Introduction
Pulmonary sarcomatoid carcinoma is a rare tumour
that accounts for approximately 0.5% of all lung tumours (1). Pulmonary pleomorphic carcinoma (PPC),
the most common subtype of pulmonary sarcomatoid carcinoma, is a
poorly differentiated non-small cell lung cancer (NSCLC) that
accounts for 0.1–0.3% of all lung tumours (2). Pleomorphic carcinoma is diagnosed when
tumours consist exclusively of spindle and/or giant cells or when
spindle and/or giant cells account for ≥10% of the total tumour
(3). Therefore, to confirm the
pathological diagnosis of PPC, the entire tumour needs to be
evaluated via surgical resection, and a biopsy specimen is
insufficient for a definitive diagnosis. This kind of tumour is
highly malignant, rapidly progressing, and refractory to various
therapies (4). The outcome of
surgical resection is poor, with 57.1% of pN0 cases reported to
have vascular invasion (5), and
distant metastases is commonly detected early after surgery. The
median survival time for patients with PPC is 10–12 months, with a
5-year survival rate of approximately 10%, and the response to
chemotherapy is poorer than that of NSCLC (6). However, recent advances in molecular
targeted therapy and immune checkpoint inhibitors (ICIs) have led
to significant progress in therapeutic strategies.
MET exon 14 skipping mutations are found in
approximately 3% of NSCLC cases (7). Unlike other driver gene
mutations/translocations, including those in EGFR, ALK, and
ROS1, the MET exon 14 skipping mutation has also been
detected in older patients and smokers (7). It is characterised by the fact that it
is not only found in pulmonary adenocarcinomas but also in
approximately 5% of pulmonary adenosquamous carcinomas and 10–32%
of pulmonary sarcomatoid carcinomas (6,8,9).
Although tepotinib and capmatinib have been approved by the Food
and Drug Administration (FDA) for the treatment of unresectable
advanced or recurrent NSCLC with MET exon 14 skipping
mutations (7,10), to our knowledge, no previous study
has reported on the use of MET inhibitors in patients with
pulmonary sarcomatoid carcinoma. Herein, we report the case of a
patient with PPC with a MET exon 14 skipping mutation that
was successfully treated with tepotinib as the primary drug and
with pembrolizumab as the subsequent ICI therapy.
Case report
A 75-year-old woman with no history of smoking
underwent left upper lobectomy, pulmonary angioplasty, and lymph
node dissection (ND2a-2) for an approximately 4-cm mass in the left
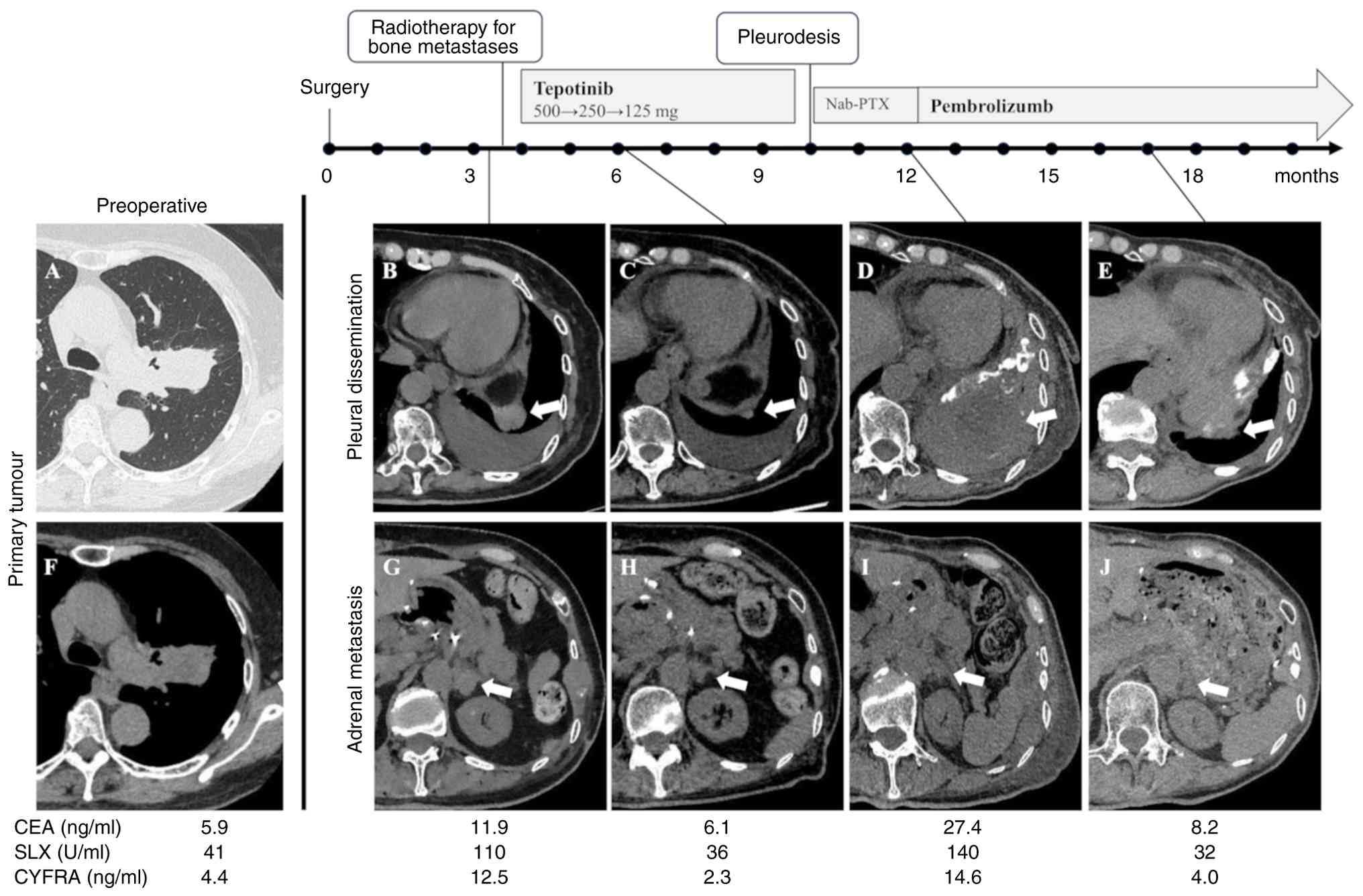
upper lobe with pulmonary artery invasion (Fig. 1A and F) in May 2022 at Niigata
University Medical and Dental Hospital (Niigata, Japan). The
patient had comorbidities such as hypertension, chronic kidney
disease, and atrial fibrillation.
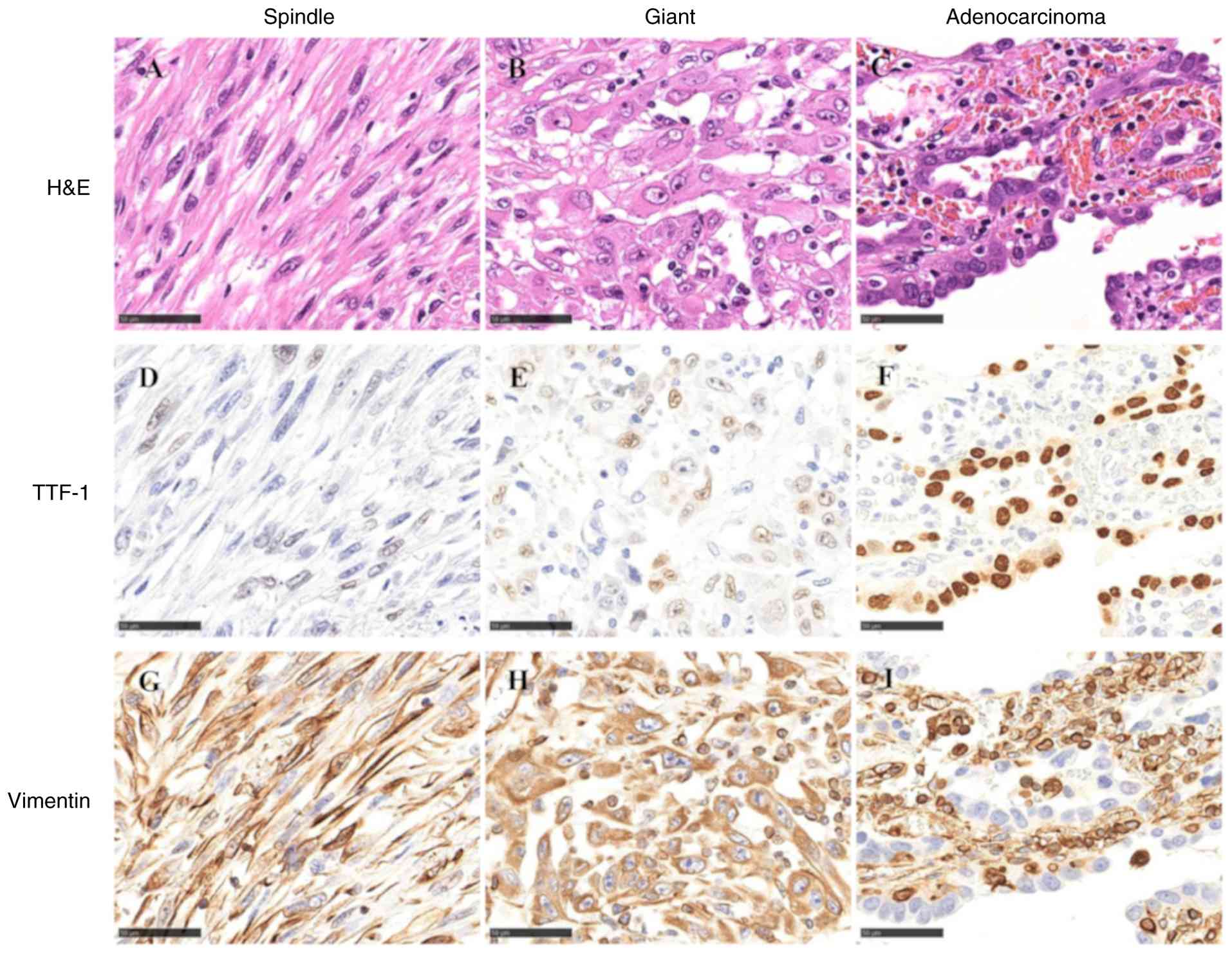
Pathological examination of the resected specimen
showed the presence of PPC consisting of spindle cell carcinoma
(50%), giant cell carcinoma (30%), and adenocarcinoma components
(20%) (Fig. 2A-C).
Immunohistochemical analysis showed that the spindle cells, giant
cells, and adenocarcinoma components (Fig. 2D-F) were weakly positive, weakly
positive, and positive, respectively, for thyroid transcription
factor-1 (TTF-1) while they were positive, positive, and negative,
respectively, for vimentin (Fig.
2G-I). For haematoxylin and eosin staining, surgically resected
specimens were fixed in 10% neutral buffered formalin at room
temperature for 48 h. Representative tissue samples were selected,
embedded in paraffin and sectioned at a thickness of 4 µm. The
sections were then deparaffinized in xylene, rehydrated through a
graded series of ethanol, and stained with haematoxylin for 5 min
and eosin for 2 min at room temperature. Immunohistochemical
staining was performed on the 4-µm sections prepared from
formalin-fixed, paraffin-embedded tissue. Briefly, antigen
retrieval was carried out using citrate buffer (pH 6.0) and
endogenous peroxidase blocking was performed with 3% hydrogen
peroxide (cat. no. 081-04215; FUJIFILM Wako Pure Chemical
Corporation) for 5 min at room temperature. The primary antibodies
used were TTF-1 (1:200; for 30 min at room temperature; clone
SPT24; cat. no. NCL-L-TTF-1; Leica Biosystems) and vimentin (1:1;
for 30 min at room temperature; clone V9; cat. no. 718511; Nichirei
Biosciences, Inc.). Histofine® Simple Stain™
MAX PO (MULTI) (1:1; for 30 min at room temperature; cat. no.
424151; Nichirei Biosciences, Inc.) was used as a secondary
antibody. Immunoreactivity was visualized using
3,3′-diaminobenzidine, and nuclei were counterstained with
haematoxylin. All slides were examined under a light
microscope.
According to the 8th TNM classification, the
pathological stage was T2aN0M0 stage IB.
Three months postoperatively, the patient
experienced left shoulder pain, and visited the hospital, with an
Eastern Cooperative Oncology Group performance status of 2 owing to
the pain and state of recovery postoperatively. Computed tomography
(CT) showed a 26-mm nodule on the left diaphragm, which was
considered to indicate pleural dissemination, bilateral adrenal
metastases (right: 11 mm, left: 21 mm), and multiple bone
metastases, including to the fourth cervical vertebra and left ribs
(Fig. 1B and G). The CEA level was
11.9 ng/ml (normal range, ≤5.0 ng/ml), SLX level was 110 U/ml
(normal range, ≤38 U/ml), and CYFRA level was 12.5 ng/ml (normal
range, ≤3.5 ng/ml). Palliative radiotherapy was administered for
bone metastases, with 30 Gy in 10 fractions to the fourth cervical
vertebra and 20 Gy in 5 fractions to the left eighth rib.
Analysis of the resected tumour using the
Oncomine™ Dx Target Test Multi CDx System with
next-generation sequencing (NGS) revealed a MET exon 14
skipping mutation, with a PD-L1 expression level of >75% by
PD-L1 IHC 22C3 pharm Dx Dako. As both analyses were performed as
outsourced tests, the raw data were not available. In September
2022, four months after surgery, the patient was hospitalized and
received tepotinib (500 mg/day) as primary drug therapy after the
completion of radiotherapy. On day 10 of tepotinib treatment, the
dose was reduced to 250 mg/day owing to a grade 2 creatinine
increase, according to the Common Terminology Criteria for Adverse
Events, version 5.0. On day 17, grade 2 liver injury occurred and
tepotinib was discontinued. One week after withdrawal, both hepatic
and renal functions recovered and tepotinib was restarted at 125
mg/day. Subsequently, the patient experienced no apparent adverse
events.
Two months after initiating tepotinib, CT imaging
showed a reduction in pleural dissemination on the left diaphragm
(5 mm) and in bilateral adrenal metastases (right: 5 mm, left: 12
mm) (Fig. 1C and H), and the
response was assessed as a partial response (PR).
However, 5 months after the initiation of tepotinib,
a CT scan showed that although the reduction in the extent of the
bilateral adrenal metastases was maintained, the pleural
dissemination had progressed and the amount of left pleural
effusion had increased (pleural dissemination: 93 mm, left adrenal
metastasis: 13 mm, Fig. 1D and I),
leading to the diagnosis of progressive disease (PD).
Consequently, the patient underwent pleural drainage
and pleurodesis using talc. At the beginning of the secondary
treatment, the patient was found to have inflammation in the left
lower lobe, which was possibly caused by pleurodesis. Owing to
concerns regarding the progression of pulmonary inflammation, ICIs
were avoided. Therefore, nab-paclitaxel was administered as the
second-line therapy. After the first course of nab-paclitaxel, the
size of the pleural dissemination increased, accompanied by an
increase in chest pain, leading to the assessment of PD. At that
time, the ground-glass opacity of the left lower lobe had
disappeared; therefore, pembrolizumab was started as third-line
therapy. Thereafter, the left pleural dissemination shrunk and the
chest pain disappeared; the response was assessed as PR (pleural
dissemination: 25 mm, left adrenal metastasis: 13 mm, Fig. 1E and J). The patient had no apparent
adverse events. Nine months after the initiation of pembrolizumab,
the patient required palliative radiotherapy for enlargement of a
left iliac metastasis. No significant disease progression was
observed at other sites, and pembrolizumab treatment was
successfully continued for a total of 19 months. Subsequently, the
patient developed infection and heart failure. Owing to a decline
in performance status, anticancer therapy was discontinued, and the
patient died of primary disease 36 months after surgery at the
receiving hospital.
Discussion
In the present case, PPC was pathologically
diagnosed using a resected specimen and the patient experienced
recurrence soon after surgery. NGS revealed a MET exon 14
skipping mutation, and PD-L1 was highly expressed. The optimal
first-line therapy for MET exon 14 skipping-positive NSCLC
remains undetermined, with differing recommendations across
guidelines regarding whether to use a MET inhibitor or standard
systemic therapy including ICI (11–13).
In this case, given the patient's symptomatic condition and poor
performance, a MET inhibitor was prioritized considering the
expectation of a favourable response characteristic of molecularly
targeted drugs. Tepotinib as a primary therapy achieved a good
short-term response. Subsequently, pembrolizumab treatment resulted
in a favourable long-term response.
Although tepotinib and capmatinib have been approved
by the FDA and are standard therapies for NSCLC with MET
exon 14 skipping mutations, little is known about their efficacy in
sarcomatoid carcinoma with MET exon 14 skipping mutations.
Previously, in a phase II VISION study on the use of tepotinib for
treating MET exon 14 skipping mutation-positive unresectable
advanced NSCLC, the overall response rate (ORR) was 46%, with a
progression-free survival (mPFS) of 8.5 months and overall survival
(mOS) of 17.1 months. However, the majority of the cases were
adenocarcinomas, and only 1/99 cases (approximately 1%) was that of
sarcoma-like NSCLC (14). Another
phase II study on the use of capmatinib (GEOMETRY mono-1 study)
showed an ORR of 68% and mPFS of 12.4 months in untreated patients
and an ORR of 41% and mPFS of 5.4 months in previously treated
patients (15). However, it was not
specified whether patients with sarcomatoid carcinomas were
included in this study. In contrast, a phase II study of
savolitinib monotherapy in locally advanced or metastatic
MET exon 14 skipping-positive NSCLC in China reported an ORR
of 40% and mPFS of 5.5 months in 25 patients with pulmonary
sarcomatoid carcinoma, suggesting a potential benefit in patients
with pulmonary sarcomatoid carcinoma (16). Nonetheless, there are insufficient
data on the effect of MET inhibitors on sarcomatoid carcinomas with
MET exon 14 skipping mutations. To the best of our
knowledge, this is the first report of a PPC harbouring a
MET exon 14 skipping mutation that was successfully treated
with tepotinib.
In recent years, research on the biological
characteristics of pulmonary sarcomatoid carcinoma has progressed,
and it has become clear that therapeutic intervention based on
genetic mutations is as important as that in other NSCLCs.
Microdissection analysis of the epithelial and sarcomatoid
components of PPCs has revealed that both components harbour
similar genomic alterations, including activating driver mutations
(17). Therefore, even in
heterogeneous cancers such as pleomorphic carcinoma, a certain
effect of molecular targeted therapies can be expected when driver
mutations are detected.
In our patient's case, the PFS with tepotinib was
relatively shorter than that reported in studies on NSCLC with
MET exon 14 skipping. Acquired resistance to the selective
tepotinib in MET exon 14 skipping NSCLC involves both
on-target and off-target mechanisms. On-target resistance is
predominantly caused by secondary mutations in the MET kinase
domain, especially at residues D1228 and Y1230, which impair drug
binding and restore MET signalling despite continued tepotinib
exposure. Off-target or bypass resistance mechanisms include
alterations in KRAS, EGFR/HER family genes, and other downstream
effectors, which reactivate proliferative signalling independent of
MET inhibition (18,19). In this case, the presence of
pleomorphic carcinoma, a histologic subtype known for its marked
heterogeneity, may have contributed to the tumour's susceptibility
to phenotypic change. In addition, the reduction of the systemic
therapy dose to one-quarter of the standard level due to renal and
hepatic dysfunction likely influenced the short PFS.
Pulmonary sarcomatoid carcinoma is known to be an
immune-hot tumour with a high tumour mutation burden, abundant
CD8+ T cell infiltration, and high expression of PD-L1
(20). For treating these tumours,
ICIs such as anti-PD-1/PD-L1 and anti-CTLA-4 antibodies are
expected to be effective. In fact, a previous analysis of 124
patients with advanced or metastatic pulmonary sarcomatoid
carcinoma treated with ICI revealed an ORR of 59%, mPFS of 10.5
months, and mOS of 32.8 months, and 81 patients (65%) were strongly
positive for PD-L1 (21).
Additionally, in the analysis of 37 patients with pulmonary
sarcomatoid carcinoma who were treated with ICI monotherapy as
secondary treatment, an ORR of 40.5%, mPFS of 4.9 months, and mOS
of 12.7 months were obtained regardless of PD-L1 expression
(22). In another single-arm phase
II study conducted at a Korean institution to evaluate the efficacy
of durvalumab and tremelimumab in 18 patients with recurrent or
metastatic pulmonary sarcomatoid carcinoma, the ORR, mPFS, and mOS
were 26.7%, 5.9 months, and 15.4 months, respectively (23). In our case, PPC showed high PD-L1
expression, for which pembrolizumab led to a durable response.
Thus, ICIs are gradually improving clinical outcomes of patients
with sarcomatoid carcinomas such as PPC. Therefore, ICIs should be
considered as key drugs for the treatment of sarcomatoid
carcinoma.
This case report has several limitations. First, the
patient's advanced age, poor performance status and the need for
pleurodesis and palliative care during the course of treatment
required careful consideration of treatment selection at each
stage. In addition, dose reduction of tepotinib was necessary,
which likely limited its efficacy. Given these constraints,
determining the optimal first-line treatment for this case,
characterized by MET exon 14 skipping mutation, high PD-L1
expression, and sarcomatoid carcinoma rather than conventional
NSCLC, remains challenging. Another limitation is that a tumour
re-biopsy could not be performed at the time the patient developed
resistance to tepotinib because of the patient's poor performance
status and the need for an urgent change in treatment, which
ultimately precluded elucidation of the underlying resistance
mechanism.
In conclusion, the present study describes the case
of patient with PPC with a MET exon 14 skipping mutation
that was treated with tepotinib and subsequently pembrolizumab
therapy that led to a durable response. Therefore, sarcomatoid
carcinoma, which is generally considered to have a poor prognosis,
may have a better prognosis when treated with ICI and MET
inhibitors. Consequently, it is critical to consider driver
mutations in PPC and other pulmonary sarcomatoid carcinomas and to
seize the opportunity to treat patients with these carcinomas using
molecular targeted medications or ICIs.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
ST contributed to conceptualization and writing the
original draft. YS conceptualized the study, wrote the original
draft, and reviewed and edited the manuscript. YA, JA, RY, TW, HW,
KK, RS, NY, MA, MS, TT, KN and SK contributed to data collection.
SW, HU and TK contributed to analysis and interpretation of the
data, supervision and editing. YS, SW, and TK confirm the
authenticity of all the raw data. All authors read and approved the
final manuscript.
Ethics approval and consent to
participate
Written informed consent was obtained from the
patient, including consent to participate.
Patient consent for publication
Written informed consent was obtained from the
patient, including consent for publication of the findings.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Steuer CE, Behera M, Liu Y, Fu C,
Gillespie TW, Saba NF, Shin DM, Pillai RN, Pakkala S, Owonikoko TK,
et al: Pulmonary sarcomatoid carcinoma: An analysis of the national
cancer data base. Clin Lung Cancer. 18:286–292. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chang YL, Lee YC, Shih JY and Wu CT:
Pulmonary pleomorphic (spindle) cell carcinoma: Peculiar
clinicopathologic manifestations different from ordinary non-small
cell carcinoma. Lung Cancer. 34:91–97. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Nicholson AG, Tsao MS, Beasley MB, Borczuk
AC, Brambilla E, Cooper WA, Dacic S, Jain D, Kerr KM, Lantuejoul S,
et al: The 2021 WHO classification of lung tumors: Impact of
advances since 2015. J Thorac Oncol. 17:362–387. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tamura Y, Fujiwara Y, Yamamoto N, Nokihara
H, Horinouchi H, Kanda S, Goto Y, Kubo E, Kitahara S, Tsuruoka K,
et al: Retrospective analysis of the efficacy of chemotherapy and
molecular targeted therapy for advanced pulmonary pleomorphic
carcinoma. BMC Res Notes. 8:8002015. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Rossi G, Cavazza A, Sturm N, Migaldi M,
Facciolongo N, Longo L, Maiorana A and Brambilla E: Pulmonary
carcinomas with pleomorphic, sarcomatoid, or sarcomatous elements:
A clinicopathologic and immunohistochemical study of 75 cases. Am J
Surg Pathol. 27:311–324. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Yuki T, Sakuma T, Ohbayashi C, Yoshimura
M, Tsubota N, Okita Y and Okada M: Pleomorphic carcinoma of the
lung: A surgical outcome. J Thorac Cardiovasc Surg. 134:399–404.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Awad MM, Oxnard GR, Jackman DM, Savukoski
DO, Hall D, Shivdasani P, Heng JC, Dahlberg SE, Jänne PA, Verma S,
et al: MET Exon 14 mutations in non-small-cell lung cancer are
associated with advanced age and stage-dependent MET genomic
amplification and c-Met overexpression. J Clin Oncol. 34:721–730.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Fishback NF, Travis WD, Moran CA, Guinee
DG Jr, McCarthy WF and Koss MN: Pleomorphic (spindle/giant cell)
carcinoma of the lung. A clinicopathologic correlation of 78 cases.
Cancer. 73:2936–2945. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Frampton GM, Ali SM, Rosenzweig M,
Chmielecki J, Lu X, Bauer TM, Akimov M, Bufill JA, Lee C, Jentz D,
et al: Activation of MET via diverse exon 14 splicing alterations
occurs in multiple tumor types and confers clinical sensitivity to
MET inhibitors. Cancer Discov. 5:850–859. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tong JH, Yeung SF, Chan AWH, Chung LY,
Chau SL, Lung RWM, Tong CY, Chow C, Tin EKY, Yu YH, et al: MET
amplification and exon 14 splice site mutation define unique
molecular subgroups of non-small cell lung carcinoma with poor
prognosis. Clin Cancer Res. 22:3048–3056. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Riely GJ, Wood DE, Aisner DL, Loo BW Jr,
Axtell AL, Bauman JR, Bharat A, Chang JY, Desai A, Dilling TJ, et
al: NCCN guidelines® insights: Non-small cell lung
cancer, version 7.2025. J Natl Compr Canc Netw. 23:354–362. 2025.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Reuss JE, Kuruvilla S, Ismaila N, Azar IH,
Feldman J, Furuya N, Wheatley-Price P, Roof L, Velazquez AI, Wang Y
and Leighl NB: Therapy for stage IV non-small cell lung cancer with
driver alterations: ASCO living guideline, version 2025.1. J Clin
Oncol. 43:e31–e44. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hendriks LEL, Cortiula F, Martins-Branco
D, Mariamidze E, Popat S and Reck M; ESMO Guidelines Committee.
Electronic address, : simpleclinicalguidelines@esmo.org:
Updated treatment recommendations for systemic treatment: From the
ESMO oncogene-addicted metastatic NSCLC living guideline. Ann
Oncol. 36:1227–1231. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Paik PK, Felip E, Veillon R, Sakai H,
Cortot AB, Garassino MC, Mazieres J, Viteri S, Senellart H, Van
Meerbeeck J, et al: Tepotinib in non-small-cell lung cancer with
MET exon 14 skipping mutations. N Engl J Med. 383:931–943. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Wolf J, Seto T, Han JY, Reguart N, Garon
EB, Groen HJM, Tan DSW, Hida T, de Jonge M, Orlov SV, et al:
Capmatinib in MET exon 14-mutated or MET-amplified non-small-cell
lung cancer. N Engl J Med. 383:944–957. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lu S, Fang J, Li X, Cao L, Zhou J, Guo Q,
Liang Z, Cheng Y, Jiang L, Yang N, et al: Once-daily savolitinib in
Chinese patients with pulmonary sarcomatoid carcinomas and other
non-small-cell lung cancers harbouring MET exon 14 skipping
alterations: A multicentre, single-arm, open-label, phase 2 study.
Lancet Respir Med. 9:1154–1164. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Nagano M, Kohsaka S, Hayashi T, Ueno T,
Kojima S, Shinozaki-Ushiku A, Morita S, Tsuda M, Tanaka S,
Shinohara T, et al: Comprehensive molecular profiling of pulmonary
pleomorphic carcinoma. NPJ Precis Oncol. 5:572021. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fujino T, Kobayashi Y, Suda K, Koga T,
Nishino M, Ohara S, Chiba M, Shimoji M, Tomizawa K, Takemoto T and
Mitsudomi T: Sensitivity and resistance of MET exon 14 mutations in
lung cancer to eight MET tyrosine kinase inhibitors in vitro. J
Thorac Oncol. 14:1753–1765. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yao Y, Yang H, Zhu B, Wang S, Pang J, Wu
X, Xu Y, Zhang J, Zhang J, Ou Q, et al: Mutations in the MET
tyrosine kinase domain and resistance to tyrosine kinase inhibitors
in non-small-cell lung cancer. Respir Res. 24:282023. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vieira T, Antoine M, Hamard C, Fallet V,
Duruisseaux M, Rabbe N, Rodenas A, Cadranel J and Wislez M:
Sarcomatoid lung carcinomas show high levels of programmed death
ligand-1 (PD-L1) and strong immune-cell infiltration by TCD3 cells
and macrophages. Lung Cancer. 98:51–58. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hazama D, Nakahama K, Kodama H, Miyazaki
A, Azuma K, Kawashima Y, Sato Y, Ito K, Shiraishi Y, Miura K, et
al: Effectiveness and safety of immune checkpoint inhibitors alone
or in combination with chemotherapy in pulmonary sarcomatoid
carcinoma. JTO Clin Res Rep. 5:1006132024.PubMed/NCBI
|
|
22
|
Domblides C, Leroy K, Monnet I, Mazières
J, Barlesi F, Gounant V, Baldacci S, Mennecier B, Toffart AC,
Audigier-Valette C, et al: Efficacy of immune checkpoint inhibitors
in lung sarcomatoid carcinoma. J Thorac Oncol. 15:860–866. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Kim M, Keam B, Ock CY, Kim SH, Kim YJ, Lim
SM, Kim JS, Kim TM, Hong SH, Ahn MS, et al: Phase II study of
durvalumab and tremelimumab in pulmonary sarcomatoid carcinoma:
KCSG-LU16-07. Thorac Cancer. 11:3482–3489. 2020. View Article : Google Scholar : PubMed/NCBI
|