Introduction
Malignant tumors are now the third leading cause of
death among hemodialysis (HD) patients in Japan (1). Therefore, appropriate cancer
management in HD patients is increasingly important for improving
clinical outcomes. Colorectal cancer (CRC), the second leading
cause of cancer-related death in Japan, is among the most
frequently observed malignancies in the HD population (2,3).
Systemic treatment for metastatic CRC (mCRC) has advanced
substantially in the general population. However, treatment
selection remains challenging due to disease heterogeneity and the
presence of distinct molecular subtypes. Traditionally, management
relied on 5-fluorouracil (5-FU)-based chemotherapy; more recently,
targeted therapies tailored to specific molecular subtypes and
primary tumor location have been developed (4). In addition, immune checkpoint
inhibitors have become an established option for selected patients
with mismatch repair-deficient or microsatellite instability-high
tumors (4). These advances have
improved survival outcomes, with 5-year survival rates approaching
26% in mCRC cohorts (5).
However, patients undergoing HD are frequently
excluded from clinical trials (6).
Consequently, data on safety, efficacy, optimal dosing and
appropriate timing of dialysis in relation to systemic therapy
remain limited, and no standardized treatment strategy has been
established for this population.
In HD patients, the pharmacokinetics of anticancer
drugs are profoundly influenced by drug-specific characteristics,
such as molecular weight, plasma protein binding and volume of
distribution (7). Consequently,
several cytotoxic agents and molecularly targeted agents commonly
used for the treatment of mCRC require strict dose modifications in
this setting, and chemotherapy in HD patients must be carefully
individualized based on pharmacokinetic considerations and clinical
tolerance (8). Accumulating these
individualized clinical management data is an essential step toward
establishing evidence-based, standardized therapies for the HD
population.
The present study reported on the case of an HD
patient with mCRC who was safely treated with sequential
chemotherapy through individualized dose and schedule
modifications.
Case report
A 61-year-old man with CRC underwent
laparoscopy-assisted low anterior resection with D3 lymph node
dissection at an external hospital in April 2014. Histopathological
examination revealed adenocarcinoma staged as pT3N1M0 (pStage IIIB)
according to the Union for International Cancer Control TNM
Classification, 7th edition (9).
The patient received adjuvant chemotherapy with S-1 for 4 months,
followed by uracil/tegafur for 5 months. In November 2018, the
patient developed a hepatic recurrence in segment S5, which was
treated with partial hepatectomy. A right lower lobectomy was
performed for a new pulmonary recurrence in February 2020. After 8
months, the patient underwent partial transverse colectomy, partial
hepatectomy and cholecystectomy for hepatic and peritoneal
recurrences, followed by oral uracil-tegafur plus leucovorin
therapy (exact dosing regimen could not be confirmed from the
available records at an external hospital).
HD was initiated in August 2023 because of
progressive chronic renal failure secondary to focal segmental
glomerulosclerosis. In October 2024, imaging revealed multiple
metastatic lesions involving the abdominal wall, right lung, liver
and the region adjacent to the hepatic portion of the inferior vena
cava. Later that month, as the previous hospital lacked experience
administering chemotherapy to patients undergoing dialysis, the
patient was referred to our university hospital (Nara Medical
University Hospital, Kashihara, Nara, Japan) to evaluate the safe
administration of anticancer therapy under HD.
The patient had an Eastern Cooperative Oncology
Group performance status (PS) of 0 (10). Molecular analysis of the recurrent
colorectal tumor was performed on a formalin-fixed
paraffin-embedded surgical specimen resected in October 2020.
Analysis using the MEBGEN RASKET-B kit (Medical & Biological
Laboratories) demonstrated wild-type status for KRAS, NRAS,
and BRAF. Additionally, a multiplex PCR-based assay for
microsatellite instability (MSI) demonstrated a
microsatellite-stable (MSS) status. Given the tumor characteristics
(left-sided, RAS/BRAF wild-type) and PS,
continuous-infusion 5-FU-based doublet chemotherapy combined with
an anti-epidermal growth factor receptor (EGFR) antibody would
typically be considered a first-line treatment option. However,
these regimens require a 46-h continuous infusion of 5-FU and close
coordination with HD (11,12), which was logistically challenging
because the dialysis facility was located ~1 h from our hospital.
In addition, FOLFOX (folinic acid, 5-FU and oxaliplatin) is often
administered with HD initiated soon after oxaliplatin infusion, and
the addition of an anti-EGFR antibody would have further prolonged
treatment time (11,12). Therefore, these regimens were
considered impractical, and reduced-dose capecitabine plus
oxaliplatin (XELOX) was initiated in November 2024.
The capecitabine and oxaliplatin doses were reduced
to 1,000 mg/m2/day for 14 days (50% of the standard
dose) and 70 mg/m2 on day 1 (54% of the standard dose),
respectively, based on previous reports (13,14).
The patient underwent HD three times weekly (Monday, Thursday and
Saturday), and each chemotherapy cycle started on Monday morning
before HD. Blood counts, renal function and electrolytes were
monitored weekly.
After the first cycle, the patient experienced
fatigue [Grade 2; Common Terminology Criteria for Adverse Events
(CTCAE) v5.0 (15)]. Platelet count
decreased (Grade 2; CTCAE v5.0, platelet count,
6.6×104/µl; institutional reference range,
15.8–34.8×104/µl) and hyperkalemia (serum K+,
7.0 mEq/l; institutional reference range, 3.6–4.8 mEq/l). Sodium
polystyrene sulfonate (15 g/day) controlled the hyperkalemia.
Following a 1-week delay to allow platelet count recovery, the
second cycle was initiated. Grade 2 fatigue persisted and Grade 2
platelet count decreased recurred during the second cycle (platelet
count, 5.9×104/µl). The patient completed two cycles of
XELOX without any serious adverse events. After 2 months of XELOX
therapy, serum carcinoembryonic antigen (CEA) levels (institutional
reference range, ≤5.0 ng/ml) increased, and computed tomography
(CT) showed that the previously identified abdominal wall
dissemination, liver metastases and the lesion adjacent to the
right side of the hepatic portion of the inferior vena cava had
become enlarged (data not shown). Although these findings met the
Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1
criteria for stable disease (16),
the overall clinical effect was deemed insufficient and the
treatment strategy was changed.
Irinotecan monotherapy was initiated as second-line
treatment for unresectable recurrent rectal cancer in February
2025. The dialysis schedule remained unchanged. As no validated
HD-specific dosing algorithm exists for patients undergoing HD,
irinotecan was initiated at 120 mg/m2 (80% of the
standard dose) on a biweekly schedule. Subsequent dose adjustments
were made pragmatically based on the patient's observed toxicity.
Uridine diphosphate glucuronosyltransferase 1A1
(UGT1A1) genotyping for *28 and *6 was
performed by SRL, Inc., using a PCR-based assay. Despite the
patient being homozygous wild-type for both UGT1A1*28 and
UGT1A1*6, diarrhea (Grade 3; CTCAE v5.0) occurred. The dose
was subsequently reduced to 105 mg/m2 (70% of the
standard dose) from the second cycle. As Grade 2 diarrhea
persisted, the dose was further reduced to 90 mg/m2 (60%
of the standard dose) from the fifth cycle. The patient received a
total of 14 cycles over 7 months. Follow-up CT revealed a new left
pulmonary metastasis (data not shown), meeting the RECIST version
1.1 criteria for progressive disease (PD), leading to
discontinuation of irinotecan.
Regorafenib was initiated as third-line treatment in
September 2025 at 40 mg/day on a 3-weeks-on/1-week-off schedule,
based on a previous report (17).
This starting dose corresponded to 25% of the standard dose and the
dialysis schedule remained unchanged. Although the patient
developed hypertension (Grade 3; CTCAE v5.0), it was successfully
managed with oral amlodipine 5 mg as needed when systolic blood
pressure was ≥160 mmHg.
After confirming tolerability, the dose was
escalated to 80 mg/day (50% of the standard dose) from the second
cycle. The patient completed a total of five cycles. Subsequent CT
revealed a new right pulmonary metastasis (data not shown) meeting
RECIST version 1.1 criteria for PD, leading to discontinuation of
regorafenib.
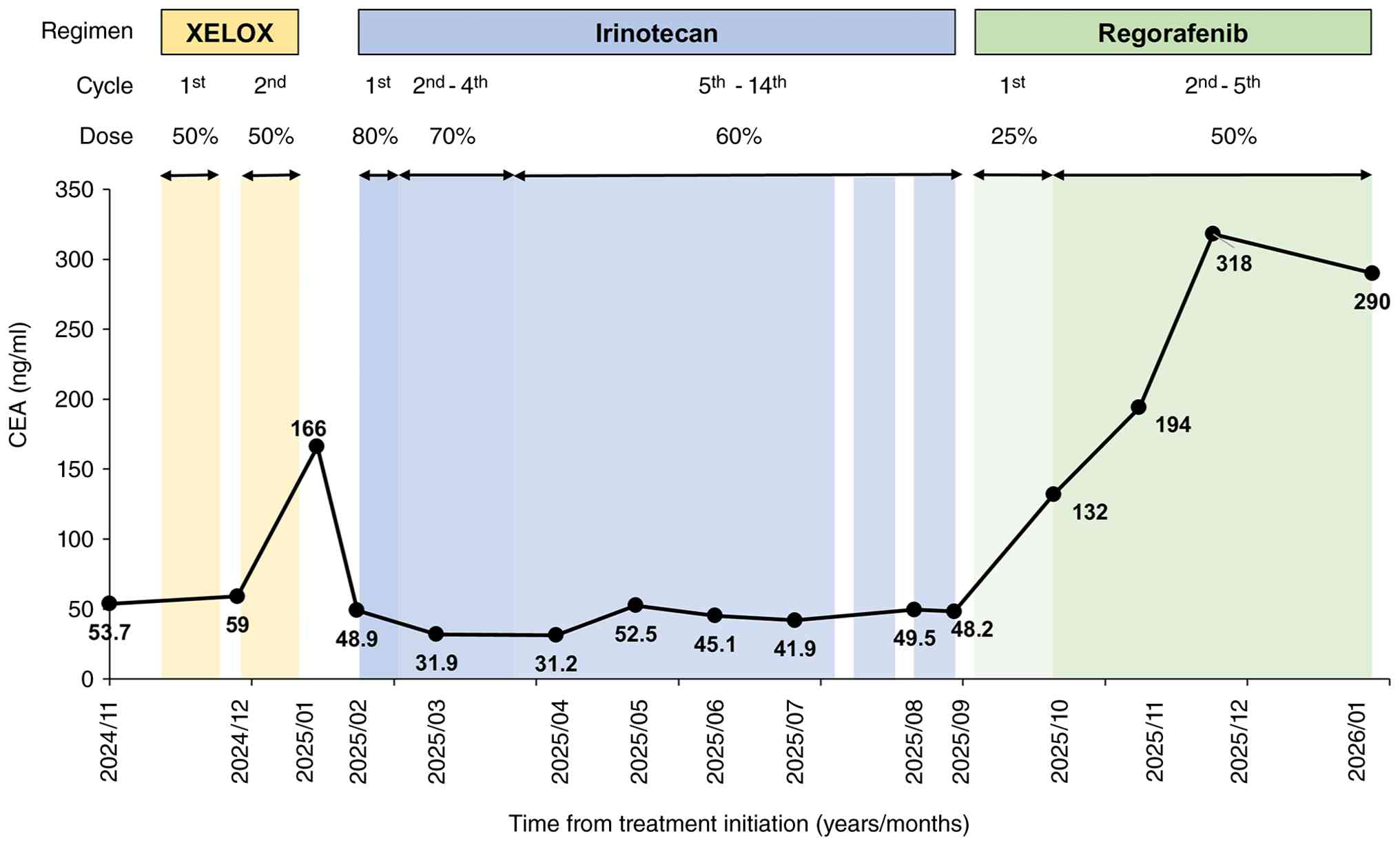
Since January 2026, the patient has received best
supportive care. The patient was alive at the last confirmed
follow-up in March 2026. Serum CEA levels and the clinical timeline
of events are summarized in Fig. 1,
and a detailed chemotherapy timeline under HD is presented in
Table I.
 | Table I.Chemotherapy regimens and associated
adverse effects in a patient undergoing hemodialysis. |
Table I.
Chemotherapy regimens and associated
adverse effects in a patient undergoing hemodialysis.
| Treatment time | Note or regimen | Details | Adverse effects
(CTCAE v5.0) |
|---|
| November
2024-January 2025 | 1st-2nd cycle of
XELOX | Capecitabine 1,000
mg/m2 (50% dose), oxaliplatin 70 mg/m2 (54%
dose) | Fatigue (G2),
platelet count decreased [G2; PLT nadir 6.6×104/µl
(C1D15), 5.9×104/µl (C2D15)], hyperkalemia |
|
|
|
| [G3; K+
7.0 mEq/l (C1D8)] |
| January 2025 | SD | Treatment
discontinued on the basis of clinical judgment despite SD | - |
| February 2025 | 1st cycle of
Irinotecan | 120
mg/m2 (80% dose) | Diarrhea (G3) |
| March 2025 | 2nd-4th cycle of
Irinotecan | 105
mg/m2 (70% dose) | Diarrhea (worst
grade: G3, subsequently improving to G2) |
| May-August
2025 | 5th-14th cycle of
Irinotecan | 90 mg/m2
(60% dose) | Diarrhea (worst
grade: G2, subsequently improving to G1) |
| August 2025 | PD | New left pulmonary
metastasis and increase in target lesion size | - |
| September 2025 | 1st cycle of
Regorafenib | 40 mg/day (25%
dose) | Hypertension
(G3) |
| September
2025-January 2026 | 2nd-5th cycle of
Regorafenib | 80 mg/day (50%
dose) | Hypertension
(G3) |
| January 2026 | PD | New right pulmonary
metastasis | - |
| January 2026 | BSC | - | - |
Discussion
The management of cancer in HD patients remains
challenging due to altered pharmacokinetics and limited evidence
regarding optimal chemotherapy dosing (18). Studies suggest that cancer
development in HD patients does not necessarily reduce overall
survival (3,19), indicating that chemotherapy can be
feasible and effective in carefully selected patients. In the CANDY
study, 28% of 178 chronic dialysis patients who developed cancer
received chemotherapy, underscoring the importance of
individualized treatment plans based on each drug's pharmacologic
properties and available pharmacokinetic data (20).
Capecitabine, a component of the XELOX regimen, is
contraindicated in patients with severe renal impairment
(creatinine clearance <30 ml/min) and is generally avoided
(18). Pharmacokinetic data support
this approach, demonstrating increased exposure to capecitabine
metabolites-particularly 5′-deoxy-5-fluorouridine and
α-fluoro-β-alanine-in patients with kidney impairment (21). In a retrospective study, patients
who initiated HD during capecitabine treatment tolerated a ~50%
dose reduction without severe toxicity (22). Accordingly, capecitabine was
administered at 50% of the standard dose in the present case to
ensure safety. However, drug removal during HD could potentially
reduce antitumor efficacy, which remains a limitation.
Oxaliplatin is predominantly excreted renally and
biphasic elevation of plasma free platinum concentrations has been
reported in HD patients (23). As
platinum compounds rapidly bind to plasma proteins and erythrocytes
shortly after infusion, initiating dialysis 1–1.5 h post-infusion
is commonly practiced and described in previous reports (24–26).
With dose reduction and early dialysis, the area under the curve
for free platinum may be slightly higher than in non-HD patients,
while peak concentrations remain comparable, resulting in
acceptable toxicity profiles (26).
Furthermore, previous studies indicate that oxaliplatin is
generally administered at reduced doses (e.g., 60–85
mg/m2) in patients undergoing HD, although higher doses
(e.g., up to 100 mg/m2) have also been reported
(13,14,23).
This variability underscores the lack of consensus and suggests
that the optimal oxaliplatin dose in HD patients remains uncertain.
In the present case, oxaliplatin was administered at 70
mg/m2 (54% of the standard dose) in the morning,
followed by HD in the afternoon at a local clinic. Adverse events
were manageable and treatment was safely continued. These findings
suggest that careful dose adjustment and appropriate HD timing can
enhance the safety of oxaliplatin in HD patients. However, the
progression-free survival (PFS) observed with XELOX in the present
case was shorter than that reported with standard XELOX in non-HD
populations (27). This finding
suggests that early HD may have reduced the antitumor activity by
removing unbound platinum before adequate tissue distribution,
particularly in the context of dose reduction. Nevertheless, as
pharmacokinetic analysis was not performed in the present case, the
relationship among HD timing, adverse events and antitumor efficacy
remains speculative.
Irinotecan is primarily metabolized in the liver to
its active metabolite SN-38, which is glucuronidated by UGT1A1 and
excreted in bile (28). As SN-38 is
highly protein-bound and poorly cleared by dialysis, the timing of
dialysis is unlikely to substantially affect its pharmacokinetics
(29). Previous reports have
described the safe administration of irinotecan at reduced doses
(50–100 mg/m2) in HD patients under clinical monitoring
(30,31). For example, a weekly regimen of
50–80 mg/m2 (3 weeks on, 1 week off) led to stable
disease in an HD patient with mCRC (32). These favorable outcomes highlight
the clinical utility of dose reduction. Conversely, severe toxicity
has also been reported with irinotecan-based chemotherapy in HD
patients; notably, one HD patient with mCRC developed grade 4
diarrhea and neutropenia after irinotecan at 180 mg/m2,
which ultimately resulted in death (33). Mechanistically, uremic toxins
associated with severe renal failure can inhibit the hepatic uptake
of SN-38, delaying its clearance and exacerbating toxicity
(34). In the present case,
treatment was initiated at 120 mg/m2 to avoid potential
underdosing; however, Grade 3 diarrhea developed despite the
absence of common UGT1A1 risk polymorphisms. Accordingly, the dose
was reduced stepwise to 105 mg/m2 and then 90
mg/m2 based on tolerability. The resulting PFS was ~7
months, which appears favorable compared with outcomes reported in
the general mCRC population (35).
Regorafenib frequently induces early severe
toxicities. The ReDOS trial demonstrated that stepwise dose
escalation from 80 mg/day improves treatment continuation (36). Regorafenib is metabolized primarily
in the liver, and its major active metabolites (M-2 and M-5) are
highly protein-bound; therefore, hemodialysis is unlikely to
substantially enhance drug elimination (37). In one reported case, regorafenib
initiated at 40 mg/day was associated with early hypotension,
altered mental status, abdominal pain and leukocytosis at the
beginning of the second cycle, ultimately progressing to septic
shock and cardiomyopathy requiring intensive care (17). By contrast, a recent case report
described regorafenib initiation at 80 mg/day with escalation to
160 mg/day in an HD patient with mCRC, with acceptable tolerability
(38). In the present case, therapy
was initiated at 40 mg/day and escalated to 80 mg/day after
confirming tolerability. Starting at a low dose, gradual titration
and frequent monitoring minimized toxicity while maintaining
treatment continuity. Rapid dose escalation may be considered if
adverse events remain tolerable to prevent underdosing and loss of
efficacy. In the present case, PFS was ~5 months, exceeding the
median PFS reported in previous studies (39,40)
and suggesting a relatively favorable outcome.
Several limitations should be acknowledged.
Pharmacokinetic analyses were not performed for any of the
administered agents and dose adjustments were based on prior
reports and clinical tolerance rather than direct pharmacokinetic
data. In addition, the patient's excellent PS may have contributed
to the favorable tolerability profile. Finally, the limited
efficacy observed with first-line therapy suggests a potential
trade-off between safety-oriented dose reduction and antitumor
activity.
In conclusion, this case demonstrates that
sequential systemic therapy is feasible in a patient with mCRC
undergoing HD when dosing and administration schedules are
appropriately adjusted. In particular, it highlights the importance
of individualized treatment strategies based on drug
characteristics, dialysis timing and patient tolerability in HD
patients for whom standard regimens are difficult to apply.
Although limited to a single case, these findings contribute to the
scarce literature on the management of mCRC in patients undergoing
HD. Further clinical data are needed to establish effective
treatment strategies for this growing HD patient population.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
RS and MT confirm the authenticity of all the raw
data. Conceptualization of the manuscript was performed by RS. Data
acquisition and interpretation were carried out by RS, NH, YK, YY,
MO, SO and MT. The original draft was written by RS, and writing,
review and editing were conducted by RS and MT. All authors read
and approved the final manuscript and agreed to be accountable for
all aspects of the work to ensure the accuracy and integrity of any
part of the study.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Written informed consent was obtained from the
patient for publication of this case report and any accompanying
images. The patient was informed that all identifying information
would be removed to maintain anonymity.
Competing interests
The authors declare that they have no competing
interests.
Use of artificial intelligence tools
During the preparation of this paper, ChatGPT-5
(https://chatgpt.com/) was used for spell checking
and grammar checking. The authors then reviewed and edited the
content as necessary and assume full responsibility for the final
manuscript.
References
|
1
|
Hanafusa N, Abe M, Joki N, Hoshino J,
Taniguchi M, Kikuchi K, Hasegawa T, Goto S, Ogawa T, Kanda E, et
al: Annual dialysis data report 2022, Japanese society for dialysis
therapy (JSDT) renal data registry. Ren Replace Ther. 11:542025.
View Article : Google Scholar
|
|
2
|
Cancer Statistics in Japan Editorial
Board, . Cancer Statistics in Japan 2025. Foundation for Promotion
of Cancer Research; Tokyo: 2025, Available at:. https://ganjoho.jp/public/qa_links/report/statistics/pdf/cancer_statistics_2025_fig_E.pdf
|
|
3
|
Toriu N, Yamamoto S, Matsubara T, Kataoka
Y, Sakai K, Funakoshi T, Horimatsu T, Tsukamoto T, Murakami N,
Jhaveri KD, et al: Cancer diagnosis and prognosis after initiation
of hemodialysis: Multicenter Japan CANcer and DialYsis (J-CANDY)
study. Clin Kidney J. 18:sfae4302024. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Morris VK, Kennedy EB, Baxter NN, Benson
AB III, Cercek A, Cho M, Ciombor KK, Cremolini C, Davis A, Deming
DA, et al: Treatment of metastatic colorectal cancer: ASCO
guideline. J Clin Oncol. 41:678–700. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Zeineddine FA, Zeineddine MA, Yousef A, Gu
Y, Chowdhury S, Dasari A, Huey RW, Johnson B, Kee B, Lee MS, et al:
Survival improvement for patients with metastatic colorectal cancer
over twenty years. NPJ Precis Oncol. 7:162023. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Delaye M, Rousseau A, Try M, Massard C,
Campedel L, Hilmi M and Bagnis C: Inclusion of patients with
chronic kidney disease in randomized phase 3 clinical trials in
patients with prostate, breast, lung, and colorectal cancer. Cancer
Med. 12:3172–3175. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Gotta V, Dao K, Rodieux F, Buclin T, Livio
F and Pfister M: Guidance to develop individual dose
recommendations for patients on chronic hemodialysis. Expert Rev
Clin Pharmacol. 10:737–752. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Matte P, Bihan K, Isnard-Bagnis C, Zahr N,
Thiery-Vuillemin A, Gougis P and Campedel L: Management of cancer
treatments in hemodialysis patients. Bull Cancer. 111:701–719.
2024. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Sobin LH, Gospodarowicz MK and Wittekind
C: TNM Classification of Malignant Tumours (7th). Wiley-Blackwell;
Chichester, UK: 2010
|
|
10
|
Oken MM, Creech RH, Tormey DC, Horton J,
Davis TE, McFadden ET and Carbone PP: Toxicity and response
criteria of the Eastern Cooperative Oncology Group. Am J Clin
Oncol. 5:649–655. 1982. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kobayashi M, Endo S, Hamano Y, Imanishi M,
Akutsu D, Sugaya A, Ochi D, Moriwaki T and Hyodo I: Successful
treatment with modified FOLFOX6 and panitumumab in a cecal cancer
patient undergoing hemodialysis. Intern Med. 55:127–130. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Janus N, Thariat J, Boulanger H, Deray G
and Launay-Vacher V: Proposal for dosage adjustment and timing of
chemotherapy in hemodialyzed patients. Ann Oncol. 21:1395–1403.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Sasaki K, Zhou Q, Matsumoto Y, Saiki T,
Moriyama M and Saijo Y: Treatment of gastric and gastroesophageal
cancer patients with hemodialysis by CapeOX. Intern Med.
58:2791–2795. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Yamagishi S, Suematsu Y, Takahashi M,
Saito H, Nakayama M, Fukabori M, Morita A, Wakabayashi K and Itoh
Y: A case of hemodialysis patients with resected synchronous
multiple metastases from colorectal cancer successfully treated
with CapeOX Therapy. Gan To Kagaku Ryoho. 43:1767–1769. 2016.(In
Japanese). PubMed/NCBI
|
|
15
|
National Cancer Institute (NCI), Common
terminology criteria for adverse events (CTCAE) version 5.0, .
Cancer Therapy Evaluation Program. NCI; Bethesda, MD: 2017
|
|
16
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Bolonesi RM, Rogers JE and Shureiqi I: A
case report-treatment of metastatic colorectal cancer in a patient
on hemodialysis. J Gastrointest Cancer. 45 (Suppl 1):S161–S165.
2014. View Article : Google Scholar
|
|
18
|
Pedrazzoli P, Silvestris N, Santoro A,
Secondino S, Brunetti O, Longo V, Mancini E, Mariucci S, Rampino T,
Delfanti S, et al: Management of patients with end-stage renal
disease undergoing chemotherapy: Recommendations of the
Associazione Italiana di Oncologia Medica (AIOM) and the Societa
Italiana di Nefrologia (SIN). ESMO Open. 2:e0001672017. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Bechade C, Dejardin O, Bara S, Bouvier V,
Guizard AV, De Mil R, Troussard X, Launoy G and Lobbedez T:
Survival of patients with cancer starting chronic dialysis: Data
from kidney and cancer registries in lower Normandy. Nephrology
(Carlton). 23:1125–1130. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Janus N, Launay-Vacher V, Thyss A,
Boulanger H, Moranne O, Islam MS, Durande JP, Ducret M, Juillard L,
Soltani Z, et al: Management of anticancer treatment in patients
under chronic dialysis: Results of the multicentric CANDY (CANcer
and DialYsis) study. Ann Oncol. 24:501–507. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Poole C, Gardiner J, Twelves C, Johnston
P, Harper P, Cassidy J, Monkhouse J, Banken L, Weidekamm E and
Reigner B: Effect of renal impairment on the pharmacokinetics and
tolerability of capecitabine (Xeloda) in cancer patients. Cancer
Chemother Pharmacol. 49:225–234. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Jhaveri KD, Flombaum C, Shah M and Latcha
S: A retrospective observational study on the use of capecitabine
in patients with severe renal impairment (GFR <30 ml/min) and
end stage renal disease on hemodialysis. J Oncol Pharm Pract.
18:140–147. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Horimatsu T, Miyamoto S, Morita S, Mashimo
Y, Ezoe Y, Muto M and Chiba T: Pharmacokinetics of oxaliplatin in a
hemodialytic patient treated with modified FOLFOX-6 plus
bevacizumab therapy. Cancer Chemother Pharmacol. 68:263–266. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Allain P, Heudi O, Cailleux A, Le Bouil A,
Larra F, Boisdron-Celle M and Gamelin E: Early biotransformations
of oxaliplatin after its intravenous administration to cancer
patients. Drug Metab Dispos. 28:1379–1384. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Wang D, Li X, Xu L, Fang W, Cai X, Wang Y,
Wang J, Wang Y, Zhao F and Gu Y: Dose-escalation of oxaliplatin in
hemodialysis patient treated with FOLFOX therapy: A case report.
Medicine (Baltimore). 98:e174622019. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Nagatani Y, Imamura Y, Nakamura T,
Yamashita K, Okuno M, Yasui H, Hiraoka J, Niigata R, Kono K, Hyogo
Y, et al: Pharmacokinetics of oxaliplatin in a hemodialysis patient
with metastatic colon cancer. Int J Oncol Res. 2:0172019.
|
|
27
|
Cassidy J, Clarke S, Diaz-Rubio E,
Scheithauer W, Figer A, Wong R, Koski S, Lichinitser M, Yang TS,
Rivera F, et al: Randomized phase III study of capecitabine plus
oxaliplatin compared with fluorouracil/folinic acid plus
oxaliplatin as first-line therapy for metastatic colorectal cancer.
J Clin Oncol. 26:2006–2012. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
de Man FM, Goey AKL, van Schaik RHN,
Mathijssen RHJ and Bins S: Individualization of irinotecan
treatment: A review of pharmacokinetics, pharmacodynamics, and
pharmacogenetics. Clin Pharmacokinet. 57:1229–1254. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Combes O, Barre J, Duche JC, Vernillet L,
Archimbaud Y, Marietta MP, Tillement JP and Urien S: In vitro
binding and partitioning of irinotecan (CPT-11) and its metabolite,
SN-38, in human blood. Invest New Drugs. 18:1–5. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Stemmler J, Weise A, Hacker U, Heinemann V
and Schalhorn A: Weekly irinotecan in a patient with metastatic
colorectal cancer on hemodialysis due to chronic renal failure.
Onkologie. 25:60–63. 2002.PubMed/NCBI
|
|
31
|
Kim DM, Kim HL, Chung CH and Park CY:
Successful treatment of small-cell lung cancer with irinotecan in a
hemodialysis patient with end-stage renal disease. Korean J Intern
Med. 24:73–75. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Czock D, Rasche FM, Boesler B, Shipkova M
and Keller F: Irinotecan in cancer patients with end-stage renal
failure. Ann Pharmacother. 43:363–369. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Venat-Bouvet L, Saint-Marcoux F, Lagarde
C, Peyronnet P, Lebrun-Ly V and Tubiana-Mathieu N: Irinotecan-based
chemotherapy in a metastatic colorectal cancer patient under
haemodialysis for chronic renal dysfunction: Two cases considered.
Anticancer Drugs. 18:977–980. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Fujita K, Sugiura T, Okumura H, Umeda S,
Nakamichi N, Watanabe Y, Suzuki H, Sunakawa Y, Shimada K, Kawara K,
et al: Direct inhibition and down-regulation by uremic plasma
components of hepatic uptake transporter for SN-38, an active
metabolite of irinotecan, in humans. Pharm Res. 31:204–215. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ulrich-Pur H, Kornek GV, Fiebiger W,
Gedlicka C, Raderer M, Lenauer A, Depisch D, Lang F, Pidlich J and
Scheithauer W: Multicenter phase II trial of dose-fractionated
irinotecan in patients with advanced colorectal cancer failing
oxaliplatin-based first-line combination chemotherapy. Ann Oncol.
12:1269–1272. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Bekaii-Saab TS, Ou FS, Ahn DH, Boland PM,
Ciombor KK, Heying EN, Dockter TJ, Jacobs NL, Pasche BC, Cleary JM,
et al: Regorafenib dose-optimisation in patients with refractory
metastatic colorectal cancer (ReDOS): A randomised, multicentre,
open-label, phase 2 study. Lancet Oncol. 20:1070–1082. 2019.
View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Zopf D, Fichtner I, Bhargava A, Steinke W,
Thierauch KH, Diefenbach K, Wilhelm S, Hafner FT and Gerisch M:
Pharmacologic activity and pharmacokinetics of metabolites of
regorafenib in preclinical models. Cancer Med. 5:3176–3185. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Takemura K, Murakawa Y, Kono H, Suemasu M,
Kuroda A, Yamaguchi T, Tanabe Y, Suyama K and Uchino K: Safe
administration of fruquintinib in a hemodialysis patient with
metastatic colorectal cancer: A case report. Case Rep Oncol.
19:29–35. 2026. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Yoshino T, Komatsu Y, Yamada Y, Yamazaki
K, Tsuji A, Ura T, Grothey A, Van Cutsem E, Wagner A, Cihon F, et
al: Randomized phase III trial of regorafenib in metastatic
colorectal cancer: Analysis of the CORRECT Japanese and
non-Japanese subpopulations. Invest New Drugs. 33:740–750. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Grothey A, Van Cutsem E, Sobrero A, Siena
S, Falcone A, Ychou M, Humblet Y, Bouche O, Mineur L, Barone C, et
al: Regorafenib monotherapy for previously treated metastatic
colorectal cancer (CORRECT): An international, multicentre,
randomised, placebo-controlled, phase 3 trial. Lancet. 381:303–312.
2013. View Article : Google Scholar : PubMed/NCBI
|