Introduction
Merkel cell carcinoma (MCC) is a rare primary
neuroendocrine carcinoma of the skin, which was first reported in
1972 and named ‘cutaneous trabecular carcinoma’ based on its
histopathological features (1). The
incidence of MCC has increased over the past few decades, with
studies revealing that the annual incidence of MCC rose from 0.5
per 1,000 individuals in 2000 to 0.7 per 1,000 individuals in 2013
(2–4). MCC is usually observed in
light-skinned older adults, most often in sun-damaged areas of the
skin. The carcinoma presents as a fast-growing, soft to elastic,
non-indurated intradermal nodule that is flesh-colored, bluish red
or purple and shiny, with a high degree of malignancy. Since 2009,
the National Comprehensive Cancer Network (NCCN) in the United
States has been releasing guidelines for the treatment of patients
with MCC. According to the latest NCCN guidelines, surgical
resection and adjuvant radiotherapy are still the preferred
strategies for treating local diseases. However, 80–90% of patients
with MCC experience recurrence within 2 years after treatment, with
a mortality rate of >80% (5). It
is not entirely unusual to diagnose a lymph node with metastasis of
MCC, but it is difficult to determine the primary location of the
tumor (6). Moreover, MCC is
considered to undergo spontaneous total or partial regression of
the primary tumor, and fluorine-18-fluorodeoxyglucose positron
emission tomography/computed tomography (18F-FDG PET/CT)
can be used to localize tumors with partial regression. The current
case study presents the diagnosis and treatment of a patient with
MCC of the eyelid, focusing on its imaging manifestations and
reviewing the relevant literature to increase awareness of this
rare disease.
Case report
A 79-year-old female patient visited the Affiliated
Hospital of Zunyi Medical University (Zunyi, China) in September
2021 due to painless swelling of the lower eyelid of the left eye
for 4 months, with photophobic tears. The patient had no personal
or family history of tumors. A physical examination showed that the
patient's left eyelid was red and swollen, and an irregular mass
was visible on the lower eyelid that was ~2.0×1.8 cm, felt hard,
and had poor mobility and an unclear boundary with the surrounding
tissues. The patient also experienced tenderness in the left
eyeball but had no other positive signs in the rest of the body.
Routine blood counts and serum tumor marker levels were within the
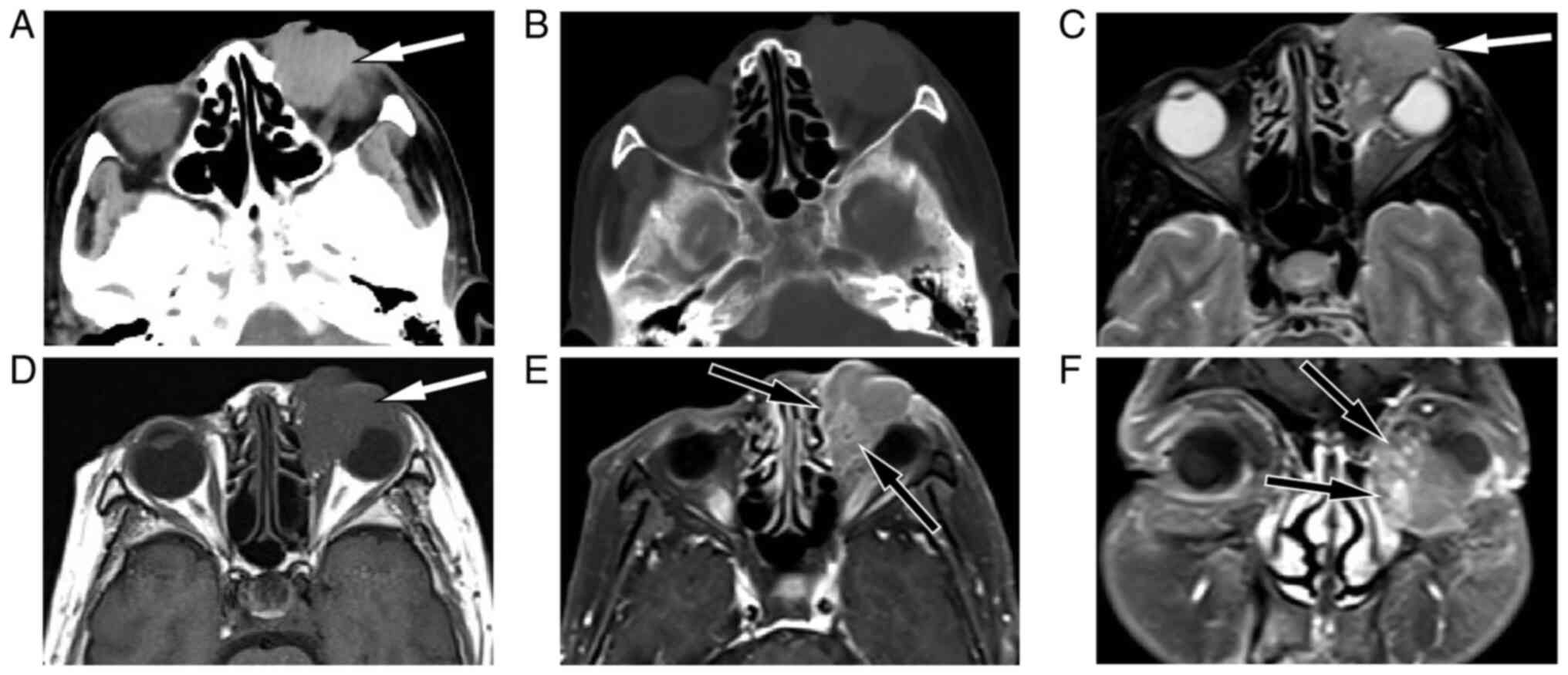
normal reference values. CT and magnetic resonance imaging (MRI) of
the head revealed a space-occupying lesion outside the left orbital
muscle cone that was poorly demarcated from the surrounding normal
tissue (Fig. 1). To further
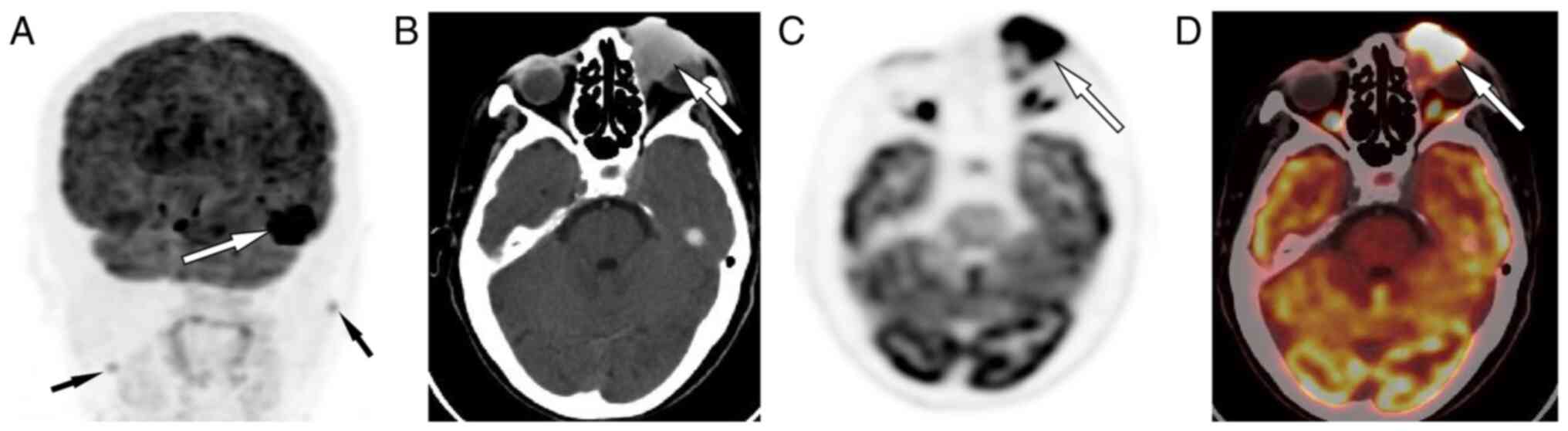
evaluate the presence of distant metastases, the patient underwent
18F-FDG PET/CT, which showed significantly increased
18F-FDG uptake at the corresponding lesion and
additional bilateral lesions in the neck with increased
18F-FDG uptake (Fig. 2).
Based on these findings, a malignant tumor of the left eyelid with
bilateral cervical lymph node metastases was suspected.
After talking to the patient and obtaining the
consent of the family, the patient underwent left eyelid mass
resection, left eyeball enucleation and bilateral neck lymph node
dissection. The excised lesion tissues were sent for postoperative
pathological examination. For hematoxylin-eosin staining (Fuzhou
Maixin Biotech Co., Ltd.), the specimen was fixed with 10% neutral
formalin, dehydrated at room temperature for ~24 h and paraffin
embedded. Next, 3- to 4-µm thick sections were stained with
hematoxylin and eosin (25°C, 5–10 min), and viewed at ×400
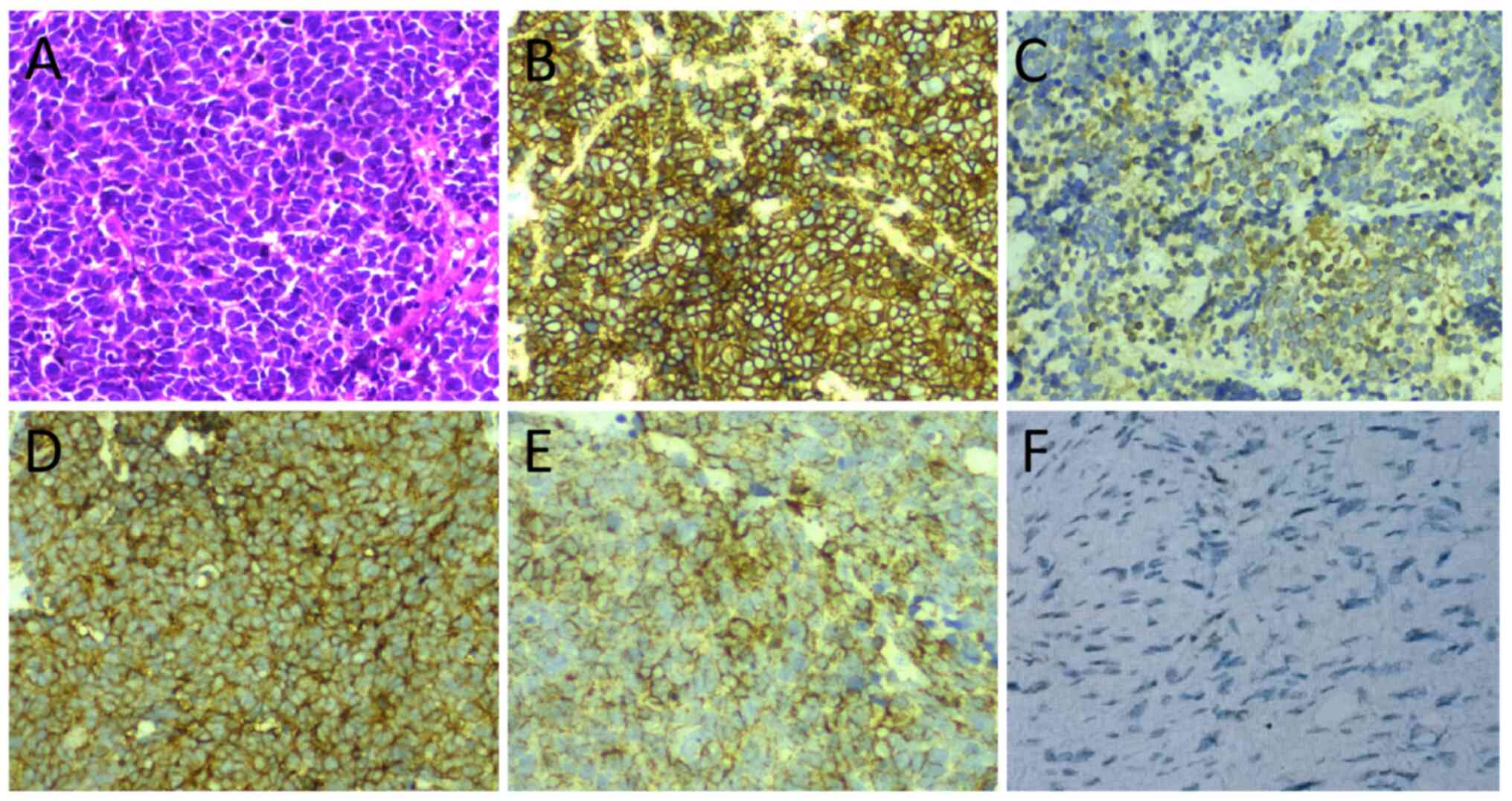
magnification under an optical microscope. Microscopically, there
was extensive occurrence of mitoses in the tumor tissues, and a
diffuse distribution of uniformly sized round or ovoid tumor cells,
with sparse cytoplasm and large, deeply stained nuclei (Fig. 3). Further immunohistochemistry (all
specimens were fixed with 10% neutral formalin, dehydrated at room
temperature for ~24 h and paraffin embedded. The 3- to 4-µm thick
sections were stained for creatine kinase, CD56, cytokeratin (CK),
CK20, synaptophysin, S-100 and Ki-67, with antibodies purchased
from Fuzhou Maixin Biotech Co., Ltd., and viewed at ×400
magnification under an optical microscope. The results showed that
the tumor cells positively expressed CD56, CK, CK20 and
synaptophysin, but did not express S-100. The Ki-67 index was ~40%,
and the diagnosis of MCC was made. The pathological examination
revealed bilateral inflammatory lesions in the lymph nodes of the
neck; however, no tumor cells were observed. The patient did not
undergo radiotherapy or chemotherapy after surgery and was
discharged from the hospital after 1 week of anti-inflammatory
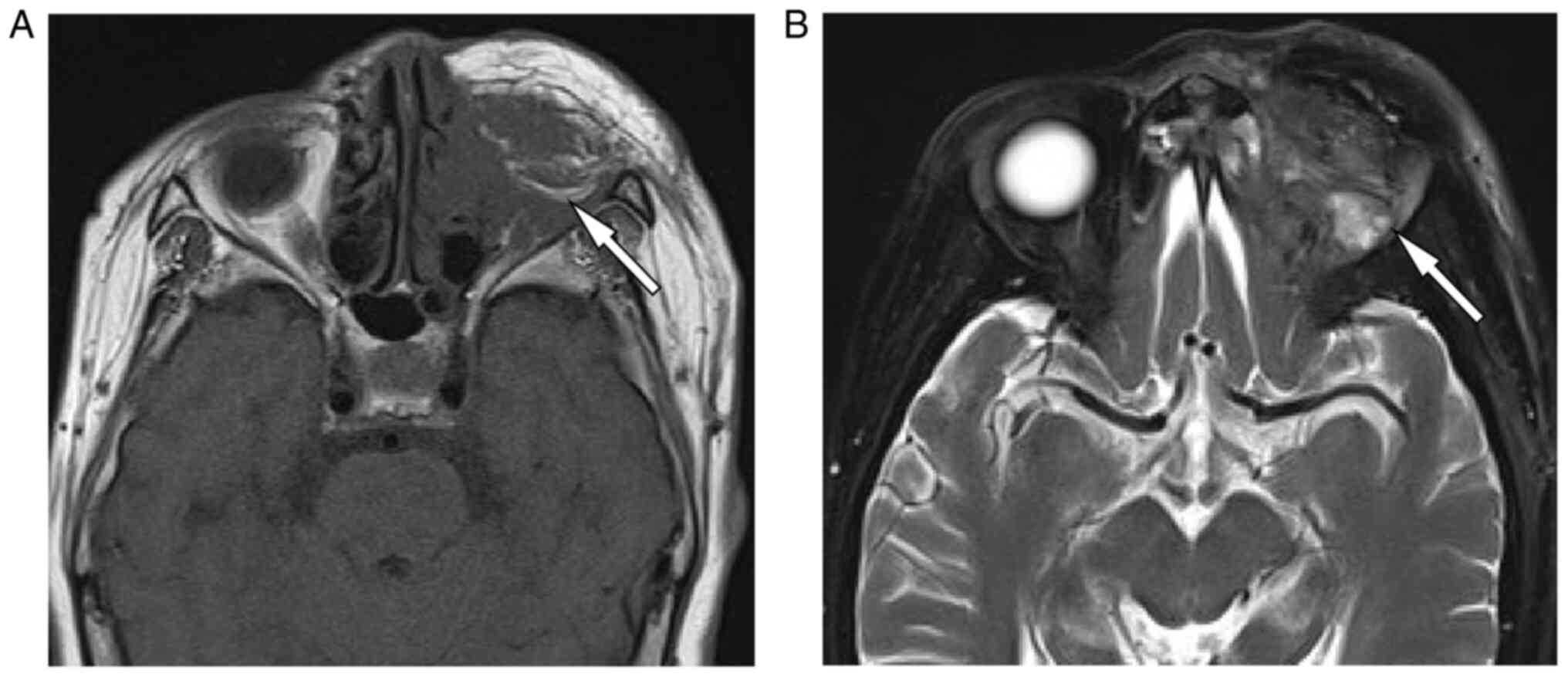
therapy (1–2 g cefixime, twice a day). At 7 months post-discharge,
the patient returned to the hospital as they felt a mass in the
surgical area of the left eye. A larger mass with abnormal signals
in the surgical area of the left eye, suggesting tumor recurrence,
was revealed by MRI (Fig. 4).
However, the patient refused treatment and was lost to follow-up.
As recurrence was exhibited 7 months after the operation, the
patient prognosis was likely to be poor.
Discussion
The etiology of MCC may be related to Merkel cell
polyomavirus infection, immunosuppression or ultraviolet radiation
(7). The origin of cancer cells in
MCC remains controversial; tumor cells have the same morphological
and histological features as normal Merkel cells, with no evidence
of direct evolution of normal Merkel cells into tumor cells, and no
benign or abnormally developed precursor lesions (8). The tissue origin, which is currently
hypothesized to be dermal or epidermal stem cells and precursor B
cells, is controversial (9). The
overall incidence of MCC is low, although studies have revealed a
high incidence in patients with lymphoproliferative malignancies,
solid organ transplantation and HIV infection. The onset of MCC
occurs at an older age, with a median age of >70 years (10,11).
Most MCCs present as fast-growing, painless nodules or lumps on the
skin (10). The present study
reports the case of a 79-year-old patient with a mass located in
the lower eyelid of the left eye, an area susceptible to
ultraviolet damage from the sun, consistent with the prevalent
elements of MCC. The clinical presentation of a rapidly enlarging
painless soft-tissue mass over a short period in the lower eyelid
is also consistent with the clinical presentation of MCC reported
in the literature.
At present, there are few imaging studies on eyelid
MCC, which may be related to the shallow location of the tumor and
the ease of sample collection for direct pathological biopsy.
Although the imaging features of MCC are considered non-specific, a
review of previously published cases of eyelid MCC identified some
common imaging features that may contribute to our understanding of
this rare solid tumor. On CT, the mass often appears to have a
uniform density slightly higher than that of the surrounding normal
soft tissue, with a few low-density cystic areas, high-density
bleeding and calcification foci within the tumor (12–14).
The MRI features of MCC in the eyelid have not been reported in the
literature, although some studies have revealed that MCC
originating from other locations presents with a slightly hypo- to
isointense signal on T1-weighted imaging (T1WI) and an iso- to
hyperintense signal on T2WI or fat-suppression T2WI (15,16).
On contrast-enhanced T1WI, lesions usually show mild, diffuse,
uneven enhancement, and larger lesions may result in unenhanced
cystic necrosis within the tumor (15). The present patient showed a uniform,
slightly high density mass on CT, without cystic necrosis,
hemorrhage or calcification. On MRI, T1WI showed an isointense
signal, T2WI showed a slightly hyperintense signal and
contrast-enhanced T1WI showed mild uneven enhancement with
significantly enhanced distorted vascular shadows, consistent with
the findings of the aforementioned literature. MCC is a highly
aggressive tumor with active glucose metabolism, showing strong
uptake of 18F-FDG on PET. The mean maximum standardized
uptake value (SUVmax) is 4.0–6.5 on 18F-FDG
PET/CT for primary MCC (17,18).
The present patient showed stronger uptake of 18F-FDG on
PET/CT, with an SUVmax of 12.8.
Imaging techniques, including CT, MRI and PET/CT,
are essential in the management of MCC, including assessing the
extent of tumor invasion, guiding the surgical plan and
radiotherapy area, and tumor staging. Studies analyzing the
performance of MRI using histomorphometric and immunohistochemical
results have found that MRI has a significant advantage in the
visualization of MCC foci and adjacent metastases, which can help
in the planning of targeted volumetric radiation therapy and
documentation of tumor characteristics to assess the tumor response
to therapy (1,19–21).
MCC can develop into osteogenic or osteolytic metastases. Bone
marrow involvement and extraosseous invasion is more likely to be
detected by MRI than by CT; however, CT has the advantage of
assessing changes in bone quality. New manifestations of
osteosclerosis on CT may originate from a response to therapy or
suggest lesion progression (19,22).
In patients with bone metastases treated with radiotherapy or
systemic therapy, the metabolic changes shown by
18FDG-PET are highly reliable, and a reduction in
metabolism shown by 18FDG-PET suggests better outcomes
(19).
Based on the clinical presentation and imaging
features of eyelid MCC, the differential diagnoses include basal
cell carcinoma, squamous cell carcinoma, eyelid adenocarcinoma,
melanoma and chalazion. The lesion location of basal cell carcinoma
is relatively shallow, mostly located in the lower eyelid near the
inner canthus, and can form a nibbling ulcer in the late stage of
the lesion. Metastasis rarely occurs (23). Squamous cell carcinoma is a
superficial nodular mass that often protrudes from the surface of
the skin and typically shows an isointense signal on T1WI and a
slightly high signal on T2WI, with uneven enhancement and
hyperperfusion on enhancement. The carcinoma may invade the
adjacent skin or superficial fascia with creeping growth and
blurred margins (24).
Adenocarcinoma of the eyelid is rare and usually occurs in elderly
individuals with heterogeneous densities or signals on CT or MRI.
During growth, it is characterized on images by an ‘arcuate sign’
in the posterior part of the lesion owing to obstruction of the
posterior ocular ring, and the arcuate structure may be disrupted
(25). Typical melanomas tend to
present as superficial skin-pigmented spots or nodules with or
without irregular borders and ulcers, and MRI shows a specific T1
high signal and a T2 low signal (26). Chalazion is a less likely
differential diagnosis, as it is located at the margin of the
eyelid, has a smooth surface and occurs preferentially in young
people, while the elderly exhibit gland atrophy with impaired
lacrimation (27).
Histopathological examination is the gold standard
for the diagnosis of MCC. Microscopically, relatively uniform tumor
cells are diffusely arranged, trabecular, nested or mixed, and
frequently infiltrate the dermis or subcutaneous tissue, whereas
the epidermis is usually not involved (28). MCC shows epithelial and
neuroendocrine differentiation characteristics; therefore, tumor
cells often express epithelial CK, neuroendocrine substances,
including chromogranin A, neuron-specific enolase, CD56 and villus
proteins, and neural markers such as the S-100 protein (29). Histopathological examination of the
patient in the present study showed that the tumor cells were
uniform in size, with a circular or oval diffuse distribution,
sparse cytoplasm, large nuclei, deep staining and positive
expression of CD56, CK, CK20 and synaptophysin, which was
consistent with the pathological and immunohistochemical
characteristics of MCC, and the diagnosis was clear.
The National Comprehensive Cancer Network guidelines
for the treatment of MCC state that surgical resection is
preferred, using a wide resection with 1- to 2-cm margins when
clinically feasible (30). However,
the operative method of enlargement and re-excision of the tumor is
more limited in the eyelid area and is prone to recurrence after
surgery (31). Some studies have
shown that even in the absence of metastasis, postoperative
adjuvant radiotherapy for tumors >1.0 cm in diameter results in
a lower recurrence rate (30,32).
Adjuvant chemotherapy is needed for MCC cases with definite lymph
node and distant metastases. However, the chemotherapy regimen is
not standardized, and one published study showed that good results
were achieved with the use of cyclophosphamide, doxorubicin and
vincristine (11). In recent years,
advancements in immunotherapy have greatly extended the survival
times of patients with metastatic MCC, especially with the use of
immunotherapy involving the programmed death 1 and programmed death
ligand 1 pathways. In particular, avelumab, the first drug
specifically for metastatic MCC approved by the US Food and Drug
Administration in March 2017, showed an overall response rate of
32% and a complete response rate of 11% in patients in whom
chemotherapy had failed (33). The
overall prognosis for MCC is poor. The overall 5-year survival rate
of patients with MCC without metastasis is 64%, whereas the 5-year
survival rate of patients with lymph node or distant metastases
decreases to 39 and 18%, respectively (34). Risk factors for a poor prognosis
include a tumor diameter >1 cm, a location in the head and neck
region, lymphovascular invasion and an immunocompromised status,
whereas a tumor diameter >2 cm is an independent risk factor for
patient death (31). The present
patient had no radiotherapy or chemotherapy after surgical removal
of the tumor, and the tumor recurred in the ninth postoperative
month, illustrating the highly aggressive nature of MCC.
As the focus of the present study is to discuss the
multimodal imaging features of eyelid MCC, only the pathological
diagnosis of this patient was reviewed and colleagues from the
Department of Pathology were not invited to join the study, which
is a shortcoming of the study. However, the current study still
provides a reference for imaging findings in the diagnosis of such
a rare entity as eyelid MCC.
In conclusion, the current study reports the
multimodal imaging features, including CT, MRI and PET/CT, of a
rare tumor, eyelid MCC. A slightly hyperdense mass on CT, with
equal T1 signals and slightly longer T2 signals on MRI, and mild
enhancement on contrast-enhanced scans, accompanied by
significantly enhanced distorted vascular shadows and increased
18F-FDG uptake on PET/CT are valuable for diagnosing
eyelid MCC. Eyelid MCC has a poor prognosis, and new methods to
improve its prognosis must be explored in future studies.
Acknowledgements
The authors would like to thank Professor Tan Na
(Department of Pathology, Affiliated Hospital of Zunyi Medical
University, Zunyi, China) for contributing to the interpretation of
the pathological diagnosis of this patient.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
GZ and LX conceived and designed the study. XH
acquired, analyzed and interpreted the data. GZ and LX confirm the
authenticity of all the raw data. GZ drafted the manuscript. XH
critically revised the manuscript for intellectual content and
approved the final version for publication. All authors agree to
the journal to which the article was submitted and take
responsibility for all aspects of the work. All authors have read
and approved the final version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of The Affiliated Hospital of Zunyi Medical University
(Zunyi, China; approval no. KLL-2023-186).
Patient consent for publication
Written informed consent was obtained from the
patient to publish this case report.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Toker C: Trabecular carcinoma of the skin.
Arch Dermatol. 105:107–110. 1972. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Paulson KG, Park SY, Vandeven NA, Lachance
K, Thomas H, Chapuis AG, Harms KL, Thompson JA, Bhatia S, Stang A
and Nghiem P: Merkel cell carcinoma: Current US incidence and
projected increases based on changing demographics. J Am Acad
Dermatol. 78:457–463.e2. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zaar O, Gillstedt M, Lindelöf B,
Wennberg-Larkö AM and Paoli J: Merkel cell carcinoma incidence is
increasing in Sweden. J Eur Acad Dermatol Venereol. 30:1708–1713.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fondain M, Dereure O, Uhry Z, Guizard AV,
Woronoff AS, Colonna M, Molinie F, Bara S, Velten M, Marrer E, et
al: Merkel cell carcinoma in France: A registries-based,
comprehensive epidemiological survey. J Eur Acad Dermatol Venereol.
32:1292–1296. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Coggshall K, Tello TL, North JP and Yu SS:
Merkel cell carcinoma: An update and review: Pathogenesis,
diagnosis, and staging. J Am Acad Dermatol. 78:433–442. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Fazio N, Maisonneuve P, Spada F, Gervaso
L, Cella CA, Pozzari M, Zerini D, Pisa E, Fumagalli C, Barberis M,
et al: Nodal merkel cell carcinoma with unknown primary site and no
distant metastasis: A single-center series. Cancers (Basel).
14:47772022. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Feng H, Shuda M, Chang Y and Moore PS:
Clonal integration of a polyomavirus in human Merkel cell
carcinoma. Science. 319:1096–1100. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Moll I, Zieger W and Schmelz M:
Proliferative Merkel cells were not detected in human skin. Arch
Dermatol Res. 288:184–187. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Zur Hausen A, Rennspiess D, Winnepenninckx
V, Speel EJ and Kurz AK: Early B-cell differentiation in Merkel
cell carcinomas: Clues to cellular ancestry. Cancer Res.
73:4982–4987. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zaggana E, Konstantinou MP, Krasagakis GH,
de Bree E, Kalpakis K, Mavroudis D and Krasagakis K: Merkel cell
carcinoma-update on diagnosis, management and future perspectives.
Cancers (Basel). 15:1032022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Tello TL, Coggshall K, Yom SS and Yu SS:
Merkel cell carcinoma: An update and review: Current and future
therapy. J Am Acad Dermatol. 78:445–454. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Chen L, Zhu L, Wu J, Lin T, Sun B and He
Y: Giant Merkel cell carcinoma of the eyelid: A case report and
review of the literature. World J Surg Oncol. 9:582011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Watanabe N, Shimizu M, Kageyama M,
Kitagawa K, Hayasaka S and Seto H: 123I-MIBG SPECT of Merkel cell
carcinoma. Br J Radiol. 71:886–887. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Feng Y, Song X and Jia R: Case Report:
Favorable response to the tyrosine kinase inhibitor apatinib in
recurrent merkel cell carcinoma. Front Oncol. 11:6253602021.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dunlop P, Sapp H, Logan PM and Walsh NM:
Merkel cell carcinoma of the abdominal wall. Skeletal Radiol.
27:396–399. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Moayed S, Maldjianb C, Adam R and
Bonakdarpour A: Magnetic resonance imaging appearance of metastatic
Merkel cell carcinoma to the sacrum and epidural space. Magn Reson
Imaging. 18:1039–1042. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hawryluk EB, O'Regan KN, Sheehy N, Guo Y,
Dorosario A, Sakellis CG, Jacene HA and Wang LC: Positron emission
tomography/computed tomography imaging in Merkel cell carcinoma: A
study of 270 scans in 97 patients at the Dana-Farber/Brigham and
Women's Cancer Center. J Am Acad Dermatol. 68:592–599. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Concannon R, Larcos GS and Veness M: The
impact of (18)F-FDG PET-CT scanning for staging and management of
Merkel cell carcinoma: Results from Westmead Hospital, Sydney,
Australia. J Am Acad Dermatol. 62:76–84. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Akaike G, Akaike T, Fadl SA, Lachance K,
Nghiem P and Behnia F: Imaging of merkel cell carcinoma: What
imaging experts should know. Radiographics. 39:2069–2084. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Peloschek P, Novotny C, Mueller-Mang C,
Weber M, Sailer J, Dawid M, Czerny C, Dudczak R, Kletter K and
Becherer A: Diagnostic imaging in Merkel cell carcinoma: Lessons to
learn from 16 cases with correlation of sonography, CT, MRI and
PET. Eur J Radiol. 73:317–323. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Kim HJ, Lee KC, Kang CH, Ahn KS and Kim
CH: Characteristic imaging features of merkel cell carcinoma: A
case report. Curr Med Imaging. 17:562–566. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Enzenhofer E, Ubl P, Czerny C and Erovic
BM: Imaging in patients with merkel cell carcinoma. J Skin Cancer.
2013:9731232013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Shoji MK, Tran AQ, Lazzarini TA, Choi CJ
and Tse BC: Basal cell carcinoma and eccrine porocarcinoma of the
eyelid. Ophthalmic Plast Reconstr Surg. 37:e53–e56. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Tang M, Huang R, Chen J, Sheng M, Zhang Z,
Xing J, Guo L and Li Y: Clinical value of high-resolution dynamic
contrast-enhanced (DCE) MRI in diagnosis of cutaneous squamous cell
carcinoma. Skin Res Technol. 27:511–520. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Soror NN, Lutaya I, Shah P, Hemrock L,
Bennett R and Gibson G: A rare case of primary adenocarcinoma of
the eyelid: Case presentation and review of literature. Cureus.
13:e165802021.PubMed/NCBI
|
|
26
|
Barat M, Guegan-Bart S, Cottereau AS,
Guillo E, Hoeffel C, Barret M, Gaujoux S, Dohan A and Soyer P: CT,
MRI and PET/CT features of abdominal manifestations of cutaneous
melanoma: A review of current concepts in the era of tumor-specific
therapies. Abdom Radiol (NY). 46:2219–2235. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Evans J, Vo KBH and Schmitt M: Chalazion:
Racial risk factors for formation, recurrence, and surgical
intervention. Can J Ophthalmol. 57:242–246. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Schrama D, Sarosi EM, Adam C, Ritter C,
Kaemmerer U, Klopocki E, König EM, Utikal J, Becker JC and Houben
R: Characterization of six Merkel cell polyomavirus-positive Merkel
cell carcinoma cell lines: Integration pattern suggest that large T
antigen truncating events occur before or during integration. Int J
Cancer. 145:1020–1032. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kervarrec T, Tallet A,
Miquelestorena-Standley E, Houben R, Schrama D, Gambichler T,
Berthon P, Le Corre Y, Hainaut-Wierzbicka E, Aubin F, et al:
Diagnostic accuracy of a panel of immunohistochemical and molecular
markers to distinguish Merkel cell carcinoma from other
neuroendocrine carcinomas. Mod Pathol. 32:499–510. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bichakjian CK, Olencki T, Aasi SZ, Alam M,
Andersen JS, Blitzblau R, Bowen GM, Contreras CM, Daniels GA,
Decker R, et al: Merkel Cell Carcinoma, Version 1.2018, NCCN
Clinical Practice Guidelines in Oncology. J Natl Compr Canc Netw.
16:742–774. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Dasanu CA, Del Rosario M, Codreanu I,
Hyams DM and Plaxe SC: Inferior outcomes in immunocompromised
Merkel cell carcinoma patients: Can they be overcome by the use of
PD1/PDL1 inhibitors. J Oncol Pharm Pract. 25:214–216. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Frohm ML, Griffith KA, Harms KL, Hayman
JA, Fullen DR, Nelson CC, Wong SL, Schwartz JL and Bichakjian CK:
Recurrence and survival in patients with merkel cell carcinoma
undergoing surgery without adjuvant radiation therapy to the
primary site. JAMA Dermatol. 152:1001–1007. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kaufman HL, Russell J, Hamid O, Bhatia S,
Terheyden P, D'Angelo SP, Shih KC, Lebbé C, Linette GP, Milella M,
et al: Avelumab in patients with chemotherapy-refractory metastatic
Merkel cell carcinoma: A multicentre, single-group, open-label,
phase 2 trial. Lancet Oncol. 17:1374–1385. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lemos BD, Storer BE, Iyer JG, Phillips JL,
Bichakjian CK, Fang LC, Johnson TM, Liegeois-Kwon NJ, Otley CC,
Paulson KG, et al: Pathologic nodal evaluation improves prognostic
accuracy in Merkel cell carcinoma: Analysis of 5823 cases as the
basis of the first consensus staging system. J Am Acad Dermatol.
63:751–761. 2010. View Article : Google Scholar : PubMed/NCBI
|