Introduction
Autoimmune hemolytic anemia (AIHA) is a rare disease
caused by immune dysfunction leading to hyperactive B cells
producing autoantibodies against red blood cells. These antibodies
bind to red blood cells and may activate complement systems,
resulting in hemolysis. International data indicates an annual
incidence rate of 0.8–3.0/100,000 cases worldwide (1). Based on the type and thermal
characteristics of the autoantibody, AIHA can be classified into
three types: Classic warm AIHA (wAIHA), cold agglutinin disease
(CAD) and mixed AIHA. Notably, ~50% of wAIHA cases are secondary
and associated with a number of underlying medical disorders
including blood malignancies, solid tumors, autoimmune diseases,
infections, solid organ and hematopoietic stem cell transplants,
and numerous drugs (including antibiotics, immune checkpoint
inhibitors anti-programmed cell death protein 1, programmed
death-ligand 1 and cytotoxic T-lymphocyte associated protein 4)
(2).
However, there are few reported cases of AIHA
associated with solid tumors. Most cases involving solid tumors in
AIHA have been documented in renal tumors, Kaposi's sarcoma,
prostate tumors, ovarian tumors and non-small cell lung cancer
(3–7). Analysis of previously reported cases
of AIHA associated with solid tumors suggests that AIHA may occur
before the diagnosis of malignant tumors, emerge concurrently with
solid malignancies, or even manifest as a sign of cancer recurrence
or complete remission following treatment (7). Cervical cancer has rarely been
identified as a cause of AIHA. Although anemia is one of the most
common post-treatment complications in cervical cancer patients
(8), autoimmune hemolysis-induced
anemia remains unreported. This rare etiology is often overlooked
by clinicians, causing delays in treatment and potentially
compromising treatment outcomes. The present study reports a case
of wAIHA in a 73-year-old patient with cervical cancer after
radical chemoradiotherapy, which, to the best of our knowledge,
revealed this rare association for the first time.
Case report
A 73-year-old woman with >20 years natural
menopause developed vaginal bleeding in November 2024. At first the
patient did not take it seriously. In January 2025, the patient was
initially admitted to Nanjing Gaochun People's Hospital (Nanjing,
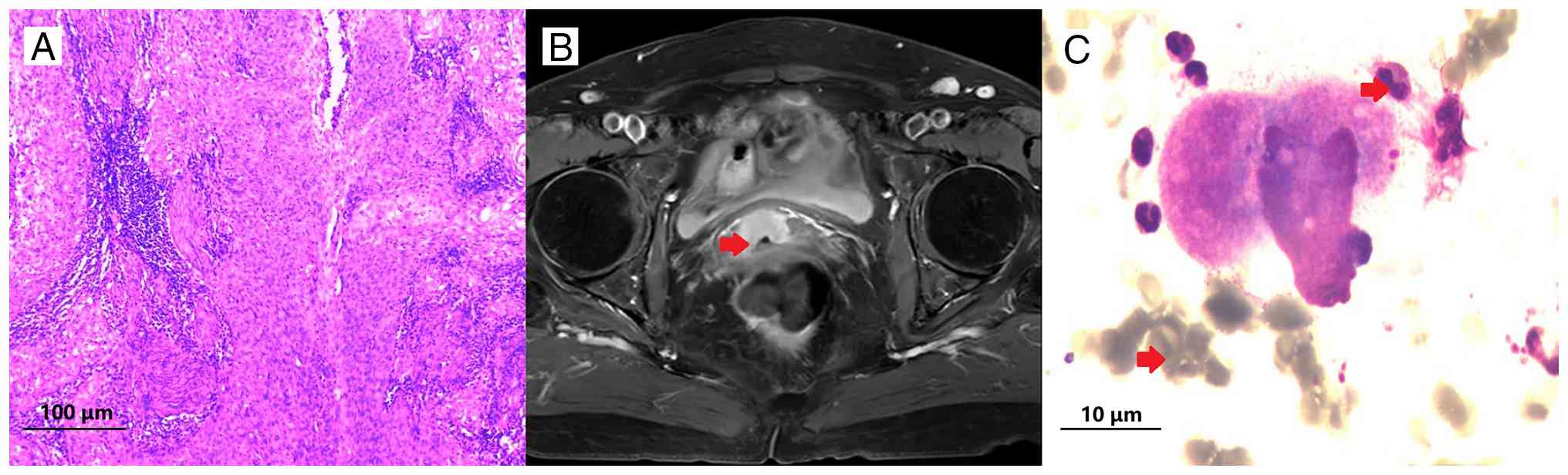
China). A colposcopy performed in January 2025 and revealed
cervical squamous cell carcinoma (Fig.
1A), with human papilloma virus (HPV) 16 (a high-risk HPV type)
detected using HPV testing. Pelvic MRI demonstrated a
space-occupying lesion on the anterior cervical wall (Fig. 1B). The clinical stage was IB using
the International Federation of Gynecology and Obstetrics 2018
staging system (9). Their
hemoglobin (Hb) level was 14.4 g/dl prior to treatment. The patient
refused surgical treatment and underwent pelvic radical
radiotherapy (95% planning target volume; 45 Gy/25F) from February
to March 2025, combined with cisplatin chemotherapy (55 mg/weekly
for 5 weeks). The final cisplatin session was administered in March
2025. Serial blood counts during external beam radiotherapy did not
show signs of myelosuppression in Hb, which was consistently >12
g/l. However, the patient experienced leukopenia and
thrombocytopenia which improved following administration of human
granulocyte colony-stimulating factor and thrombopoietin.
In March 2025, the patient began intracavitary
brachytherapy with a prescribed total dose (DT) of 35 Gy/7F. By
April 2025, when the DT reached 25 Gy/5F, a follow-up blood test
showed Hb levels at 4.9 g/dl. The patient received supportive
treatments including hematopoietic agents, erythropoietin and blood
transfusions. Following this, in April 2025, brachytherapy
continued. After finishing intracavitary brachytherapy, the Hb
levels remained persistently low, although aggressive blood
transfusion, erythropoietin and supportive treatment were
adopted.
In May 2025, Hb was only 4.3 g/dl. Abnormal
elevation of bilirubin levels, predominantly unconjugated
bilirubin, were observed with total bilirubin 51.4 µmol/l and
direct bilirubin 9.8 µmol/l. Laboratory examination showed the
following: Irregular antibody screening, negative; direct
antiglobulin test (DAT), positive; and indirect antiglobulin test
(IAT), positive. The reticulocyte percentage was 21.07%. DAT was
performed using monospecific anti-human globulin reagents against
IgG and C3d. The result showed elevated monospecific anti-IgG
levels (mono-Coombs IgG positive), confirming the diagnosis of
autoimmune hemolytic anemia (AIHA). DAT and IAT were performed in
the Department of Clinical Laboratory of Nanjing Gaochun People's
Hospital (Nanjing, China) following routine clinical protocols. For
DAT, the following reagents were used: anti-C3d (cat. no.
20153401143), anti-IgG (cat. no. 20153401142) and anti-human
globulin (AHG; cat. no. 20153401144), all from Shanghai Blood
Biological Medicine Co., Ltd. For IAT, LISS solution (batch no.
20231101; Changchun Bioxun Biotech Co., Ltd.) was used as
enhancement medium, with IgG anti-D (cat. no. 20223401104; Shanghai
Blood Biological Medicine Co., Ltd.) as positive control and IgG
anti-Fya (cat. no. MFyaM21o-1; CE-Immun diagnostika GmbH) as
specificity control; the same AHG reagent was employed. All tests
followed the hospital's standard operating procedures.
Bone marrow smear cytology (Fig. 1C) was performed using standard
Wright-Giemsa staining (methanol fixation at room temperature for
15 min, staining for 20 min). For H&E staining, specimens were
routinely fixed in 3.7% neutral formalin at room temperature for
6–24 h, followed by conventional procedures including dehydration
and paraffin embedding. The specimens were then cut into 3-µm-thick
sections and stained with H&E for light microscopy examination.
Hematoxylin staining was performed for 5 min and eosin staining for
3 min at room temperature. The slides were examined under a BX53
Olympus standard light microscope. The cytology (Fig. 1C) showed active proliferation of
nucleated cells with a granulocyte-to-lymphocyte ratio of 2.12:1.
Erythroid hyperplasia was prominent, with a marked increase in
late-stage erythrocytes. Screening for underlying conditions
(lymphoproliferative disorders, autoimmune diseases, infections,
immunodeficiencies and medications) was performed by reviewing the
patient's medical history, aforementioned laboratory blood tests
and medication history. All results were negative or unremarkable
except for the elevated direct Coombs test and hemolytic
parameters. Therefore, secondary autoimmune hemolysis caused by
cervical cancer was confirmed. After diagnosis, the patient
initiated daily oral prednisone treatment at 50 mg. After 10 days
medication, Hb levels rose to 11.9 g/dl. Subsequent weekly
monitoring revealed Hb levels at 12.3 and 11.8 g/dl. The patient
was followed up at the outpatient clinic every 2–4 weeks.
Prednisone was gradually tapered over 8 weeks and completely
withdrawn by the end of July 2025. At the most recent follow-up in
April 2026, the patient remained asymptomatic with no evidence of
hemolysis. Hemoglobin level was 12.5 g/dl. No recurrence of vaginal
bleeding or other adverse events were observed.
Discussion
Anemia is common in patients with cancer. AIHA, as a
rare manifestation of tumor-associated anemia, primarily occurs
secondary to lymphoproliferative disorders including non-Hodgkin's
lymphoma and an estimated 10% of chronic lymphocytic leukemia cases
(10). The association between AIHA
and solid malignant tumors has been rarely reported, including in
gastric, ovarian, breast and kidney cancers (7,11). To
the best of our knowledge, the present case reported the rare
association between AIHA and cervical cancer for the first time. It
is a further addition to tumor-associated AIHA and has notable
clinical relevance.
Before confirming AIHA as secondary to cervical
cancer, other more common related diseases must be ruled out.
Firstly, the patient showed no hematopoietic or lymphatic system
proliferative disorders. Secondly, all autoantibody tests of the
patient were negative, and there was no recent history of
infection, thus the association of AIHA with autoimmune diseases or
infections were excluded. Previous studies (12,13)
have indicated that cisplatin can cause non-immunologic protein
adsorption onto the red blood cell (RBC) membrane; adsorbed
proteins (including albumin, complement components and
immunoglobulins, in particular IgG) can react with receptors on
macrophages which can induce hemolytic anemia and lead to DAT
positivity (14). This makes
cisplatin a suspected cause of AIHA in the present patient. However
in non-immunologic protein adsorption, the IAT is usually negative
because the adsorbed proteins are not specific autoantibodies. The
patient in the present study had a positive IAT, indicating the
presence of circulating autoantibodies against native RBCs which is
a hallmark of wAIHA. Furthermore, cisplatin-induced hemolysis
usually develops during or shortly after drug administration and
resolves spontaneously after drug withdrawal (15,16).
The patient developed anemia >1 month after the last cisplatin
chemotherapy, and the anemia still not alleviated after cisplatin
withdrawal; therefore, cisplatin-induced immune hemolytic anemia
was excluded.
The potential mechanism of AIHA secondary to solid
neoplasms is not known. It is hypothesized that antibodies against
tumor cells may crossly react with erythrocyte antigens, leading to
hemolysis (7). Kitao et al
(17) described an AIHA case
secondary to colorectal cancer with ectopic band 3 expression, an
anion transporter normally restricted to erythrocytes and renal
cells. After further research, the authors found that ectopic band
3 expression was associated with increased erythrocyte
membrane-bound IgG in patients with colorectal cancer which can
lead to shortened RBC lifespan. Immunoprecipitation revealed
increased anti-band 3 autoantibodies in serum from patients.
Ectopic band 3 expression was also reported as a cause of mature
ovarian teratoma-associated secondary autoimmune hemolytic anemia
(18). This may be a potential
mechanism of tumor-associated immune hemolysis. Future studies
should investigate whether ectopic band 3 or cross-reactive
antibodies serve a role in cervical cancer-associated AIHA.
The first-line treatment for wAIHA is usually
glucocorticoids. However, during tapering and discontinuation,
approximately a third of patients relapse and require further
treatment (10). The anti-CD20
monoclonal antibody rituximab has become the first choice of
second-line treatment, being able to induce hematologic responses
in 70–80% of patients (1). For
severely anemic patients whose Hb <8 g/dl, rituximab was
recommended for first-line treatment in addition to steroids.
Splenectomy is also an effective treatment option; the response
rates can be 70–80%. Due to the increased risk of infection and
thrombosis, splenectomy is rarely used today and is only recommend
as a the third-line or subsequent treatment (19). Treatment for suspected
complement-mediated hemolysis can include complement pathway
inhibitors such as eculizumab (anti-C5) and sutimlimab (anti-C1s)
(20). For patients resistant to or
relapsing after rituximab and not suitable for splenectomy, the use
of cytotoxic immunosuppressants such as azathioprine,
cyclophosphamide, cyclosporine, mycophenolate mofetil, bortezomib
might be considered, relying predominantly on evidence from small
retrospective series and case reports (21,22).
The treatment of malignant tumor-associated AIHA has
not been well established. The efficacy of steroids varies
considerably among different populations. Puthenparambil et
al (7) found that patients who
had a response to resection of the tumor were often resistant to
steroid treatment before surgery, while some hematologic responses
to steroids were observed in patients with metastatic cancer.
However, some cases of patients with AIHA secondary to metastatic
cancer who received steroid therapy showed no efficacy, and the
disease was controlled by palliative chemotherapy (23). In the present case, the patient had
undergone radical concurrent chemoradiotherapy. Under these
circumstances, the use of glucocorticoids led to notable
improvement in anemia. In the present case, glucocorticoids were
effective, supporting their consideration as a first-line option in
similar patients, although responses may vary as noted in the
literature. For patients unresponsive to glucocorticoids, some may
benefit from tumor resection (even in metastatic cases), while some
might respond to antitumor therapy.
The present case showed that autoimmune hemolysis is
a potential cause of anemia after chemoradiotherapy in patients
with cervical cancer, and it is occasionally difficult to
distinguish from drug-induced hemolytic anemia and
myelosuppression. Therefore, when unexplained anemia occurs after
chemoradiotherapy in patients with cervical cancer, clinicians
should perform direct antiglobulin test (Coombs test) and indirect
antiglobulin test to screen for autoimmune hemolysis.
Distinguishing it from drug-induced hemolysis and myelosuppression
is essential, as prompt recognition allows early initiation of
corticosteroids. Future work should prioritize mechanistic research
to elucidate how cervical cancer affects immune tolerance and
triggers red blood cell autoimmunity.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
YK and LZ conceptualized the case report, wrote the
manuscript and performed additional data analysis. YK and YX were
involved in the treatment and follow-up of the case. YX critically
revised the manuscript, provided supervision and approved the final
manuscript for publication. All authors read and approved the final
version of the manuscript. YK and YX confirm the authenticity of
all raw data.
Ethics approval and consent to
participate
Ethics approval was not required for the present
study in accordance with local and institutional requirements. The
study was conducted in accordance with local legislation and
institutional requirements. The participant provided written
informed consent to participate in the present study.
Patient consent for publication
Written informed consent for publication of the
present article was obtained from the participant.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Fattizzo B and Barcellini W: Autoimmune
hemolytic anemia: Causes and consequences. Expert Rev Clin Immunol.
18:731–745. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Barcellini W and Fattizzo B: Autoimmune
hemolytic anemias: Challenges in diagnosis and therapy. Transfus
Med Hemother. 51:321–331. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Arias de la Vega F, Torres López A, Piedra
Roset P, Barco Burguete A, Rosas Gutiérrez L and Sola Galarza A:
Paraneoplastic hemolytic anemia associated with prostate cancer. A
case report. An Sist Sanit Navar. 45:e10232022.(In Spanish).
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Isotani S, Horiuchi A, Koja M, Noguchi T,
Sugiura S, Shimoyama H, Noma Y, Kitamura K, China T, Tokiwa S, et
al: Autoimmune hemolytic anemia associated with renal urothelial
cancer: A case report and literature review. BMC Urol. 15:752015.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zemek L, Strom L, Gordon G and Elguezabel
A: Hemolytic anemia with Kaposi's sarcoma. Report of a case JAMA.
187:232–234. 1964.PubMed/NCBI
|
|
6
|
Loh KP, Kansagra A, Asik A, Ali S and
Dahiya S: Paraneoplastic autoimmune hemolytic anemia in ovarian
cancer: A marker of disease activity. Rare Tumors. 7:55982015.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Puthenparambil J, Lechner K and Kornek G:
Autoimmune hemolytic anemia as a paraneoplastic phenomenon in solid
tumors: A critical analysis of 52 cases reported in the literature.
Wien Klin Wochenschr. 122:229–236. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Berta DM, Teketelew BB, Chane E, Bayleyegn
B, Tamir M, Cherie N, Seyoum M, Mekuanint A and Aynalem M:
Hematological changes in women with cervical cancer before and
after cancer treatment: Retrospective cohort study. Sci Rep.
14:276302024. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bhatla N, Berek JS, Cuello Fredes M, Denny
LA, Grenman S, Karunaratne K, Kehoe ST, Konishi I, Olawaiye AB,
Prat J, et al: Revised FIGO staging for carcinoma of the cervix
uteri. Int J Gynaecol Obstet. 145:129–135. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Loriamini M, Cserti-Gazdewich C and Branch
DR: Autoimmune hemolytic anemias: Classifications, pathophysiology,
diagnoses and management. Int J Mol Sci. 25:42962024. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kamesaki T: Autoimmune hemolytic anemia as
a paraneoplastic syndrome associated with solid tumors. Rinsho
Ketsueki. 56:778–784. 2015.(In Japanese). PubMed/NCBI
|
|
12
|
Zeger G, Smith L, McQuiston D and
Goldfinger D: Cisplatin-induced nonimmunologic adsorption of
immunoglobulin by red cells. Transfusion. 28:493–495. 1988.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Dacha S, Reddivari AK, Latta S, Devidi M
and Iroegbu N: Carboplatin induced fatal autoimmune hemolytic
anemia: First reported case. World J Oncol. 1:173–175.
2010.PubMed/NCBI
|
|
14
|
Nguyen TN, Maenulein E, Fihman V, Vinatier
I and Moh Klaren J: Serologic characteristics of oxaliplatin
antibodies in 15 patients with drug-induced immune hemolytic
anemia. Transfusion. 61:1609–1616. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Lu H, Wang N, Wang P, Zhang H, Zhao R, Liu
H, He X, Liu Z, Chang Y, Cao Y and Wang S: Case report: First case
of pemetrexed plus cisplatin-induced immune hemolytic anemia in a
patient with lung adenocarcinoma. Front Med (Lausanne).
9:9174852022. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Getaz EP, Beckley S, Fitzpatrick J and
Dozier A: Cisplatin-induced hemolysis. N Engl J Med. 302:334–335.
1980. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kitao A, Kawamoto S, Kurata K, Hayakawa I,
Yamasaki T, Matsuoka H, Sumi Y, Kakeji Y, Kamesaki T and Minami H:
Band 3 ectopic expression in colorectal cancer induces an increase
in erythrocyte membrane-bound IgG and may cause immune-related
anemia. Int J Hematol. 111:657–666. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Ochiai T, Yasuda H, Akiba H, Ashizawa K,
Hosoya E, Ando J, Miyake S and Ando M: Ectopic band 3 expression as
a cause of mature ovarian teratoma-associated secondary autoimmune
hemolytic anemia. Int J Lab Hematol. 46:744–746. 2024. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Patel NY, Chilsen AM, Mathiason MA,
Kallies KJ and Bottner WA: Outcomes and complications after
splenectomy for hematologic disorders. Am J Surg. 204:1014–1020.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Bortolotti M, Barcellini W and Fattizzo B:
Molecular pharmacology in complement-mediated hemolytic disorders.
Eur J Haematol. 111:326–336. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Barcellini W and Fattizzo B: How I treat
warm autoimmune hemolytic anemia. Blood 137: 1283–1294, 2021.
Erratum in [No authors listed] Blood. 438–439. 2023.
|
|
22
|
Fattizzo B, Cantoni S, Giannotta JA,
Bandiera L, Zavaglia R, Bortolotti M and Barcellini W: Efficacy and
safety of cyclosporine A treatment in autoimmune cytopenias: The
experience of two Italian reference centers. Ther Adv Hematol.
13:204062072210977802022. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Agrawal K and Alfonso F: A rare
association of autoimmune hemolytic anemia with gastric
adenocarcinoma. Case Rep Oncol Med. 2017:84146022017.PubMed/NCBI
|