Introduction
Hepatocellular carcinoma (HCC) is the 5th most
common type of cancer and the 3rd leading cause of cancer-related
mortality worldwide, presenting a major public health challenge
(1–3). HCC is characterized by highly
aggressive biological behavior and a pronounced propensity for
vascular (invasion, frequently resulting in the development of
tumor thrombus (TT). Although the portal vein is the most commonly
involved site, tumor invasion into the hepatic vein, inferior vena
cava (IVC), and, in rare cases, the right atrium (RA) may also
occur (4). According to the
American Association for the Study of Liver Diseases guidelines and
the Barcelona Clinic Liver Cancer (BCLC) staging system, HCC with
IVC/RA TT is classified as BCLC stage C disease (5). This condition is associated with a
poor prognosis due to the increased risk of distant metastasis,
pulmonary embolism, cardiac outflow obstruction and multi-organ
dysfunction (5–7). Despite notable advances in the
management of HCC over the past few decades, the optimal treatment
strategy for patients with IVC/RA TT remains controversial. Several
retrospective studies conducted in Japan have suggested that
surgical resection can provide survival benefit, particularly in
the absence of other effective treatment options (8,9).
However, surgery in this setting is technically demanding and
requires meticulous perioperative management due to the high risk
of perioperative mortality (9).
For patients with advanced HCC, current clinical
guidelines recommend systemic therapy with sorafenib as the
standard first-line treatment due to its established efficacy and
safety profile (5). IMbrave150
trial revealed that systemic therapy with atezolizumab plus
bevacizumab could achieve prolonged overall survival (OS) and
progression-free survival (PFS) compared with sorafenib
monotherapy. In addition, other systemic therapy regimens, such as
lenvatinib, donafenib and immune checkpoint inhibitors (ICIs) such
as nivolumab and pembrolizumab, have also shown survival benefits
(7,10,11).
Locoregional treatments, including transarterial chemoembolization
(TACE) and stereotactic body radiation therapy (SBRT), have also
demonstrated promising efficacy with a favorable safety and
tolerability profile (12).
Furthermore, multidisciplinary team (MDT)-based management has
emerged as a key approach for optimizing treatment selection and
integrating multimodal therapies in patients with advanced HCC
(13,14).
The present study aimed to evaluate the clinical
characteristics and treatment outcomes of patients with HCC and
IVC/RA TT who underwent non-surgical treatment with MDT
participation. The primary objective was to assess the efficacy and
safety of these combination therapeutic strategies.
Materials and methods
Patient selection
In this retrospective study, a total of 41 patients
with HCC and IVC/RA TT who were admitted to the MDT clinic for HCC
with vascular TT at the West China Hospital of Sichuan University
(Chengdu, China) between January 2019 and December 2023 were
reviewed. The diagnosis of HCC was confirmed using
contrast-enhanced CT or MRI. Each scan was independently evaluated
by two experienced radiologists, and all imaging examinations were
completed ≤2 weeks prior to treatment initiation. The inclusion
criteria were as follows: i) Confirmed diagnosis of HCC based on
imaging findings; ii) radiological confirmation of the location and
extent of IVC or RA TT; iii) Child-Pugh grade A or B and an Eastern
Cooperative Oncology Group performance status of 0 or 1; and iv)
prior MDT evaluation with complete treatment records available. The
exclusion criteria were the following: i) Presence of other primary
tumors or metastatic liver cancer; ii) severe liver failure
(Child-Pugh grade C); iii) incomplete medical records; and iv) loss
to follow-up ≤2 months after initial treatment. For TT
classification, the HV/IVC TT system proposed by Cheng Shuqun was
applied (15). According to this
system, TT was categorized into three types based on its anatomical
extent in the IVC: Type I (hepatic venous type), confined to the
hepatic vein; Type II (subphrenic), located below the diaphragm in
the IVC; and Type III (supraphrenic type), extending above the
diaphragm into the RA. Patients and the public were not involved in
the design, conduct, reporting or dissemination of the present
study.
Treatment protocols
All patients received MDT-guided treatment
recommendations. The MDT consisted of several experts from the
departments of liver surgery, medical oncology, radiation therapy,
interventional therapy and imaging. Following comprehensive
clinical evaluation and supplementary examinations, individualized
treatment plans were developed by the MDT experts based on the
specific clinical condition of each patient. Treatment strategies
included targeted therapy (sorafenib, lenvatinib and bevacizumab),
immunotherapy (camrelizumab, tisleilizumab and atezolizumab), SBRT
and TACE. All therapeutic regimens were administered according to
established clinical guidelines.
Follow-up and monitoring
Patients were regularly monitored to assess
treatment response, disease progression and survival outcomes.
Follow-up assessments were performed every 3 months during the 1st
year after treatment initiation and included clinical evaluation,
laboratory testing of liver function and tumor markers and
contrast-enhanced imaging examinations (CT or MRI). To ensure
consistency across treatment modalities, tumor response and disease
progression were independently assessed by two senior radiologists
according to the modified Response Evaluation Criteria in Solid
Tumors (mRECIST). Disease progression was defined as radiological
evidence of enlargement of target tumor lesions, development of new
lesions or expansion of the TT based on mRECIST criteria,
regardless of the treatment received (16). Any discrepancies between reviewers
were resolved by consensus or by a third senior radiologist.
Follow-up was maintained until mortality or the end of the study
period. The primary endpoint was OS, and the secondary endpoint was
PFS. Both survival periods were calculated from the date of
treatment initiation to the date of mortality from any cause or the
first documented disease progression based on the mRECIST criteria,
respectively. Patients who remained alive or free of progression at
the final follow-up were censored at the date of their last
hospital visit.
Statistical analysis
Baseline patient characteristics were summarized
using continuous variables, expressed as the mean or median and
categorical variables, presented as frequencies and percentages.
Comparisons among multiple groups were performed using one-way
ANOVA for normally distributed continuous variables and the
Kruskal-Wallis test for non-normally distributed data. If
statistical significance was observed, Tukey's honest significant
difference (HSD) test or Dunn's test was applied for post hoc
pairwise comparisons, respectively. Categorical variables were
compared using the Pearson χ2 test or Fisher's exact
test, as appropriate. OS and PFS were analyzed utilizing the
Kaplan-Meier method and compared using the log-rank test. All
statistical tests were two-sided, and P<0.05 was considered to
indicate a statistically significant difference. In the Cox
regression, variables with P<0.10 were entered in the
multivariable Cox regression model, with a P<0.05 considered
statistically significant. To minimize overfitting and ensure the
stability of the multivariable Cox proportional hazards model in
this relatively small cohort, variables with extremely low event
frequencies, such as pulmonary embolism, were excluded from the
multivariable analysis. All data analyses were conducted using R
software version 4.4.1 (R Foundation for Statistical Computing;
http://www.R-project.org/).
Results
Baseline characteristics
In the present study, a total of 41 patients
diagnosed with HCC and IVC/RA TT were enrolled. The median
follow-up duration was 10 months (range, 4–14 months), during which
31 mortalities (75.61%) were recorded. Key baseline
characteristics, including age, sex, liver function parameters,
tumor burden and underlying liver diseases, are summarized in
Table I. According to the IVC/RA TT
classification, 22 patients (53.66%) were classified as type I,
eight (19.51%) as type II and 11 (26.83%) as type III. PVTT was
also common in this cohort. Particularly, two patients (4.87%)
exhibited type I PVTT, nine (21.95%) had type II, 16 (39.02%) had
type III, two (4.87%) had type IV, whereas 12 (29.27%) showed no
evidence of PVTT. Extrahepatic metastasis was observed at first
presentation in 20 patients (48.78%), with the lungs, adrenal
glands, peritoneum and bones representing the most common
metastatic sites. Regarding treatment modalities, eight patients
(19.51%) received systemic therapy alone (S), four (9.76%) received
mono-locoregional therapy with either SBRT or TACE (T/R), 14
(34.15%) received dual therapy (S + T/R) and 15 (36.59%) received
triple therapy consisting of systemic therapy combined with SBRT
and TACE (S + R + T). Detailed information regarding the specific
treatment combinations and sequential alterations in the
triple-modality therapy group is presented in Table SI. No statistically significant
differences in baseline characteristics were observed among the
different treatment groups (Table
SII).
 | Table I.Baseline characteristics of
hepatocellular carcinoma with IVC/RA TT. |
Table I.
Baseline characteristics of
hepatocellular carcinoma with IVC/RA TT.
|
Characteristics | Value |
|---|
| Age, years | 53.46±11.29 |
| Sex, n (%) |
|
|
Male | 34 (82.93) |
|
Female | 7 (17.07) |
| AFP, n (%) |
|
| ≤400
ng/ml | 17 (41.46) |
| >400
ng/ml | 24 (58.54) |
| PIVKA-II |
|
| ≤1,000
mAU/ml | 5 (12.20) |
|
>1,000 mAU/ml | 36 (87.80) |
| ALT, n (%) |
|
| ≤40
U/l | 18 (43.90) |
| >40
U/l | 23 (56.10) |
| AST, n (%) |
|
| ≤40
U/l | 9 (21.95) |
| >40
U/l | 32 (78.05) |
| TB, µmol/l | 25.2 |
|
| (15.5–37.6) |
| Ab, g/l | 39.49±4.88 |
| ALBI, n (%) |
|
|
Grade1 | 14 (34.15) |
|
Grade2 | 27 (65.85) |
| Child-Pugh stage, n
(%) |
|
| A | 32 (78.05) |
| B | 9 (21.95) |
| Cirrhosis, n
(%) |
|
| No | 7 (17.07) |
|
Yes | 34 (82.93) |
| Hepatitis, n
(%) |
|
| No | 39 (95.12) |
|
HBV | 2 (4.87) |
| Tumor number, n
(%) |
|
| ≤3 | 9 (21.95) |
|
>3 | 32 (78.05) |
| Tumor diameter, n
(%) |
|
| ≤10
cm | 22 (53.66) |
| >10
cm | 19 (46.34) |
| Intrahepatic
metastasis, n (%) |
|
| No | 4 (9.76) |
|
Yes | 37 (90.24) |
| Lymph metastasis, n
(%) |
|
| No | 31 (75.61) |
|
Yes | 10 (24.39) |
| Metastasis, n
(%) |
|
| No | 21 (51.22) |
|
Yes | 20 (48.78) |
| CNLC stage, n
(%) |
|
|
IIIa | 21 (51.22) |
|
IIIb | 20 (48.78) |
| PVTT, n (%) |
|
| No | 12 (29.27) |
| I | 2 (4.87) |
| II | 9 (21.95) |
|
III | 16 (39.02) |
| IV | 2 (4.87) |
| IVC/RA TT, n
(%) |
|
| I | 22 (53.66) |
| II | 8 (21.95) |
|
III | 11 (24.39) |
| Pulmonary embolism,
n (%) |
|
| No | 39 (95.12) |
|
Yes | 2 (4.87) |
| Treatment, n
(%) |
|
| S | 8 (19.51) |
|
T/R | 4 (9.76) |
|
S+T/R | 14 (34.15) |
|
S+T+R | 15 (36.59) |
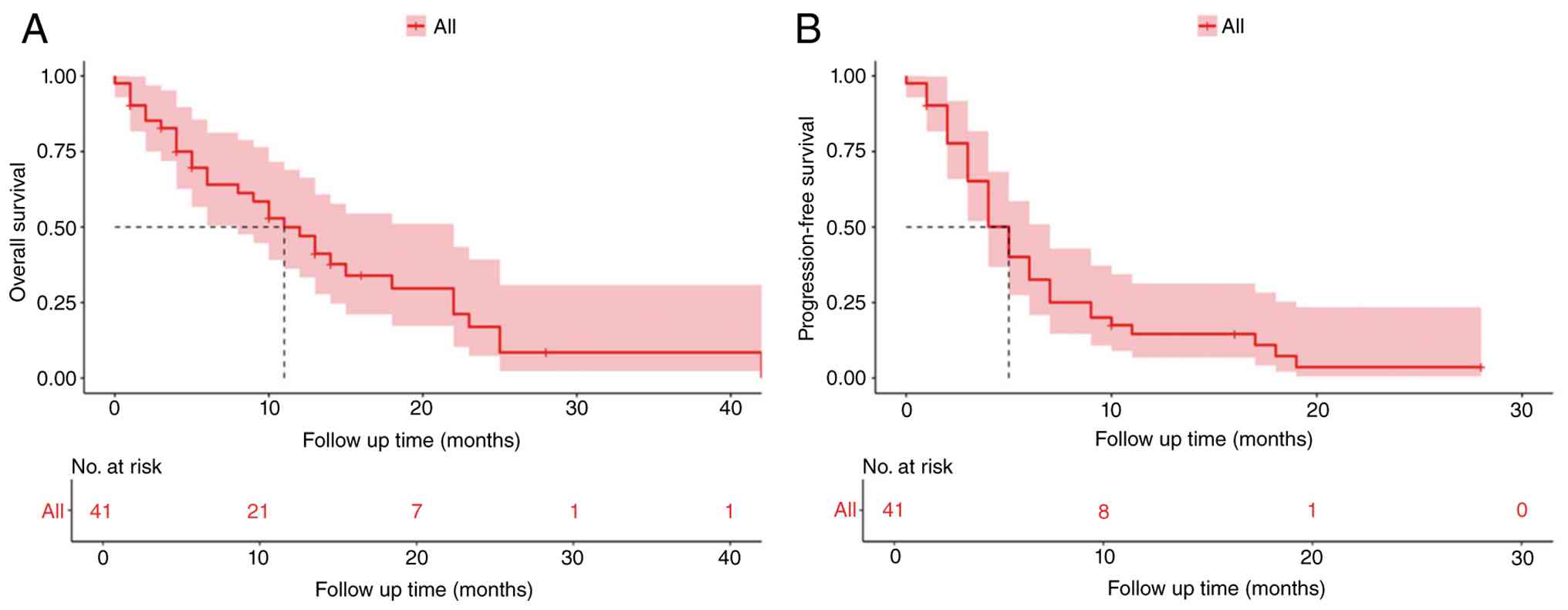
OS and PFS analysis in patients with
HCC and IVC/RA TT
Follow-up was completed for all patients and
concluded in December 2024. The median OS for the entire cohort was
11 months [95% confidence interval (CI), 8–22 months], with OS
rates of 82.7, 64.0 and 47.0% at 3, 6 and 12 months, respectively
(Fig. 1A). The median PFS was 5
months (95% CI, 4–7 months), with PFS rates of 65.2, 32.6 and 14.6%
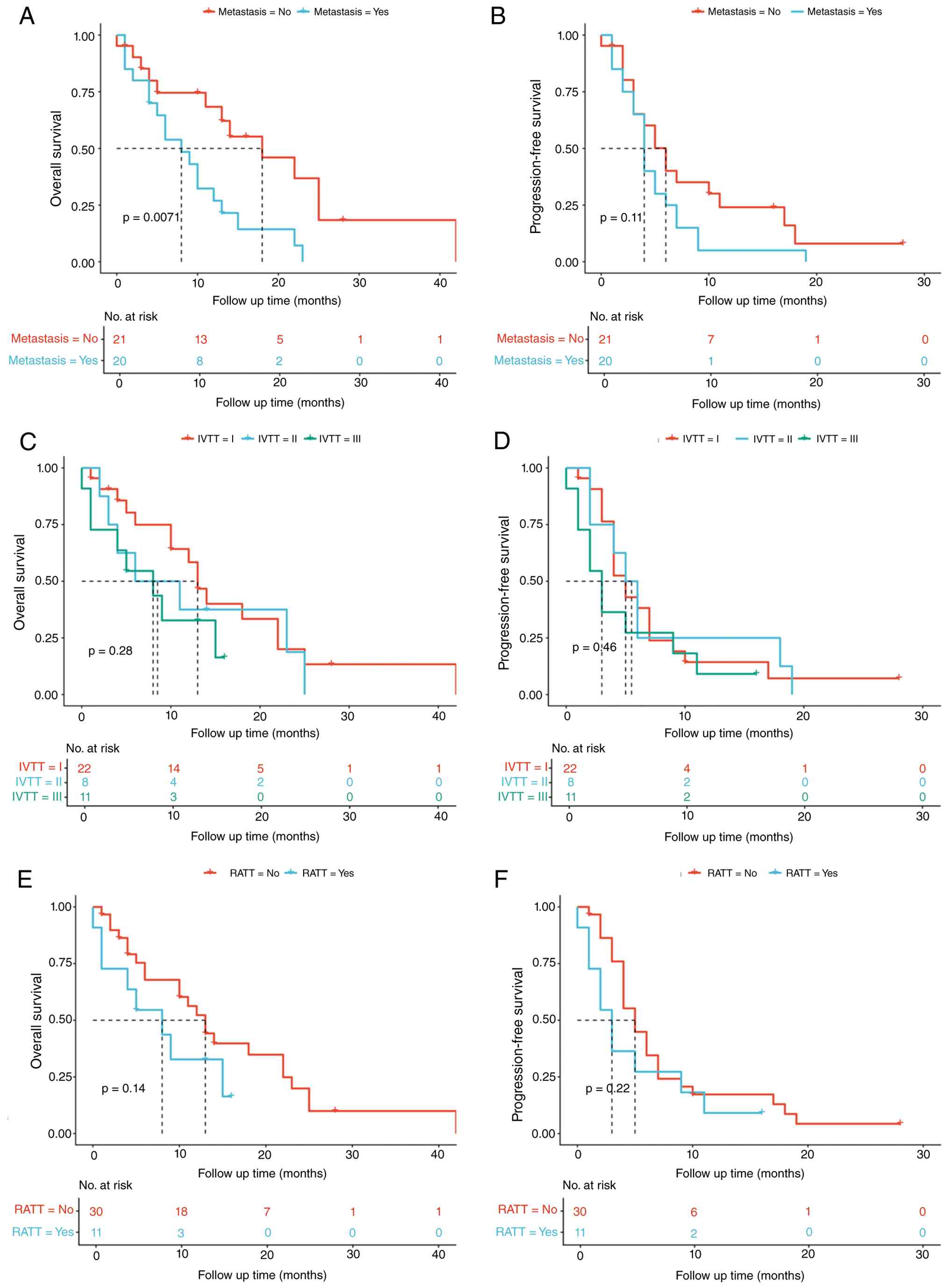
at 3, 6 and 12 months, respectively (Fig. 1B). Patients with distant metastasis
exhibited significantly worse survival outcomes compared with those
without metastasis (median OS, 8 months; 95% CI, 5–15 months vs. 18
months; 95% CI, 13 months-NR; P=0.0071; Fig. 2A). The 3-, 6- and 12-month OS rates
were 80.0, 53.8 and 26.9% in patients with metastasis compared with
85.2, 74.6 and 68.3% in the non-metastatic group. Median PFS was 4
months (95% CI, 3–7 months) in the metastatic group and 6 months
(95% CI, 3–17 months) in the non-metastatic group (Fig. 2B), though this difference did not
reach statistical significance (P=0.11). Stratified analyses
according to the anatomical extent of the thrombus revealed that
patients with type III IVC/RA TT or RATT extension tended to have
worse survival outcomes (Fig.
2C-F). However, these differences did not reach statistical
significance for either OS or PFS (all P>0.05).
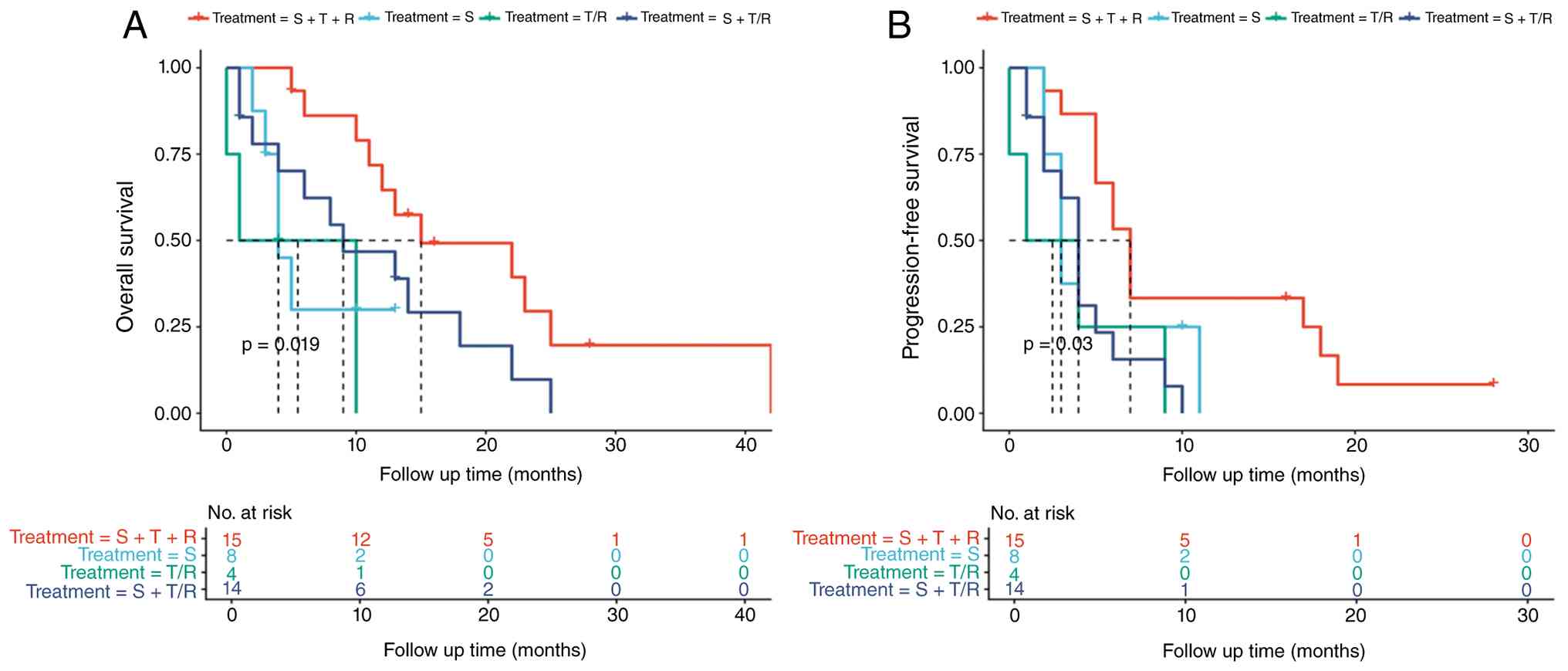
Efficacy of different treatment groups
in patients with HCC and IVC/RA TT
Median OS varied significantly across different
treatment groups (P=0.019; Fig.
3A). Patients treated with systemic therapy alone had a median
OS of 4 months (95% CI, 4 months-NR), while those receiving
mono-locoregional therapy achieved a median OS of 5.5 months (95%
CI, 0 months-NR). Patients treated with dual therapy showed a
median OS of 9 months (95% CI, 4 months-NR), whereas those
receiving triple therapy achieved the longest median OS of 15
months (95% CI, 12 months-NR). A similar pattern was also observed
for PFS (P=0.03; Fig. 3B).
Similarly, median PFS was 3 months (95% CI, 3 months-NR) in the
systemic therapy alone group, 2.5 months (95% CI, 0 months-NR) in
the mono-locoregional therapy group, 4 months (95% CI, 2 months-NR)
in the dual therapy group and 7 months (95% CI, 5 months-NR) in the
triple-modality therapy group.
Prognostic factors of OS and PFS
Univariable and multivariable Cox regression
analyses were performed to identify prognostic factors associated
with OS and PFS. To ensure model stability in this small cohort,
pulmonary embolism was excluded from the multivariable model due to
its extremely low event rate. For OS, multivariable analysis
revealed that the choice of treatment regimen was an independent
prognostic factor (Table II).
Compared with triple therapy (S + T + R), both systemic therapy
alone [S; hazard ratio (HR), 4.31; 95% CI, 1.25–14.83; P=0.021] and
mono-locoregional therapy (T/R; HR, 5.73; 95% CI, 1.33–24.62;
P=0.019) were independently associated with a higher risk of
mortality. Additionally, the presence of distant metastasis was
confirmed as an independent risk factor for worse OS (HR, 2.73; 95%
CI, 1.17–6.39; P=0.021). For PFS, multivariable analysis indicated
that mono-locoregional therapy (T/R; HR, 5.89; 95% CI, 1.51–22.94;
P=0.011), dual therapy (S + T/R; HR, 4.24; 95% CI, 1.55–11.62;
P=0.005) and tumor diameter >10 cm (HR, 3.94; 95% CI, 1.79–8.65;
P<0.001) were independent predictors of disease progression
(Table SIII).
| Table II.Univariable and multivariable
analysis of variables for OS. |
Table II.
Univariable and multivariable
analysis of variables for OS.
|
| Univariable
analysis | Multivariable
analysis |
|---|
|
|
|
|
|---|
| Variable | HR (95% CI) | P-value | HR (95% CI) | P-value |
|---|
| Age |
|
|
|
|
| >50
vs. ≤50 years | 0.61
(0.29–1.32) | 0.21 |
|
|
| Sex |
|
|
|
|
| Male
vs. female | 0.73
(0.27–1.93) | 0.52 |
|
|
| AFP |
|
|
|
|
| >400
vs. ≤400 ng/ml | 1.08
(0.52–2.23) | 0.84 |
|
|
| PIVKA-II |
|
|
|
|
|
>1,000 vs. ≤1,000
mAU/ml | 0.95
(0.33–2.77) | 0.93 |
|
|
| ALT |
|
|
|
|
| >40
vs. ≤40 U/l | 1.16
(0.56–2.39) | 0.69 |
|
|
| AST |
|
|
|
|
| >40
vs. ≤40 U/l | 2.48
(0.94–6.52) | 0.07 | 2.06
(0.72–5.87) | 0.178 |
| ALBI |
|
|
|
|
| Grade 2
vs. Grade 1 | 1.59
(0.72–3.50) | 0.25 |
|
|
| Child Pugh
stage |
|
|
|
|
| B vs.
A | 1.03
(0.42–2.53) | 0.95 |
|
|
| Cirrhosis |
|
|
|
|
| Yes vs.
No | 0.81
(0.28–2.39) | 0.71 |
|
|
| Hepatitis |
|
|
|
|
| HBV vs.
No | 0.66
(0.15–2.83) | 0.58 |
|
|
| Tumor number |
|
|
|
|
| >3
vs. ≤3 | 0.94
(0.42–2.11) | 0.88 |
|
|
| Tumor diameter |
|
|
|
|
| >10
vs. ≤10 cm | 1.48
(0.72–3.05) | 0.29 |
|
|
| Intrahepatic
metastasis |
|
|
|
|
| Yes vs.
No | 1.01
(0.35–2.92) | 0.99 |
|
|
| Lymph
metastasis |
|
|
|
|
| Yes vs.
No | 1.75
(0.76–4.00) | 0.19 |
|
|
| Metastasis |
|
|
|
|
| Yes vs.
No | 2.85
(1.30–6.28) | 0.01a | 2.73
(1.17–6.39) | 0.021a |
| PVTT |
|
|
|
|
| I vs.
No | 0.65
(0.08–5.17) | 0.68 |
|
|
| II vs.
No | 0.77
(0.29–2.09) | 0.61 |
|
|
| III vs.
No | 0.96
(0.40–2.34) | 0.94 |
|
|
| IV vs.
No | 2.97
(0.61–14.48) | 0.18 |
|
|
| IVTT |
|
|
|
|
| II vs.
I | 1.34
(0.54–3.31) | 0.52 |
|
|
| III vs.
I | 2.02
(0.82–4.96) | 0.12 |
|
|
| RATT |
|
|
|
|
| Yes vs.
No | 1.86
(0.79–4.37) | 0.15 |
|
|
| Pulmonary
embolism |
|
|
|
|
| Yes vs.
No | 10.43
(2.00–54.31) | 0.01 |
|
|
| Treatment |
|
|
|
|
| S vs.
S+T+R | 3.68
(1.14–11.84) | 0.029a | 4.31
(1.25–14.83) | 0.021a |
| T/R vs.
S+T+R | 6.53
(1.63–26.15) | 0.008b | 5.73
(1.33–24.62) | 0.019a |
| S+T/R
vs. S+T+R | 2.28
(0.97–5.35) | 0.058 | 2.08
(0.88–4.89) | 0.094 |
Discussion
Patients with HCC and IVC/RA TT generally face a
poor prognosis due to extensive intrahepatic tumor burden and the
limited availability of therapeutic options (17). In the present study, the results
demonstrated that patients undergoing triple therapy (systemic
therapy combined with SBRT and TACE) achieved a significantly
prolonged median OS of 15 months compared with those treated with
single- or dual-modality therapy. Notably, this triple therapy
showed a favorable safety profile, as no grade ≥3 treatment-related
adverse events were reported, indicating robust tolerability in
this clinically advanced and vulnerable patient cohort.
Historically, surgical resection has been considered
the primary radical treatment option for these advanced cases.
However, its clinical utility remains limited. A previous
large-scale multicenter study from Japan demonstrated that although
surgery could achieve a median survival of 1–2 years, it was
accompanied by a remarkably high recurrence rate (median time to
recurrence, 0.48 years) and considerable perioperative mortality
(9). Surgery in this setting is
technically demanding and carries substantial risks of severe
complications, including massive hemorrhage, liver failure and
pulmonary embolism (9,18,19).
Given that the majority of patients with IVC/RA TT present with
impaired liver reserves and extensive tumor burden, several are
inherently ineligible for such highly invasive interventions.
Therefore, the development of effective non-surgical treatment
approaches with low toxicity represents a key unmet clinical need
for patients with advanced HCC. The results of the present study
suggested that triple therapy could serve as a viable and safe
therapeutic alternative for this high-risk population, providing
significant survival benefits while avoiding the substantial risks
associated with aggressive surgical intervention.
The rationale for non-surgical treatment approaches
has been further strengthened by the rapid evolution of systemic
oncology. Since sorafenib was established as the first-line
standard therapy in 2007 (17,20,21),
the therapeutic landscape has evolved substantially with the
introduction of ICIs. Agents targeting cytotoxic
T-lymphocyte-associated antigen 4, programmed cell death protein
(PD-1) or PD-1 ligand 1 can enhance intratumoral T cell
infiltration, thereby amplifying antitumor immune responses
(22–24). Landmark clinical trials, including
HIMALAYA (tremelimumab plus durvalumab) and IMbrave150
(atezolizumab plus bevacizumab), demonstrated notably improved OS
and PFS compared with sorafenib monotherapy, while also preserving
patient quality of life (25–27).
Nevertheless, systemic therapy alone commonly shows
limited efficacy in patients with large-volume and obstructive
tumor thrombi. This limitation underscores the necessity of
integrating locoregional interventions to achieve synergistic local
and systemic control. Interventional therapies, such as TACE, can
directly reduce tumor burden by embolizing tumor-supplying arteries
(13,28,29).
Concurrently, SBRT can induce precise DNA damage and apoptosis
within the thrombus area (30–32).
In addition to its cytotoxic effects, localized radiotherapy can
promote the release of tumor-related antigens, thereby transforming
the cold tumor microenvironment and markedly enhancing the efficacy
of systemic immunotherapy (30–32).
Emerging clinical evidence supports this synergy. For example, the
combination of TACE with lenvatinib and PD-1 inhibitors has yielded
substantial improvements in objective response rates and survival
outcomes (28). Similarly,
combining SBRT with systemic therapy could notably improve PFS in
patients with locally advanced HCC (30).
For patients with IVC/RA TT, balancing the efficacy
of multimodal treatment against cumulative toxicity is clinically
important. The findings of the present study align with those of
previous ones indicating that combining targeted therapies with
ICIs can maintain a manageable safety profile, with common side
effects, including hypertension, fatigue and hand-foot syndrome,
easily mitigated through supportive care or dose modification
(25,26,33,34).
Additionally, the incorporation of SBRT and TACE introduces minimal
severe toxicities, as post-embolization syndrome and transient
elevations in liver enzyme levels are commonly self-limiting or
easily managed by experienced clinicians (31,32).
Collectively, the aforementioned findings suggested that multimodal
non-surgical regimens could offer a favorable therapeutic index for
these high-risk cohorts, holding the potential to achieve
meaningful tumor control comparable to that of surgical
interventions, while markedly reducing the risk of severe
complications.
MDT management plays a key role in the successful
application of these complex treatment combinations. By integrating
expertise across liver surgery, oncology, hepatology,
interventional radiology and radiotherapy, the MDT approach enables
personalized, timely and well-balanced interventions (13,14,35,36).
However, a key limitation of MDT-guided allocation is the inherent
risk of selection bias. Because treatment decisions in this
retrospective cohort were based on multidisciplinary consensus
rather than prospective randomization, the improved survival
outcomes observed in the triple-modality therapy group could
partially reflect a clinical bias toward patients with improved
baseline performance and improved-preserved liver function.
The present study provided a valuable, detailed
evaluation of individualized sequencing strategies for systemic and
locoregional therapies in a rare patient population. Nevertheless,
several limitations should be acknowledged. First, the
retrospective and MDT-driven nature of the present study introduced
inherent selection bias. However, this concern was largely
mitigated by the lack of statistically significant differences in
key pre-treatment baseline characteristics among the different
treatment groups (P>0.05; Table
SI). Second, the clinical rarity of IVC/RA TT limited the
sample size, thereby reducing the statistical power of subgroup
analyses. Third, the therapeutic heterogeneity among combination
regimens could introduce variability in outcome assessment.
However, such treatment adaptations could reflect the clinical
reality, in which tailored precision medicine strategies within an
MDT framework could ensure patient safety in this hyper-advanced
cohort. Lastly, as this was a single-center study, the
generalizability of the findings requires further validation in
larger prospective multicenter cohorts.
In conclusion, the present study demonstrated that a
multimodal non-surgical approach, particularly triple-modality
therapy integrating systemic therapy, SBRT and TACE under MDT
management, could provide promising survival benefits with an
excellent safety profile for patients with HCC and advanced IVC/RA
TT. By achieving notable tumor control with manageable toxicity,
this multidisciplinary regimen could serve as a feasible
alternative to highly invasive surgical interventions. These
findings could offer valuable clinical insights into individualized
treatment sequencing and help inform the design of future
prospective trials aimed at optimizing therapeutic strategies for
this high-risk patient population.
Supplementary Material
Supporting Data
Acknowledgements
Not applicable.
Funding
The present study was funded by the National Natural Science
Foundation of China (grant no. 82270643).
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
PT contributed to the conception and design of the
study, data collection and assembly, data analysis and
interpretation, and manuscript drafting. JL contributed to the
provision of patient data, critical revision of the manuscript for
important intellectual content, language editing and data analysis.
JD made substantial contributions to the acquisition, assembly and
quality control of the data. XW and JZ were responsible for the
conception of the study, and the substantial acquisition and
validation of study materials and clinical patient data. YY and YZ
provided administrative and financial support, supervised the
entire study, made substantial contributions to the conception of
the project and the critical interpretation of data, critically
revised the manuscript for important intellectual content, and gave
final approval of the version to be published. All authors have
read and approved the final manuscript. PT, JZ and YY confirm the
authenticity of all the raw data.
Ethics approval and consent to
participate
This retrospective cohort study was conducted in
accordance with the Declaration of Helsinki (approval no.
2025-Review-2783) and was approved by the Institutional Review
Board (or Ethics Committee) of West China Hospital of Sichuan
University (Chengdu, China). The requirement for informed consent
was waived by the IRB due to the retrospective nature of the
present study and the use of anonymized patient data.
Patient consent for publication
Patient consent for publication was waived by the
Institutional Review Board due to the retrospective nature of the
study and the use of anonymized patient data.
Competing interests
All authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
AFP
|
α-fetoprotein
|
|
ALBI
|
albumin-bilirubin (grade)
|
|
ALT
|
alanine aminotransferase
|
|
AST
|
aspartate aminotransferase
|
|
BCLC
|
The Barcelona Clinic Liver Cancer
(staging classification)
|
|
ECOG
|
Eastern Cooperative Oncology Group
(performance status)
|
|
HBV
|
Hepatitis B virus
|
|
HCC
|
hepatocellular carcinoma
|
|
IVC/RA TT
|
inferior vena cava/right atrial tumor
thrombus
|
|
MDT
|
multidisciplinary team
|
|
OS
|
overall survival
|
|
PFS
|
progression-free survival
|
|
PIVKA-II
|
protein induced by vitamin K absence
or antagonist-II
|
|
PVTT
|
portal vein tumor thrombus
|
|
SBRT
|
stereotactic body radiation
therapy
|
|
TACE
|
transarterial chemoembolization
|
References
|
1
|
Hwang SY, Danpanichkul P, Agopian V, Mehta
N, Parikh ND, Abou-Alfa GK, Singal AG and Yang JD: Hepatocellular
carcinoma: Updates on epidemiology, surveillance, diagnosis and
treatment. Clin Mol Hepatol. 31 (Suppl):S228–S254. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Vogel A, Meyer T, Sapisochin G, Salem R
and Saborowski A: Hepatocellular carcinoma. Lancet. 400:1345–1362.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Marrero JA, Kulik LM, Sirlin CB, Zhu AX,
Finn RS, Abecassis MM, Roberts LR and Heimbach JK: Diagnosis,
staging, and management of hepatocellular carcinoma: 2018 practice
guidance by the American association for the study of liver
diseases. Hepatology. 68:723–750. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Lou J, Li Y, Liang K, Guo Y, Song C, Chen
L, Wang L, Wang F, Zhang L, Chen X, et al: Hypofractionated
radiotherapy as a salvage treatment for recurrent hepatocellular
carcinoma with inferior vena cava/right atrium tumor thrombus: A
multi-center analysis. BMC Cancer. 19:6682019. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Reig M, Forner A, Rimola J, Ferrer-Fàbrega
J, Burrel M, Garcia-Criado Á, Kelley RK, Galle PR, Mazzaferro V,
Salem R, et al: BCLC strategy for prognosis prediction and
treatment recommendation: The 2022 update. J Hepatol. 76:681–693.
2022. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Singal AG, Llovet JM, Yarchoan M, Mehta N,
Heimbach JK, Dawson LA, Jou JH, Kulik LM, Agopian VG, Marrero JA,
et al: AASLD practice guidance on prevention, diagnosis, and
treatment of hepatocellular carcinoma. Hepatology. 78:1922–1965.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Llovet JM, Castet F, Heikenwalder M, Maini
MK, Mazzaferro V, Pinato DJ, Pikarsky E, Zhu AX and Finn RS:
Immunotherapies for hepatocellular carcinoma. Nat Rev Clin Oncol.
19:151–172. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kokudo T, Hasegawa K, Matsuyama Y,
Takayama T, Izumi N, Kadoya M, Kudo M, Kubo S, Sakamoto M,
Nakashima O, et al: Liver resection for hepatocellular carcinoma
associated with hepatic vein invasion: A Japanese nationwide
survey. Hepatology. 66:510–517. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ichida A, Kokudo T, Shimada S, Hatano E,
Kubo S, Kato Y, Ishikawa Y, Mori A, Baba H, Matsuyama Y, et al:
Liver resection for hepatocellular carcinoma with tumor thrombus in
the inferior vena cava or right atrium: A large-scale multicenter
survey conducted in Japan. Ann Surg. 278:e549–e555. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Psilopatis I, Damaskos C, Garmpi A,
Sarantis P, Koustas E, Antoniou EA, Dimitroulis D, Kouraklis G,
Karamouzis MV, Vrettou K, et al: FDA-approved monoclonal antibodies
for unresectable hepatocellular carcinoma: What do we know so far?
Int J Mol Sci. 24:26852023. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ahn JC, Tran NH and Yang JD: Systemic
therapy in advanced hepatocellular carcinoma. Clin Mol Hepatol.
29:516–519. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Llovet JM, De Baere T, Kulik L, Haber PK,
Greten TF, Meyer T and Lencioni R: Locoregional therapies in the
era of molecular and immune treatments for hepatocellular
carcinoma. Nat Rev Gastroenterol Hepatol. 18:293–313. 2021.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
European Association for the Study of the
Liver, . EASL clinical practice guidelines: Management of
hepatocellular carcinoma. J Hepatol. 69:182–236. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Naugler WE, Alsina AE, Frenette CT,
Rossaro L and Sellers MT: Building the multidisciplinary team for
management of patients with hepatocellular carcinoma. Clin
Gastroenterol Hepatol. 13:827–835. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen ZH, Wang K, Zhang XP, Feng JK, Chai
ZT, Guo WX, Shi J, Wu MC, Lau WY and Cheng SQ: A new classification
for hepatocellular carcinoma with hepatic vein tumor thrombus.
Hepatobiliary Surg Nutr. 9:717–728. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lencioni R and Llovet JM: Modified RECIST
(mRECIST) assessment for hepatocellular carcinoma. Semin Liver Dis.
30:52–60. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Xia Y, Zhang J and Ni X: Diagnosis,
treatment and prognosis of hepatocellular carcinoma with inferior
vena cava/right atrium tumor thrombus. Oncol Lett. 20:1012020.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Wang Y, Yuan L, Ge RL, Sun Y and Wei G:
Survival benefit of surgical treatment for hepatocellular carcinoma
with inferior vena cava/right atrium tumor thrombus: Results of a
retrospective cohort study. Ann Surg Oncol. 20:914–922. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Wakayama K, Kamiyama T, Yokoo H, Kakisaka
T, Kamachi H, Tsuruga Y, Nakanishi K, Shimamura T, Todo S and
Taketomi A: Surgical management of hepatocellular carcinoma with
tumor thrombi in the inferior vena cava or right atrium. World J
Surg Oncol. 11:2592013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Llovet JM, Ricci S, Mazzaferro V, Hilgard
P, Gane E, Blanc JF, de Oliveira AC, Santoro A, Raoul JL, Forner A,
et al: Sorafenib in advanced hepatocellular carcinoma. N Engl J
Med. 359:378–390. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yang X, Yang C, Zhang S, Geng H, Zhu AX,
Bernards R, Qin W, Fan J, Wang C and Gao Q: Precision treatment in
advanced hepatocellular carcinoma. Cancer Cell. 42:180–197. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Shen KY, Zhu Y, Xie SZ and Qin LX:
Immunosuppressive tumor microenvironment and immunotherapy of
hepatocellular carcinoma: Current status and prospectives. J
Hematol Oncol. 17:252024. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Yang C, Zhang H, Zhang L, Zhu AX, Bernards
R, Qin W and Wang C: Evolving therapeutic landscape of advanced
hepatocellular carcinoma. Nat Rev Gastroenterol Hepatol.
20:203–222. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Maker AV, Attia P and Rosenberg SA:
Analysis of the cellular mechanism of antitumor responses and
autoimmunity in patients treated with CTLA-4 blockade. J Immunol.
175:7746–7754. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Sangro B, Galle PR, Kelley RK, Charoentum
C, De Toni EN, Ostapenko Y, Heo J, Cheng AL, Wilson Woods A, Gupta
C, et al: Patient-reported outcomes from the phase III HIMALAYA
study of tremelimumab plus durvalumab in unresectable
hepatocellular carcinoma. J Clin Oncol. 42:2790–2799. 2024.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Finn RS, Qin S, Ikeda M, Galle PR, Ducreux
M, Kim TY, Kudo M, Breder V, Merle P, Kaseb AO, et al: Atezolizumab
plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J
Med. 382:1894–1905. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Cheng AL, Qin S, Ikeda M, Galle PR,
Ducreux M, Kim TY, Lim HY, Kudo M, Breder V, Merle P, et al:
Updated efficacy and safety data from IMbrave150: Atezolizumab plus
bevacizumab vs. sorafenib for unresectable hepatocellular
carcinoma. J Hepatol. 76:862–873. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Xin Y, Zhang X, Liu N, Peng G, Huang X,
Cao X, Zhou X and Li X: Efficacy and safety of lenvatinib plus PD-1
inhibitor with or without transarterial chemoembolization in
unresectable hepatocellular carcinoma. Hepatol Int. 17:753–764.
2023. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Raoul JL, Forner A, Bolondi L, Cheung TT,
Kloeckner R and de Baere T: Updated use of TACE for hepatocellular
carcinoma treatment: How and when to use it based on clinical
evidence. Cancer Treat Rev. 72:28–36. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Dawson LA, Winter KA, Knox JJ, Zhu AX,
Krishnan S, Guha C, Kachnic LA, Gillin MT, Hong TS, Craig TD, et
al: Stereotactic body radiotherapy vs sorafenib alone in
hepatocellular carcinoma: The NRG oncology/RTOG 1112 phase 3
randomized clinical trial. JAMA Oncol. 11:136–144. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Vilgrain V, Pereira H, Assenat E, Guiu B,
Ilonca AD, Pageaux GP, Sibert A, Bouattour M, Lebtahi R, Allaham W,
et al: Efficacy and safety of selective internal radiotherapy with
yttrium-90 resin microspheres compared with sorafenib in locally
advanced and inoperable hepatocellular carcinoma (SARAH): An
open-label randomised controlled phase 3 trial. Lancet Oncol.
18:1624–1636. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Garin E, Tselikas L, Guiu B, Chalaye J,
Edeline J, de Baere T, Assenat E, Tacher V, Robert C,
Terroir-Cassou-Mounat M, et al: Personalised versus standard
dosimetry approach of selective internal radiation therapy in
patients with locally advanced hepatocellular carcinoma
(DOSISPHERE-01): A randomised, multicentre, open-label phase 2
trial. Lancet Gastroenterol Hepatol. 6:17–29. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Ren Z, Xu J, Bai Y, Xu A, Cang S, Du C, Li
Q, Lu Y, Chen Y, Guo Y, et al: Sintilimab plus a bevacizumab
biosimilar (IBI305) versus sorafenib in unresectable hepatocellular
carcinoma (ORIENT-32): A randomised, open-label, phase 2–3 study.
Lancet Oncol. 22:977–990. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Cai M, Huang W, Huang J, Shi W, Guo Y,
Liang L, Zhou J, Lin L, Cao B, Chen Y, et al: Transarterial
chemoembolization combined with lenvatinib plus PD-1 inhibitor for
advanced hepatocellular carcinoma: A retrospective cohort study.
Front Immunol. 13:8483872022. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Qiu G, Xie K, Jin Z, Jiang C, Liu H, Wan H
and Huang J: The multidisciplinary management of hepatocellular
carcinoma with portal vein tumor thrombus. Biosci Trends.
15:148–154. 2021. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Yang JD and Heimbach JK: New advances in
the diagnosis and management of hepatocellular carcinoma. BMJ.
371:m35442020. View Article : Google Scholar : PubMed/NCBI
|