Introduction
Granular cell tumors (GCTs) account for only 0.5% of
soft tissue tumors and can manifest in various tissues and organs
within the body (1). Among them,
the skin and the head-neck region are the most prevalent sites
(2). Among all GCTs, 2–6% occur in
the respiratory system, with the majority occurring in the larynx,
while primary bronchial GCTs (BGCTs) are exceptionally rare
(1,3). Both domestic and international reports
of BGCTs are limited, with most being isolated case reports. The
clinical manifestations and imaging features of BGCTs lack
specificity, making misdiagnosis and missed diagnosis common
(4). Given that BGCTs typically
exhibit benign behavior, an accurate preoperative diagnosis is
crucial to avoid overtreatment.
The present study reports the case of a 36-year-old
male patient who was admitted for the investigation of a ‘thyroid
mass’, whereupon a BGCT was incidentally discovered. The objective
of the present study was to explore the clinical and pathological
features of GCTs in this uncommon location, contributing to a more
refined diagnostic understanding of these lesions.
Case report
Case presentation
A 36-year-old male patient was admitted to Cangzhou
Fifth Hospital (People's Hospital of Qingxian), Cangzhou, China on
August 5, 2023 due to the discovery of a neck mass 3 months prior.
The patient incidentally noticed the neck mass without associated
pain, fever, cough, dyspnea, palpitations, diaphoresis or prior
treatment. As the mass had gradually increased in size,
necessitating surgical intervention, the patient was admitted
following an outpatient evaluation, during which a provisional
diagnosis of a ‘thyroid mass’ was made. The patient had no history
of viral hepatitis, tuberculosis, prior surgeries, blood
transfusions, drug or food allergies and smoking or alcohol
consumption.
On admission, the patient's vital signs were stable
with a temperature of 35.8°C, pulse rate of 84 beats per min,
respiratory rate of 18 breaths per min and blood pressure of 150/90
mmHg. The superficial lymph nodes were not palpably enlarged, and
examination of the head and face revealed no abnormalities. The
cardiorespiratory and abdominal examinations were also
unremarkable. In addition, there were no jugular vein distension or
abnormal pulsations in the neck. Palpation of the right side of the
neck revealed a localized lump, measuring ~3.5×3 cm, with no
tenderness, a firm consistency, smooth surface, limited mobility
and slight movement upon swallowing. The initial diagnosis upon
admission was pending confirmation of the nature of the thyroid
mass.
Upon further investigation post-admission, the
laboratory test results showed a white blood cell count of
4.73×109/l (normal range, 4.0–10.0×109/l), a
neutrophil percentage of 59.5% (normal range, 50–70%), a hemoglobin
level of 159 g/l (normal range, 110–160 g/l) and a platelet count
of 100×109/l (normal range, 100–300×109/l).
C-reactive protein was elevated at 68.94 mg/l (normal range, 0–10
mg/l), while the other tumor markers [CEA, neuron-specific enolase,
cytokeratin fragment-19, cancer antigen (CA)125 and CA199] were
within the normal limits. The thyroid function tests revealed a
slightly elevated serum thyroid-stimulating hormone level of 5.781
mIU/l (normal range, 0.5–5.1). Thyroid antibody testing
demonstrated normal values. Electrolytes, blood glucose and
glycosylated hemoglobin were all within the normal ranges. The
patient tested negative for hepatitis B and showed no evidence of
syphilis or HIV antibodies. The urinalysis was unremarkable.
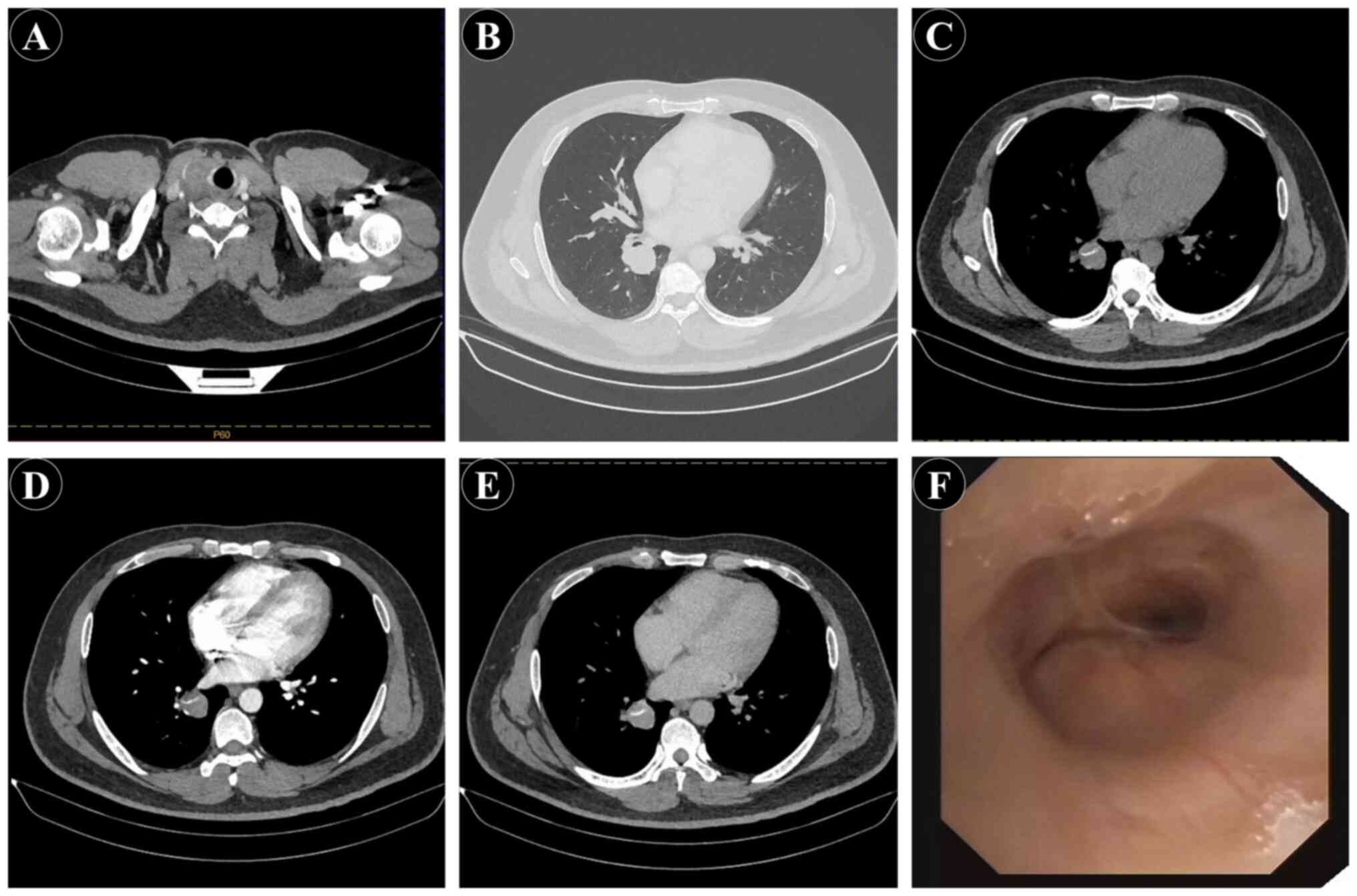
Ultrasound examination identified a solid nodule in
the right thyroid lobe (TI-RADS 4b) and a low-density nodule in the
left thyroid lobe (TI-RADS 4a), according to the American College
of Radiology Thyroid Imaging Reporting and Data System (TI-RADS),
version 2017 (5). Multiple lymph
nodes were observed in the right cervical level IV area, and lymph
nodes were present bilaterally in the neck. A thyroid right lobe
mass and a low-density lesion in the left thyroid lobe was
therefore considered (Fig. 1A).
Subsequent ultrasound-guided bilateral thyroid mass biopsies
confirmed papillary thyroid carcinoma. Chest computed tomography
(CT) revealed a mass near the hilum of the right lower lobe
measuring ~2.9×2.3 cm (Fig. 1B).
Enhanced CT suggested mild enhancement, and the lesion exhibited
characteristics suggestive of a benign lesion, including a linear
calcification (Fig. 1C-E).
Contrast-enhanced chest CT demonstrated heterogeneous enhancement
of the lesion, which initially raised suspicion for a metastatic
lesion from thyroid carcinoma. Local bronchial dilation was noted
in the right lower lobe, along with inflammatory changes in both
lower lobes. Subsequently, bronchoscopy (Fig. 1F) revealed a smooth mucosal surface
in the basal segment of the right lower lobe bronchus, with
extrinsic narrowing.
The patient underwent video-assisted thoracoscopic
surgery for right lower lobe resection under general anesthesia.
Intraoperatively, it was observed that the tumor, closely situated
to the hilum, could not be separately excised. Consequently, a
right lower lobe resection was performed. The bronchus specimen
from the lower right lobe was fixed in 10% formalin and underwent
routine dehydration, paraffin embedding and hematoxylin and eosin
(H&E) staining, which showed GCT features (Fig. 2A and B). Specifically, the tumor
cells displayed larger, round or polygonal shapes, with small, oval
or plump nuclei centrally located. Rare nuclear inclusions were
observed, and the cytoplasm appeared rich with red-staining fine
granules. The tumor cells exhibited no atypia, mitotic figures or
necrosis, and were arranged in nests and sheets. The
immunohistochemistry results (Fig. 2C
and D) revealed positivity for CD68 and S-100, while Ki-67 was
<1%, supporting the final diagnosis of BGCT (right lower lobe
bronchus). The patient experienced an uneventful postoperative
course, exhibiting satisfactory recovery. Subsequently, 1 month
later, the patient underwent thyroid cancer surgery. No further
treatment was administered postoperatively. Follow-up assessments
have revealed no discernible discomfort or complications. The
latest follow-up was conducted on March 5, 2025.
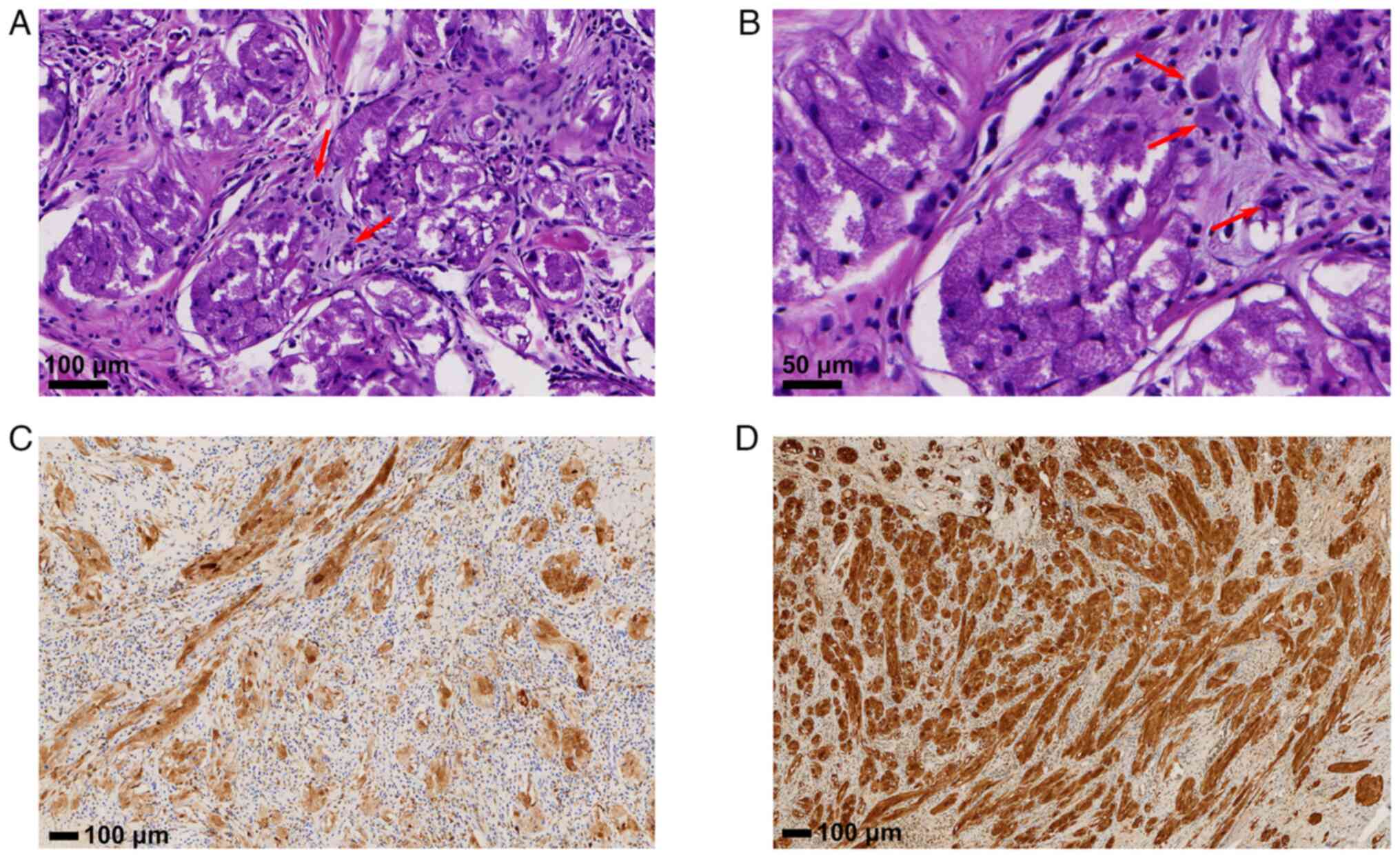 | Figure 2.Pathological and immunohistochemical
diagnosis. (A) Pathological examination at low magnification showed
tumor-like lesions with intact capsules (H&E; magnification,
×200). (B) High magnification view (H&E; magnification, ×400)
showed enlarged tumor cells, predominantly round or polygonal, with
small centrally located nuclei, rich cytoplasm and visible
red-staining granules. No atypia, mitotic figures or necrosis are
observed, presenting a nested and sheet-like arrangement,
consistent with granular cell tumor. Immunohistochemical staining
reveals positive staining for (C) CD68 and (D) S-100
(magnification, ×100). H&E, hematoxylin and eosin. |
Materials and methods
Histological examination
The bronchial specimen was fixed in 10% neutral
buffered formalin at 4°C for 24 h. Tissues were then processed
through a graded ethanol series for dehydration, embedded in
paraffin and sectioned at 4 sm thickness. The sections were
rehydrated through a descending alcohol series (100, 95, 85 and
75%, and distilled water). H&E staining (cat. no. G1120;
Beijing Solarbio Science & Technology Co., Ltd.) was performed
at room temperature, with hematoxylin staining for 5 min and eosin
staining for 1 min. All stained slides were examined using a
Nexcope NE910 light microscope (Ningbo Yongxin Optics Co.,
Ltd.).
Immunohistochemistry
Paraffin-embedded sections (4 µm) were
deparaffinized, rehydrated through a descending alcohol series and
subjected to antigen retrieval by heating in citrate buffer (pH
6.0; cat. no. G1202; Wuhan Servicebio Technology Co., Ltd.) at 95°C
for 20 min. Endogenous peroxidase activity was blocked by
incubation with 3% hydrogen peroxide for 10 min. Sections were then
incubated with 5% normal goat serum (cat. no. ab7481; Abcam) at
room temperature for 30 min to block non-specific binding. The
sections were incubated with the following primary antibodies at
4°C overnight: CD68 (1:100; cat. no. ab955; Abcam), S-100 (1:100,
cat. no. MA1-26621; Invitrogen; Thermo Fisher Scientific, Inc.) and
Ki-67 (1:100; cat. no. M7240; Dako; Agilent Technologies, Inc.).
After washing, goat anti-mouse HRP-conjugated secondary antibodies
(1:500; cat. no. ab6789; Abcam) were applied at room temperature
for 30 min. Immunoreactivity was visualized using DAB chromogen
(cat. no. K3468; Dako; Agilent Technologies, Inc.), followed by
counterstaining with hematoxylin as aforementioned. Slides were
observed using a Nexcope NE910 light microscope.
Discussion
BGCT is clinically rare, and most reported cases
worldwide are individual case reports (1,6). The
exact etiology and pathogenesis of BGCT remain unclear. Current
research suggests that BGCT originates primarily from Schwann
cells, presenting as a neurogenic tumor (4,6). BGCT
can occur at any age, with a peak incidence between 30 and 50
years, and shows no significant sex predilection (7). The majority of patients present with
symptoms such as cough, sputum production, hemoptysis, dyspnea,
fever and chest pain due to tumor invasion or obstruction of the
bronchus (8). Cases may be
incidentally discovered during bronchoscopic examinations or chest
imaging studies (9). In the present
case, the BGCT was incidentally discovered during preoperative
evaluation for thyroid cancer in a 36-year-old male patient, who
was asymptomatic and without pain, fever, cough or respiratory
distress. Although both BGCT and thyroid cancer were identified in
this patient, there is currently no evidence to support a direct
relationship between BGCT and thyroid malignancies, to the best of
our knowledge.
The imaging characteristics of respiratory GCTs
reveal pulmonary lesions with diameters ranging from 0.3 to 6.0 cm,
with an average diameter of 1.0 cm (10). By CT, tracheal GCTs may manifest as
well-defined, round intraluminal masses or may be located around
the bronchi. Tracheal GCTs can cause bronchial obstruction, leading
to bronchitis, pneumonia, bronchiectasis, pulmonary fibrosis,
atelectasis or recurrent episodes of lobar pneumonia (11). High-resolution CT may reveal
segmental consolidation or central nodules distributed within the
affected lobe, indicating lobar bronchitis or atelectasis (12). In the present case,
contrast-enhanced CT demonstrated heterogeneous enhancement,
raising initial concerns of a potential thyroid cancer lung
metastasis. Additionally, the lesion in the present case exhibited
linear calcifications, warranting further distinction from
malignant lesions. To establish a definitive diagnosis,
bronchoscopy was performed, revealing smooth mucosa in the basal
segment of the right lower lobe with extrinsic compressive
narrowing.
The definitive diagnosis of BGCT relies on
pathological and immunohistochemical examinations. Macroscopically,
GCTs often present as pedunculated or sessile polypoid elevations
protruding into the bronchial lumen, exhibiting a lobulated
appearance on cut sections, with colors ranging from gray-white to
pink or light yellow. The texture is moderate, with clear
boundaries from surrounding tissues, lacking a capsule and with
minimal stroma. Surface epithelial coverage may show squamous
metaplasia, simulating pseudoepitheliomatous hyperplasia,
potentially leading to misdiagnosis as squamous cell carcinoma
(13). Microscopically, tumor cells
are round, oval or polygonal, with abundant eosinophilic granular
cytoplasm, small nuclei, occasional visible nucleoli, rare mitoses
and minimal necrosis (14,15). Immunohistochemistry typically
reveals positivity for S-100 protein and CD68, while Ki-67
expression is rare. Conversely, cytokeratin and epithelial membrane
antigen show negative staining, indicating an origin from
mesenchymal tissue (14,15). A study has demonstrated high
sensitivity and specificity for S-100 protein and CD68 in GCT, with
rates ranging from 100 to 65–100%, respectively (16). Therefore, S-100 protein and CD68
serve as valuable immunohistochemical markers for diagnosing GCT
(17). In the present case, the
diagnosis was confirmed through bronchoscopy, histopathology and
immunohistochemical staining, revealing diffusely distributed round
and polygonal cells with lightly stained cytoplasm beneath the
bronchial mucosa. Immunohistochemistry demonstrated positive
staining for S-100 protein and CD68, and negative staining for
Ki-67, consistent with the literature, confirming the diagnosis of
BGCT (18).
Kim et al (19) reported a predilection of BGCT in the
upper lung lobes (10/13) compared with the lower lobes (3/13), with
a seemingly higher incidence in the right lung. In the present
case, BGCT occurred in the lower right lobe. Current standardized
treatment approaches for BGCT remain controversial. Daniel et
al (20) argue that, due to the
lack of a capsule and infiltrative growth, endoscopic treatments
(such as argon plasma coagulation, laser therapy, microwave or
cryoablation) carry a risk of recurrence, with reported rates as
high as 54%. Therefore, complete surgical resection is advocated as
the primary treatment methods, yielding low recurrence rates and
favorable outcomes. van der Maten et al (21) considered endoscopic treatment under
electronic bronchoscopy as a common therapeutic approach for BGCT.
One study reported that patients diagnosed with GCT who do not
undergo any treatment did not experience any deaths during
subsequent follow-ups (21). In the
present case, the patient underwent video-assisted thoracoscopic
surgery for right lower lobe resection under general anesthesia.
Intraoperatively, the tumor was found to be situated near the
hilum, preventing independent excision and necessitating a right
lower lobe resection.
In summary, BGCT is an exceedingly rare pulmonary
tumor often presenting with subtle or non-specific clinical
manifestations. Radiological findings lack specificity,
necessitating reliance on histopathological examination for
accurate diagnosis. While predominantly benign, complete surgical
excision remains the cornerstone of treatment and recurrence
prevention for this condition.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
BW, CL and ML were involved in the diagnosis and
treatment of the patient. BW, CL, RH and GL contributed to data
acquisition and analysis. BL, RH, GL and JZ participated in the
interpretation of findings. BL, ML and JZ provided critical
revisions for important intellectual content and supervised the
manuscript preparation. BW and ML confirm the authenticity of all
the raw data. All authors read and approved the final version of
the manuscript.
Ethics approval and consent to
participate
The study involving human participants was reviewed
and approved by the Ethics Committee of Cangzhou Fifth Hospital
(People's Hospital of Qingxian, Cangzhou, China; approval no.
20240503) and was conducted in accordance with the Declaration of
Helsinki of 1975.
Patient consent for publication
Written informed consent was obtained from the
patient for the publication of any potentially identifiable images
or data contained herein.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Xu GX, Wang C, Sui JJ, Gao SY, Wang XY,
Zhao SL and Tang LJ: A case report of bronchial granular cell
tumor. Zhonghua Jie He He Hu Xi Za Zhi. 46:1121–1123. 2023.(In
Chinese).
|
|
2
|
Cardis MA, Ni J and Bhawan J: Granular
cell differentiation: A review of the published work. J Dermatol.
44:251–258. 2017. View Article : Google Scholar
|
|
3
|
Meyer MA, Becker JM and Quinones W:
Endobronchial granular cell tumor: A case report. J Radiol Case
Rep. 4:29–35. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lin N, Liu T and Wang R: Lung squamous
cell carcinoma combined with bronchial granular cell tumor: Report
of 1 case and review of literature. Cancer Res Clin. 36:698–702.
2024.
|
|
5
|
Tessler FN, Middleton WD, Grant EG, Hoang
JK, Berland LL, Teefey SA, Cronan JJ, Beland MD, Desser TS, Frates
MC, et al: ACR thyroid imaging, reporting and data system
(TI-RADS): White paper of the ACR TI-RADS committee. J Am Coll
Radiol. 14:587–595. 2017. View Article : Google Scholar
|
|
6
|
Houcine Y, Mlika M, Moussa C, Rouis H,
Brahem E, Ismail O, Maȃlej S and El Mezni F: Granular cell tumor of
the lung and tracheobronchial tree: Two case-presentation with a
review of the literature. Rare Tumors. 15:203636132311878222023.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tian G, Ge J and Liu X: A case of
bronchial granular cell tumour with literature review. Chin J
Respir Crit Care Med. 18:76–80. 2019.
|
|
8
|
Joung MK, Lee YJ, Chung CU, Lee JE, Jung
SS, Kim SY and Kim JO: A case of granular cell tumor of the
trachea. Korean J Intern Med. 22:101–105. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Jobrack AD, Goel S and Cotlar AM: Granular
cell tumor: Report of 13 cases in a veterans administration
hospital. Mil Med. 183:e589–e593. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Deavers M, Guinee D, Koss MN and Travis
WD: Granular cell tumors of the lung. Clinicopathologic study of 20
cases. Am J Surg Pathol. 19:627–635. 1995. View Article : Google Scholar
|
|
11
|
Miyake M, Tateishi U, Maeda T, Arai Y,
Hasegawa T and Sugimura K: Bronchial granular cell tumor: A case
presenting secondary obstructive changes on CT. Radiat Med.
24:154–157. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kutuya N and Akiduki A: Radiologic
appearance of a bronchial granular cell tumor with secondary
obstructive changes. Clin Imaging. 34:148–151. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ping H, Guangyu Y and Xia G:
Tracheobronchial benign tumour diagnosed by bronchoscopic biopsy: A
clinicopathologic analysis of 11 cases. Chin J Clin Exp Pathol.
28:415–418. 2012.
|
|
14
|
Grove J, Meier C, Youssef B and Costello
P: A rare case of granular cell tumor in the right upper lung of an
adolescent patient. Cureus. 14:e215582022. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yamada S, Katayama Y, Fujimoto Y, Kobori
I, Kusano Y, Soga K, Sato T, Matsushima J, Ban S and Tamano M: A
granular cell tumor arising in a patient with long-segment
Barrett's esophagus. Intern Med. 64:557–561. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
An S, Jang J, Min K, Kim MS, Park H, Park
YS, Kim J, Lee JH, Song HJ, Kim KJ, et al: Granular cell tumor of
the gastrointestinal tract: Histologic and immunohistochemical
analysis of 98 cases. Hum Pathol. 46:813–819. 2015. View Article : Google Scholar
|
|
17
|
Liu HF, Huang Y, Wu CY, Li Y, Wang YC,
Zhang LP, Hou LK and Xie HK: Pulmonary granular cell tumors: A
clinicopathological analysis of five cases. Zhonghua Bing Li Xue Za
Zhi. 52:136–141. 2023.(In Chinese).
|
|
18
|
Jian W and Xiongzeng Z: Pathology of Soft
Tissue Tumours. People's Health Press; Beijing: 2008
|
|
19
|
Kim HJ, An S and Kim HR: Primary bronchial
granular cell tumor in an adult male. Korean J Thorac Cardiovasc
Surg. 47:193–196. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Daniel TM, Smith RH, Faunce HF and Sylvest
VM: Transbronchoscopic versus surgical resection of
tracheobronchial granular cell myoblastomas. Suggested approach
based on follow-up of all treated cases. J Thorac Cardiovasc Surg.
80:898–903. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
van der Maten J, Blaauwgeers JL, Sutedja
TG, Kwa HB, Postmus PE and Wagenaar SS: Granular cell tumors of the
tracheobronchial tree. J Thorac Cardiovasc Surg. 126:740–743. 2003.
View Article : Google Scholar : PubMed/NCBI
|