocytopenia | 4 (17.39) | 0 | 3 (12.00) | 0 |
| Transaminase
elevation | 2 (8.70) | 0 | 5 (20.00) | 1 (4.00%) |
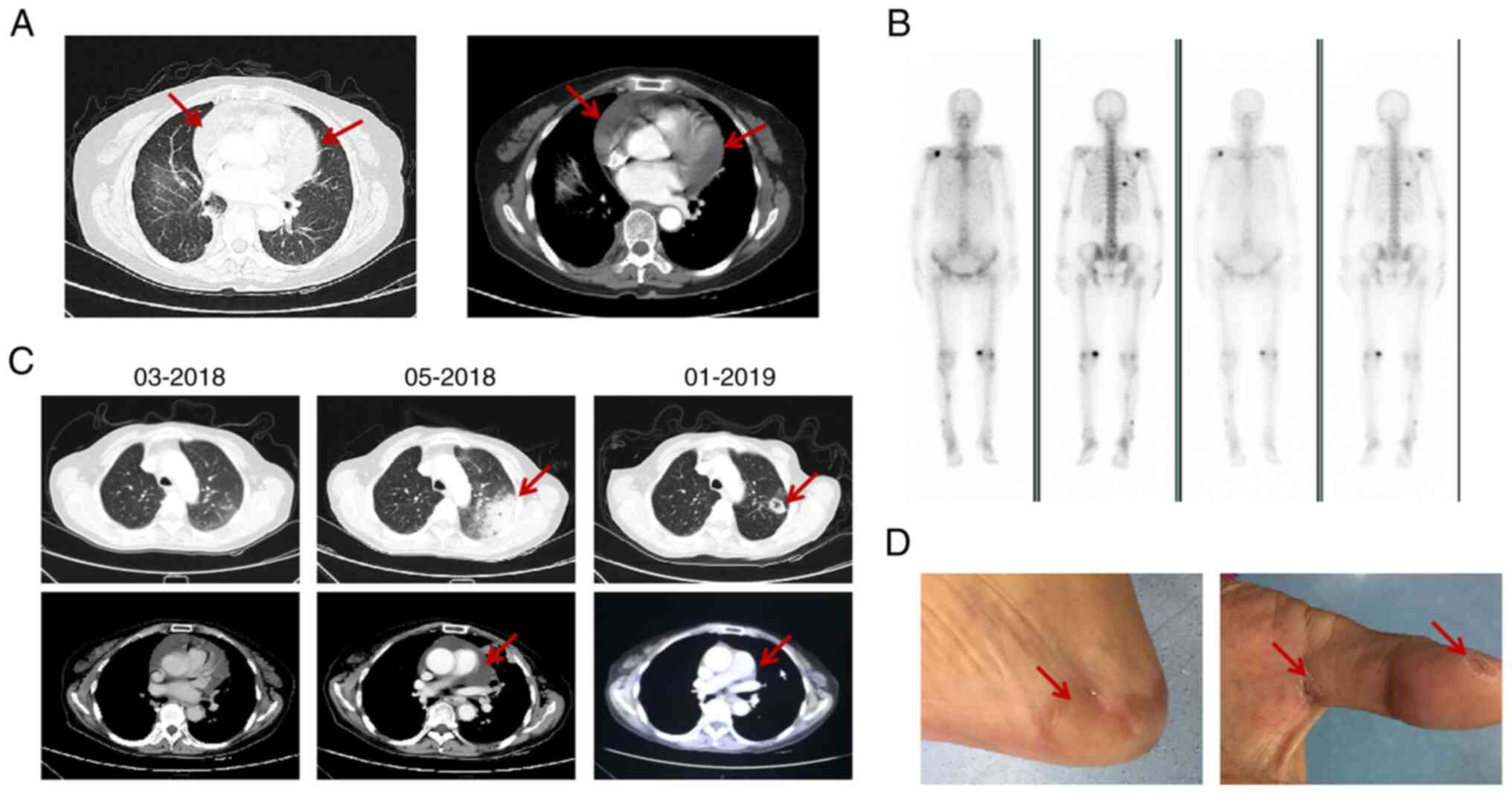
Typical case
A 74-year-old woman was pathologically diagnosed
with right lower lobe adenocarcinoma with pericardial effusion and
bone metastasis in Jiangsu Provincial Hospital of Traditional
Chinese Medicine in January 2015 (Fig.
5A and B). The EGFR L858R mutation was confirmed. From January
2015, icotinib (125 mg, three times daily) was taken orally as
first-line treatment, during which hand, foot skin and oral mucosa
reactions occurred. In March 2018, computerized tomography (CT) and
echocardiography showed enlargement of the lesion and PD was
reached, suggesting acquired resistance to icotinib. In addition,
genetic testing results again showed that T790M had no
mutations.
After she had refused second-line chemotherapy, the
patient began oral antitumor therapy with anlotinib in April 2018.
A CT scan was performed in May, which showed progression (Fig. 5C). After written informed consent
was obtained, the treatment was switched to anlotinib in
combination with icotinib. The treatment was well tolerated, and
the clinical symptoms, such as decreased physical strength and
chest tightness, were gradually relieved. In addition, repeated
chest CT showed lesions with cavitation (Fig. 5C) Solid tumor lesions show internal
cavitation, which is also a sign of tumor improvement. The dose of
anlotinib was reduced during treatment, due to hand and foot
syndrome, and was gradually increased to normal after symptom
remission (Fig. 5D). Unfortunately,
cryptococcal infection developed in February 2019 and the treatment
was abandoned, leading to tumor progression. Overall, the PFS of
this patient achieved 9 months as a result of the anlotinib
combined with EGFR-TKI in the third treatment line.
Discussion
EGFR is a transmembrane receptor tyrosine kinase
often upregulated in NSCLC (26).
This protein can lead to cell proliferation and survival, and may
inhibit apoptosis and activate angiogenesis (9,27).
Oral EGFR-TKIs have shown initial clinical efficacy, significantly
prolonging PFS in patients with EGFR mutations (4,11);
however, drug resistance is the biggest barrier to EGFR-TKI
treatment for patients with NSCLC (13). It has been reported that the
mechanism underlying EGFR-TKI resistance is complex, with the T790M
mutation and mesenchymal-epithelial transition factor amplification
being the most common causes, accounting for 50 and 20% of
resistance, respectively (13).
Although osimertinib has achieved outstanding efficacy in patients
with EGFR T790M-mutant NSCLC in terms of PFS and OS (28), most people inevitably develop
resistance, which presents another challenge in the treatment of
NSCLC. For T790M-negative patients with third- or first-generation
TKI resistance, chemotherapy with or without antiangiogenic
inhibitors is often used sequentially, but the side effects are
severe and the efficacy is unsatisfactory (29). There is an urgent need to find a new
treatment mode for elderly patients with cancer who cannot tolerate
chemotherapy. The present study suggested that anlotinib combined
with TKI may be an effective and tolerable new treatment mode.
Anlotinib is a novel oral multi-targeted TKI, which
is characterized by a broad spectrum of inhibitory action on tumor
angiogenesis and growth (20). The
effect of anlotinib has been revealed in ALTER-0303, a
multi-center, double-blind, phase 3 randomized clinical trial
(22). The results of this trial
showed that anlotinib improved OS compared with a placebo (9.6 vs.
6.3 months; P=0.002), and the primary PFS was longer in the
anlotinib group (4.8 months; 95% CI, 3.5-6.4) compared with that in
the placebo group (1.2 months, 95% CI, 0.7-1.6); furthermore, the
overall response rate (ORR) was 10.0% and the disease control rate
(DCR) was 83.3% in the anlotinib group. Moreover, a subgroup
analysis reported that anlotinib improved the survival of patients
with adenocarcinoma treated with at least two lines of chemotherapy
or TKIs (22). Anlotinib has been
approved in China for the third-line treatment of patients with
locally advanced or metastatic NSCLC, and is well tolerated,
especially in elderly patients (19).
VEGF serves an important role in the formation of
new blood vessels (30), and
inhibition of VEGF is a key therapeutic strategy for cancer
treatment (31). EGFR-TKI
resistance is often accompanied by increased levels of VEGF
(14), and dual inhibition of EGFR
and VEGF in NSCLC with EGFR mutations is theoretically a promising
strategy. Several studies have reported long-term clinical benefits
from continued use of original EGFR-TKIs and anti-angiogenic
inhibitors, such as bevacizumab and apatinib (VEGFR2 inhibitors),
after EGFR-TKI resistance (32–35).
In addition, preclinical data showed that anlotinib can overcome
the acquired EGFR-TKI resistance by inhibiting the FGFR1 signaling
pathway, or by downregulating the ERK and AKT signaling pathway
(36–38). These data suggested that anlotinib
combined with TKIs may be considered a new treatment mode, which
provides a basis for the treatment of elderly patients with
TKI-resistant NSCLC.
In the present study, the efficacy of anlotinib
combined with EGFR-TKI was compared with that of anlotinib
monotherapy in elderly patients with acquired EGFR-TKI resistance.
Low-dose anlotinib ensured tolerance and compliance in elderly
patients. Although there was no statistical difference in ORR and
DCR between the two groups, the mPFS in the combination group was
longer than that in the anlotinib monotherapy group (6 vs. 4
months, HR=0.425; 95% CI, 0.224-0.805; P=0.002), suggesting that
the addition of anlotinib after EGFR-TKI treatment failure can
reverse drug resistance to some extent and gain survival benefits.
It has recently been reported that anlotinib combined with TKIs or
immune checkpoint inhibitors, compared with anlotinib alone, can
prolong PFS in elderly patients with lung cancer and EGFR mutations
(39). In this study, the research
population was not all patients with lung adenocarcinoma, 20% of
patients had rare EGFR mutations (not 19Del or L858R mutation), and
the combination therapy included anlotinib combined with immune
checkpoint inhibitors (4/13 patients); these confounding factors
contributed to the bias of the study results (39). However, the present study focused on
a population of elderly patients with lung adenocarcinoma, with
exon 19 deletion or L858R mutation, and explored the efficacy of
anlotinib alone or in combination with TKIs as second- or
third-line therapy, which differs from previous studies (39,40).
The present study revealed that anlotinib combined with EGFR-TKI
can benefit the PFS of TKI-resistant elderly patients with lung
cancer; however, this benefit could not be translated into
prolonged OS. This finding may be due to the retrospective nature
of the study, which failed to achieve randomization of patients,
which inevitably had a slight impact on the statistical
results.
Further stratification analysis showed that EGFR-TKI
combined with anlotinib as second-line treatment had a significant
benefit on PFS than as third-line treatment (7.5 vs. 3.7 months;
HR=3.477; 95% CI, 1.117-10.820; P=0.031), indicating that early
application of EGFR-TKI and anlotinib may lead to better survival.
Stratification analysis based on the EGFR-TKI failure mode
demonstrated that patients with gradual/local progression were more
likely to benefit from this combination strategy than those with
dramatic progression (7.5 vs. 6.0 months; HR=5.875; 95% CI,
1.414-10.460; P=0.015), consistent with previous findings (41). As for PFS, multivariate Cox
regression suggested that combination therapy with anlotinib and
EGFR-TKI (HR=0.438; 95% CI, 0.220-0.871; P=0.019) was considered a
protective factor for prognosis, whereas dramatic progression
(HR=2.637; 95% CI, 1.218-5.706; P=0.014) had adverse effects on
subsequent treatment (Table
III).
Subgroup analysis showed that the combination
therapy was superior to anlotinib monotherapy for the majority of
patients, and was better in young, female, non-smoking patients,
and in those without brain metastasis and with gradual/local
progression. Significant differences were also observed in
subgroups of patients with first-generation EGFR-TKI resistance and
third-generation EGFR-TKI resistance, indicating that the
combination strategy of EGFR-TKI and anlotinib will be more
beneficial to the first-generation EGFR-TKI in improving the PFS of
drug-resistant patients. The advantage of combination therapy was
more obvious for patients with the EGFR L858R mutation than those
with the 19Del mutation, implying a potential mechanism of
sensitivity that requires further study. Several clinical trials
have reported that bevacizumab or apatinib combined with
first-generation EGFR-TKI can be used as a treatment option for TKI
resistance in EGFR-mutant lung adenocarcinoma (35,42).
Another retrospective study suggested the superiority of
osimertinib + bevacizumab over chemotherapy + bevacizumab after the
failure of osimertinib (43). The
present study suggested that anlotinib combined with EGFR-TKI was
more advantageous than anlotinib alone, especially anlotinib
combined with first-generation EGFR-TKI. These findings
demonstrated that EGFR-TKI combined with anti-tumor angiogenesis
drugs, including bevacizumab, apatinib and anlotinib can be
effective after EGFR-TKI resistance. In the present study, a novel
treatment mode of anlotinib combined with EGFR-TKI was proposed for
EGFR-TKI-resistant patients with EGFR-mutant lung adenocarcinoma,
especially for elderly patients.
In view of the efficacy of drugs, a number of
previous studies (44,45) did not consider the dosage of drugs
as the main obstacle to the prognosis of elderly patients with
cancer. However, the tolerance of elderly lung cancer patients to
anticancer drugs was specifically considered in the present study.
The potential for different people to tolerate different drugs may
also attract more attention in further studies. Due to the low dose
of anlotinib used in the present study, there were no AEs of grade
3 or higher. Elderly patients with lung cancer have a poor
constitution and often suffer from a variety of complications,
including pulmonary heart disease, chronic obstructive pulmonary
disease and atelectasis. In view of this, based on genetic testing,
elderly patients are more willing to choose targeted drug therapy
(46,47). Anlotinib, as a small-molecule
multi-targeted anti-angiogenic drug, also has the same side effects
as other targeted drugs, including high blood pressure, fatigue,
diarrhea and elevated transaminase. In the present study, low-dose
anlotinib was used, which could better control the AEs of patients,
and ensure the persistence and compliance of treatment. With the
advent of precision cancer treatment, real-time gene detection is
performed throughout lung cancer treatment, which can provide more
elderly patients with individualized treatment. TKI resistance
remains an issue to be solved, and it is imperative to understand
the mechanism of drug resistance and seek new treatment
options.
In conclusion, low-dose anlotinib in combination
with EGFR-TKI provides an effective and well-tolerated treatment
mode for elderly patients with TKI-resistant EGFR-mutant NSCLC,
with significant improvements in disease burden and time to
progression.
Acknowledgements
Not applicable.
Funding
This work was supported by the National Natural Science
Foundation of China (grant nos. 81972188 and 81502623).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
RG conceived the idea for the study and supervised
it. YiC and NJ were responsible for designing and writing the
manuscript. XL and NC performed the collection and analysis of
clinical data. YuC and CZ were responsible for interpretation of
data and revising the manuscript critically for important
intellectual content. JS performed data interpretation, editing the
manuscript and guaranteed the integrity of the study. YiC and RG
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
The present retrospective study was approved by the
Ethics Committee of First Affiliated Hospital of Nanjing Medical
University (Nanjing, China; Approval no. 2020-SR-279) and was
conducted according to the principles of The Declaration of
Helsinki as revised in 2013. Written informed consent was obtained
from the patients for the collection/analysis of their personal
information. If patients had succumbed at the time of signing, the
consent form was signed by their immediate family.
Patient consent for publication
The next of kin of the patient whose images are
displayed provided written informed consent for the publication of
their data and images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2020. CA Cancer J Clin. 70:7–30. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ettinger DS, Wood DE, Aisner DL, Akerley
W, Bauman JR, Bharat A, Bruno DS, Chang JY, Chirieac LR, D'Amico
TA, et al: NCCN guidelines insights: Non-small cell lung cancer,
version 2.2021. J Natl Compr Canc Netw. 19:254–266. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Fukuoka M, Wu YL, Thongprasert S,
Sunpaweravong P, Leong SS, Sriuranpong V, Chao TY, Nakagawa K, Chu
DT, Saijo N, et al: Biomarker analyses and final overall survival
results from a phase III, randomized, open-label, first-line study
of gefitinib versus carboplatin/paclitaxel in clinically selected
patients with advanced non-small-cell lung cancer in Asia (IPASS).
J Clin Oncol. 29:2866–2874. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Yang JC, Sequist LV, Geater SL, Tsai CM,
Mok TS, Schuler M, Yamamoto N, Yu CJ, Ou SHI, Zhou C, et al:
Clinical activity of afatinib in patients with advanced
non-small-cell lung cancer harbouring uncommon EGFR mutations: A
combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung
6. Lancet Oncol. 16:830–838. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Soria JC, Ohe Y, Vansteenkiste J,
Reungwetwattana T, Chewaskulyong B, Lee KH, Dechaphunkul A, Imamura
F, Nogami N, Kurata T, et al: Osimertinib in untreated EGFR-mutated
advanced non-small-cell lung cancer. N Engl J Med. 378:113–125.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Lu S, Dong X, Jian H, Chen J, Chen G, Sun
Y, Ji Y, Wang Z, Shi J, Lu J, et al: AENEAS: A randomized phase III
trial of aumolertinib versus gefitinib as first-line therapy for
locally advanced or metastaticnon-small-cell lung cancer With EGFR
exon 19 deletion or L858R mutations. J Clin Oncol. 40:3162–3171.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shi Y, Chen G, Wang X, Liu Y, Wu L, Hao Y,
Liu C, Zhu S, Zhang X, Li Y, et al: Furmonertinib (AST2818) versus
gefitinib as first-line therapy for Chinese patients with locally
advanced or metastatic EGFR mutation-positive non-small-cell lung
cancer (FURLONG): A multicentre, double-blind, randomised phase 3
study. Lancet Respir Med. 10:1019–1028. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shi Y, Au JS, Thongprasert S, Srinivasan
S, Tsai CM, Khoa MT, Heeroma K, Itoh Y, Cornelio G and Yang PC: A
prospective, molecular epidemiology study of EGFR mutations in
Asian patients with advanced non-small-cell lung cancer of
adenocarcinoma histology (PIONEER). J Thorac Oncol. 9:154–162.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Liam CK, Leow HR, How SH, Pang YK, Chua
KT, Lim BK, Lai NL, Kuan YC, Pailoor J and Rajadurai P: Epidermal
growth factor receptor mutations in non- small cell lung cancers in
a multiethnic malaysian patient population. Asian Pac J Cancer
Prev. 15:321–326. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Rosell R, Carcereny E, Gervais R,
Vergnenegre A, Massuti B, Felip E, Palmero R, Garcia-Gomez R,
Pallares C, Sanchez JM, et al: Erlotinib versus standard
chemotherapy as first-line treatment for European patients with
advanced EGFR mutation-positive non-small-cell lung cancer
(EURTAC): A multicentre, open-label, randomised phase 3 trial.
Lancet Oncol. 13:239–246. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Zhou C, Wu YL, Chen G, Feng J, Liu XQ,
Wang C, Zhang S, Wang J, Zhou S, Ren S, et al: Erlotinib versus
chemotherapy as first-line treatment for patients with advanced
EGFR mutation-positive non-small-cell lung cancer (OPTIMAL,
CTONG-0802): A multicentre, open-label, randomised, phase 3 study.
Lancet Oncol. 12:735–742. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Maemondo M, Inoue A, Kobayashi K, Sugawara
S, Oizumi S, Isobe H, Gemma A, Harada M, Yoshizawa H, Kinoshita I,
et al: Gefitinib or chemotherapy for non-small-cell lung cancer
with mutated EGFR. N Engl J Med. 362:2380–2388. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Camidge DR, Pao W and Sequist LV: Acquired
resistance to TKIs in solid tumours: Learning from lung cancer. Nat
Rev Clin Oncol. 11:473–481. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hung MS, Chen IC, Lin PY, Lung JH, Li YC,
Lin YC, Yang CT and Tsai YH: Epidermal growth factor receptor
mutation enhances expression of vascular endothelial growth factor
in lung cancer. Oncol Lett. 12:4598–4604. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rotow J and Bivona TG: Understanding and
targeting resistance mechanisms in NSCLC. Nat Rev Cancer.
17:637–658. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Pore N, Jiang Z, Gupta A, Cerniglia G, Kao
GD and Maity A: EGFR tyrosine kinase inhibitors decrease VEGF
expression by both hypoxia-inducible factor (HIF)-1-independent and
HIF-1-dependent mechanisms. Cancer Res. 66:3197–3204. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Fang L, Yu Y, Li Y, Wang S, He J, Zhang R
and Sun YP: Upregulation of AREG, EGFR, and HER2 contributes to
increased VEGF expression in granulosa cells of patients with
OHSSdagger. Biol Reprod. 101:426–432. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Osude C, Lin L, Patel M, Eckburg A, Berei
J, Kuckovic A, Dube N, Rastogi A, Gautam S, Smith TJ, et al:
Mediating EGFR-TKI resistance by VEGF/VEGFR autocrine pathway in
non-small cell lung cancer. Cells. 11:16942022. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Syed YY: Correction to: Anlotinib: First
global approval. Drugs. 78:12872018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Xie C, Wan X, Quan H, Zheng M, Fu L, Li Y
and Lou L: Preclinical characterization of anlotinib, a highly
potent and selective vascular endothelial growth factor receptor-2
inhibitor. Cancer Sci. 109:1207–1219. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lin B, Song X, Yang D, Bai D, Yao Y and Lu
N: Anlotinib inhibits angiogenesis via suppressing the activation
of VEGFR2, PDGFRbeta and FGFR1. Gene. 654:77–86. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Han B, Li K, Wang Q, Zhang L, Shi J, Wang
Z, Cheng Y, He J, Shi Y, Zhao Y, et al: Effect of anlotinib as a
third-line or further treatment on overall survival of patients
with advanced non-small cell lung cancer: The ALTER 0303 phase 3
randomized clinical trial. JAMA Oncol. 4:1569–1575. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Yang JJ, Chen HJ, Yan HH, Zhang XC, Zhou
Q, Su J, Wang Z, Xu CR, Huang YS, Wang BC, et al: Clinical modes of
EGFR tyrosine kinase inhibitor failure and subsequent management in
advanced non-small cell lung cancer. Lung Cancer. 79:33–39. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
da Cunha Santos G, Shepherd FA and Tsao
MS: EGFR mutations and lung cancer. Annu Rev Pathol. 6:49–69. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Tomas A, Futter CE and Eden ER: EGF
receptor trafficking: Consequences for signaling and cancer. Trends
Cell Biol. 24:26–34. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Mok TS, Wu YL, Ahn MJ, Garassino MC, Kim
HR, Ramalingam SS, Shepherd FA, He Y, Akamatsu H, Theelen WSME, et
al: Osimertinib or platinum-pemetrexed in EGFR T790M-positive lung
cancer. N Engl J Med. 376:629–640. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Wu SG and Shih JY: Management of acquired
resistance to EGFR TKI-targeted therapy in advanced non-small cell
lung cancer. Mol Cancer. 17:382018. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Apte RS, Chen DS and Ferrara N: VEGF in
signaling and disease: Beyond discovery and development. Cell.
176:1248–1264. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Manzo A, Montanino A, Carillio G, Costanzo
R, Sandomenico C, Normanno N, Piccirillo MC, Daniele G, Perrone F,
Rocco G and Morabito A: Angiogenesis inhibitors in NSCLC. Int J Mol
Sci. 18:20212017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yu HA, Schoenfeld AJ, Makhnin A, Kim R,
Rizvi H, Tsui D, Falcon C, Houck-Loomis B, Meng F, Yang JL, et al:
Effect of osimertinib and bevacizumab on progression-free survival
for patients with metastatic EGFR-mutant lung cancers: A phase 1/2
single-group open-label trial. JAMA Oncol. 6:1048–1054. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Zhou Q, Xu CR, Cheng Y, Liu YP, Chen GY,
Cui JW, Yang N, Song Y, Li XL, Lu S, et al: Bevacizumab plus
erlotinib in Chinese patients with untreated, EGFR-mutated,
advanced NSCLC (ARTEMIS-CTONG1509): A multicenter phase 3 study.
Cancer Cell. 39:1279–1291. e32021. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hata A, Katakami N, Kaji R, Yokoyama T,
Kaneda T, Tamiya M, Inoue T, Kimura H, Yano Y, Tamura D, et al:
Afatinib plus bevacizumab combination after acquired resistance to
EGFR tyrosine kinase inhibitors in EGFR-mutant non-small cell lung
cancer: Multicenter, single-arm, phase 2 trial (ABC Study). Cancer.
124:3830–3838. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Li F, Zhu T, Cao B, Wang J and Liang L:
Apatinib enhances antitumour activity of EGFR-TKIs in non-small
cell lung cancer with EGFR-TKI resistance. Eur J Cancer.
84:184–192. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zhang C, Cao H, Cui Y, Jin S, Gao W, Huang
C and Guo R: Concurrent use of anlotinib overcomes acquired
resistance to EGFR-TKI in patients with advanced EGFR-mutant
non-small cell lung cancer. Thorac Cancer. 12:2574–2584. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Lian Z, Du W, Zhang Y, Fu Y, Liu T, Wang
A, Cai T, Zhu J, Zeng Y, Liu Z and Huang JA: Anlotinib can overcome
acquired resistance to EGFR-TKIs via FGFR1 signaling in non-small
cell lung cancer without harboring EGFR T790M mutation. Thorac
Cancer. 11:1934–1943. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Li T, Qian Y, Zhang C, Uchino J, Provencio
M, Wang Y, Shi X, Zhang Y and Zhang X: Anlotinib combined with
gefitinib can significantly improve the proliferation of epidermal
growth factor receptor-mutant advanced non-small cell lung cancer
in vitro and in vivo. Transl Lung Cancer Res. 10:1873–1888. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Wang W, Shao L, Xu Y, Song Z, Lou G, Zhang
Y and Chen M: Efficacy and safety of anlotinib with and without
EGFR-TKIs or immunotherapy in the treatment of elder patients with
non-small-cell lung cancer: A retrospective study. BMC Pulm Med.
22:1792022. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Chu T, Zhong R, Zhong H, Zhang B, Zhang W,
Shi C, Qian J, Zhang Y, Chang Q, Zhang X, et al: Phase 1b study of
sintilimab plus anlotinib as first-line therapy in patients with
advanced NSCLC. J Thorac Oncol. 16:643–652. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Barron F, Cardona AF, Corrales L,
Ramirez-Tirado LA, Caballe-Perez E, Sanchez G, Flores-Estrada D,
Zatarain-Barrón ZL and Arrieta O; Latin American Consortium for the
Study of Lung Cancer (CLICaP), : Characteristics of progression to
tyrosine kinase inhibitors predict overall survival in patients
with advanced non-small cell lung cancer harboring an EGFR
mutation. J Thorac Dis. 10:2166–2178. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Otsuka K, Hata A, Takeshita J, Okuda C,
Kaji R, Masago K, Fujita S and Katakami N: EGFR-TKI rechallenge
with bevacizumab in EGFR-mutant non-small cell lung cancer. Cancer
Chemother Pharmacol. 76:835–841. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Cui Q, Hu Y, Cui Q, Wu D, Mao Y, Ma D and
Liu H: Osimertinib rechallenge with bevacizumab vs. chemotherapy
plus bevacizumab in EGFR-mutant NSCLC patients with osimertinib
resistance. Front Pharmacol. 12:7467072021. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Wedding U, Honecker F, Bokemeyer C,
Pientka L and Hoffken K: Tolerance to chemotherapy in elderly
patients with cancer. Cancer Control. 14:44–56. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Robinson L and Xavier NA: Managing older
patients with cancer. JAAPA. 33:31–34. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Tan AC and Tan DSW: Targeted therapies for
lung cancer patients with oncogenic driver molecular alterations. J
Clin Oncol. 40:611–625. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Imyanitov EN, Iyevleva AG and Levchenko
EV: Molecular testing and targeted therapy for non-small cell lung
cancer: Current status and perspectives. Crit Rev Oncol Hematol.
157:1031942021. View Article : Google Scholar : PubMed/NCBI
|