Introduction
Radiofrequency ablation (RFA) has become a
favourable technique for the treatment of small hepatocellular
carcinoma (HCC) because of its feasibility, effectiveness,
repeatability and safety (1–6). Local
therapy for HCC is widely employed, including percutaneous ethanol
injection and RFA. A prospective study demonstrated that RFA
requires fewer sessions than percutaneous ethanol injection in
patients with small HCCs (1). In
most HCC patients, treatment options are limited by patient liver
dysfunction caused by underlying chronic inflammation and
cirrhosis. Although complete surgical resection of HCC offers the
best chance of long-term survival, cirrhosis may limit the extent
of parenchymal resection that can be tolerated, increasing the risk
of postoperative liver failure and death (7). There is no significant difference of
overall or disease-free survival between surgical resection and RFA
when HCC patients are in Child-Pugh class B (8). However, some cases of rapid and
aggressive recurrence of HCC after RFA were reported (9–11). In
this study, we reviewed 15 resected HCC patients who developed
local recurrence after RFA therapy, and we compared their
pathological and clinical features with those of resected HCC
patients without RFA.
Materials and methods
Patients
Between January 2000 and December 2006, 174 HCC
patients underwent surgery at the Department of Gastroenterological
Surgery of Kanazawa University Hospital (Kanazawa, Japan). Among
them, 15 patients had developed local recurrence of HCC after RFA
therapy. They included 12 men and 3 women with an average age of
62.5 years (range 44–79). In 6 patients, needle biopsy of the HCC
was performed before RFA at the Department of Internal Medicine (I)
of Kanazawa University Hospital.
Pathological specimens
For this study, formalin-fixed and paraffin-embedded
specimens were retrieved from the surgical pathology files of the
Pathology Department of Kanazawa University Hospital. The tumors
were evaluated according to the general rules for the clinical and
pathological study of liver cancer proposed by the Japanese Liver
Cancer Group.
Statistical analysis
For statistical analysis, p-values were calculated
by a two-tailed test and p<0.05 was considered to indicate
statistical significance.
Results
Four of the 15 HCC patients with local recurrence
after RFA therapy had a fatal outcome. One patient presenting with
cirrhosis due to hepatitis C, succumbed to hepatic failure caused
by fibrosing cholestatic hepatitis after living-related donor liver
transplantation, and one patient succumbed to liver failure
postoperatively. The other two patients succumbed to tumor
recurrence.
There were no significant differences of baseline
characteristics, including gender, age and type of hepatitis virus,
in patients who developed local recurrence of HCC after RFA and HCC
patients without RFA (Table I).
 | Table IBaseline data of the two groups. |
Table I
Baseline data of the two groups.
| Local recurrence
after RFA therapy | Without RFA | p-value |
|---|
| Age | 60.5 | 63.5 | N.S. |
| Gender
(male:female) | 11:04 | 117:33 | N.S. |
| Hepatitis B
virus | 7 (46.7%) | 52 (33.8%) | N.S. |
| Hepatitis C
virus | 7 (46.7%) | 76 (49.4%) | N.S. |
| Non-B non-C | 1 (6.6%) | 26 (16.8%) | N.S. |
In the 15 patients with local recurrence after RFA,
the tumors showed significantly more invasive growth, more vascular
invasion and less differentiation compared with those of the 144
patients without RFA (Tables
II–IV).
| Table IIPattern of tumor growth. |
Table II
Pattern of tumor growth.
| Pattern | Local recurrence
after RFA | Without RFA |
|---|
| Expansive | 10 (66.7%) | 138 (94.5%) |
| Invasive | 5 (33.3%) | 8 (5.5%) |
| Table IVVascular invasion. |
Table IV
Vascular invasion.
| Vascular
invasion | Local recurrence
after RFA (%) | Without RFA (%) |
|---|
| Positive | 12 (80.0) | 56 (39.2) |
| Negative | 3 (20.0) | 87 (60.8) |
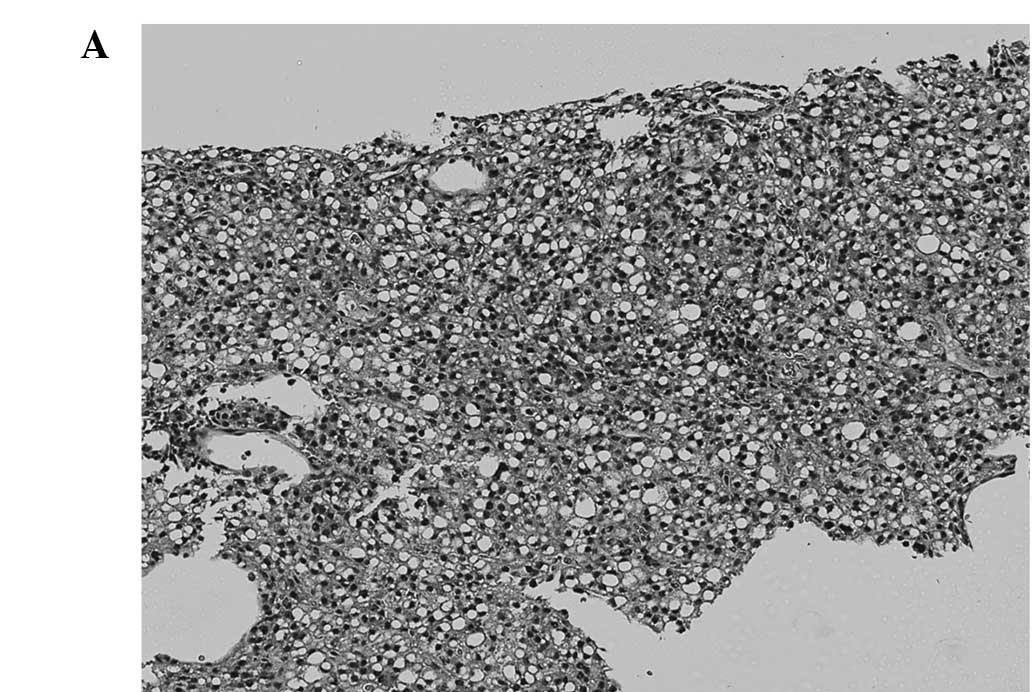
Six patients who developed local recurrence
underwent tumor biopsy before starting RFA. In 5 of these 6
patients, dedifferentiation of HCC was observed. One
well-differentiated HCC changed to poorly differentiated HCC
(Fig. 1), three well-differentiated
HCCs changed to moderately differentiated and one
well-to-moderately differentiated HCC changed to moderately
differentiated. Only one moderately differentiated HCC was
unchanged after RFA therapy (Table
V).
| Table VTumor differentiation before and after
RFA. |
Table V
Tumor differentiation before and after
RFA.
| Case number | Differentiation
before RFA (tumor biopsy) | Differentiation of
the recurrent tumor (resected specimen) |
|---|
| 1 | Well diff. | Poorly diff. |
| 2 | Well diff. | Moderately diff. |
| 3 | Well diff. | Moderately diff. |
| 4 | Well diff. | Moderately diff. |
| 5 | Well-to-moderately
diff. | Moderately diff. |
| 6 | Moderately diff. | Moderately diff. |
Discussion
RFA is now accepted as a curative procedure for
liver tumors. The intratumoral application of RF energy for 15–30
min causes coagulative necrosis in a 2.5- to 5-cm sphere (12). In order to achieve a good
oncological result, this sphere has to include a margin of
cancer-free liver tissue that extends at least 1 cm beyond the
tumor. RFA is now used widely and some studies about risk factors
for local recurrence of HCC after RFA have been reported (13–14).
Hori et al suggested that the most important variables
influencing the local recurrence rate were tumor size and location
relative to the liver surface (13). It was reported that the laparoscopic
approach combined with the artificial pleural effusion and ascites
method of percutaneous treatment was effective for the treatment of
HCC located just beneath the diaphragm and close to the liver
surface (15–17).
The necrotic zone is not spherical when a tumor is
located near vessels that can be detected by abdominal computed
tomography, magnetic resonance imaging or ultrasonography (18). This is because larger vessels
influence the extent of coagulative necrosis produced by RFA via
the well-known cooling effect. The final size of the coagulated
zone depends on heat loss due to convection through blood flow.
This reduction of the necrotic zone by the cooling effect raises
the possibility that the local recurrence rate would be higher for
tumors situated near vessels. Yamasaki et al reported on the
efficacy of RFA with balloon occlusion of the hepatic artery for
the treatment of tumors >30 mm in diameter (19). However, in the present study, tumor
location in relation to blood vessels had no significant influence
on the local recurrence rate and tumor vascularity showed no
significant relationship to local recurrence after a single session
of RFA. These results suggest that arterial blood flow is not
likely to decrease the volume of the necrotic zone when a tumor is
<3.0 cm in diameter.
However, some cases of rapid and aggressive
recurrence of HCC after RFA, whose tumors were found to be <3.0
cm in diameter, were reported (9–11).
Nicoli et al suggested that the RFA needle was able to
connect between two vascular territories (the arteries and the
portal veins) (4). A possible
explanation for the rapid spread of neoplastic cells is that
seeding along this new link facilitates the migration of tumor
cells from the high-pressure arterial territory to the low-pressure
portal territory. It is well known that once HCC cells reach the
portal branches, invasion of other liver segments occurs. Thus, in
addition to the risk of seeding along the needle track, the risk of
intrahepatic spread after insertion of the RFA needle must be
considered. The risk of seeding may be high if an arteriovenous
fistula is created by the RFA needle. Portolani et al
suggested that the thermal energy emitted by the RFA instrument can
induce local hypertension and rupture the pseudocapsule, leading to
the spread of viable neoplastic cells in the perilesional liver
parenchyma or directly into blood vessels or the biliary tract
(10). Thus, it is possible that a
vascular link between the hepatic arteries and portal veins or an
increase of intratumoral pressure resulting from the high
temperature during the ablation process releases tumor cells, or
that the penetration of the RFA needle into a small portal branch
leads to intraportal tumor spread.
In addition, heat stress induces the tyrosine
phosphorylation and activation of a human carcinoma
dedifferentiation modulator (20).
Accordingly, it is suspected that the thermal effect of RFA may
increase the malignant potential of the residual viable tumor
cells, resulting in rapid and aggressive progression.
Vivarelli et al compared overall and
disease-free survival in surgical resection and RFA patients. They
reported that resection was superior to RFA in terms of overall and
disease-free survival. However, they also reported that there were
no significant differences of overall and disease-free survival
between surgical resection and RFA when the patients were in
Child-Pugh class B (8). The
incidence of local failure after RFA was reported to be as low as
1.8%, but reached 12–18% as reported by other authors (21–23).
In our department, the local recurrence rate after RFA is higher
compared with that for surgery, but the difference is not
significant (8.3 vs. 1.3%, p=0.13).
The impact of the complications reported here may
temper the optimistic outcome reported in some initial series
(21), suggesting that caution is
needed with regard to the indications and application of RFA,
particularly in patients who are also suitable for surgery. In such
patients, the advantage of low mortality and morbidity may be
reduced by the possibility of non-curative treatment leading to
tumor progression. The risk of aggressive recurrence after RFA must
be considered when assessing the options for treatment of HCC.
Recurrence after RFA may lead to aggressive tumor evolution that
precludes any possibility of cure. RFA should only be considered a
suitable alternative to surgery in high-risk patients.
References
|
1
|
Rossi S, Garbagnati F, Lencioni R, et al:
Percutaneous radio-frequency thermal ablation of nonresectable
hepatocellular carcinoma after occlusion of tumor blood supply.
Radiology. 217:119–126. 2000. View Article : Google Scholar
|
|
2
|
Livraghi T, Goldberg SN, Lazzaroni S, et
al: Small hepatocellular carcinoma: treatment with radio-frequency
ablation versus ethanol injection. Radiology. 210:655–661. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Allgaier HP, Deibert P, Zuber I, et al:
Percutaneous radiofrequency interstitial thermal ablation of small
hepatocellular carcinoma. Lancet. 353:1676–1677. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Nicoli N, Casaril A, Marchiori L, et al:
Intraoperative and percutaneous radiofrequency thermal ablation in
the treatment of hepatocellular carcinoma. Chir Ital. 52:29–40.
2000.PubMed/NCBI
|
|
5
|
Nicoli N, Casaril A, Marchiori L, et al:
Treatment of recurrent hepatocellular carcinoma by radiofrequency
thermal ablation. J Hepatobiliary Pancreat Surg. 8:417–421. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Solbiati L, Livraghi T, Goldberg SN, et
al: Percutaneous radio-frequency ablation of hepatic metastases
from colorectal cancer: long-term result in 117 patients.
Radiology. 221:159–166. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Steven AC, Francesco I, Lee ME, Vauthey JN
and Paolo V: Radiofrequency ablation of hepatocellular cancer in
110 patients with cirrhosis. Ann Surg. 232:381–391. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Vivarelli M, Guglielmi A, Ruzzenente A, et
al: Surgical resection versus percutaneous radiofrequency ablation
in the treatment of hepatocellular carcinoma on cirrhotic liver.
Ann Surg. 204:102–107. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Nicoli N, Casaril A, Hilal MA, et al: A
case of rapid intrahepatic dissemination of hepatocellular
carcinoma after radiofrequency thermal ablation. Am J Surg.
188:165–167. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Portolani N, Tiberio GA, Ronconi M, et al:
Aggressive recurrence after radiofrequency ablation of liver
neoplasms. Hepatogastroenterology. 50:2179–2184. 2003.PubMed/NCBI
|
|
11
|
Takada Y, Kurata M and Ohkohchi N: Rapid
and aggressive recurrence accompanied by portal tumor thrombus
after radiofrequency ablation for hepatocellular carcinoma. Int
Clin Oncol. 8:332–335. 2003. View Article : Google Scholar
|
|
12
|
Wood TF and Bilchik AJ: Radiofrequency
thermal ablation as treatment for liver cancer at the John Wayne
Cancer Institute. Onc Issue. 16:17–20. 2001.
|
|
13
|
Hori T, Nagata K, Hasuike S, et al: Risk
factor for the local recurrence of hepatocellular carcinoma after a
single session of percutaneous radiofrequency ablation. J
Gastroenterol. 38:977–981. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ono K, Kokubu S, Hidaka H, et al: Risk
factors of delay in restoration of hepatic reserve capacity and
local recurrence after radiofrequency ablation therapy for
hepatocellular carcinoma (HCC). Hepatology Res. 31:172–177. 2005.
View Article : Google Scholar
|
|
15
|
Abe T, Shinzawa H, Wakabayashi H, Aoki M,
et al: Value of laparoscopic microwave coagulation therapy for
hepatocellular carcinoma in relation to tumor size and location.
Endoscopy. 32:598–603. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Horigome H, Nomura T, Saso K, Joh T, Ohara
H and Itoh M: Artificial ascites method: percutaneous treatments
for hepatocellular carcinoma located just beneath the diaphragm. Am
J Gastroenterol. 95:2404–2405. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Montorsi M, Santambrogio R, Bianchi P, et
al: Radiofrequency interstitial thermal ablation of hepatocellular
carcinoma in liver cirrhosis. Role of the laparoscopic approach.
Surg Endosc. 15:141–145. 2001. View Article : Google Scholar
|
|
18
|
Patterson EJ, Scudamore CH, Owen DA, Nagy
AG and Buczkowski AK: Radiofrequency ablation of porcine liver in
vivo: effects of blood flow and treatment time on lesion size. Ann
Surg. 227:559–565. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yamasaki T, Kurokawa F, Shirahashi H,
Kusano N, Hironaka K and Okita K: Percutaneous radiofrequency
ablation therapy for patients with hepatocellular carcinoma during
occlusion of hepatic blood flow. Comparison with standard
percutaneous radiofrequency ablation therapy. Cancer. 95:2353–2360.
2002. View Article : Google Scholar
|
|
20
|
Yang SD, Lee SC and Chang HC: Heat stress
induces tyrosine phosphorylation/activation of kinase FA/GSK-3
alpha (a human carcinoma dedifferentiation modulator) in A431
cells. J Cell Biochem. 66:16–26. 1997. View Article : Google Scholar
|
|
21
|
Llovet JM, Vilana R, Bru C, et al:
Increased risk of tumor seeding after percutaneous radiofrequency
ablation for single hapatocellular carcinoma. Hepatology.
33:1124–1129. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Siperstein A, Garland A, Engle K, et al:
Local recurrence after laparoscopic radiofrequency thermal ablation
of hepatic tumors. Ann Surg Oncol. 7:106–113. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wood TF, Rose DM, Chung M, Allegra DP,
Foshag LJ and Bilchik AJ: Radiofrequency ablation of 231
unresectable hepatic tumors: indications, limitations and
complications. Ann Surg Oncol. 7:593–600. 2000. View Article : Google Scholar : PubMed/NCBI
|