Introduction
Brain metastases (BMs) are the most common type of
tumor in the central nervous system in adults, occurring in ~20% of
malignant tumors (1). BMs are most
common in patients with lung cancer compared with other types of
cancer and lung cancer is responsible for ~50% of all BM cases
worldwide, which poses a threat to the improvement and
effectiveness of oncological treatment (2). In addition to traditional methods such
as chemotherapy, radiation therapy, surgery and molecularly
targeted therapy that have been used in the past, emerging
immunotherapeutic agents, such as checkpoint inhibitors, are also
demonstrating promising therapeutic results in the treatment of
lung cancer BMs (3). The
development of immune checkpoint inhibitor (ICI) therapy, such as
anti-programmed cell death-ligand 1 (PD-L1) therapy, has been
reported to be effective in numerous types of cancer, including
non-small cell lung cancer and small cell lung cancer (4). In addition, ICI therapies have been
evaluated in patients receiving combination therapy, especially
radiotherapy. The results obtained from clinical trials provide
evidence supporting the safety and efficacy of radiotherapy in
combination with anti-PD-1/PD-L1 treatment, which could be more
effective than monotherapy (5).
Magnetic resonance imaging (MRI) is the most commonly used modality
to investigate radionecrosis (RN) (6). However, the imaging features of RN and
tumor recurrence overlap considerably, with both entities
demonstrating a degree of contrast enhancement and perilesional
edema (7,8). Accordingly, a range of clinical and
imaging strategies are being developed to evaluate tumor responses
and to rule out pseudo-progression or RN. An accurate differential
diagnosis is required for decision-making in the management of
patients.
Case report
A 61-year-old female patient with stage IV
adenocarcinoma of the lung was initially admitted to Suning County
People's Hospital (Cangzhou, China) with a 6-month history of a
dull headache and left upper limb weakness in December 2020. In
Suning County People's Hospital, the patient ordered a service to
perform next-generation sequencing (NGS) and PD-L1
immunohistochemistry (Topgen-Biopharm). The NGS was performed using
an OncoDrug-Seq™ kit (Topgen-Biopharm) for a panel of 33
tumor-targeting genes and was performed on the NextSeq500 system
(Illumina, Inc.). The lung cancer samples were fixed with 10%
formalin at room temperature for 24 h and 4-µm paraffin-embedded
samples were used for PD-L1 immunohistochemistry. Rabbit anti-human
monoclonal antibodies to PD-L1 (1:50; cat. no. ab205921; Abcam)
were used. Briefly, sections were dewaxed, dehydrated with a series
of alcohol (70, 80 and 95%) at room temperature (1 h for each
alcohol concentration) and the tissues were then placed in toluene
for 30 min at room temperature for deparaffinization. After
neutralization of endogenous peroxidase with 3%
H2O2 at room temperature for 15 min and
microwave antigen retrieval (800 W in 0.01 M citrate buffer pH 6),
slides were preincubated with 5% bovine serum albumin blocking
buffer (Thermo Fisher Scientific, Inc.) for 1 h at room temperature
and then incubated overnight with monoclonal antibodies at 4°C.
Subsequently, the sections were serially rinsed, incubated with
Goat anti-Rabbit IgG H&L (HRP) secondary antibodies (1:200;
cat. no. ab97051; Abcam) and avidin-biotinylated peroxidase complex
for 1 h at 37°C, and again washed for 10 min with PBS at 37°C.
Nuclear counterstaining was performed with DAPI (cat. no. C1005;
Beyotime Institute of Biotechnology) at room temperature for 5 min.
The immunohistochemistry images were obtained using a light
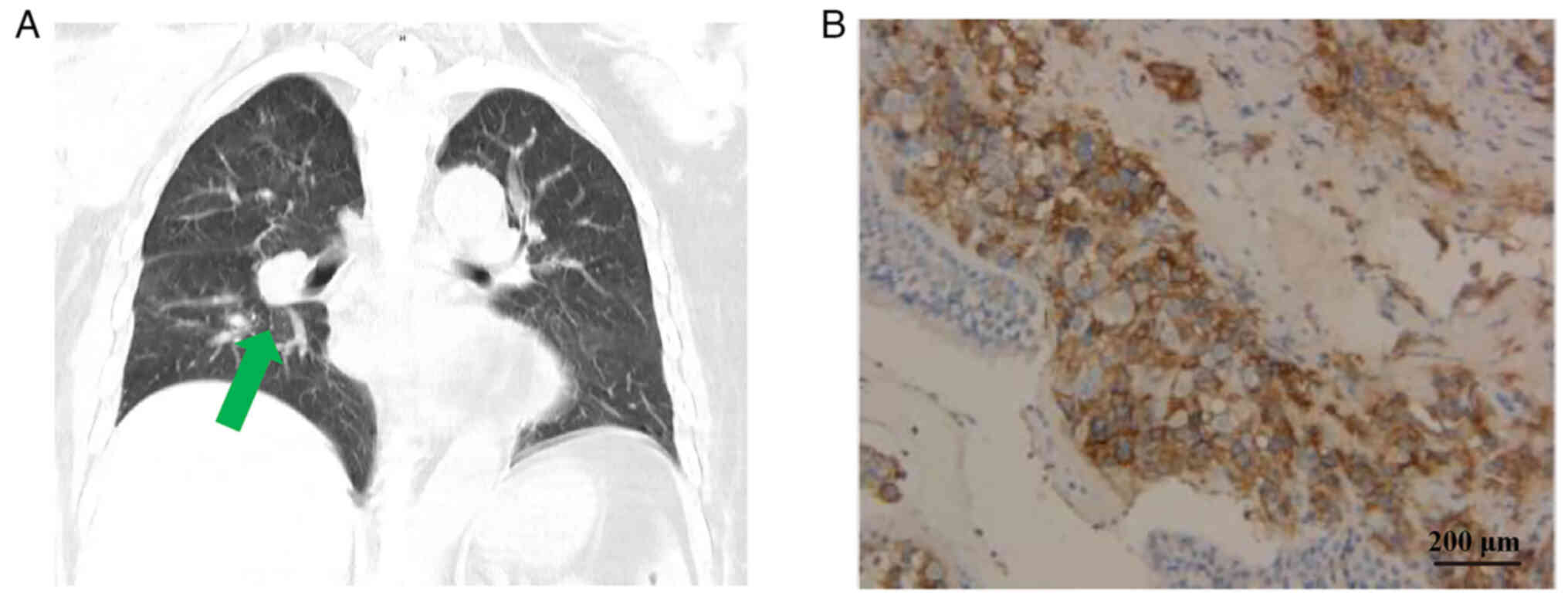
microscope. The results of immunohistochemistry indicated PD-L1
positivity (Fig. 1).
Based on these results, the patient decided to
undergo further clinical treatment at the Department of Oncology of
the Affiliated Hospital of Hebei University (Hebei, China). An
initial computed tomography scan in the Affiliated Hospital of
Hebei University revealed that the patient presented with a
space-occupying lesion in the superior lobe of the right lung, with
multiple bilateral pulmonary nodules and with masses in the
mediastinal lymph nodes and liver. Brain MRI revealed a
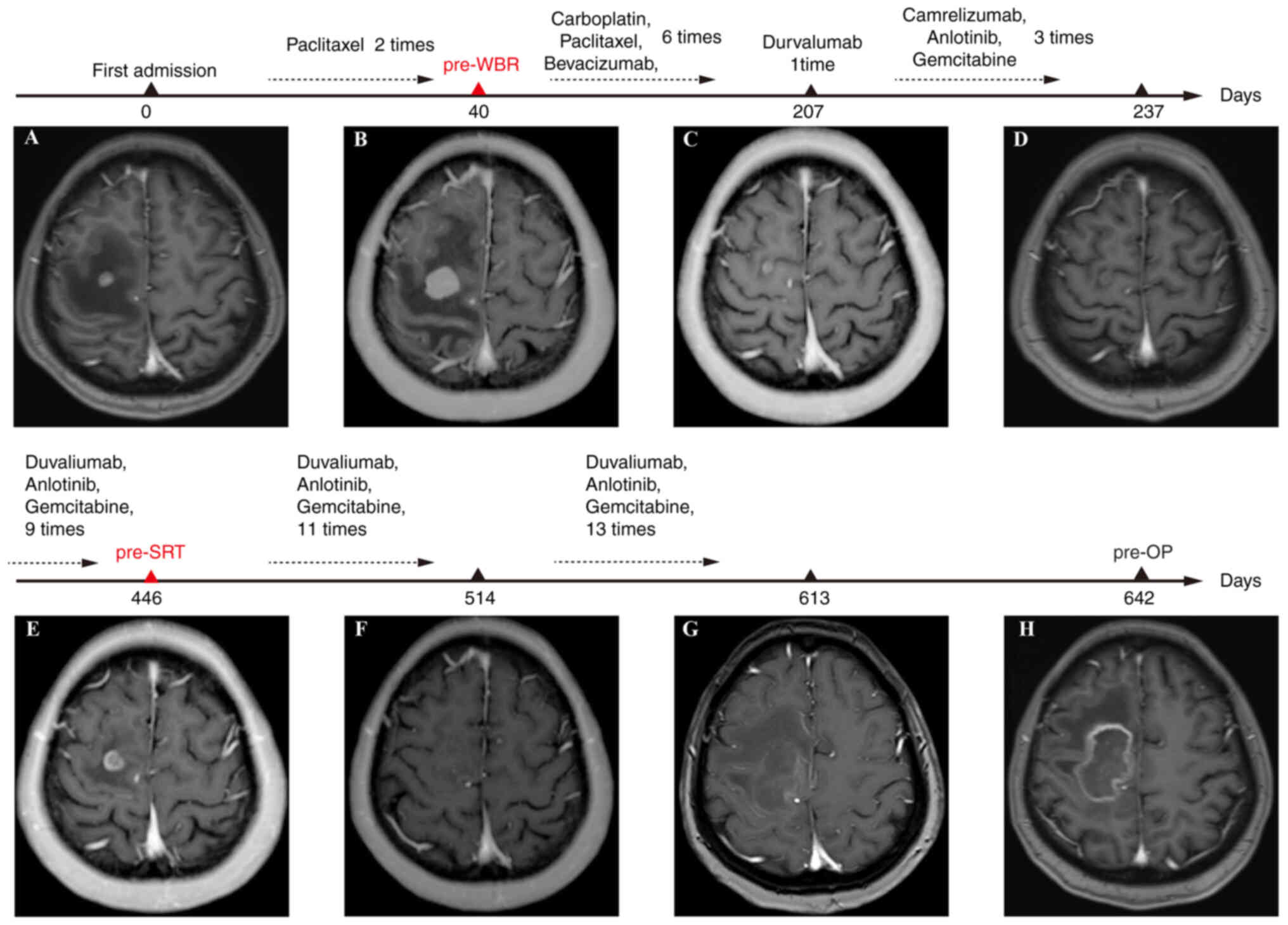
space-occupying lesion in the frontal parietal lobe (Fig. 2A). The patient received single-agent
paclitaxel therapy for 2 cycles (intravenously; 135
mg/m2, 3 weeks per cycle). On routine reexamination, MRI
revealed an enlarged space-occupying lesion (Fig. 2B). The patient was then treated with
direct tomotherapy (planning target volume, 36 Gy/3 Gy/12 fx).
Bevacizumab (intravenously, 15 mg/kg) and paclitaxel
(intravenously, 175 mg/m2)-carboplatin (intravenously, 5
mg) chemotherapy was used for 6 cycles (21 days per cycle), which
demonstrated regression in BM (Fig.
2C). However, new extrapulmonary metastases in the pancreas,
kidney and ovaries were detected. Based on the results of the PD-L1
immunohistochemistry, the PD-L1 inhibitor, durvalumab
(intravenously, 20 mg/kg), and systemic chemotherapy (camrelizumab
(intravenously, 20 mg) plus anlotinib (orally, 12 mg) and
gemcitabine (intravenously, 1,000 mg/m2) for 3 cycles
and duvaliumab (intravenously, 10 mg/kg) plus anlotinib (orally, 12
mg) and gemcitabine (intravenously, 1,000 mg/m2) for 9
cycles (21 days per cycle) were administered to the patient
(Fig. 2D). However, the progression
of BM prompted stereotactic radiotherapy (SRT) with 12 Gy
radiosurgical volume (Fig. 2E).
Therapy with a combination of anlotinib (orally, 12 mg) and
gemcitabine (intravenously, 1,000 mg/m2) was then
administered to the patient for 11 cycles (21 days per cycle).
Brain MRI revealed an abnormal signal (no enhancement) and
intracranial nodular enlargement (Fig.
2F). After 13 cycles of treatment with anlotinib and
gemcitabine, brain MRI demonstrated an enlarged nodule with strong
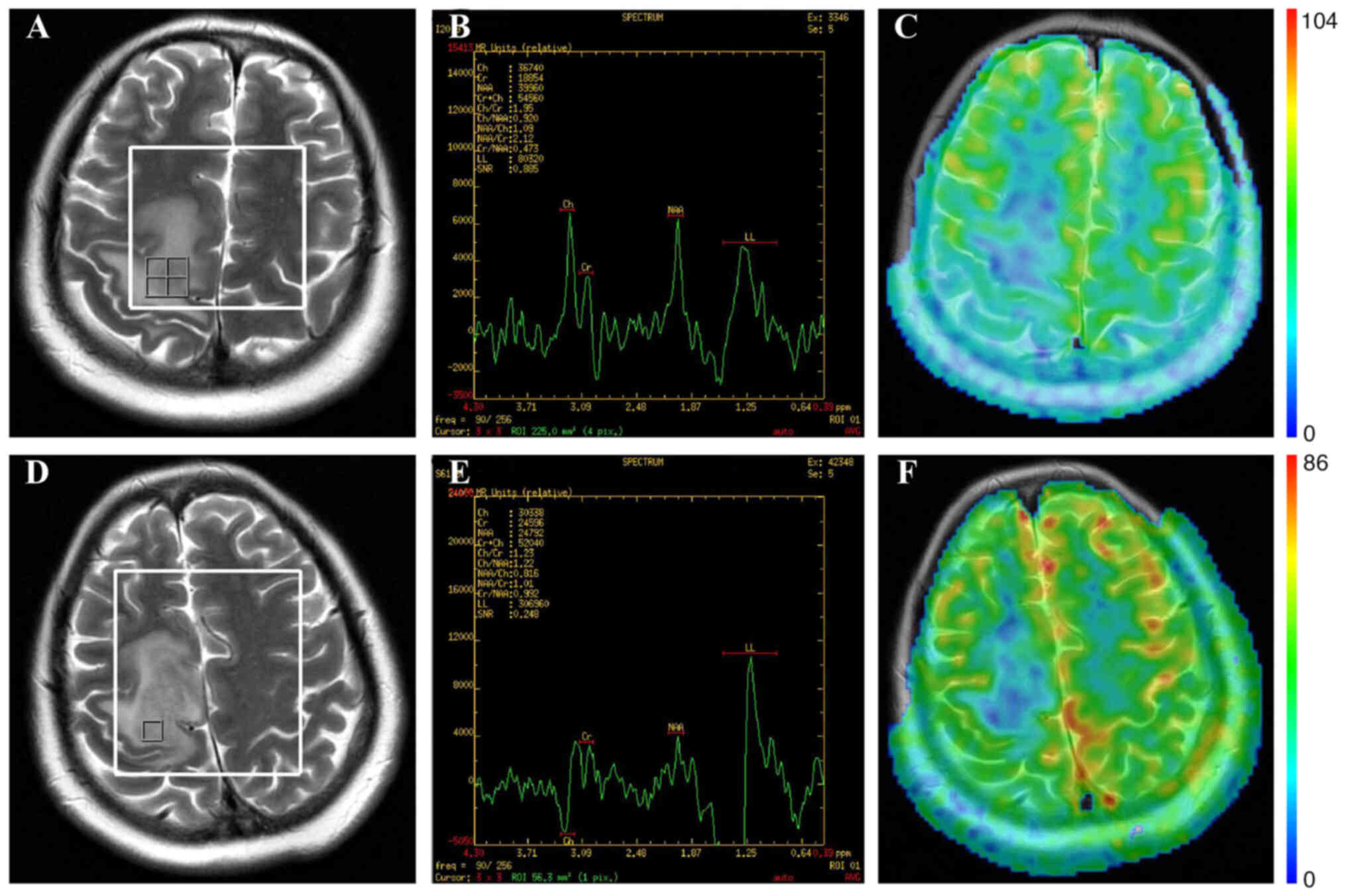
enhancement (Fig. 2G and H). Before
SRT, magnetic resonance spectroscopy (MRS) was performed. The
results suggested pseudo-progression with
choline/N-acetyl-aspartate ratio (Cho/NAA) 0.92, choline/creatine
ratio (Cho/Cr) 1.95 and N-acetyl-aspartate/creatine ratio (NAA/Cr)
2.12. In the contralateral normal brain tissue, the metabolite
ratios of Cho/NAA Cho/Cr and NAA/Cr were 0.672, 1.08 and 1.16,
respectively. Three-dimensional arterial spin labeling (3DASL) of
the brain revealed low perfusion in the intracranial nodule
(Fig. 3A-C). Before the surgical
operation, the patients had another MRS scan and the results
suggested RN with Cho/NAA 1.54, Cho/Cr 1.79 and NAA/Cr 1.16. In the
contralateral normal brain tissue, the metabolite ratios of Cho/NAA
Cho/Cr and NAA/Cr were 0.537, 0.904 and 1.68, respectively. The
3DASL of the brain also revealed low perfusion in the intracranial
nodule (Fig. 3D-F). The patient
decided to undergo surgical treatment at the Department of
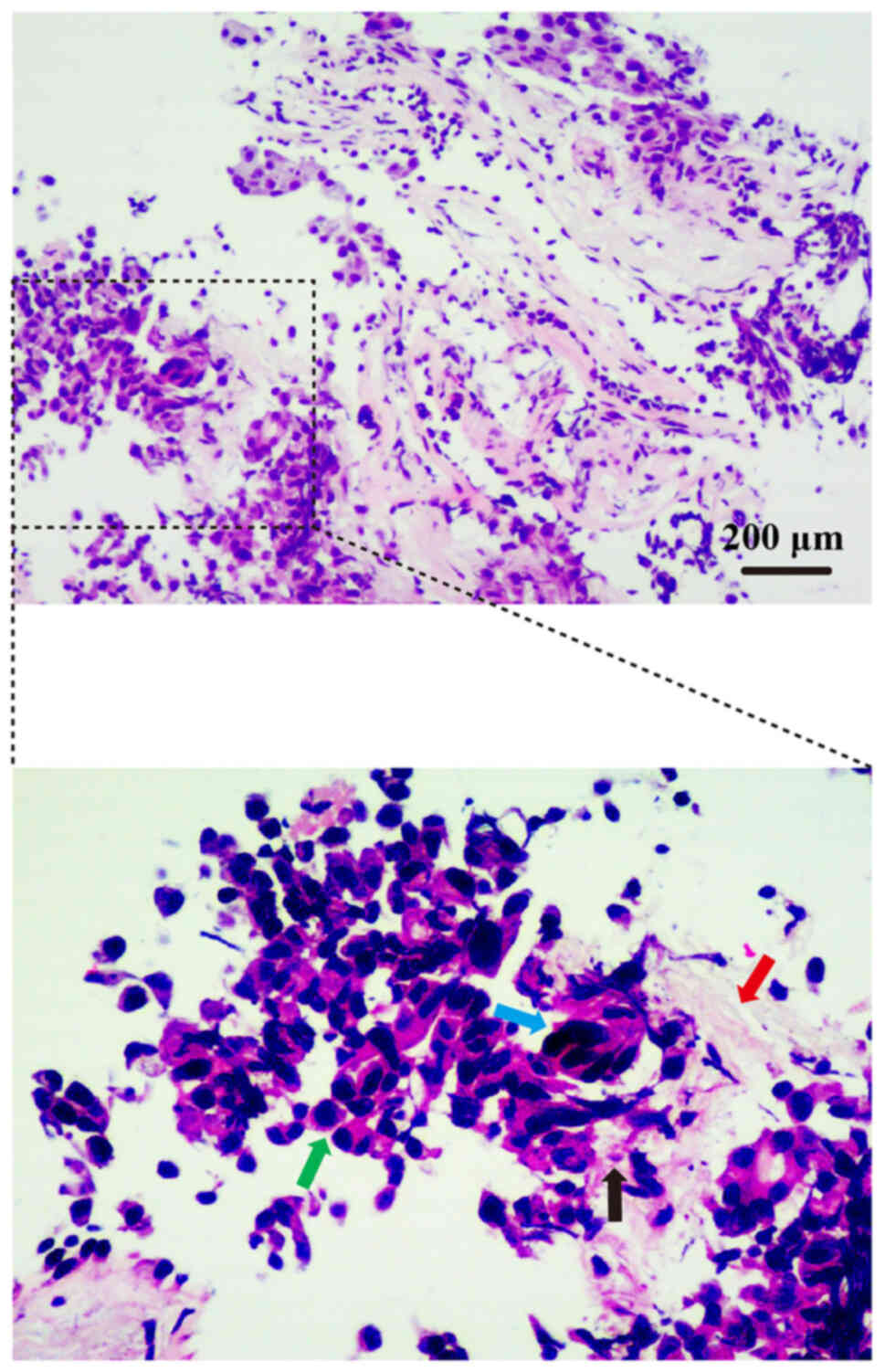
Neurosurgery of the Affiliated Hospital of Hebei University. The
progressive BM was surgically removed and subjected to
neuropathological examination. The brain tumor tissue was fixed
with 10% buffered formalin at 37°C for 8–10 min. Subsequently,
sections (5 µm) were cut from paraffin blocks and stained with
hematoxylin and eosin at room temperature for 5 min (cat. no.
C0105M; Beyotime Institute of Biotechnology), and DAPI for
histopathological examination under a light microscope (Leica
DM4000 M; Leica Microsystems GmbH). Histopathological analysis
revealed RN with no evidence of metastatic lung cancer (Fig. 4).
Discussion
The present case demonstrated the side effects of
the concurrent use of radiotherapy and anti-PD-L1 inhibitors in
patients with BM. The principle of anti-programmed cell death
protein 1 (PD-1)/PD-L1 therapy is to block the negative regulatory
process of the PD-1/PD-L1 signaling pathway on T-cell activation
and proliferation by inhibiting the complex formed by PD-1 and its
ligand, PD-L1. Thus, T cells gradually recover immune activity by
reactivation of the recognition and necrotic function of tumor
cells (9). PD-1/PD-L1 inhibitors
combined with radiotherapy mediate the antitumor effect in the
dynamic interaction between effector cells and regulatory cells,
such as CD8-positive T cells and tumor-infiltrating Tregs (10). In a previous study, melanoma tumors
were irradiated with 10 Gy radiation; after tumor radiation, two
important co-stimulatory molecules, CD86 and CD70, were revealed to
be substantially upregulated on dendritic cells, which serve an
important role in T-cell-mediated immune responses (11). Radiotherapy can regulate the
expression of immune checkpoints, affect the expression levels of
cytokines and promote the antitumor effects of immune drugs.
Evidence has shown that several inflammatory cytokines, including
tumor necrosis factor α, interleukin 1 and interleukin 2 can be
upregulated by radiation therapy, which may be caused by an
acute-phase inflammatory response (12). Conversely, radiation therapy can
lead to substantial increases in the immunosuppressive cytokine
transforming growth factor β in in response to cell death and
stress, which have important roles in dampening radiation-induced
immune responses (13).
Inflammatory cytokines released from the irradiated tissue and the
upregulation of checkpoint ligands can prevent autoimmune responses
against healthy and malignant cells. In one study,
radiation-induced upregulation of PD-L1 on the surface of tumor
cells was shown to be dependent on interferon γ derived from CD8 T
cells (14). In contrast,
PD-1/PD-L1 inhibitors can promote radiotherapeutic effects by
inhibition of negative immune-regulatory cells or molecules
(15–17). For example, a previous study have
showed that PD-1/PD-L1 monoclonal antibody could restore T-cell
activity, reduce Treg numbers and increase CD8+T/Treg
ratio, thus enhancing tumor cell death (18). A case-control trial with 93 patients
by Trommer et al (19)
suggested that the use of PD-1 inhibitors combined with
radiotherapy had benefits and could improve overall survival rates.
However, with the wide application of combination therapy in
clinical practice, an increasing number of studies have reported
adverse reactions after the use of PD-1/PD-L1 inhibitors (20–22). A
previous study indicated that anti-PD-1 therapy could increase the
risk of RN when combined with radiotherapy (23). The present case highlights the
difficulty in differentiating between RN and pseudo-progression,
following sequential treatment with PD-1/PD-L1 inhibitors and
radiotherapy.
In the present case, the patient also received
bevacizumab. Bevacizumab, a recombinant human monoclonal antibody,
binds vascular endothelial growth factor (VEGF) and prevents VEGF
from binding its receptors (VEGFR-1 and kinase insert domain
receptor) on the endothelial cell surface, which serves a role in
pruning blood vessels, regulating vascular permeability, reducing
brain edema caused by brain necrosis and treating brain necrosis
(24). In 2007, Gonzalez et
al (25) first reported using
bevacizumab to treat radiation brain necrosis. At present, clinical
studies have proven the clinical efficacy of bevacizumab. For
example, Dashti et al (26)
reported that a single low-dose targeted bevacizumab infusion
resulted in durable clinical and imaging improvements in 80% of
patients. Another randomized double-blind study with 14 patients
also supported consideration of this treatment option for patients
with RN (27). At present, the
majority of patients respond well to bevacizumab. However, the
effect of bevacizumab on RN could not be ruled out in the present
case. Jeyaretna et al (28)
reported an exacerbation of cerebral RN by bevacizumab, which could
lead to the hypothesis that initial treatment with bevacizumab
might result in a reduction in cerebral edema. However, prolonged
treatment might result in the over-pruning of at-risk blood vessels
within the radiation field. The underlying mechanisms of
bevacizumab-induced enlargement of RN remains unclear. At present,
the duration, optimal dose and dosing interval of bevacizumab,
require further evaluation.
A previous study has reported that the incidence of
radiation-induced brain necrosis in patients with melanoma brain
metastasis treated with SRT combined with PD-L1 immunotherapy was
increased in a retrospective analysis of patients with melanoma
treated with SRT (29). The study
by Pires da Silva et al (30) followed-up 135 patients with melanoma
that received radiotherapy combined with PD-L1 immunotherapy for an
average of 23.6 months and revealed reported the probability of RN
was 17% along with a cumulative incidence rate of 18% in 2 years.
Furthermore, it was proposed that the time of occurrence of
RN-associated symptoms was similar to the time of occurrence of
radiological abnormalities (30).
It has been previously reported that the rate of RN was increased
with the addition of concurrent systemic therapies to SRT and whole
brain radiotherapy (WBRT) (Table I)
(30–35). A corresponding increase in RN was
not reported in patients treated with concurrent therapies and SRT
alone. The present case is consistent with the findings of a
previous study (30), suggesting
that anti-PD-1 therapy may increase the risk of RN when combined
with radiotherapy. In the present case, the patient received the
PD-L1 inhibitor duvaliumab and SRT. Approximately 3 months
following the combined therapy, the brain MRI indicated an abnormal
signal (no enhancement), and ~7 months later, the intracranial
nodule was enlarged. MRS suggested RN. The 3DASL of the brain also
indicated low perfusion in the intracranial nodule. Pathological
examination also indicated RN. Numerous previous studies have
reported that SRT combined with immunotherapy increased the risk of
radiation necrosis (31,36,37).
Therefore, the concern regarding the potential risk of RN following
SRT combined with PD-L1 immunotherapy has increased. Numerous
previous studies have reported that PD-L1 immunotherapy combined
with brain radiotherapy is effective and feasible. However, due to
the potential of adverse reactions, the sequence, dosage and volume
should be strictly controlled during the combined treatment, and
imaging should be closely monitored to reduce the occurrence of
adverse reactions such as RN. In the present case, it was
demonstrated that the size of the intracranial nodules gradually
decreased. After SRT, brain MRI indicated an abnormal signal
(without enhancement), and that the intracranial nodule was
enlarged. At this stage, it was not easy to differentially diagnose
RN from tumor recurrence because of their shared clinical symptoms
such as symptoms of increased intracranial pressure and/or
seizures, and conventional imaging and pathological biopsy are
still the best methods for differential diagnosis. However, it is
difficult to perform surgery in the early clinical stage.
Therefore, dynamic MRI sequence monitoring is often used to confirm
the diagnosis in the clinic. In the early stages, traditional
imaging of RN and tumor progression may demonstrate contrast
enhancement on MRI, and large edema zones are usually observed
around the lesions. In the long-term follow-up, RN indicated a
decrease in tumor volume, while tumor progression indicated an
increase in tumor volume (38–40).
In these patients, the T2-weighted image margin ‘mismatched’ the
contrast-enhanced T1-weighted image margin. When the lesion appears
indistinct on T2, the histology usually indicated necrosis and
contrast enhancement when the contrast-enhanced rim on the
T1-weighted image is associated with a distinct border on T2, and
the pathology was usually a recurrent tumor (39). MRI findings of RN are often
described as ‘Swiss cheese’ or ‘soap bubble’ lesions (40). At present, RN, tumor
pseudo-progression and tumor recurrence have different treatment
strategies. Pseudo-progression is defined as a radiographic
increase in enhancement and/or edema on MRI without tumor
progression. This transient increase in enhancement and/or edema
exhibits spontaneous recovery, which usually occurs within a few
weeks or months after the onset of pseudo-progression (41). Tumor recurrence may require surgical
intervention. For RN, therapy involves corticosteroids, bevacizumab
or surgical intervention (42). It
is difficult to distinguish between RN, tumor pseudo-progression
and tumor recurrence using conventional structural MRI at an early
stage. Currently, regional cerebral blood volume and amino acid
positron emission computed tomography (PET) are used to
differentiate the diagnosis of these conditions. The most common
imaging marker of RN in conventional MRI is the ‘Swiss cheese’
pattern with diffuse enhancements at the margins between the cortex
and white matter (43). In the
present case, these features were not apparent on enhanced MRI.
Therefore, it was suspected that the local tumor had recurred.
However, bevacizumab treatment might influence the results of MRS.
Pseudo-progression usually occurs 2–5 months after radiotherapy, is
self-limiting and curable. Post-radiation damage occurs after a
delay of >6 months from the time of radiation and consists
principally of necrosis caused by blood-brain barrier (BBB)
disruption and radiation-induced demyelination leading to white
matter injury (44). RN involves a
space-occupying necrotic lesion with a mass effect and neurological
dysfunction (45). It is not a
self-limiting disease and therefore requires specialized treatment
(46).
 | Table I.Reported rates of radiation necrosis
with anti-PD-1 therapy combined with radiation therapy. |
Table I.
Reported rates of radiation necrosis
with anti-PD-1 therapy combined with radiation therapy.
| First author,
year | Histology | Cases, n | Systemic
treatment | Radiation necrosis
rate (%) | (Refs.) |
|---|
| Pires da Silva
et al, 2019 | Melanoma | 137 | Anti-CTLA4,
anti-PD-1 and all patients received immunotherapy combined with
radiotherapy | 27 | (30) |
| Kim et al,
2017 | Melanoma | 135 | Radiotherapy and
anti-PD-1 therapy | 17 | (31) |
| Colaco et
al, 2016 | Melanoma, lung,
breast, renal and colorectal cancer | 42/180 received
immunotherapy | Anti-CTLA4,
anti-PD-1 and all patients received immunotherapy combined with
radiotherapy | 37.5 with
immunotherapy only | (32) |
| Martin et
al, 2018 | Melanoma and lung
cancer | 115 | Immune checkpoint
inhibitors therapy combined with radiotherapy | 20 | (33) |
| Weingarten et
al, 2019 | Melanoma,
renal-cell carcinoma, lung and breast cancer | 57 | Immunotherapy
combined with radiotherapy | 7 | (34) |
| Andring et
al, 2023 | Melanoma and lung
cancer | 63 | Anti-CTLA4,
anti-PD-1 and radiotherapy | 22 | (35) |
Generally, MRS could not be used to obtain an
affirmative conclusion to diagnose ‘pseudo-progression’ or ‘RN’.
One of the main challenges for neurosurgeons or treating clinicians
is to make a differential diagnosis of either tumor recurrence, RN
or pseudo-progression in clinical settings. Even with improving
neuroimaging methods or different diagnostic imaging modalities,
such as diffusion-weighted imaging/diffusion tensor imaging, MRS
and PET/single photon emission computed tomography, it is still
challenging (47). MRS is a
metabolic imaging technique that could provide value in
differentiating pseudo-progression from recurrent tumors by
identifying specific metabolites within the tumor that are present
during active tumor growth (48).
Previous studies have reported increased total choline levels in
recurrent disease and reduced choline levels in tumors which
exhibited pseudo-progression (49,50).
Tumor recurrence has been reported to show higher Cho/Cr and
Cho/NAA values compared with those of RN (51,52).
In the present case, bevacizumab treatment might have influenced
the results of MRS. Previous studies have reported that bevacizumab
treatment could impact tumor energy and membrane metabolism, which
resulted in increased intracellular pH and a decrease in the ratio
of phosphatidylcholine to glycerophosphocholine or Cho/NAA values
(53,54). However, in the present study, this
finding was confirmed using histological examination. In the
present case, there was a longitudinal change in the MRI of RN
following SRT and anti-PD-L1 combined therapy. Dynamic changes in
RN on enhanced MRI was demonstrated. By employing longitudinal MRI,
the present case revealed atypical images of RN. These
treatment-associated imaging changes were necessary for clinicians
to make an accurate preoperative diagnosis in this case.
However, the exact molecular mechanism of
SRT-induced RN is still unclear and has not been fully elucidated.
Evidence has indicated that high-dose SRT can damage the vascular
endothelium by destroying the BBB on a large scale, leading to
intracranial vasogenic edema and then further to ischemia of the
surrounding brain tissue (55).
Furthermore, this leads to an increase in the levels of hypoxia
inducible factor-1A and VEGF and finally leads to infarction and
necrosis of the brain parenchyma. A previous study indicated that
RN is associated with abnormalities in vascular structures,
including telangiectasia, hyaline thickening of vessels and
fibrinoid necrosis with intravascular thromboses (56). The expression of VEGF promotes these
abnormalities in newly formed vascular structures, increases the
brittleness and permeability of vascular structures, and increases
edema around the lesion (57).
Certain scholars have proposed that radiation damage occurs through
the combination of demyelination and vascular abnormalities
(35,58). In the penumbra around the necrotic
nucleus, astrocytes, microglia and oligodendrocytes produce factors
(e.g. VEGF) that promote cytokine release and increase the
permeability of the BBB (37).
However, the mechanisms by which the combination of anti-PD-L1 and
radiotherapy promotes RN are still unclear. The main limitation of
the present case report is that the patient received multiple
different agents. As well as radiotherapy and anti-PD-1 therapy,
the patient also received chemotherapy; therefore, the role of
chemotherapy in the formation of RN could not be ruled out. The
effect of bevacizumab on RN is uncertain. In the present case, it
was hypothesized that neurological symptoms and radiologically
suspected radioactive brain necrosis and tumor progression may
occur after 7 months of treatment with a PD-L1 inhibitor and 2
months of treatment with SRT. The side effects of WBRT in the early
stage are uncertain, and, to the best of our knowledge, there is
not any literature which clearly reports that the simultaneous
application of anlotinib and gemcitabine can increase the
probability of radioactive brain necrosis.
In conclusion, the present study reported a case of
RN following sequential PD-1/PD-L1-directed immunotherapy, WBRT and
SRT. RN mimicked cancer progression with enlarged intracranial
nodules. For the first time, the present study demonstrated the
dynamic changes in RN on enhanced MRI.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
XJ, LW, YT, YS, RH, CF, CL and LZ participated in
the conception, design and data acquisition for the paper. XJ and
LW participated in drafting and revising the manuscript. LZ
critically revised the paper. LW ensured that questions related to
the integrity of any part of the work were appropriately
investigated and resolved. YT, YS, RH and CF confirm the
authenticity of all the raw data. All authors read and approved the
final version of the manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of anonymized data and any accompanying
images.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Achrol AS, Rennert RC, Anders C, Soffietti
R, Ahluwalia MS, Nayak L, Peters S, Arvold ND, Harsh GR, Steeg PS
and Chang SD: Brain metastases. Nat Rev Dis Primers. 5:52019.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rybarczyk-Kasiuchnicz A, Ramlau R and
Stencel K: Treatment of brain metastases of non-small cell lung
carcinoma. Int J Mol Sci. 22:5932021. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yang X, Zeng Y, Tan Q, Huang Z, Jia J and
Jiang G: Efficacy of PD-1/PD-L1 inhibitors versus chemotherapy in
lung cancer with brain metastases: A systematic review and
meta-analysis. J Immunol Res. 2022:45188982022. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Horn L, Mansfield AS, Szczęsna A, Havel L,
Krzakowski M, Hochmair MJ, Huemer F, Losonczy G, Johnson ML, Nishio
M, et al: First-line atezolizumab plus chemotherapy in
extensive-stage small-cell lung cancer. N Engl J Med.
379:2220–2229. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Takamori S, Toyokawa G, Takada K, Shoji F,
Okamoto T and Maehara Y: Combination therapy of radiotherapy and
anti-PD-1/PD-L1 treatment in non-small-cell lung cancer: A
mini-review. Clin Lung Cancer. 19:12–16. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Vellayappan B, Tan CL, Yong C, Khor LK,
Koh WY, Yeo TT, Detsky J, Lo S and Sahgal A: Diagnosis and
management of radiation necrosis in patients with brain metastases.
Front Oncol. 8:3952018. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Barajas RF, Chang JS, Sneed PK, Segal MR,
McDermott MW and Cha S: Distinguishing recurrent intra-axial
metastatic tumor from radiation necrosis following gamma knife
radiosurgery using dynamic susceptibility-weighted
contrast-enhanced perfusion MR imaging. AJNR Am J Neuroradiol.
30:367–372. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Forsyth PA, Kelly PJ, Cascino TL,
Scheithauer BW, Shaw EG, Dinapoli RP and Atkinson EJ: Radiation
necrosis or glioma recurrence: Is computer-assisted stereotactic
biopsy useful? J Neurosurg. 82:436–344. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Budimir N, Thomas GD, Dolina JS and
Salek-Ardakani S: Reversing T-cell exhaustion in cancer: Lessons
learned from PD-1/PD-L1 immune checkpoint blockade. Cancer Immunol
Res. 10:146–153. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Gong X, Li X, Jiang T, Xie H, Zhu Z, Zhou
F and Zhou C: Combined radiotherapy and anti-PD-L1 antibody
synergistically enhances antitumor effect in non-small cell lung
cancer. J Thorac Oncol. 12:1085–1097. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gupta A, Probst HC, Vuong V, Landshammer
A, Muth S, Yagita H, Schwendener R, Pruschy M, Knuth A and van den
Broek M: Radiotherapy promotes tumor-specific effector CD8+ T cells
via dendritic cell activation. J Immunol. 189:558–566. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hong JH, Chiang CS, Campbell IL, Sun JR,
Withers HR and McBride WH: Induction of acute phase gene expression
by brain irradiation. Int J Radiat Oncol Biol Phys. 33:619–626.
1995. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hong JH, Chiang CS, Tsao CY, Lin PY,
McBride WH and Wu CJ: Rapid induction of cytokine gene expression
in the lung after single and fractionated doses of radiation. Int J
Radiat Biol. 75:1421–1427. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Dovedi SJ, Adlard AL, Lipowska-Bhalla G,
McKenna C, Jones S, Cheadle EJ, Stratford IJ, Poon E, Morrow M,
Stewart R, et al: Acquired resistance to fractionated radiotherapy
can be overcome by concurrent PD-L1 blockade. Cancer Res.
74:5458–5468. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Luke JJ, Lemons JM, Karrison TG, Pitroda
SP, Melotek JM, Zha Y, Al-Hallaq HA, Arina A, Khodarev NN, Janisch
L, et al: Safety and clinical activity of pembrolizumab and
multisite stereotactic body radiotherapy in patients with advanced
solid tumors. J Clin Oncol. 36:1611–1618. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Theelen WSME, Peulen HMU, Lalezari F, van
der Noort V, de Vries JF, Aerts JGJV, Dumoulin DW, Bahce I,
Niemeijer AN, de Langen AJ, et al: Effect of pembrolizumab after
stereotactic body radiotherapy vs pembrolizumab alone on tumor
response in patients with advanced non-small cell lung cancer:
Results of the PEMBRO-RT phase 2 randomized clinical trial. JAMA
Oncol. 5:1276–1282. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Su Z, Zhou L, Xue J and Lu Y: Integration
of stereotactic radiosurgery or whole brain radiation therapy with
immunotherapy for treatment of brain metastases. Chin J Cancer Res.
32:448–466. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wen L, Tong F, Zhang R, Chen L, Huang Y
and Dong X: The research progress of PD-1/PD-L1 inhibitors
enhancing radiotherapy efficacy. Front Oncol. 11:7999572021.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Trommer M, Adams A, Celik E, Fan J, Funken
D, Herter JM, Linde P, Morgenthaler J, Wegen S, Mauch C, et al:
Oncologic outcome and immune responses of radiotherapy with
anti-PD-1 treatment for brain metastases regarding timing and
benefiting subgroups. Cancers (Basel). 14:12402022. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Antonia SJ, Villegas A, Daniel D, Vicente
D, Murakami S, Hui R, Yokoi T, Chiappori A, Lee KH, de Wit M, et
al: Durvalumab after chemoradiotherapy in stage III non-small-cell
lung cancer. N Engl J Med. 377:1919–1929. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ahn JS, Ahn YC, Kim JH, Lee CG, Cho EK,
Lee KC, Chen M, Kim DW, Kim HK, Min YJ, et al: Multinational
randomized phase III trial with or without consolidation
chemotherapy using docetaxel and cisplatin after concurrent
chemoradiation in inoperable stage III non-small-cell lung cancer:
KCSG-LU05-04. J Clin Oncol. 33:2660–2666. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Wozniak AJ, Moon J, Thomas CR Jr, Kelly K,
Mack PC, Gaspar LE, Raben D, Fitzgerald TJ, Pandya KJ and Gandara
DR: A pilot trial of cisplatin/etoposide/radiotherapy followed by
consolidation docetaxel and the combination of bevacizumab
(NSC-704865) in patients with inoperable locally advanced stage III
non-small-cell lung cancer: SWOG S0533. Clin Lung Cancer.
16:340–347. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mowery YM, Patel K, Chowdhary M, Rushing
CN, Roy Choudhury K, Lowe JR, Olson AC, Wisdom AJ, Salama JK, Hanks
BA, et al: Retrospective analysis of safety and efficacy of
anti-PD-1 therapy and radiation therapy in advanced melanoma: A
bi-institutional study. Radiother Oncol. 138:114–120. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zhuang H, Shi S, Yuan Z and Chang JY:
Bevacizumab treatment for radiation brain necrosis: Mechanism,
efficacy and issues. Mol Cancer. 18:212019. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gonzalez J, Kumar AJ, Conrad CA and Levin
VA: Effect of bevacizumab on radiation necrosis of the brain. Int J
Radiat Oncol Biol Phys. 67:323–326. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Dashti SR, Kadner RJ, Folley BS, Sheehan
JP, Han DY, Kryscio RJ, Carter MB, Shields LBE, Plato BM, La Rocca
RV, et al: Single low-dose targeted bevacizumab infusion in adult
patients with steroid-refractory radiation necrosis of the brain: A
phase II open-label prospective clinical trial. J Neurosurg.
137:1676–1686. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Levin VA, Bidaut L, Hou P, Kumar AJ, Wefel
JS, Bekele BN, Grewal J, Prabhu S, Loghin M, Gilbert MR and Jackson
EF: Randomized double-blind placebo-controlled trial of bevacizumab
therapy for radiation necrosis of the central nervous system. Int J
Radiat Oncol Biol Phys. 79:1487–1495. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Jeyaretna DS, Curry WT Jr, Batchelor TT,
Stemmer-Rachamimov A and Plotkin SR: Exacerbation of cerebral
radiation necrosis by bevacizumab. J Clin Oncol. 29:e159–e162.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Fang P, Jiang W, Allen P, Glitza I, Guha
N, Hwu P, Ghia A, Phan J, Mahajan A, Tawbi H and Li J: Radiation
necrosis with stereotactic radiosurgery combined with CTLA-4
blockade and PD-1 inhibition for treatment of intracranial disease
in metastatic melanoma. J Neurooncol. 133:595–602. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Pires da Silva I, Glitza IC, Haydu LE,
Johnpulle R, Banks PD, Grass GD, Goldinger SMA, Smith JL, Everett
AS, Koelblinger P, et al: Incidence, features and management of
radionecrosis in melanoma patients treated with cerebral
radiotherapy and anti-PD-1 antibodies. Pigment Cell Melanoma Res.
32:553–563. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Kim JM, Miller JA, Kotecha R, Xiao R,
Juloori A, Ward MC, Ahluwalia MS, Mohammadi AM, Peereboom DM,
Murphy ES, et al: The risk of radiation necrosis following
stereotactic radiosurgery with concurrent systemic therapies. J
Neurooncol. 133:357–368. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Colaco RJ, Martin P, Kluger HM, Yu JB and
Chiang VL: Does immunotherapy increase the rate of radiation
necrosis after radiosurgical treatment of brain metastases? J
Neurosurg. 125:17–23. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Martin AM, Cagney DN, Catalano PJ,
Alexander BM, Redig AJ, Schoenfeld JD and Aizer AA: Immunotherapy
and symptomatic radiation necrosis in patients with brain
metastases treated with stereotactic radiation. JAMA Oncol.
4:1123–1124. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Weingarten N, Kruser TJ and Bloch O:
Symptomatic radiation necrosis in brain metastasis patients treated
with stereotactic radiosurgery and immunotherapy. Clin Neurol
Neurosurg. 179:14–18. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Andring L, Squires B, Seymour Z, Fahim D,
Jacob J, Ye H, Marvin K and Grills I: Radionecrosis (RN) in
patients with brain metastases treated with stereotactic
radiosurgery (SRS) and immunotherapy. Int J Neurosci. 133:186–193.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Shaw E, Scott C, Souhami L, Dinapoli R,
Kline R, Loeffler J and Farnan N: Single dose radiosurgical
treatment of recurrent previously irradiated primary brain tumors
and brain metastases: final report of RTOG protocol 90–05. Int J
Radiat Oncol Biol Phys. 47:291–298. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Vaios EJ, Winter SF, Shih HA, Dietrich J,
Peters KB, Floyd SR, Kirkpatrick JP and Reitman ZJ: Novel
mechanisms and future opportunities for the management of radiation
necrosis in patients treated for brain metastases in the era of
immunotherapy. Cancers (Basel). 15:24322023. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Yaman E, Buyukberber S, Benekli M, Oner Y,
Coskun U, Akmansu M, Ozturk B, Kaya AO, Uncu D and Yildiz R:
Radiation induced early necrosis in patients with malignant gliomas
receiving temozolomide. Clin Neurol Neurosurg. 112:662–667. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Leeman JE, Clump DA, Flickinger JC, Mintz
AH, Burton SA and Heron DE: Extent of perilesional edema
differentiates radionecrosis from tumor recurrence following
stereotactic radiosurgery for brain metastases. Neuro Oncol.
15:1732–1738. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Smith EJ, Naik A, Shaffer A, Goel M, Krist
DT, Liang E, Furey CG, Miller WK, Lawton MT, Barnett DH, et al:
Differentiating radiation necrosis from tumor recurrence: A
systematic review and diagnostic meta-analysis comparing imaging
modalities. J Neurooncol. 162:15–23. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Le Fèvre C, Lhermitte B, Ahle G,
Chambrelant I, Cebula H, Antoni D, Keller A, Schott R, Thiery A,
Constans JM and Noël G: Pseudoprogression versus true progression
in glioblastoma patients: A multiapproach literature review: Part
1-molecular, morphological and clinical features. Crit Rev Oncol
Hematol. 157:1031882021. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Kano H, Kondziolka D, Lobato-Polo J, Zorro
O, Flickinger JC and Lunsford LD: T1/T2 matching to differentiate
tumor growth from radiation effects after stereotactic
radiosurgery. Neurosurgery. 66:486–491. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Kumar AJ, Leeds NE, Fuller GN, Van Tassel
P, Maor MH, Sawaya RE and Levin VA: Malignant gliomas: MR imaging
spectrum of radiation therapy- and chemotherapy-induced necrosis of
the brain after treatment. Radiology. 217:377–384. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Parvez K, Parvez A and Zadeh G: The
diagnosis and treatment of pseudoprogression, radiation necrosis
and brain tumor recurrence. Int J Mol Sci. 15:11832–11846. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Zikou A, Sioka C, Alexiou GA, Fotopoulos
A, Voulgaris S and Argyropoulou MI: Radiation necrosis,
pseudoprogression, pseudoresponse, and tumor recurrence: Imaging
challenges for the evaluation of treated gliomas. Contrast Media
Mol Imaging. 2018:68283962018. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Metaweh NAK, Azab AO, El Basmy AAH,
Mashhour KN and El Mahdy WM: Contrast-enhanced perfusion MR imaging
to differentiate between recurrent/residual brain neoplasms and
radiation necrosis. Asian Pac J Cancer Prev. 19:941–948.
2018.PubMed/NCBI
|
|
47
|
Miyatake SI, Nonoguchi N, Furuse M,
Yoritsune E, Miyata T, Kawabata S and Kuroiwa T: Pathophysiology,
diagnosis, and treatment of radiation necrosis in the brain. Neurol
Med Chir (Tokyo). 55 (Suppl 1):S50–S59. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Mayo ZS, Halima A, Broughman JR, Smile TD,
Tom MC, Murphy ES, Suh JH, Lo SS, Barnett GH, Wu G, et al:
Radiation necrosis or tumor progression? A review of the
radiographic modalities used in the diagnosis of cerebral radiation
necrosis. J Neurooncol. 161:23–31. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Zeng QS, Li CF, Liu H, Zhen JH and Feng
DC: Distinction between recurrent glioma and radiation injury using
magnetic resonance spectroscopy in combination with
diffusion-weighted imaging. Int J Radiat Oncol Biol Phys.
68:151–158. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Rock JP, Scarpace L, Hearshen D, Gutierrez
J, Fisher JL, Rosenblum M and Mikkelsen T: Associations among
magnetic resonance spectroscopy, apparent diffusion coefficients,
and image-guided histopathology with special attention to radiation
necrosis. Neurosurgery. 54:1111–1119. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Kamada K, Houkin K, Abe H, Sawamura Y and
Kashiwaba T: Differentiation of cerebral radiation necrosis from
tumor recurrence by proton magnetic resonance spectroscopy. Neurol
Med Chir (Tokyo). 37:250–256. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Shah R, Vattoth S, Jacob R, Manzil FF,
O'Malley JP, Borghei P, Patel BN and Curé JK: Radiation necrosis in
the brain: Imaging features and differentiation from tumor
recurrence. Radiographics. 32:1343–1359. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Hattingen E, Bähr O, Rieger J, Blasel S,
Steinbach J and Pilatus U: Phospholipid metabolites in recurrent
glioblastoma: In vivo markers detect different tumor phenotypes
before and under antiangiogenic therapy. PLoS One. 8:e564392013.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Hattingen E, Jurcoane A, Bähr O, Rieger J,
Magerkurth J, Anti S, Steinbach JP and Pilatus U: Bevacizumab
impairs oxidative energy metabolism and shows antitumoral effects
in recurrent glioblastomas: A 31P/1H MRSI and quantitative magnetic
resonance imaging study. Neuro Oncol. 13:1349–1363. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Turnquist C, Harris BT and Harris CC:
Radiation-induced brain injury: Current concepts and therapeutic
strategies targeting neuroinflammation. Neurooncol Adv.
2:vdaa0572020.PubMed/NCBI
|
|
56
|
Katsura M, Sato J, Akahane M, Furuta T,
Mori H and Abe O: Recognizing radiation-induced changes in the
central nervous system: Where to look and what to look for.
Radiographics. 41:224–248. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Nonoguchi N, Miyatake S, Fukumoto M,
Furuse M, Hiramatsu R, Kawabata S, Kuroiwa T, Tsuji M, Fukumoto M
and Ono K: The distribution of vascular endothelial growth
factor-producing cells in clinical radiation necrosis of the brain:
Pathological consideration of their potential roles. J Neurooncol.
105:423–431. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Yoshii Y: Pathological review of late
cerebral radionecrosis. Brain Tumor Pathol. 25:51–58. 2008.
View Article : Google Scholar : PubMed/NCBI
|