Introduction
Clear cell sarcoma (CCS) is a tumor that arises from
neural crest cells and accounts for ~1% of all diagnosed soft
tissue sarcomas; it was first described by Enzinger in 1965
(1) and is most commonly found in
tendinous sheaths and aponeuroses (1–4). CCS
commonly involves the lower limbs, particularly the ankles and feet
(2); however, sporadic
presentations in the kidney, thorax, abdomen, head and neck have
been described. Male and female patients of any age are equally
affected, with a peak incidence in the third and fourth decades of
life (5,6), Nevertheless, isolated cases have been
reported in pediatrics and adolescents (2,7).
CCS usually presents as a small tender lump or
swelling, and may involve subcutaneous tissue, the adjacent dermis
and ulceration of the overlying skin (2,8).
Although rare, CCS has been reported in the hand, where it can pose
notable diagnostic challenges as it often resembles more benign
conditions, such as glomus tumors, highlighting the importance of
maintaining a high index of suspicion. The prognosis for CCS is
generally poor, with reported distant metastasis rates ranging
between 60 and 70%, primarily to the lungs or lymph nodes (4,9). This
high risk of metastasis underscores the need for early detection
and appropriate management. The present study describes an unusual
case of CCS manifesting as a subungual swelling on the right index
finger of a 14-year-old girl. The aim of the report is to provide a
comprehensive review of the diagnostic and treatment approaches for
CCS, as well as to discuss the importance of accurate clinical
evaluation to avoid misdiagnosis and ensure early multidisciplinary
management. While CCS is rare and similar cases have been reported
(1,2), the current case represents the seventh
case of CCS presenting in the finger and the second pediatric case
published. Notably, to the best of our knowledge, it is the first
pediatric case with a favorable prognosis and no recurrence, which
adds valuable insight into the potential for long-term survival in
this population of patients. These aspects may contribute to the
current understanding of CCS, particularly in pediatric
patients.
Case report
The present study describes the case of a
14-year-old girl who presented to the orthopedic clinic at King
Khalid University Hospital (King Saud University Medical City,
Riyadh, Saudi Arabia, on January 2023 with a 4-year history of
right index finger swelling, associated with severe pain, rapid
progression in size over the last year, and no history of trauma or
fever. The patient had no other lumps elsewhere, and denied any
constitutional symptoms, or personal or family history of
neoplasms. Physical examination of the right hand revealed a
swelling with dark skin pigmentation of the tip of the second
finger and melanonychia (brownish-black discoloration of the nail
plate) associated with tenderness but no ulceration or discharge
(Figs. 1 and 2). The systemic examination was
unremarkable. Initial radiographic investigation with X-ray, which
was performed at another institution before presenting to the
aforementioned orthopedic clinic, revealed a well-circumscribed
lytic lesion involving the volar aspect of the distal phalanx of
the right index finger, with no evidence of pathological
fracture.
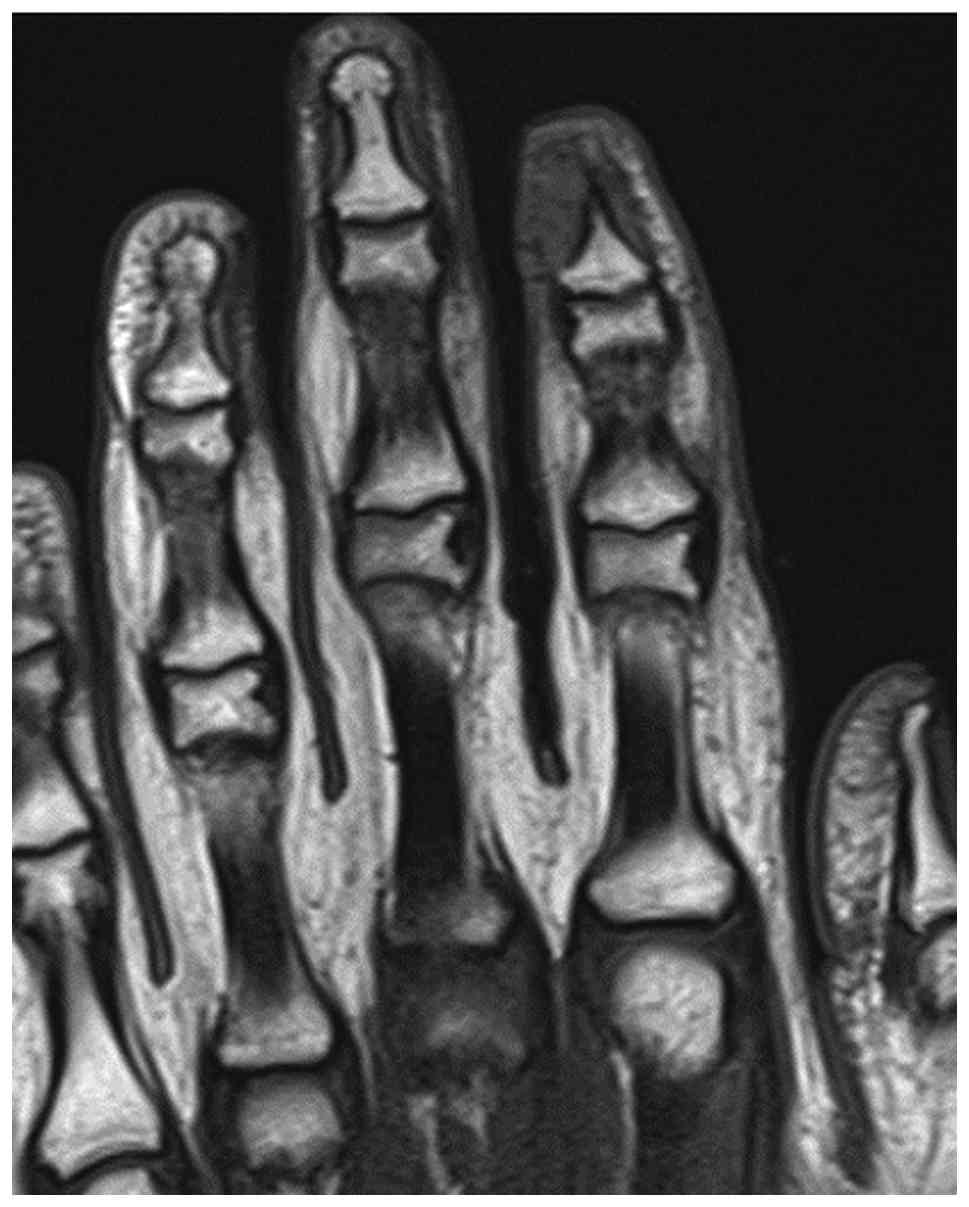
Further evaluation with contrast-enhanced magnetic
resonance imaging (MRI) was performed, including axial, sagittal
and coronal projections on T1-weighted, fat-saturated-T2-weighted,
proton density and post-contrast T1-weighted images. MRI revealed a
well-defined, rounded soft tissue lesion seen dorsal to the distal
phalanx of the right index finger, measuring 0.5×0.2×0.5 cm,
demonstrating low signal intensity on the T1-weighted images, high
signal intensity on the T2-weighted images and intense homogenous
enhancement on the post-contrast images (Fig. 3, Fig.
4, Fig. 5, Fig. 6). Moreover, surrounding subcutaneous
tissue and bone marrow edema was observed, with underlying bone
remodeling of the distal phalanx. No other lesions or fractures
were observed. Considering the location and radiological features
of the lesion; the initial impression suggested a glomus tumor.
Consequently, intralesional surgical excision of the
lesion was performed using an ulnar-sided approach to the distal
phalanx of the second finger with nail bed flap elevation; and the
resected tissues were sent for histopathological assessment, as
informed by previously published literature (10–12).
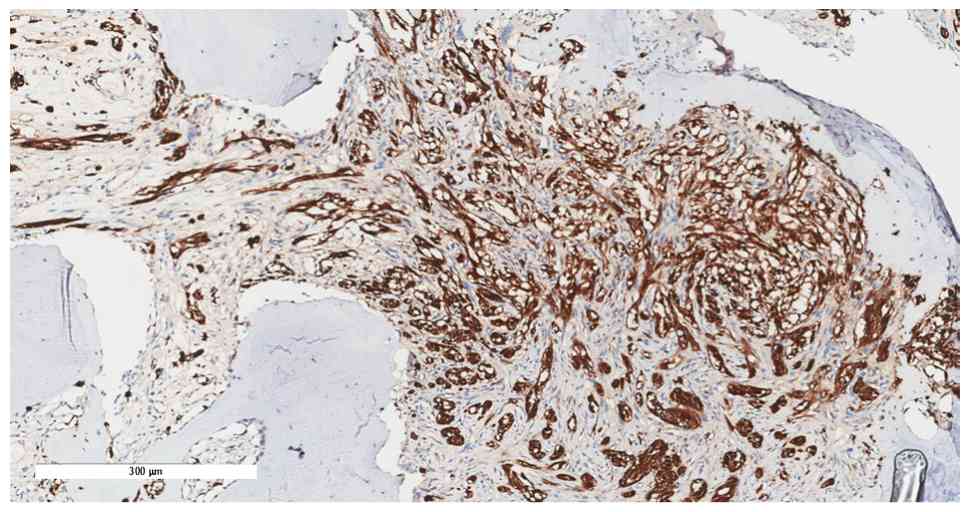
Notably, the histopathological assessment revealed minute fragments
of bone with fibrous tissue and entrapped clear cells suggestive of
CCS (Fig. 7, Fig. 8, Fig.
9, Fig. 10). The tumor showed
diffuse cytoplasmic staining for the immunohistochemical markers
HMB-45 and S-100 protein, supporting the diagnosis of CCS. The
results were subsequently sent to a specialized sarcoma pathologist
in the oncology center King Faisal Specialist Hospital and Research
Centre (Riyadh, Saudi Arabia), who concurred with the
diagnosis.
Further local and systemic staging evaluation was
performed and confirmed localized disease (stage II) using the
American Joint Committee on Cancer staging system (13). Hence, the patient was informed and
referred to a tertiary oncology center. A discussion at a
multidisciplinary sarcoma tumor board meeting recommended local
control with wide surgical resection by amputation through the
middle phalanx, considering the potential contamination of the
distal phalanx during the previous unplanned surgical resection.
Neither local radiotherapy nor systemic chemotherapy was
recommended by the tumor board, given the location and small size
of the tumor and the absence of metastasis.
At the tertiary center, the proposed surgical
treatment was explained to the patient and their parents, and
informed consent was obtained. The patient underwent amputation
through the middle phalanx of the right index finger, aiming to
achieve local control with negative margins. During the procedure,
meticulous dissection was performed to isolate digital
neurovascular bundles, which were transected proximally while
maintaining hemostasis. The flexor digitorum superficialis (FDS)
tendon was preserved while flexor digitorum profundus tenotomy was
performed at the base of the middle phalanx level, followed by
tenodesis to the FDS tendon. An osteotomy was then performed of the
middle phalanx at the proximal third level using a handheld
oscillating saw. Complete amputation was achieved as planned, with
negative margins. Primary closure of the amputation stump was
conducted in layers, and a sterile dressing was applied.
The received specimen was preserved in formalin and
comprised a finger segment measuring 4.5×2.0×1.5 cm. Examination of
the segment revealed an ulcerated, ill-defined mass at the nail
tip, measuring 0.7×0.4×0.4 cm, grossly abutting the underlying
bone. The ulcerated mass was situated 2.5 cm from the resection
margin. The diagnosis confirmed the presence of CCS in the distal
phalanx of the right index finger. The tumor, measuring 0.7 cm at
its greatest dimension, extended from the subungual soft tissue to
the underlying bone and demonstrated perineural invasion. All
resection margins, including the bone margin, were free of tumor,
indicating successful surgical removal without residual malignant
tissue. The specimen was sent for cytogenetic study (fluorescence
in situ hybridization) (14); the results were positive for EWSR1
(22q12) gene rearrangement confirming the diagnosis of CCS
(3) (Fig. 11).
The patient has since had routine surveillance
follow-up visits at the orthopedic oncology clinic as per sarcoma
protocol, with the most recent follow-up being 24 months
postoperatively. The patient initially experienced phantom and
neuropathic pain at the amputation stump, which was subsequently
resolved with multimodal analgesia. They also underwent
physiotherapy and occupational therapy during the postoperative
course. The hand function of the patient has been preserved, and
they can perform daily activities after being fitted with a
silicone prosthetic finger (Figs.
12 and 13). They have high
functional scores of 86.6 out of 100 for the Musculoskeletal Tumor
Society scoring system for the upper extremity, and 1.7 out of 100
for the Disabilities of Arm, Shoulder, and Hand score (15,16),
suggesting minimal disability.
Discussion
CCS was initially described as a ‘malignant melanoma
of soft parts’ due to histological similarities; however, CCS can
be challenging to diagnose as it resembles more common benign
lesions, leading to inappropriate management or delayed referral to
specialized facilities (17,18).
Plain radiographs and MRI are the standard-of-care initial
investigations for assessing CCS (19,20),
and biopsy is the gold standard to confirm a histopathological
diagnosis (21). In gross
appearance, CCS resembles a well-defined solid tumor that is matte
gray in color, and typically infiltrates tendons and aponeuroses.
Microscopically, findings are small compact nests with uniform
neoplastic cells divided into variably sized clusters by fibrous
septa along the tendons and aponeuroses (1,22).
Most CCSs are associated with a t(12;22)(q13-14;q12) translocation,
which corresponds to the EWSR1 (22q12) gene rearrangement (23,24),
which is the same translocation identified in the current case.
Treatment of CCS involves local control with free margin excision
of the tumor as soon as the diagnosis is established, with no
recorded benefits from chemotherapy and radiotherapy (18,25).
In addition, some studies have indicated that chemotherapy or
radiotherapy has minimal effect at stopping CCS recurrence,
particularly when there is an inadequate margin of excision
(26–28). The presence of necrosis, metastasis
and local recurrence, as well as a tumor size >5 cm, are poor
prognostic factors (18,25). The overall estimated 5- and 10-year
survival rates are ~50 and 38%, respectively, with the lung being
the most common site of metastasis (5).
For the present case report, a literature review of
all reported cases of CCS involving the fingers was conducted
through searches of the PubMed (https://pubmed.ncbi.nlm.nih.gov/), Google Scholar
(https://scholar.google.com/) and Web of
Science (https://www.webofscience.com)
databases. The search terms included ‘clear cell sarcoma’, ‘CCS’,
‘hand’ and ‘finger’. Each publication was reviewed, and six cases
of CCS of the finger were identified (Tables I and II) (29–34).
Percentages were calculated for all six patients showing the
distribution of clinical and pathological features; a dash in the
table indicates the absence of the feature, and missing information
from the Maiorana et al (33) case was classified as ‘unknown’ due
to the original full report not being available. Patients were aged
between 13 and 59 years (median age: 42 years), with three male
patients (50%) and three female patients (50%). Cases originated
from the USA (two patients), Japan (one patient), Turkey (one
patient), Iran (one patient) and Italy (one patient). Clinical
presentation involved having a painful mass or nodule (four
patients, 67%), while one patient (17%) presented with a painless
mass and one case (17%) was unknown due to incomplete reporting
(33). A history of trauma was
documented in three patients (50%), absent in two (33%) and unknown
in one (17%). Tumor size was available in five patients (83%) and
ranged from 1.0×1.0×2.0 cm to 6×8 cm; the size was not retrievable
in one patient (17%) (33).
Cytogenetic confirmation of the EWSR1 translocation was not
reported in any of the six cases; it was demonstrated only in the
patient described in the present study. Metastatic spread was
documented in four patients (67%) absent in one patient (17%) and
unknown in one case (17%). In one case, axillary node, lung and
bone metastases were reported after 6 years, with a survival of 6.5
years (29), and in another case,
axillary node and lung metastases within 1.5 years were described
(30). Lung and brain metastases
within 9 and 14 months of diagnosis, respectively, were observed in
a further case (31). Pulmonary
metastases were also reported in another report, and the patient
died after a short period (32).
One of the earliest reports could not be fully retrieved, which
accounts for missing clinical details in the analysis (33). Overall, the available literature
highlights the rarity of CCS in the finger, its wide age
distribution, and the potential for both early and delayed
metastatic spread despite initial local control (29–34).
 | Table I.Demographic and clinical features of
reported clear cell sarcoma cases of the finger. |
Table I.
Demographic and clinical features of
reported clear cell sarcoma cases of the finger.
| First author,
year | No. of
patients | Year | Age | Sex | Country | Clinical
presentation | History of
trauma | (Refs.) |
|---|
| Ozuguz, 2014 | 1 | 2014 | 58 | Female | Turkey | Painful mass | No | (32) |
| Tyler, 1980 | 1 | 1980 | 13 | Female | USA | Painful firm
mass | Yes | (29) |
| Tavakoli, 2011 | 1 | 2011 | 56 | Male | Iran | Painless mass | Yes | (34) |
| Raynor, 1979 | 1 | 1979 | 59 | Male | USA | Painful nodule | Yes | (30) |
| Maiorana, 1979 | 1 | 1990 | 28 | Female | Italy | N/A | N/A | (33) |
| Ikeda, 1996 | 1 | 1996 | 17 | Male | Japan | Painful mass | No | (31) |
| Table II.Tumor features and outcomes of
reported clear cell sarcoma cases of the finger. |
Table II.
Tumor features and outcomes of
reported clear cell sarcoma cases of the finger.
| First author,
year | Tumor size, cm | Translocation | Metastasis | Interval between
lesion appearance and metastasis, years | Recurrence | Survival | Remarks | (Refs.) |
|---|
| Ozuguz, 2014 | 6×8 | - | Lung | - | - | - | Patient died after
a short period | (32) |
| Tyler, 1980 | 1×1×2 | - | Axillary nodes,
lungs and bone | 6 | - | 6.5 years | - | (29) |
| Tavakoli, 2011 | 3×4×4 | - | - | - | - | - | - | (34) |
| Raynor, 1979 | 2.2 | - | Axillary nodes,
lungs | 1.5 | - | - | - | (30) |
| Maiorana, 1979 | N/A | N/A | N/A | N/A | N/A | N/A | - | (33) |
| Ikeda, 1996 | 1.8×1 | - | Lung, brain | 9-14 months | - | - | - | (31) |
Compared with existing case reports, the present
case shares histopathological and molecular findings, including the
presence of diffuse cytoplasmic staining for immunohistochemical
markers HMB-45 and S-100 protein (10,11),
which have been reported (32,34).
However, unlike cases presenting with poor prognostic factors
(29,32), the patient described in the current
report presented with a well-circumscribed tumor <5 cm and no
evidence of distant metastasis, suggesting a favorable prognosis.
Consistent with other cases emphasizing the challenge of early
detection due to the resemblance of the tumor to other benign
neoplasms (29,33), the present case study shows that
prompt recognition is key to achieving optimal outcomes.
It is essential for clinicians to maintain a low
threshold for considering CCS, given its slow-growing yet
aggressive nature. Early detection and intervention are still
important, as these tumors often remain small for years before
rapidly metastasizing. The initial misdiagnosis as a glomus tumor
highlights the risk of unplanned excisions in digital lesions,
which can compromise margins in the amputation and general
outcomes, highlighting the need for early biopsy and molecular
confirmation in such presentations. The patient described in the
current study is currently being followed up once every 3 months,
and is now 2 years post-amputation, has had no recurrence and is
doing well.
Ultimately, a high index of suspicion and timely
diagnosis can improve outcomes, but the inherent biology of CCS
poses notable challenges, even with appropriate management. Given
the small number of reported cases, it is difficult to establish
definitive treatment protocols for CCS, particularly considering
the limited number of pediatric cases. However, the fact that
metastasis often occurs long after the appearance of the primary
lesion suggests that vigilant long-term monitoring is necessary.
Additionally, the present findings support the notion that
amputation remains an effective treatment even in the case of
recurrence, emphasizing the potential value of early, aggressive
surgical intervention. These insights may help to guide future
treatment decisions, especially in the absence of dissemination,
and could contribute to diagnostic guidelines for CCS in pediatric
populations.
In conclusion, to the best of our knowledge, only
six cases of CCS presenting in the finger have been reported in the
literature to date. The current case represents the second
pediatric case reported and the only one with confirmed EWSR1
translocation, further contributing to the limited literature. This
highlights the rarity of CCS presentation in the hand, and
emphasizes the importance of maintaining a high index of suspicion
to identify, accurately diagnose, avoid mistreatment and prevent
delays in referral to specialized centers. In addition, including
CCS in the differential diagnosis of atypical digital lesions is
needed. Multidisciplinary management in a specialized oncology
center is crucial to optimize oncological and functional outcomes.
Finally, future research should focus on exploring genetic markers
and prognostic factors, and developing optimal management
strategies for CCS, especially in rare presentations, to improve
diagnostic accuracy and treatment outcomes.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study are included
in the figures and/or tables of this article.
Authors' contributions
BA and AAla conceptualized the study. HK performed
the histopathology evaluation of the resected tumor and wrote the
pathology section of this case, including the histopathology
pictures. EN was involved in the radiological evaluation of the
case, including interpretation of imaging with clinicoradiological
correlation, and contributed to the supervision of the project. ABD
and KM prepared the original draft of the manuscript. AAla and SA
reviewed and edited the manuscript. AAla and EN supervised the
work. SA was responsible for table preparation and assisted in data
analysis. KM contributed to figure acquirement and modifications.
NA conducted the literature review and contributed to data
interpretation. ABD and BA managed project administration. AAlm and
AAlh provided resources. All authors contributed to writing the
manuscript and approved the final version. AAla and BA confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication:
Written informed consent was obtained from the
patient's guardian for the publication of this case
Competing interests
The authors declare that they have no competing
interests
Use of artificial intelligence tools
During the preparation of this work, an AI tool
(ChatGPT; OpenAI) was used to improve the readability and language
of the manuscript, and subsequently, the authors revised and edited
the content produced by the AI tools as necessary, taking full
responsibility for the ultimate content of the present
manuscript
References
|
1
|
Enzinger FM: Clear-cell sarcoma of tendons
and aponeuroses. An analysis of 21 cases. Cancer. 18:1163–1174.
1965. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Dim DC, Cooley LD and Miranda RN: Clear
cell sarcoma of tendons and aponeuroses: A review. Arch Pathol Lab
Med. 131:152–156. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Wang WL, Mayordomo E, Zhang W, Hernandez
VS, Tuvin D, Garcia L, Lev DC, Lazar AJ and López-Terrada D:
Detection and characterization of EWSR1/ATF1 and EWSR1/CREB1
chimeric transcripts in clear cell sarcoma (melanoma of soft
parts). Mod Pathol. 22:1201–1209. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Pavlidis NA, Fisher C and Wiltshaw E:
Clear-cell sarcoma of tendons and aponeuroses: A clinicopathologic
study. Presentation of six additional cases with review of the
literature. Cancer. 54:1412–1417. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gonzaga MI, Grant L, Curtin C, Gootee J,
Silberstein P and Voth E: The epidemiology and survivorship of
clear cell sarcoma: A national cancer database (NCDB) review. J
Cancer Res Clin Oncol. 144:1711–1716. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Abdollahi A, Khatami F and Tavangar SM:
Clear cell sarcoma: A case report and review of literature. Int J
Hematol Oncol Stem Cell Res. 12:65–68. 2018.PubMed/NCBI
|
|
7
|
Murugan P, Basu D, Kumar S and Jagadish S:
Clear cell sarcoma of the soft parts arising in the rectus
abdominis in a child-aspiration cytology of a rare case.
Cytojournal. 4:152007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kazakos CJ, Galanis VG, Giatromanolaki A,
Verettas DA and Sivridis E: Clear cell sarcoma of the scapula. A
case report and review of the literature. World J Surg Oncol.
4:482006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Steger GG, Wrba F, Mader R, Schlappack O,
Dittrich C and Rainer H: Complete remission of metastasised clear
cell sarcoma of tendons and aponeuroses. Eur J Cancer Clin Oncol.
27:254–256. 1991. View Article : Google Scholar
|
|
10
|
Kim SW, Roh J and Park CS:
Immunohistochemistry for pathologists: Protocols, pitfalls, and
tips. J Pathol Transl Med. 50:411–418. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
McCampbell AS, Raghunathan V, Tom-Moy M,
Workman RK, Haven R, Ben-Dor A, Rasmussen OF, Jacobsen L, Lindberg
M, Yamada NA and Schembri C: Tissue thickness effects on
immunohistochemical staining intensity of markers of cancer. Appl
Immunohistochem Mol Morphol. 27:345–355. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Lemes CC, Germano da Silva A, Ribeiro DA
and Malinverni ACM: Challenges and solutions in FISH for
formalin-fixed paraffin-embedded tissue: A scoping review. Microsc
Res Tech. 88:270–278. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Amin MB, Greene FL, Edge SB, Compton CC,
Gershenwald JE, Brookland RK, Meyer L, Gress DM, Byrd DR and
Winchester DP: The eighth edition AJCC cancer staging manual:
Continuing to build a bridge from a population-based to a more
‘personalized’ approach to cancer staging. CA Cancer J Clin.
67:93–99. 2017.PubMed/NCBI
|
|
14
|
Murthy S, Gundimeda S, Challa S, Manjula
V, Fonseca D, Rao VB, Rajappa SJ, N Raju KVV and Rao TS: FISH for
EWSR1 in Ewing's sarcoma family of tumors: Experience from a
tertiary care cancer center. Indian J Pathol Microbiol. 64:96–101.
2021. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Enneking WF, Dunham W, Gebhardt MC,
Malawar M and Pritchard DJ: A system for the functional evaluation
of reconstructive procedures after surgical treatment of tumors of
the musculoskeletal system. Clin Orthop Relat Res. 241–246.
1993.PubMed/NCBI
|
|
16
|
Hudak PL, Amadio PC and Bombardier C:
Development of an upper extremity outcome measure: The DASH
(disabilities of the arm, shoulder, and head) [corrected]. Am J Ind
Med. 29:602–608. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Malchau SS, Hayden J, Hornicek F and
Mankin HJ: Clear cell sarcoma of soft tissues. J Surg Oncol.
95:519–522. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Jones RL, Constantinidou A, Thway K,
Ashley S, Scurr M, Al-Muderis O, Fisher C, Antonescu CR, D'Adamo
DR, Keohan ML, et al: Chemotherapy in clear cell sarcoma. Med
Oncol. 28:859–863. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Expert Panel on Musculoskeletal Imaging, .
Bestic JM, Wessell DE, Beaman FD, Cassidy RC, Czuczman GJ,
Demertzis JL, Lenchik L, Motamedi K, Pierce JL, et al: ACR
appropriateness criteria® primary bone tumors. J Am Coll
Radiol. 17:S226–S238. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Caracciolo JT and Letson GD: Radiologic
approach to bone and soft tissue sarcomas. Surg Clin North Am.
96:963–976. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ibrahim RM, Steenstrup Jensen S and Juel
J: Clear cell sarcoma-A review. J Orthop. 15:963–966. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Kindblom LG, Lodding P and Angervall L:
Clear-cell sarcoma of tendons and aponeuroses. An
immunohistochemical and electron microscopic analysis indicating
neural crest origin. Virchows Arch A Pathol Anat Histopathol.
401:109–128. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Segal NH, Pavlidis P, Noble WS, Antonescu
CR, Viale A, Wesley UV, Busam K, Gallardo H, DeSantis D, Brennan
MF, et al: Classification of clear-cell sarcoma as a subtype of
melanoma by genomic profiling. J Clin Oncol. 21:1775–1781. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Zucman J, Delattre O, Desmaze C, Epstein
AL, Stenman G, Speleman F, Fletchers CD, Aurias A and Thomas G: EWS
and ATF-1 gene fusion induced by t(12;22) translocation in
malignant melanoma of soft parts. Nat Genet. 4:341–345. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Bianchi G, Charoenlap C, Cocchi S, Rani N,
Campagnoni S, Righi A, Frisoni T and Donati DM: Clear cell sarcoma
of soft tissue: A retrospective review and analysis of 31 cases
treated at Istituto Ortopedico Rizzoli. Eur J Surg Oncol.
40:505–510. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Clark MA, Johnson MB, Thway K, Fisher C,
Thomas JM and Hayes AJ: Clear cell sarcoma (melanoma of soft
parts): The Royal Marsden Hospital experience. Eur J Surg Oncol.
34:800–804. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pradhan A, Cheung YC, Grimer RJ, Peake D,
Al-Muderis OA, Thomas JM and Smith M: Soft-tissue sarcomas of the
hand: Oncological outcome and prognostic factors. J Bone Joint Surg
Br. 90:209–214. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Finley JW, Hanypsiak B, Mcgrath B,
Kraybill W and Gibbs JF: Clear cell sarcoma: The Roswell Park
experience. J Surg Oncol. 77:16–20. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Tyler G, Wirman J and Neale HW: Melanin
containing clear cell sarcoma in a fingertip. Case report and
review of the literature. Hand. 12:308–315. 1980. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Raynor AC, Vargas-Cortes F, Alexander RW
and Bingham HG: Clear-cell sarcoma with melanin pigment: A possible
soft-tissue variant of malignant melanoma. Case report. J Bone
Joint Surg Am. 61:276–280. 1979. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ikeda E and Umeda T: A Case of Clear Cell
Sarcoma -A Case of Clear Cell Sarcoma in the Right Finger. Skin
Cancer. 11:72–75. 1996.(In Japanese). View Article : Google Scholar
|
|
32
|
Ozuguz P, Kocak M, Atasoy P, Vargel I and
Cavusoglu T: Clear cell sarcoma. Indian Dermatol Online J.
5:488–490. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Maiorana A, Bagni A, Sannicola C and Barca
F: Clear cell sarcoma of the hand. Description of a case.
Pathologica. 82:95–100. 1990.(In Italian). PubMed/NCBI
|
|
34
|
Tavakoli R, Sheibani K and Khayatkhoei M:
Clear cell sarcoma of the hand: A case of malignant melanoma of
soft parts. Iranian J Blood Cancer. 4:25–30. 2011.
|