Introduction
Lung adenocarcinoma (LUAD) is the most common
subtype of non-small cell lung carcinoma (NSCLC), accounting for
40–50% of cases, characterized by a high histological, cellular and
molecular heterogeneity (1–3). Positive driver genes are detected in
most patients with LUAD, and with the emergence of targeted
therapies, the 1-year survival rates of these patients receiving
targeted therapy have been improved compared with those receiving
chemotherapy (24 vs. 9%) (4–8).
However, ~10% of patients with advanced LUAD carry negative driver
genes (9,10). According to the National
Comprehensive Cancer Network (NCCN) Clinical Practice Guidelines in
Oncology, chemotherapy is the recommended treatment for patients
with advanced LUAD carrying negative driver genes. However, certain
patients do not respond well to chemotherapy, and there is a lack
of effective treatment options for those patients (11,12).
Therefore, exploring potential treatments for patients with
advanced LUAD carrying negative driver genes is necessary.
Apatinib is an orally-administered, small-molecule
vascular endothelial growth factor receptor-2 inhibitor that
suppresses tumor angiogenesis (13). Recent studies have reported the
potential benefit of apatinib plus chemotherapy for the treatment
of advanced NSCLC (14–16). For instance, the overall remission
rate has been reported to be improved by apatinib plus chemotherapy
vs. chemotherapy alone in patients with advanced NSCLC (37 vs. 10%,
respectively) (15). However,
evidence for patients with advanced NSCLC carrying negative driver
genes is scarce, and only one study has reported that the median
progression-free survival (PFS; 5.47 vs. 2.97 months) and disease
control rate (DCR; 95 vs. 73%) are increased following second-line
apatinib plus chemotherapy compared with chemotherapy alone in
patients with advanced NSCLC carrying negative driver genes
(16). In addition, that study had
several limitations, such as a small sample size (n=33), and it
only assessed the potential of apatinib plus chemotherapy as a
second-line treatment (16).
Therefore, the effect of apatinib plus chemotherapy in patients
with advanced LUAD carrying negative driver genes requires further
exploration.
The present study included 145 patients with
advanced LUAD carrying negative driver genes to assess the efficacy
and safety of apatinib plus chemotherapy compared with chemotherapy
alone.
Patients and methods
Patients
A total of 145 patients with advanced LUAD who
underwent treatment with either apatinib plus chemotherapy or
chemotherapy alone between February 2019 and November 2022 at the
Yueqing People's Hospital (Yueqing, China) were included in the
present study. Specifically, 61 patients were retrospectively
recruited before July 2020. Considering the number of patients was
relatively small, 84 patients were prospectively recruited between
July 2020 and November 2022. The inclusion criteria were as
follows: i) Diagnosis of LUAD by histopathological examination; ii)
>18 years; iii) presence of negative driver genes (epidermal
growth factor receptor, anaplastic lymphoma kinase and reactive
oxygen species proto-oncogene 1, receptor tyrosine kinase);
Next-generation sequencing was carried out by 3D Medicines Inc. to
identify gene mutations (17); iv)
tumor-node-metastasis (TNM) stage IIIB-IV (18); v) treatment with either apatinib
plus chemotherapy or chemotherapy alone; and vi) accessible and
available data on clinical characteristics, treatment, radiological
results and follow-up. The exclusion criteria were as follows: i)
History of other malignancies prior to being diagnosed with LUAD;
and ii) pregnancy or lactation. The present study was approved by
the Medical Ethics Committee of Yueqing Hospital Affiliated to
Wenzhou Medical University (Yueqing, China; approval no.
YQYY202001003), and written informed consent was obtained from the
patients or their guardians.
Next-generation sequencing
Next-generation sequencing using Illumina, Inc.
technology was carried out by 3D Medicines Inc. to identify gene
mutations. The kit used to prepare DNA/RNA samples for sequencing
was FFPE automation (cat. no. 3103010048; 3D Medicines Inc.). The
method used to verify the quality/integrity of the processed
samples was Agilent 4200 (Agilent Technologies, Inc.), and the type
of sequencing was double-ended, 2×150. The sequencing kit used was
DNBSEQ-T7RS High-Throughput Sequencing Reagent Kit (App-A FCL
PE150; version 2.0; cat. no. 940-000003-00; MGI Tech Co., Ltd.).
The loading concentration of the final library was ≥33 nM measured
using Qubit (Thermo Fisher Scientific, Inc.). The software used to
analyze the data included: i) AdapterRemoval (version 2.3.1;
http://adapterremoval.readthedocs.io/en/stable/index.html)
was used for preprocessing; ii) Sentieon-bwa (version 0.7.17;
http://support.sentieon.com/manual/),
Sambamba (version 0.5.9; http://github.com/biod/sambamba/releases) and blat
(version 35×1; DOI: 10.1101/gr.229202) were used for comparison
process; iii) bedtools (version 2.25.0; http://bedtools.readthedocs.io/en/latest/index.html)
was used for post-processing; and iv) Python (version 3.6.6;
http://www.python.org/downloads/release/python-366/)
was used for mutation detection. The raw sequencing data are not
available as these were not provided by the company. The number of
genes and mutations that was investigated was 35. No patient had
more than one gene mutation as all patients carried negative driver
genes.
Treatment regimens
Patients received apatinib plus chemotherapy or
chemotherapy alone, with a mean treatment cycle of8.3 (mean
treatment cycle duration, 5.8 months). The chemotherapy regimens
included the following: i) docetaxel monotherapy (60–75
mg/m2; day 1); ii) TP, paclitaxel (135–175
mg/m2; day 1) plus cisplatin (75 mg/m2; day
1) or carboplatin [area under the curve (AUC), 5–6 mg/ml/min; day
1]; iii) AP, pemetrexed (500 mg/m2; day 1) plus
cisplatin (75 mg/m2; day 1) or carboplatin (AUC, 5–6
mg/ml/min; day 1); iv) DP, docetaxel (60–75 mg/m2; day
1) plus cisplatin (75 mg/m2; day 1) or carboplatin (AUC,
5–6 mg/ml/min; day 1); and v) pemetrexed monotherapy (500
mg/m2; day 1). A dosage of 500 mg/day apatinib was
administered and adjusted to 250 mg/day if intolerance occurred.
For patients who received apatinib plus chemotherapy, apatinib was
administered for maintenance treatment until the patients developed
disease progression, intolerable toxicity (still uncontrolled
following dosage adjustment) or death. The decision of which
treatment regimen was given was based on patient willingness and
physician's suggestions, and physicians were guided by the NCCN
Clinical Practice Guidelines in Oncology (19).
Data collection and evaluation
Patient data on clinical characteristics,
radiological results of magnetic resonance imaging or computed
tomography, and follow-up were obtained. Based on the radiological
information, the best response, referring to the best results from
multiple assessments, was assessed using the Response Evaluation
Criteria in Solid Tumors (20). At
the end of the follow-up in February 2023, PFS and overall survival
(OS) were determined. PFS was considered to be the interval from
treatment initiation to disease progression or patient death; OS
was considered to be the interval from treatment initiation to
patient death. Furthermore, data on adverse events (AEs) were
obtained for a safety evaluation according to Common Terminology
Criteria for Adverse Events version 5.0 (21). No artificial intelligence tools were
used during the present study or in the preparation of the present
article.
Statistical analysis
Statistical analysis was performed using SPSS
(version 24.0; IBM Corp.). Graphic rendering was completed using
GraphPad Prism (version 7.0; Dotmatics). The comparison between
groups was analyzed using a χ2 test, Fisher's exact
test, Wilcoxon rank-sum test or an unpaired Student's t-test. PFS
and OS were determined using Kaplan-Meier curves and the log-rank
test. Factors associated with PFS and OS were analyzed using Cox
proportional hazards regression analysis, and multivariate Cox
regression analysis was performed using the forward stepwise
method. P<0.05 was considered to indicate a statistically
significant difference.
Results
Clinical features
Patients who received apatinib plus chemotherapy had
a mean age of 57.7±9.6 years, with 32.3 and 67.7% being female and
male, respectively. Patients who received chemotherapy alone had a
mean age of 60.4±9.5 years, with 37.5 and 62.5% being female and
male, respectively. There were no significant differences in any
clinical characteristics such as age and sex between patients who
received apatinib plus chemotherapy and those who received
chemotherapy alone (P>0.05). The detailed clinical information
of these two groups of patients with advanced LUAD is listed in
Table I.
 | Table I.Clinical characteristics of patients
with advanced lung adenocarcinoma who received either chemotherapy
(n=80) or apatinib plus chemotherapy (n=65). |
Table I.
Clinical characteristics of patients
with advanced lung adenocarcinoma who received either chemotherapy
(n=80) or apatinib plus chemotherapy (n=65).
|
Characteristics | Chemotherapy, n
(%) | Apatinib plus
chemotherapy, n (%) | P-value |
|---|
| Mean age,
years | 60.4±9.5 | 57.7±9.6 | 0.094 |
| Age, years |
|
| 0.139 |
|
<60 | 32 (40.0) | 34 (52.3) |
|
|
≥60 | 48 (60.0) | 31 (47.7) |
|
| Sex |
|
| 0.515 |
|
Female | 30 (37.5) | 21 (32.3) |
|
|
Male | 50 (62.5) | 44 (67.7) |
|
| Smoking
history |
|
| 0.381 |
| No | 44 (55.0) | 31 (47.7) |
|
|
Yes | 36 (45.0) | 34 (52.3) |
|
| ECOG PS score |
|
| 0.192 |
| 0 | 39 (48.8) | 39 (60.0) |
|
| 1 | 40 (50.0) | 25 (38.5) |
|
| 2 | 1 (1.2) | 1 (1.5) |
|
| TNM stage |
|
| 0.404 |
|
IIIB/C | 18 (22.5) | 11 (16.9) |
|
| IV | 62 (77.5) | 54 (83.1) |
|
| Bone
metastasis |
|
| 0.214 |
| No | 68 (85.0) | 50 (76.9) |
|
|
Yes | 12 (15.0) | 15 (23.1) |
|
| Brain
metastasis |
|
| 0.320 |
| No | 70 (87.5) | 53 (81.5) |
|
|
Yes | 10 (12.5) | 12 (18.5) |
|
| Treatment line |
|
| 0.096 |
|
First | 39 (48.8) | 23 (35.4) |
|
|
Second | 39 (48.8) | 39 (60.0) |
|
|
Third | 2 (2.4) | 3 (4.6) |
|
Patients who received first-line apatinib plus
chemotherapy had a mean age of 55.9±8.8 years, and patients who
received first-line chemotherapy alone had a mean age of 59.9±9.4
years (P=0.101). There were six female patients (26.1%) and 17 male
patients (73.9%) who received first-line apatinib plus
chemotherapy, and there were 17 female patients (43.6%) and 22 male
patients (56.4%) who received first-line chemotherapy alone
(P=0.168). Notably, there were no significant differences for any
of the clinical characteristics investigated between patients who
received first-line apatinib plus chemotherapy and those who
received first-line chemotherapy alone (P>0.05). The clinical
information on patients who received either first-line apatinib
plus chemotherapy or first-line chemotherapy alone is shown in
Table SI.
Of those patients who received apatinib plus
chemotherapy, 52.3% of patients received apatinib and docetaxel,
12.3% received apatinib and TP, 12.3% received apatinib and AP,
12.3% received apatinib and pemetrexed and 10.8% received apatinib
and DP. Of those patients who received chemotherapy alone, 38.8%
received docetaxel monotherapy, 20.0% received TP, 15.0% received
AP, 15.0% received DP, and 11.2% received pemetrexed monotherapy
(Table II).
| Table II.Treatment regimen of patients with
advanced lung adenocarcinoma receiving either chemotherapy (n=80)
or apatinib plus chemotherapy (n=65). |
Table II.
Treatment regimen of patients with
advanced lung adenocarcinoma receiving either chemotherapy (n=80)
or apatinib plus chemotherapy (n=65).
| Regimen | Chemotherapy, n
(%) | Apatinib plus
chemotherapy, n (%) |
|---|
| Docetaxel
monotherapy | 31 (38.8) | 0 (0.0) |
| TP | 16 (20.0) | 0 (0.0) |
| AP | 12 (15.0) | 0 (0.0) |
| DP | 12 (15.0) | 0 (0.0) |
| Pemetrexed
monotherapy | 9 (11.2) | 0 (0.0) |
| Apatinib and
docetaxel | 0 (0.0) | 34 (52.3) |
| Apatinib and
TP | 0 (0.0) | 8 (12.3) |
| Apatinib and
AP | 0 (0.0) | 8 (12.3) |
| Apatinib and
pemetrexed | 0 (0.0) | 8 (12.3) |
| Apatinib and
DP | 0 (0.0) | 7 (10.8) |
Treatment response
The best response rate was significantly improved by
apatinib plus chemotherapy compared with chemotherapy alone. In
detail, the complete response (CR), partial response (PR), stable
disease (SD) and progressive disease (PD) rates in patients who
received apatinib plus chemotherapy were 1.5, 52.3, 35.4 and 10.8%,
respectively, and those in patients who received chemotherapy alone
were 0.0, 36.3, 42.5 and 21.3%, respectively. The overall response
rate (ORR) was significantly improved by apatinib plus chemotherapy
compared with chemotherapy alone (P=0.034), whereas there was no
significant difference in DCR between groups (P=0.091; Table III).
| Table III.Best response rates of patients with
advanced lung adenocarcinoma receiving either chemotherapy (n=80)
or apatinib plus chemotherapy (n=65). |
Table III.
Best response rates of patients with
advanced lung adenocarcinoma receiving either chemotherapy (n=80)
or apatinib plus chemotherapy (n=65).
| Response rate | Chemotherapy, n
(%) | Apatinib plus
chemotherapy, n (%) | P-value |
|---|
| Best response |
|
| 0.018 |
| CR | 0 (0.0) | 1 (1.5) |
|
| PR | 29 (36.3) | 34 (52.3) |
|
| SD | 34 (42.5) | 23 (35.4) |
|
| PD | 17 (21.3) | 7 (10.8) |
|
| ORR |
|
| 0.034 |
|
Yes | 29 (36.2) | 35 (53.8) |
|
| No | 51 (63.8) | 30 (46.2) |
|
| DCR |
|
| 0.091 |
|
Yes | 63 (78.8) | 58 (89.2) |
|
| No | 17 (21.2) | 7 (10.8) |
|
Survival analysis
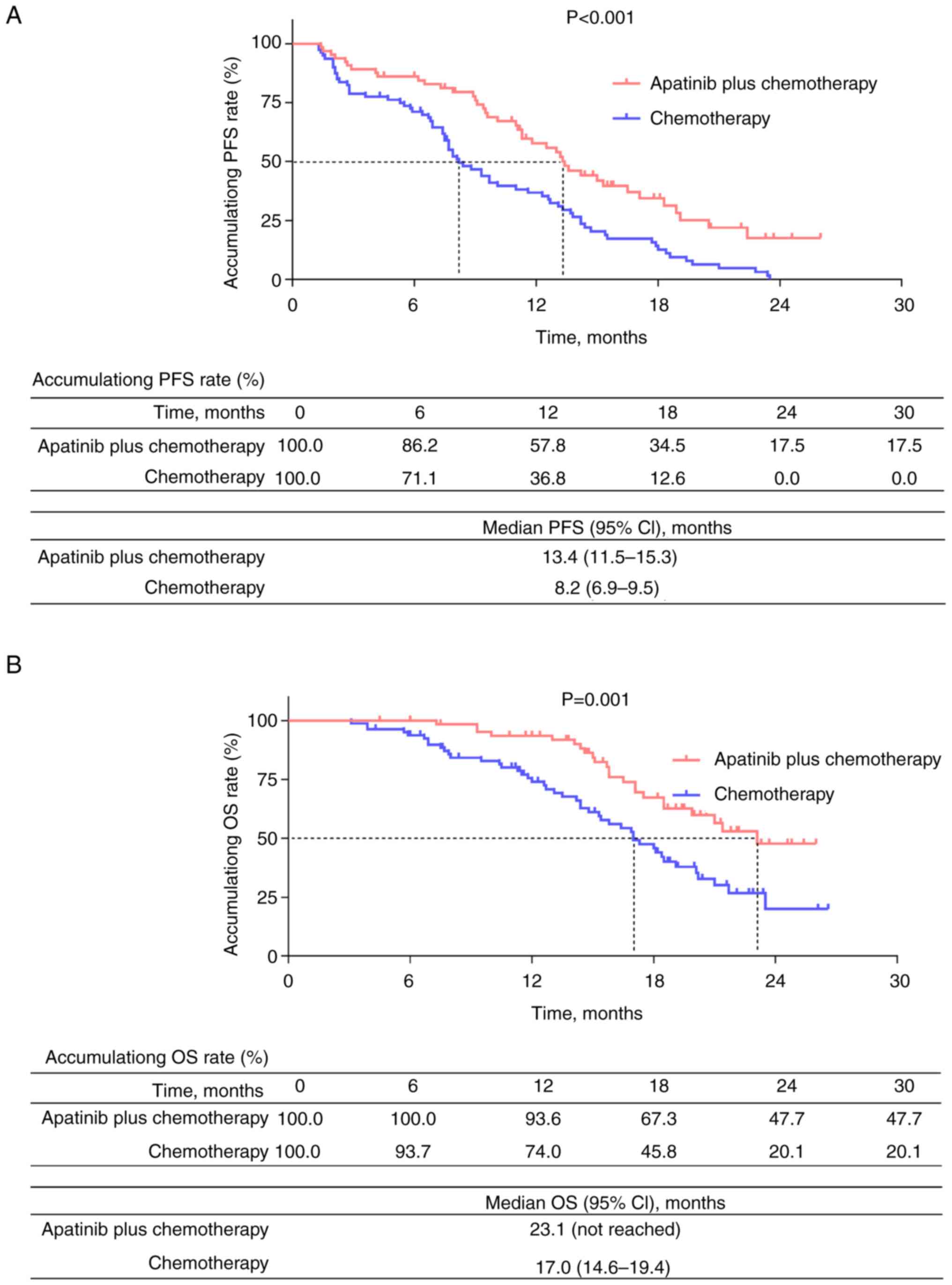
Accumulating PFS rate was significantly increased
following apatinib plus chemotherapy compared with chemotherapy
alone (P<0.001). The median PFS (95% CI) was 13.4 months
(11.5–15.3) in patients who underwent apatinib plus chemotherapy,
and 8.2 months (6.9–9.5) in patients who underwent chemotherapy
alone (Fig. 1A). The accumulating
OS rate was also significantly prolonged following apatinib plus
chemotherapy compared with chemotherapy alone(P=0.001). The median
OS (95% CI) was 23.1 months (not reached) in patients who underwent
apatinib plus chemotherapy and 17.0 months (14.6–19.4) in patients
who underwent chemotherapy alone (Fig.
1B).
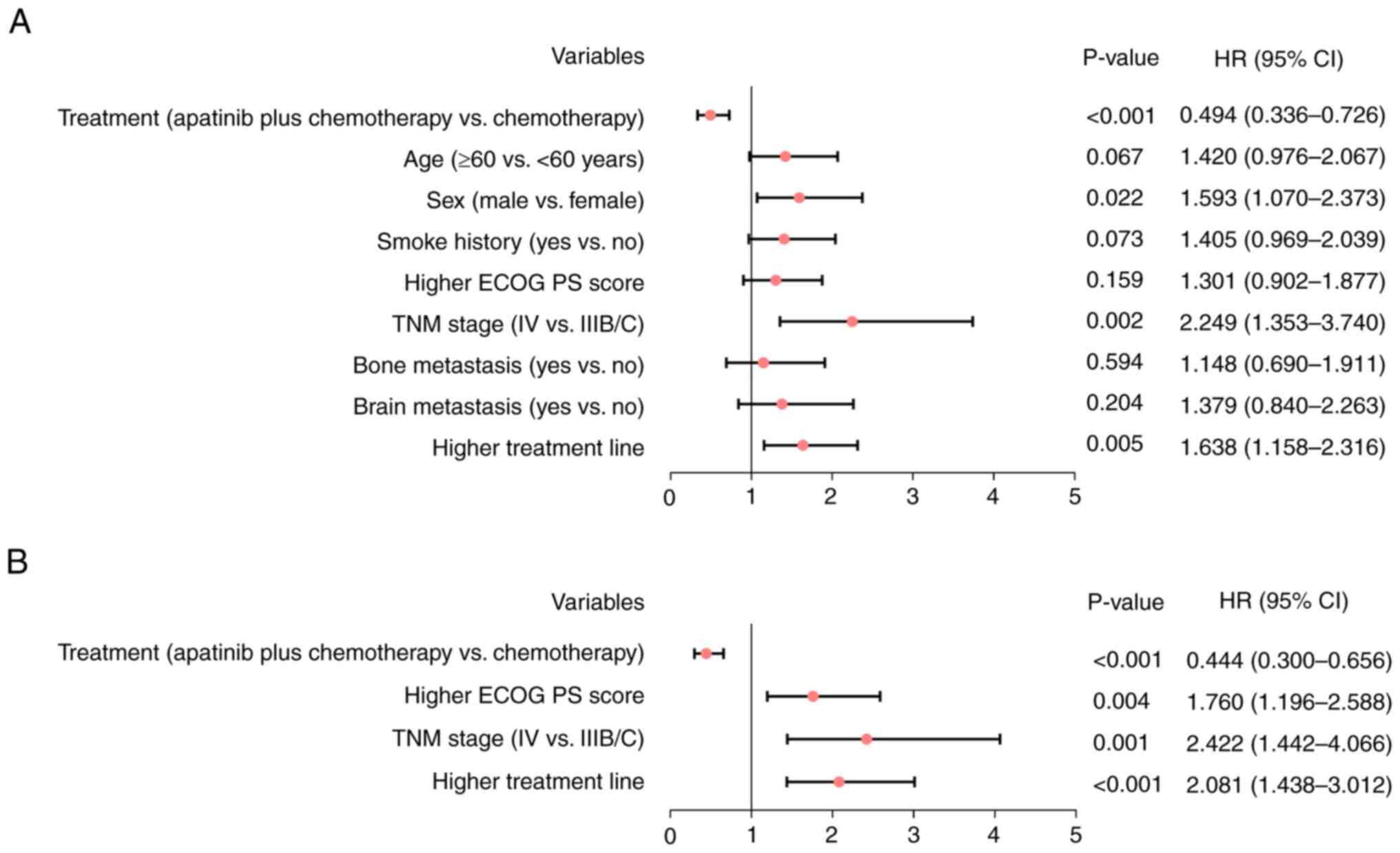
Independent factors associated with
survival
Apatinib plus chemotherapy was significantly
associated with an increased PFS [hazard ratio (HR), 0.494;
P<0.001]. However, sex (male vs. female; HR, 1.593; P=0.022),
TNM stage (IV vs. IIIB/C; HR, 2.249; P=0.002) and higher line of
treatment (HR, 1.638; P=0.005) were significantly associated with
decreased PFS (Fig. 2A). Following
adjustment by multivariate Cox regression analysis, apatinib plus
chemotherapy was significantly independently associated with longer
PFS (HR, 0.444; P<0.001), whereas higher Eastern Cooperative
Oncology Group Performance Status score (22) (HR, 1.760; P=0.004), TNM stage (IV
vs. IIIB/C; HR, 2.422; P=0.001) and higher line of treatment (HR,
2.081; P<0.001) were significantly independently associated with
decreased PFS in patients with advanced LUAD (Fig. 2B).
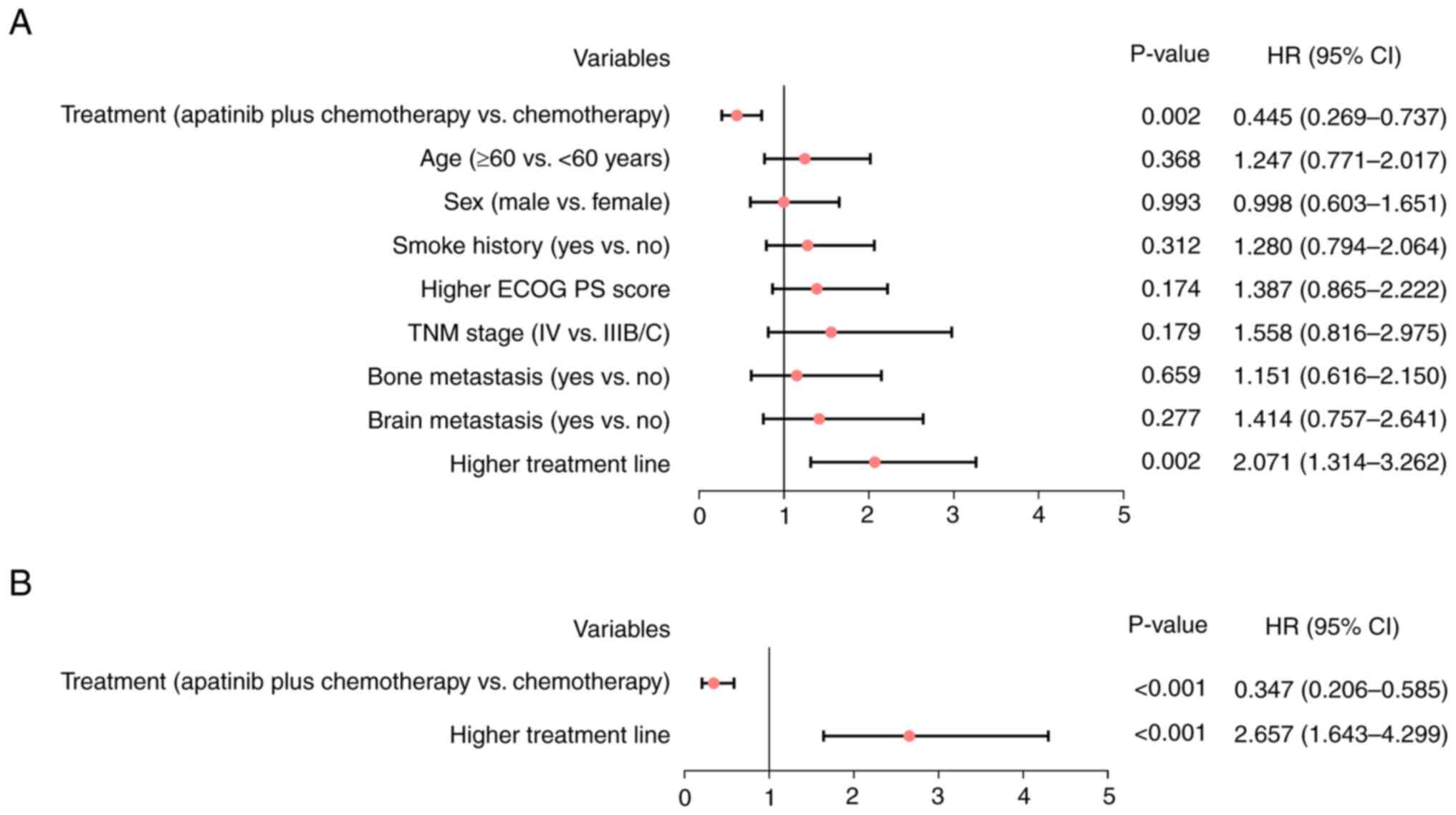
Apatinib plus chemotherapy was significantly
associated with increased OS (HR, 0.445; P=0.002), and higher line
of treatment line was significantly associated with decreased OS
(HR, 2.071; P=0.002; Fig. 3A).
Following adjustment by multivariate Cox regression analysis,
apatinib plus chemotherapy was significantly independently
associated with longer OS (HR, 0.347; P<0.001), whereas higher
line of treatment was significantly independently associated with
reduced OS in patients with advanced LUAD (HR, 2.657; P<0.001;
Fig. 3B).
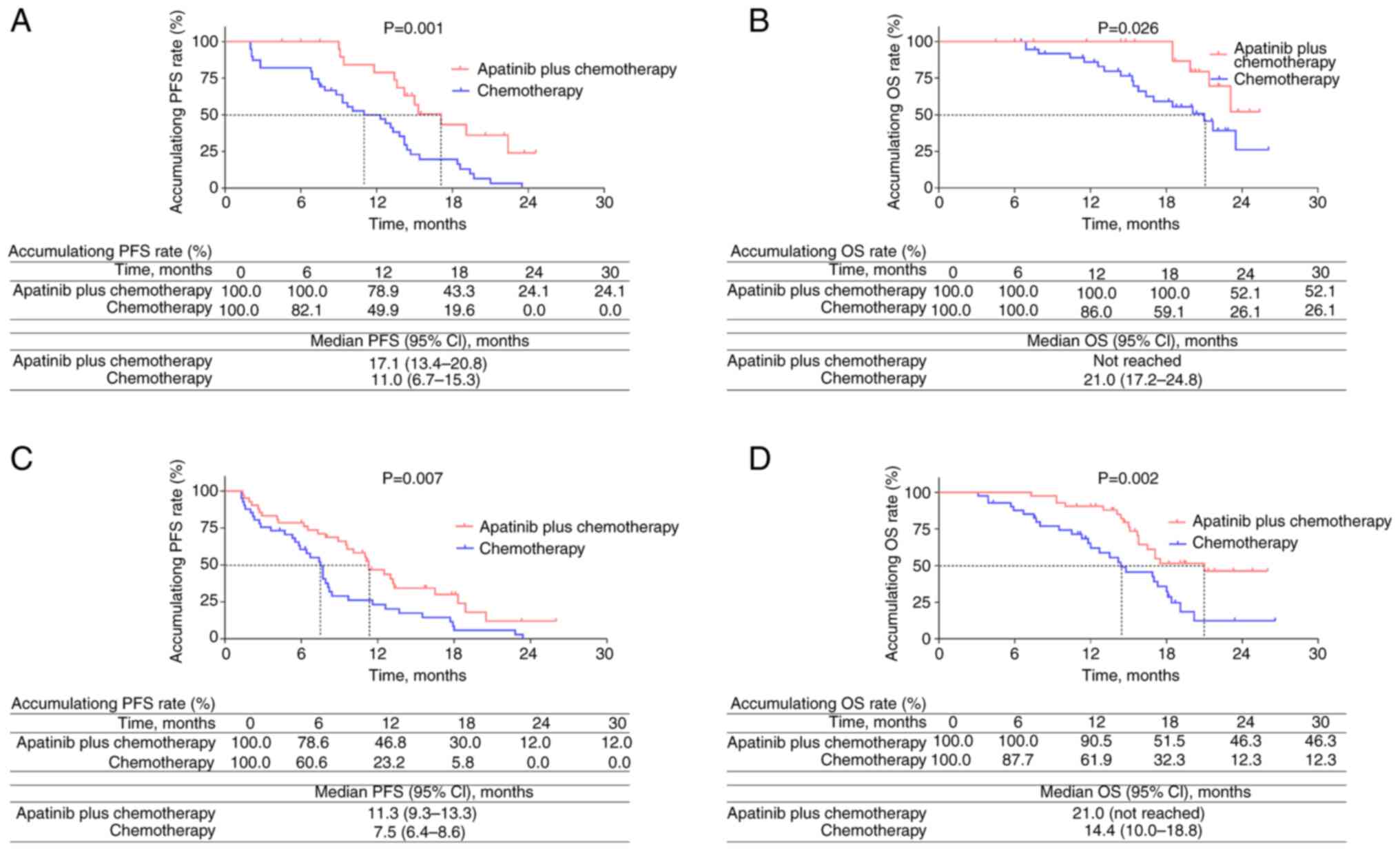
Subgroup analysis of survival based on
treatment lines
In patients who underwent first-line apatinib plus
chemotherapy or chemotherapy alone, accumulating PFS rates
(P=0.001; Fig. 4A) and OS rates
(P=0.026; Fig. 4B) were
significantly elevated following apatinib plus chemotherapy
compared with chemotherapy alone. In patients who underwent these
two regimens as second-line treatment or higher, accumulating PFS
rates (P=0.007; Fig. 4C) and OS
rates (P=0.002; Fig. 4D) were
significantly increased following apatinib plus chemotherapy
compared with chemotherapy alone.
Subgroup analysis of treatment
response and survival based on different chemotherapy regimens
OS was significantly prolonged by apatinib plus
docetaxel compared with docetaxel alone (P=0.025), whilst ORR, DCR
and PFS were not significantly affected by apatinib plus docetaxel
or docetaxel alone (P>0.05). Moreover, ORR, DCR, PFS and OS were
not significantly influenced by apatinib plus TP or TP alone
(P>0.05). However, ORR (P=0.017) and PFS (P=0.022) were
significantly prolonged by apatinib plus DP compared with DP alone.
Conversely, ORR and OS were not significantly affected by apatinib
plus DP or DP alone. Additionally, only PFS was significantly
prolonged by apatinib plus pemetrexed compared with pemetrexed
alone (P=0.017); however, ORR, DCR and OS were not significantly
affected (P>0.05; Table
SII).
AEs
The occurrence rate of hypertension was
significantly elevated in patients who received apatinib plus
chemotherapy compared with those who received chemotherapy alone
(43.1 vs. 25.0%; P=0.021). However, there was no significant
difference in the incidence of other AEs between patients who
received the two regimens (P>0.05). In addition, the incidence
of grade 3–4 AEs did not significantly differ between patients who
received either treatment (P>0.05); however, the incidence of
grade 3–4 AEs was relatively low in patients who received apatinib
plus chemotherapy compared with those who received chemotherapy
alone: i) Of those patients receiving apatinib plus chemotherapy,
13.8, 10.8, 4.6 and 3.1% experienced the grade 3–4 hematological
AEs leukopenia, neutropenia, anemia and thrombopenia, respectively;
and ii) of those patients receiving apatinib plus chemotherapy,
7.7, 6.2, 4.6, 4.6, 4.6 and 1.5% experienced the grade 3–4
non-hematological AEs hypertension, nausea and vomiting, elevated
transaminase, anorexia, rash and hand-food syndrome, respectively
(Table IV).
| Table IV.Adverse events of patients with
advanced lung adenocarcinoma receiving either chemotherapy (n=80)
or apatinib plus chemotherapy (n=65). |
Table IV.
Adverse events of patients with
advanced lung adenocarcinoma receiving either chemotherapy (n=80)
or apatinib plus chemotherapy (n=65).
|
| Chemotherapy, n
(%) | Apatinib plus
chemotherapy, n (%) | P-value |
|---|
|
|
|
|
|
|---|
| AE | Total | Grade 1–2 | Grade 3–4 | Total | Grade 1–2 | Grade 3–4 | Total | Grade 3–4 |
|---|
| Hematological |
|
|
|
|
|
|
|
|
|
Leukopenia | 27 (33.8) | 17 (21.3) | 10 (12.5) | 25 (38.5) | 16 (24.6) | 9 (13.8) | 0.556 | 0.811 |
|
Neutropenia | 25 (31.3) | 18 (22.5) | 7 (8.8) | 22 (33.8) | 15 (23.1) | 7 (10.8) | 0.740 | 0.682 |
|
Anemia | 17 (21.3) | 16 (20.0) | 1 (1.3) | 18 (27.7) | 15 (23.1) | 3 (4.6) | 0.367 | 0.219 |
|
Thrombopenia | 16 (20.0) | 14 (17.5) | 2 (2.5) | 12 (18.5) | 10 (15.4) | 2 (3.1) | 0.815 | 1.000 |
|
Non-hematological |
|
|
|
|
|
|
|
|
|
Hypertension | 20 (25.0) | 19 (23.8) | 1 (1.3) | 28 (43.1) | 23 (35.4) | 5 (7.7) | 0.021 | 0.090 |
|
Hand-foot syndrome | 20 (25.0) | 20 (25.0) | 0 (0.0) | 25 (38.5) | 24 (36.9) | 1 (1.5) | 0.081 | 0.448 |
|
Elevated transaminase | 25 (31.3) | 24 (30.0) | 1 (1.3) | 24 (36.9) | 21 (32.3) | 3 (4.6) | 0.473 | 0.326 |
| Nausea
and vomiting | 19 (23.8) | 16 (20.0) | 3 (3.8) | 20 (30.8) | 16 (24.6) | 4 (6.2) | 0.343 | 0.701 |
|
Anorexia | 18 (22.5) | 16 (20.0) | 2 (2.5) | 19 (29.2) | 16 (24.6) | 3 (4.6) | 0.355 | 0.657 |
|
Alopecia | 24 (30.0) | 24 (30.0) | 0 (0.0) | 16 (24.6) | 16 (24.6) | 0 (0.0) | 0.471 | - |
|
Diarrhea | 13 (16.3) | 13 (16.3) | 0 (0.0) | 15 (23.1) | 15 (23.1) | 0 (0.0) | 0.300 | - |
|
Rash | 14 (17.5) | 12 (15.0) | 2 (2.5) | 15 (23.1) | 12 (18.5) | 3 (4.6) | 0.404 | 0.657 |
|
Elevated bilirubin | 12 (15.0) | 12 (15.0) | 0 (0.0) | 12 (18.5) | 12 (18.5) | 0 (0.0) | 0.577 | - |
|
Constipation | 7 (8.8) | 7 (8.8) | 0 (0.0) | 11 (16.9) | 11 (16.9) | 0 (0.0) | 0.138 | - |
Discussion
Apatinib plus chemotherapy has potential benefits in
treating patients with advanced NSCLC (23,24).
For example, a previous study reported that 22.9% of patients with
advanced NSCLC receiving apatinib plus chemotherapy achieved PR,
45.8% achieved SD and 25% achieved PD, resulting in an ORR of 29.2%
and a DCR of 75.0% (24). Another
previous study reported that second-line treatment or above of
apatinib plus chemotherapy achieved an ORR of 33.33% in patients
with advanced LUAD (23).
Furthermore, the present study demonstrated that apatinib plus
chemotherapy significantly increased the ORR compared with
chemotherapy alone in patients with advanced LUAD. The potential
reasons for this are as follows: i) Apatinib may inhibit
angiogenesis and tumor growth in LUAD, which would help improve
treatment response (25–28); and ii) apatinib may have a
synergistic effect with chemotherapy by sensitizing LUAD cells to
chemotherapy, thereby enhancing the treatment response (15,29).
Survival is also prolonged by apatinib plus
chemotherapy in patients with advanced NSCLC, according to previous
studies (16,23,30).
For example, a previous study reported that second-line treatment
of apatinib plus chemotherapy notably increased PFS compared with
chemotherapy alone (median, 5.47 vs. 2.97 months) in patients with
advanced NSCLC (16). Moreover, the
present study found that survival was significantly prolonged by
apatinib plus chemotherapy compared with chemotherapy alone in
patients with advanced LUAD, which was further demonstrated by
multivariate Cox regression analysis. Notably, the median PFS was
13.4 vs. 8.2 months, and the median OS was 23.1 vs. 17.0 months in
patients who received apatinib plus chemotherapy and chemotherapy
alone, respectively. This may be due to the potential enhancement
of the treatment response by apatinib plus chemotherapy, which may
have helped further prolong the survival. In addition, subgroup
analysis demonstrated that apatinib plus chemotherapy significantly
prolonged survival compared with chemotherapy alone, in patients
with first-line treatment and with second-line treatment or above.
This finding was partly in line with that of a previous study which
reported that apatinib plus docetaxel as second- or above-line
treatment was effective in prolonging survival in patients with
advanced non-squamous NSCLC (23).
Moreover, data from the present study showed the benefit of
apatinib plus chemotherapy as a first-line treatment in prolonging
PFS, indicating the potential of apatinib plus chemotherapy as a
first-line treatment in patients with advanced LUAD carrying
negative driver genes. However, further research is required to
confirm this hypothesis.
Notably, the incidence of most AEs did not
significantly differ between treatments, except for hypertension,
which was significantly elevated by apatinib plus chemotherapy
compared with chemotherapy alone. This finding was partly in
accordance with that of a previous study which indicated that the
incidence of both hypertension and hand-foot syndrome were
increased by apatinib plus docetaxel compared with docetaxel alone
in patients with advanced NSCLC (15). Apatinib may regulate the production
of nitric oxide, oxidative stress response, endothelial dysfunction
and endothelin receptor 1, which are responsible for the
development of hypertension (31–33).
According to previous studies, the countermeasures for hypertension
caused by apatinib were as follows (34–36):
For patients with grade 1 hypertension [systolic blood pressure
(SBP) range, 140–159 mmHg and/or diastolic blood pressure (DBP)
range, 90–99 mmHg], apatinib could be continued without dose
adjustment, but close monitoring of blood pressure was required
(34–36); for patients with grade 2
hypertension (SBP range, 160–179 mmHg and/or DBP range, 100–109
mmHg), apatinib could be continued and usually did not need dose
adjustment, but antihypertensive drugs could be applied, such as
calcium channel blockers, angiotensin-converting enzyme inhibitors,
angiotensin II receptor antagonists, thiazide diuretics and
β-blockers (34–36); for patients with grade 3
hypertension (SBP, >180 mmHg and/or DBP, >110 mmHg), apatinib
should be discontinued immediately (34–36).
If treatment with a single antihypertensive drug could not control
hypertension, combined antihypertensive drugs should be considered
(34–36). Although apatinib may induce
hypertension, apatinib plus chemotherapy may also suit patients
with underlying hypertension (35).
However, the blood pressure of these patients should be controlled
within the normal range before administering apatinib, and their
blood pressure should be closely monitored during treatment, with
timely adjustment of antihypertensive drugs in the case of an
increase in blood pressure (23,24).
The present study also determined that the common
AEs that occurred in patients who received apatinib plus
chemotherapy were hypertension (43.1%), hand-food syndrome (38.5%),
leukopenia (38.5%) and elevated transaminase (36.9%). In addition,
a few grade 3–4 AEs occurred in patients with advanced LUAD. These
findings were partially consistent with those of a previous study
(16) which revealed that the
common AEs that occurred in patients receiving apatinib plus
chemotherapy were fatigue (58%), cough (39%), hand-food syndrome
(38%), febrile neutropenia (23%) and hypertension (20%); meanwhile,
grade 3–5 AEs rarely occurred in patients with advanced NSCLC
(16). The findings demonstrated
that apatinib plus chemotherapy can be effective in the treatment
of patients with advanced LUAD (16,23).
Clinical evidence for the use of apatinib in the
treatment of patients with advanced LUAD carrying negative driver
genes is limited, and only one study has investigated the efficacy
and safety of apatinib plus chemotherapy in patients with advanced
NSCLC carrying negative driver genes (16). To the best of our knowledge, there
is no theoretical evidence regarding the role of apatinib in NSCLC
cell lines carrying negative driver genes, but, certain previous
studies have assessed the synergistic effect of apatinib plus
chemotherapy in general NSCLC cell lines (15,29).
For instance, one study reported that apatinib investigated the
effect of docetaxel in treating advanced NSCLC patients and
chemoresistant NSCLC cells by regulating autophagy (15). Moreover, apatinib sensitized NSCLC
cells to cisplatin by decreasing the expression of multidrug
resistance protein 1 and inactivating the extracellular
signal-regulated kinase pathway (29). The findings indicate that apatinib
plus chemotherapy may improve the prognosis of patients with
advanced NSCLC who carry negative driver genes. However, further
research is required to validate the findings.
The present study had several limitations: i) It is
a non-intervention study and thus, further randomized, controlled
trials are required to validate its findings; ii) it is a
single-center study, which may have led to selection biases; iii)
apatinib was developed in China and therefore, the effect of
apatinib plus chemotherapy in patients from other regions with
advanced LUAD carrying negative driver genes should be assessed
further.
In conclusion, apatinib plus chemotherapy is
associated with a greater efficacy than chemotherapy alone, with a
satisfactory safety profile in patients with advanced LUAD carrying
negative driver genes. As there is a lack of effective treatment
options for these patients, apatinib plus chemotherapy may have the
potential to serve as a treatment option to further improve
prognosis.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
JL and LZ contributed to the study conception and
design, and provided supervision. HY and WY made contributions to
data collection. YN and XB analyzed the data. XZ, YL and AC were
responsible for the interpretation of data for the work. JL and LZ
confirm the authenticity of all the raw data. All authors have read
and approved the final manuscript.
Ethics approval and consent to
participate
The present study was approved by the Medical Ethics
Committee of Yueqing Hospital Affiliated to Wenzhou Medical
University (Yueqing, China; approval no. YQYY202001003), and
written informed consent was obtained from the patients or their
guardians.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Seguin L, Durandy M and Feral CC: Lung
adenocarcinoma tumor origin: A guide for personalized medicine.
Cancers (Basel). 14:17592022. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chen Z, Fillmore CM, Hammerman PS, Kim CF
and Wong KK: Non-small-cell lung cancers: A heterogeneous set of
diseases. Nat Rev Cancer. 14:535–546. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Melocchi V, Dama E, Mazzarelli F, Cuttano
R, Colangelo T, Di Candia L, Lugli E, Veronesi G, Pelosi G,
Ferretti GM, et al: Aggressive early-stage lung adenocarcinoma is
characterized by epithelial cell plasticity with acquirement of
stem-like traits and immune evasion phenotype. Oncogene.
40:4980–4991. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tan AC and Tan DSW: Targeted therapies for
lung cancer patients with oncogenic driver molecular alterations. J
Clin Oncol. 40:611–625. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Karimi N and Moghaddam SJ: KRAS-Mutant
lung cancer: Targeting molecular and immunologic pathways,
therapeutic advantages and restrictions. Cells. 12:7492023.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kim SY, Kim SM, Lim S, Lee JY, Choi SJ,
Yang SD, Yun MR, Kim CG, Gu SR, Park C, et al: Modeling clinical
responses to targeted therapies by patient-derived organoids of
advanced lung adenocarcinoma. Clin Cancer Res. 27:4397–4409. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lu Y, Fan Z, Zhu SJ, Huang X, Zhuang Z, Li
Y, Deng Z, Gao L, Hong X, Zhang T, et al: A new ALK inhibitor
overcomes resistance to first- and second-generation inhibitors in
NSCLC. EMBO Mol Med. 14:e142962022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Rusdi F, Iskandar H, Hardjianti T, Bakri
S, Udaya W, Kasim H, Arief E and Seweng A: The one year survival
rate of lung adenocarcinoma patients treated with chemotherapy or
targeted therapy. Enfermería Clínica. 30:456–460. 2020. View Article : Google Scholar
|
|
9
|
Lopez-Chavez A, Thomas A, Rajan A, Raffeld
M, Morrow B, Kelly R, Carter CA, Guha U, Killian K, Lau CC, et al:
Molecular profiling and targeted therapy for advanced thoracic
malignancies: A biomarker-derived, multiarm, multihistology phase
II basket trial. J Clin Oncol. 33:1000–1007. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cui Y, Fang W, Li C, Tang K, Zhang J, Lei
Y, He W, Peng S, Kuang M, Zhang H, et al: Development and
validation of a novel signature to predict overall survival in
‘Driver Gene-negative’ Lung Adenocarcinoma (LUAD): Results of a
multicenter study. Clin Cancer Res. 25:1546–1556. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Gao X, Chen M, Liu X, Shi Y, Liang H, Zhou
Q, Zhao J, Pan R, Zhong W, Xu Y and Wang M: Prognostic factors and
survival benefits of antitumor treatments for advanced non-small
cell lung cancer patients with central nervous system metastasis
with or without driver genes: A Chinese single-center cohort study.
Front Oncol. 12:8795542022. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hames ML, Chen H, Iams W, Aston J, Lovly
CM and Horn L: Correlation between KRAS mutation status and
response to chemotherapy in patients with advanced non-small cell
lung cancer☆. Lung Cancer. 92:29–34. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Scott LJ: Apatinib: A review in advanced
gastric cancer and other advanced cancers. Drugs. 78:747–758. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cui YJ, Liu J, Liu MM and Zhang HZ:
Observation on the clinical effect of apatinib combined with
chemotherapy in the treatment of advanced non-small cell lung
cancer. Pak J Med Sci. 37:1036–1041. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Hu R, Li T, Hui K, Chen Z, Wang N, Wu X,
Ge L and Zhou L: Apatinib sensitizes chemoresistant NSCLC cells to
doxetaxel via regulating autophagy and enhances the therapeutic
efficacy in advanced and refractory/recurrent NSCLC. Mol Med Rep.
22:3935–3943. 2020.PubMed/NCBI
|
|
16
|
Yu Z, Cai X, Xu Z, He Z, Lai J, Wang W,
Zhang J, Kong W, Huang X, Chen Y, et al: Apatinib plus chemotherapy
as a second-line treatment in unresectable non-small cell lung
carcinoma: A randomized, controlled, multicenter clinical trial.
Oncologist. 25:e1640–e1649. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Cainap C, Balacescu O, Cainap SS and Pop
LA: Next generation sequencing technology in lung cancer diagnosis.
Biology (Basel). 10:8642021.PubMed/NCBI
|
|
18
|
Chansky K, Detterbeck FC, Nicholson AG,
Rusch VW, Vallières E, Groome P, Kennedy C, Krasnik M, Peake M,
Shemanski L, et al: The IASLC lung cancer staging project: External
Validation of the Revision of the TNM Stage Groupings in the Eighth
Edition of the TNM Classification of Lung Cancer. J Thorac Oncol.
12:1109–1121. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ettinger DS, Wood DE, Aisner DL, Akerley
W, Bauman J, Chirieac LR, D'Amico TA, DeCamp MM, Dilling TJ,
Dobelbower M, et al: Non-Small cell lung cancer, version 5.2017,
NCCN clinical practice guidelines in oncology. J Natl Compr Canc
Netw. 15:504–535. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Freites-Martinez A, Santana N,
Arias-Santiago S and Viera A: Using the common terminology criteria
for adverse events (CTCAE – Version 5.0) to Evaluate the severity
of adverse events of anticancer therapies. Actas Dermosifiliogr
(Engl Ed). 112:90–92. 2021.(In English, Spanish). View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Azam F, Latif MF, Farooq A, Tirmazy SH,
AlShahrani S, Bashir S and Bukhari N: Performance status assessment
by using ECOG (Eastern Cooperative Oncology Group) Score for cancer
patients by oncology healthcare professionals. Case Rep Oncol.
12:728–736. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Jiang Q, Zhang NL, Ma DY, Tan BX, Hu X and
Fang XD: Efficacy and safety of apatinib plus docetaxel as the
second or above line treatment in advanced nonsquamous NSCLC: A
multi center prospective study. Medicine (Baltimore).
98:e160652019. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xu J, Liu X, Yang S and Shi Y: Efficacy,
safety, and prognostic factors of apatinib plus platinum doublet
chemotherapy in advanced non-small cell lung cancer. J Cancer Res
Ther. 18:1425–1431. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Huang MP, Gu SZ, Huang B, Li GW, Xiong ZP,
Tang T and Zeng SN: Apatinib inhibits angiogenesis in intrahepatic
cholangiocarcinoma by regulating the vascular endothelial growth
factor receptor-2/signal transducer and activator of transcription
factor 3/hypoxia inducible factor 1 subunit alpha signaling axis.
Pharmacology. 106:509–519. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Song J, Guan Z, Song C, Li M, Gao Z and
Zhao Y: Apatinib suppresses the migration, invasion and
angiogenesis of hepatocellular carcinoma cells by blocking VEGF and
PI3K/AKT signaling pathways. Mol Med Rep. 23:4292021. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Hu Y, Jing J, Shi Y, Zhang P, Dong D, Wu
Y, Dong X, Li E and Fan Y: Apatinib inhibits pancreatic cancer
growth, migration and invasion through the PI3K/AKT and ERK1/2/MAPK
pathways. Transl Cancer Res. 10:3306–3316. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Xie C, Zhou X, Liang C, Li X, Ge M, Chen
Y, Yin J, Zhu J and Zhong C: Apatinib triggers autophagic and
apoptotic cell death via VEGFR2/STAT3/PD-L1 and ROS/Nrf2/p62
signaling in lung cancer. J Exp Clin Cancer Res. 40:2662021.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Liu ZL, Jin BJ, Cheng CG, Zhang FX, Wang
SW, Wang Y and Wu B: Apatinib resensitizes cisplatin-resistant
non-small cell lung carcinoma A549 cell through reversing multidrug
resistance and suppressing ERK signaling pathway. Eur Rev Med
Pharmacol Sci. 21:5370–5377. 2017.PubMed/NCBI
|
|
30
|
Zhang X, Xiong Y, Xia Q, Wu F, Liu L, Zhou
Y, Zeng L, Zhou C, Xia C, Jiang W, et al: Efficacy and safety of
apatinib plus vinorelbine in patients with wild-type advanced
non-small cell lung cancer after second-line treatment failure: A
nonrandomized clinical trial. JAMA Netw Open. 3:e2012262020.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Wang W, He Q, Li C, Zhuang C, Zhang H,
Wang Q, Fan X, Qi M, Sun R and Yu J: Research on the mechanism and
prevention of hypertension caused by apatinib through the RhoA/ROCK
signaling pathway in a mouse model of gastric cancer. Front
Cardiovasc Med. 9:8738292022. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Cohen JB, Brown NJ, Brown SA, Dent S, van
Dorst DCH, Herrmann SM, Lang NN, Oudit GY, Touyz RM; American Heart
Association Council on Hypertension, ; et al: Cancer
therapy-related hypertension: A scientific statement from the
american heart association. Hypertension. 80:e46–e57. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Camarda N, Travers R, Yang VK, London C
and Jaffe IZ: VEGF receptor inhibitor-induced hypertension:
Emerging mechanisms and clinical implications. Curr Oncol Rep.
24:463–474. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Caletti S, Paini A, Coschignano MA, De
Ciuceis C, Nardin M, Zulli R, Muiesan ML, Salvetti M and Rizzoni D:
Management of VEGF-Targeted therapy-induced hypertension. Curr
Hypertens Rep. 20:682018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Maitland ML, Bakris GL, Black HR, Chen HX,
Durand JB, Elliott WJ, Ivy SP, Leier CV, Lindenfeld J, Liu G, et
al: Initial assessment, surveillance, and management of blood
pressure in patients receiving vascular endothelial growth factor
signaling pathway inhibitors. J Natl Cancer Inst. 102:596–604.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Patel S, Dushenkov A, Jungsuwadee P,
Krishnaswami A and Barac A: Team-Based approach to management of
hypertension associated with angiogenesis inhibitors. J Cardiovasc
Transl Res. 13:463–477. 2020. View Article : Google Scholar : PubMed/NCBI
|