Introduction
Composite lymphoma is defined as the presence of two
or more distinct lymphomas synchronously or heterochronously
occurring in the same patient (1).
Most of the reported cases are composite aggressive B-cell
lymphomas and indolent B-cell lymphomas, including diffuse large
B-cell lymphoma (DLBCL) combined with follicular lymphoma (FL) or
margin zone lymphoma (MZL). However, composite B-cell lymphoma and
extranodal natural killer/T-cell lymphoma (ENKTL) are extremely
rare. To the best of our knowledge, only two cases of composite
DLBCL and ENKTL have been reported, while no previous case of
composite FL and ENKTL has been reported (2,3). Nagai
et al (2) documented the
first case of synchronous ENKTL and DLBCL. In this instance, the
patient underwent a transbronchial lung biopsy and a gastroscopic
biopsy, which revealed histopathological results consistent with
ENKTL and DLBCL, respectively. Kawai et al (3) reported another case where the patient
first had a biopsy of the nasal cavity, which showed ENKTL,
followed by a uterine cervix biopsy that indicated DLBCL. Both
cases presented as synchronous composite lymphoma. The present
study reports one case of the heterochronous occurrence of FL and
ENKTL, and one case of the simultaneous occurrence of DLBCL and
ENKTL. Although the diagnosis of composite lymphoma depends on
pathological analysis, including immunohistochemical staining and
in situ hybridization, clonal evolution analysis can provide
clearer insights into the origins of the two different lymphomas
present.
Case report
Case 1
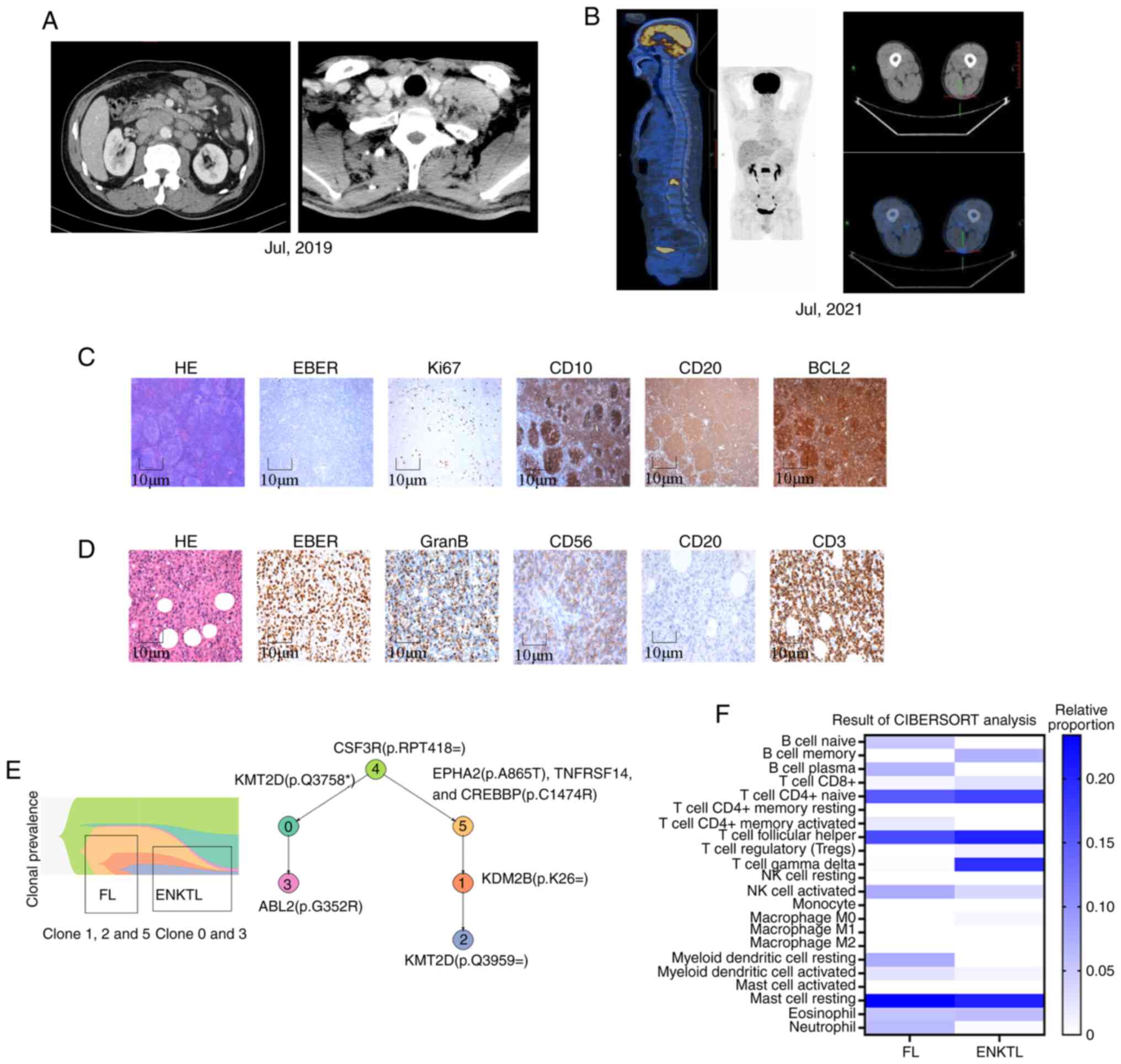
Heterochronous occurrence of FL and ENKTL (Fig. 1). In June 2019, a 60-year-old male
patient was admitted to the Cancer Center, Union Hospital (Wuhan,
China) with multiple enlarged lymph nodes. The patient received a
diagnosis of FL, stage IV (Fig.
1A). The FL was classified as grade 1–2 according to the World
Health Organization Classification 2016 (4), and the immunohistochemical results
showed that the samples were positive for BCL2, CD10 and CD20.
Additionally, the patient was Epstein-Barr encoding region (EBER)
in situ hybridization (ISH)-negative (Fig. 1C). The patient received four cycles
of R-CHOP chemotherapy (375 mg/m2 rituximab on day 1,
750 mg/m2 cyclophosphamide on day 2, 50 mg/m2
Adriamycin on day 2, 2 mg vincristine on day 2 and 100 mg
prednisone on days 2–6) and four cycles of R-FC (375
mg/m2 rituximab on day 1, 25 mg/m2
fludarabine on days 2–4 and 250 mg/m2 cyclophosphamide
on days 2–4) to achieve complete remission (CR). The FL treatment
was ended in January 2020. In March 2020, the patient presented
with a painful erythematous ulcerated plaque on the right upper
leg. A biopsy of the lesion was performed in May 2020, and the
pathological diagnosis was ENKTL, with EBER ISH positivity
(Fig. 1D). Positron emission
tomography-computed tomography (PET-CT) scans showed
hypermetabolism in the right lower extremity skin and lumbar spine
(Fig. 1B), and bone marrow puncture
and exfoliative cytology examinations showed abnormal cells.
Therefore, the patient was diagnosed with ENKTL stage IV and
received six cycles of PP-GEMOX (200 mg programmed cell death
protein 1 inhibitor sintilimab on day 1, 2,500 U/m2
pegaspargase on day 1, 1,000 mg/m2 gemcitabine on day 1
and 130 mg/m2 oxaliplatin on day 1) and achieved CR,
thereafter receiving maintenance treatment with sintilimab (200 mg,
every 3 weeks) for 1 year. The patient remained disease-free for
>40 months after this second CR.
To further elucidate the pathogenesis, targeted DNA
sequencing (Table S1) and bulk RNA
sequencing (Data S1) were
performed in these two paired samples. The results demonstrated
that the predominant mutated genes were CREBBP, CIITA, EPHA2,
BUB1B, CARD11 and TNFRSF14 in the FL specimen, while the
predominant mutated genes were KMT2D, STAT3, MGA, SYK, FAT1 and
FAT4 in the ENKTL specimen. There was no overlapping mutated gene
between the FL and ENKTL specimens. Clone evolution analysis was
also performed (Data S1). As shown
in Fig. 1E, clones 0 and 3,
harbored predominantly in ENKTL samples, were already present at
the diagnosis of FL and expanded to full clonal prevalence when
ENKTL was later diagnosed.
To better understand the nature of the tumor
microenvironment (TME), CIBERSORT analysis was applied based on
bulk RNA sequencing. As shown in Fig.
1F, the results of the CIBERSORT (immunedeconv v2.1.0) analysis
showed that the composite lymphoma of FL and ENKTL had individual
distinct TME compositions.
Case 2
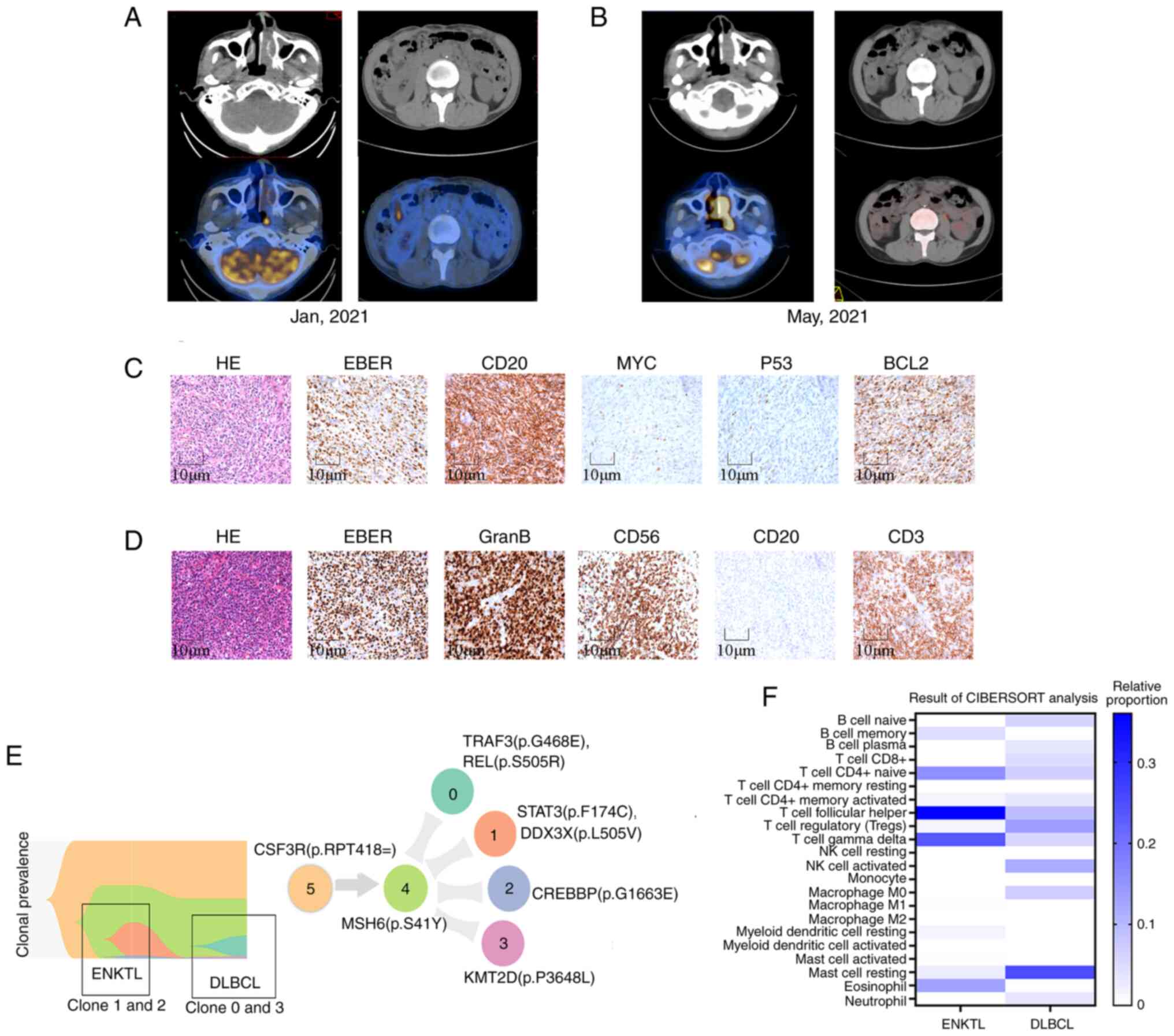
Synchronous occurrence of DLBCL and ENKT (Fig. 2). In January 2021, a 51-year-old
male patient with a recent diagnosis of DLBCL was referred to
Cancer Center, Union Hospital. The patient had undergone a partial
ileectomy and ileal-ileal side-to-end anastomosis due to ileum
perforation. PET-CT revealed pathological FDG uptake in the nasal
cavity, nasopharynx, liver, subcapsular region of liver, right
mesenteric nodes and right external iliac nodes (Fig. 2A). The postoperative pathological
diagnosis was EBV-positive DLBCL, not otherwise specified (NOS),
with immunohistochemical staining results as follows:
CD20+, CD5−, CD10−,
BCL2+, BCL6+, MUM1+,
MYC+ (30%), p53−, and EBER ISH+
(Fig. 2C). The patient was
therefore diagnosed as EBV-positive DLBCL stage IV according to the
results of pathology and PET/CT scan. The patient received R-CHOP
chemotherapy (doses as aforementioned) as the first-line treatment.
After four cycles of R-CHOP, an interim PET-CT revealed that most
of the lesions had disappeared, but the lesions of the nasal
cavity, nasopharynx and subcapsular region of the liver persisted.
Notably, fluorodeoxyglucose uptake in the nasal and nasopharyngeal
lesions was markedly increased [interim maximum standardized uptake
value (SUVmax), 16.8; baseline SUVmax, 7.9]
(Fig. 2B). A biopsy of the nasal
and nasopharyngeal lesions was performed in May 2021, and the
pathological result revealed ENKTL, nasal type. Immunohistochemical
results showed that GranB, CD3, CD56 and EBER ISH staining was
positive, while CD20 staining was negative (Fig. 2D). Therefore, the patient was
re-diagnosed with composite DLBCL and ENKTL, and treated with
pegaspargase-based chemotherapy plus sintilimab (2,500
IU/m2 pegaspargase on day 1 and 200 mg sintilimab on day
1, every 3 weeks). After six cycles of immunochemotherapy and
radiation to the nasal cavity and nasopharynx (54 Gy/27 fractions),
the patient achieved CR and received maintenance treatment with
sintilimab (200 mg, every 3 weeks) for 1 year. The patient has
remained disease-free for >30 months by far.
The results of targeted DNA sequencing demonstrated
that the predominant mutated genes were AR, BCL7H, CD79A, P2RY8,
PTPRO, REL, RELN and TRAF3 in the DLBCL specimen, while the
predominant mutated genes were PRDM1, ABL2, B2M, CREBBP, DDX3X,
FAT4, FLT1 and STAT3 in the ENKTL specimen. There was no
overlapping mutated gene between the DLBCL and ENKTL specimens.
Clone evolution analysis revealed that this case of synchronous
composite lymphoma exhibited a pattern of clonal dynamics that was
markedly different from that of case 1 (heterochronous composite
lymphoma). The ancestral clones of both the DLBCL and ENKTL samples
were characterized using CSF3R and MSH6 mutations. However, the
clonal lineages harboring PRDM1, DDX3X and STAT3 mutations
(clusters 1 and 2) in the ENKTL sample were exclusive to the clonal
lineages dominating in the DLBCL sample (clusters 0 and 3)
(Fig. 2E). The results suggested
that the two lymphomas may have evolved from totally divergent
clones.
To better understand the TME of this type of
heterochronous composite lymphoma, bulk RNA sequencing was also
conducted in these two paired samples (Fig. 2F). Results of CIBERSORT analysis
showed that the TME of synchronous composite lymphoma can vary
considerably between different subtypes.
Discussion
Composite lymphoma containing both ENKTL and B-cell
lymphoma is extremely rare. The two cases reported in the present
study broaden our understanding of composite lymphoma and allow
some speculation on such exceptional events.
The definite mechanisms behind the development of
two synchronous or heterochronous lymphoid neoplasms are not well
established due to the complexity and rarity of composite lymphoma,
and the diverse causes of different subtypes of lymphoma. One
possibility is immune dysfunction, which may induce mixed
neoplastic clones (5). EBV
infection is closely linked to the development of lymphoma,
particularly in the subtypes of ENKTL and EBV-positive DLBCL, which
reflects immune dysregulation. It is worth noting that EBV
infection may not always be present in both parts of composite
lymphoma (6,7). In some cases, previous
immunochemotherapy for malignancies could result in
immunosuppression, thus contributing to a subsequent EBV infection
and the development of lymphoma.
The present study examined EBV infection in two
cases. In the first case, EBV infection was only found in ENKTL but
not in FL. We speculated that the immunochemotherapy for the
patient's first FL could have caused immunosuppression, which led
to a subsequent EBV infection and the development of ENKTL. In the
second case, EBV infection was found in both DLBCL and ENKTL. It
was concluded that the virus infected both B-cells and NK/T cells
simultaneously, then transformed the B cells and NK/T cells
independently, forming two independent neoplastic clones.
The clonal association between the two distinct
lymphoma components is a major concern in composite lymphoma. A
number of studies have reported contradicting findings, namely that
these two components may be clonally related or unrelated (8–10).
However, the clonal association in composite DLBCL/FL and ENKTL has
not been analyzed by sequencing due to its rarity. The present
sequencing results demonstrated that composite B-cell lymphoma and
ENKTL could evolve from divergent clones.
The composition of the TME can vary widely in
synchronous or heterochronous composite lymphomas, affecting the
treatment and prognosis of patients. Notably, abundant
CD68+ macrophages were observed in the FL, DLBCL and
ENKTL samples of the present two patients. CD68+
macrophages are closely associated with the poor prognosis of
lymphoma, involving tumor growth and drug resistance (11,12).
Targeting macrophages could be a desirable treatment option.
In summary, composite B-cell lymphoma and ENKTL
lymphoma are extremely rare, with potentially distinct clonal
evolution models and TMEs. Understanding their genetic and TME
features guides accurate treatment; however, further studies are
needed to confirm the findings and interpretations of the present
study.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author. The raw sequencing data
generated in the present study may be found in the National Center
for Biotechnology Information BioProject database under accession
number PRJNA1249522 or at the following URL: https://www.ncbi.nlm.nih.gov/sra/PRJNA1249522.
Authors' contributions
QW, QL and LZ had the original idea and designed the
study. WY, XC, FZ and HP advised on patient treatment strategies,
and obtained and analyzed data. WY and FZ interpreted clinical
data. QW and QL wrote the draft. WY, XC, HP and LZ assisted in
revising the manuscript. All authors have read and approved the
final manuscript. WY, XC, FZ, HP and LZ confirm the authenticity of
all the raw data.
Ethics approval and consent to
participate
This study was approved by the Ethical Committees of
Union Hospital, Tongji Medical College, Huazhong University of
Science and Technology (Wuhan, China; approval no. 2024-0986). This
study was conducted in accordance with the principles of the
Declaration of Helsinki.
Patient consent for publication
Written consent was obtained from the patients for
their information to be published.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Küppers R, Dührsen U and Hansmann ML:
Pathogenesis, diagnosis, and treatment of composite lymphomas.
Lancet Oncol. 15:e435–e446. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Nagai S, Hiraga J, Suzuki N, Suzuki N,
Takagi Y, Narita M and Kagami Y: Composite lymphoma comprising
extranodal NK/T-cell lymphoma and diffuse Large B-cell lymphoma.
Case Rep Hematol. 2018:15839252018.PubMed/NCBI
|
|
3
|
Kawai H, Matsushita H, Kawakami S, Furuya
D, Shiraiwa-Hara S, Ichiki A, Hara R, Aoyama Y, Ogiya D, Suzuki R,
et al: A case of composite lymphoma with extranodal NK/T-cell
lymphoma, nasal-type and diffuse large B-cell lymphoma. J Clin Exp
Hematop. 59:34–39. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Swerdlow SH, Campo E, Pileri SA, Harris
NL, Stein H, Siebert R, Advani R, Ghielmini M, Salles GA, Zelenetz
AD and Jaffe ES: The 2016 revision of the World Health Organization
classification of lymphoid neoplasms. Blood. 127:2375–2390. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Suefuji N, Niino D, Arakawa F, Karube K,
Kimura Y, Kiyasu J, Takeuchi M, Miyoshi H, Yoshida M, Ichikawa A,
et al: Clinicopathological analysis of a composite lymphoma
containing both T- and B-cell lymphomas. Pathol Int. 62:690–698.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Hirose Y, Fukushima T, Masaki Y, Shimoyama
K, Karasawa H, Ogawa N and Wano Y: Epstein-Barr virus-associated
composite lymphoma composed of peripheral T-cell lymphoma and an
anaplastic variant of a diffuse large B-cell type of non-Hodgkin's
lymphoma and strongly expressing p53 protein. Int J Hematol.
79:260–265. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Campidelli C, Sabattini E, Piccioli M,
Rossi M, De Blasi D, Miraglia E, Rodriguez-Abreu D, Franscini LL,
Bertoni F, Mazzucchelli L, et al: Simultaneous occurrence of
peripheral T-cell lymphoma unspecified and B-cell small lymphocytic
lymphoma. Report of 2 cases. Hum Pathol. 38:787–792. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Pescarmona E, Pignoloni P, Orazi A, Lo
Coco F, Lavinia AM, Martelli M and Baroni CD: ‘Composite’ lymphoma,
lymphoplasmacytoid and diffuse large B-cell lymphoma of the spleen:
molecular-genetic evidence of a common clonal origin. Virchows
Arch. 435:442–446. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Dong Q, Wang Y, Xiu Y, Sakr H, Burnworth
B, Xu D, O'Brien T, Burke J, Hu S, Zeng G and Zhao C: Clonally
related composite chronic lymphocytic leukaemia and mantle cell
lymphoma. Br J Haematol. 200:660–664. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hoeller S, Zhou Y, Kanagal-Shamanna R,
Xu-Monette ZY, Hoehn D, Bihl M, Swerdlow SH, Rosenwald A, Ott G,
Said J, et al: Composite mantle cell lymphoma and chronic
lymphocytic leukemia/small lymphocytic lymphoma: A
clinicopathologic and molecular study. Hum Pathol. 44:110–121.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Barros MH, Hassan R and Niedobitek G:
Tumor-associated macrophages in pediatric classical Hodgkin
lymphoma: Association with Epstein-Barr virus, lymphocyte subsets,
and prognostic impact. Clin Cancer Res. 18:3762–3771. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gotti M, Nicola M, Lucioni M, Fiaccadori
V, Ferretti V, Sciarra R, Costanza M, Bono E, Molo S, Maffi A, et
al: Independent prognostic impact of tumour-infiltrating
macrophages in early-stage Hodgkin's lymphoma. Hematol Oncol.
35:296–302. 2017. View
Article : Google Scholar : PubMed/NCBI
|