Introduction
Intraocular cancer metastasis is rare. The most
common site of intraocular metastasis is the uvea, which includes
the choroid, iris, and ciliary body. Choroidal metastases account
for 62–88% of intraocular metastases (1). In a study of 420 patients with uveal
metastases, the primary lesions were as follows: breast cancer
(47%), lung cancer (21%), liver cancer (14%), gastric cancer (9%),
and colorectal cancer (2%) (2).
Meanwhile, biliary tract caner is quite rare as a primary lesion of
intraocular metastasis. To date, there was only one case reported
in 2003 who had choroidal metastasis from cholangiocarcinoma
(3).
Several therapeutic options for intraocular
metastasis have been reported, including chemotherapy,
photocoagulation, radiation therapy, or enucleation. However, there
exist no data showing the survival advantage among them (4,5). Thus,
there is no consensus about the treatment modality for intraocular
metastasis in terms of survival, while preserving visual acuity and
keeping quality of life hold the priority in the treatment
selection.
Stereotactic radiotherapy (SRT) is a noninvasive
treatment modality, and potentially has advantage in preserving the
normal function compared with other invasive treatment methods
(6). Thus, SRT was initially
applied for focal intracranial vascular lesions and small neoplasms
(6). Recently, SRT has been applied
for the treatment of intraocular tumors considering the ability to
reduce tumor margins and to preserve critical normal structures
around the tumor (6). Herein, we
reported a case of choroidal metastasis from distal
cholangiocarcinoma, which was successfully treated utilizing SRT
without decreasing the visual acuity.
Case report
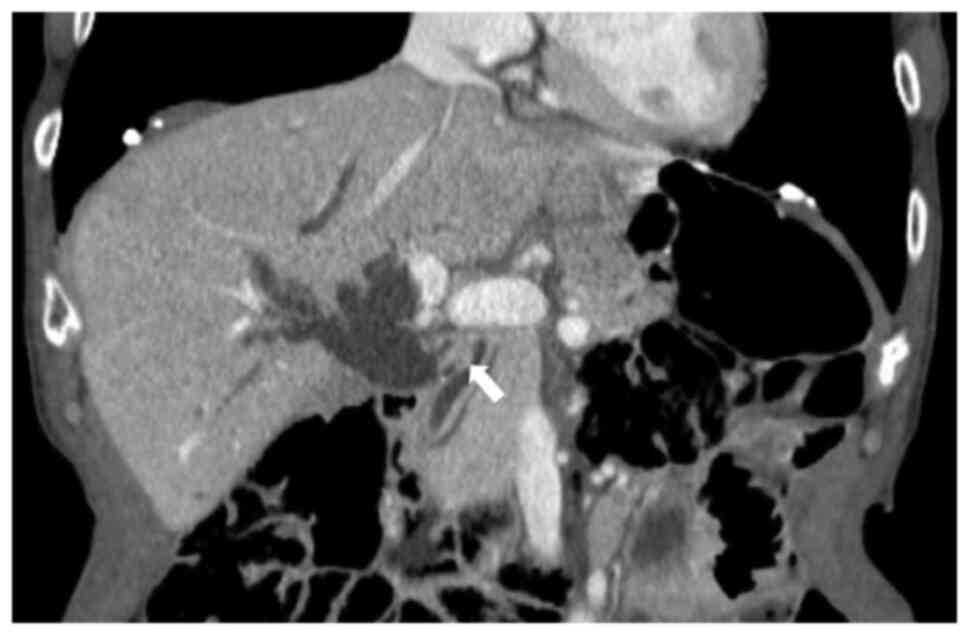
A 67-year-old Japanese man with elevated liver
enzyme levels was admitted to Niigata Cancer Center Hospital
(Niigata, Japan) in February 2017. Multidetector-row computed
tomography (CT) revealed dilation of the biliary tree and a 10-mm
enhanced nodule in the distal bile duct (Fig. 1). He underwent percutaneous
transhepatic biliary drainage via the left segment III of the
intrahepatic bile duct. Prior to surgical resection, tumor markers
of serum carcinoembryonic antigen and carbohydrate antigen 19-9
(CA19-9) levels were within the normal range. Thereafter, the
patient underwent pancreaticoduodenectomy (PD) and regional
lymphadenectomy. Intraoperative frozen section examination of the
proximal margin of the bile duct revealed an invasive carcinoma.
The proximal margin was additionally resected, and the final
pathological diagnosis of the proximal margin confirmed the
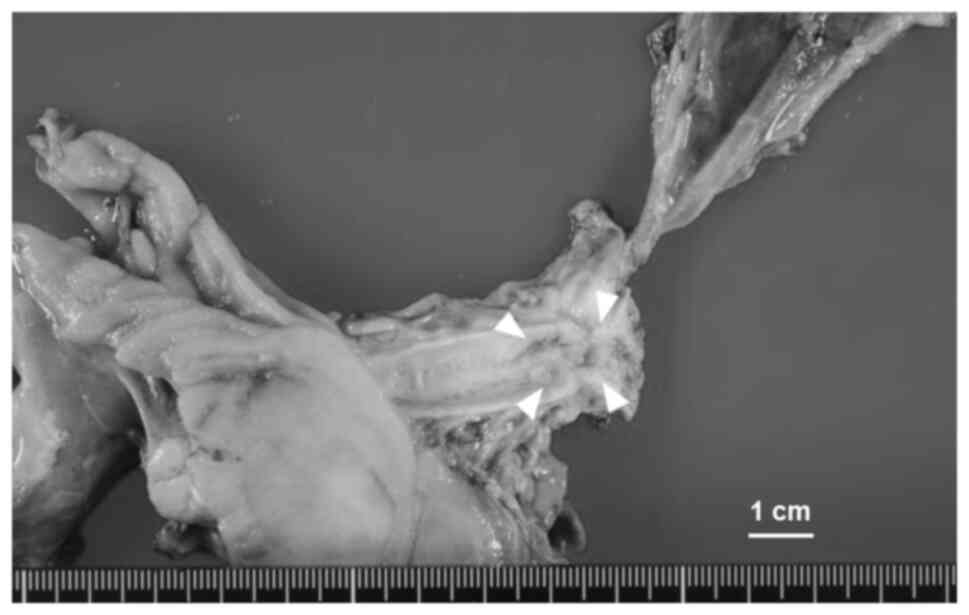
presence of carcinoma in situ. The pathological stage of the
distal cholangiocarcinoma was T2N0M0 Stage IIA, according to Union
for International Cancer Control 8th edition (Fig. 2). Pathological examination revealed
that the tumor was poorly differentiated adenocarcinoma measuring
45×20 mm, exhibiting lymphatic invasion and perineural invasion.
Following the PD, the patient received adjuvant chemotherapy with
oral TS-1® at 100 mg/day (Taiho Pharmaceutical, Tokyo,
Japan) for 1 month. Subsequently, after 2 months of the PD, he was
readmitted to our hospital due to decreased visual acuity.
Fundoscopic examination revealed a macular hole in the right eye,
which was determined to be the cause of the visual acuity decline.
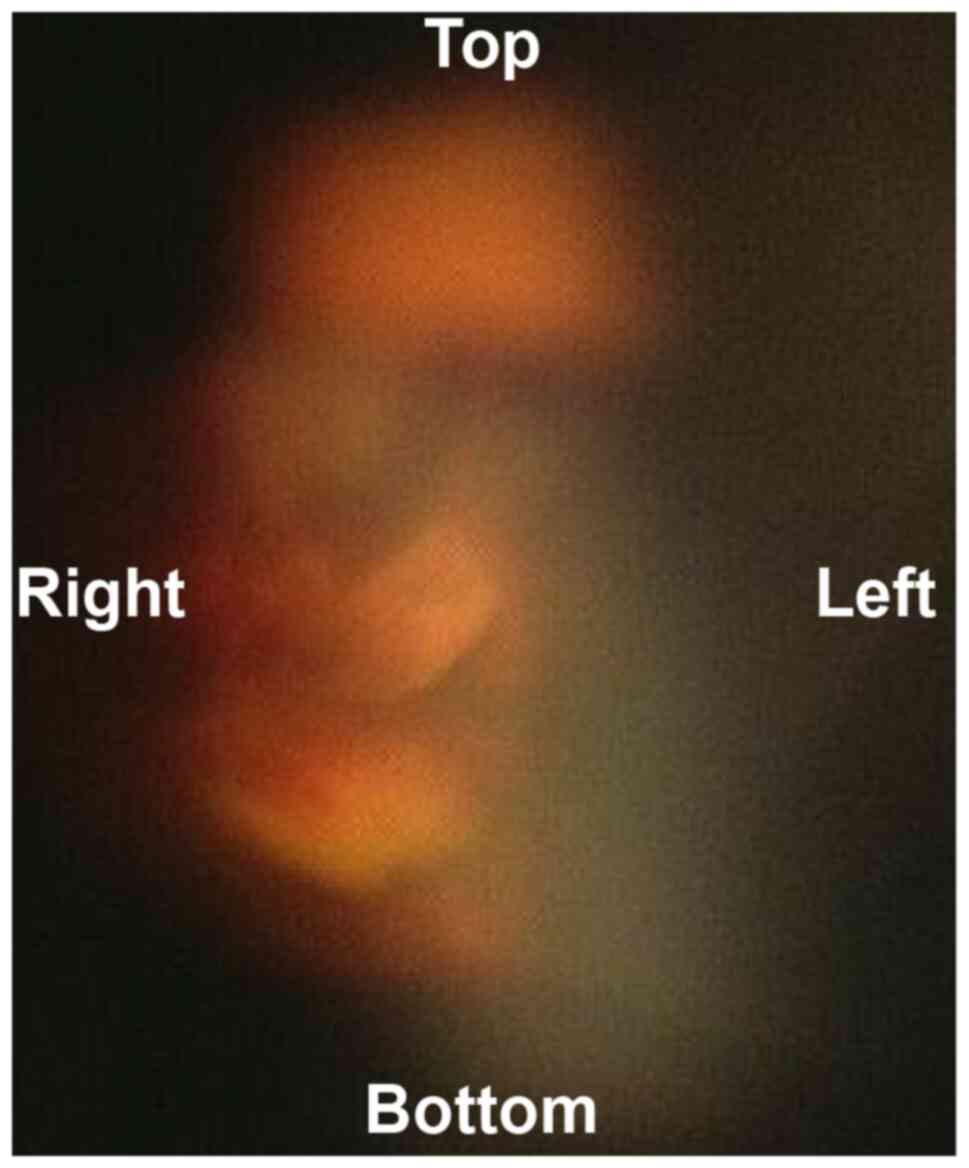
Furthermore, Goldmann three-mirror contact lens examination
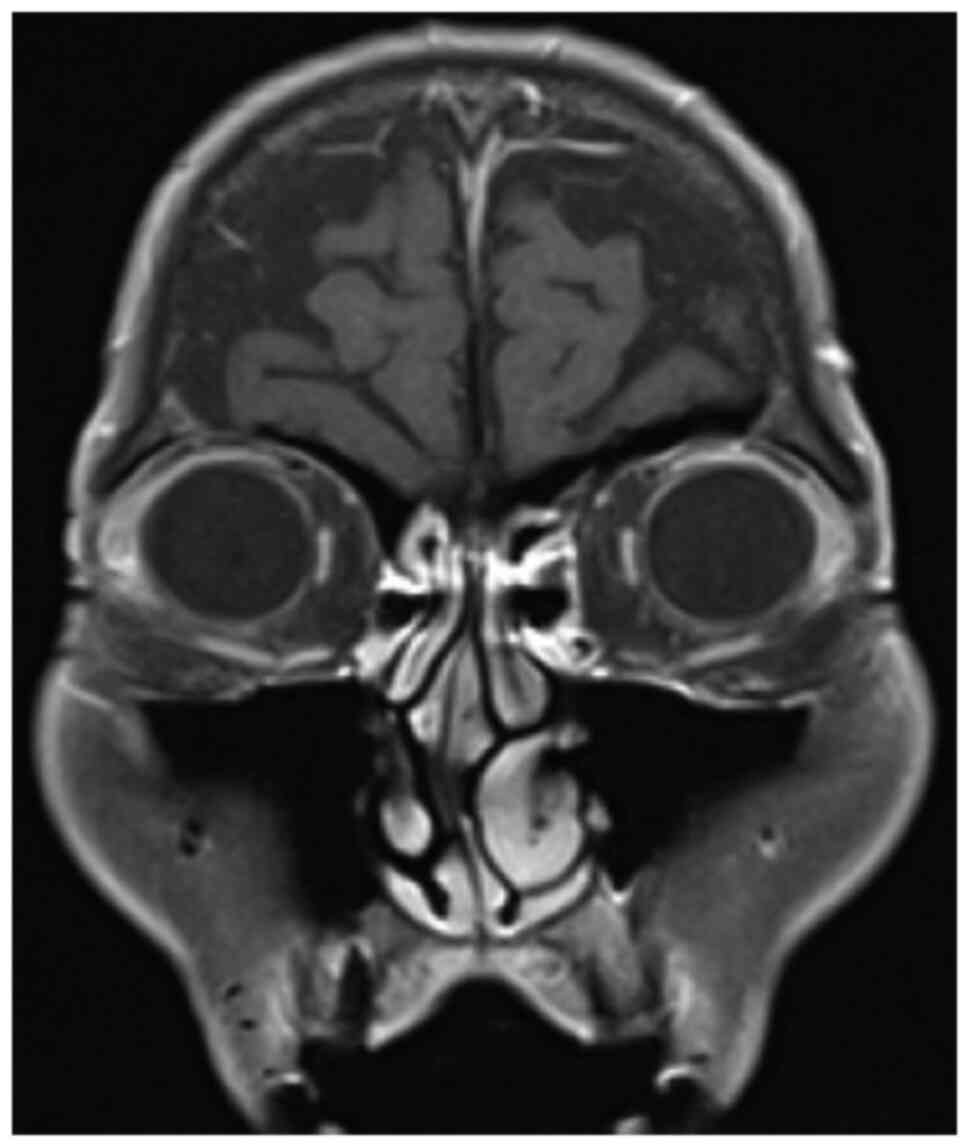
revealed a 4-mm, yellowish choroidal mass (Fig. 3). The tumor was considered unrelated
to the decreased visual acuity due to its location far from the
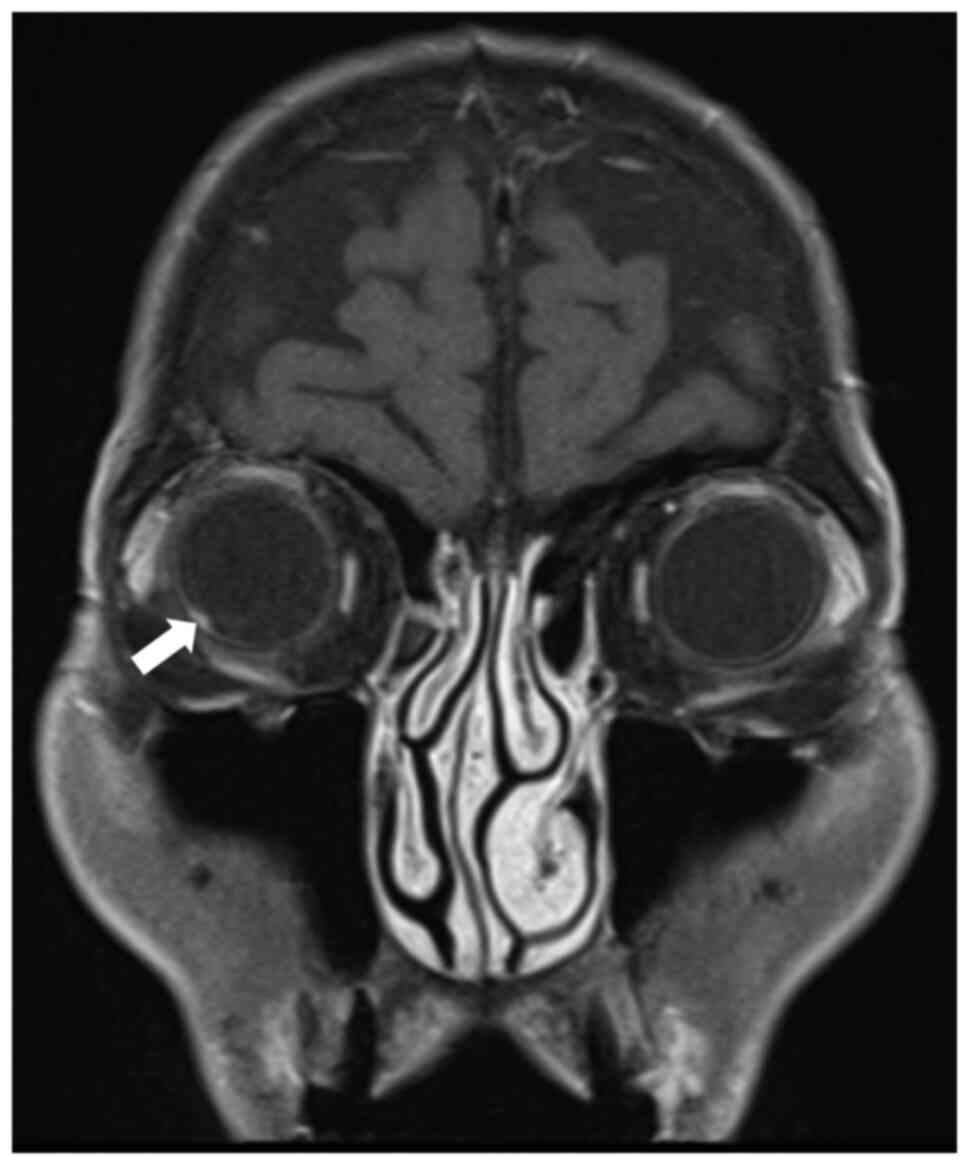
optic nerve. Magnetic resonance imaging (MRI) revealed a 4-mm
enhanced choroidal mass (Fig. 4).
Positron emission tomography CT exhibited no remarkable findings
that indicated recurrence. Based on the results of these
ophthalmological examinations and the patient's history of distal
cholangiocarcinoma, he was diagnosed with choroidal metastasis from
distal cholangiocarcinoma. Photocoagulation was initially performed
for the choroidal lesion. However, this was insufficient due to the
location of the tumor. Therefore, the patient underwent
stereotactic radiotherapy (SRT) with a cumulative dose of 40 Gy
administered in 8 Gy fractions. At the initiation of SRT, serum
CA19-9 level was elevated to 55.2 U/ml. Following 1 year of the
radiotherapy, the choroidal lesion became obscured, and a complete
remission was successfully achieved with SRT (Fig. 5). Following SRT, serum CA19-9 level
returned to the normal range. He had been regularly followed up
every 6 months as an outpatient with ophthalmologic examinations,
contrast-enhanced abdominal CT scans, and orbital MRI scans. The
patient remains alive and in good health, showing no signs of
recurrence, 4 years after the diagnosis of choroidal
metastasis.
Discussion
The occurrence of cancer metastasis within the
intraocular region is rare. Choroidal metastases constitute a
significant majority of intraocular metastases, ranging from 62 to
88% (1). Generally, patients with
choroidal metastasis exhibit poor prognosis; median survival time
of patients with choroidal metastasis is reported to be 4.2 months
in pancreatic cancer, 11.5 months in lung cancer, 12.4 months in
gastrointestinal cancer, and 22.2 months in breast cancer (7). To the best of our knowledge, this is
the second reported case of intraocular metastasis from
cholangiocarcinoma (3), and he
exhibited no evidence of recurrence 4 years after the curative
treatment for choroidal metastasis.
The chief complaints of patients with choroidal
metastasis are blurred vision (81%), flashes and floaters (5–12%),
and eye pain (5–14%); however, 9–11% of those with choroidal
metastasis exhibit no symptoms (1).
In the present case, the patient was referred to our hospital due
to decreased visual acuity. However, the choroidal mass was
considered to be unrelated to the patient's complaint because the
tumor was distant from the optic nerve and a macular hole was
suspected as the cause instead.
Most choroidal tumors are either malignant melanomas
or metastatic tumors. Macroscopic appearance is valuable for
clinically discriminating between the two types of tumors.
Malignant melanomas typically exhibit a dark blackish color,
whereas metastatic choroidal tumors tend to display a yellowish
color. In the present case, Goldmann three-mirror contact lens
examination revealed a 4-mm choroidal mass with a yellowish color,
which supported the diagnosis of metastatic choroidal tumor.
However, it is important to note the existence of a variant of
melanoma, known as amelanotic melanoma, which does not exhibit a
blackish color but rather presents as pink, red, or brown lesion,
thereby resembling a metastatic choroidal tumor in terms of gross
coloration. In the present case, serum CA19-9 level, an established
tumor marker for adenocarcinoma, was elevated at the initiation of
SRT for the choroidal tumor. Considering the macroscopic
characteristics of the choroidal tumor and the elevated serum
CA19-9 level, the patient was diagnosed with choroidal metastasis
from distal cholangiocarcinoma. Considering the aforementioned
information, even for small choroidal masses measuring <5 mm,
the macroscopic coloration of the choroidal tumor can serve as a
useful feature in distinguishing between malignant melanoma and
metastatic choroidal tumors. Nevertheless, in the absence of
histologic examination, several clinical factors, such as gross
observations, imaging findings, and tumor markers, should be
considered to discriminate between the two.
No established standard treatment for choroidal
metastasis is available (8).
Treatment options for choroidal metastasis encompass chemotherapy,
photocoagulation, radiation therapy, or enucleation. However, these
treatment modalities do not result in significant variations in
survival outcomes (4,5). Thus, prioritizing the preservation of
visual acuity and enhancing quality of life is a crucial goal in
the treatment of choroidal metastasis. Therefore, various radiation
therapies have been employed.
One such approach is external-beam radiotherapy
(EBRT), which is a conventional treatment for uveal metastasis that
was first used in 1979 (9). The
response rate to EBRT for choroidal metastases, defined as tumor
shrinkage or visual stabilization, is approximately 80% (10,11).
The recommended dose typically ranges from 26 to 46 Gy (median,
38.4 Gy) (12,13). Nonetheless, complications including
cataracts, exposure keratopathy, iris neovascularization, radiation
retinopathy, and radiation papillopathy are relatively common with
EBRT. Approximately 12% of patients experience complications over a
median follow-up period of 5.8 months (11), and the incidence of these
complications is dose-dependent: 0% at doses ≤30 Gy and 100% at
doses ≥57 Gy (13,14). A disadvantage of EBRT is the need
for daily treatment for 2–4 weeks (15).
SRT is a non-invasive treatment option for choroidal
metastases. Meticulous computerized treatment planning and accurate
repositioning based on high-resolution orbital CT can reduce tumor
margins and preserve critical structures, such as the optic nerve,
lens, and lacrimal gland (6). In
addition, SRT provides low-dose radiation from multiple directions
with high accuracy (16).
Therefore, patients can receive treatment aimed at minimizing the
adverse effects of radiation on surrounding normal tissues. Haidar
et al (17) conducted SRT
for choroidal metastases from breast cancer with a total dose of 25
Gy in 5 Gy fractions for 5 days. They reported that the patient's
vision remained stable, and no recurrence was reported for 3 years
following SRT of the choroidal metastases (17). Bellmann et al (6) treated 10 patients with unifocal
choroidal metastases (3 breast carcinomas, 3 lung carcinomas, 3
colon carcinomas, and 1 cutaneous melanoma) using SRT with a single
dose ranging from 12 Gy to 20 Gy or a total dose of 30 Gy over 10
days (3 Gy per session). They reported that local tumor control was
achieved in all patients during follow-up periods ranging from 1
month to 34 months (median, 6.5 months) (6). In the present case of choroidal
metastasis from distal cholangiocarcinoma, the patient underwent
SRT with a total dose of 40 Gy administered in 8 Gy fractions over
5 days. The patient remains alive and in good health without any
evidence of recurrence or signs of decline in visual acuity, 4
years after the diagnosis of choroidal metastasis. This suggested
that SRT could be a viable treatment option for choroidal
metastases, facilitating local tumor control while minimizing the
adverse effects of radiation.
Even after curative resection for distal
cholangiocarcinoma, 5-year survival rate ranges from 18 to 54%
(18). This unfavorable prognosis
can be attributed to the high recurrence rate after resection, with
over 50% of patients experiencing distant metastasis within 5 years
of curative resection (19). In the
case of periampullary cancer, perineural invasion and lymph node
metastasis have been identified as independent predictive factors
for distant metastasis after curative resection (20,21).
In the context of distant cholangiocarcinoma, Komaya et al
(18) demonstrated that perineural
invasion, pancreatic invasion, and lymph node metastasis were
independent prognostic factors for time taken for recurrence after
resection, while Kim et al (19) reported that poor differentiation and
lymph node metastasis were predictors of distant metastasis. In the
present case, the primary tumor exhibited poor differentiation and
perineural invasion. Therefore, in cases of
histologically-confirmed poor differentiation, perineural invasion,
or lymph node metastasis following resection for distal
cholangiocarcinoma, a close follow up utilizing tumor markers and
imaging studies is recommended.
To the best of our knowledge, this is the second
reported case of intraocular metastasis of cholangiocarcinoma. SRT
may provide an opportunity to control metastatic choroidal
carcinoma without decreasing the visual acuity.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author upon reasonable
request.
Authors' contributions
YS, YH, TN, KT, HH, TB, MA, HN, AM, SM, YT, HY, JS,
TW, SS, and SN participated in the conception and design for the
paper. YS and YH drafted and revised the manuscript, and are
responsible for the paper. HH provided advice on ophthalmic
findings and contributed to the writing of the manuscript. TN, JS,
TW and SS critically revised the paper. TN, KT, and HH interpreted
the imaging data. YS and YH confirm the authenticity of all the
data. All authors have read and approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
The patient provided written informed consent for
the publication of the data.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
CT
|
computed tomography
|
|
CA19-9
|
carbohydrate antigen 19-9
|
|
PD
|
pancreaticoduodenectomy
|
|
MRI
|
magnetic resonance imaging
|
|
SRT
|
stereotactic radiotherapy
|
|
EBRT
|
external-beam radiotherapy
|
References
|
1
|
Wu SQ, Li QS, Zhang Y and Zhu LW:
Spontaneous rupture of the eyeball due to choroidal metastasis of
gastric carcinoma A case report. Medicine (Baltimore).
98:e174412019. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shields CL, Shields JA, Gross NE, Schwartz
GP and Lally SE: Survey of 520 eyes with uveal metastases.
Ophthalmology. 104:1265–1276. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Lee J, Lee S, Sohn J and Yoon YH: Clinical
features of uveal metastases in Korean patients. Retina.
23:491–494. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Kurashige Y, Otani A and Yoshimura N:
Choroidal metastasis of renal cell carcinoma: A case report. Jpn J
Ophthalmol. 54:111–112. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Reddy SC, Madhavan M and Mutum SS:
Anterior uveal and episcleral metastases from carcinoma of the
breast. Ophthalmologica. 214:368–372. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Bellmann C, Fuss M, Holz FG, Debus J,
Rohrschneider K, Völcker HE and Wannenmacher M: Stereotactic
radiation therapy for malignant choroidal tumors: Preliminary,
short-term results. Ophthalmology. 107:358–365. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shields CL, Welch RJ, Malik K,
Acaba-Berrocal LA, Selzer EB, Newman JH, Mayro EL, Constantinescu
AB, Spencer MA, McGarrey MP, et al: Uveal metastasis: Clinical
features and survival outcome of 2214 tumors in 1111 patients based
on primary tumor origin. Middle East Afr J Ophthalmol. 25:81–90.
2018. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Jardel P, Sauerwein W, Olivier T,
Bensoussan E, Maschi C, Lanza F, Mosci C, Gastaud L, Angellier G,
Marcy PY, et al: Management of choroidal metastases. Cancer Treat
Rev. 40:1119–1128. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Stephens RF and Shields JA: Diagnosis and
management of cancer metastatic to the uvea: A study of 70 cases.
Ophthalmology. 86:1336–1349. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Small W Jr: Management of ocular
metastasis. Cancer Control. 5:326–332. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen CJ, McCoy AN, Brahmer J and Handa JT:
Emerging treatments for choroidal metastases. Surv Ophthalmol.
56:511–521. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Okuma Y, Hosomi Y, Kitamura K, Iguchi M,
Okamura T, Fukami S, Hishima T and Shibuya M: Choroidal metastasis
in a patient with small cell lung cancer discovered during
treatment with chemotherapy. Int J Clin Oncol. 14:541–544. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Trikha R, Morse LS, Zawadzki RJ, Werner JS
and Park SS: Ten-year follow-up of eyes treated with stereotactic
fractionated external beam radiation for neovascular age-related
macular degeneration. Retina. 31:1303–1315. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Rudoler SB, Corn BW, Shields CL, De Potter
P, Hyslop T, Shields JA and Curran WJ Jr: External beam irradiation
for choroid metastases: Identification of factors predisposing to
long-term sequelae. Int J Radiat Oncol Biol Phys. 38:251–256. 1997.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Demirci H, Shields CL, Chao AN and Shields
JA: Uveal metastasis from breast cancer in 264 patients. Am J
Ophthalmol. 136:264–271. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Guckenberger M, Baus WW, Blanck O, Combs
SE, Debus J, Engenhart-Cabillic R, Gauer T, Grosu AL, Schmitt D,
Tanadini-Lang S and Moustakis C: Definition and quality
requirements for stereotactic radiotherapy: Consensus statement
from the DEGRO/DGMP Working Group Stereotactic Radiotherapy and
Radiosurgery. Strahlenther Onkol. 196:417–420. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Haidar YM, Korn BS and Rose MA: Complete
regression of a choroidal metastasis secondary to breast cancer
with stereotactic radiation: Case report and review of literature.
J Radiosurg SBRT. 2:155–164. 2013.PubMed/NCBI
|
|
18
|
Komaya K, Ebata T, Shirai K, Ohira S,
Morofuji N, Akutagawa A, Yamaguchi R and Nagino M; Nagoya Surgical
Oncology Group, : Recurrence after resection with curative intent
for distal cholangiocarcinoma. Br J Surg. 104:426–433. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Kim K, Chie EK, Jang JY, Kim SW, Han SW,
Oh DY, Im SA, Kim TY, Bang YJ and Ha SW: Distant metastasis risk
stratification for patients undergoing curative resection followed
by adjuvant chemoradiation for extrahepatic bile duct cancer. Int J
Radiat Oncol Biol Phys. 84:81–87. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bhandare MS, Mondal A, Chaudhari V, Bal M,
Yadav S, Ramaswamy A, Ostwal V, Shetty N and Shrikhande SV: Factors
influencing local and distant recurrence following resection of
periampullary cancer. Br J Surg. 108:427–434. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lee DH, Kim HJ, Cho CW, Yun SS and Lee DS:
Factors influencing patterns of recurrence following
pancreaticoduodenectomy for patients with distal bile duct cancer
and ampulla of Vater cancer. Ann Hepatobiliary Pancreat Surg.
26:138–143. 2022. View Article : Google Scholar : PubMed/NCBI
|