Introduction
Renal cell carcinoma (RCC) accounts for 3–5% of all
cancer cases worldwide, and while improved screening has increased
the detection of early stage disease, a total of 20–30% of patients
with RCC are diagnosed with metastases at the initial presentation
(1). Although in the past, there
was no systemic therapy regimen that could be expected to be
effective enough for patients with advanced RCC, the advent of
molecular-targeted agents, including tyrosine kinase inhibitors
(TKIs) and immune checkpoint inhibitors (ICIs), has changed the
treatment of metastatic RCC (mRCC) (2,3).
Furthermore, combination regimens of the aforementioned drugs have
been introduced over several years, and the prognosis of patients
with mRCC has improved (4–8). The combination regimens approved by
the health insurance system in Japan can be broadly classified into
two types: Regimens combining two ICIs (ipilimumab and nivolumab;
ICI–ICI) and regimens combining a TKI with an ICI (ICI-TKI). Four
ICI-TKI regimens have been introduced: Avelumab + axitinib,
pembrolizumab + axitinib, nivolumab + cabozantinib, and
pembrolizumab + lenvatinib. All regimens have been shown to improve
treatment efficacy and prognosis through randomized control trials
(RCTs) (4–8). While the introduction of multiple
effective systemic treatment options has been encouraging,
nephrectomy as a treatment approach has been controversial
(9–14). A number of retrospective studies
have demonstrated the benefit of upfront cytoreductive nephrectomy
(CN) in mRCC treated with TKIs (9,10) and
ICIs (11,12); however, several RCTs have shown
negative data for upfront CN in mRCC treated with TKIs (13,14).
It is important to clarify the association between treatment
efficacy and surgical therapy to select the optimal systemic
treatment regimen. The present study aimed to determine the
relationship between the therapeutic outcome of combination
regimens, including ICIs and/or TKIs, and CN for mRCC.
Materials and methods
Patients
Inclusion criteria for the present study included:
i) Treatment of mRCC between January 2018 and June 2022 at Kobe
University Hospital or affiliated institutes: Hyogo Prefectural
Amagasaki General Medical Center (Amagasaki, Japan), Hyogo Cancer
Center (Akashi, Japan), Japanese Red Cross Society Himeji Hospital
(Himeji, Japan), Kobe City Medical Center West Hospital (Kobe,
Japan), Hyogo Prefectural Kakogawa Medical Center (Kakogawa,
Japan), Kansai Rosai Hospital (Amagasaki, Japan), Kita-harima
Medical Center (Himeji, Japan) and Yodogawa Christian Hospital
(Osaka, Japan), from January 2018 to June 2022; ii) treatment with
a combination regimen including TKI or ICI as first-line therapy;
and iii) mRCC classified as intermediate or poor risk by the
International mRCC Database Consortium (IMDC) (15). Exclusion criteria included: i)
Treatment with a combination regimen as presurgical therapy; and
ii) unknown pathology. A total of 8/172 patients with mRCC whose
pathological diagnosis was not determined, and a total of 13/172
patients who were categorized as favorable risk, were excluded. As
a result, 151 patients were included in the current study, and were
retrospectively studied by reviewing the relevant
clinicopathological data. Ethics approval was granted by the Ethics
Committee of Kobe University (approval no. B230087).
Patients treated with ipilimumab + nivolumab, and
those treated with either avelumab + axitinib, pembrolizumab +
axitinib, nivolumab + cabozantinib or pembrolizumab + lenvatinib,
were divided into the ICI–ICI and ICI-TKI groups, respectively.
Clinicopathological data, including age, sex, pathological
findings, Karnofsky performance status (KPS) score (16), metastasis status, choice of
first-line regimen and IMDC risk, were evaluated for all patients,
and the distribution of these parameters in each group was
compared. The objective response (OR), OR rate (ORR), and the
progression-free survival (PFS) and overall survival (OS) times for
each group were determined. These analyses were performed for all
patients, and patients were further classified into three patterns:
Recurrence after primary tumor resection diagnosed as RCC (pattern
A), mRCC at initial diagnosis with upfront CN (pattern B) and mRCC
at initial diagnosis without upfront CN (pattern C).
Statistical analysis
The differences in the distribution of categorical
variables between the groups were analyzed using a χ2
test, and when >20% of expected counts were ≤5, they were
analyzed using Fisher's exact test. Tumor responses were determined
by investigator assessment on the basis of RECIST version 1.1
(17). The PFS and OS times were
determined using the Kaplan-Meier method, and the differences
between the two groups were analyzed using log-rank test. All
statistical analyses were conducted using Statview (version 5.0;
Abacus Concepts, Inc.), and P<0.05 was considered to indicate a
statistically significant difference.
Results
All patients
The median age of the patients was 71 years (range,
30–86 years). The median observation period was 16.6 months (range,
1–93.8 months). The first-line regimens were the ICI–ICI and
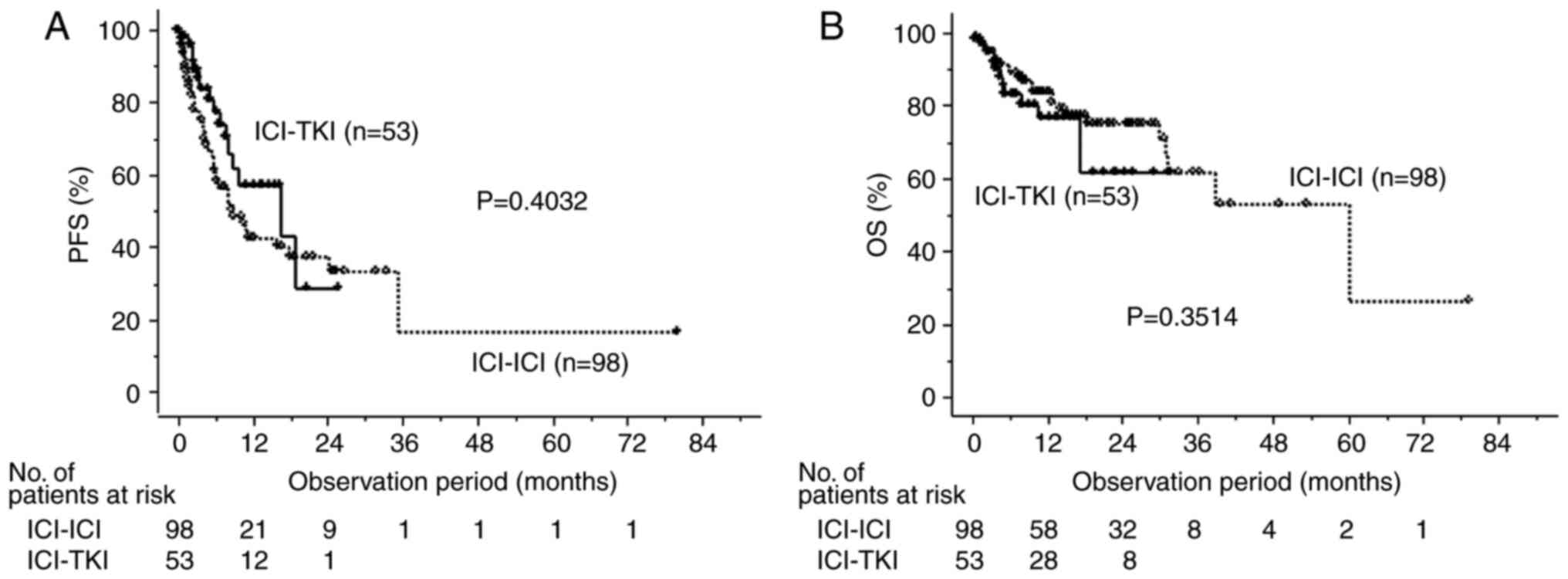
ICI-TKI regimens in 98 and 53 cases, respectively. The number of
patients with lymph node metastasis in the ICI–ICI group was
significantly higher than that in the ICI-TKI group (Table IA). There was no statistically
significant difference in either PFS or OS between the two regimen
groups when all patients were assessed (Fig. 1).
 | Table I.Comparison of characteristics of
patients between the ICI–ICI (n=98) and ICI-TKI (n=53) groups. |
Table I.
Comparison of characteristics of
patients between the ICI–ICI (n=98) and ICI-TKI (n=53) groups.
| A, All patients
(n=151) |
|---|
|
|---|
| Characteristics | ICI–ICI, n (%) | ICI-TKI, n (%) | P-value | Total, n (%) |
|---|
| Age, years |
|
|
|
|
| ≥70 | 54 (55.1) | 31 (58.5) | 0.6887 | 85 (56.3) |
| ≤69 | 44 (44.9) | 22 (41.5) |
| 66 (43.7) |
| Sex |
|
|
|
|
| Male | 76 (77.6) | 43 (81.1) | 0.6073 | 119 (78.8) |
|
Female | 22 (22.4) | 10 (18.9) |
| 32 (21.2) |
| Histological
type |
|
|
|
|
|
Clear | 72 (73.5) | 45 (84.9) | 0.1083 | 117 (77.5) |
|
Non-clear | 26 (26.5) | 8 (15.1) |
| 34 (22.5) |
| KPS score, % |
|
|
|
|
| ≥80 | 82 (83.7) | 37 (69.8) | 0.0467 | 119 (78.8) |
|
<80 | 16 (16.3) | 16 (30.2) |
| 32 (21.2) |
| No. of metastatic
disease sites |
|
|
|
|
| 1 | 35 (35.7) | 20 (37.7) | 0.8054 | 55 (36.4) |
| ≥2 | 63 (64.3) | 33 (62.3) |
| 96 (63.6) |
| Metastatic disease
sites |
|
|
|
|
| Lung | 58 (59.2) | 33 (62.3) | 0.712 | 91 (60.3) |
| Bone | 32 (32.7) | 23 (43.4) | 0.1904 | 55 (36.4) |
| Lymph
node | 44 (44.9) | 11 (20.8) | 0.0033 | 55 (36.4) |
| Adrenal
gland | 9 (9.2) | 6 (11.3) | 0.6752 | 15 (9.9) |
|
Liver | 14 (14.3) | 11 (20.8) | 0.3074 | 25 (16.6) |
|
Pancreas | 6 (6.1) | 4 (7.6) | 0.7412 | 10 (6.6) |
|
Brain | 5 (5.1) | 6 (11.3) | 0.7563 | 11 (7.3) |
| IMDC risk |
|
|
|
|
|
Intermediate | 56 (57.1) | 27 (50.9) | 0.4649 | 83 (55.0) |
|
Poor | 42 (42.9) | 26 (49.1) |
| 68 (45.0) |
| First-line
regimen |
|
|
|
|
|
Ipilimumab + nivolumab | 98 (100.0) | 0 (0.0) |
| 98 (64.9) |
|
Avelumab + axitinib | 0 (0.0) | 19 (35.8) |
| 19 (12.6) |
|
Pembrolizumab + axitinib | 0 (0.0) | 11 (20.8) |
| 11 (7.3) |
|
Nivolumab + cabozantinib | 0 (0.0) | 20 (37.7) |
| 20 (13.2) |
|
Pembrolizumab +
lenvatinib | 0 (0.0) | 3 (5.7) |
| 3 (2.0) |
|
| B, Patients with
recurrence after radical surgery for renal cell carcinoma
(n=62) |
|
|
Characteristics | ICI–ICI, n
(%) | ICI-TKI, n
(%) | P-value | Total, n
(%) |
|
| Age, years |
|
|
|
|
|
≥70 | 20 (50.0) | 14 (63.6) | 0.3019 | 34 (54.8) |
|
≤69 | 20 (50.0) | 8 (36.4) |
| 28 (45.2) |
| Sex |
|
|
|
|
|
Male | 30 (75.0) | 17 (77.3) | 0.8415 | 47 (75.8) |
|
Female | 10 (25.0) | 5 (22.7) |
| 15 (24.2) |
| Histological
type |
|
|
|
|
|
Clear | 34 (85.0) | 19 (86.4) | >0.9999 | 53 (85.5) |
|
Non-clear | 6 (15.0) | 3 (13.6) |
| 9 (14.5) |
| KPS score, % |
|
|
|
|
|
≥80 | 37 (92.5) | 17 (77.3) | 0.1190 | 54 (87.1) |
|
<80 | 3 (7.5) | 5 (22.7) |
| 8 (12.9) |
| No. of metastatic
disease sites |
|
|
|
|
| 1 | 19 (47.5) | 10 (45.5) | 0.8773 | 29 (46.8) |
| ≥2 | 21 (52.5) | 12 (54.5) |
| 33 (53.2) |
| Metastatic disease
sites |
|
|
|
|
|
Lung | 19 (47.5) | 13 (59.1) | 0.3822 | 32 (51.6) |
|
Bone | 7 (17.5) | 7 (31.8) | 0.197 | 14 (22.6) |
| Lymph
node | 11 (27.5) | 4 (18.2) | 0.5409 | 15 (24.2) |
| Adrenal
gland | 2 (5.0) | 2 (9.1) | 0.6104 | 4 (6.5) |
|
Liver | 10 (25.0) | 3 (13.6) | 0.3481 | 13 (21.0) |
|
Pancreas | 3 (7.5) | 3 (13.6) | 0.6566 | 6 (9.7) |
|
Brain | 1 (2.5) | 1 (4.5) | >0.9999 | 2 (3.2) |
| IMDC risk |
|
|
|
|
|
Intermediate | 30 (75.0) | 16 (72.7) | 0.8449 | 46 (74.2) |
|
Poor | 10 (25.0) | 6 (27.3) |
| 16 (25.8) |
| First-line
regimen |
|
|
|
|
|
Ipilimumab + nivolumab | 40 (100.0) | 0 (0.0) |
| 40 (64.5) |
|
Avelumab + axitinib | 0 (0.0) | 8 (36.4) |
| 8 (12.9) |
|
Pembrolizumab + axitinib | 0 (0.0) | 5 (22.7) |
| 5 (8.1) |
|
Nivolumab + cabozantinib | 0 (0.0) | 9 (40.9) |
| 9 (14.5) |
|
Pembrolizumab +
lenvatinib | 0 (0.0) | 0 (0.0) |
| 0 (0.0) |
|
| C, Patients with
metastatic renal cell carcinoma at initial diagnosis who underwent
upfront cytoreductive nephrectomy (n=38) |
|
|
Characteristics | ICI–ICI, n
(%) | ICI-TKI, n
(%) | P-value | Total, n
(%) |
|
| Age, years |
|
|
|
|
|
≥70 | 13 (52.0) | 8 (61.5) | 0.5748 | 21 (55.3) |
|
≤69 | 12 (48.0) | 5 (38.5) |
| 17 (44.7) |
| Sex |
|
|
|
|
|
Male | 18 (72.0) | 10 (76.9) | >0.9999 | 28 (73.7) |
|
Female | 7 (28.0) | 3 (23.1) |
| 10 (26.3) |
| Histological
type |
|
|
|
|
|
Clear | 17 (68.0) | 11 (84.6) | 0.2698 | 28 (73.7) |
|
Non-clear | 8 (32.0) | 2 (15.4) |
| 10 (26.3) |
| KPS score, % |
|
|
|
|
|
≥80 | 22 (88.0) | 9 (69.2) | 0.2025 | 31 (81.6) |
|
<80 | 3 (12.0) | 4 (39.8) |
| 7 (18.4) |
| No. of metastatic
disease sites |
|
|
|
|
| 1 | 7 (28.0) | 6 (46.2) | 0.2631 | 13 (34.2) |
| ≥2 | 18 (72.0) | 7 (53.8) |
| 25 (65.8) |
| Metastatic disease
sites |
|
|
|
|
|
Lung | 19 (76.0) | 9 (69.2) | 0.7092 | 28 (73.7) |
|
Bone | 6 (24.0) | 3 (23.1) | >0.9999 | 9 (23.7) |
| Lymph
node | 14 (56.0) | 2 (15.4) | 0.0140 | 16 (42.1) |
| Adrenal
gland | 1 (4.0) | 2 (15.4) | 0.2651 | 3 (7.9) |
|
Liver | 2 (8.0) | 2 (15.4) | 0.5959 | 4 (10.5) |
|
Pancreas | 1 (4.0) | 0 (0.0) | >0.9999 | 1 (2.6) |
|
Brain | 1 (4.0) | 2 (15.4) | 0.2651 | 3 (7.9) |
| IMDC risk |
|
|
|
|
|
Intermediate | 17 (68.0) | 5 (38.5) | 0.0802 | 22 (57.9) |
|
Poor | 8 (32.0) | 8 (61.5) |
| 16 (42.1) |
| First-line
regimen |
|
|
|
|
|
Ipilimumab + nivolumab | 25 (100.0) | 0 (0.0) |
| 25 (65.8) |
|
Avelumab + axitinib | 0 (0.0) | 9 (69.2) |
| 9 (23.7) |
|
Pembrolizumab + axitinib | 0 (0.0) | 4 (30.8) |
| 4 (10.5) |
|
| D, Patients with
metastatic renal cell carcinoma at initial diagnosis who did not
undergo upfront cytoreductive nephrectomy (n=51) |
|
|
Characteristics | ICI–ICI, n
(%) | ICI-TKI, n
(%) | P-value | Total, n
(%) |
|
| Age, years |
|
|
|
|
|
≥70 | 21 (63.6) | 9 (50.0) | 0.3444 | 30 (58.8) |
|
≤69 | 12 (36.4) | 9 (50.0) |
| 21 (41.2) |
| Sex |
|
|
|
|
|
Male | 28 (84.8) | 16 (88.9) | >0.9999 | 44 (86.3) |
|
Female | 5 (15.2) | 2 (11.1) |
| 7 (13.7) |
| Histological
type |
|
|
|
|
|
Clear | 21 (63.6) | 15 (83.3) | 0.2025 | 36 (70.6) |
|
Non-clear | 12 (36.4) | 3 (16.7) |
| 15 (29.4) |
| KPS score, % |
|
|
|
|
|
≥80 | 23 (69.7) | 11 (61.1) | 0.5342 | 34 (66.7) |
|
<80 | 10 (30.3) | 7 (38.9) |
| 17 (33.3) |
| No. of metastatic
disease sites |
|
|
|
|
| 1 | 9 (27.3) | 4 (22.2) | 0.7502 | 13 (25.5) |
| ≥2 | 24 (72.7) | 14 (77.8) |
| 38 (74.5) |
| Metastatic disease
sites |
|
|
|
|
|
Lung | 20 (60.6) | 11 (61.1) | 0.9718 | 31 (60.8) |
|
Bone | 19 (57.6) | 9 (50.0) | 0.6033 | 28 (54.9) |
| Lymph
node | 19 (57.6) | 5 (27.8) | 0.0416 | 24 (47.1) |
| Adrenal
gland | 6 (18.2) | 2 (11.1) | 0.6959 | 8 (15.7) |
|
Liver | 2 (6.1) | 6 (33.3) | 0.0171 | 8 (15.7) |
|
Pancreas | 2 (6.1) | 1 (5.6) | >0.9999 | 3 (5.9) |
|
Brain | 3 (9.1) | 3 (16.7) | 0.6524 | 6 (11.8) |
| IMDC risk |
|
|
|
|
|
Intermediate | 9 (27.3) | 6 (33.3) | 0.6499 | 15 (29.4) |
|
Poor | 24 (72.7) | 12 (66.7) |
| 36 (70.6) |
| First-line
regimen |
|
|
|
|
|
Ipilimumab + nivolumab | 33 (100) | 0 (0.0) |
| 33 (64.7) |
|
Avelumab + axitinib | 0 (0.0) | 2 (11.1) |
| 2 (3.9) |
|
Pembrolizumab + axitinib | 0 (0.0) | 2 (11.1) |
| 2 (3.9) |
|
Nivolumab + cabozantinib | 0 (0.0) | 11 (61.1) |
| 11 (21.6) |
|
Pembrolizumab +
lenvatinib | 0 (0.0) | 3 (16.7) |
| 3 (5.9) |
Patients' characteristics in each
pattern
Patterns A, B and C consisted of 62, 38 and 51
patients, respectively. The frequency of patients with non-clear
histology, low KPS, multiple metastatic organs, bone metastasis,
lymph node metastasis and poor IMDC risk was significantly lower in
pattern A than in the other two patterns (Table II). The frequency of patients with
poor IMDC risk in pattern B was significantly lower than that in
pattern C (Table II). There was no
significant difference in the background of patients between the
ICI–ICI and the ICI-TKI groups in every pattern, except for a
higher number of patients with lymph node metastasis in the ICI–ICI
group in pattern B and C, and a higher number of patients with
liver metastasis in the ICI-TKI group in pattern C (Table IB-D).
| Table II.Characteristics of patients in
pattern A (n=62), pattern B (n=38) and pattern C (n=51). |
Table II.
Characteristics of patients in
pattern A (n=62), pattern B (n=38) and pattern C (n=51).
|
Characteristics | Pattern A, n
(%) | Pattern B, n
(%) | Pattern C, n
(%) | P-value, pattern A
vs. patterns B + C | P-value, pattern B
vs. pattern C | Total,n (%) |
|---|
| Age, years |
|
|
|
|
|
|
|
≥70 | 34 (54.8) | 21 (55.3) | 30 (58.8) | 0.7639 | 0.7370 | 85 (56.3) |
|
≤69 | 28 (45.2) | 17 (44.7) | 21 (41.2) |
|
| 66 (43.7) |
| Sex |
|
|
|
|
|
|
|
Male | 47 (75.8) | 28 (73.7) | 44 (86.3) | 0.4513 | 0.1350 | 119 (78.8) |
|
Female | 15 (24.2) | 10 (26.3) | 7 (13.7) |
|
| 32 (21.2) |
| Histological
type |
|
|
|
|
|
|
|
Clear | 53 (85.5) | 28 (73.7) | 36 (70.6) | 0.0495 | 0.7479 | 117 (77.5) |
|
Non-clear | 9 (14.5) | 10 (26.3) | 15 (29.4) |
|
| 34 (22.5) |
| KPS |
|
|
|
|
|
|
|
≥80% | 54 (87.1) | 31 (81.6) | 34 (66.7) | 0.0375 | 0.1169 | 119 (78.8) |
|
<80% | 8 (12.9) | 7 (18.4) | 17 (33.3) |
|
| 32 (21.2) |
| No. of metastatic
organs |
|
|
|
|
|
|
| 1 | 29 (46.8) | 13 (34.2) | 13 (25.5) | 0.0274 | 0.3709 | 55 (36.4) |
| ≥2 | 33 (53.2) | 25 (65.8) | 38 (74.5) |
|
| 96 (63.6) |
| Metastatic disease
sites |
|
|
|
|
|
|
|
Lung | 32 (51.6) | 28 (73.7) | 31 (60.8) | 0.0698 | 0.2029 | 91 (60.3) |
|
Bone | 14 (22.6) | 13 (34.2) | 28 (54.9) | 0.0032 | 0.0527 | 55 (36.4) |
| Lymph
node | 15 (24.2) | 16 (42.1) | 24 (47.1) | 0.0091 | 0.6422 | 55 (36.4) |
| Adrenal
gland | 4 (6.5) | 3 (7.9) | 8 (15.7) | 0.2789 | 0.3409 | 15 (9.9) |
|
Liver | 13 (21.0) | 4 (10.5) | 8 (15.7) | 0.2235 | 0.5457 | 25 (16.6) |
|
Pancreas | 6 (9.7) | 1 (2.7) | 3 (5.9) | 0.2077 | 0.6329 | 10 (6.6) |
|
Brain | 2 (3.2) | 3 (7.9) | 6 (11.8) | 0.2011 | 0.7272 | 11 (7.3) |
| IMDC risk |
|
|
|
|
|
|
|
Intermediate | 46 (74.2) | 22 (57.9) | 15 (29.4) | <0.0001 | 0.0070 | 83 (55.0) |
|
Poor | 16 (25.8) | 16 (42.1) | 36 (70.6) |
|
| 68 (45.0) |
| First-line
regimen |
|
|
|
|
|
|
|
Ipilimumab + nivolumab | 40 (64.5) | 25 (65.8) | 33 (64.7) | 0.9341 | 0.9155 | 98 (64.9) |
|
Avelumab + axitinib | 8 (12.9) | 9 (23.7) | 2 (3.9) | 0.9211 | 0.0077 | 19 (12.6) |
|
Pembrolizumab + axitinib | 5 (8.1) | 4 (10.5) | 2 (3.9) | 0.7583 | 0.3954 | 11 (7.3) |
|
Nivolumab + cabozantinib | 9 (14.5) | 0 (0.0) | 11 (21.6) | 0.7005 | 0.0020 | 20 (13.2) |
|
Pembrolizumab +
lenvatinib | 0 (0.0) | 0 (0.0) | 3 (5.9) | 0.2691 | 0.2577 | 3 (1.9) |
Treatment outcomes in each
pattern
In the ICI-TKI group of pattern C and in that of all
patients, the ORR [the frequency of patients with complete response
(CR) or partial response (PR) as the best OR] was significantly
higher, while the frequency of patients with CR and that with
progressive disease (PD) as the best OR were significantly lower
than that in the ICI–ICI group (Table
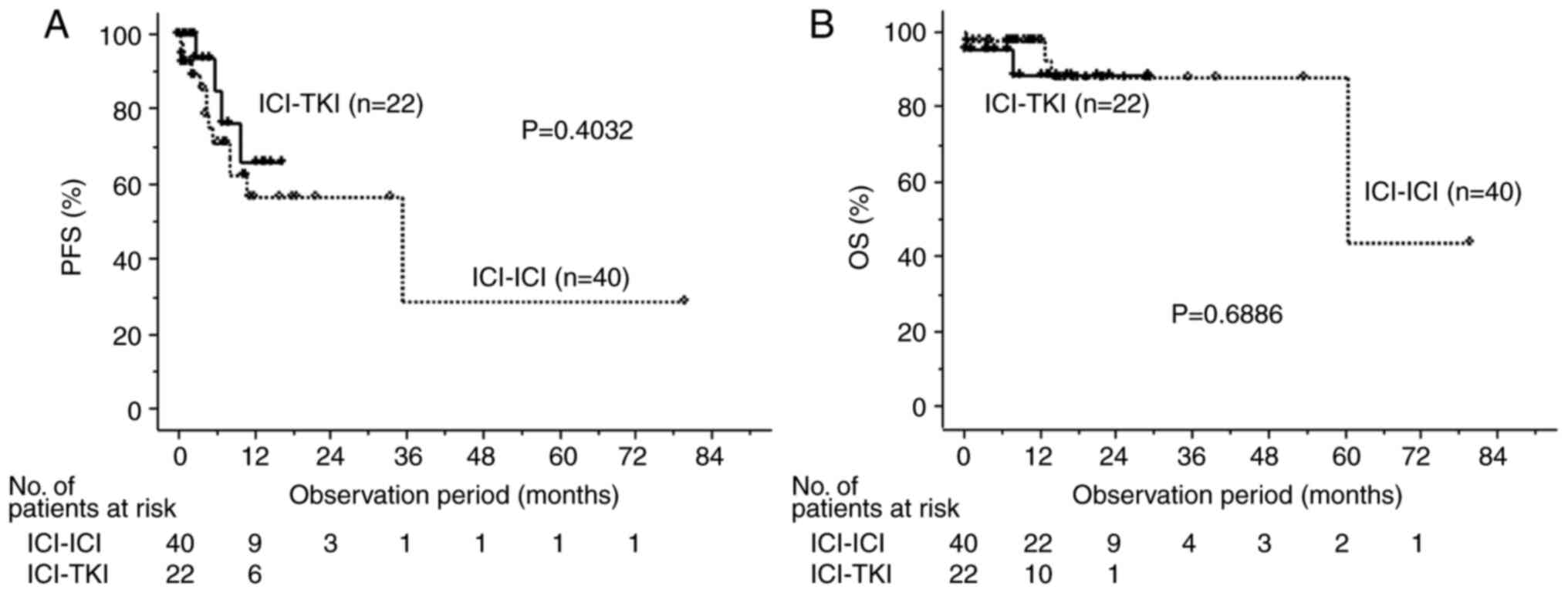
III). In pattern A, the 50% PFS times of the ICI–ICI and the
ICI-TKI groups were 33.6 months and not reached (NR) (Fig. 2A), respectively, and the 50% OS
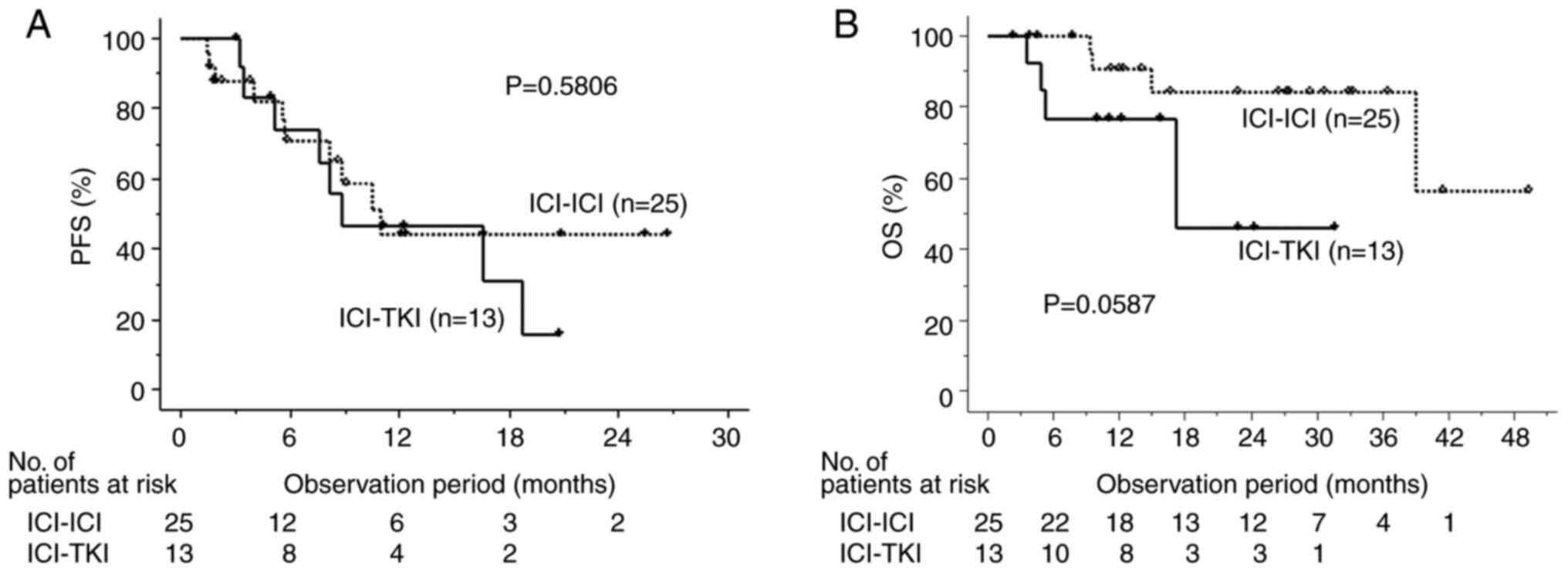
times were 53.7 months and NR, respectively (Fig. 2B). In pattern B, the 50% PFS times
of the ICI–ICI and ICI-TKI groups were 10.5 and 8.2 months
(Fig. 3A), respectively, and the
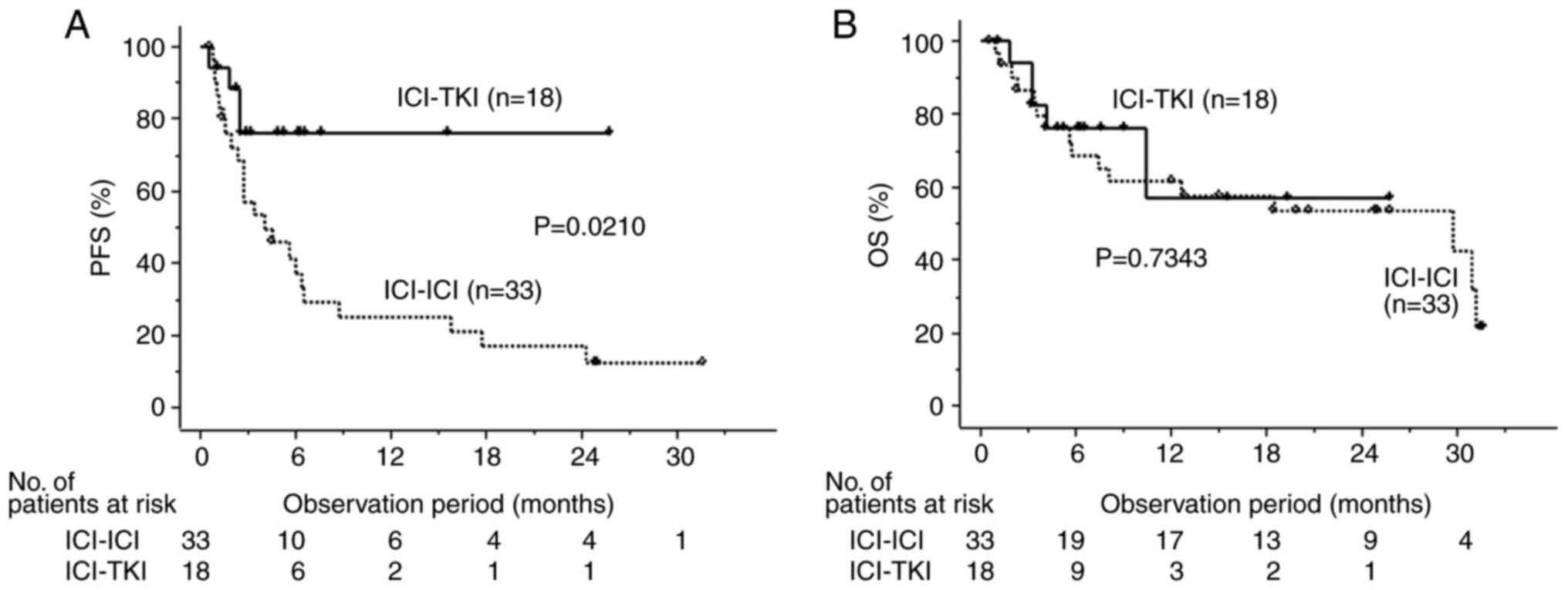
50% OS times were NR and 15.8 months, respectively (Fig. 3B). In pattern C, the 50% PFS time in
the ICI-TKI group was significantly better than that in the ICI–ICI
group (4.1 months and NR, respectively; Fig. 4A), and the 50% OS time was 29.8
months and NR, respectively (Fig.
4B).
| Table III.OR of first-line therapy in all
patients (n=151), and patterns A (n=58), B (n=38) and C (n=42). |
Table III.
OR of first-line therapy in all
patients (n=151), and patterns A (n=58), B (n=38) and C (n=42).
| A, All patients
(n=151) |
|---|
|
|---|
|
| First-line
combination regimen |
|---|
|
|
|
|---|
| OR | ICI–ICI, n (%)
(n=92) | ICI-TKI, n (%)
(n=46) |
|---|
| CR | 14 (15.2) | 1 (2.2) |
| PR | 28 (30.4) | 30 (65.2) |
| SD | 28 (30.4) | 11 (23.9) |
| PD | 22 (23.9) | 4 (8.7) |
|
| B, Pattern A,
recurrence after radical surgery (n=58) |
|
|
| First-line
combination regimen |
|
|
|
| OR | ICI–ICI, n (%)
(n=39) | ICI-TKI, n (%)
(n=19) |
|
| CR | 9 (23.1) | 1 (5.3) |
| PR | 12 (30.8) | 13 (68.4) |
| SD | 12 (30.8) | 5 (26.3) |
| PD | 6 (15.4) | 0 (0.0) |
|
| C, Pattern B,
mRCC with upfront CN (n=38) |
|
|
| First-line
combination regimen |
|
|
|
| OR | ICI–ICI, n (%)
(n=25) | ICI-TKI, n (%)
(n=13) |
|
| CR | 5 (20.0) | 0 (0.0) |
| PR | 8 (32.0) | 7 (53.8) |
| SD | 8 (32.0) | 4 (30.8) |
| PD | 4 (16.0) | 2 (15.4) |
|
| D, Pattern C,
mRCC without upfront CN (n=42) |
|
|
| First-line
combination regimen |
|
|
|
| OR | ICI–ICI, n (%)
(n=28) | ICI-TKI, n (%)
(n=14) |
|
| CR | 0 (0.0) | 0 (0.0) |
| PR | 8 (28.6) | 10 (71.4) |
| SD | 8 (28.6) | 2 (14.3) |
| PD | 12 (42.9) | 2 (14.3) |
Discussion
The introduction of molecular-targeted agents and
ICIs has changed the therapeutic strategy of systemic therapy for
mRCC in recent years. The use of various combination regimens with
these agents has notably contributed to improved efficacy of
treatment for patients with mRCC (4–8). The
increase in therapeutic options has enabled the selection of
treatment approaches that are expected to be effective for patients
with diverse backgrounds (18,19).
While the number of treatment options has increased, selecting the
most appropriate therapy can be challenging. A previous study
attempted to characterize every regimen by comparing results from
multiple RCTs using network meta-analysis (20). To the best of our knowledge, no RCTs
that directly compare first-line combination regimen options for
mRCC have been performed; therefore, analyses derived from
real-world data will be important in making treatment
selections.
ORR was significantly higher in the ICI-TKI group
than that in the ICI–ICI group, whereas there was no significant
difference in either PFS or OS times when comparing all patients.
However, the backgrounds of patients who had postoperative
recurrence after radical surgery for low-stage RCC, and those who
had metastasis from the initial diagnosis as high-stage RCC were
considered to be different. In addition, since the physician
decides whether to perform upfront CN on the basis of a
comprehensive evaluation of the patient's condition, the
pathophysiology of mRCC may notably vary between those cases where
upfront CN was performed and those where it was not performed. In
particular, the IMDC classification has been reported to be useful
in the prognostic stratification of patients treated with combined
regimens (21). The notable
difference in the distribution of IMDC classification among the
three patterns suggests that they should be separately
examined.
First, in patients with recurrence after radical
surgery (pattern A), satisfactory PFS and OS times, and ORR were
obtained regardless of the selection of the first-line regimen, and
no patient in the ICI-TKI group had PD as the best response. The
proportion of patients with parameters that seemed to represent a
poor prognosis, including non-clear histology, poor KPS and poor
IMDC risk classification, was significantly lower in pattern A than
in other patients with mRCC at initial diagnosis. Additionally,
since recurrence was detected during regular follow-up, the
frequency of patients with multiple sites of metastatic disease was
also significantly lower. These characteristics of metastatic
status were considered to be one of the reasons for the difference
of treatment efficacy and prognosis of patients in pattern B
compared with those in pattern C. The treatment outcome trends in
ORR and PFS differed significantly between patients with and
without upfront CN in patients with mRCC. Patients in pattern B,
i.e. those with mRCC who underwent upfront CN, showed no difference
in ORR, or PFS or OS times between the ICI–ICI and the ICI-TKI
groups.
Second, the frequency of poor IMDC risk cases was
significantly lower in pattern B compared with that in pattern C,
indicating a tendency to choose upfront CN when the overall
condition of the patient was good. A total of ~40% of patients in
the ICI–ICI group had no recurrence, reflecting a trend towards
improved OS in the ICI–ICI group. The results of the current study
suggested that treatment with ICI–ICI may be more likely to be
effective in such cases with relatively improved conditions
(22). These results are consistent
with a previously reported sub-analysis of an RCT showing the
efficacy of ipilimumab + nivolumab therapy for mRCC by the number
of IMDC risk factors (23).
In contrast to pattern B, in patients with mRCC who
did not undergo upfront CN (pattern C), PFS times and ORR in the
ICI-TKI group were significantly higher than those in the ICI–ICI
group. Patients in pattern C had more advanced disease with
multiple metastases than those patients in pattern B, and it was
hypothesized that for many of these patients in pattern C they
would not exhibit a durable response, which is an important feature
of the effect of ICI–ICI therapy. Despite significant differences
in ORR and PFS times, there was no significant difference in OS
times between the two groups. It is biologically reasonable to
assume that TKI-naïve patients who receive ICI–ICI as first-line
therapy will have an improved response when they receive TKI in the
second line or later, and that the ICI-TKI group will have fewer
options for substantial therapy. A previous study also reported
that even though ORR was higher in the ICI-TKI group, there was no
difference in OS times between these regimens because there were
fewer post-treatment options, and since the ICI–ICI group did not
receive TKIs in first-line therapy, better efficacy of TKIs in
subsequent therapy after failure of first-line therapy can be
expected (24). However, patients
in the ICI-TKI group, which offers good PFS times and ORR even in
patients with poor IMDC risk, are more likely to choose surgical
and radiotherapeutic options, including deferred CN and
metastasectomy, for shrinking primary tumors and metastases,
compared with the ICI–ICI group. These options are likely to become
further available with increasing proficiency in the use of various
systemic combination regimens and collaboration with other
departments. In the current study, patients who were administered
for the purpose of presurgical therapy were excluded, and deferred
CN was performed in only one patient. The OS times may be further
improved by multidisciplinary treatment with these aggressive
interventions in the future.
The present study has several limitations. It is
based on the analysis of real-world data and is a retrospective
study with a relatively small sample size. Additionally, different
regimens are included within the ICI-TKI group. The choice of
regimen and whether to perform upfront CN depend on patient
background, as the decision is made by the physician, taking into
account the patient's overall medical condition, thus leading to
potential selection bias in each regimen. Further analyses with a
larger volume and longer follow-up period are warranted to confirm
the findings of the present study.
In conclusion, the outcomes following treatment with
ICI–ICI and ICI-TKI regimens were detected in patients with mRCC,
including in those who exhibited recurrence after radical surgery,
and those who did and did not undergo upfront CN before systemic
therapy. Therapeutic efficacy could be achieved with any regimen in
patients with recurrence after radical surgery, whereas improved
results of PFS and ORR were archived with ICI-TKI in patients
without upfront CN. The efficacy of systemic treatment is more
promising than in the past decade; to further improve the
effectiveness of treatment it is necessary to understand the
characteristics of each regimen, and work towards multidisciplinary
treatment with surgery and radiation therapy.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
ToT, JH, HU, NW, KH, YN, YO and MF contributed to
the conception and design of the study, providing supervision and
drafting the manuscript. JF, TaT, YB and TH contributed to the
conception and design of the study, acquisition of data and
drafting the manuscript. JT and YS contributed to the conception
and design of the study, acquisition of data, drafting and critical
revision of the manuscript, and clinical analysis. YS and YO
confirm the authenticity of the raw data. All authors read and
approved the final manuscript.
Ethics approval and consent to
participate
The protocol of the current study was approved by
the Ethics Committee of Kobe University (approval no. B190010 and
B230087), and was carried out according to the approved guidelines.
No informed consent was obtained due to data anonymization as no
identifying information associated with the participants was
included.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD, Fuchs HE and Jemal
A: Cancer statistics, 2022. CA Cancer J Clin. 72:7–33. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Rini BI, Battle D, Figlin RA, George DJ,
Hammers H, Hutson T, Jonasch E, Joseph RW, McDermott DF, Motzer RJ,
et al: The society for immunotherapy of cancer consensus statement
on immunotherapy for the treatment of advanced renal cell carcinoma
(RCC). J Immunother Cancer. 7:3542019. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Pal SK, Ghate SR, Li N, Swallow E, Peeples
M, Zichlin ML, Perez JR, Agarwal N and Vogelzang NJ: Real-world
survival outcomes and prognostic factors among patients receiving
first targeted therapy for advanced renal cell carcinoma: A
SEER-medicare database analysis. Clin Genitourin Cancer.
15:e573–e582. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Motzer RJ, Tannir NM, McDermott DF, Arén
Frontera O, Melichar B, Choueiri TK, Plimack ER, Barthélémy P,
Porta C, George S, et al: Nivolumab plus ipilimumab versus
sunitinib in advanced renal-cell carcinoma. N Engl J Med.
378:1277–1290. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Motzer RJ, Penkov K, Haanen J, Rini B,
Albiges L, Campbell MT, Venugopal B, Kollmannsberger C, Negrier S,
Uemura M, et al: Avelumab plus axitinib versus sunitinib for
advanced renal-cell carcinoma. N Engl J Med. 380:1103–1115. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rini BI, Plimack ER, Stus V, Gafanov R,
Hawkins R, Nosov D, Pouliot F, Alekseev B, Soulières D, Melichar B,
et al: Pembrolizumab plus axitinib versus sunitinib for advanced
renal-cell carcinoma. N Engl J Med. 380:1116–1127. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Choueiri TK, Powles T, Burotto M, Escudier
B, Bourlon MT, Zurawski B, Oyervides Juárez VM, Hsieh JJ, Basso U,
Shah AY, et al: Nivolumab plus cabozantinib versus sunitinib for
advanced renal-cell carcinoma. N Engl J Med. 384:829–841. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Motzer R, Alekseev B, Rha SY, Porta C, Eto
M, Powles T, Grünwald V, Hutson TE, Kopyltsov E, Méndez-Vidal MJ,
et al: Lenvatinib plus pembrolizumab or everolimus for advanced
renal cell carcinoma. N Engl J Med. 384:1289–1300. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Choueiri TK, Xie W, Kollmannsberger C,
North S, Knox JJ, Lampard JG, McDermott DF, Rini BI and Heng DY:
The impact of cytoreductive nephrectomy on survival of patients
with metastatic renal cell carcinoma receiving vascular endothelial
growth factor targeted therapy. J Urol. 185:60–66. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Bhindi B, Abel EJ, Albiges L, Bensalah K,
Boorjian SA, Daneshmand S, Karam JA, Mason RJ, Powles T and Bex A:
Systematic review of the role of cytoreductive nephrectomy in the
targeted therapy era and beyond: An individualized approach to
metastatic renal cell carcinoma. Eur Urol. 75:111–128. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Singla N, Hutchinson RC, Ghandour RA,
Freifeld Y, Fang D, Sagalowsky AI, Lotan Y, Bagrodia A, Margulis V,
Hammers HJ and Woldu SL: Improved survival after cytoreductive
nephrectomy for metastatic renal cell carcinoma in the contemporary
immunotherapy era: An analysis of the national cancer database.
Urol Oncol. 38:604.e9–604.e17. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hall ME, Bhindi B, Luckenbaugh AN, Laviana
AA, Moses KA, Satkunasivam R, Rini B, Klaassen Z and Wallis CJD:
Association between cytoreductive nephrectomy and survival among
patients with metastatic renal cell carcinoma receiving modern
therapies: A systematic review and meta-analysis examining effect
modification according to systemic therapy approach. Cancer Causes
Control. 32:675–680. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Bex A, Mulders P, Jewett M, Wagstaff J,
van Thienen JV, Blank CU, van Velthoven R, Del Pilar Laguna M, Wood
L, van Melick HHE, et al: Comparison of immediate vs deferred
cytoreductive nephrectomy in patients with synchronous metastatic
renal cell carcinoma receiving sunitinib: The SURTIME randomized
clinical trial. JAMA Oncol. 5:164–170. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Méjean A, Ravaud A, Thezenas S, Colas S,
Beauval JB, Bensalah K, Geoffrois L, Thiery-Vuillemin A, Cormier L,
Lang H, et al: Sunitinib alone or after nephrectomy in metastatic
renal-cell carcinoma. N Engl J Med. 379:417–427. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Heng DYC, Xie W, Regan MM, Warren MA,
Golshayan AR, Sahi C, Eigl BJ, Ruether JD, Cheng T, North S, et al:
Prognostic factors for overall survival in patients with metastatic
renal cell carcinoma treated with vascular endothelial growth
factor-targeted agents: Results from a large, multicenter study. J
Clin Oncol. 27:5794–5799. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Yates JW, Chalmer B and McKegney FP:
Evaluation of patients with advanced cancer using the Karnofsky
performance status. Cancer. 45:2220–2224. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Stühler V, Herrmann L, Rausch S, Stenzl A
and Bedke J: Real world data on IO-based therapy for metastatic
renal cell carcinoma. J Cancer Res Clin Oncol. 149:3249–3258. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Iinuma K, Yamada T, Kameyama K, Taniguchi
T, Kawada K, Ishida T, Nagai S, Enomoto T, Ueda S, Takagi K, et al:
The efficacy and safety of immune checkpoint inhibitor and tyrosine
kinase inhibitor combination therapy for advanced or metastatic
renal cell carcinoma: A multicenter retrospective real-world cohort
study. Cancers (Basel). 15:9472023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bosma NA, Warkentin MT, Gan CL, Karim S,
Heng DYC, Brenner DR and Lee-Ying RM: Efficacy and safety of
first-line systemic therapy for metastatic renal cell carcinoma: A
systematic review and network meta-analysis. Eur Urol Open Sci.
37:14–26. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ernst MS, Navani V, Wells JC, Donskov F,
Basappa N, Labaki C, Pal SK, Meza L, Wood LA, Ernst DS, et al:
Outcomes for international metastatic renal cell carcinoma database
consortium prognostic groups in contemporary first-line combination
therapies for metastatic renal cell carcinoma. Eur Urol.
84:109–116. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Hara T, Furukawa J, Shiraishi Y, Okamura
Y, Bando Y, Terakawa T, Harada K, Nakano Y and Fujisawa M: Impact
of cytoreductive nephrectomy prior to combination therapy of
ipilimumab plus nivolumab in metastatic renal cell carcinoma. Int J
Urol. May 2–2023.(Epub ahead of print). View Article : Google Scholar
|
|
23
|
Escudier B, Motzer RJ, Tannir NM, Porta C,
Tomita Y, Maurer MA, McHenry MB and Rini BI: Efficacy of nivolumab
plus ipilimumab according to number of IMDC risk factors in
CheckMate 214. Eur Urol. 77:449–453. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Dudani S, Graham J, Wells JC, Bakouny Z,
Pal SK, Dizman N, Donskov F, Porta C, de Velasco G, Hansen A, et
al: First-line immuno-oncology combination therapies in metastatic
renal-cell carcinoma: Results from the international metastatic
renal-cell carcinoma database consortium. Eur Urol. 76:861–867.
2019. View Article : Google Scholar : PubMed/NCBI
|