Introduction
Sarcomatoid carcinoma (SC) is a rare type of
biphasic cancer characterized by the presence of both epithelial
and mesenchymal tumor cells. According to Xu et al (1) the age-adjusted incidence of SC was
1.26/100,000 individuals in 2014, and the average onset age of SC
is 68±13 years (1). The prevalence
of SC is highest in the respiratory system, followed by digestive,
urinary and female genital systems (1). SC of the lungs, urinary bladder and
liver is reported to predominantly affect male patients (2–4).
Mediastinal SC is an aggressive malignancy with limited
documentation in existing literature. It may originate from the
thymus or pulmonary tissue. Patients often present with
non-specific symptoms such as cough, chest pain and breathlessness
(5–10). Due to the invasiveness and frequent
metastasis, SC is often diagnosed at an advanced stage (2). Patients with early-stage SC can
benefit from surgical intervention. For advanced stage SC, the
therapeutic efficacy of chemotherapy and radiotherapy remains
modest (2–4). Due to its high malignancy, late
detection and poor response to conventional chemoradiotherapy, the
prognosis for SC is generally unfavorable (2). In the present case report, a patient
with mediastinal SC who achieved prolonged progression-free
survival (PFS) after treatment is described. This case is notable
not only because of the uncommon anatomical location but also due
to the favorable clinical outcome challenging the established
perception of universally poor prognosis in this malignancy.
Through detailed presentation and comprehensive review of clinical
features, pathological features and treatment, the present case
report aims to expand the extremely limited evidence base for this
rare disease entity and identify potential therapeutic strategies,
addressing the key knowledge gap regarding optimal management of
mediastinal SC.
Case report
Case presentation
A 74-year-old female patient with no history of
smoking presented to The First People's Hospital of Xiaoshan
(Hangzhou, China) in January 2022 with cough and chest pain for 50
days, and breathlessness and dysphagia for 10 days. Physical
examination revealed a mobile 3 cm lymph node in the right neck,
and audible wheezing sounds from both lungs. The patient had a
history of hypertension and diabetes for >20 years, but blood
pressure and blood glucose levels were well-controlled with
medication. In addition, the patient reported no family history of
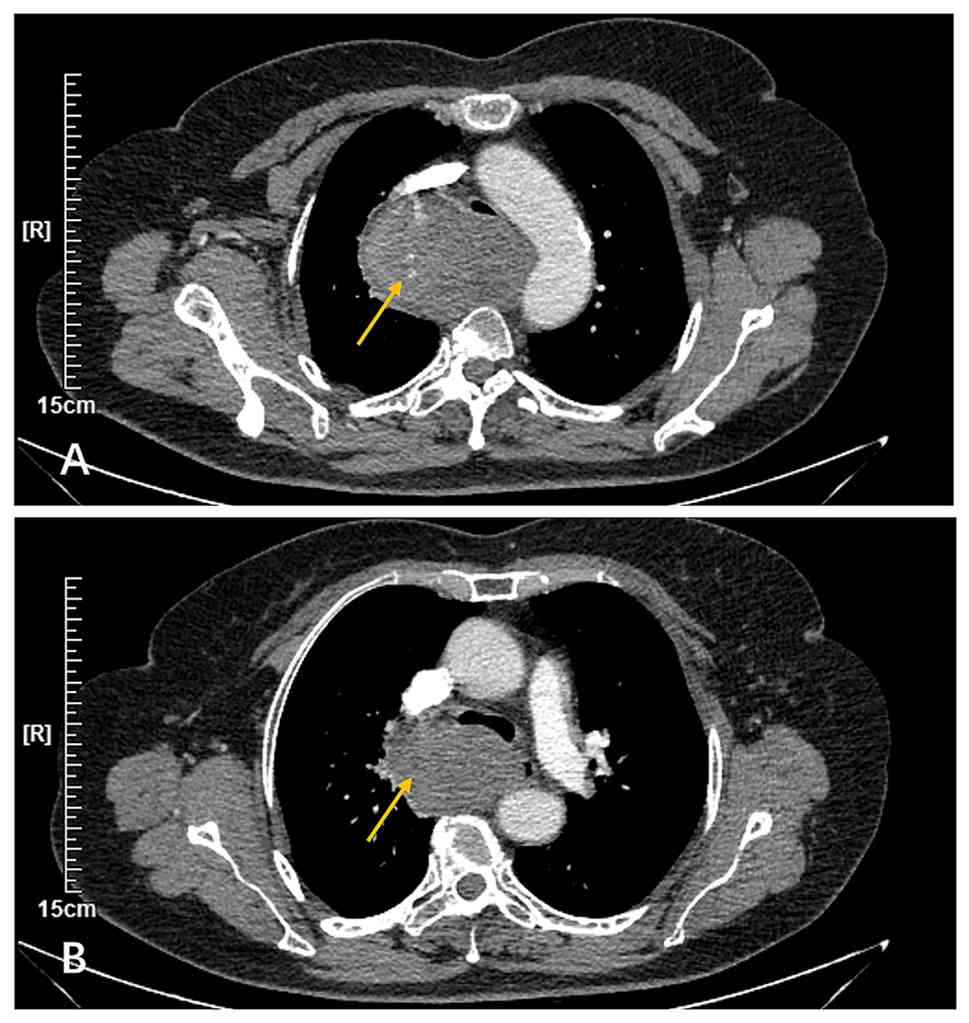
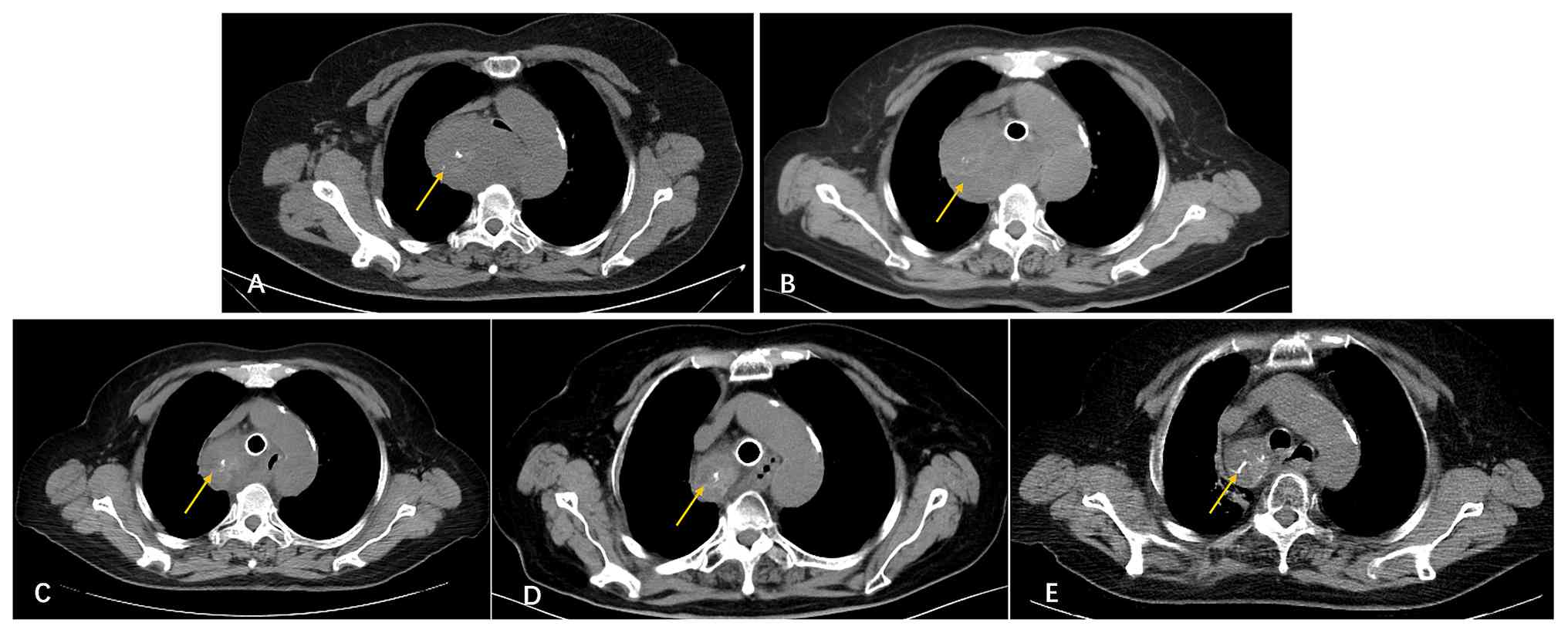
cancer. A chest computed tomography (CT) scan was performed, which
revealed a mass with soft tissue density and spotted calcification
at the right posterior upper mediastinum (maximum cross-section,
8.5×6.2 cm). Furthermore, the trachea and esophagus were compressed
and deformed. Finally, a contrast-enhanced chest CT scan was
performed the following day, which showed inhomogeneous enhancement
contrast (Fig. 1).
A total of 4 days after the patient presented to the
hospital, a bronchoscopy examination was performed, which revealed
notable stenosis in the middle and lower segments of the trachea
due to external pressure. In addition, an endobronchial ultrasound
showed abnormal low-density echogenicity on the right posterior
side of the trachea. Transbronchial needle aspiration was performed
and a tracheal stent of 16×40 mm was placed, which notably
alleviated bronchial stenosis. H&E staining of the specimen
showed multiple small clusters of atypical cells scattered in the
background of mucus and inflammatory cells, with an abundant
cytoplasm and lack of specificity in immunohistochemical markers.
Fluorodeoxyglucose positron emission tomography (FDG PET) was
performed the following day at Zhejiang Aibo Medical Imaging
Diagnosis Center (Hangzhou, China), which showed a soft tissue
density mass with increased FDG uptake in the posterior mediastinum
with unclear margins relative to the bronchus, carina and right
main bronchus, suggesting a high probability of mediastinal-type
lung cancer. FDG PET also showed multiple enlarged lymph nodes in
the right supraclavicular, cervical, mediastinal 2R and 4R lymph
nodes with a mild increase in FDG metabolism. These findings
suggested reactive lymph node hyperplasia, with a very low
possibility of lymph node metastasis to be excluded. A fine-needle
aspiration biopsy of the lymph node in the right cervical was
conducted and the pathological results indicated chronic
inflammation of the lymph nodes.
Only a small portion of the specimen consisted of
tumor cells, and it lacked specificity in immunohistochemical
markers, thus a clear pathological diagnosis was not achieved. The
patient was sent to The First Affiliated Hospital of Medical School
of Zhejiang University (Hangzhou, China) at the end of January 2022
for further treatment. The patient underwent gastroscopy and
endoscopic ultrasound-guided fine needle aspiration (EUS-FNA).
After tissue was fixed with 4% formalin, 4-µm paraffin sections
were prepared and processed according to standard procedures. The
staining steps included hematoxylin nuclear staining at room
temperature (RT) for 5–10 min, followed by eosin cytoplasmic
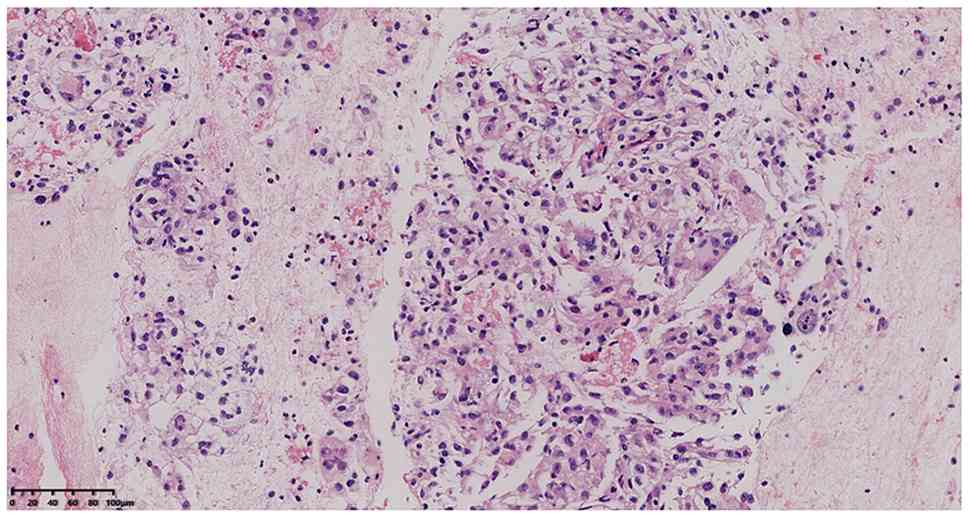
staining at RT for 2–3 min. Microscopically, H&E staining
(Fig. 2) revealed sarcoma-like
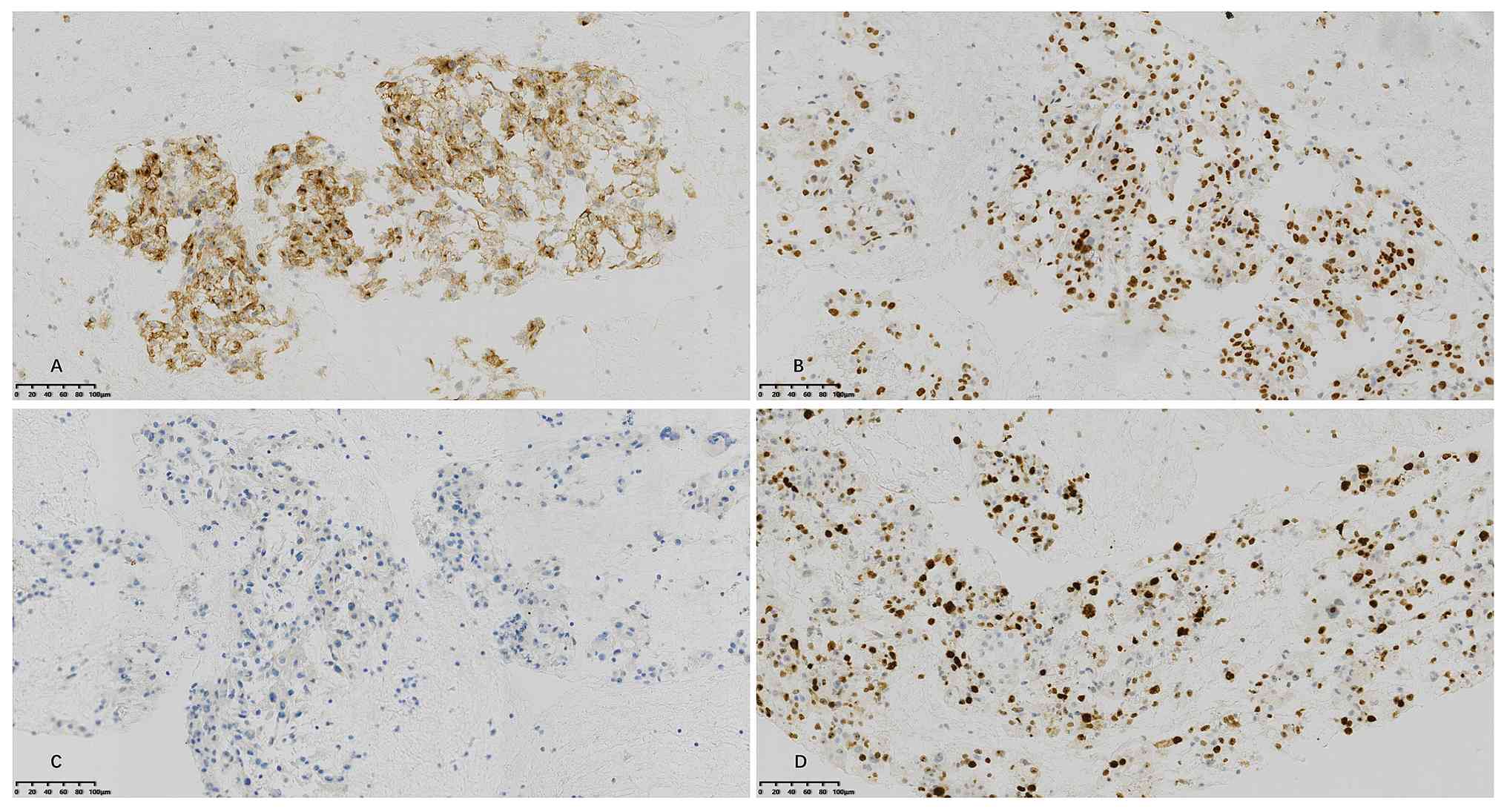
neoplasms. Immunohistochemical (IHC) analysis demonstrated
positivity for epithelial membrane antigen (EMA) (Fig. 3A), transducing-like enhancer of
split 1 (TLE1) (Fig. 3B) and smooth
muscle actin (SMA), along with other immunological markers
including histone h3 lysine 27 trimethylation (H3K27Me3), mouse
double minute 2 homolog (MDM2), caldesmon and epithelial cadherin
(E-Cad). By contrast, the sample was negative for several markers
including cytokeratin (CK) (Fig.
3C), cluster of differentiation 117 (CD117), S-100 protein
(S-100), desmin (Des), CD34, human melanoma black 45 antigen
(HMB45), anaplastic lymphoma kinase (ALK), SRY-box transcription
factor 10 (SOX-10), signal transducer and activator of
transcription 6 (STAT6), tumor protein p63 (P63), CK5/6, CD68,
myogenic differentiation 1 (MyoD1), CD30, spalt-like transcription
factor 4 (SALL4), CK7, CD10, estrogen receptor (ER), discovered on
gist 1 (DOG-1) and cyclin-dependent kinase inhibitor 2a (P16).
Additionally, high expression of proliferation index (Ki-67) (70%
positive; Fig. 3D) was noted. IHC
protocol summary: The samples were fixed in 10% neutral buffered
formalin for 24–48 h at RT, embedded in paraffin and sectioned at a
thickness of 3–5 µm. After epitope retrieval (EDTA repair solution,
100°C, 20 min), samples were blocked with endogenous peroxidase
blocker included in the DAB Detection Kit (ready-to-use) for 10 min
at RT. They were then incubated with primary antibodies at RT for
40 min and then with secondary antibody (sheep anti-rat/rabbit IgG
polymer horseradish peroxidase; cat. no. PV8000D; ready-to-use;
Beijing Zhongshan Jinqiao Biotechnology Co., Ltd.) at RT for 15
min. Primary antibodies against EMA (cat. no. Kit-0011;
ready-to-use), CD117 (cat. no. Kit-0029; ready-to-use), CD34 (cat.
no. Kit-0004; ready-to-use), MyoD1 (cat. no. MAB-0822;
ready-to-use), CD30 (cat. no. MAB-0023; ready-to-use), SALL4 (cat.
no. MAB-0691; ready-to-use), CD10 (cat. no. MAB-0668;
ready-to-use), P16 (cat. no. MAB-0673; ready-to-use) and Des (cat.
no. MAB-0766; 1:100 dilution) were from Fuzhou Maixin Biotechnology
Development Co., Ltd. Primary antibodies against MDM2 (cat. no.
ZM-0425; ready-to-use), Cladesmon (cat. no. ZA-0535; ready-to-use),
E-Cad (cat. no. ZA-0565; ready-to-use), S-100 (cat. no. ZM-0224;
ready-to-use), HMB45 (cat. no. ZM-0187; ready-to-use), ALK (cat.
no. ZM-0848; ready-to-use), SOX-10 (cat. no. ZA-0624;
ready-to-use), STAT6 (cat. no. ZA-0647; ready-to-use), CK5/6 (cat.
no. ZM-0313; ready-to-use), CD68 (cat. no. ZM-0060; ready-to-use),
CK (cat. no. ZM-0069; 1:200), P63 (cat. no. ZM-0406; 1:200), CK7
(cat. no. ZM-0071; 1:100), Ki-67 (cat. no. ZM-0166; 1:200) and SMA
(cat. no. ZM-003; 1:100) were from Beijing Zhongshan Jinqiao
Biotechnology Co., Ltd. Primary antibodies against TLE1 (cat. no.
ab183742; 1:250), H3K27Me3 (cat. no. ab6002; 1:1,000) and ER (cat.
no. ab16660; 1:200) were from Abcam plc. Primary antibody against
DOG-1 (cat. no. 54598S; 1:200) was from Cell Signaling Technology,
Inc. Diaminobenzidine was used to visualize the staining and then
the slides were counterstained with hematoxylin, followed by
observation with a light microscope. Fluorescence in situ
hybridization (FISH) analysis revealed no significant amplification
of MDM2/centromere 12 (CEP12). FISH protocol summary: Tissue
samples were fixed in 10% neutral buffered formalin for 12–24 h and
routinely processed into paraffin blocks. Formalin-fixed
paraffin-embedded (FFPE) tissue sections (4 µm) were baked at 70°C
for 10 min, deparaffinized in xylene (10 min, 2 times) and
rehydrated through a graded ethanol series (100, 100, 90, and 70%;
5 min each). Heat pretreatment was performed using the Vysis
Paraffin Pretreatment Reagent Kit (Abbott Molecular, Inc.).
Briefly, slides were immersed in pretreatment solution at 80°C for
25–30 min, rinsed in distilled water (2 min, 2 times) and digested
with Protease IV at 37°C for 15 min. After a 3-min wash in
distilled water, sections were dehydrated in ethanol (70, 85 and
100%; 1 min each) and air-dried. The Vysis LSI MDM2/CEP12 FISH
Probe Kit (cat. no. 01N15-010; Abbott Molecular Inc.) was then
applied according to the manufacturer's instructions. Briefly, 10
µl of probe mixture was pipetted onto each specimen, covered with a
22×22 mm coverslip and sealed with rubber cement. Probe and target
DNA were co-denatured on a HYBrite denaturation/hybridization
system at 72°C for 5 min and hybridized overnight (16–24 h) at 37°C
in a humidified chamber. Post-hybridization washes were conducted
in prewarmed 0.4X saline-sodium citrate containing 0.3% Nonidet
P-40 at 73°C for 2 min, followed by dehydration in ethanol (70, 85
and 100%; 1 min each). Slides were counterstained with DAPI II
antifade solution (Abbott Molecular) and examined under a
fluorescence microscope equipped with single-bandpass filters for
DAPI (excitation 358–405 nm), Spectrum Green (excitation ~495 nm)
and Spectrum Orange (excitation ~546 nm), using a ×100
oil-immersion objective. Signal enumeration and MDM2/CEP12 ratio
calculations were performed using GenASIs software. A case was
considered MDM2-amplified when the MDM2/CEP12 signal ratio was ≥2.0
in at least 50 evaluable tumor nuclei. The EUS-FNA specimen was
sent to Shanghai Fudan University Affiliated Zhongshan Hospital
(Shanghai, China), where the SYT gene mutation was tested using
FISH; the result was negative. The EMA-positive results combined
with the morphological features suggested a diagnosis of SC or
synovial sarcoma. However, the absence of SYT gene mutation ruled
out the possibility of synovial sarcoma. Therefore, the patient was
diagnosed with EMA-positive SC [specifically mediastinal SC
(cT4N0M0, IIIA)] in February 2022. Although pathological findings
alone were inconclusive for determining tumor origin, when
considered in conjunction with radiological features, a pulmonary
origin was regarded as the most likely diagnosis.
The specimen obtained via bronchoscopy was sent to
Amoy Diagnostics Co., Ltd. for genomic and programmed cell death
ligand 1 (PD-L1) testing; no pathogenic gene mutations were
detected. PD-L1 expression was evaluated using Leica Bond-Max
(Leica Biosystems), with antibody clone E1L3N. The samples were
prepared into FFPE tissue section, with a thickness of 3–5 µm.
After epitope retrieval (Bond epitope retrieval ER2 solution,
100°C, 20 min), samples were blocked with peroxide block (included
in the Leica BOND Polymer Refine Detection kit; cat. no. DS9800;
ready-to-use; Leica Biosystems) at RT for 5 min. They were then
incubated with primary antibody (PD-L1 antibody; cat. no. 13684;
ready-to-use; Cell Signaling Technology, Inc.) at RT for 10 min and
then with secondary antibody (polymer; cat. no. DS9800;
ready-to-use; Leica Biosystems) at RT for 12 min. Diaminobenzidine
was used to visualize the staining and then the slides were
counterstained with hematoxylin, followed by observation with a
light microscope. Positive, negative and blank controls were
included in each staining run. The Positive control consisted of
one weakly positive and one strongly positive PD-L1-expressing
non-small cell lung cancer (NSCLC) formalin-fixed paraffin-embedded
tissue section. CPS was calculated as the ratio of viable tumor
cells and tumor-associated immune cells (lymphocytes and
macrophages) with any staining intensity to the total viable
invasive tumor cells, multiplied by 100. Pathologists determined
the final results via light microscopy. Firstly, the entire tissue
section was scanned at 10× magnification to ensure ≥100 viable
tumor cells for sample adequacy; then staining tumor cells and
tumor-associated immune cells were counted at 20× magnification
(confirmation at 40× magnification if needed) and applied to the
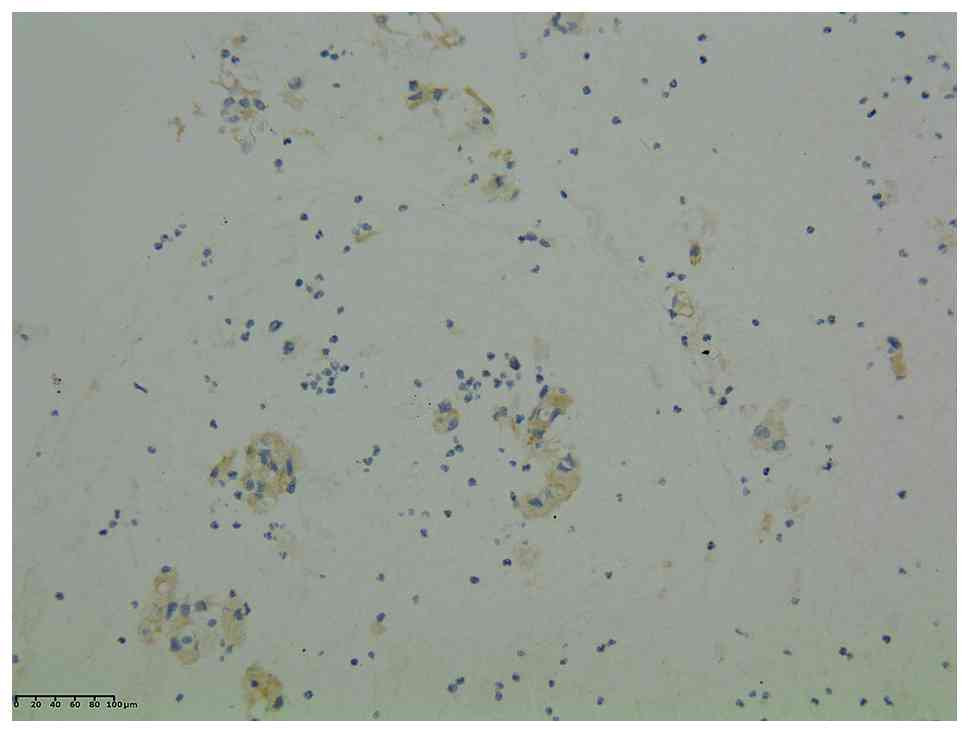
formula. Immunohistochemistry revealed high expression of PD-L1,
with a combined positive score (CPS) of 80 (Fig. 4).
Treatment process
The patient received multiple treatment protocols
consecutively. Initial first-line treatment, which commenced in
February 2022, consisted of chemotherapy (cisplatin and
albumin-bound paclitaxel) and antiangiogenic targeted therapy
(anlotinib; 12 mg once daily). Due to severe gastrointestinal
adverse reactions, the second chemotherapy regimen was changed to
carboplatin and albumin-bound paclitaxel in March 2022. Concurrent
radiotherapy (4,000 cGy/20F to 95% PTV) was initiated in March
2022, while anlotinib was maintained. After the second chemotherapy
cycle, treatment was discontinued due to a grade-3
myelosuppression. A chest CT in March 2022 revealed a mass
measuring 8.3×6.2 cm at the maximum cross-section (Fig. 5B), which was slightly decreased in
size compared with the initial measurement taken in January 2022
(Fig. 5A). The overall treatment
response was evaluated as stable disease (SD).
The patient received two cycles of immunotherapy
(durvalumab; 1,000 mg) in April 2022 and May 2022, whilst
continuing treatment with anlotinib (10 mg once daily). A total of
7 days after the second immunotherapy cycle, the patient developed
limb weakness, pain in the proximal limbs and chest pain, and was
subsequently hospitalized again in May 2022. In May 2022,
laboratory results demonstrated elevated levels of biomarkers,
including aspartate aminotransferase at 488 U/l (upper limit, 35
U/l), alanine aminotransferase at 209 U/l (upper limit, 40 U/l),
creatine kinase at 7,933 U/l (upper limit, 35 U/l), creatine kinase
isoenzyme MB at 142.65 µg/l (upper limit, 5 µg/l) and troponin T at
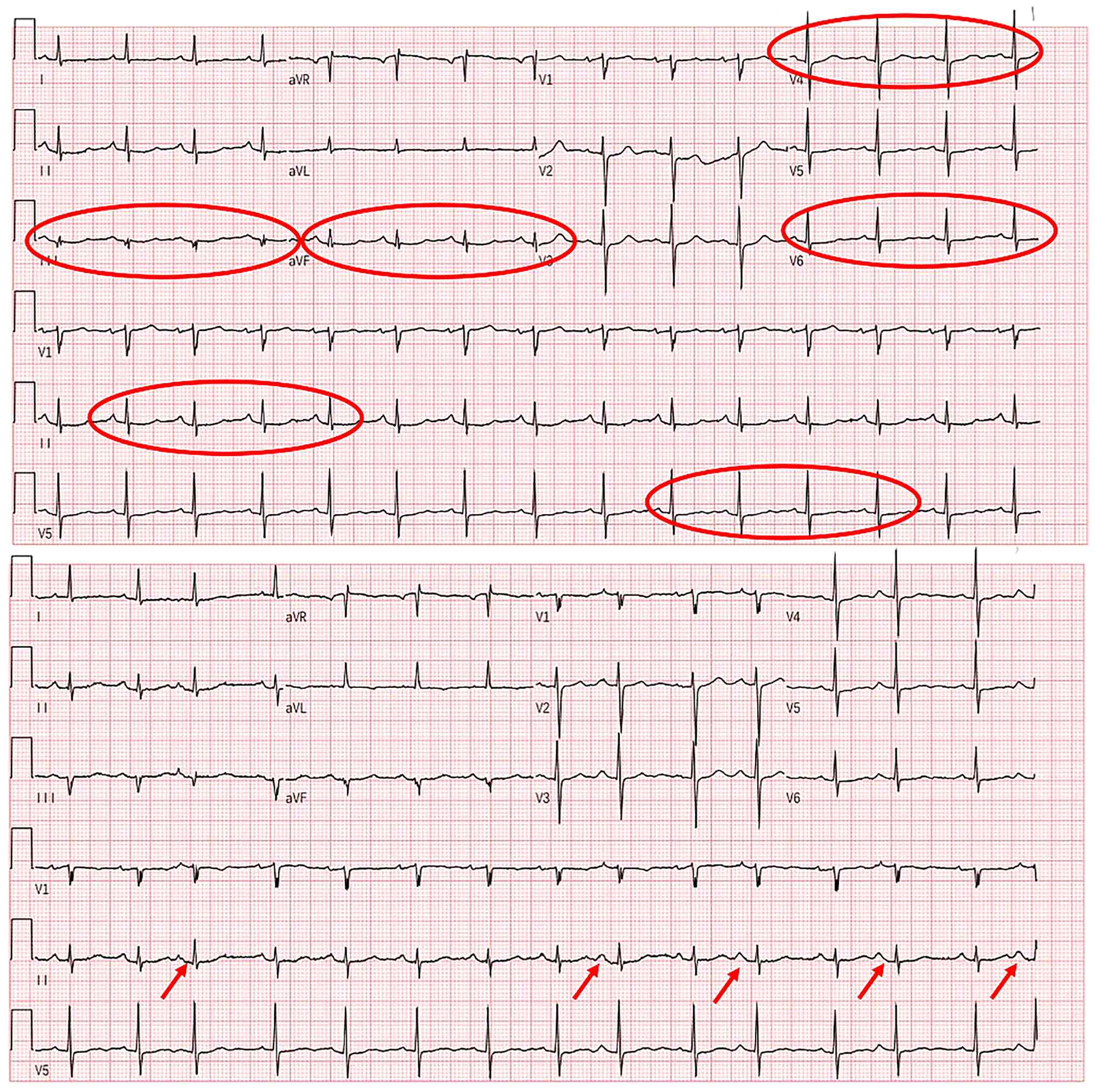
0.585 µg/l (upper limit, 0.014 µg/l). Results from an
electrocardiogram performed in May 2022 were normal. However, when
retested 8 days later in June 2022, ST-segment abnormalities and
frequent premature atrial beats were recorded (Fig. 6). Transthoracic echocardiography in
May 2022 demonstrated mild regurgitation of the aortic, mitral and
tricuspid valves. Single photon emission computed tomography
(SPECT) myocardial perfusion imaging performed in June 2022
revealed no significant perfusion defects in the left ventricular
myocardium and normal left ventricular systolic function.
During the exacerbation of symptoms, the patient
exhibited no fever or other infectious manifestations. Laboratory
results demonstrated normal leukocyte counts at 6.73×109/l
(reference range,3.50–9.50×109/l), normal neutrophil counts at
5.18×109/l (reference range, 1.8–6.3×109/l) and mildly elevated CRP
at 26 mg/l (upper limit, 8 mg/l). The magnitude of CRP elevation
was substantially disproportionate to the degree of clinical
worsening observed, thereby rendering an infectious etiology
unlikely. Serological tests demonstrated mildly elevated serum IgG
levels at 26.1 g/l (upper limit, 16 g/l), whereas antinuclear
antibodies profiles, antineutrophil cytoplasmic antibodies
profiles, rheumatoid factor, anti-cyclic citrullinated peptide,
immunoglobulins (IgA, IgM) and complements (C3, C4) were all
negative; hence, autoimmune diseases were excluded. Following
exclusion of infection and autoimmune diseases, and given the lack
of exposure to other potentially causative medications, the patient
was diagnosed with grade-3 immune-related myocarditis, grade-3
immune-related myositis and grade-3 immune-related hepatitis.
In May 2022, the patient started receiving high-dose
methylprednisolone (80 mg every 12 h). Additionally, intravenous
immunoglobulin pulse therapy (20 g/day) was administered for 3
days. The detailed methylprednisolone tapering regimen was as
follows: The patient received intravenous methylprednisolone 80 mg
every 12 h for 4 days, 40 mg every 8 h for 4 days, 40 mg every 12 h
for 6 days and 30 mg every 12 h for 6 days. The route was
subsequently switched to oral administration at 40 mg once daily
for 7 days, and further reduced to 32 mg once daily, followed by
gradual dose reduction for long-term maintenance. The patient
gradually recovered from the severe condition and was discharged in
June 2022. Due to the severe immune-related myocarditis, myositis
and hepatitis, immunotherapy was halted and long-term
anti-angiogenic targeted therapy with anlotinib (10 mg once daily)
was maintained, with the last prescription date in September
2025.
Treatment outcomes and follow-up
After two cycles of immunotherapy combined with
anti-angiogenic targeted therapy, the patient underwent multiple
follow-up chest CT scans. A chest CT in May 2022 (Fig. 5C) and July 2022 (Fig. 5D) indicated that the mediastinal
mass continued to shrink. In May 2022, the soft tissue mass was
5.5×4.8 cm at the maximum cross-sectional area. By July 2022, the
soft tissue mass had decreased to 3.5×2.4 cm, confirming a clinical
evaluation of partial response (PR). Subsequent follow-up chest CT
showed that the mediastinal mass remained stable until July 2025
(last chest CT date; Fig. 5E). FDG
PET was performed again in May 2024 and showed a soft tissue mass
in the right upper mediastinum with mildly increased FDG uptake,
suggesting tumor activity after therapy. At present (as of July
2025), the patient is alive and the PFS is >42 months. The
diagnostic procedures, therapeutic procedures and tumor responses
are all summarized in Table I.
 | Table I.Timeline of the case. |
Table I.
Timeline of the case.
| Date | February 2022 | February-March
2022 | March 2022 | April-May 2022 | May 2022-July
2025 |
|---|
| Event | Diagnosis | Chemotherapy,
anlotinib | Radiotherapy,
anlotinib | Immunotherapy,
anlotinib | anlotinib |
| Response | N/A | SD | SD | PR | PR |
| Toxicities | N/A | Gastrointestinal
adverse reactions and grade-3 myelosuppression | Not observed | Grade-3
immune-related myocarditis, myositis and hepatitis | Not observed |
Discussion
SC is a rare and aggressive subtype of cancer
(1). It is characterized by the
presence of both epithelial and mesenchymal components, with the
mesenchymal components considered epithelial in origin (2). The epithelial components typically
possess varying degrees of CK and EMA expression, while the
sarcomatoid components commonly express vimentin (2). Previous studies have shown an
increased Ki67 index in SC, which is associated with a worse
prognosis (11,12). In addition, a lack of CK expression
does not rule out the diagnosis of SC (12). In the present case report,
microscopy revealed the presence of scattered spindle and polygonal
cells, indicating mesenchymal differentiation. Immunohistochemical
analysis demonstrated positivity for EMA, confirming epithelial
origin, while high expression of Ki67 (70%) confirmed the
aggressiveness of tumor cell proliferation.
SC can occur in various systems and organs, but is
mainly in the respiratory system (1). The occurrence of SC in the mediastinum
is particularly rare. It typically originates from the thymus or
pulmonary tissue. Several case reports have previously documented
mediastinal thymic SC (5–9). However, to the best of our knowledge,
there has been only one published case report describing a patient
with mediastinal pulmonary SC (PSC) (10).
Differential diagnosis between thymic SC and PSC
remains challenging given their morphologic overlap, yet they carry
key therapeutic implications. As summarized in Table II, these two entities diverge
markedly in anatomic distribution, immunophenotype, molecular
profiles and treatment outcomes (13–16).
Specifically, thymic SC typically localizes to the anterior
mediastinum with possible CD5/CD117 positivity and lacks
well-defined driver mutations (13,14),
whereas PSC arises from pulmonary parenchyma, bronchus or posterior
mediastinum, shows MET/KRAS/EGFR/TP53/ALK alterations and exhibits
distinct immunohistochemistry patterns (15,16).
| Table II.Comparison between pulmonary SC and
thymic SC. |
Table II.
Comparison between pulmonary SC and
thymic SC.
| Diseases | Pulmonary SC | Thymic SC | (Refs.) |
|---|
| Incidence | 0.3–3% of all
pulmonary types of cancer | ~4% of thymic types
of cancer | (13,15) |
| Location | Lung; trachea and
bronchus; posterior mediastinum, involving trachea/bronchus | Anterior
mediastinum | (14,15) |
| IHC markers | CKs+;
EMA+; vimentin+; TTF-1+ and Napsin
A+ in case of adenocarcinoma origin; p40+ and
high-molecular-weight CKs+ in case of squamous cell
carcinoma origin | CK+;
vimentin+; CK5/6+; CK7+;
p63/p40+; PAX8+; CD5+/−;
CD117+/− | (14,15) |
| Molecular | MET exon 14
skipping mutation; KRAS | Not reported | (14,15) |
| landscape | (mostly G12C)
mutation; EGFR mutation; TP53 mutation; ALK mutation; |
|
|
| Treatments | Surgery; molecular
targeted therapy; immunotherapy; chemotherapy; radiotherapy | Surgery; standard
chemotherapy/radiotherapy, subtype-specific data lacking | (14–16) |
| Prognosis | Median OS: 6.3
months in the chemotherapy era; 22.8 months in the immunotherapy
era (small-scale retrospective study); | OS: 2 months to 3
years [no statistical data, only case reports] | (5–9,16) |
In the present case, the absence of p63, CK5/6 and
CK7 expression argues against a conventional pulmonary squamous
cell carcinoma origin, while the absence of TTF-1 and Napsin A
staining data precludes definitive determination of a pulmonary
adenocarcinoma origin. Additionally, the positive EMA staining
confirms the epithelial derivation of this neoplasm. Due to
exhaustion of available tissue specimens, additional
immunohistochemical staining for TTF-1 and Napsin A could not be
performed. However, SC frequently undergo extensive
epithelial-mesenchymal transition, resulting in diminished or
complete loss of conventional lung-lineage markers, including
TTF-1, Napsin A, p63 and CK5/6 (17). Therefore, the absence of these
immunohistochemical markers does not necessarily exclude a
pulmonary origin. The pathological findings, in conjunction with
radiological examination, support a clinical diagnosis of PSC in
the present case report.
The prognosis for SC is generally unfavorable
(2). Specifically, patients with
PSC have a median overall survival (OS) of ~6.3 months (3). For individuals with mediastinal thymic
SC, the OS ranges from 2 months to 3 years (6–9).
However, due to the rarity of thymic SC, comprehensive statistical
data regarding OS remains unavailable. Although, with the emergence
of novel treatment methods, the therapeutic effects and survival
time for PSC have improved notably.
Similar to other types of cancer, patients with
early-stage SC can benefit from surgical intervention. Patients
with SC of the lungs or liver who receive surgical treatment
generally have longer OS than those who do not (18,19). A
case report describing a case of mediastinal thymic SC reported
that the patient had an OS of 13 months after receiving surgery as
the only treatment (6).
For advanced stage SC, the therapeutic efficacy of
chemotherapy remains modest. According to Vieira et al
(20), the median PFS of patients
with PSC receiving first-line chemotherapy was 2.0 months, and the
median OS was 6.3 months (20).
This was markedly shorter than other NSCLC subtypes (median PFS,
4.3 months; median OS, 8.9 months) (21). Similarly, chemotherapy regimens that
are effective for other intestinal malignancies have demonstrated
limited efficacy in patients with small-intestinal SC (22). This is demonstrated by a case report
describing a patient with thymic SC who experienced progressive
disease after two cycles of chemotherapy with paclitaxel and
carboplatin (8).
Studies on the effect of radiotherapy in SC have
different outcomes. For example, in a retrospective study, patients
with PSC who received adjuvant radiotherapy had a 5-year survival
rate of 55.4%, while those who did not had a 5-year survival rate
of 29.4% (P<0.01) (23).
However, Rahouma et al (24)
reported a decreased OS for patients with PSC who received
radiotherapy. Furthermore, a study by Zhu et al (22) concluded that radiotherapy is
ineffective for small intestine SC. Although, one case report
described a patient with thymic SC that had an OS of 28 months
after chemotherapy and radiotherapy, indicating the possible
effectiveness of radiotherapy in thymic SC (8).
In the present case report, after two cycles of
chemotherapy and one cycle of radiotherapy, the efficacy evaluation
was considered SD. This indicated the limited effectiveness of
chemotherapy and radiotherapy in mediastinal SC, but further
studies are needed to confirm this.
Immune checkpoint inhibitors (ICIs) monotherapy or
combination therapy have shown good efficacy in NSCLC and other
types of epithelial cancer (25).
Multiple studies have shown that ICIs achieve substantially
improved outcomes in patients with advanced NSCLC with high PD-L1
expression (tumor proportion score, ≥50%) compared with
conventional chemotherapy (25–27).
At present, PD-L1 is an FDA-approved biomarker for predicting the
efficacy of ICIs in patients with pulmonary cancer (25). PD-L1 has high expression in PSC,
with expression in the sarcomatoid component higher than in the
epithelial component (28). A
retrospective study showed that 83% of cases with pancreatic SC had
a CPS ≥1 and 50% of the cases had a CPS ≥50 (29).
There are several retrospective studies
investigating the efficacy of ICIs in SC. In a study by Roesel
et al (30), patients with
PSC had favorable responses to ICIs after first-line and
second-line chemotherapy failed to show positive results. Qian
et al (31) reported a
median PFS of 9.2 months and median OS of 22.8 months in a cohort
of 21 patients with PSC that received first-line immunotherapy
(31), notably surpassing the
2.0-month PFS and 6.3-month OS previously observed with
chemotherapy alone (20). Notably,
there are no statistical differences in PFS or OS among different
ICIs (31). In a retrospective
study, PD-L1-positive patients with PSC have longer median PFS than
PD-L1-negative patients (17.50 months vs. 6.07 months; P=0.812)
(32). Wang et al (33) also observed that ICIs demonstrate
enhanced efficacy in patients with SC of the head and neck that
have higher PD-L1 expression. These two studies indicate that PD-L1
may be a useful biomarker for predicting the effect of ICIs in
advanced SC. However, more prospective studies are required to
confirm this.
Angiogenesis is essential for the growth and
metastasis of carcinomas; consequently, anti-angiogenic targeted
therapy has been widely used in epithelial cancer as second-line or
subsequent treatments (34). In
terms of SC, anti-angiogenic targeted therapy has shown favorable
efficacy in PSC. Specifically, anti-angiogenic monotherapy with
apatinib has shown favorable efficacy in a patient with PSC with no
notable adverse side effects (34).
A retrospective study included 16 patients with PSC who received
chemotherapy combined with bevacizumab or chemotherapy alone.
Patients receiving combination therapy achieved a median PFS of 4.2
months and an OS of 11.2 months, outperforming chemotherapy-alone
(median PFS, 1.2 months; OS, 7.9 months) (35). Anlotinib is a multi-target tyrosine
kinase inhibitor of tumor neovascularization, which has shown
favorable efficacy in SC as well as in epithelial cancer. In one
case report, a patient with PSC achieved complete response for
>20 months after treatment with anlotinib combined with
tislelizumab as a second-line treatment (36). Furthermore, a patient with recurrent
SC of the head and neck achieved long term PFS (>2 years) after
treatment with sintilimab combined with anlotinib (33).
The tumor microenvironment (TME) functions as a key
determinant in modulating immune responses and can impact the
efficacy of ICIs (37). The
anti-tumor immune response begins with the release of tumor cell
antigen, followed by antigen processing and presentation by
antigen-presenting cells (APCs), subsequent priming and
mobilization of adaptive immunity, translocation of effector
lymphocytes to the tumor site, infiltration of these immune
effectors in the TME, recognition and finally destruction of cancer
cells by effector cytotoxic T lymphocytes (mainly CD8+ T
lymphocytes) (37). The vascular
landscape within the TME, along with diverse immune cells and
cytokines, exerts distinct modulatory effects on the antitumor
immune response. By modulating these elements, the efficacy of
immunotherapy can be influenced.
The patient described in the present case report
achieved PR following two cycles of durvalumab combined with
anlotinib, despite having only achieving SD with prior treatment
with chemoradiotherapy and anlotinib. This sequential efficacy
pattern raises important questions regarding the baseline immune
status of the tumor and the potential role of anlotinib and
chemoradiotherapy in remodeling the TME.
The elevated CPS of 80 in the present case indicates
a potentially immune-hot TME. The high PD-L1 expression likely
reflects an adaptive reaction to lymphocyte-derived cytokines,
specifically IFN-γ released by cytotoxic CD8+ cells. Paradoxically,
the same immune surveillance that detects malignancy simultaneously
equips the tumor with inhibitory defenses, creating a primed yet
suppressed microenvironment where ICIs can unleash pre-existing
antitumor potential (38). However,
while frequently associated with elevated PD-L1 levels, this is not
a universal rule, and necessitates further immunohistochemical
validation.
We hypothesize that the prior chemoradiotherapy and
anlotinib treatment may have functioned as a ‘priming’ phase that
further amplified this pre-existing immune-hot state. As documented
in the literature, chemoradiotherapy triggers immunogenic cell
death mechanisms, leading to the liberation of tumor-specific
antigens, alongside various damage-associated molecular patterns,
which include heat shock proteins (HSP70/90), high-mobility group
box 1 and calreticulin (39). These
molecules can promote the maturation of APCs and potentiate CD8+ T
cell functions (36). Furthermore,
platinum agents can reshape immune landscapes by selectively
eliminating myeloid-derived suppressor cells and regulatory T
cells, thus relieving the inhibition of effector T cells (39). Simultaneously, radiotherapy promotes
type I interferon responses and enhances dendritic cell (DC)
cross-presentation, thus strengthening antitumor immunity (40).
Anlotinib appears to exert synergistic effects when
combined with immunotherapy during cancer treatment. Mouse models
of different types of cancer show that anlotinib can enhance ICIs
efficacy through remodeling of tumor vasculature (41,42).
Vascular normalization can reverse the immunosuppressive state of
tumors and allow CD8+ T cells to infiltrate tumors
(41,42). Anlotinib can also downregulate PD-1,
mucin domain-containing protein 3, immune checkpoint T-cell
immunoglobulin and lymphocyte-activation gene 3, as well as
increase the secretion of IFN-γ and TNF-α from T cells, thus
preserving CD8+ T-cell cytotoxicity (41,42).
Furthermore, anlotinib can increase the levels of M1-polarized
macrophages and reduce M2 subtypes, enhance major
histocompatibility complex-I/II expression on tumor cells and
promote DC maturation and antigen presentation, thus shifting the
TME from an immunosuppressive to an immunostimulatory state and
sustain immune memory (42).
Accordingly, we hypothesize that prior exposure to anlotinib could
potentiate tumor responsiveness to immunotherapeutic
interventions.
However, it must be acknowledged that without serial
biopsies during treatment, a definitive distinction cannot be made
between: i) A pre-existing immune-hot TME that was activated by
ICIs; ii) an anlotinib-mediated conversion from an intermediate
state to an immune-hot state; and iii) the induction of an
immune-hot TME state by chemoradiotherapy. Nevertheless, due to
evidence from prior studies, the high baseline CPS and the pattern
of treatment response, it may be hypothesized that the patient
exhibited a baseline immune-hot state that was subsequently
amplified by chemoradiotherapy and in particular anlotinib.
Although immunotherapy demonstrated promising
efficacy, it was terminated due to severe adverse events in the
present case. Maintenance therapy with anlotinib was continued and
the tumor remains stable to date. To the best of our knowledge,
this case study is among the first case reports to investigate the
efficacy of ICIs and anti-angiogenic targeted therapy in
mediastinal SC. The present case demonstrates the efficacy of
immunotherapy combined with anlotinib on mediastinal SC with high
expression of PD-L1.
There are several possible mechanisms underlying the
sustained efficacy of anlotinib after ICI discontinuation in the
present case. Firstly, treatment-free survival after
discontinuation of ICIs has been observed in numerous patients with
objective response, especially in those who stop use of ICIs due to
immune-related adverse events (43). ICIs achieve clinical efficacy by
activation and expansion of T and B lymphocytes, including memory T
cells. Memory T cells can exhibit notable longevity and can exert
an antitumor response following recognition of tumor-associated
antigens; consequently, ICIs may maintain efficacy following
discontinuation (43). Furthermore,
immunotherapy combined with anlotinib appears to exert synergistic
effects in cancer treatment as previously described (41,42).
Through pleiotropic mechanisms, anlotinib reverses TME
immunosuppression while promoting antigen-specific memory T cell
persistence (41,42). Consequently, Even ICIs is stopped,
anlotinib can sustain the efficacy of it.
In conclusion, the present case report demonstrates
the potential of ICIs combined with anti-angiogenic targeted
therapy in treating PD-L1-positive mediastinal SC, despite the
life-threatening adverse reactions caused by ICIs. However, more
prospective studies are required to confirm its efficacy and
safety.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
SW and DW were responsible for data collection,
literature review and writing the manuscript. SW and QF were
responsible for collecting images and data. SW, YD made substantial
contributions to conception and design, revising the manuscript
critically for important intellectual content. All authors have
read and approved the manuscript. SW and YD confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
The study was approved by the Medical Ethics
Committee of The First People's Hospital of Xiaoshan District
(approval no. XYYLS Zi 2025No.01).
Patient consent for publication
Written informed consent was obtained from the
patient's legal representative for the publication of this case
report, including the publication of all images, clinical data and
other data included in the manuscript.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Xu Z, Wang L, Tu L, Liu Y, Xie X, Tang X
and Luo F: Epidemiology of and prognostic factors for patients with
sarcomatoid carcinoma: A large population-based study. Am J Cancer
Res. 10:3801–3814. 2020.PubMed/NCBI
|
|
2
|
Malla M, Wang JF, Trepeta R, Feng A and
Wang J: Sarcomatoid carcinoma of the urinary bladder. Clin
Genitourin Cancer. 14:366–372. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Li X, Wu D, Liu H and Chen J: Pulmonary
sarcomatoid carcinoma: Progress, treatment and expectations. Ther
Adv Med Oncol. 12:17588359209502072020. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Liao SH, Su TH, Jeng YM, Liang PC, Chen
DS, Chen CH and Kao JH: Clinical manifestations and outcomes of
patients with sarcomatoid hepatocellular carcinoma. Hepatology.
69:209–221. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Piao ZH, Chen JP, Chen HR and Zhou XC:
Malignant transformation of metaplastic thymoma into high-grade
sarcomatoid carcinoma: A case report. Int J Surg Pathol.
30:564–568. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Moritani S, Ichihara S, Mukai K, Seki Y,
Inoue S, Yasuda A, Hakiri S, Yatabe Y and Eimoto T: Sarcomatoid
carcinoma of the thymus arising in metaplastic thymoma.
Histopathology. 52:409–411. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Wick MR, Scheithauer BW, Weiland LH and
Bernatz PE: Primary thymic carcinomas. Am J Surg Pathol. 6:613–630.
1982. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Shimizu J, Kamesui T, Moriya M, Murata S,
Nakanishi I, Sasaki M and Minato H: Four cases of invasive anterior
mediastinal tumors definitively diagnosed by the chamberlain
procedure. Ann Thorac Cardiovasc Surg. 20:434–440. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Chalabreysse L, Etienne-Mastroianni B,
Adeleine P, Cordier JF, Greenland T and Thivolet-Bejui F: Thymic
carcinoma: A clinicopathological and immunohistological study of 19
cases. Histopathology. 44:367–374. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Wang Y, Yang L, Wang J, Gui L, Li W, Liu
Z, Ma X, Yang Y, Wang L and Bi N: Case report: First case of
consolidation immunotherapy after definitive chemoradiotherapy in
mediastinal lymph node metastatic sarcomatoid carcinoma. Front
Oncol. 11:7888562022. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Karakuchi N, Yanagawa S, Kushitani K,
Kodama S, Takeshima Y and Sumimoto K: Primary small intestinal
sarcomatoid carcinoma: Report of a rare case and literature review.
Case Rep Oncol. 14:538–544. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Wenig BM: Squamous cell carcinoma of the
upper aerodigestive tract: Dysplasia and select variants. Mod
Pathol. 30 (Suppl 1):S112–S118. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Marx A, Chan JKC, Chalabreysse L, Dacic S,
Detterbeck F, French CA, Hornick JL, Inagaki H, Jain D, et al: The
2021 WHO Classification of Tumors of the Thymus and Mediastinum:
What is New in Thymic, Epithelial, Germ Cell, and Mesenchymal
Tumors? J Thorax Oncol. 17:200–213. 2022. View Article : Google Scholar
|
|
14
|
Weissferdt A: Spindle cell thymoma and its
histological mimickers. Mediastinum. 7:322023. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Baldovini C, Rossi G and Ciarrocchi A:
Approaches to tumor classification in pulmonary sarcomatoid
carcinoma. Lung Cancer (Auckl). 10:131–149. 2019.PubMed/NCBI
|
|
16
|
Ding K, Peng Z and Xu Y: Role of
immunotherapy in pulmonary sarcomatoid carcinoma: Review of current
approaches and related biomarkers. Ther Adv Med Oncol.
16:175883592412490412024. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Huang Y, Guo J, Li S, Liu J, Xu J, Ye W,
Zhang L, Dong Z, Wu W and Wu C: The correlation between histologic,
immunophenotypic, and molecular characteristics of pulmonary
sarcomatoid carcinoma reveals that sarcomatoid change is
potentially derived from epithelial carcinoma cells undergoing
epithelial-mesenchymal transition. Appl Immunohistochem Mol
Morphol. 31:17–25. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zeng Q, Li J, Sun N, Xue Q, Gao Y, Zhao J,
Mao Y, Mu J, Wang D, Gao S and He J: Preoperative systemic
immune-inflammation index predicts survival and recurrence in
patients with resected primary pulmonary sarcomatoid carcinoma.
Transl Lung Cancer Res. 10:18–31. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Ma S, Li C, Ma Y, Wang X, Zhang D and Lu
Z: A retrospective study on the clinical and pathological features
of hepatic sarcomatoid carcinoma: Fourteen cases of a rare tumor.
Medicine (Baltimore). 101:e300052022. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Vieira T, Girard N, Ung M, Monnet I, Cazes
A, Bonnette P, Duruisseaux M, Mazieres J, Antoine M, Cadranel J and
Wislez M: Efficacy of first-line chemotherapy in patients with
advanced lung sarcomatoid carcinoma. J Thorac Oncol. 8:1574–1577.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Lara PN Jr, Redman MW, Kelly K, Edelman
MJ, Williamson SK, Crowley JJ and Gandara DR; Southwest Oncology
Group, : Disease control rate at 8 weeks predicts clinical benefit
in advanced non-small-cell lung cancer: Results from southwest
oncology group randomized trials. J Clin Oncol. 26:463–467. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhu Z, Liu X, Li W, Wen Z, Ji X, Zhou R,
Tuo X, Chen Y, Gong X, Liu G, et al: A rare multiple primary
sarcomatoid carcinoma (SCA) of small intestine harboring driver
gene mutations: A case report and a literature review. Transl
Cancer Res. 10:1150–1161. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sun L, Dai J, Chen Y, Duan L, He W, Chen
Q, Wang H, Zhu Y, Zhang H, Jiang G and Zhang P: Pulmonary
sarcomatoid carcinoma: Experience from SEER database and Shanghai
pulmonary hospital. Ann Thorac Surg. 110:406–413. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Rahouma M, Kamel M, Narula N, Nasar A,
Harrison S, Lee B, Stiles B, Altorki NK and Port JL: Pulmonary
sarcomatoid carcinoma: An analysis of a rare cancer from the
surveillance, epidemiology, and end results database. Eur J
Cardiothorac Surg. 53:828–834. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Reck M, Rodríguez-Abreu D, Robinson AG,
Hui R, Csőszi T, Fülöp A, Gottfried M, Peled N, Tafreshi A, Cuffe
S, et al: Pembrolizumab versus chemotherapy for PD-L1-positive
non-small-cell lung cancer. N Engl J Med. 375:1823–1833. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Mok TSK, Wu YL, Kudaba I, Kowalski DM, Cho
BC, Turna HZ, Castro G Jr, Srimuninnimit V, Laktionov KK,
Bondarenko I, et al: Pembrolizumab versus chemotherapy for
previously untreated, PD-L1-expressing, locally advanced or
metastatic non-small-cell lung cancer (KEYNOTE-042): A randomised,
open-label, controlled, phase 3 trial. Lancet. 393:1819–1830. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Sezer A, Kilickap S, Gümüş M, Bondarenko
I, Özgüroğlu M, Gogishvili M, Turk HM, Cicin I, Bentsion D, Gladkov
O, et al: Cemiplimab monotherapy for first-line treatment of
advanced non-small-cell lung cancer with PD-L1 of at least 50%: A
multicentre, open-label, global, phase 3, randomised, controlled
trial. Lancet. 397:592–604. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kim S, Kim MY, Koh J, Go H, Lee DS, Jeon
YK and Chung DH: Programmed death-1 ligand 1 and 2 are highly
expressed in pleomorphic carcinomas of the lung: Comparison of
sarcomatous and carcinomatous areas. Eur J Cancer. 51:2698–2707.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Silvestris N, Argentiero A, Brunetti O,
Sonnessa M, Colonna F, Delcuratolo S, Luchini C, Scarpa A, Lonardi
S, Nappo F, et al: PD-L1 and Notch as novel biomarkers in
pancreatic sarcomatoid carcinoma: a pilot study. Expert Opin Ther
Targets. 25:1007–1016. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Roesel C, Kambartel K, Kopeika U, Berzins
A, Voshaar T and Krbek T: Lazarus-type tumour response to therapy
with nivolumab for sarcomatoid carcinomas of the lung. Curr Oncol.
26:e270–e273. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Qian X, Wang Y, Liu F, Yuan Y, Fang C,
Zhang X, Yuan S, Chen R, Yu B, Wang T, et al: The efficacy and
safety analysis of first-line immune checkpoint inhibitors in
pulmonary sarcomatoid carcinoma. Front Immunol. 13:9569822022.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Wei JW, Hao Y, Xiang J, Pu XX, Wang LP,
Jiang ZS, Wu JX, Wang Q, Xu CW, Wang WX and Song ZB: The prognostic
impact of immune checkpoint inhibitors for the treatment of
pulmonary sarcomatoid carcinoma: A multicenter retrospective study.
Neoplasma. 69:1437–1444. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wang L, Huang Y and Sun X: Sintilimab
combined with anlotinib as first-line treatment for advanced
sarcomatoid carcinoma of head and neck: A case report and
literature review. Front Oncol. 14:13621602024. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Li X, He Y, Zhu J, Pang H, Lin Y and Zheng
J: Apatinib-based targeted therapy against pulmonary sarcomatoid
carcinoma: A case report and literature review. Oncotarget.
9:33734–33738. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Oizumi S, Takamura K, Harada T, Tachihara
M, Morikawa N, Honda R, Watanabe S, Asao T, Kunisaki M, Fukuhara T,
et al: Phase II study of carboplatin-paclitaxel alone or with
bevacizumab in advanced sarcomatoid carcinoma of the lung:
HOT1201/NEJ024. Int J Clin Oncol. 27:676–683. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Li YF, Zhao XF, Tian Y, Xiao XY, Yan CY
and Shen H: Case report: Pulmonary sarcomatoid carcinoma
complicating TP53 mutation treated successfully with Tislelizumab
combined with Anlotinib-a case report. Front Genet. 13:9499892022.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Wang P, Xu S, Guo Q and Zhao Y: Discovery
of PAK2 as a key regulator of cancer stem cell in head and neck
squamous cell carcinoma using multi-omic techniques. Stem Cells
Int. 2025:13252622025. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Dosset M, Vargas TR, Lagrange A, Boidot R,
Végran F, Roussey A, Chalmin F, Dondaine L, Paul C, Lauret
Marie-Joseph E, et al: PD-1/PD-L1 pathway: An adaptive immune
resistance mechanism to immunogenic chemotherapy in colorectal
cancer. Oncoimmunology. 7:e14339812018. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Wang Y, Lu K, Xu Y, Xu S, Chu H and Fang
X: Antibody-drug conjugates as immuno-oncology agents in colorectal
cancer: Targets, payloads, and therapeutic synergies. Front
Immunol. 16:16789072025. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Saxena A: Combining radiation therapy with
immune checkpoint blockade for the treatment of small cell lung
cancer. Semin Cancer Biol. 90:45–56. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Shan Y, Zhong C, Ni Q, Zhang M, Wang G and
Zhou F: Anlotinib enhanced penpulimab efficacy through remodeling
of tumor vascular architecture and immune microenvironment in
hPD-L1/hPD-1 humanized mouse model. J Clin Oncol. 39
(15Suppl):S25812021. View Article : Google Scholar
|
|
42
|
Su Y, Luo B, Lu Y, Wang D, Yan J, Zheng J,
Xiao J, Wang Y, Xue Z, Yin J, et al: Anlotinib induces a T
cell-inflamed tumor microenvironment by facilitating vessel
normalization and enhances the efficacy of PD-1 checkpoint blockade
in neuroblastoma. Clin Cancer Res. 28:793–809. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Vacher L, Bernadach M, Molnar I,
Passildas-Jahanmohan J and Dubray-Longeras P: The efficacy of
immune checkpoint inhibitors following discontinuation for
long-term response or toxicity in advanced or metastatic
non-small-cell lung cancers: A retrospective study. Health Sci Rep.
7:e18252024. View Article : Google Scholar : PubMed/NCBI
|