Introduction
Skin cancer is the most frequently diagnosed cancer
among Caucasian individuals, and despite extensive public health
campaigns and preventative initiatives, its incidence continues to
rise globally (1–3). Skin cancer comprises malignant
melanoma and non-melanoma skin cancers (NMSCs), with basal cell
carcinoma (BCC) and squamous cell carcinoma (SCC) being the most
clinically significant NMSCs due to their potential for local
invasion and metastasis (4,5).
BCC, originating from basal epidermal cells,
represents 70–80% of skin cancer diagnoses, making it one of the
most prevalent types of cancer worldwide (6). BCC is histologically characterised by
basophilic nests of basal-like cells arranged in a peripheral
palisade pattern and typically exhibits slow growth (7). Although BCC is a malignant tumour, it
exhibits almost no metastatic potential (8). SCC constitutes ~20% of NMSC cases and
carries a higher risk of metastasis compared with BCC, reported to.
Be between 0.1 and 13.7% (9,10). The
lifetime risk of SCC in the United States is estimated to be 7–11%,
with its incidence increasing over recent decades; risk factors
include advanced age, fair skin and cumulative ultraviolet (UV)
radiation exposure (11–14). Clinically, SCC may present as
enlarging plaques or nodules that may ulcerate, and often arises
from the precursor lesion actinic keratosis (AK) (15). Early diagnosis and surgical
intervention typically result in excellent outcomes (16).
Melanoma, while less common, is the most aggressive
form of skin cancer and poses the greatest mortality risk due to
its high metastatic potential and resistance to therapy (17). Cutaneous melanoma originates from
melanocytes and constitutes >90% of melanoma cases in Caucasian
populations. Pathophysiologically, it is predominantly associated
with UV radiation-induced mutations, with UV radiation accounting
for >75% of melanoma cases in Caucasian populations; however,
non-UV-related subtypes exist (18–20).
Risk factors include sun exposure, high nevus count, the presence
of atypical moles, genetic predisposition and family history
(21,22). The incidence of melanoma has risen
sharply since the 1950s, with current estimates reporting ~25 new
cases per 100,000 individuals annually in Europe, 30 in the United
States, and 60 in Australia and New Zealand (23–25).
Telomeres are specialized nucleoprotein structures
capping the ends of eukaryotic chromosomes, consisting of
repetitive hexameric sequences (5′-TTAGGG-3′) that span 10–15
kilobases in humans (26–28). Telmoeres serve a critical role in
maintaining genomic integrity by safeguarding chromosome ends from
degradation and preventing end-to-end fusions (26,29).
The shelterin complex ensures telomere protection, regulates their
length and affects telomerase activity (27,28).
During DNA replication, the inability of DNA polymerase to fully
replicate 3′ends results in progressive telomere shortening by
30–200 base pairs per cell division (30). The progressive telomere attrition
results in a cellular replicative limit, termed the Hayflick limit
(31). In cells with functional
cell cycle checkpoints, critical telomere shortening results in
replicative senescence, whereas in cells with disrupted
checkpoints, telomere crisis ensues, which is resolved either by
apoptosis or the activation of telomere maintenance mechanisms
(31,32). Telomerase, a ribonucleoprotein
enzyme, permits the elongation of telomeres and is tightly
regulated, being predominantly active in stem cells, germ cells and
certain highly proliferative somatic cell populations, whereas most
somatic cells exhibit low or negligible telomerase activity
(32–34). The aberrant reactivation of
telomerase is found in most malignancies and is considered a
critical tumourigenic event (35–37).
The pathophysiology of telomere length (TL) in
cancer is complex, with research underscoring its dual role as both
a tumour suppressor via induction of apoptosis and senescence, and
an enabler of carcinogenesis via genomic instability (38–40).
The primary proposed mechanism in carcinogenesis consists of short
telomeres inducing chromosomal instability and promoting genomic
aberrations, subsequently TL is stabilized above the apoptotic
threshold through telomerase activation or alternative lengthening
mechanisms, enabling unlimited replicative potential (41,42).
The relationship between TL and cancer risk is an area of active
investigation, with findings varying by cancer type. Short
telomeres have been associated with an increased risk in
urological, head and neck, and digestive system cancers (43–46).
Studies on breast and colorectal cancers, and NMSCs, have yielded
inconclusive results, failing to demonstrate a statistically
significant association, whereas studies have indicated a
significant association between long TL and increased risk of lung
cancer and melanoma (47–51).
Corollary to the rising incidence of skin cancer is
the need for novel risk stratification and early detection
strategies aimed at prevention and timely therapeutic intervention.
Given that TL can be readily assessed through peripheral leukocyte
measurements and its centrality to cancer biology, it constitutes a
promising cancer biomarker (52–54).
The present systematic review and meta-analysis aimed to evaluate
and synthesise the current evidence on the association between TL
and skin cancer, specifically in melanoma, BCC and SCC, elucidating
the potential of TL as a risk biomarker in dermatologic
oncology.
Materials and methods
Search strategy
A systematic review and meta-analysis was conducted
to investigate the association between TL and skin cancer risk,
specifically focusing on melanoma, BCC and SCC. The present study
was developed in accordance with the Preferred Reporting Items for
Systematic Reviews and Meta-Analyses guidelines (55).
A comprehensive literature search was performed to
identify relevant studies published up to October 2024 across the
electronic databases PubMed (https://pubmed.ncbi.nlm.nih.gov/), Cochrane Library
(https://www.cochranelibrary.com/) and
Scopus (https://www.scopus.com/). The search
strategy utilized a combination of Medical Subject Headings terms
and key words related to TL and skin cancer risk. The following
terms were used: ‘telomere’, ‘telomere length’, ‘skin cancer’,
‘melanoma’, ‘basal cell carcinoma’, ‘squamous cell carcinoma’ and
‘skin neoplasms’. Logical operators ‘AND’ and ‘OR’ were employed to
combine the search terms effectively. Additionally, bibliographies
of relevant reviews were examined to identify any further eligible
studies.
Eligibility criteria
Studies were included based on predefined
eligibility criteria, with additional criteria applied for
inclusion in the quantitative synthesis. The eligibility criteria
were structured based on the PICO framework, as follows:
P (population), eligible studies investigated
individuals at risk for developing melanoma, SCC or BCC. Studies
focusing on non-malignant or premalignant conditions, such as AK
and Bowen's disease (BD), were excluded. Similarly, extracutaneous
melanoma, including mucosal and ocular melanoma, and malignancies
of the skin other than melanoma, BCC and SCC, such as cutaneous
lymphoma, were excluded from both the quantitative and qualitative
analyses. All included studies involved human populations, studies
involving non-human subjects or cell lines were excluded.
I (intervention/exposure), to be eligible, studies
had to explore the relationship between TL and the risk of skin
cancer by directly measuring TL in any human biological sample,
including tissue or peripheral blood leukocytes (PBLs), while
studies reporting indirect measurements, such as genetic risk
score, were excluded.
C (comparison), the comparison groups included
individuals with and without skin cancer, or patient samples from
malignant tissue and normal skin tissue. Studies that lacked a
control group or comparator were excluded.
O (outcome), for the qualitative synthesis, a
descriptive analysis of the relevant association was required. For
inclusion in the quantitative analysis of risk, studies were
required to report relative risk estimates, including odds ratios
(ORs), risk ratios or hazard ratios (HRs), with corresponding 95%
confidence intervals (CIs).
Eligible studies followed an observational design
employing a cohort, case-control or nested case-control design.
Review articles, meta-analyses, case reports, conference abstracts
and dissertations were excluded. Only articles published in English
were included, but no restrictions were applied regarding the
publication date.
Study selection and data
extraction
All retrieved articles were initially screened
against the eligibility criteria based on titles and abstracts.
Full-text articles were thoroughly examined in studies that
appeared to meet the inclusion criteria or when eligibility was
uncertain. Two independent reviewers conducted the initial
screening and the evaluation of the full-text articles to determine
inclusion. Any conflicts were resolved through discussion and
consensus.
Data extraction was conducted independently by two
reviewers using a standardized data extraction form developed for
the present study. Any discrepancies were resolved by consensus.
For all eligible studies, the extracted data included: Study name,
first author name, year of publication, location, cancer type, the
racial or ethnic composition of the study population, information
about the source of cases, study design, age and sex distribution
among both cases and controls, number of cases and controls, method
of TL measurement, tissue source of the DNA, cut-off values used
for categorizing TL, relative risk measure and the corresponding
95% CIs. If an article included multiple non-overlapping datasets,
they were considered independent individual studies. Between
studies with overlapping samples for the same outcome, the study
with the largest number of cases was included in the meta-analysis.
If sample sizes were similar, the study that adjusted for the
greatest number of covariates was selected.
Qualitative synthesis
All studies that met the inclusion criteria,
including those incorporated into the quantitative synthesis
(meta-analysis), were included in the qualitative synthesis. This
synthesis involved systematically reviewing and interpreting the
findings of each study.
Quantitative synthesis
Data preparation
In the quantitative synthesis, the relative risk for
comparing patients with the longest TLs to the shortest was
utilized, with the longest being used as the reference. In studies
reporting TL as a continuous variable, the reported effect estimate
per unit decrease in TL was utilized. To maintain consistency in
the direction of the effect, effect estimates were transformed when
necessary, so that long TL was always the reference. In studies
with multiple relative risk measures, the most fully adjusted risk
measure was included in the meta-analysis.
Meta-analysis
The statistical heterogeneity between studies was
assessed using Cochran's Q test and quantified with the
I2 statistic. P<0.10 for the Q test was considered
indicative of significant heterogeneity. The I2
statistic, describing the percentage of total variation across
studies due to heterogeneity rather than chance, was utilised to
quantify heterogeneity, with values of 25, 50 and 75% representing
low, moderate and high heterogeneity, respectively (56,57).
The random-effects model, based on the DerSimonian and Laird
method, which accounts for both within-study and between-study
variability was used (58). When
pooling risk measures, they were transformed by taking the natural
logarithm and their standard errors were utilised for the
meta-analysis (57).
To explore potential sources of heterogeneity and to
assess the robustness of the findings, subgroup analyses were
performed based on sex, location, subtype by genetic predisposition
(familial vs. sporadic), population source (hospital vs. general
population), and adjustment for skin cancer specific confounders.
Sensitivity analyses were conducted by sequentially removing each
study to evaluate its influence on the overall pooled
estimates.
All statistical analyses were conducted using R
software (version R 4.4.1; http://www.r-project.org/) with the ‘meta’ (https://cran.r-project.org/package=meta)
and ‘metafor’ (https://cran.r-project.org/package=metafor) packages.
Two-tailed P<0.05 was considered to indicate a statistically
significant difference, except where otherwise specified.
Assessment of publication bias
Publication bias was evaluated using funnel plots
for visual inspection, and Egger's regression asymmetry test was
conducted to statistically assess the presence of small-study
effects (59,60). P<0.05 was considered indicative
of potential publication bias.
Quality assessment
Risk of bias was independently assessed by two
reviewers using the Newcastle-Ottawa Scale (NOS) for observational
studies (61). The NOS evaluates
studies based on three domains: Selection of participants,
comparability of study groups, and ascertainment of exposure and
outcomes. The maximum score a study could receive is nine stars.
Studies scoring seven or more stars were considered high quality,
those scoring five to six were considered moderate quality, and
those scoring below five were considered low quality. Any
discrepancies in quality assessments were resolved by
consensus.
Results
Study selection
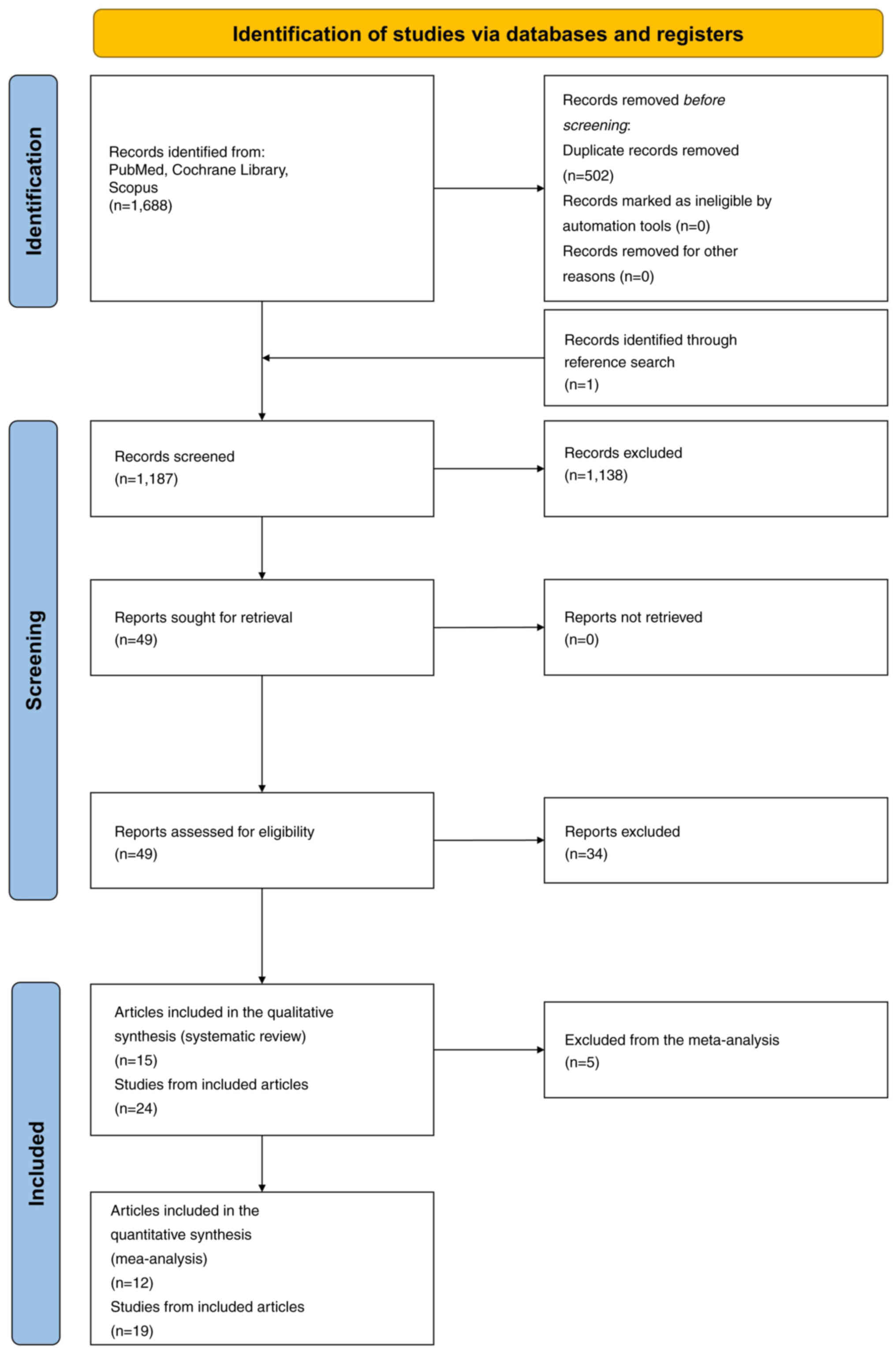
The systematic search yielded a total of 1,688
articles from PubMed, Cochrane Library and Scopus (Fig. 1). One additional study was
identified through cross-referencing. After removing duplicates,
1,187 articles were screened based on title and abstract, and 1,138
were excluded as irrelevant to the research question. The full
manuscripts for the remaining 49 articles were acquired. Upon
thorough examination, 34 articles were excluded based on the
eligibility criteria, including lack of a control group, non-human
subjects and insufficient information on TL.
Subsequently, all studies with overlapping samples
for the same outcome were excluded from the present analysis.
Specifically, the study by Han et al (2009) (62) on BCC in the Nurses' Health Study
(NHS) population, the study by Nan et al (2011) (63) on melanoma in the NHS population, and
the study by Weischer et al (2013) (64) on melanoma in the Copenhagen City
Heart Study & Copenhagen General Population Study population
were not included, thus the included studies were 24 derived from
15 articles.
Study characteristics
The key characteristics of the included studies are
detailed in Table ITable IITable III [country, study type and
design, population demographics (ethnicity, sex distribution, age
of cases and controls), sample sizes, TL measurement methods, DNA
source, effect estimates with 95% confidence intervals, TL
categorization and covariates adjusted for]. Among the 24 studies
included, 12 focused on melanoma, seven on BCC, and five on SCC.
The studies eligible for quantitative analysis comprised 19
studies, among which 12 focused on melanoma, four on BCC and three
on SCC.
 | Table I.General characteristics of studies
included in the meta-analysis. |
Table I.
General characteristics of studies
included in the meta-analysis.
| First author,
year | Country | Type | Population | Ethnicity | Male cases | Male controls | Mean age of cases,
years | Mean age of
controls, years | (Refs.) |
|---|
| Han, 2009 | USA | Melanoma | NHS | European | 0% | 0% | 63.3 | 64.5 | (62) |
| Han, 2009 | USA | SCC | NHS | European | 0% | 0% | 64.7 | 64.5 | (62) |
| Nan, 2011 | USA | Melanoma | WHI-OS | European | 0% | 0% | 68.2 | 63.9 | (63) |
| Nan, 2011 | USA | Melanoma | HPFS | European | 100% | 100% | 65.3 | 59.9 | (63) |
| Liang, 2011 | USA | SCC | HPFS | Caucasian | 100% | 100% | 69 | 63.1 | (75) |
| Liang, 2011 | USA | BCC | NHS | Caucasian | 0% | 0% | 66.1 | 56.3 | (75) |
| Liang, 2011 | USA | BCC | NHS | Caucasian | 0% | 0% | 69.3 | 61 | (75) |
| Bodelon, 2012 | Italy | Melanoma | Hospital-based | Mediterranean
Caucasian | Mixed-not
specified | Mixed-not
specified | Not specified | Not specified | (69) |
| Anic, 2013 | USA | Melanoma | Hospital-based | European | 57% | 35% | 58.6 | 56.3 | (66) |
| Anic, 2013 | USA | SCC | Hospital-based | European | 67% | 35% | 64.8 | 56.3 | (66) |
| Anic, 2013 | USA | BCC | Hospital-based | European | 60% | 35% | 63 | 56.3 | (66) |
| Burke, 2013 | USA | Melanoma | Hospital-based | Caucasian | 50.40% | 41.80% | Not specified | Not specified | (72) |
| Llorca-Cardeñosa,
2014 | Spain | Melanoma | Hospital-based | Caucasian (Spanish
origin) | 45.40% | 42.90% | 53 | 48 | (70) |
| Menin, 2016 | Italy | Familial
melanoma | Hospital-based | Caucasian | 45.00% | 43.50% | 54.2 | 53.8 | (71) |
| Menin, 2016 | Italy | Sporadic
melanoma | Hospital-based | Caucasian | 42.00% | 43.50% | 53.5 | 53.8 | (71) |
| Rode, 2016 | Denmark | Melanoma | CGPS &
CCHS/Population | Danish
(European) | Mixed-Not
specified | Mixed-Not
specified | Not specified | Not specified | (50) |
| Rachakonda,
2018 | Germany | Melanoma | Hospital-based | Caucasian | 0.405 | 0.448 | 54 | 44 | (67) |
| Srinivas, 2019 |
Hungary/Romania/Slovakia | BCC | Hospital-based | Central/Eastern
European | 44.70% | 51.40% | 67 | 61 | (74) |
| Schneider,
2022 | UK | Melanoma | UK
Biobank/Population | Predominantly
Caucasian | Mixed-not
specified | 46% | Not specified | 57 | (68) |
| Table II.Summary of study characteristics and
associated risk estimates across studies included in the
meta-analysis. |
Table II.
Summary of study characteristics and
associated risk estimates across studies included in the
meta-analysis.
| First author,
year | Study design | Cases/controls | Measurement
method | DNA source | Relative risk (95%
CI) | TL
categorization | Factors
adjusted | (Refs.) |
|---|
| Han, 2009 Melanoma
(NHS) | Nested
case-control | 218/870 | RTL (T/S ratio)
qPCR | PBLs | 0.62
(0.31–1.23) | RTL Q4 (longest)/Q1
(shortest) | Age, number of
moles | (62) |
| Han, 2009 SCC
(NHS) | Nested
case-control | 285/870 | RTL (T/S ratio)
qPCR | PBLs | 0.72
(0.33–1.55) | RTL Q4 (longest)/Q1
(shortest) | Age, number of
moles | (62) |
| Nan, 2011 Melanoma
(WHI-OS) | Nested
case-control | 233/237 | RTL (T/S ratio)
qPCR | PBLs | 0.40
(0.18–0.88) | RTL Q4 (longest)/Q1
(shortest) | Age | (63) |
| Nan, 2011 Melanoma
(HPFS) | Nested
case-control | 120/120 | RTL (T/S ratio)
qPCR | PBLs | 0.18
(0.06–0.56) | RTL Q4 (longest)/Q1
(shortest) | Age | (63) |
| Liang, 2011 SCC
(HPFS) | Nested
case-control | 241/241 | RTL (T/S ratio)
qPCR | PBLs | 1.09
(0.62–1.93) | RTL Q4 (longest)/Q1
(shortest) | Age | (75) |
| Liang, 2011 BCC
(NHS 1) | Nested
case-control | 260/260 | RTL (T/S ratio)
qPCR | PBLs | 0.96
(0.49–1.87) | RTL Q4 (longest)/Q1
(shortest) | Age | (75) |
| Liang, 2011 BCC
(NHS 2) | Nested
case-control | 363/1683 | RTL (T/S ratio)
qPCR | PBLs | 0.91
(0.66–1.25) | RTL Q4 (longest)/Q1
(shortest) | Age | (75) |
| Bodelon, 2012
Melanoma | Case-control | 172/196 | RTL (T/S ratio)
qPCR | PBLs | 0.87
(0.46–1.64) | RTL as a continuous
variable | Age, sex | (69) |
| Anic, 2013
Melanoma | Case-control | 198/372 | RTL (T/S ratio)
qPCR | PBLs | 0.22
(0.13–0.38) | RTL Q3 (longest)/Q1
(shortest) | Age, sex | (66) |
| Anic, 2013 SCC | Case-control | 136/372 | RTL (T/S ratio)
qPCR | PBLs | 25.00
(11.11–50.00) | RTL Q3 (longest)/Q1
(shortest) | Age, sex | (66) |
| Anic, 2013 BCC | Case-control | 185/372 | RTL (T/S ratio)
qPCR | PBLs | 10.00
(5.26–16.67) | RTL Q3 (longest)/Q1
(shortest) | Age, sex | (66) |
| Burke, 2013
Melanoma | Case-control | 119/208 | RTL (T/S ratio)
qPCR | PBLs | 0.36
(0.13–0.98) | RTL Q3 (longest)/Q1
(shortest) | Age, sex, DNA
source, CDKN2A status, number of moles, solar injury, MC1R
genotype | (72) |
| Llorca-Cardeñosa,
2014 Melanoma | Case-control | 406/406 | RTL (T/S ratio)
qPCR | PBLs | 0.04
(0.01–0.10) | RTL Q4 (longest)/Q1
(shortest) | Age | (70) |
| Menin, 2016 FM | Case-control | 109/216 | RTL (T/S ratio)
qPCR | PBLs | 0.46
(0.23–0.95) | RTL Q4 (longest)/Q1
(shortest) | Age, sex | (71) |
| Menin, 2016 SM | Case-control | 201/216 | RTL (T/S ratio)
qPCR | PBLs | 1.74
(1.00–3.04) | RTL Q4 (longest)/Q1
(shortest) | Age, sex | (71) |
| Rode, 2016
Melanoma | Cohort study | 289/64750 | RTL (T/S ratio)
qPCR | PBLs | 0.98
(0.95–1.01) | RTL as a continuous
variable, per 200 base-pairs decrease | Age, sex, body mass
index, smoking status, tobacco consumption, alcohol intake | (50) |
| Rachakonda, 2018
Melanoma | Case-control | 1275/904 | RTL (T/S ratio)
qPCR | PBLs | 0.41
(0.33–0.52) | RTL as continuous
variable | Age, sex, skin
phototype, hair colour, eye colour, sun burns, outdoor occupation,
number of nevi | (67) |
| Srinivas, 2019
BCC | Case-control | 506/513 | RTL (T/S ratio)
qPCR | PBLs | 4.09
(2.86–5.85) | RTL Q3 (longest)/Q1
(shortest) | Age, sex, country,
arsenic exposure, skin complexion, skin response, MC1R genotype,
XRCC3 rs861539 | (74) |
| Schneider, 2022
Melanoma | Cohort study | NR/472 432 | RTL (T/S ratio)
qPCR | PBLs | 0.80
(0.71–0.89) | RTL as a continuous
variable, decreased telomere length (per SD) | Age, sex, body mass
index, ethnicity, current smoking, cumulative smoking, alcohol
intake, Charlson Comorbidity Index | (68) |
| Table III.General characteristics and findings
of studies included in the systematic review but not in the
meta-analysis. |
Table III.
General characteristics and findings
of studies included in the systematic review but not in the
meta-analysis.
| First author,
year | Country | Type | Cases/controls | Measurement
method | DNA source | Findings | (Refs.) |
|---|
| Wainwright,
1995 | UK | BCC | 20/19 | Southern
blotting | Fresh/frozen skin
tissue | Telomeres in 13/20
BCC cases were longer than in the adjacent epidermis (no measure of
significance reported) | (76) |
| Perrem, 2007 | Ireland | SCC | 44/10 (RTR) | TEL-FISH | Archival tissue
samples | Telomeres in SCC
tissue from RTRs were significantly shorter than those in normal
skin from RTRs (P=0.0001) | (77) |
| Perrem, 2007 | Ireland | SCC | 44/10 | TEL-FISH | Archival tissue
samples | Telomeres in SCC
tissue from non-RTRs were significantly shorter than those in
normal skin (P=0.0001) | (77) |
| Perrem, 2008 | Ireland | BCC | 35/10 (RTR) | TEL-FISH | Archival tissue
samples | Telomeres in BCC
tissue from RTRs were significantly shorter than those in normal
skin (P=0.0130) | (73) |
| Perrem, 2008 | Ireland | BCC | 35/10 | TEL-FISH | Archival tissue
samples | Telomeres in BCC
were shorter than those in normal skin, but the observation did not
reach statistical significance (P=0.2530) | (73) |
The majority of the studies included in the present
qualitative synthesis were conducted in the United States (11
studies), with additional studies from Ireland (four studies),
Italy (three studies), Germany (one study), UK (two studies),
Denmark (one study), Spain (one study) and Hungary/Romania/Slovakia
(one study). In the meta-analysis, the United States (11 studies)
was the most prevalent location, followed by Italy (three studies),
Denmark (one study), Spain (one study), Hungary/Romania/Slovakia
(one study), Germany (one study) and the UK (one study).
Participants in the included studies were predominantly of European
and American ancestry. In the meta-analysis, the population was
exclusively Western. The age of participants ranged from mid-50s to
early 70s. Two studies focused exclusively on male patients and
five exclusively on female patients. In studies included in the
meta-analysis, a combination of nested case-control designs (seven
studies), prospective cohort studies (two studies) and case-control
studies (10 studies) was observed. The source of DNA was PBL in 19
studies and malignant tissue samples in five studies. Quantitative
polymerase chain reaction (qPCR) was the primary method for TL
determination (19 studies), followed by telomere fluorescence in
situ hybridization (TEL-FISH) (four studies) and Southern
blotting (one study). All studies in the meta-analysis measured TL
using qPCR techniques on PBLs, ensuring methodological
consistency.
Relative risk measures were reported as ORs with 95%
CIs provided, or as HRs in some melanoma studies, where the rare
disease principle applies, thus HRs were considered equivalent to
ORs (65). In four studies where
the short TL was used as the reference, the relative risk was
inverted to achieve homogeneity (66,67).
Two studies analysed TL as a continuous variable, assessing risk
per unit decrease or increase in TL. In studies reporting risk per
increase, the relative risk was inverted to maintain homogeneity in
the direction of the effect (50,68).
Qualitative synthesis
The association between TL and melanoma risk was
investigated in the study by Han et al (2009) (62), where no significant association was
found between TL and melanoma risk (OR: 0.62; 95% CI: 0.31–1.23).
Similarly, Bodelon et al (2012) (69) reported no significant association
(OR: 0.87; 95% CI: 0.46–1.64).
Nan et al (2011) (63) revealed a significant inverse
association in the Women's Health Initiative Observational Study
cohort (OR: 0.40; 95% CI: 0.18–0.88) and the Health Professionals
Follow-up Study cohort (OR: 0.18; 95% CI: 0.06–0.56), indicating
that shorter telomeres were associated with reduced melanoma risk.
Anic et al (2013) (66) also
observed a strong inverse association (OR: 0.22; 95% CI:
0.13–0.38). Llorca-Cardeñosa et al (2014) (70) reported a significant inverse
association between shorter telomeres and melanoma risk (OR: 0.04;
95% CI: 0.01–0.10). Rachakonda et al (2018) (67) also demonstrated a significant
association (OR: 0.41; 95% CI: 0.33–0.52), reinforcing the
hypothesis that shorter telomeres reduce melanoma risk. By
contrast, Menin et al (2016) (71) reported that, in sporadic melanoma
cases, shorter telomeres were associated with an increased risk
(OR: 1.74; 95% CI: 1.00–3.04; P=0.051), although the association
did not reach statistical significance, whereas in familial cases,
shorter telomeres were associated with a reduced risk (OR: 0.46;
95% CI: 0.23–0.95). Burke et al (2013) (72) also identified an inverse association
between short TL and familial melanoma risk (OR: 0.36; 95% CI:
0.13–0.98). Large cohort studies provided mixed results. Rode et
al (2016) (50) found no
significant association (OR: 0.98; 95% CI: 0.95–1.01) in a Danish
population-based cohort. Schneider et al (2022) (68), analysing the UK Biobank data,
observed that shorter telomeres were associated with decreased
melanoma risk (OR: 0.80; 95% CI: 0.71–0.89).
In studies in BCC, Perrem et al (2008)
(73) found significantly shorter
telomeres in BCC in renal transplant recipients compared with in
normal skin; however, in non-transplant patients the relationship
did not reach significance. Anic et al (2013) (66) observed a strong significant
association, suggesting that shorter telomeres may increase BCC
risk (OR: 10.00; 95% CI: 5.26–16.67). Srinivas et al (2019)
(74) concurred, finding a
significant association, with shorter telomeres increasing BCC risk
(OR: 4.09; 95% CI: 2.86–5.85). By contrast, Liang et al
(2011) (75) conducted two nested
case-control studies within the NHS and found no significant
association (NHS 1: OR: 0.96; 95% CI: 0.49–1.87; NHS 2: OR: 0.91;
95% CI: 0.66–1.25). Wainwright et al (1995) (76) found that in BCC tissue samples,
telomeres were longer than in the adjacent epidermis, but no
measure of significance was reported.
In SCC, Perrem et al (2007) (77) found significantly shorter telomeres
in SCC in both renal transplant recipients and non-transplant
patients compared with that in normal skin. Anic et al
(2013) (66) observed a strong
significant association (OR: 25.00; 95% CI: 11.11–50.00),
indicating shorter telomeres increase SCC risk. By contrast, Han
et al (2009) (62) found no
significant association between TL and SCC risk (OR: 0.72; 95% CI:
0.33–1.55). Liang et al (2011) (75) also reported no significant
association (OR: 1.09; 95% CI: 0.62–1.93).
Meta-analysis results
The meta-analysis was conducted using the
random-effects model, based on the DerSimonian and Laird method,
due to the substantial heterogeneity observed among the studies, as
indicated by high I2 statistics and significant
Cochran's Q tests. This model accounts for both within-study and
between-study variability attributable to heterogeneity across
studies (56,58).
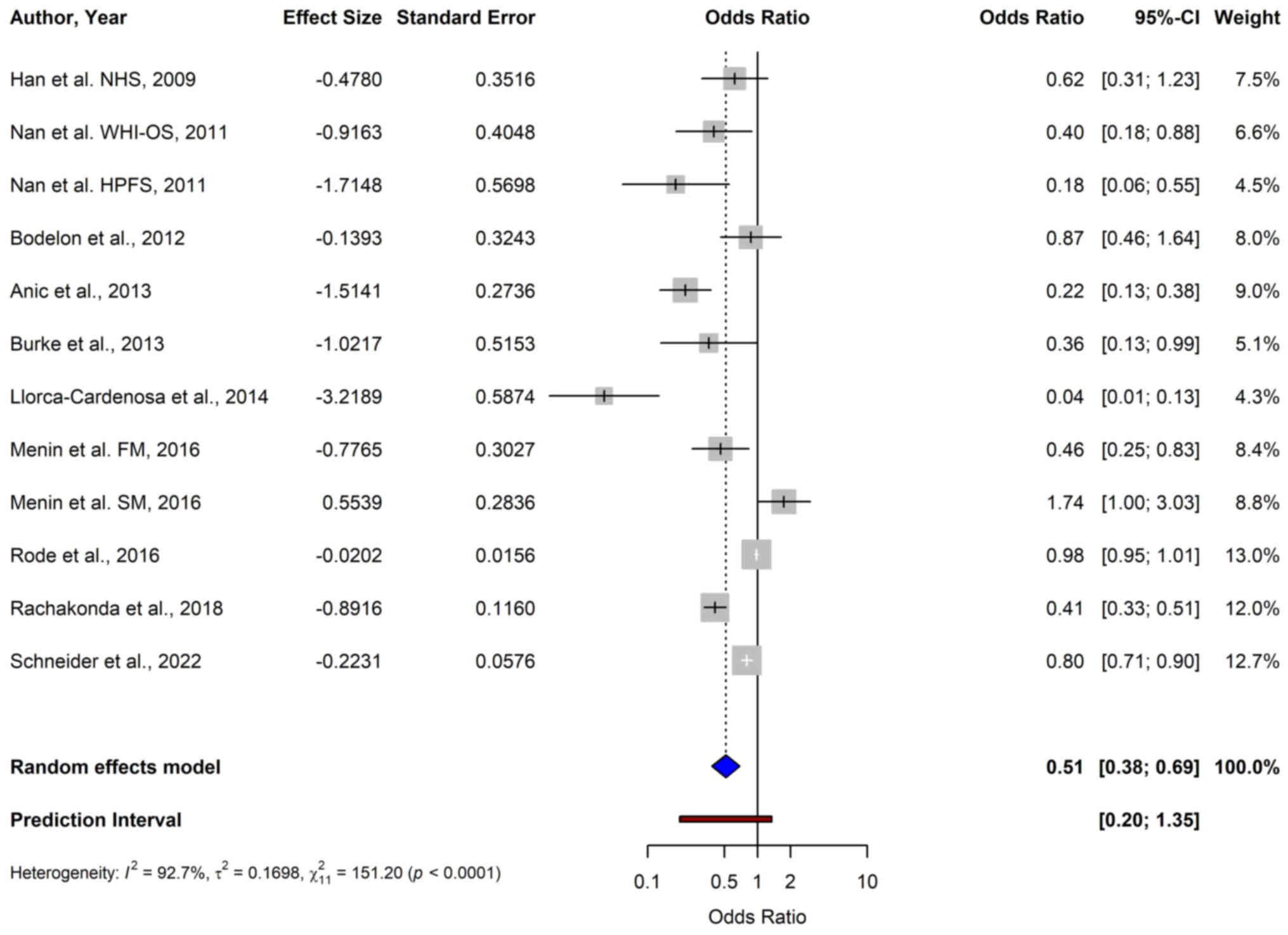
For melanoma, the pooled OR from 12 studies using
the random-effects model was 0.51 (95% CI: 0.38–0.69),
demonstrating a significant association between shorter TL and a
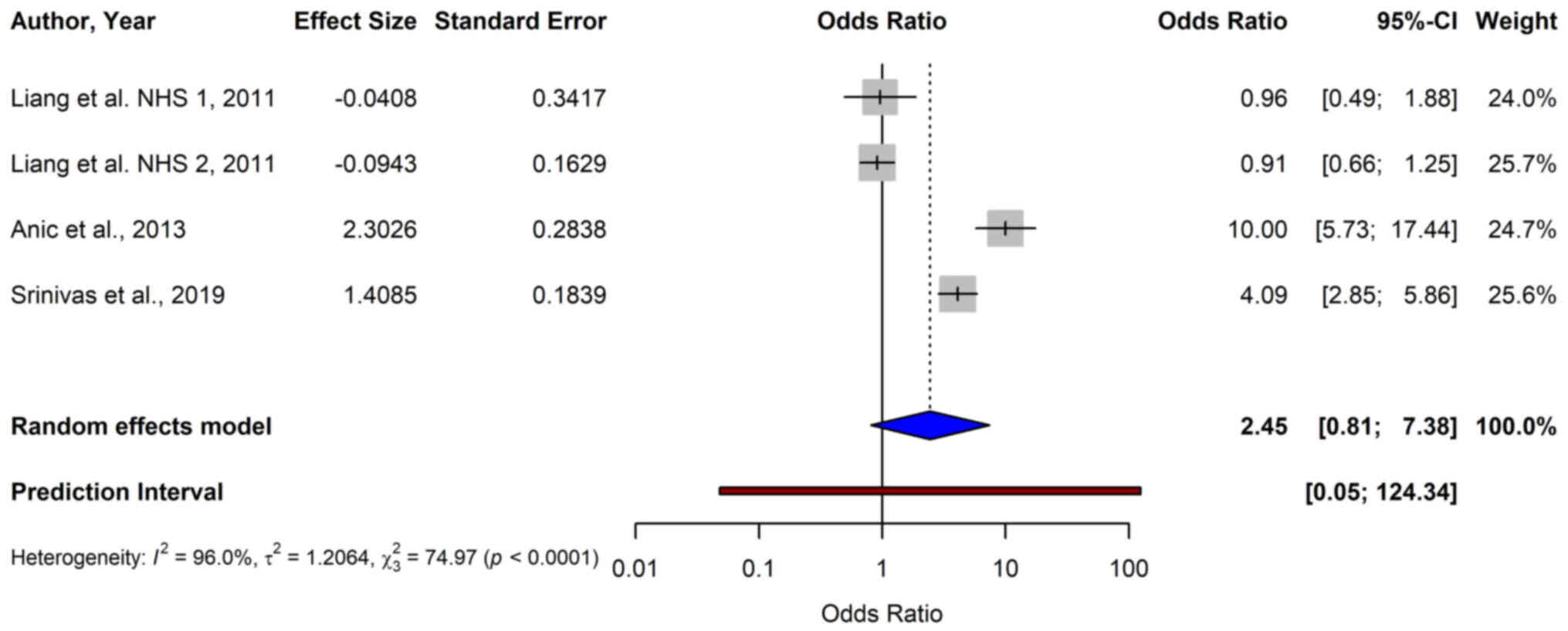
reduced risk of melanoma (P<0.0001) (Fig. 2). For BCC, the data from four
studies yielded a pooled OR of 2.45 (95% CI: 0.81–7.38), indicating
no significant association between TL and BCC risk (P=0.1124)
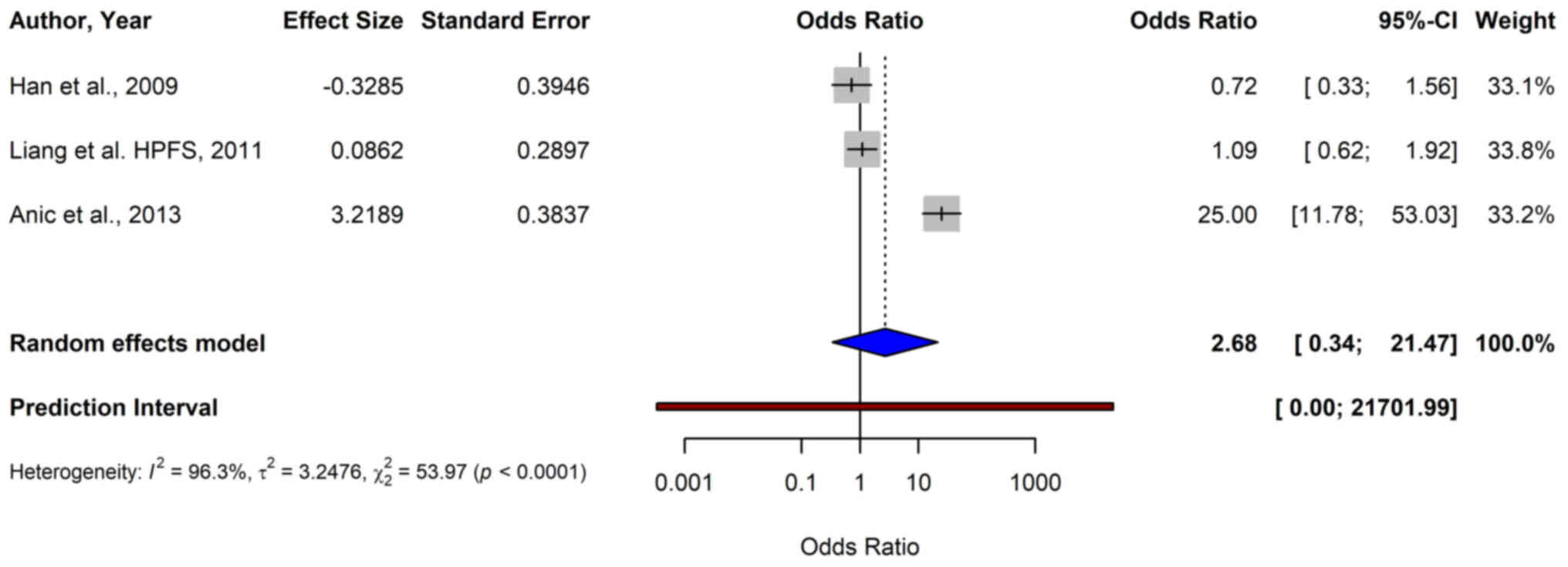
(Fig. 3). The meta-analysis of SCC
included three studies, and resulted in a pooled OR of 2.68 (95%
CI: 0.34–21.47), which was not statistically significant (P=0.3519)
(Fig. 4).
Subgroup analysis results
To further elucidate the relationship between TL and
melanoma risk, subgroup analyses were conducted based on geographic
location, sex, genetic predisposition, population source and level
of adjustment. Subgroup analyses for BCC and SCC were not performed
due to paucity of data.
Geographic location
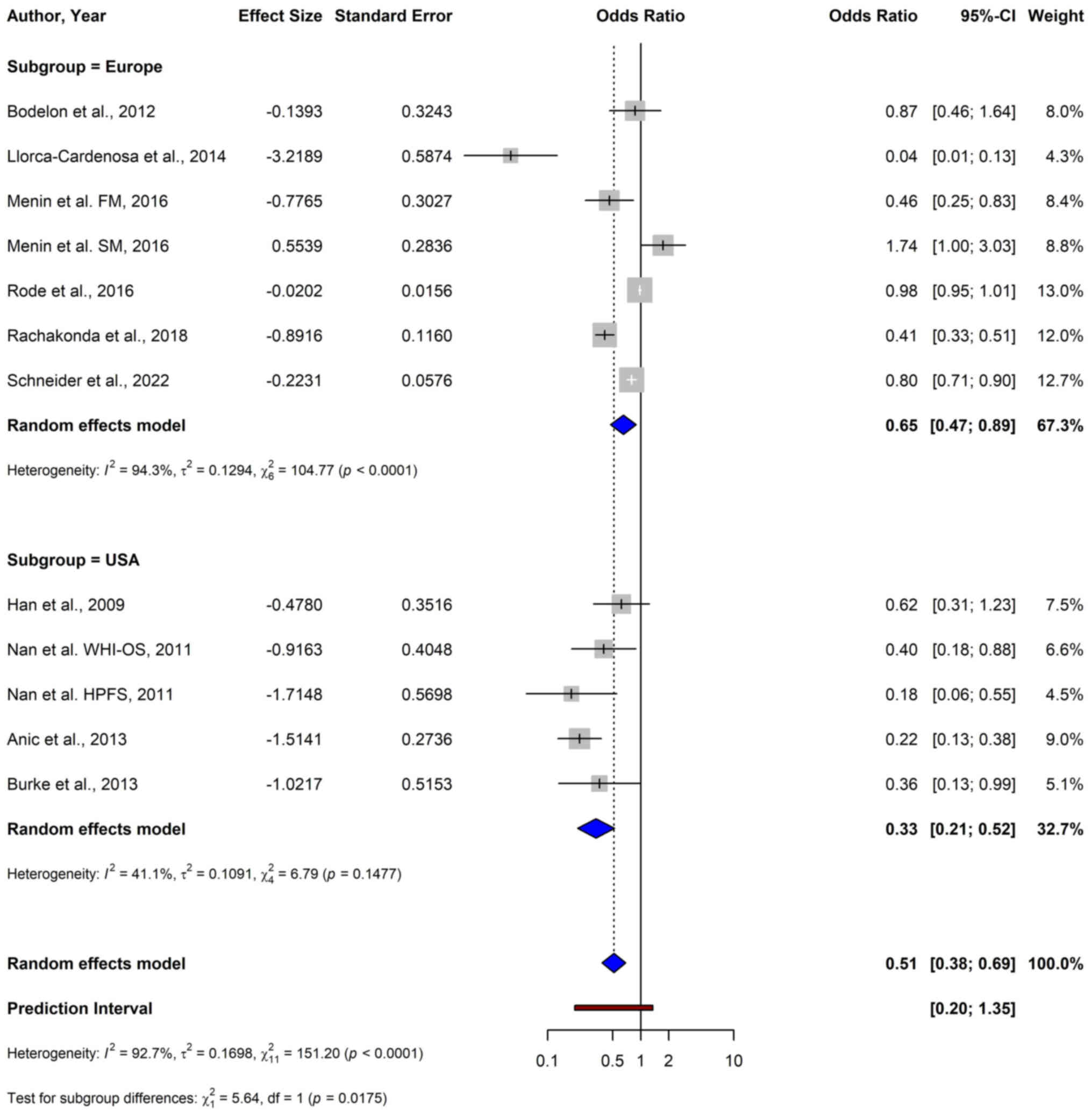
In subgroup analyses based on geographic location, a
significant inverse association between short TL and melanoma risk
was observed across geographic locations. Studies conducted in the
USA demonstrated a stronger association, with a pooled OR of 0.33
(95% CI: 0.21–0.52), compared with studies conducted in Europe,
which reported a pooled OR of 0.65 (95% CI: 0.47–0.89) (Fig. 5). The test for subgroup differences
was statistically significant (P=0.0175), indicating that while the
association was significant in both groups, the magnitude of the
effect may vary by geographic region.
Sex
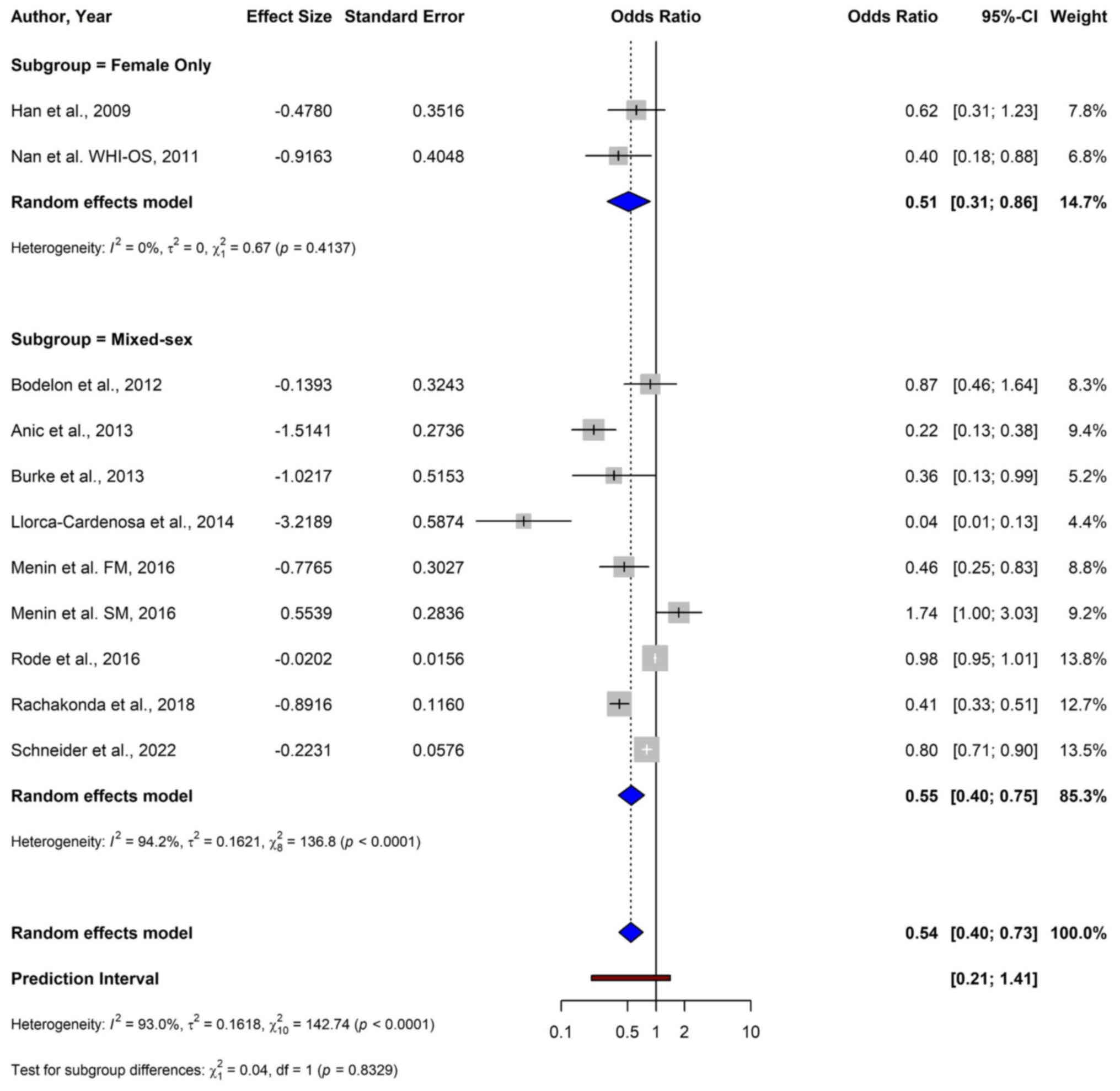
In studies restricted to female patients, a
significant inverse association between shorter TL and melanoma
risk, with a pooled OR of 0.51 (95% CI: 0.31–0.86) was reported
(Fig. 6). Mixed-sex studies
demonstrated a similar association, with a pooled OR of 0.55 (95%
CI: 0.40–0.75). The test for subgroup differences between
female-only studies and mixed-sex studies was not statistically
significant (P=0.833), suggesting that the effect of TL on melanoma
risk was consistent across the sexes.
Genetic predisposition
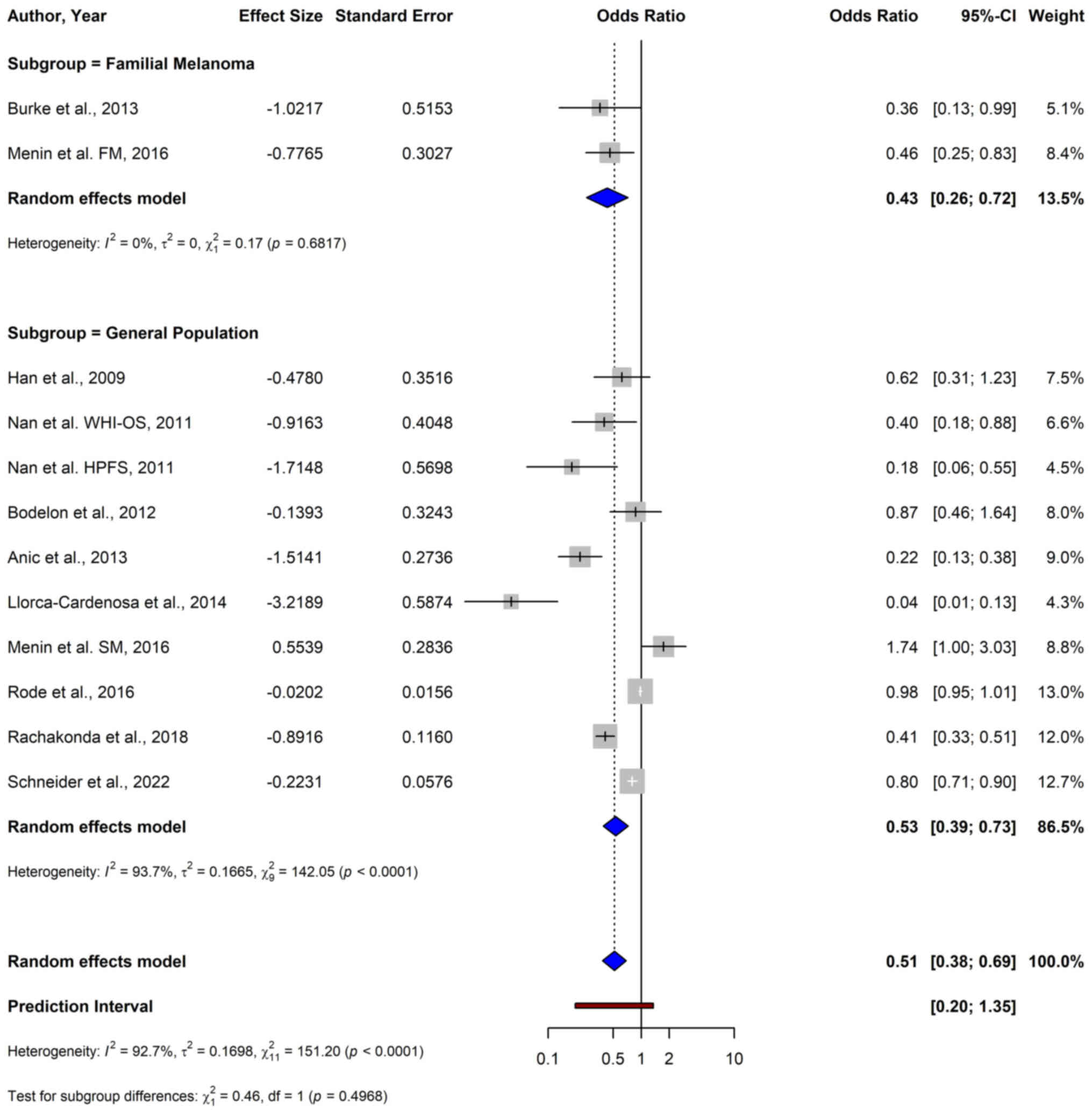
In familial melanoma, a significant inverse
association between shorter TL and melanoma risk was shown (pooled
OR: 0.43; 95% CI: 0.26–0.72) (Fig.
7). In the general population studies, the pooled OR was 0.53
(95% CI: 0.39–0.73), indicating a similar significant association.
The test for subgroup differences was not significant (P=0.497).
Additionally, to examine the potential impact of familial melanoma
cases that may have been included in the general population
studies, an analysis was performed assuming 10% familial melanoma
cases in the general population. It was assumed that familial cases
in the general population had an effect of OR=0.43, as indicated by
the subgroup analysis, and sporadic cases had an OR of 1,
indicating no association. As ORs are multiplicative, the
calculation was performed on the logarithmic scale: A weighted
average of the log(OR) values was computed, with weights reflecting
the assumed proportions of familial and sporadic cases. The
resulting weighted log(OR) was then exponentiated to obtain the
expected overall OR of 0.92.
Population source
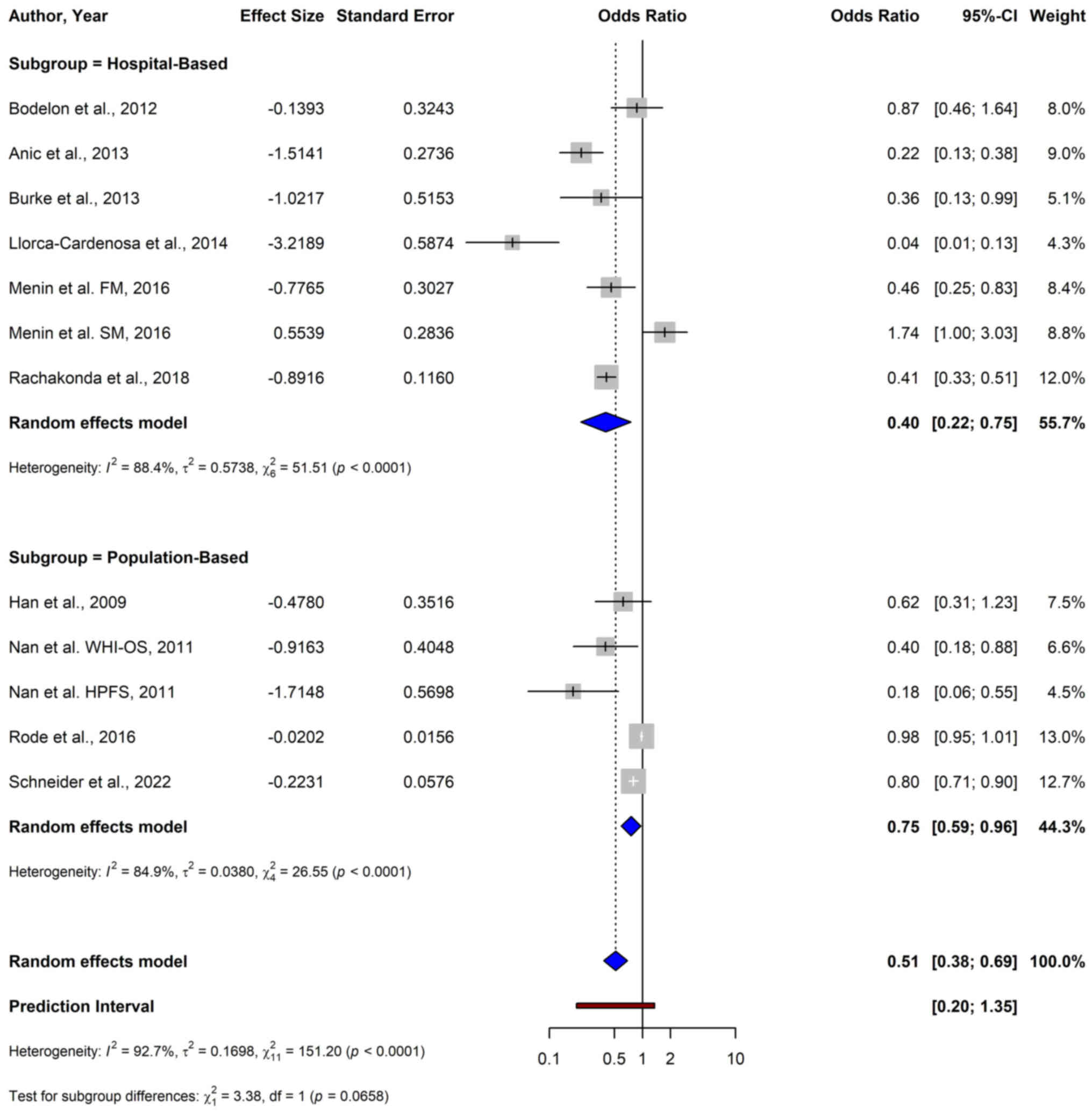
Subgroup analysis based on the source of the sample
reported a significant inverse association between shorter TL and
melanoma risk, with a pooled OR of 0.40 (95% CI: 0.22–0.75) in
hospital-based studies (Fig. 8).
Similarly, in population-based studies, a significant protective
association, with a pooled OR of 0.75 (95% CI: 0.59–0.96) was
shown. The test for subgroup differences between hospital- and
population-based studies was not significant (P=0.066).
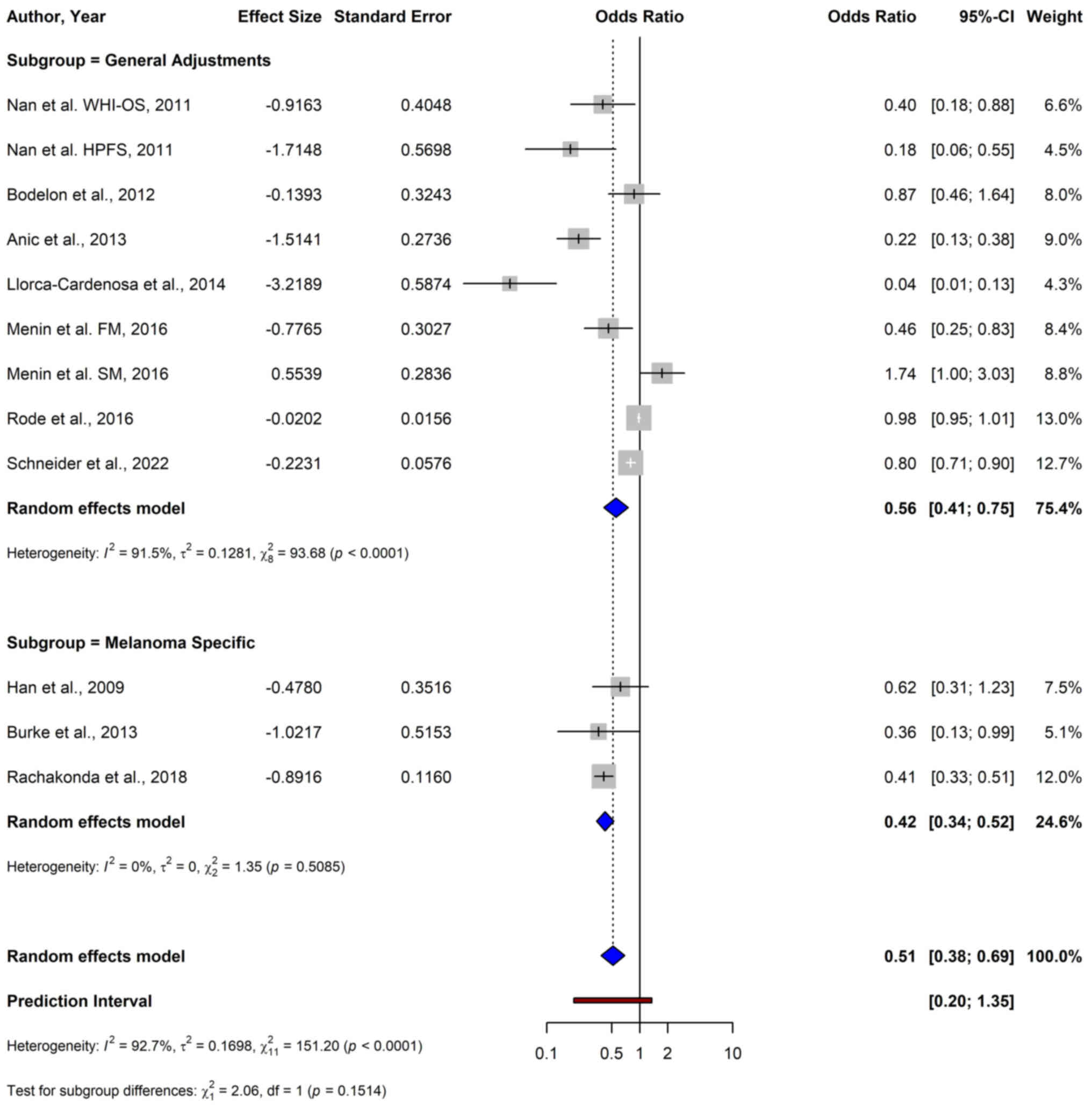
Adjustment level
Subgroup analysis based on stratification by
adjustment level demonstrated significant inverse associations
between TL and melanoma risk, with a pooled OR of 0.42 (95% CI:
0.34–0.52) in the melanoma-specific subgroup and a pooled OR of
0.56 (95% CI: 0.41–0.75) in the subgroup with general adjustments
[non-melanoma-specific adjustments, such as demographic factors
(e.g., age, sex) and lifestyle variables (e.g., smoking, alcohol
consumption)] (Fig. 9). The test
for subgroup differences was not significant (P=0.151).
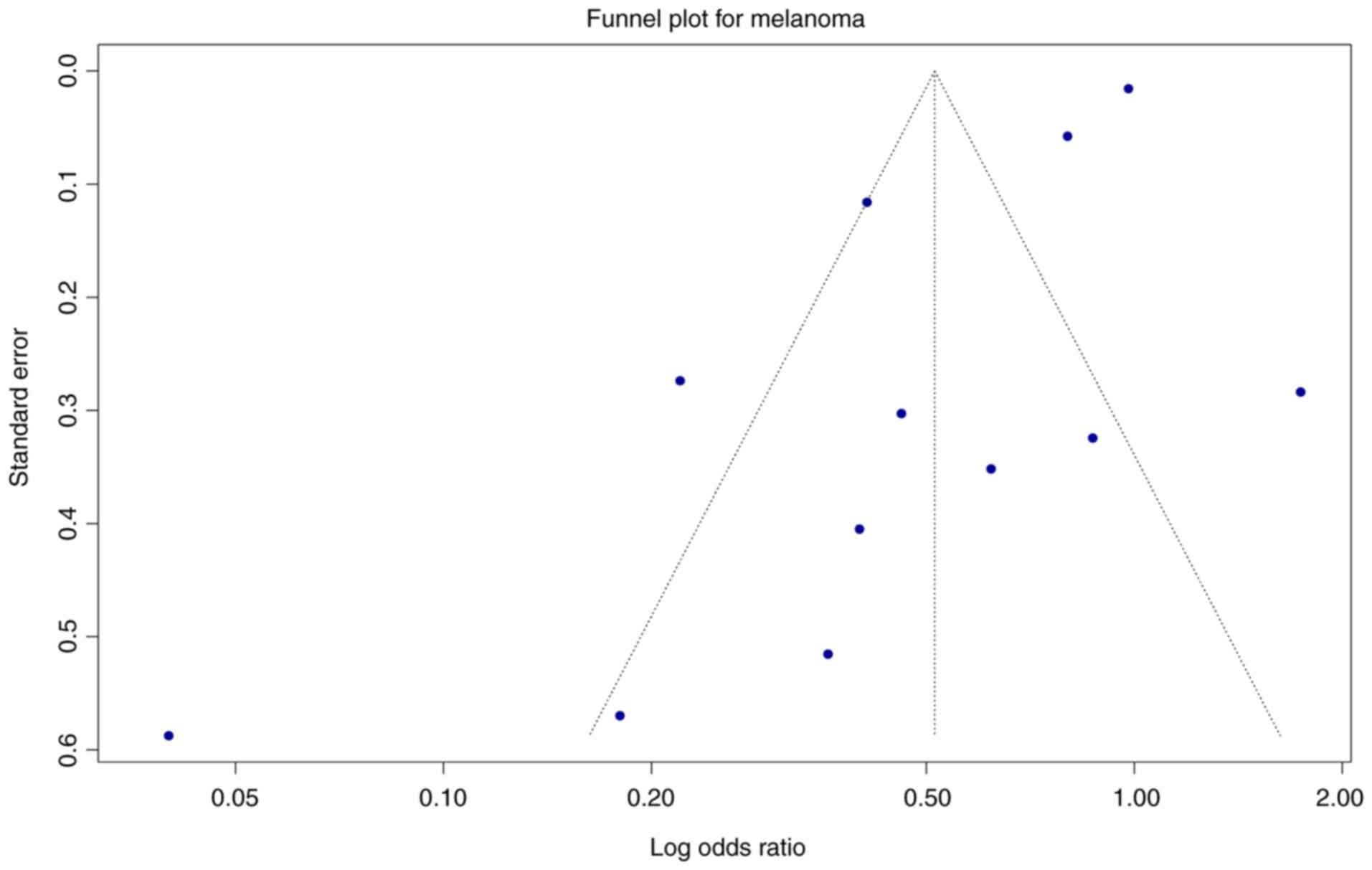
Publication bias
The visual inspection of the funnel plot suggested
some asymmetry, especially at the lower end among the smaller
studies (Fig. 10). Publication
bias was evaluated quantitatively using Egger's test for funnel
plot asymmetry. For melanoma studies, Egger's test indicated
significant evidence of funnel plot asymmetry, which can be
suggestive of publication bias, with a bias estimate of −2.94
(SE=0.89), suggesting potential small-study effects (59,60).
For BCC and SCC, publication bias could not be assessed due to the
small number of included studies (n=4 studies for BCC, n=3 studies
for SCC); this limitation reflects the methodological constraints
that require a minimum of 10 studies to produce reliable results
(59,60).
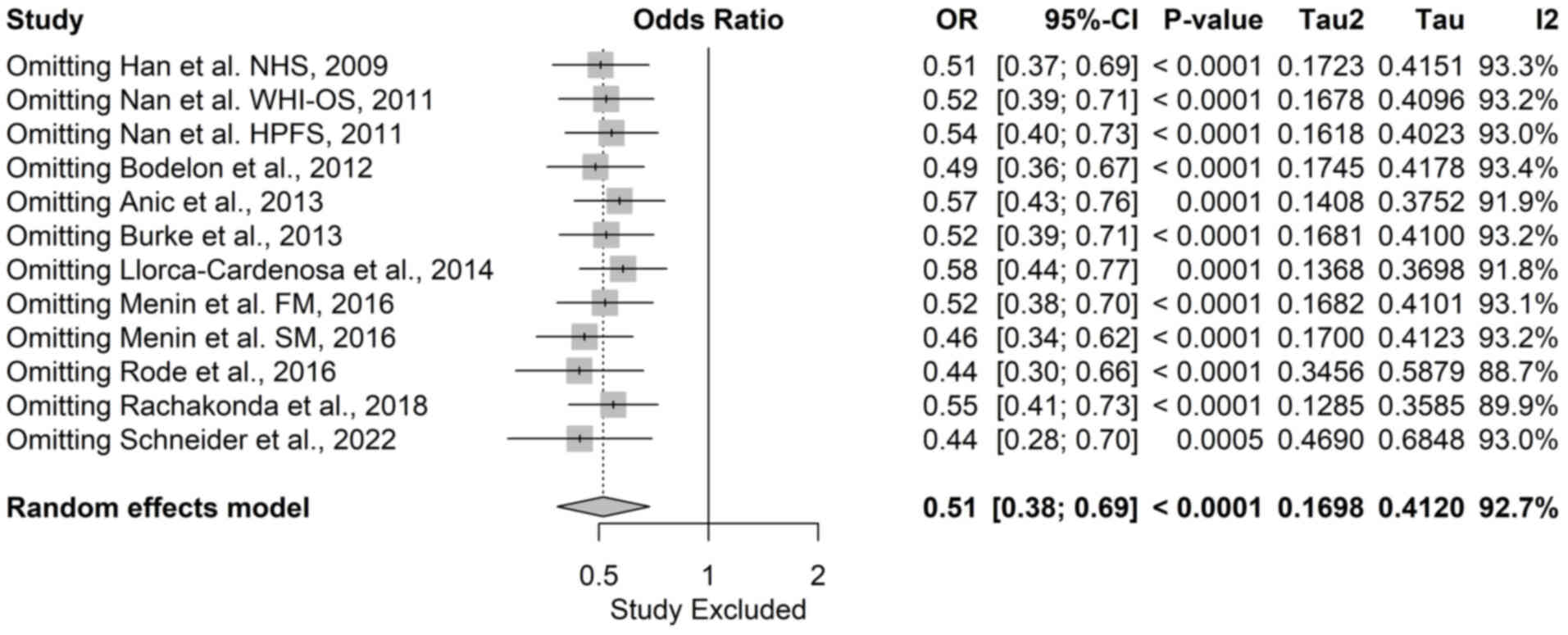
Sensitivity analysis
A sensitivity analysis was conducted to evaluate the
robustness of the meta-analysis by systematically omitting each
study and recalculating the pooled effect size and heterogeneity
measures.
In melanoma, the pooled OR ranged from 0.44 (95% CI:
0.28–0.70) to 0.58 (95% CI: 0.44–0.77), indicating that no single
study disproportionately influenced the overall findings (Fig. 11). The sensitivity analysis
confirmed the stability of the meta-analysis, with the association
between shorter TL and reduced melanoma risk remaining
statistically significant under all scenarios.
For BCC, the sensitivity analysis showed a wide
range of pooled ORs, from 1.55 (95% CI: 0.52–4.57) to 3.46 (95% CI:
1.13–10.58) (Fig. S1). In the case
of SCC, the pooled OR ranged from 0.94 (95% CI: 0.60–1.49) to 5.17
(95% CI: 0.24–111.31) (Fig. S2).
The results for BCC and SCC reflected the substantial variability
and suggested that the findings may not be robust.
Quality assessment
Quality assessment using the NOS showcased a
predominance of high-quality studies. All studies included in the
meta-analysis were high quality, demonstrating robust
methodologies. Among the studies included only in the qualitative
analysis, most were categorized as of moderate quality (Table SI, Table SII, Table SIII).
Discussion
The present meta-analysis revealed a significant
association between longer TL and increased melanoma risk, whereas
the associations for BCC and SCC, did not reach statistical
significance. Nonetheless, a trend towards increased risk being
linked with shorter telomeres was observed in the qualitative
synthesis for BCC and SCC.
The association between longer TL and melanoma risk
demonstrated in the current meta-analysis may appear
counterintuitive, as telomere shortening is generally associated
with genomic instability and increased cancer risk (28,33,78,79).
Telomere biology exhibits a complex role in oncogenesis; while
short telomeres can promote chromosomal instability and
tumourigenesis, they may also inhibit tumour progression by
enforcing replicative limits (40,80).
The present findings align with those of a previous meta-analysis
in melanoma by Caini et al (2015) (49), and similar associations have been
noted in other types of cancer (49–51).
Further exploration of the underlying biological mechanisms is
warranted.
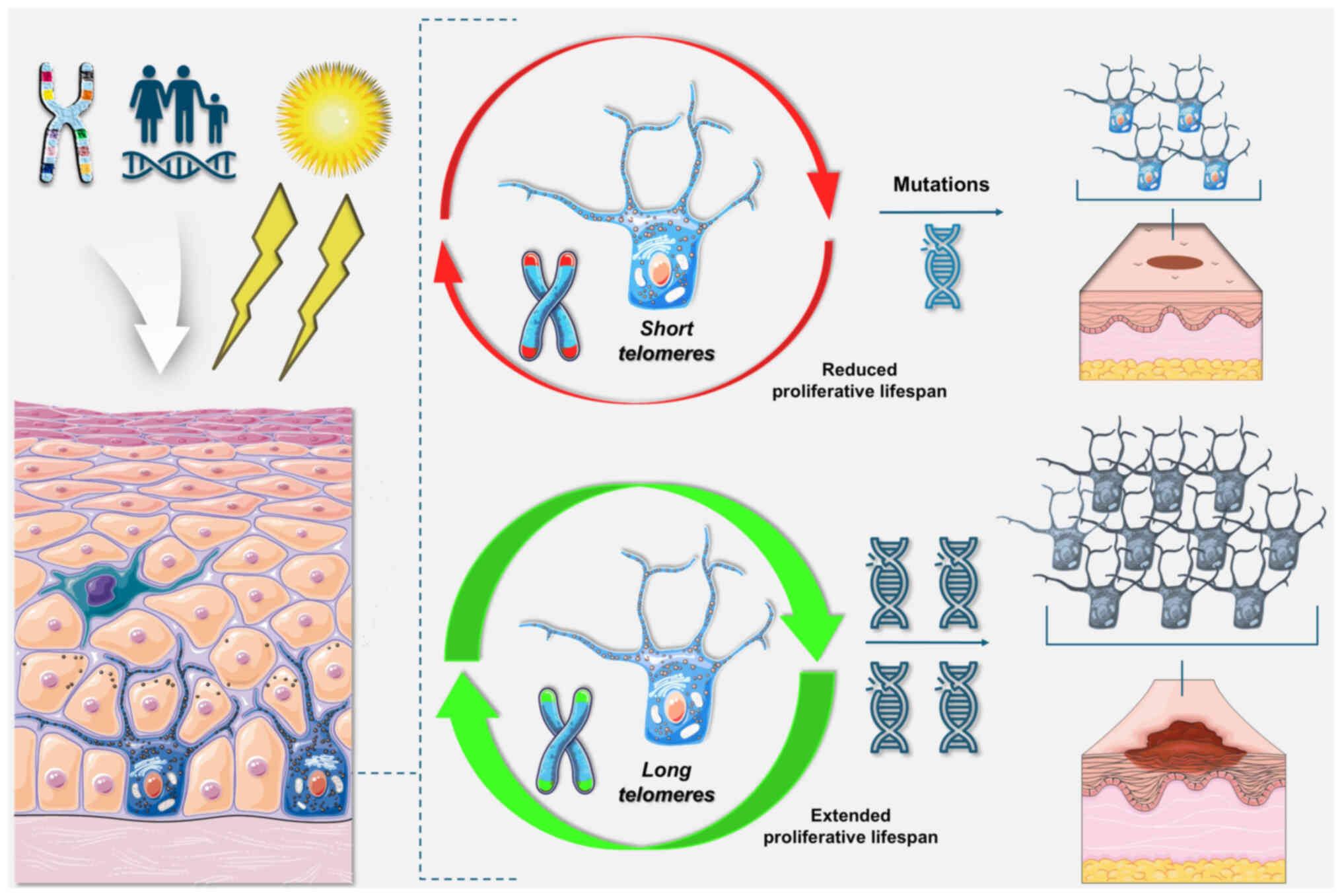
Melanocytes are characterised by low proliferative
rates and limited apoptotic capacity, and they may be prone to
senescence in response to oncogenic stress rather than apoptosis
(62,63,81).
Longer telomeres might extend the proliferative lifespan of
melanocytes harbouring oncogenic mutations, thereby increasing the
likelihood of accumulating additional genetic alterations that
could precipitate malignant transformation (Fig. 12) (19,62,63).
While an association has been demonstrated between increased TL and
total number of nevi, there is evidence that longer TL is
associated with increased melanoma risk independently of nevus
count, as the protective role of shorter telomeres persists even
after adjusting for nevus count and other risk factors (22,62,63,82).
Genetic contributions to telomere dynamics also
serve a crucial role in melanoma susceptibility, with genetic loci
regulating TL implicated in melanoma pathogenesis (83–85).
Evidence has suggested that telomere elongation appears to be the
mechanism linking telomerase reverse transcriptase (TERT) promoter
and shelterin mutations to cancer, rather than telomere
deprotection (86). Carriers of
TERT promoter and protection of telomeres 1 (POT1) mutations
exhibit longer telomeres compared with unaffected relatives, and
families with POT1 and TPP1 mutations demonstrate genetic
anticipation for both cancer onset and mortality, suggesting
successive telomere elongation across generations (67,86,87).
The association between long telomere-associated single nucleotide
polymorphisms and increased cancer risk has been observed in
multiple types of cancer, including melanoma, glioma and chronic
lymphocytic leukaemia (50,86,88,89).
Concurrently, short telomeres have been associated with poorer
survival outcomes in patients with melanoma (85,90). A
potential explanation for this is that longer telomeres confer an
increased melanoma risk; however, once the cancer has developed,
shorter telomeres may lead to increased genomic instability, thus
contributing to worse survival outcomes (85,90).
It has been suggested that the mechanism of
interaction between telomere dynamics and melanoma risk may vary
between sporadic and familial melanoma (71). Menin et al (2016) (71) demonstrated the association between
increased familial melanoma risk and longer telomeres, concurring
with evidence in familial melanoma from another study (72); however, Menin et al (71) also reported an inverse relationship
in sporadic melanoma, with shorter TL being associated with
increased risk. Studies have observed a similar phenomenon in other
types of cancer, including breast and ovarian cancers, where short
telomeres are linked to increased risk in familial but not in
sporadic cancer (91,92).
In the subgroup analysis of exclusively familial
melanoma and melanoma in the general population, the test for
subgroup differences was not significant. In both subgroups, there
was a significant inverse relation between TL and melanoma risk,
and the difference in magnitude of the effect did not reach
significance. The exact distribution of familial cases in each
general population study was not available; however, familial
melanoma constitutes 5–10% of melanoma cases (93,94).
To further examine the validity of the present findings, an
analysis was performed assuming 10% familial melanoma cases in the
general population and concluded that familial cases alone cannot
account for the observed overall association. The analysis showed
that familial cases alone could not account for the overall
association as the expected overall OR would have been 0.92 not the
observed 0.51 (95% CI: 0.38–0.68). Therefore, the present study
indicated that there may be no significant difference in the
association of TL and melanoma risk between sporadic and familial
melanoma cases. Nevertheless, this analysis is speculative in
nature and further large cohort studies that explicitly delineate
between familial and sporadic melanoma are imperative to validate
the results.
The subgroup analysis based on geographic location
revealed significant differences in the magnitude of the
association between TL and melanoma risk, with studies conducted in
the USA showing a stronger inverse association between TL and
melanoma risk (test for subgroup difference P=0.0175). In both
groups the subjects were primarily of European or Caucasian
descent, so while ethnic differences in TL have been documented,
they may not account for the findings (95). Environmental factors may serve a
role, particularly UV radiation exposure, the intensity of which
varies geographically, and has been documented to impact telomere
dynamics and serve a crucial role in melanoma development (21,96–98).
Methodological differences among studies, including study design
and adjustment for confounders, might also explain part of the
variation. Standardization of methodologies is essential to reduce
heterogeneity and enable more accurate comparisons across regions,
as well as the inclusion of environmental exposure biomarkers.
It has been suggested that telomere dynamics may
differ between the sexes, with women having longer telomeres
compared with men (48,99); a potential mechanism for this is the
potential protective role oestrogen may serve, as it can stimulate
telomerase activity through the oestrogen-responsive element
present in the human TERT gene (100). In a meta-analysis of the
association of colorectal cancer risk and TL, a shift in effect
estimates was observed in female patients (48). However, the present subgroup
analysis revealed no statistically significant difference in the
association between TL and melanoma risk between female-only and
mixed-sex studies (test for subgroup differences P=0.833). The
similar OR suggested that the reduced risk of melanoma associated
with shorter TL is consistent across the sexes, although due to the
limited number of male-only studies further research with
sex-stratified analyses is warranted to confirm this
observation.
Subgroup analysis based on the source of cases
revealed significant associations in both hospital-based studies
and population-based studies. The test for subgroup differences was
not significant (P=0.0658), suggesting that the source of cases may
not substantially influence the overall findings. The consistent
findings across sample populations indicate the robustness in the
association between longer TL and melanoma risk. To explore
potential sources of heterogeneity and to assess the potential
effect of confounding factors on the robustness of the results, a
subgroup analysis was performed on the basis of adjustments for
melanoma-specific confounding factors. All studies included in the
analysis provided risk estimates adjusted for age, one of the most
critical factors affecting TL; however, a minority adjusted for
melanoma-specific risk factors (such as number of nevi and UV
exposure) (22,31). In the subgroup analysis, the test
for the adjustment stratified subgroups found no significant
difference (P=0.151), indicating the relationship between melanoma
risk and longer telomeres is true and not a confounding artefact.
Due to the limited number of melanoma-specific adjusted studies,
future research should prioritize collecting comprehensive data on
both general and melanoma-specific confounders, enhancing the
validity of future findings.
To enable the clinical translation of TL as a skin
cancer biomarker, it is recommended that future research implements
a multicentre validation framework across geographically and
ethnically diverse cohorts. Prospective studies should standardize
TL measurement methods and integrate additional biomarkers, such as
UV exposure biomarkers, and genomic profiling to refine risk
stratification. Measurable clinical endpoints should be
prospectively collected to establish the predictive validity of TL.
These studies may facilitate the development of comprehensive risk
models and the translation of TL measurements into actionable
clinical screening and preventative strategies.
In the meta-analysis for associations between TL and
BCC risk, and TL and SCC risk, the results did not reach
statistical significance and high heterogeneity was observed. Among
studies included only in qualitative synthesis, significantly
shorter telomeres were detected in SCC tissues compared with in
normal skin, whereas the results were mixed in BCC. Given the
non-significant quantitative results, caution is warranted in
interpreting these findings.
The different associations between TL and skin
cancer types may be attributed to the unique proliferative and
apoptotic characteristics of melanocytes, basal cells and squamous
keratinocytes. Squamous keratinocytes exhibit a high apoptotic
threshold and primarily respond to DNA damage by programmed cell
death, especially in response to UV-induced genotoxic stress
(66,101). Basal cells have a lower senescence
rate and reduced apoptotic susceptibility compared with melanocytes
(102). These characteristics,
combined with the high proliferative demand, may predispose skin
cells with shorter telomeres to genomic instability under UV
exposure, increasing the risk of malignancy (62,66,102).
Conventionally, telomere crisis results in genomic aberrations
leading to cancer; however, the specific mechanisms in NMSC remain
unclear, the absence of a significant association between TL and
telomerase activity suggesting that telomerase-independent
mechanisms may serve a role (35,66,101).
Moreover, it has been observed that SCC and BCC exhibit
significantly shorter TL compared with BD and AK (101,103). Yamada-Hishida et al (2018)
(103) suggested that TL may be
associated with the malignant potential of NMSCs, with shorter
telomeres in SCC and BCC being associated with higher invasive and
metastatic risks, positioning TL as a valuable parameter in
understanding the biological behaviour of NMSCs (101).
The lack of significant associations for NMSCs in
the present meta-analysis may be attributed to the limited number
of studies and the substantial heterogeneity observed. Large-scale
studies are needed to clarify the relationship between TL and the
risk of BCC and SCC, and to ascertain if TL could potentially serve
as a biomarker for risk stratification.
Significant heterogeneity was observed in the
present meta-analyses, which may stem from numerous factors,
including differences in study design, population characteristics
and adjustments for confounding variables (104,105). Although subgroup and sensitivity
analyses were conducted to explore the sources of heterogeneity,
residual heterogeneity remained. A potential contributor to
heterogeneity may be the differences in melanoma genomic subtype,
unfortunately due to the paucity of data, subgroup analysis on the
basis of genomic subtypes was not possible. To address the issue of
heterogeneity, future research should aim to standardize
methodologies, including genomic subtypes, and to ensure
comprehensive adjustment for confounding variables.
Despite the homogeneity in TL measurement
methodology and DNA tissue source in the quantitative synthesis, a
potential limitation of the present systematic review is the
heterogeneity of methods used to measure TL among the qualitative
synthesis-only studies. In the quantitative study, qPCR methods
were universally employed to measure TL, but studies in the
qualitative synthesis used Southern blotting and TEL-FISH analysis,
which may vary in precision and sensitivity (106,107). Furthermore, while the quantitative
study exclusively used PBLs as the DNA source with independent
healthy controls, qualitative synthesis-only studies measured TL in
tumour tissue and utilised adjacent normal skin as the control
group. These methodological differences could contribute to
variability in TL estimates and may partly explain the discrepancy
between findings in the quantitative and qualitative synthesis for
SCC and BCC.
The present meta-analysis may also be limited by the
possibility of publication bias. The results of the Egger's test of
melanoma studies suggested funnel plot asymmetry, which can be
suggestive of publication bias (59,60).
Publication bias may lead to inflation of the estimated effect size
in meta-analyses, indicating caution in interpreting the magnitude
of the association between TL and melanoma risk (60). However, the reliability of the
Egger's test in this context is limited, given the substantial
variability in sample sizes, which can inflate the type I error
rate. Furthermore, the current analysis included large-scale cohort
studies and studies reporting non-significant associations,
suggesting that studies with null results were not systematically
excluded (60,108). The visual inspection of the funnel
plot revealed moderate asymmetry. For BCC and SCC, the small number
of included studies (n=4 for BCC, n=3 for SCC) did not allow for
formal assessments of publication bias (60). Caution is recommended in
interpreting the magnitude of the association as publication bias
cannot be entirely ruled out.
Quality assessment using the NOS revealed that
almost all studies included in the meta-analysis were of high
quality, underscoring the reliability of the present meta-analysis.
However, among the qualitative-only studies, most were categorized
as of moderate quality. One other potential limitation could be the
differences in parametrization of TL, while the majority reported
the risk estimates based on quartiles, some studies reported
tertiles or continuous measurements. Unfortunately, the studies did
not provide sufficient data to recalculate ORs and homogenize TL
parametrization, which may contribute to heterogeneity. The present
findings may also have limited applicability in diverse ethnic
groups, as most studies were conducted in Western countries and had
primarily Caucasian patient populations. The lack of diversity
highlights the need for further studies with populations from
different ethnic backgrounds.
Adjustments for confounding variables also varied
among studies. All studies included in the analysis provided risk
estimates adjusted for age; however, a minority adjusted for
melanoma-specific risk factors. In subgroup analysis, the test for
subgroup differences was non-significant (P=0.151), indicating that
adjustment for confounders does not influence the observed
associations. Nevertheless, due to the limited number of
melanoma-specific adjusted studies, future research should
prioritize collecting comprehensive data on both general and
melanoma-specific confounders, enhancing the validity of future
findings.
In conclusion, the findings of the present study
suggested a significant association between long TL and increased
melanoma risk, challenging the conventional view of an association
between telomere shortening and increased cancer risk, and
highlighting the complex role of telomere dynamics in
carcinogenesis. In melanoma, the robustness of the present findings
was indicated by their persistence when adjusting for confounding
factors and examining different populations. Furthermore, the
association was consistent across the sexes and in familial
melanoma. By contrast, the associations between TL and the risks of
BCC and SCC were not statistically significant in the quantitative
analyses. Qualitative synthesis reported non-significant results in
BCC and shorter telomeres in SCC tissues compared with in healthy
skin. Further research is imperative to clarify the role of
telomere dynamics in BCC and SCC, and to explore the mechanisms
underlying the association in melanoma. Future large-scale
prospective cohort studies with standardized methodology are
essential to validate these findings and to ascertain the utility
of TL as a clinically significant skin cancer biomarker.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are
included in the figures and/or tables of this article.
Authors' contributions
DAA conceptualized the study. Both DAA and DAS
developed the methodology. The investigation was conducted by DAA
and DAS. Validation of the data and findings was carried out by
both authors. DAA prepared the original draft of the manuscript,
while both DAA and DAS contributed to the review and editing
process. DAS supervised the overall project. DAA and DAS confirm
the authenticity of all the raw data. Both authors have read and
approved the final manuscript.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
DAS is the Editor-in-Chief for the journal, but had
no personal involvement in the reviewing process, or any influence
in terms of adjudicating on the final decision, for this article.
The other authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the proofreading stage, artificial
intelligence-powered tools were used exclusively to improve the
readability and language of the manuscript, and subsequently, the
authors revised and edited the content produced as necessary,
taking full responsibility for the ultimate content of the present
manuscript.
References
|
1
|
Apalla Z, Nashan D, Weller RB and
Castellsagué X: Skin cancer: Epidemiology, disease burden,
pathophysiology, diagnosis, and therapeutic approaches. Dermatol
Ther (Heidelb). 7 (Suppl 1):S5–S19. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lomas A, Leonardi-Bee J and Bath-Hextall
F: A systematic review of worldwide incidence of nonmelanoma skin
cancer. Br J Dermatol. 166:1069–1080. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Smith H, Wernham A and Patel A: When to
suspect a non-melanoma skin cancer. BMJ. 368:m6922020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Grabowski J, Saltzstein SL, Sadler GR,
Tahir Z and Blair S: A Comparison of merkel cell carcinoma and
melanoma: Results from the California cancer registry. Clin Med
Oncol. 2:327–333. 2008.PubMed/NCBI
|
|
5
|
Yanofsky VR, Mercer SE and Phelps RG:
Histopathological variants of cutaneous squamous cell carcinoma: A
review. J Skin Cancer. 2011:2108132011. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Wong CSM: Basal cell carcinoma. BMJ.
327:794–798. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Peterson SC, Eberl M, Vagnozzi AN, Belkadi
A, Veniaminova NA, Verhaegen ME, Bichakjian CK, Ward NL, Dlugosz AA
and Wong SY: Basal cell carcinoma preferentially arises from stem
cells within hair follicle and mechanosensory niches. Cell Stem
Cell. 16:400–412. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kim RH and Armstrong AW: Nonmelanoma skin
cancer. Dermatol Clin. 30:125–139. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Motley R, Kersey P and Lawrence C; British
Association of Dermatologists; British Association of Plastic
Surgeons; Royal College of Radiologists, Faculty of Clinical
Oncology, : Multiprofessional guidelines for the management of the
patient with primary cutaneous squamous cell carcinoma. Br J
Dermatol. 146:18–25. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Preston DS and Stern RS: Nonmelanoma
cancers of the Skin. N Engl J Med. 327:1649–1662. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Miller DL and Weinstock MA: Nonmelanoma
skin cancer in the United States: Incidence. J Am Acad Dermatol.
30:774–778. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Gloster HM and Brodland DG: The
epidemiology of skin cancer. Dermatol Surg. 22:217–326. 1996.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Revenga Arranz F, Paricio Rubio J, Mar
Vázquez Salvado M and Del Villar Sordo V: Descriptive epidemiology
of basal cell carcinoma and cutaneous squamous cell carcinoma in
Soria (north-eastern Spain) 1998–2000: A hospital-based survey. J
Eur Acad Dermatol Venereol. 18:137–141. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
De Vries E, Trakatelli M, Kalabalikis D,
Ferrandiz L, Ruiz-de-Casas A, Moreno-Ramirez D, Sotiriadis D,
Ioannides D, Aquilina S, Apap C, et al: Known and potential new
risk factors for skin cancer in European populations: A multicentre
case-control study: Risk factors for skin cancer in European
populations. Br J Dermatol. 167 (Suppl 2):S1–S13. 2012. View Article : Google Scholar
|
|
15
|
Fargnoli MC, Piccioni A, Neri L, Tambone
S, Pellegrini C and Peris K: Long-term efficacy and safety of
daylight photodynamic therapy with methyl amninolevulinate for
actinic keratosis of the face and scalp. Eur J Dermatol. 27:89–91.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Alam M and Ratner D: Cutaneous
Squamous-cell carcinoma. N Engl J Med. 344:975–983. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Braeuer RR, Watson IR, Wu C, Mobley AK,
Kamiya T, Shoshan E and Bar-Eli M: Why is melanoma so metastatic?
Pigment Cell Melanoma Res. 27:19–36. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Cust AE, Armstrong BK, Goumas C, Jenkins
MA, Schmid H, Hopper JL, Kefford RF, Giles GG, Aitken JF and Mann
GJ: Sunbed use during adolescence and early adulthood is associated
with increased risk of early-onset melanoma. Int J Cancer.
128:2425–2435. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Arnold M, De Vries E, Whiteman DC, Jemal
A, Bray F, Parkin DM and Soerjomataram I: Global burden of
cutaneous melanoma attributable to ultraviolet radiation in 2012.
Int J Cancer. 143:1305–1314. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Elder DE, Bastian BC, Cree IA, Massi D and
Scolyer RA: The 2018 World Health Organization classification of
cutaneous, mucosal, and uveal melanoma: Detailed analysis of 9
distinct subtypes defined by their evolutionary pathway. Arch
Pathol Lab Med. 144:500–522. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gandini S, Sera F, Cattaruzza MS, Pasquini
P, Picconi O, Boyle P and Melchi CF: Meta-analysis of risk factors
for cutaneous melanoma: II. Sun exposure. Eur J Cancer. 41:45–60.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Rastrelli M, Tropea S, Rossi CR and
Alaibac M: Melanoma: Epidemiology, risk factors, pathogenesis,
diagnosis and classification. In Vivo. 28:1005–1011.
2014.PubMed/NCBI
|
|
23
|
Ferlay J, Soerjomataram I, Dikshit R, Eser
S, Mathers C, Rebelo M, Parkin DM, Forman D and Bray F: Cancer
incidence and mortality worldwide: Sources, methods and major
patterns in GLOBOCAN 2012. Int J Cancer. 136:E359–E86. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Chang C, Murzaku EC, Penn L, Abbasi NR,
Davis PD, Berwick M and Polsky D: More skin, more sun, more tan,
more melanoma. Am J Public Health. 104:e92–e99. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Leonardi GC, Falzone L, Salemi R, Zanghï
A, Spandidos DA, Mccubrey JA, Candido S and Libra M: Cutaneous
melanoma: From pathogenesis to therapy (Review). Int J Oncol.
52:1071–1080. 2018.PubMed/NCBI
|
|
26
|
Blackburn EH, Epel ES and Lin J: Human
telomere biology: A contributory and interactive factor in aging,
disease risks, and protection. Science. 350:1193–1198. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Moon IK and Jarstfer MB: The human
telomere and its relationship to human disease, therapy, and tissue
engineering. Front Biosci J Virtual Libr. 12:4595–4620. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
O'Sullivan RJ and Karlseder J: Telomeres:
Protecting chromosomes against genome instability. Nat Rev Mol Cell
Biol. 11:171–1781. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
De Lange T: How telomeres solve the
End-protection problem. Science. 326:948–952. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Monaghan P and Haussmann MF: Do telomere
dynamics link lifestyle and lifespan? Trends Ecol Evol. 21:47–53.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Shay JW and Wright WE: Hayflick, his
limit, and cellular ageing. Nat Rev Mol Cell Biol. 1:72–76. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Shay JW and Wright WE: Role of telomeres
and telomerase in cancer. Semin Cancer Biol. 21:349–353. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Artandi SE and DePinho RA: Telomeres and
telomerase in cancer. Carcinogenesis. 31:9–18. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Shay JW and Bacchetti S: A survey of
telomerase activity in human cancer. Eur J Cancer. 33:787–791.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Maciejowski J and de Lange T: Telomeres in
cancer: Tumour suppression and genome instability. Nat Rev Mol Cell
Biol. 18:175–186. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Robinson NJ and Schiemann WP: Telomerase
in cancer: Function, regulation, and clinical translation. Cancers.
14:8082022. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Xu Y and Goldkorn A: Telomere and
telomerase therapeutics in cancer. Genes. 7:222016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Dratwa M, Wysoczańska B, Łacina P, Kubik T
and Bogunia-Kubik K: TERT-Regulation and roles in cancer formation.
Front Immunol. 11:5899292020. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Tsatsakis A, Oikonomopoulou T,
Nikolouzakis TK, Vakonaki E, Tzatzarakis M, Flamourakis M, Renieri
E, Fragkiadaki P, Iliaki E, Bachlitzanaki M, et al: Role of
telomere length in human carcinogenesis (Review). Int J Oncol.
63:782023. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
López-Otín C, Pietrocola F, Roiz-Valle D,
Galluzzi L and Kroemer G: Meta-hallmarks of aging and cancer. Cell
Metab. 35:12–35. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Hanahan D and Weinberg RA: Hallmarks of
cancer: The next generation. Cell. 144:646–674. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Okamoto K and Seimiya H: Revisiting
telomere shortening in cancer. Cells. 8:1072019. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Andreikos D, Kyrodimos E, Kotsinas A,
Chrysovergis A and Papacharalampous GX: The Association between
telomere length and head and neck cancer risk: A systematic review
and Meta-analysis. Int J Mol Sci. 25:90002024. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Karimi B, Yunesian M, Nabizadeh R,
Mehdipour P and Aghaie A: Is leukocyte telomere length related with
lung cancer risk?: A Meta-Analysis. Iran Biomed J. 21:142–153.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Ma H, Zhou Z, Wei S, Liu Z, Pooley KA,
Dunning AM, Svenson U, Roos G, Hosgood HD III, Shen M and Wei Q:
Shortened telomere length is associated with increased risk of
cancer: A meta-analysis. PLoS One. 6:e204662011. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Zhu X, Han W, Xue W, Zou Y, Xie C, Du J
and Jin G: The association between telomere length and cancer risk
in population studies. Sci Rep. 6:222432016. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Benites-Zapata VA, Ulloque-Badaracco JR,
Alarcón-Braga EA, Fernández-Alonso AM, López-Baena MT and
Pérez-López FR: Telomerase activity and telomere length in women
with breast cancer or without malignancy: A systematic review and
meta-analysis. Maturitas. 180:1078822024. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Naing C, Aung K, Lai PK and Mak JW:
Association between telomere length and the risk of colorectal
cancer: A meta-analysis of observational studies. BMC Cancer.
17:242017. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Caini S, Raimondi S, Johansson H, De
Giorgi V, Zanna I, Palli D and Gandini S: Telomere length and the
risk of cutaneous melanoma and non-melanoma skin cancer: A review
of the literature and meta-analysis. J Dermatol Sci. 80:168–174.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Rode L, Nordestgaard BG and Bojesen SE:
Long telomeres and cancer risk among 95 568 individuals from the
general population. Int J Epidemiol. 45:1634–1643. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Fabiani R, Chiavarini M, Rosignoli P and
Giacchetta I: Leucocyte telomere length and lung cancer risk: A
systematic review and Meta-analysis of prospective studies. Cancers
(Basel). 16:32182024. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Chen S, Hu S, Zhou B, Cheng B, Tong H, Su
D, Li X, Chen Y and Zhang G: Telomere-related prognostic biomarkers
for survival assessments in pancreatic cancer. Sci Rep.
13:105862023. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Holesova Z, Krasnicanova L, Saade R, Pös
O, Budis J, Gazdarica J, Repiska V and Szemes T: Telomere length
changes in cancer: Insights on carcinogenesis and potential for
Non-invasive diagnostic strategies. Genes (Basel). 14:7152023.
View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Wentzensen IM, Mirabello L, Pfeiffer RM
and Savage SA: The association of telomere length and cancer: A
meta-analysis. Cancer Epidemiol Biomarkers Prev. 20:1238–1250.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Page MJ, McKenzie JE, Bossuyt PM, Boutron
I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan
SE, et al: The PRISMA 2020 statement: An updated guideline for
reporting systematic reviews. BMJ. 372:n712021. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Higgins JPT: Measuring inconsistency in
meta-analyses. BMJ. 327:557–560. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
57
|
Green S and Higgins JPT: Cochrane Handbook
for Systematic Reviews of Interventions. The Cochrane
Collaboration. http://training.cochrane.org/handbookMarch
20–2025
|
|
58
|
DerSimonian R and Laird N: Meta-analysis
in clinical trials. Control Clin Trials. 7:177–188. 1986.
View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Egger M, Smith GD, Schneider M and Minder
C: Bias in meta-analysis detected by a simple, graphical test. BMJ.
315:629–634. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Sterne JAC, Gavaghan D and Egger M:
Publication and related bias in meta-analysis. J Clin Epidemiol.
53:1119–1129. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Wells GA, Shea B, O'Connell D, Peterson J,
Welch V, Losos M and Tugwell P: The Newcastle-Ottawa Scale (NOS)
for Assessing the Quality of Nonrandomised Studies in
Meta-Analyses. 2013. http://www.ohri.ca/programs/clinical_epidemiology/oxford.aspMarch
20–2025
|
|
62
|
Han J, Qureshi AA, Prescott J, Guo Q, Ye
L, Hunter DJ and De Vivo I: A Prospective study of telomere length
and the risk of skin cancer. J Invest Dermatol. 129:415–421. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
63
|
Nan H, Du M, De Vivo I, Manson JE, Liu S,
McTiernan A, Curb JD, Lessin LS, Bonner MR, Guo Q, et al: Shorter
telomeres associate with a reduced risk of melanoma development.
Cancer Res. 71:6758–6763. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Weischer M: Short telomere length, cancer
survival, and cancer risk in 47102 individuals. J Natl Cancer Inst.
105:459–468. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Greenland S, Thomas DC and Morgenstern H:
The rare-disease assumption revisited. Am J Epidemiol. 124:869–876.
1986. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Anic GM, Sondak VK, Messina JL, Fenske NA,
Zager JS, Cherpelis BS, Lee JH, Fulp WJ, Epling-Burnette PK, Park
JY and Rollison DE: Telomere length and risk of melanoma, squamous
cell carcinoma, and basal cell carcinoma. Cancer Epidemiol.
37:434–439. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Rachakonda S, Kong H, Srinivas N,
Garcia-Casado Z, Requena C, Fallah M, Heidenreich B, Planelles D,
Traves V, Schadendorf D, et al: Telomere length, telomerase reverse
transcriptase promoter mutations, and melanoma risk. Genes
Chromosomes Cancer. 57:564–572. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Schneider CV, Schneider KM, Teumer A,
Rudolph KL, Hartmann D, Rader DJ and Strnad P: Association of
telomere length with risk of disease and mortality. JAMA Intern
Med. 182:291–300. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Bodelon C, Pfeiffer RM, Bollati V,
Debbache J, Calista D, Ghiorzo P, Fargnoli MC, Bianchi-Scarra G,
Peris K, Hoxha M, et al: On the interplay of telomeres, nevi and
the risk of melanoma. PLoS One. 7:e524662012. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Llorca-Cardeñosa MJ, Peña-Chilet M, Mayor
M, Gomez-Fernandez C, Casado B, Martin-Gonzalez M, Carretero G,
Lluch A, Martinez-Cadenas C, Ibarrola-Villava M and Ribas G: Long
telomere length and a TERT-CLPTM1 locus polymorphism association
with melanoma risk. Eur J Cancer. 50:3168–3177. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Menin C, Bojnik E, Del Bianco P, Elefanti
L, Gianesin K, Keppel S, Stagni C, Mocellin S, Vecchiato A and De
Rossi A: Differences in telomere length between sporadic and
familial cutaneous melanoma. Br J Dermatol. 175:937–943. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Burke LS, Hyland PL, Pfeiffer RM, Prescott
J, Wheeler W, Mirabello L, Savage SA, Burdette L, Yeager M, Chanock
S, et al: Telomere length and the risk of cutaneous malignant
melanoma in Melanoma-Prone families with and without CDKN2A
mutations. PLoS One. 8:e711212013. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Perrem K, Lynch A, Al Nooh F, Leader M and
Elaine Kay: The different telomere lengths in basal and squamous
cell carcinomas also differ between the nontransplant and renal
transplant population. Hum Pathol. 39:1034–1041. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Srinivas N, Rachakonda S, Hielscher T,
Calderazzo S, Rudnai P, Gurzau E, Koppova K, Fletcher T and Kumar
R: Telomere length, arsenic exposure and risk of basal cell
carcinoma of skin. Carcinogenesis. 40:715–723. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Liang G, Qureshi AA, Guo Q, De Vivo I and
Han J: No association between telomere length in peripheral blood
leukocytes and the risk of nonmelanoma skin cancer. Cancer
Epidemiol Biomarkers Prev. 20:1043–1045. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Wainwright LJ, Rees JL and Middleton PG:
Changes in mean telomere length in basal cell carcinomas of the
skin. Genes Chromosomes Cancer. 12:45–49. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Perrem K, Lynch A, Conneely M, Wahlberg H,
Murphy G, Leader M and Kay E: The higher incidence of squamous cell
carcinoma in renal transplant recipients is associated with
increased telomere lengths. Hum Pathol. 38:351–358. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
78
|
De Vitis M, Berardinelli F and Sgura A:
Telomere length maintenance in cancer: At the crossroad between
telomerase and alternative lengthening of telomeres (ALT). Int J
Mol Sci. 19:6062018. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Andreikos D, Spandidos D and
Georgakopoulou V: Telomeres and telomerase in mesothelioma:
Pathophysiology, biomarkers and emerging therapeutic strategies
(Review). Int J Oncol. 66:232025. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Mooi WJ and Peeper DS: Oncogene-induced
cell Senescence-halting on the road to cancer. N Engl J Med.
355:1037–1046. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Gray-Schopfer VC, Cheong SC, Chong H, Chow
J, Moss T, Abdel-Malek ZA, Marais R, Wynford-Thomas D and Bennett
DC: Cellular senescence in naevi and immortalisation in melanoma: A
role for p16? Br J Cancer. 95:496–505. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
82
|
Bataille V, Kato BS, Falchi M, Gardner J,
Kimura M, Lens M, Perks U, Valdes AM, Bennett DC, Aviv A and
Spector TD: Nevus size and number are associated with telomere
length and represent potential markers of a decreased senescence in
vivo. Cancer Epidemiol Biomarkers Prev. 16:1499–1502. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
83
|
Robles-Espinoza CD, Velasco-Herrera M del
C, Hayward NK and Adams DJ: Telomere-regulating genes and the
telomere interactome in familial cancers. Mol Cancer Res.
13:211–222. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Toussi A, Mans N, Welborn J and Kiuru M:
Germline mutations predisposing to melanoma. J Cutan Pathol.
47:606–616. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Son N, Cui Y and Xi W: Association between
telomere length and skin cancer and aging: A mendelian
randomization analysis. Front Genet. 13:9317852022. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
McNally EJ, Luncsford PJ and Armanios M:
Long telomeres and cancer risk: The price of cellular immortality.
J Clin Invest. 129:3474–3481. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Stanley SE and Armanios M: The short and
long telomere syndromes: Paired paradigms for molecular medicine.
Curr Opin Genet Dev. 33:1–9. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Barrett ELB, Burke TA, Hammers M, Komdeur
J and Richardson DS: Telomere length and dynamics predict mortality
in a wild longitudinal study. Mol Ecol. 22:249–259. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
89
|
Speedy HE, Di Bernardo MC, Sava GP, Dyer
MJS, Holroyd A, Wang Y, Sunter NJ, Mansouri L, Juliusson G, Smedby
KE, et al: A genome-wide association study identifies multiple
susceptibility loci for chronic lymphocytic leukemia. Nat Genet.
46:56–60. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Rachakonda S, Srinivas N, Mahmoudpour SH,
Garcia-Casado Z, Requena C, Traves V, Soriano V, Cardelli M,
Pjanova D, Molven A, et al: Telomere length and survival in primary
cutaneous melanoma patients. Sci Rep. 8:109472018. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Martinez-Delgado B, Yanowsky K,
Inglada-Perez L, De La Hoya M, Caldes T, Vega A, Blanco A, Martin
T, Gonzalez-Sarmiento R, Blasco M, et al: Shorter telomere length
is associated with increased ovarian cancer risk in both familial
and sporadic cases. J Med Genet. 49:341–344. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Martinez-Delgado B, Yanowsky K,
Inglada-Perez L, Domingo S, Urioste M, Osorio A and Benitez J:
Genetic anticipation is associated with telomere shortening in
hereditary breast cancer. PLoS Genet. 7:e10021822011. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Rossi M, Pellegrini C, Cardelli L,
Ciciarelli V, Di Nardo L and Fargnoli MC: Familial melanoma:
Diagnostic and management implications. Dermatol Pract Concept.
9:10–16. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Zocchi L, Lontano A, Merli M, Dika E,
Nagore E, Quaglino P, Puig S and Ribero S: Familial Melanoma and
susceptibility genes: A review of the most common clinical and
dermoscopic phenotypic aspect, associated malignancies and
practical tips for management. J Clin Med. 10:37602021. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Hansen MEB, Hunt SC, Stone RC, Horvath K,
Herbig U, Ranciaro A, Hirbo J, Beggs W, Reiner AP, Wilson JG, et
al: Shorter telomere length in Europeans than in Africans due to
polygenetic adaptation. Hum Mol Genet. 25:2324–2330. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
96
|
Chang YM, Barrett JH, Bishop DT, Armstrong
BK, Bataille V, Bergman W, Berwick M, Bracci PM, Elwood JM,
Ernstoff MS, et al: Sun exposure and melanoma risk at different
latitudes: A pooled analysis of 5700 cases and 7216 controls. Int J
Epidemiol. 38:814–830. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Armstrong BK and Kricker A: The
epidemiology of UV induced skin cancer. J Photochem Photobiol B.
63:8–18. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Lundsgaard NU, Cramp RL and Franklin CE:
Early exposure to UV radiation causes telomere shortening and
poorer condition later in life. J Exp Biol. 225:jeb2439242022.
View Article : Google Scholar : PubMed/NCBI
|
|
99
|
Gardner M, Bann D, Wiley L, Cooper R,
Hardy R, Nitsch D, Martin-Ruiz C, Shiels P, Sayer AA, Barbieri M,
et al: Gender and telomere length: Systematic review and
meta-analysis. Exp Gerontol. 51:15–27. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Kyo S, Takakura M, Kanaya T, Zhuo W,
Fujimoto K, Nishio Y, Orimo A and Inoue M: Estrogen activates
telomerase. Cancer Res. 59:5917–5921. 1999.PubMed/NCBI
|
|
101
|
Ventura A, Pellegrini C, Cardelli L, Rocco
T, Ciciarelli V, Peris K and Fargnoli MC: Telomeres and telomerase
in cutaneous squamous cell carcinoma. Int J Mol Sci. 20:13332019.
View Article : Google Scholar : PubMed/NCBI
|
|
102
|
Gilchrest BA, Eller MS, Geller AC and Yaar
M: The pathogenesis of melanoma induced by ultraviolet radiation. N
Engl J Med. 340:1341–1348. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
103
|
Yamada-Hishida H, Nobeyama Y and Nakagawa
H: Correlation of telomere length to malignancy potential in
non-melanoma skin cancers. Oncol Lett. 15:393–399. 2018.PubMed/NCBI
|
|
104
|
Grimes DA and Schulz KF: Bias and causal
associations in observational research. Lancet. 359:248–252. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
105
|
Glasziou PP and Sanders SL: Investigating
causes of heterogeneity in systematic reviews. Stat Med.
21:1503–1511. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
106
|
Montpetit AJ, Alhareeri AA, Montpetit M,
Starkweather AR, Elmore LW, Filler K, Mohanraj L, Burton CW,
Menzies VS, Lyon DE and Jackson-Cook CK: Telomere length: A review
of methods for measurement. Nurs Res. 63:289–299. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
107
|
Gutierrez-Rodrigues F, Santana-Lemos BA,
Scheucher PS, Alves-Paiva RM and Calado RT: Direct comparison of
Flow-FISH and qPCR as diagnostic tests for telomere length
measurement in humans. PLoS One. 9:e1137472014. View Article : Google Scholar : PubMed/NCBI
|
|
108
|
Lin L: Bias caused by sampling error in
meta-analysis with small sample sizes. PLoS One. 13:e02040562018.
View Article : Google Scholar : PubMed/NCBI
|