Introduction
Peliosis hepatis, a hepatic lesion characterized by
blood-filled parenchymal cavities randomly scattered throughout the
liver (1–3), was first described by Wagner (4), but its pathogenesis is a matter of
debate. Peliosis hepatis-like blood-filled cavities are also
frequently observed in the tumors of hepatocellular carcinoma (HCC)
(5–7). This finding is generally referred to
as ‘peliotic change’ in HCC. Almost no clinicopathological
assessment of this peliotic change has been conducted, and it is
still considered little more than an often observed incidental or
accidental finding. However, along with the advances in diagnostic
imaging, peliotic change has drawn attention as a morphological
feature that modifies image findings of HCC.
In the present study, we conducted a
clinicopathological study of HCC with peliotic change (PHCC).
Materials and methods
A total of 294 HCCs without preoperative anticancer
therapies were consecutively resected at Kurume University Hospital
between January 1991 and December 2003. Cases showing a peliosis
hepatis-like change (peliotic change) in the tumor were included
for the study as PHCC and compared with cases of a common type of
HCC as control. The resected liver specimens were fixed in 10%
buffered formalin immediately after hepatectomy, cut serially into
5 mm slices and macroscopically examined. Sections containing tumor
tissues as well as the surrounding liver tissues were embedded in
paraffin, cut into 4-μm sections and routinely stained with
hematoxylin and eosin. Immunohistochemical staining of CD34 was
performed on 20 PHCC cases to examine the endothelial cells of the
sinusoidal blood spaces of the tumor, using mouse monoclonal
antibody against CD34 (anti-CD34; Dako, CA, USA) and the
Streptavidin Peroxidase technique (MaxiTags kits, Immunon™,
Lipshaw, PA, USA). Clinical data were obtained from clinical
charts. Informed consent was obtained from the patients included in
the study.
Statistical analysis was performed using Stat View
version J-5.0 (Abacus Concepts Inc., Berkeley, CA, USA). Difference
of means was assessed by the unpaired Student’s t-test or
Mann-Whitney U test. P<0.05 was considered statistically
significant.
Results
Clinical findings of PHCC
PHCC was observed in 116 (39.5%) out of 294 cases.
Ages ranged from 41 to 78 years (mean 63.2±7.8 SD) in the PHCCs and
from 16 to 80 years (mean 64.5±8.8 SD) in the control group. The
PHCC group included 89 males and 27 females (3.3:1), while the
control group comprised 140 males and 38 females (3.7:1). No
significant difference was noted in gender between the two
groups.
Hepatitis B surface antigen (HBsAg) was found to be
positive in 16 cases (15%) out of 104 in the PHCC group and in 20
cases (12%) out of 163 in the control group. Hepatitis C virus
antibody (HCVAb) was found to be positive in 82 cases (77%) out of
107 in the PHCC group and in 132 cases (80%) out of 166 cases in
the control group, indicating no significant difference between the
two groups. In the remaining 27 and 21 of the 294 cases,
respectively, HBsAg- and HCVAb-positives were unknown.
The laboratory data for asparate aminotransferase,
alanine aminotransferase, albumin, as well as platelet and serum
α-fetoprotein were not significantly different between the two
groups.
Imaging findings of PHCC
Among 59 PHCCs in which abdominal ultrasound
findings were available, 12 (20%) had a hyperechoic pattern and 18
(31%) a mosaic pattern. Among 88 cases of the control group, 17
(19%) had a hyperechoic pattern and 11 (13%) a mosaic pattern,
indicating significantly more lesions with a mosaic pattern in the
PHCC group (P<0.01; Table I).
Furthermore, the mean tumor diameter in the cases with a
hyperechoic pattern and/or mosaic pattern was 3.5±0.8 cm in the
PHCC group and 2.3±0.9 cm in 28 controls. The tumor size of PHCCs
with hyperechoic and/or mosaic patterns was significantly larger
than that of the control (P<0.001).
 | Table IComparison of the ultrasonographic
pattern between hepatocellular carcinoma with peliotic change and a
common type of HCC (control) according to the tumor size. |
Table I
Comparison of the ultrasonographic
pattern between hepatocellular carcinoma with peliotic change and a
common type of HCC (control) according to the tumor size.
| Tumor size (cm) | 0.0–1.0 | 1.1–2.0 | 2.1–3.0 | 3.1–4.0 | 4.1–5.0 | Total (%) |
|---|
| PHCC group |
| Hyperechoic | 0 | 0 | 3 | 5 | 4 | 12 (20) |
| Mosaic | 0 | 1 | 7 | 5 | 5 | 18 (31)a |
| Isoechoic | 0 | 2 | 2 | 2 | 2 | 8 (14) |
| Hypoechoic | 0 | 4 | 7 | 10 | 0 | 21 (36) |
| Total | 0 | 7 | 19 | 22 | 11 | 59 (100) |
| Control group |
| Hyperechoic | 3 | 7 | 6 | 1 | 0 | 17 (19) |
| Mosaic | 0 | 3 | 6 | 1 | 1 | 11 (13) |
| Isoechoic | 2 | 3 | 6 | 5 | 2 | 18 (20) |
| Hypoechoic | 2 | 17 | 19 | 4 | 0 | 42 (48) |
| Total | 7 | 30 | 37 | 11 | 3 | 88 (100) |
In the majority of 50 cases in the PHCC group that
underwent dynamic CT scans, typical HCC patterns were observed,
such as high attenuation in the early enhanced phase and wash-out
in the delay enhanced phase. No specific difference in CT findings
was noted in PHCCs.
Pathological findings of PHCC
Tumor diameter ranged from 1.5 to 5.0 cm (average
3.4±0.9 SD) in the PHCC group and from 0.7 to 4.8 cm (average
2.5±0.9 SD) in the control group, indicating significantly larger
tumors in the PHCC group (P<0.001; Table II). The incidence of PHCC was
related to the increase of tumor diameter. Tumors <2 cm were
found in 10 cases (9%) in the PHCC group and in 65 cases (37%) in
the control. No tumors <1 cm in diameter were detected in the
PHCC group.
| Table IIComparison in tumor size between
hepatocellular carcinoma with peliotic change and a common type of
HCC (control). |
Table II
Comparison in tumor size between
hepatocellular carcinoma with peliotic change and a common type of
HCC (control).
| Tumor size (cm) | PHCC (%) | Control (%) |
|---|
| Average ± SD | 3.4±0.9a | 2.5±0.9 |
|---|
| 0.0–1.0 | 0 (0) | 11 (100) |
| 1.1–2.0 | 10 (16) | 54 (84) |
| 2.1–3.0 | 37 (32) | 77 (68) |
| 3.1–4.0 | 44 (61) | 28 (39) |
| 4.1–5.0 | 25 (76) | 8 (24) |
| Total | 116 (100) | 178 (100) |
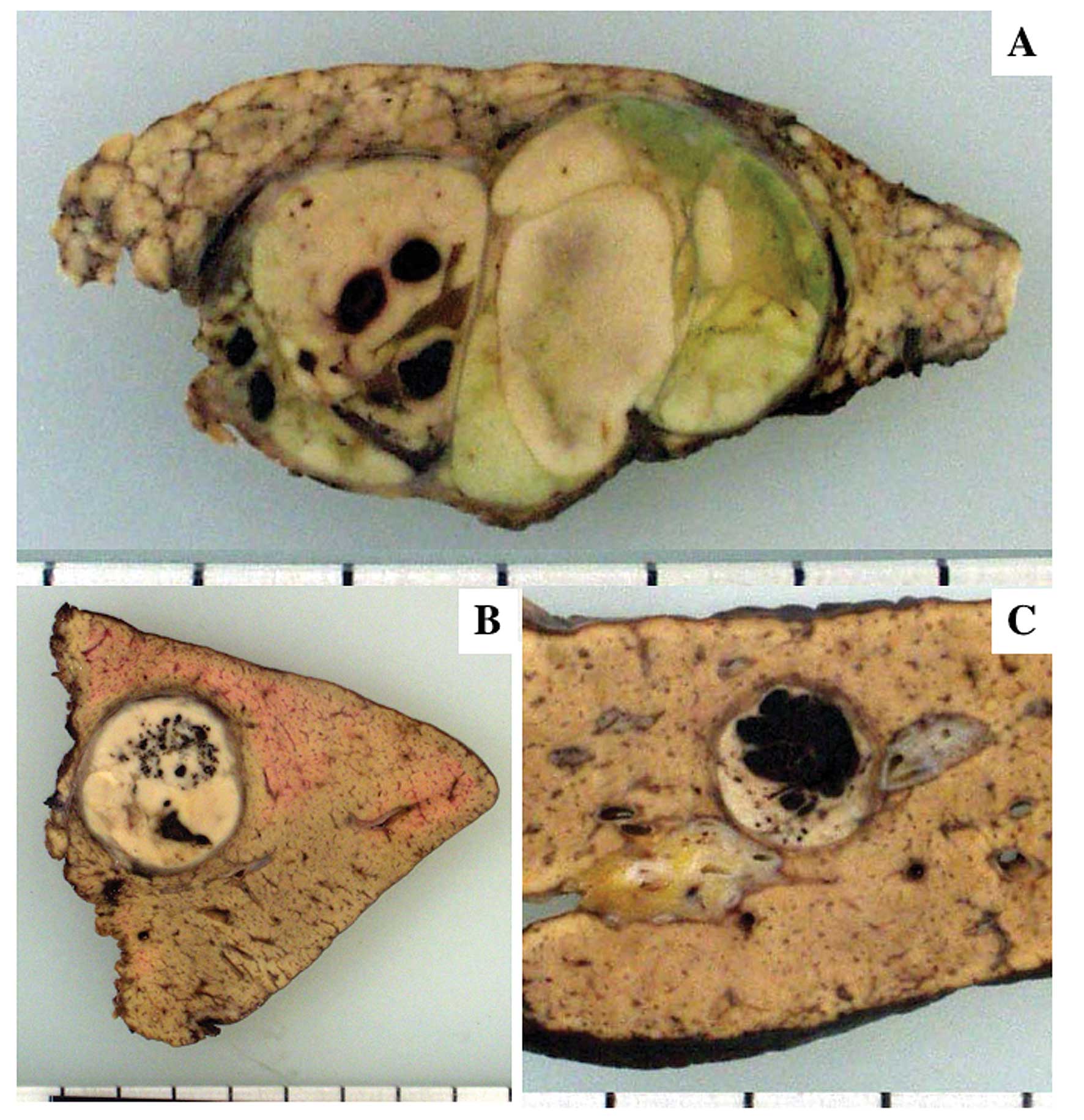
The tumors were completely encapsulated in 108 (93%)
of the 116 PHCCs, but incompletely encapsulated in the remaining 8
cases. On the other hand, encapsulated HCC was observed in 106
(60%) out of 178 tumors in the control group, indicating a
significantly higher frequency of encapsulation in the PHCC group
(P<0.001). Peliotic change was observed as varying sized blood
lakes and hemorrhagic honeycomb-like appearance (Fig. 1A and B). In some cases, peliotic
changes occupied ~2/3 of the cut surface of the tumor. Peliotic
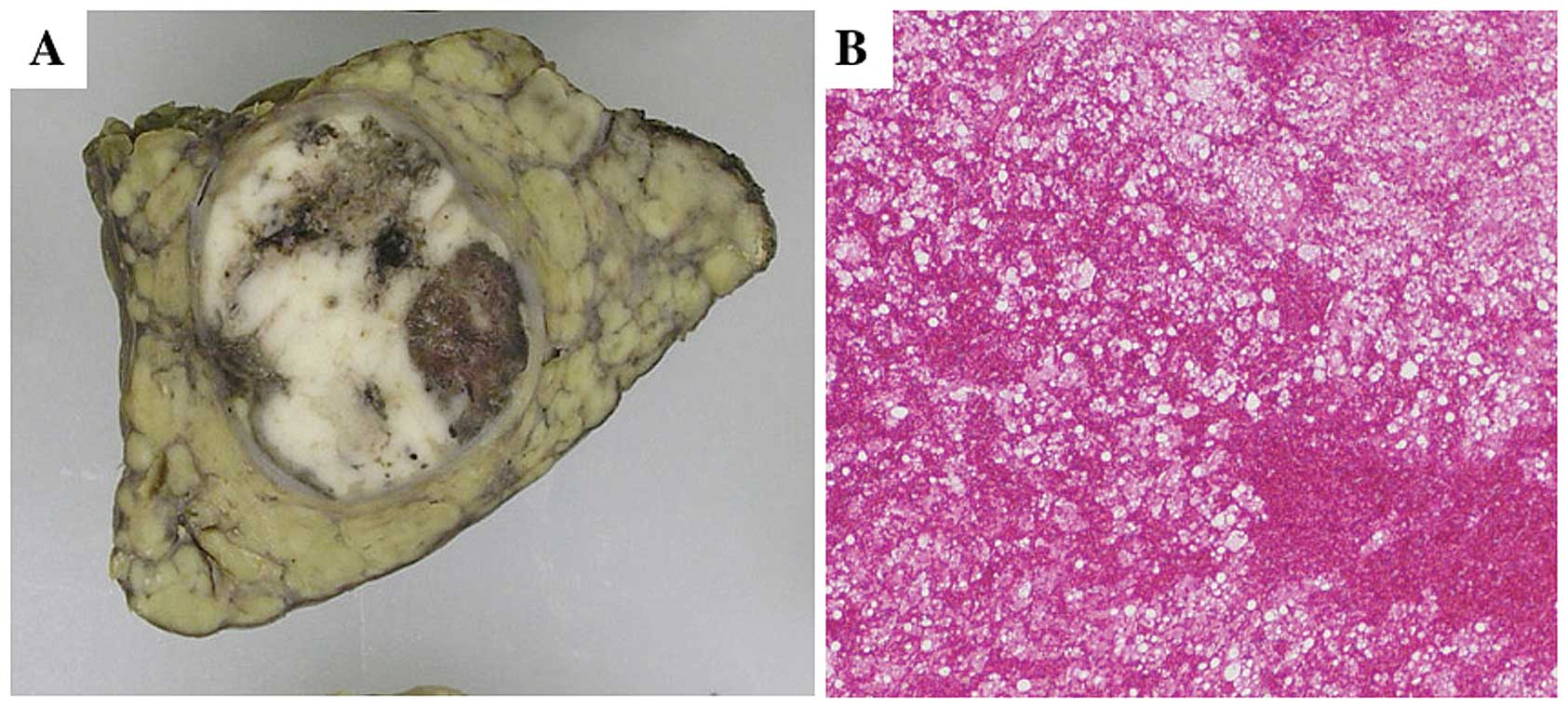
changes were easily distinguished from hemorrhage because the
latter was accompanied by degeneration and/or necrosis of the tumor
tissue (Fig. 2). Fibrous septa were
observed in 76 PHCCs (68%) and in 112 cases (63%) in the control
group.
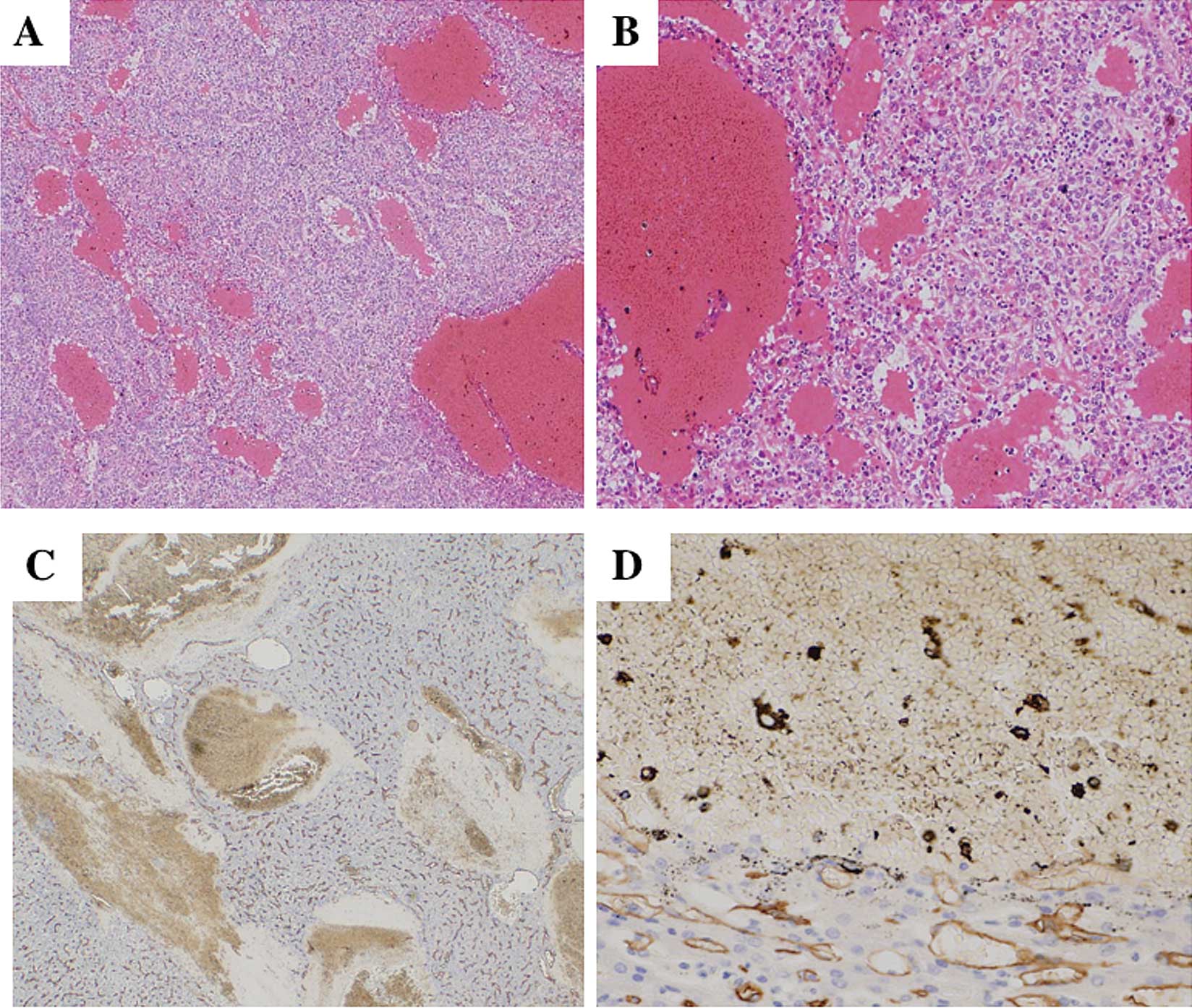
Peliotic change was observed as varying sized blood
lakes without obvious lining of the endothelial cells (Fig. 3A). The lack of endothelial cells was
also confirmed by immunostaining for CD34 (Fig. 3B). The majority of PHCCs were
moderately differentiated showing a trabecular or pseudoglandular
or both patterns. No well-differentiated type was found.
Degeneration or necrosis was not observed around peliotic changes.
A varying degree of sinusoidal dilatation was observed around
peliotic changes. In the control group, 116 tumors (66%) were
moderately differentiated, 55 tumors (31%) were poorly or
moderately to poorly differentiated and 6 tumors (3%) were
well-differentiated. Among 111 PHCCs in which non-cancerous areas
were examined, 66 cases (59%) were chronic hepatitis associated
with varying degrees of fibrosis and 45 (41%) were liver cirrhosis.
Among the 176 cases in the control group, 85 cases (48%) were
chronic hepatitis and 91 (52%) cirrhosis. No significant difference
was ntoed in the background liver between the groups.
Recurrence rate after resection
Follow-up data following surgery were obtained in 32
PHCC cases and in 39 controls. Follow-up periods ranged from 4 to
105 months (mean 38±25.7 SD). Recurrence occurred in 18 PHCC cases
(56%) and in 17 controls (44%). There was no significant difference
between the 2 groups.
Discussion
Peliotic changes are frequently observed in HCCs.
However, the question raised is whether peliotic change is
essentially different from hemorrhage of the tumor. In general,
degenerative change and/or necrosis are observed around hemorrhage
of HCC tumors. Put differently, degeneration and/or necrosis of
tumor tissue cause hemorrhage in HCC. On the other hand, tumor
tissues around peliotic changes are not degenerative or necrotic
and blood is localized within the spaces. Thus, it is suggested
that peliotic changes are different from hemorrhage. However, when
peliotic changes become extensive, they may rupture and hemorrhage
may develop.
Various factors are suggested in the pathogenesis of
peliosis hepatis. These factors are excessive alcohol intake,
hormonal agents such as oral contraceptives and anabolic steroids,
as well as chronic wasting diseases, including malignant tumors and
tuberculosis (8–12). It was also suggested that blood
constituents infiltrate the Disse’s spaces resulting in cyst-like
change of the sinusoids following the mechanical disorder of the
sinusoidal endothelial cells (13).
In a study of 12 cases of peliosis hepatis, Zafrani et al
suggested that the developmental mechanism of peliosis hepatis
obstructed blood channels caused by sinusoidal destruction
accompanying hepatocellular necrosis or the abnormal bonding of
sinusoids and the central vein (2).
Based on the fact that peliotic changes were frequently observed in
the encapsulated tumors, the mechanism of peliotic change in HCC
was explained by endothelial damage due to sinusoidal dilatation
following increased intratumoral pressure. This assumption is
supported by the fact that similar peliotic changes are frequently
observed in liver cell adenoma, which is also an expansive tumor
with frequent encapsulation. Sugimachi et al suggested a
particular relationship between peliotic change in HCC and
angiopoietin-2 (Ang-2), which play a regulatory role in tumor
vessel remodeling (14).
No significant clinical differences were noted
between the PHCC and control groups other than the significantly
higher frequency of hyperechoic and/or mosaic patterns in PHCCs on
ultrasonography. The most common histological feature reflecting
hyperechogenecity in HCC is fatty change of the tumor which most
frequently occurs in small well-differentiated tumors up to ~2 cm
in diameter (15). HCC tumors with
hyperechoic and/or mosaic patterns among tumors >3–4 cm in
diameter are rarely found. In the present study, these tumors
proved to be PHCCs.
Although peliotic change in HCC has little clinical
significance, it is necessary for clinicians and pathologists to
distinguish the presence of peliotic change as a morphological
feature that modifies ultrasonographic patterns of HCC.
Acknowledgements
We thank Ms. Sachiyo Maeda and Ms. Misato Shiraishi
for their technical assistance on immunohistochemical staining.
This study was supported in part by the Sarah Cousins Memorial
Fund, Boston, MA, USA.
References
|
1
|
Karasawa T, Shikata T and Roger DS:
Peliosis hepatis: report of nine cases. Acta Pathol Jpn.
29:457–469. 1979.PubMed/NCBI
|
|
2
|
Zafrani ES, Cazier A, Baudelot AM and
Feldmann G: Ultrastructural lesions of the liver in human peliosis.
A report of 12 cases. Am J Pathol. 114:349–359. 1984.PubMed/NCBI
|
|
3
|
Asano S, Wakasa H, Kaise S, Nishimaki T
and Kasukawa R: Peliosis hepatis: Report of two autopsy cases with
a review of literature. Acta Pathol Jpn. 32:861–877.
1982.PubMed/NCBI
|
|
4
|
Wagner E: Fall von Blutcysten der Leber
(In German). Arch Heilk. 2:369–370. 1861.
|
|
5
|
Kojiro M: Peliosis hepatis (In Japanese).
Acta Hepatol Jpn (KANZO). 38:583–586. 1997. View Article : Google Scholar
|
|
6
|
Grazioli L, Morana G, Caudana R, et al:
Hepatocellular carcinoma: correlation between gadobenate
dimeglumine-enhanced MRI and pathological findings. Invest Radiol.
35:25–34. 2000. View Article : Google Scholar
|
|
7
|
Brancatelli G, Baron RL, Peterson MS and
Marsh W: Helical CT screening for hepatocellular carcinoma in
patient with cirrhosis: frequency and cases of false-positive
interpretation. Am J Roentgenol. 180:1007–1014. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Loomus GN, Aneja P and Bota RA: A case of
peliosis hepatis in association with tamoxifen therapy. Am J Clin
Pathol. 80:881–882. 1983.PubMed/NCBI
|
|
9
|
Dejgaard A, Krogsgaard K and Jacobsen M:
Veno-occlusive disease and peliosis of the liver after thorotrast
administration. Virchows Arch A Pathol Anat Histopathol. 403:87–94.
1984. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Czapar CA, Weldon-Linne CM, Moore DM and
Rhone DP: Peliosis hepatis in the acquired immunodeficiency
syndrome. Arch Pathol Lab Med. 110:611–613. 1986.PubMed/NCBI
|
|
11
|
Russmann S, Zimmermann A, Krahenbuhl S,
Kern B and Reichen J: Veno-occlusive disease, nodular regenerative
hyperplasia and hepatocellular carcinoma after azathioprine
treatment in a patient with uncreative colitis. Eur J Gastroenterol
Hepatol. 13:287–290. 2001. View Article : Google Scholar
|
|
12
|
Drevelengas A, Chourmouzi D and
Boulogianni G: Peliosis of the liver in a patient with prostate
carcinoma. JBR-BTR. 86:158–159. 2003.PubMed/NCBI
|
|
13
|
Shim SG, Paik SW, Hyun JG, et al: Lipiodol
accumulation in focal peliosis hepatis with sinusoidal dilatation.
J Clin Gastroenterol. 32:356–358. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Sugimachi K, Tanaka S, Taguchi K, Aishima
S, Shimada M and Tsuneyoshi M: Angiopoietin switching regulates
angiogenesis and progression of human hepatocellular carcinoma. J
Clin Pathol. 56:854–860. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Kutami R, Nakashima Y, Nakashima O, Shiota
K and Kojiro M: Pathomorphologic study on the mechanism of fatty
change in small hepatocellular carcinoma of humans. J Hepatol.
33:282–289. 2000. View Article : Google Scholar : PubMed/NCBI
|