Introduction
Lung cancer is the leading cause of death due to
cancer in China, accounting for 828,000 new cases and 657,000
deaths annually. Small cell lung cancer (SCLC) is highly malignant
and accounts for 15–20% of all lung cancer cases (1–3).
Overall, 60–70% of patients with SCLC are in the advanced stages at
diagnosis and have already lost the opportunity for radical surgery
(4). The standard first-line
doublet chemotherapy (etoposide plus cisplatin) results in a
relatively dismal overall survival (OS) time of only 6.5–10.3
months in advanced extensive-stage SCLC (ES-SCLC), with a high rate
of grade >3 adverse events (AEs) (1,4–9). As
first-line treatment, immune checkpoint inhibitors (ICIs) plus
chemotherapy have increased the OS time to 12–13 months. However,
progressive disease may occur in the short term after first-line
immunotherapy, with a progression-free survival (PFS) time of 4–5
months (4,10,11).
When first-line treatment for patients with ES-SCLC fails,
second-line chemotherapy is generally used, but the efficacy is
often limited (4,12). Although topotecan and lurbinectedin
provide treatment options, the OS time of patients with ES-SCLC
receiving second-line treatment remains poor at only 6–9 months
(4,13,14).
Therefore, more effective second-line treatment options are needed
to improve the prognosis of patients with ES-SCLC who failed
first-line standard treatment.
Notably, ICI retreatment is an emerging concept for
patients who have received first-line immunotherapy (15). In the context of the present study,
‘immunotherapy retreatment’ specifically refers to the
administration of a second-line ICI with a distinct mechanism of
action [such as switching from a programmed cell death 1 ligand 1
(PD-L1) inhibitor to a programmed cell death protein 1 (PD-1)
inhibitor] after progression on first-line ICI therapy. Preclinical
studies have suggested that the resistance to PD-L1 inhibitors
could be related to the loss of JAK1/2 function or the
downregulation of interferon-γ, and that retreatment with a
second-line PD-1 inhibitor might circumvent the acquired resistance
(16,17). To elaborate, ICIs exert their
antitumor effects by blocking inhibitory pathways that suppress
T-cell activity (18,19). PD-1 is an inhibitory receptor
expressed on activated T cells, while its primary ligand, PD-L1, is
often expressed on tumor cells or other cells within the tumor
microenvironment (20,21). PD-1 inhibitors (such as serplulimab)
directly target the PD-1 receptor on T cells, preventing its
interaction with both PD-L1 and PD-L2 (22). By contrast, PD-L1 inhibitors (such
as atezolizumab or durvalumab) specifically block PD-L1 on tumor
cells, preventing its binding to PD-1 (23). Although both strategies aim to
disinhibit T-cell function, their distinct binding targets offer a
mechanistic rationale for sequential therapy (16,17). A
case report suggested that PD-1 inhibitors had good therapeutic
effects in a patient with hepatocellular carcinoma who progressed
after PD-L1 inhibitors (24). A
retrospective study showed that patients with SCLC progressing
after first-line immunotherapy could benefit from second-line
immunotherapy (>6 weeks) and achieve median PFS and OS times of
4.8 and 17.4 months, respectively (25). Hence, ICI retreatment with PD-1
inhibitors might be a promising treatment strategy for patients
with ES-SCLC who have experienced failed standard first-line
immunotherapy with PD-L1 inhibitors (such as atezolizumab or
durvalumab).
Serplulimab is a humanized anti-PD-1 IgG4 monoclonal
antibody that can enhance the functional activity of human T cells
(26). The ASTRUM-005 study
demonstrated that additional serplulimab significantly prolonged
the PFS and OS times of patients with ES-SCLC when compared with
chemotherapy alone (27). A network
meta-analysis also suggested the advantage of first-line
serplulimab treatment for ES-SCLC over other regimens (28). Nevertheless, the effectiveness of
second-line serplulimab treatment for ES-SCLC, especially after the
failure of first-line immunotherapy, remains unknown.
Therefore, the objective of the present real-world
retrospective cohort study was to examine the effectiveness of
immunotherapy retreatment with serplulimab vs. chemotherapy in
patients with ES-SCLC who were previously treated with first-line
immunotherapy. The study responds to the urgent need for an
effective second-line treatment for ES-SCLC, considering the
potential of ICI retreatment.
Patients and methods
Study design and patients
In the present real-world retrospective cohort
study, data was collected from patients with ES-SCLC who did not
respond to first-line immunotherapy and were treated at Shandong
Cancer Hospital and Institute (Jinan, China) between January 31,
2019, and May 1, 2023.
The inclusion criteria were as follows: i) ≥18 years
of age; ii) histologically or cytologically confirmed stage IV
ES-SCLC (4); iii) previously
treated with standard first-line immunotherapy (such as
atezolizumab or durvalumab) combined with chemotherapy; and iv)
second-line treatment with serplulimab or chemotherapy. Consistent
with the aforementioned definition, patients in the serplulimab
group received immunotherapy retreatment by switching from a
first-line PD-L1 inhibitor to the PD-1 inhibitor serplulimab.
Patients with incomplete data on effectiveness or who died within 2
months from the start of second-line treatment were excluded. The
cut-off of 2 months was selected as it represented the median time
to response for immunotherapy and the first routine response
evaluation, which was conducted 2 months after the initial dose of
treatment (29).
Treatment
The patients were grouped into the serplulimab and
chemotherapy groups according to the second-line treatment they
received. The routine serplulimab treatment was an intravenous
infusion of 4.5 mg/kg of serplulimab every 3 weeks. The
chemotherapy regimens were chosen by the physicians based on the
specific situation of the patients. Other treatment options, such
as anti-angiogenesis drugs, radiotherapy and combining serplulimab
with chemotherapy, were all at the discretion of the
physicians.
Data collection
The baseline characteristics of the patients were
collected from their medical records, including demographic
characteristics at the diagnosis of advanced ES-SCLC, the
first-line immunotherapy regimen, the PFS time for the first-line
immunotherapy and the reasons for discontinuation of first-line
immunotherapy. The reasons for discontinuing first-line
immunotherapy were divided into AEs and primary and secondary
resistance (30).
Outcome
The outcomes of the present study included the PFS
time, objective response rate (ORR) and disease control rate (DCR)
of the second-line treatment. PFS time was calculated from the
start of second-line treatment to progressive disease or death from
any cause, whichever occurred first. OS time was measured from the
start of second-line treatment to death from any cause. ORR was the
proportion of patients with a complete response (CR) or partial
response (PR), and DCR was the proportion of patients with a CR, PR
or stable disease. The response to treatment was evaluated
according to the Response Evaluation Criteria in Solid Tumors
version 1.1 criteria (31). The
metastatic sites of the patients who progressed after second-line
treatment were recorded.
A combination of AEs, immune-related AEs (irAEs) and
irAEs requiring systemic glucocorticoid treatment were collected.
The severity of AEs was graded according to the National Cancer
Institute-Common Terminology Criteria for Adverse Events version
5.0 (32). The second-line
treatment pattern was recorded, including a combination of other
systemic therapy and radiotherapy.
Statistical analysis
The continuous data were tested for normal
distribution using the Kolmogorov-Smirnov test. Normally
distributed continuous variables are presented as the mean ±
standard deviation and were analyzed using unpaired Student's
t-test; otherwise, the data are presented as the median and
interquartile ranges (IQR) and were analyzed using the Mann-Whitney
U-test. The categorical data are represented as n (%), and the
groups were compared using the χ2 test when the expected
frequency in each category was ≥5; otherwise, Fisher's exact test
was used. The median PFS and OS, and the 95% confidence interval
(CI), were evaluated using the Kaplan-Meier method. The comparison
of PFS and OS between groups was performed using the log-rank test,
and the hazard ratio (HR) was calculated using Cox regression. The
multivariable Cox regression model was used to analyze the factors
associated with the PFS and OS of the second-line treatment. The
variables with P<0.10 in the univariable analysis were included
in the multivariable analysis. Two-sided P<0.05 was considered
to indicate a statistically significant difference. The statistical
analysis software was R 4.2.3 (The R Project for Statistical
Computing; www.r-project.org).
Results
Characteristics of the
participants
The present study included 160 patients with ES-SCLC
who failed first-line immunotherapy, and included 67 treated with
serplulimab and 93 treated with chemotherapy as second-line
treatment. Most patients (n=148; 92.5%) discontinued first-line
immunotherapy due to secondary resistance, while primary resistance
and adverse events were the reasons in 5 (3.1%) and 7 (4.4%)
patients, respectively.
Table I shows that
age, sex distribution, Karnofsky performance status scores and
Eastern Cooperative Oncology Group Performance Status scores were
similar between the two groups (all P>0.05) (33,34).
Compared with the chemotherapy group, the serplulimab showed a
higher proportion of smokers (53.7 vs. 28.0%; P=0.001) and a lower
frequency of radiotherapy in the first-line treatment (38.8 vs.
64.5%; P=0.001). Notably, the first-line immunotherapy regimen
(P=0.391), reasons for discontinuation of first-line immunotherapy
(P>0.999) and median PFS of the first-line treatment (8.40 vs.
8.82 months; P=0.531) were similar between the two groups.
 | Table I.Baseline characteristics. |
Table I.
Baseline characteristics.
| Patient
characteristics | Total (n=160) | Serplulimab
(n=67) | Chemotherapy
(n=93) | P-value |
|---|
| Mean age ± SD,
years | 60.98±8.56 | 60.10±8.65 | 61.61±8.49 | 0.273 |
| Sex, n (%) |
|
|
| 0.195 |
|
Male | 125 (78.1) | 49 (73.1) | 76 (81.7) |
|
|
Female | 35 (21.9) | 18 (26.9) | 17 (18.3) |
|
| KPS score, n
(%) |
|
|
| 0.058 |
| 70 | 7 (4.4) | 0 (0.0) | 7 (7.5) |
|
| 80 | 79 (49.4) | 34 (50.7) | 45 (48.4) |
|
| 90 | 73 (45.6) | 32 (47.8) | 41 (44.1) |
|
|
100 | 1 (0.6) | 1 (1.5) | 0 (0.0) |
|
| ECOG PS, n (%) |
|
|
| 0.248 |
| 0 | 109 (68.1) | 49 (73.1) | 60 (64.5) |
|
| 1 | 51 (31.9) | 18 (26.9) | 33 (35.5) |
|
| Smoking history, n
(%) |
|
|
| 0.001a |
|
Smoking | 62 (38.8) | 36 (53.7) | 26 (28.0) |
|
| No
smoking | 98 (61.3) | 31 (46.3) | 67 (72.0) |
|
| First-line
immunotherapy regimen, n (%) |
|
|
| 0.391 |
|
Durvalumab | 94 (58.8) | 42 (62.7) | 52 (55.9) |
|
|
Atezolizumab | 66 (41.3) | 25 (37.3) | 41 (44.1) |
|
| Combined
chemotherapy regimen with first-line immunotherapy, n (%) |
|
|
| 0.680 |
|
Etoposide plus cisplatin | 115 (71.9) | 47 (70.1) | 68 (73.1) |
|
|
Etoposide plus
carboplatin | 45 (28.1) | 20 (29.9) | 25 (26.9) |
|
| Received
radiotherapy in first-line treatment, n (%) | 86 (53.8) | 26 (38.8) | 60 (64.5) | 0.001a |
| Timing of
radiotherapy, n (%)b |
|
|
|
|
| Before
systemic treatment | 16 (10.0) | 10 (14.9) | 6 (6.5) | 0.078 |
| After
systemic treatment | 20 (12.5) | 8 (11.9) | 12 (12.9) | 0.856 |
|
Synchronous | 50 (31.3) | 8 (11.9) | 42 (45.2) |
<0.001a |
| PFS of first-line
treatmentc | 8.62 | 8.40 | 8.82 | 0.531d |
|
| (7.87–9.33) | (7.56–9.45) | (7.80–9.80) |
|
| Reasons for
discontinuation of first-line treatment, n (%) |
|
|
| >0.999 |
|
Secondary resistance | 148 (92.5) | 62 (92.5) | 86 (92.5) |
|
| Primary
resistance | 5 (3.1) | 2 (3.0) | 3 (3.2) |
|
|
AEs | 7 (4.4) | 3 (4.5) | 4 (4.3) |
|
| Second-line
treatment pattern, n (%) |
|
|
|
|
| Serplulimab
group |
|
|
|
|
|
Monotherapy | - | 4 (6.0) | - |
|
|
Combined with
chemotherapy | - | 35 (52.2) | - |
|
|
Combined with anlotinib and
chemotherapy | - | 20 (29.9) | - |
|
|
Combined with anlotinib | - | 8 (11.9) | - |
|
| Chemotherapy group,
n (%) |
|
|
|
|
|
Monotherapy | - | - | 69 (74.2) |
|
|
Combined with anlotinib | - | - | 24 (25.8) |
|
Treatment patterns
In the serplulimab group, serplulimab was
administered as monotherapy in 4 patients (6.0%), combined with
chemotherapy in 35 patients (52.2%), combined with
anti-angiogenesis drugs plus chemotherapy in 20 patients (29.9%) or
combined with anti-angiogenesis drugs in 8 patients (11.9%). In the
chemotherapy group, chemotherapy was administered as monotherapy in
the majority of the patients (n=69; 74.2%) and combined with
anti-angiogenesis drugs in 24 patients (25.8%) (Table SI).
In the serplulimab group, the combined chemotherapy
regimens involved etoposide plus cisplatin (n=31; 46.3%),
nab-paclitaxel (n=16; 23.9%) and etoposide plus carboplatin (n=8;
11.9%). Similarly, in the chemotherapy group, the most commonly
used regimen was also etoposide plus cisplatin (n=55; 59.1%),
followed by nab-paclitaxel (n=25; 26.9%), and etoposide plus
carboplatin (n=13; 14.0%). The anti-angiogenesis drugs in this
study were all anlotinib (Table
SI).
Compared with the chemotherapy group, the
serplulimab group showed significantly higher use of
anti-angiogenesis drugs (41.8 vs. 25.8%; P=0.033) and radiotherapy
(16.4 vs. 6.5%; P=0.044). There were no differences in the timing
of radiotherapy between the two groups (synchronous: 27.3 vs.
33.3%; P>0.999). Specifically, 4 and 3 patients received
prophylactic cranial irradiation as part of their treatment regimen
in the two groups, respectively (Table
SI).
Effectiveness
Table II presents
the responses to treatments. There were no statistical differences
in ORR (53.7 vs. 40.9%; P=0.107) and DCR (100 vs. 100%; P=1.000)
between the two groups. The median follow-up time was 21.28 months
(range, 5.44–34.62 months) in the overall population, 22.7 months
(range, 7.45–34.40 months) in the serplulimab group and 20.66
months (range, 5.44–34.62 months) in the chemotherapy group (data
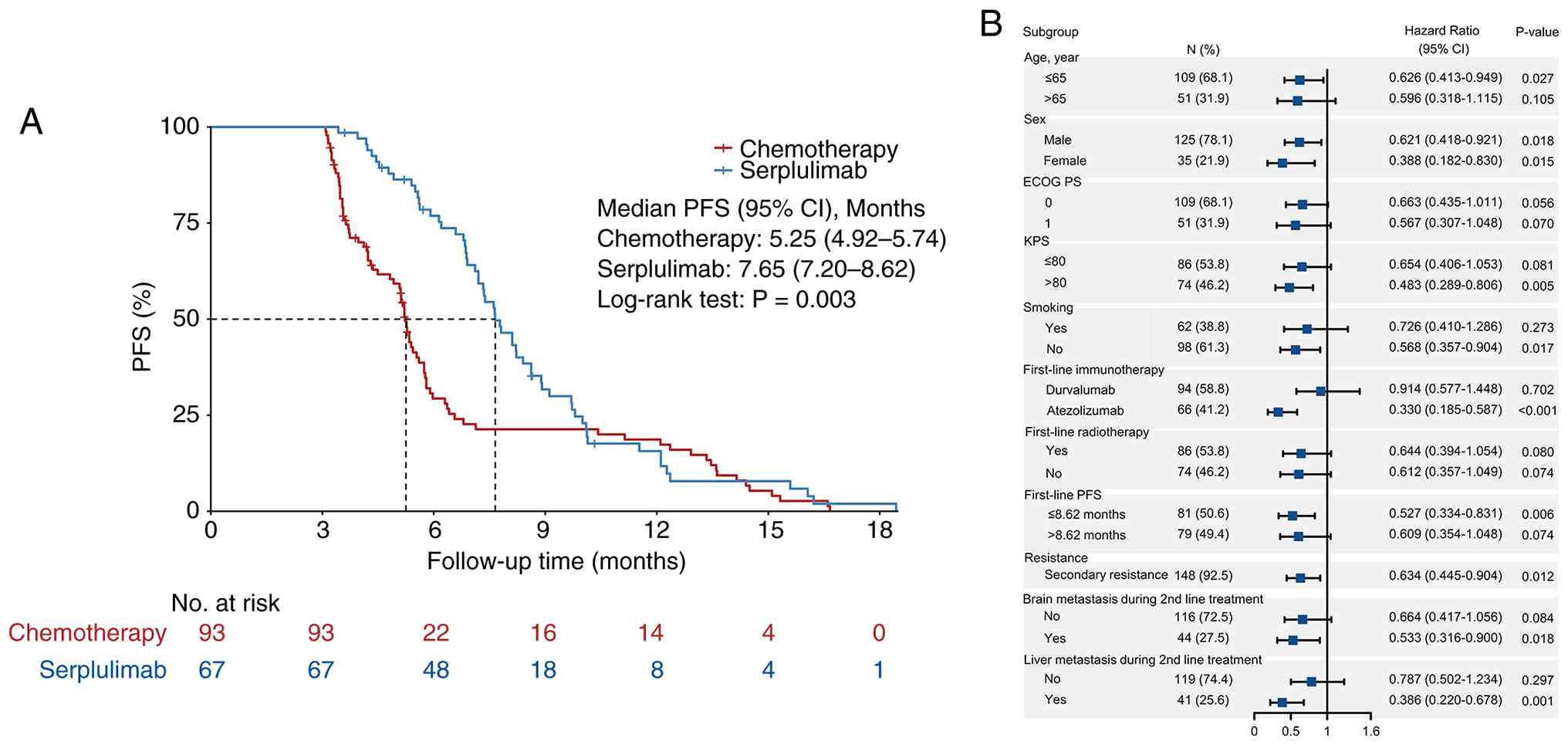
not shown). As shown in Fig. 1A,
the median PFS time was significantly longer with serplulimab (7.65
months; 95% CI, 7.20–8.62) compared with chemotherapy (5.25 months;
95% CI, 4.92–5.74) (HR, 0.601; 95% CI, 0.426–0.848; P=0.003). As
shown in Fig. 2A, the serplulimab
group also had a longer median OS time of 15.56 months (95% CI,
14.13–17.12) than the chemotherapy group (13.48 months; 95% CI,
12.84–14.40) (HR, 0.680; 95% CI, 0.478–0.966; P=0.031).
| Table II.Tumor response. |
Table II.
Tumor response.
| Best response, n
(%) | Total (n=160) | Serplulimab
(n=67) | Chemotherapy
(n=93) | P-value |
|---|
| CR | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| PR | 74 (46.3) | 36 (53.7) | 38 (40.9) | - |
| SD | 86 (53.8) | 31 (46.3) | 55 (59.1) | - |
| PD | 0 (0.0) | 0 (0.0) | 0 (0.0) | - |
| ORR (CR + PR) | 74 (46.3) | 36 (53.7) | 38 (40.9) | 0.107 |
| DCR (CR + PR +
SD) | 160 (100.0) | 67 (100.0) | 93 (100.0) | 1.000 |
After second-line treatment, the proportion of
patients developing metastases was comparable in the serplulimab
group to that in the chemotherapy group (67.1 vs. 73.2%; P=0.415).
There were no significant differences in the development of the
brain (41.8 vs. 45.2%; P=0.672), liver (38.8 vs. 36.6%; P=0.772),
lung (13.4 vs. 17.2%; P=0.517), or adrenal gland (10.4 vs. 9.7%;
P=0.873) metastases, but the serplulimab group showed a lower
frequency of bone metastases (25.4 vs. 50.5%; P=0.001) (Fig. 3).
Subgroup analysis and risk factor of
PFS and OS
Similar to the results in the total population, in
the patients with secondary resistance to first-line immunotherapy,
serplulimab achieved significantly longer median PFS (7.78 vs. 5.28
months; HR, 0.634; 95% CI, 0.445–0.904; P=0.012; Fig. 1B) and OS (15.58 vs. 13.53 months;
HR, 0.691; 95% CI, 0.480–0.994; P=0.046; Fig. 2B) times compared with chemotherapy.
In other subgroup analyses for PFS, (Fig. 1B), compared with the chemotherapy
group, serplulimab provided significantly superior benefits in
patients aged ≤65 years (P=0.027), males (P=0.018), females
(P=0.015), non-smokers (P=0.017), those who received first-line
atezolizumab (P<0.001), patients with secondary resistance
(P=0.012), and those with a first-line PFS ≤8.62 months (P=0.006).
Notably, serplulimab also demonstrated a significant PFS advantage
over chemotherapy in patients with brain metastases (P=0.018) or
liver metastases (P=0.001) during second-line treatment. For other
subgroups, including patients aged >65 years, those with ECOG PS
0 or 1, and those with first-line radiotherapy, serplulimab showed
an improved PFS, although these results did not reach statistical
significance compared with the chemotherapy group (all P>0.05).
For OS (Fig. 2B), serplulimab
achieved significantly better outcomes than chemotherapy in male
patients (P=0.014), smokers (P=0.020), patients with ECOG PS 0
(P=0.038) and those with secondary resistance (P=0.046). Similarly,
compared with chemotherapy, serplulimab significantly prolonged OS
in patients with a first-line PFS ≤8.62 months (P <0.001), as
well as in those with brain metastases (P=0.023) or liver
metastases (P=0.014) during second-line treatment. In the remaining
subgroups, serplulimab showed a trend of OS benefit, but the
differences compared with the chemotherapy group were not
statistically significant (all P>0.05).
In addition, the different second-line treatment
patterns among the serplulimab and chemotherapy groups separately
did not impact the PFS (log-rank P=0.358 and 0.480, respectively;
Fig. S1A and B) or the OS
(log-rank P=0.222 and 0.793, respectively; Fig. S2A and B). In the subgroup analysis
(Fig. S1C), serplulimab combined
with anti-angiogenesis treatment showed a longer median PFS time
(8.21 months; 95% CI, 6.80–9.72) compared with serplulimab alone or
chemotherapy with/without anti-angiogenesis drugs (P=0.021).
Serplulimab combined with radiotherapy was also associated with a
longer median PFS time (8.89 months; 95% CI, 7.2-NA) compared with
serplulimab alone or chemotherapy with/without radiotherapy
(P=0.004) (Fig. S1D). However,
these subgroups showed no statistically significant difference in
terms of OS (log-rank P=0.127 and 0.087, respectively; Fig. S2C and D).
Tables III and
IV show the univariable and
multivariable analysis of the factors associated with the PFS and
OS, respectively. In the multivariable analysis, second-line
serplulimab was independently associated with a higher PFS time
after adjusting for other confounding factors (HR, 0.572; 95% CI,
0.395–0.828; P=0.003). Additionally, a longer PFS time after
first-line treatment was identified as a significant independent
predictor for better second-line PFS (HR, 0.921; 95% CI,
0.867–0.978; P=0.007). Similarly, second-line serplulimab was also
independently associated with a higher OS time (HR, 0.158; 95% CI,
0.096–0.261; P<0.001). Furthermore, the reason for
discontinuation of first-line treatment was significantly
associated with OS; specifically, patients with primary resistance
to first-line therapy exhibited a significantly higher risk of
death compared to those without (HR, 4.338; 95% CI, 1.422–13.232;
P=0.010).
| Table III.Risk factors of PFS. |
Table III.
Risk factors of PFS.
|
| Univariable
analysis | Multivariable
analysis |
|---|
|
|
|
|
|---|
| Patient
characteristics | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age | 1.003
(0.983–1.023) | 0.795 |
|
|
| Sex |
|
|
|
|
|
Male | Reference |
|
|
|
|
Female | 1.173
(0.784–1.753) | 0.438 |
|
|
| KPS score |
|
|
|
|
|
≤80 | Reference |
|
|
|
|
>80 | 1.287
(0.919–1.801) | 0.142 |
|
|
| ECOG PS |
|
|
|
|
| 0 | Reference |
|
|
|
| 1 | 1.288
(0.903–1.837) | 0.162 |
|
|
| Smoking
history |
|
|
|
|
| No
smoking | Reference |
|
|
|
|
Smoking | 0.827
(0.587–1.167) | 0.280 |
|
|
| First-line
immunotherapy regimen |
|
|
|
|
|
Durvalumab | Reference |
|
|
|
|
Atezolizumab | 1.172
(0.834–1.646) | 0.361 |
|
|
| Radiotherapy in
first-line treatment |
|
|
|
|
| No | Reference |
| Reference |
|
|
Yes | 1.361
(0.973–1.903) | 0.072 | 1.090
(0.762–1.560) | 0.638 |
| Reasons for
discontinuation of first-line treatment |
|
|
|
|
|
Secondary resistance | Reference |
| Reference |
|
| Primary
resistance | 3.210
(1.298–7.937) | 0.012 | 2.387
(0.901–6.320) | 0.080 |
|
AEs | 1.424
(0.523–3.878) | 0.489 | 2.128
(0.754–6.000) | 0.153 |
| Second-line
treatment |
|
|
|
|
|
Chemotherapy | Reference |
| Reference |
|
|
Serplulimab | 0.601
(0.426–0.848) | 0.003 | 0.572
(0.395–0.828) | 0.003 |
| Second-line
treatment with anti-angiogenesis drugs |
|
|
|
|
| No | Reference |
|
|
|
|
Yes | 0.921
(0.648–1.309) | 0.646 |
|
|
| Second-line
treatment with chemotherapy |
|
|
|
|
| No | Reference |
|
|
|
|
Yes | 1.101
(0.661–1.835) | 0.711 |
|
|
| PFS of first-line
treatment | 0.922
(0.872–0.974) | 0.004 | 0.921
(0.867–0.978) | 0.007 |
| PFS of first-line
treatment, months |
|
|
|
|
|
≤8.62 | Reference |
|
|
|
|
>8.62 | 0.746
(0.530–1.051) | 0.094 |
|
|
| Brain metastasis
during second-line treatment |
|
|
|
|
| No | Reference |
| Reference |
|
|
Yes | 1.399
(1.001–1.956) | 0.050 | 1.350
(0.962–1.895) | 0.083 |
| Liver metastasis
during second-line treatment |
|
|
|
|
| No | Reference |
|
|
|
|
Yes | 1.318
(0.937–1.854) | 0.113 |
|
|
| Table IV.Risk factors of overall survival. |
Table IV.
Risk factors of overall survival.
|
| Univariable
analysis | Multivariable
analysis |
|---|
|
|
|
|
|---|
| Patient
characteristics | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age | 1.014
(0.994–1.034) | 0.184 |
|
|
| Sex |
|
|
|
|
|
Male | Reference |
|
|
|
|
Female | 0.944
(0.624–1.427) | 0.784 |
|
|
| KPS score |
|
|
|
|
|
≤80 | Reference |
|
|
|
|
>80 | 0.938
(0.664–1.324) | 0.715 |
|
|
| ECOG PS |
|
|
|
|
| 0 | Reference |
|
|
|
| 1 | 1.282
(0.891–1.845) | 0.181 |
|
|
| Smoking
history |
|
|
|
|
| No
smoking | Reference |
|
|
|
|
Smoking | 0.824
(0.578–1.175) | 0.285 |
|
|
| First-line
immunotherapy regimen |
|
|
|
|
|
Durvalumab | Reference |
|
|
|
|
Atezolizumab | 1.108
(0.783–1.569) | 0.561 |
|
|
| Radiotherapy in
first-line treatment |
|
|
|
|
| No | Reference |
| Reference |
|
|
Yes | 1.448
(1.025–2.047) | 0.036 | 1.229
(0.813–1.857) | 0.328 |
| Reasons for
discontinuation of first-line treatment |
|
|
|
|
|
Secondary resistance | Reference |
| Reference |
|
| Primary
resistance | 24.237
(8.987–65.360) | <0.001 | 4.338
(1.422–13.232) | 0.010 |
|
AEs | 0.503
(0.185–1.366) | 0.178 | 2.282
(0.806–6.462) | 0.120 |
| Second-line
treatment |
|
|
|
|
|
Chemotherapy | Reference |
| Reference |
|
|
Serplulimab | 0.680
(0.478–0.966) | 0.031 | 0.158
(0.096–0.261) | <0.001 |
| Second-line
treatment with anti-angiogenesis drugs |
|
|
|
|
| No | Reference |
|
|
|
|
Yes | 0.851
(0.591–1.227) | 0.388 |
|
|
| Second-line
treatment with chemotherapy |
|
|
|
|
| No | Reference |
|
|
|
|
Yes | 1.195
(0.708–2.017) | 0.505 |
|
|
| PFS of first-line
treatment | 0.619
(0.572–0.670) | <0.001 | 0.520
(0.472–0.574) | <0.001 |
| PFS of first-line
treatment, months |
|
|
|
|
|
≤8.62 | Reference |
|
|
|
|
>8.62 | 0.184
(0.125–0.269) | <0.001 |
|
|
| Brain metastasis
during second-line treatment |
|
|
|
|
| No | Reference |
|
|
|
|
Yes | 1.265
(0.897–1.784) | 0.181 |
|
|
| Liver metastasis
during second-line treatment |
|
|
|
|
| No | Reference |
|
|
|
|
Yes | 1.318
(0.928–1.872) | 0.122 |
|
|
Safety
The incidence of AEs of any grade and grade ≥3 in
the serplulimab group was 74.6% (n=50) and 29.9% (n=20),
respectively, which was 81.7% (n=76) and 34.4% (n=32) with
chemotherapy. The occurrence of any irAEs was reported in 17.9%
(n=12) of the patients with serplulimab, and 9 were treated with
systemic glucocorticoid. The most common hematological toxicities
with serplulimab were thrombocytopenia (35.8%), leukopenia (31.3%)
and anemia (28.4%), while non-hematological toxicities were mostly
drug-induced liver injury (23.9%), loss of appetite (19.4%) and
immune-associated pneumonia (17.9%). In the chemotherapy group, the
most common AEs were hematological toxicities, including leukopenia
(41.9%), thrombocytopenia (36.6%), anemia (36.6%), and neutropenia
(30.1%), as listed in Table V.
| Table V.AEs. |
Table V.
AEs.
| AE | Total (n=160) | Serplulimab
(n=67) | Chemotherapy
(n=93) |
|---|
| Any AE | 126 (78.8) | 50 (74.6) | 76 (81.7) |
| Any ≥grade 3
AE | 52 (32.5) | 20 (29.9) | 32 (34.4) |
| Any irAE | 28 (17.5) | 12 (17.9) | 16 (17.2) |
| irAE treated with
systemic glucocorticoids | 24 (15.0) | 9 (13.4) | 15 (16.1) |
| Specific AE |
|
|
|
|
Leukopenia | 60 (37.5) | 21 (31.3) | 39 (41.9) |
|
Thrombocytopenia | 58 (36.2) | 24 (35.8) | 34 (36.6) |
|
Anemia | 53 (33.1) | 19 (28.4) | 34 (36.6) |
|
Neutropenia | 40 (25.0) | 12 (17.9) | 28 (30.1) |
|
Nausea | 33 (20.6) | 11 (16.4) | 22 (23.7) |
| Loss of
appetite | 33 (20.6) | 13 (19.4) | 20 (21.5) |
|
Drug-induced liver injury | 33 (20.6) | 16 (23.9) | 17 (18.3) |
|
Rash | 32 (20.0) | 10 (14.9) | 22 (23.7) |
| Immune
associated pneumonia | 28 (17.5) | 12 (17.9) | 16 (17.2) |
|
Vomiting | 27 (16.9) | 10 (14.9) | 17 (18.3) |
|
Hypothyroidism | 13 (8.1) | 8 (11.9) | 5 (5.4) |
| Specific grade ≥3
AE |
|
|
|
|
Thrombocytopenia | 18 (11.2) | 9 (13.4) | 9 (9.7) |
|
Anemia | 17 (10.6) | 6 (9.0) | 11 (11.8) |
|
Rash | 11 (6.9) | 3 (4.5) | 8 (8.6) |
|
Neutropenia | 9 (5.6) | 2 (3.0) | 7 (7.5) |
|
Leukopenia | 9 (5.6) | 3 (4.5) | 6 (6.5) |
|
Drug-induced liver injury | 5 (3.1) | 3 (4.5) | 2 (2.2) |
|
Nausea | 4 (2.5) | 3 (4.5) | 1 (1.1) |
| Immune
associated pneumonia | 4 (2.5) | 2 (3.0) | 2 (2.2) |
| Loss of
appetite | 3 (1.9) | 0 (0.0) | 3 (3.2) |
|
Vomit | 1 (0.6) | 0 (0.0) | 1 (1.1) |
|
Hypothyroidism | 1 (0.6) | 0 (0.0) | 1 (1.1) |
Discussion
The present study compared the real-world
effectiveness of immunotherapy retreatment with serplulimab vs.
chemotherapy in patients with ES-SCLC after failure of first-line
immunotherapy. The findings suggested that second-line serplulimab
can significantly prolong the PFS time compared with chemotherapy
in patients with ES-SCLC previously treated with first-line
immunotherapy, regardless of the first-line immunotherapy regimen
or the duration of PFS for first-line immunotherapy. This study may
provide evidence for the feasibility of immunotherapy retreatment
by switching to a PD-1 inhibitor after failure of a first-line
PD-L1 inhibitor.
As a highly malignant disease, ES-SCLC treated with
first-line systemic therapy will eventually relapse and require
second-line therapy. Second-line chemotherapy is associated with
relatively poor survival, with a median PFS time of 4.7 months for
carboplatin/etoposide (35).
Systematic reviews and meta-analyses revealed a PFS time of 4.5–8.1
months (12,36), similar to the PFS time with
chemotherapy reported in the present study (5.25 months). Regarding
second-line immunotherapy in general, the KEYNOTE-028 trial
reported a median PFS time of 1.9 months with pembrolizumab
(37), while the IFCT-1603 trial
reported 1.4 months with atezolizumab (38). Furthermore, the exploration of
doublet immunotherapy failed to demonstrate benefits in PFS, with a
similar median PFS time of 1.4 vs. 1.5 months for nivolumab vs.
nivolumab/ipilimumab in the CheckMate 032 trial (39). Indeed, in previous studies of
second-line immunotherapy, the median PFS time was numerically
short (36–39). Notably, in these studies of
second-line chemotherapy or immunotherapy, a relatively small
proportion of patients had received first-line immunotherapy. As
for immunotherapy retreatment, a previous retrospective study
reported that for patients with ES-SCLC with progression after
first-line immunotherapy, the median PFS time of patients given
second-line immunotherapy for <6 weeks was 2.8 months, while the
median PFS time of those receiving >6 weeks of treatment could
reach 4.8 months (25),
highlighting the potential of immunotherapy retreatment.
Nevertheless, the second-line immunotherapy in the aforementioned
studies included both PD-1 and PD-L1 inhibitors, and none examined
serplulimab in that context.
The ASTRUM-005 study demonstrated that first-line
serplulimab improved the PFS and OS outcomes of patients with
previously untreated ES-SCLC compared with chemotherapy alone
(27). On the other hand, caution
has been raised regarding the conclusions of the ASTRUM-005 trial
(40), suggesting the need for
real-world data. Indeed, in ASTRUM-005, the control intervention
was not the standard therapy used nowadays; the trial enrolled
exclusively Eastern European and Asian patients and 20% of the
participants were non-smokers. Therefore, the results of the
ASTRUM-005 trial might be taken with caution and need to be
confirmed by additional studies. For instance, the high proportion
of non-smokers might be a potential limitation to the conclusions
in the ASTRUM-005 study (40), as
non-smokers with SCLC might have better efficacy outcomes. Although
the proportion of non-smokers was smaller in the serplulimab group
in the present study, the results suggest a better efficacy of
serplulimab compared with chemotherapy alone. A Bayesian
meta-analysis of 4,352 patients treated with nine regimens
suggested that the combination of serplulimab with chemotherapy as
first-line therapy should be recommended for patients with ES-SCLC
since it achieved the highest probability for better PFS (94.5%)
(28). Although such results
highlight the clinical value of serplulimab, the present study
examined the clinical value of challenging patients with ES-SCLC
with a PD-1 inhibitor after failure of a PD-L1 inhibitor. In the
present study, although there were no differences in ORR and DCR
between immunotherapy retreatment with serplulimab and chemotherapy
in second-line treatment, PFS and OS were significantly prolonged
with serplulimab as supported by the results from the multivariable
analysis. Nevertheless, as this study was retrospective,
large-scale head-to-head studies are needed for validation.
Serplulimab, as an anti-PD-1 drug, targets the PD-1
receptor directly on T cells, whereas atezolizumab or durvalumab
target the PD-L1 ligand (10,17).
This difference in binding targets offers several potential
explanations for the observed efficacy of PD-1 inhibitors after
PD-L1 blockade failure. First is the circumvention of
PD-L1-specific resistance mechanisms: Resistance to anti-PD-L1
agents can arise from various mechanisms, including downregulation
or structural alterations of PD-L1 on tumor cells, which may reduce
the binding affinity of PD-L1 inhibitors (16,41).
In such scenarios, directly blocking the PD-1 receptor on T cells
with a PD-1 inhibitor such as serplulimab can bypass these
PD-L1-specific resistance mechanisms, as it can still effectively
block the interaction of PD-1 with any remaining PD-L1 or other
ligands such as PD-L2 (42). Second
are the dynamic changes in the tumor microenvironment: The tumor
microenvironment is highly dynamic (43,44),
and the initial PD-L1 blockade may induce adaptive changes that,
while leading to resistance to the initial agent, could render the
tumor more susceptible to subsequent PD-1 blockade (45). For instance, the initial therapy may
alter the immune cell composition or cytokine milieu, creating a
more favorable environment for PD-1 inhibitor activity. Finally is
the re-invigoration of exhausted T cells: Even if resistance to
PD-L1 inhibitors develops, T cells may still exhibit PD-1-mediated
exhaustion (46). Direct PD-1
blockade can re-invigorate these exhausted T cells, restoring their
cytotoxic potential and antitumor activity (47). Therefore, targeting the receptor
instead of solely the ligands represents a valid and
mechanistically sound strategy to improve survival in patients who
have progressed on PD-L1 inhibitors.
The subgroup analysis of the secondary resistance
population in the present study indicated that serplulimab can
still be an effective choice for second-line treatment when
patients benefit from first-line immunotherapy. In addition, the
PFS time with first-line therapy is also considered an important
prognostic factor for the second-line PFS time (12,48).
Most patients in the serplulimab group in the present study were
simultaneously treated with anti-angiogenesis targeted drugs,
chemotherapy or radiotherapy, and the combination of these
treatment modalities may affect the tumor microenvironment of the
patients (49), allowing
immunotherapy to exert antitumor effects once again. Nevertheless,
due to the sample size in this study, the number of subgroups of
patients with different combination therapies was relatively small,
and further research is needed to determine the optimal combination
treatment strategies. In addition, only a small proportion of
patients stopped first-line immunotherapy due to primary resistance
or AEs. The effectiveness of serplulimab in patients' primary
resistance or intolerance to first-line immunotherapy needs to be
verified in future studies.
In the present study, the rates of any grade and
grade ≥3 AEs in the serplulimab and chemotherapy groups were
similar, which may be related to the combined chemotherapy for most
patients in the serplulimab group. In this study, no new safety
signals were found for serplulimab treatment. Of note was that it
was a real-world study, and no formal active monitoring of AEs was
performed, as in clinical trials. The present study collected AE
data from the medical record, which can lead to underreporting.
Although a multivariable Cox regression analysis was
performed to adjust for potential confounders, including smoking
history, first-line radiotherapy and concomitant use of
anti-angiogenic agents, the retrospective nature of this study
precludes complete elimination of selection bias. Several baseline
characteristics differed significantly between the serplulimab and
chemotherapy groups. Notably, the serplulimab group had a higher
proportion of smokers (53.7 vs. 28.0%; P=0.001) and a lower
frequency of first-line radiotherapy (38.8 vs. 64.5%; P=0.001).
Smoking status is a known prognostic factor in SCLC and may also
influence the efficacy of immunotherapy, potentially biasing the
observed PFS and OS benefit in favor of serplulimab (50). Conversely, the lower use of
first-line radiotherapy in the serplulimab group may have placed
these patients at a disadvantage, as radiotherapy can synergize
with immunotherapy by modulating the tumor microenvironment
(51). The direction and magnitude
of these opposing biases are difficult to quantify. Additionally,
the use of anti-angiogenic agents (anlotinib) was more frequent in
the serplulimab group (41.8 vs. 25.8%; P=0.033), which may have
contributed to the observed survival benefits independent of
serplulimab. While the multivariable analysis adjusted for these
factors, residual confounding from unmeasured variables (such as
tumor mutational burden, PD-L1 expression levels and detailed
smoking pack-years) cannot be excluded. Therefore, prospective
studies with balanced treatment arms are warranted to confirm the
superiority of serplulimab retreatment over chemotherapy.
There were limitations to the present study. Tumor
assessments and follow-ups are not as strict and regular in real
life as in randomized controlled trials. Therefore, the duration of
the response could not be accurately evaluated. The treatment
pattern in the serplulimab group was complex, including various
chemotherapy combinations or given alone, and the PFS and OS
benefits might not be attributed merely to serplulimab, despite the
independent association revealed by the multivariable analysis.
Future prospective studies are needed to address these issues.
Immunotherapy retreatment with serplulimab can
significantly prolong PFS and OS times compared with chemotherapy
for patients with ES-SCLC who have been treated with first-line
immunotherapy. As immunotherapy is the standard first-line
treatment for ES-SCLC, a feasible treatment strategy may include
switching to a PD-1 inhibitor as second-line immunotherapy after
first-line PD-L1 inhibitor failure. Further research is needed to
validate this hypothesis and identify the patients who would
benefit the most from second-line immunotherapy.
Supplementary Material
Supporting Data
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was supported by the Young Elite Sponsorship
Program (grant no. 2024-GJ-0059), the Research Project of Shandong
Provincial Medical Association (grant no. YXH2024YS053) and Wu
Jieping Foundation (grant no. 320.6750.2025-06-192).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
XG was responsible for conceptualization,
methodology, data curation, formal analysis, investigation, writing
the original draft and visualization. XW was responsible for
conceptualization, methodology, supervision, visualization,
writing, reviewing and editing. JG was responsible for
conceptualization, methodology and visualization. YW was
responsible for conceptualization, methodology, supervision,
visualization, writing, reviewing and editing. CL was responsible
for conceptualization, methodology, supervision, formal analysis,
visualization, writing, reviewing, editing and funding acquisition.
XG and CL confirm the authenticity of all the raw data. All authors
have made substantial intellectual contributions to the conception,
design, and execution of this study. Each author has actively
participated in drafting the work and revising it critically for
important intellectual content. All authors have read and approved
the final version of the manuscript. Furthermore, all authors agree
to be accountable for all aspects of the work, ensuring that
questions related to any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
This study was conducted in accordance with the
Declaration of Helsinki and its subsequent amendments. The study
was approved by the Ethics Committee of Shandong Cancer Hospital
and Institute (Jinan, China; approval no. SDTHEC202410078) on
October 12, 2024. The requirement for informed consent was waived
due to the retrospective nature of this research.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Petty WJ and Paz-Ares L: Emerging
strategies for the treatment of small cell lung cancer: A review.
JAMA Oncol. 9:419–429. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
van Meerbeeck JP, Fennell DA and De
Ruysscher DK: Small-cell lung cancer. Lancet. 378:1741–1755. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Ost DE, Jim Yeung SC, Tanoue LT and Gould
MK: Clinical and organizational factors in the initial evaluation
of patients with lung cancer: Diagnosis and management of lung
cancer, 3rd ed: American College of Chest Physicians evidence-based
clinical practice guidelines. Chest. 143 (5 Suppl):e121S–e141S.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
NCCN Clinical Practice Guidelines in
Oncology (NCCN Guidelines), . Small Cell Lung Cancer. Version
3.2023. National Comprehensive Cancer Network; Fort Washington:
2022
|
|
5
|
Karim SM and Zekri J: Chemotherapy for
small cell lung cancer: A comprehensive review. Oncol Rev.
6:e42012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Noda K, Nishiwaki Y, Kawahara M, Negoro S,
Sugiura T, Yokoyama A, Fukuoka M, Mori K, Watanabe K, Tamura T, et
al: Irinotecan plus cisplatin compared with etoposide plus
cisplatin for extensive small-cell lung cancer. N Engl J Med.
346:85–91. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Lara PN Jr, Natale R, Crowley J, Lenz HJ,
Redman MW, Carleton JE, Jett J, Langer CJ, Kuebler JP, Dakhil SR,
et al: Phase III trial of irinotecan/cisplatin compared with
etoposide/cisplatin in extensive-stage small-cell lung cancer:
Clinical and pharmacogenomic results from SWOG S0124. J Clin Oncol.
27:2530–2535. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hanna N, Bunn PA Jr, Langer C, Einhorn L,
Guthrie T Jr, Beck T, Ansari R, Ellis P, Byrne M, Morrison M, et
al: Randomized phase III trial comparing irinotecan/cisplatin with
etoposide/cisplatin in patients with previously untreated
extensive-stage disease small-cell lung cancer. J Clin Oncol.
24:2038–2043. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Lima JP, dos Santos LV, Sasse EC, Lima CS
and Sasse AD: Camptothecins compared with etoposide in combination
with platinum analog in extensive stage small cell lung cancer:
Systematic review with meta-analysis. J Thorac Oncol. 5:1986–1993.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Horn L, Mansfield AS, Szczęsna A, Havel L,
Krzakowski M, Hochmair MJ, Huemer F, Losonczy G, Johnson ML, Nishio
M, et al: First-line atezolizumab plus chemotherapy in
Extensive-Stage Small-Cell lung cancer. N Engl J Med.
379:2220–2229. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Paz-Ares L, Dvorkin M, Chen Y, Reinmuth N,
Hotta K, Trukhin D, Statsenko G, Hochmair MJ, Özgüroğlu M, Ji JH,
et al: Durvalumab plus platinum-etoposide versus platinum-etoposide
in first-line treatment of extensive-stage small-cell lung cancer
(CASPIAN): A randomised, controlled, open-label, phase 3 trial.
Lancet. 394:1929–1939. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Owonikoko TK, Behera M, Chen Z, Bhimani C,
Curran WJ, Khuri FR and Ramalingam SS: A systematic analysis of
efficacy of second-line chemotherapy in sensitive and refractory
small-cell lung cancer. J Thorac Oncol. 7:866–872. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
O'Brien ME, Ciuleanu TE, Tsekov H, Shparyk
Y, Cuceviá B, Juhasz G, Thatcher N, Ross GA, Dane GC and Crofts T:
Phase III trial comparing supportive care alone with supportive
care with oral topotecan in patients with relapsed small-cell lung
cancer. J Clin Oncol. 24:5441–5447. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Aix SP, Ciuleanu TE, Navarro A, Cousin S,
Bonanno L, Smit EF, Chiappori A, Olmedo ME, Horvath I, Grohé C, et
al: Combination lurbinectedin and doxorubicin versus physician's
choice of chemotherapy in patients with relapsed small-cell lung
cancer (ATLANTIS): A multicentre, randomised, open-label, phase 3
trial. Lancet Respir Med. 11:74–86. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zaremba A, Eggermont AMM, Robert C, Dummer
R, Ugurel S, Livingstone E, Ascierto PA, Long GV, Schadendorf D and
Zimmer L: The concepts of rechallenge and retreatment with immune
checkpoint blockade in melanoma patients. Eur J Cancer.
155:268–280. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Kim JM and Chen DS: Immune escape to
PD-L1/PD-1 blockade: Seven steps to success (or failure). Ann
Oncol. 27:1492–1504. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Sun JY, Zhang D, Wu S, Xu M, Zhou X, Lu XJ
and Ji J: Resistance to PD-1/PD-L1 blockade cancer immunotherapy:
Mechanisms, predictive factors, and future perspectives. Biomark
Res. 8:352020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
19
|
Chen L and Flies DB: Molecular mechanisms
of T cell co-stimulation and co-inhibition. Nat Rev Immunol.
13:227–242. 2013. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Ishida Y, Agata Y, Shibahara K and Honjo
T: Induced expression of PD-1, a novel member of the immunoglobulin
gene superfamily, upon programmed cell death. EMBO J. 11:3887–3895.
1992. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Dong H, Zhu G, Tamada K and Chen L: B7-H1,
a third member of the B7 family, co-stimulates T-cell proliferation
and interleukin-10 secretion. Nat Med. 5:1365–1369. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Latchman Y, Wood CR, Chernova T, Chaudhary
D, Borde M, Chernova I, Iwai Y, Long AJ, Brown JA, Nunes R, et al:
PD-L2 is a second ligand for PD-1 and inhibits T cell activation.
Nat Immunol. 2:261–268. 2001. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Bojko M, Węgrzyn K, Sikorska E, Kocikowski
M, Parys M, Battin C, Steinberger P, Kogut MM, Winnicki M,
Sieradzan AK, et al: Design, synthesis and biological evaluation of
PD-1 derived peptides as inhibitors of PD-1/PD-L1 complex formation
for cancer therapy. Bioorg Chem. 128:1060472022. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cerniglia M, Klepadlo M, Sheneman D and
Kim SS: Response to PD-1 inhibitor after progression on PD-L1
inhibitor in advanced HCC. BMJ Case Rep. 15:e2500092022. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Li L, Liu T, Liu Q, Mu S, Tao H, Yang X,
Li Y, Xiong Q, Wang L and Hu Y: Rechallenge of immunotherapy beyond
progression in patients with extensive-stage small-cell lung
cancer. Front Pharmacol. 13:9675592022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Qin S, Li J, Zhong H, Jin C, Chen L, Yuan
X, Fan Q, Chen K, Cao P, Xiao J, et al: Serplulimab, a novel
anti-PD-1 antibody, in patients with microsatellite
instability-high solid tumours: An open-label, single-arm,
multicentre, phase II trial. Br J Cancer. 127:2241–2248. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cheng Y, Han L, Wu L, Chen J, Sun H, Wen
G, Ji Y, Dvorkin M, Shi J, Pan Z, et al: Effect of First-line
serplulimab vs placebo added to chemotherapy on survival in
patients with extensive-stage small cell lung cancer: The
ASTRUM-005 randomized clinical trial. JAMA. 328:1223–1232. 2022.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Zhang T, Li W, Diwu D, Chen L, Chen X and
Wang H: Efficacy and safety of first-line immunotherapy plus
chemotherapy in treating patients with extensive-stage small cell
lung cancer: A Bayesian network meta-analysis. Front Immunol.
14:11970442023. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chen S, Zhang Z, Zheng X, Tao H, Zhang S,
Ma J, Liu Z, Wang J, Qian Y, Cui P, et al: Response efficacy of
PD-1 and PD-L1 inhibitors in clinical trials: A systematic review
and Meta-analysis. Front Oncol. 11:5623152021. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kluger HM, Tawbi HA, Ascierto ML, Bowden
M, Callahan MK, Cha E, Chen HX, Drake CG, Feltquate DM, Ferris RL,
et al: Defining tumor resistance to PD-1 pathway blockade:
Recommendations from the first meeting of the SITC immunotherapy
resistance taskforce. J Immunother Cancer. 8:e0003982020.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
U.S. Department of Health and Human
Services, . Common Terminology Criteria for Adverse Events (CTCAE).
Version 5.0. https://ctep.cancer.gov/protocoldevelopment/electronic_applications/docs/CTCAE_v5_Quick_Reference_5×7.pdfNovember
19–20242017.
|
|
33
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the eastern cooperative oncology group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Mor V, Laliberte L, Morris JN and Wiemann
M: The karnofsky performance status scale. An examination of its
reliability and validity in a research setting. Cancer.
53:2002–2007. 1984. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Baize N, Monnet I, Greillier L, Geier M,
Lena H, Janicot H, Vergnenegre A, Crequit J, Lamy R, Auliac JB, et
al: Carboplatin plus etoposide versus topotecan as second-line
treatment for patients with sensitive relapsed small-cell lung
cancer: An open-label, multicentre, randomised, phase 3 trial.
Lancet Oncol. 21:1224–1233. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Zugazagoitia J and Paz-Ares L:
Extensive-stage small-cell lung cancer: First-line and Second-line
treatment options. J Clin Oncol. 40:671–680. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ott PA, Elez E, Hiret S, Kim DW, Morosky
A, Saraf S, Piperdi B and Mehnert JM: Pembrolizumab in patients
with Extensive-stage small-cell lung cancer: Results from the phase
Ib KEYNOTE-028 study. J Clin Oncol. 35:3823–3829. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Pujol JL, Greillier L, Audigier-Valette C,
Moro-Sibilot D, Uwer L, Hureaux J, Guisier F, Carmier D, Madelaine
J, Otto J, et al: A Randomized non-comparative phase II study of
anti-programmed cell death-ligand 1 atezolizumab or chemotherapy as
second-line therapy in patients with small cell lung cancer:
Results from the IFCT-1603 trial. J Thorac Oncol. 14:903–913. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ready NE, Ott PA, Hellmann MD,
Zugazagoitia J, Hann CL, de Braud F, Antonia SJ, Ascierto PA,
Moreno V, Atmaca A, et al: Nivolumab monotherapy and nivolumab plus
ipilimumab in recurrent small cell lung cancer: Results from the
CheckMate 032 randomized cohort. J Thorac Oncol. 15:426–435. 2020.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Choudhury NJ and Riely GJ: Serplulimab
with chemotherapy in Extensive-Stage SCLC. JAMA. 328:1205–1207.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Yuan Y, Adam A, Zhao C and Chen H: Recent
advancements in the mechanisms underlying resistance to PD-1/PD-L1
blockade immunotherapy. Cancers (Basel). 13:6632021. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Garcia-Diaz A, Shin DS, Moreno BH, Saco J,
Escuin-Ordinas H, Rodriguez GA, Zaretsky JM, Sun L, Hugo W, Wang X,
et al: Interferon receptor signaling pathways regulating PD-L1 and
PD-L2 expression. Cell Rep. 19:1189–1201. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Binnewies M, Roberts EW, Kersten K, Chan
V, Fearon DF, Merad M, Coussens LM, Gabrilovich DI,
Ostrand-Rosenberg S, Hedrick CC, et al: Understanding the tumor
immune microenvironment (TIME) for effective therapy. Nat Med.
24:541–550. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Zhang P, Zhang C, Li X, Chang C, Gan C, Ye
T and Cao D: Immunotherapy for gastric cancer: Advances and
challenges. Med Comm Oncol. 3:e922024.
|
|
45
|
Sharma P, Hu-Lieskovan S, Wargo JA and
Ribas A: Primary, adaptive, and acquired resistance to cancer
immunotherapy. Cell. 168:707–723. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Wherry EJ and Kurachi M: Molecular and
cellular insights into T cell exhaustion. Nat Rev Immunol.
15:486–499. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Zitvogel L and Kroemer G: Targeting
PD-1/PD-L1 interactions for cancer immunotherapy. Oncoimmunology.
1:1223–1225. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Dingemans AC, Fruh M, Ardizzoni A, Besse
B, Faivre-Finn C, Hendriks LE, Lantuejoul S, Peters S, Reguart N,
Rudin CM, et al: Small-cell lung cancer: ESMO Clinical Practice
Guidelines for diagnosis, treatment and follow-up☆. Ann Oncol.
32:839–853. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Hu H, Wang K, Jia R, Zeng ZX, Zhu M, Deng
YL, Xiong ZJ, Tang JN, Xie H, Wang Y, et al: Current Status in
rechallenge of immunotherapy. Int J Biol Sci. 19:2428–2442. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Ou SH, Ziogas A and Zell JA: Prognostic
factors for survival in extensive stage small cell lung cancer
(ED-SCLC): The importance of smoking history, socioeconomic and
marital statuses, and ethnicity. J Thorac Oncol. 4:37–43. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Meng K and Lu H: Clinical application of
high-LET radiotherapy combined with immunotherapy in malignant
tumors. Precis Radiat Oncol. 8:42–46. 2024. View Article : Google Scholar : PubMed/NCBI
|