Introduction
Lung cancer is a leading cause of cancer-related
mortality worldwide, and ~80% of cases with lung cancer are
non-small cell lung cancer (NSCLC) (1,2). The
majority of NSCLC patients present with advanced disease at
diagnosis. Cytotoxic chemotherapy, specifically, platinum-based
doublets, has been recommended as standard treatment for these
patients (3). However, standard
chemotherapy for advanced NSCLC has reached a therapeutic plateau
with a median survival of ~1 year (4,5).
Therefore, more effective strategies must be explored.
Metronomic chemotherapy (MET) is a therapeutic
approach by chronic administration of chemotherapeutic agents at a
relatively low and minimally toxic dose without a prolonged
drug-free break (6). During the
past decade, MET with different chemotherapeutic agents has been
demonstrated to significantly reduce side effects associated with
standard chemotherapy, and to inhibit tumor growth and metastasis
by antagonizing angiogenesis (6,7), a
hallmark event during cancer development and a key component for
the continuous growth and metastasis of tumor cells. Additionally,
recent studies have suggested that MET may be a multi-targeted
anti-tumor strategy by restoring anti-tumor immunity and inducing
tumor dormancy (7). A previous
study has shown that metronomic administration of cyclophosphamide
(CPA) in drinking water at low doses (10–40 mg/kg) on a daily basis
is effective in delaying the growth of orthotopic breast or ectopic
colon cancer xenografts in nude or SCID mice (8). This study, together with many
preclinical experiments and clinical trials, provides accumulative
evidence that MET can maintain the therapeutic response, minimize
the relapse after conventional chemotherapy, and overcome the
resistance (6,7,9).
Endostar is a recombinant human endostatin with an
additional nine-amino acid sequence at the N-terminal of the
protein to help in protein purification, solubility and stability
(10). This anti-angiogenic drug is
used in combination with standard chemotherapy for the treatment of
advanced NSCLC in China and being investigated in other types of
cancer, including breast, colon and pancreatic cancers (11). However, whether Endostar combined
with MET CPA could enhance anti-tumor and anti-angiogenic effects
in advanced NSCLC remains unclear. In the present study, we
employed a xenograft model of human NSCLC to evaluate the role of
MET CPA and/or Endostar on the growth and angiogenesis of implanted
lung cancers as well as survival of tumor-bearing animals.
Materials and methods
Cell culture and chemicals
A human lung adenocarcinoma cell line, A549, was
purchased from the Chinese Academy of Sciences (Shanghai, China)
and cultured in Dulbecco’s modified Eagle’s medium (DMEM, Gibco
BRL, Carlsbad, CA, USA) supplemented with 10% fetal bovine serum
(FBS, Gibco) at 37°C in a humidified atmosphere containing 5%
CO2. Endostar was obtained from Simcere Pharmaceutical
Group (Nanjing, China) and cyclophosphamide monohydrate (CPA) was
purchased from International Laboratory (San Bruno, CA, USA).
Mouse xenograft model and treatments
The experimental protocols were approved by the
Institutional Animal Care and Use Committees of Bengbu Medical
College (Anhui, China). Four-week-old BALB/c nude mice were
purchased from the Experimental Animal Center, Chinese Academy of
Sciences (Shanghai, China). Mice were housed (5 mice/per cage) in a
specific pathogen-free facility at a constant temperature of
25–27°C, a constant humidity of 40–50% on a cycle of 12/12-h
light/dark, with access to autoclaved food and water ad
libitum. To establish the xenograft model, A549 cells
(2.5×106 in 100 μl of DMEM) were injected subcutaneously
into the back close to the right axilla of individual animals. The
tumor growth was monitored every 3 days by measuring the length (L)
and width (W) of the tumors, with the volume (V) calculated as V =
0.52 × L × W2, as previously described (12). When the tumors grew to ~200
mm3, the tumor-bearing mice were randomly assigned and
injected intraperitoneally (i.p.) with saline vehicle daily as the
control group (Ctrl), or treated with 10 mg/kg body weight (bw) of
CPA daily by gavage as the metronomic CPA group (MET CPA) (8,12), or
4 mg/kg bw of Endostar i.p. daily as the Endostar group (Endo), or
the same routes and doses of metronomic CPA and Endostar as the MET
CPA combined with Endostar group (MET CPA + Endo), or 100 mg/kg bw
of CPA i.p. on days 1, 3 and 5, and repeated every 21 days as the
maximum tolerance dose group (MTD CPA), respectively (n=14–15 per
group). The growth of xenograft tumors was monitored up to 12 weeks
post-treatment, and survival of mice was recorded. Eight mice from
individual groups were sacrificed randomly at 9 weeks
post-treatment, with the blood samples collected and the tumor
tissues dissected out for further analysis.
Flow cytometry analysis of peripheral
blood circulating endothelial cells (CECs)
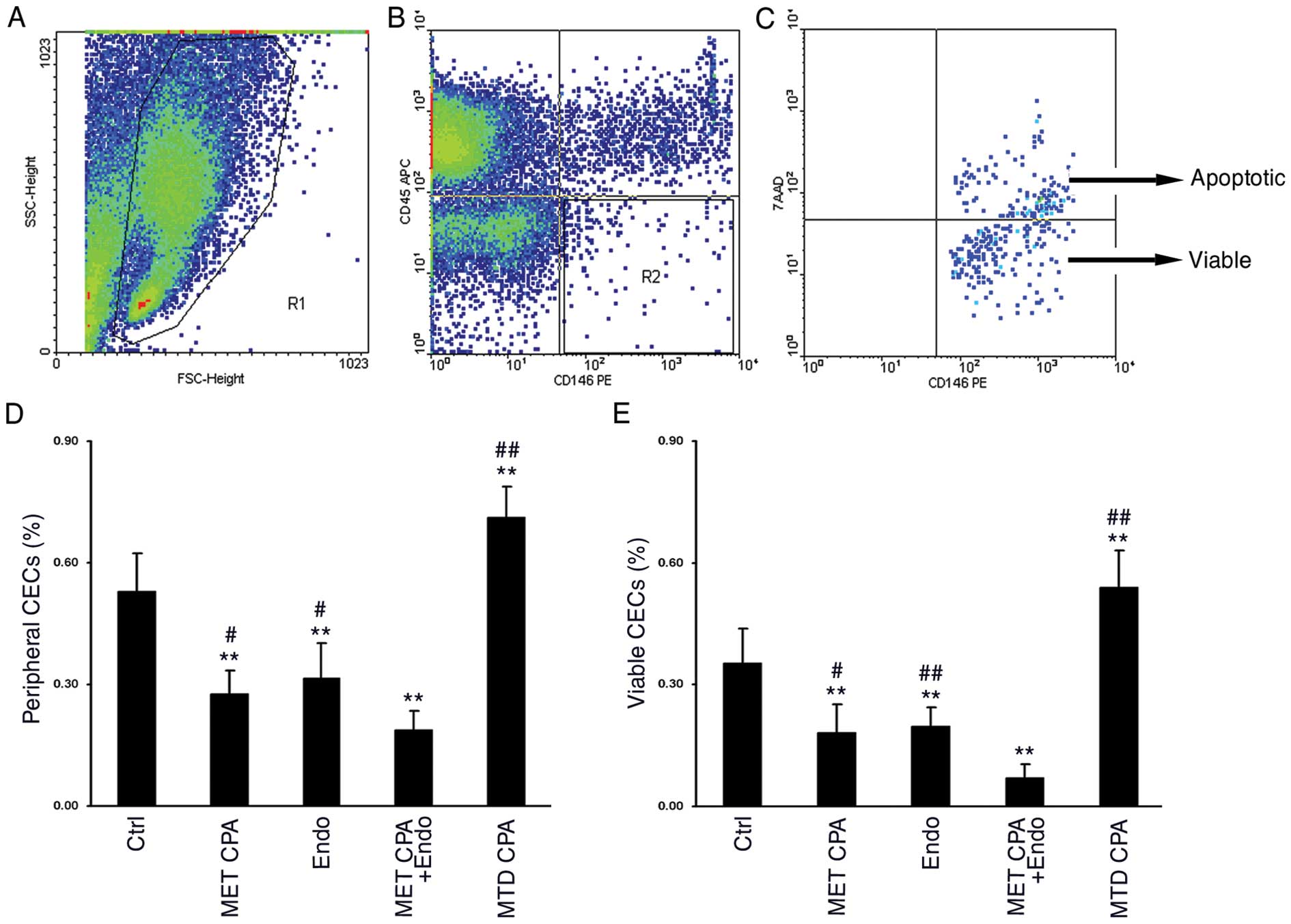
The frequency of peripheral blood CECs was
determined using four-color flow cytometry (FACSCalibur, BD
Biosciences, San Jose, CA), as described previously (13,14).
Briefly, peripheral blood nuclear cells were prepared from
individual mice after lyzing red blood cells. Subsequently, the
cells were stained with APC-anti-CD45 (1:10, Biolegend, San Diego,
CA, USA) to exclude hematopoietic cells, PE-anti-CD146 (1:10,
Biolegend), and 7-amino-actinomycin D (7AAD, 1:10, Biolegend) to
distinguish viable CECs from dead ones. The APC-rat-IgG2b (1:10,
Biolegend) and PE-rat-IgG2a (1:10, Biolegend) were used as isotype
controls. A total of 100,000 events from individual samples were
gated on R1 to exclude platelets, dead cells, and debris and the
CD45−CD146+ cells (R2) were further analyzed
for their 7AAD staining. As a result,
CD146+7AAD+ cells represent apoptotic CECs
while CD146+7AAD− cells represent viable
ones.
Immunofluorescence staining
The MVD and pericyte coverage in xenograft tumors
were quantified using a laser confocal microscope (Nikon, Japan)
(12). Briefly, tumor tissues from
individual mice at 9 weeks post-treatment were fixed in 10%
zinc-formalin for 1 h at 4°C, and dehydrated in 30% sucrose in PBS
until the tissues sank to the bottom. The tumor tissues were
embedded in optimal cutting temperature (OCT) medium, frozen and
sectioned. At least 20 tissue sections at 4 μm were prepared for
individual tumors. Five inconsecutive sections from individual
tumors were selected for immunofluorescence staining. Individual
sections were stained with monoclonal antibodies against CD31
(1:50, Biolegend), NG2 (1:50, Abcam, Cambridge, UK) or isotype
controls at 4°C overnight. After being washed with PBS 3 times (10
min each), the tissue sections were probed with fluorescent-labeled
secondary antibodies (1:100, Abcam) at 37°C for 1 h. The sections
were mounted with mounting buffer containing
4′,6-diamidino-2-phenylindole (DAPI, Santa Cruz, CA, USA) and
covered with a coverslip. The value of MVD was counted as the
number of CD31+ tubular structures from five random
fields and pericyte coverage was quantified as the percent of
NG2+ signals among circumference of CD31+
cross-sections or length of CD31+ longitudinal-sections
from five vessel profiles under high-power field (magnification
×400) per section.
Statistical analysis
Statistical analysis was performed with SPSS 11.0
software. All measurements were presented as mean ± SD. Statistical
comparisons were first tested for homogeneity of variances.
Multiple comparisons were performed using One-way ANOVA analysis,
with two-two comparisons using Student-Newman-Keul (SNK) test.
Survival analysis was performed with the log-rank test. P<0.05
was considered statistically significant.
Results
MET CPA combined with Endostar inhibits
the growth of xenograft tumors in vivo
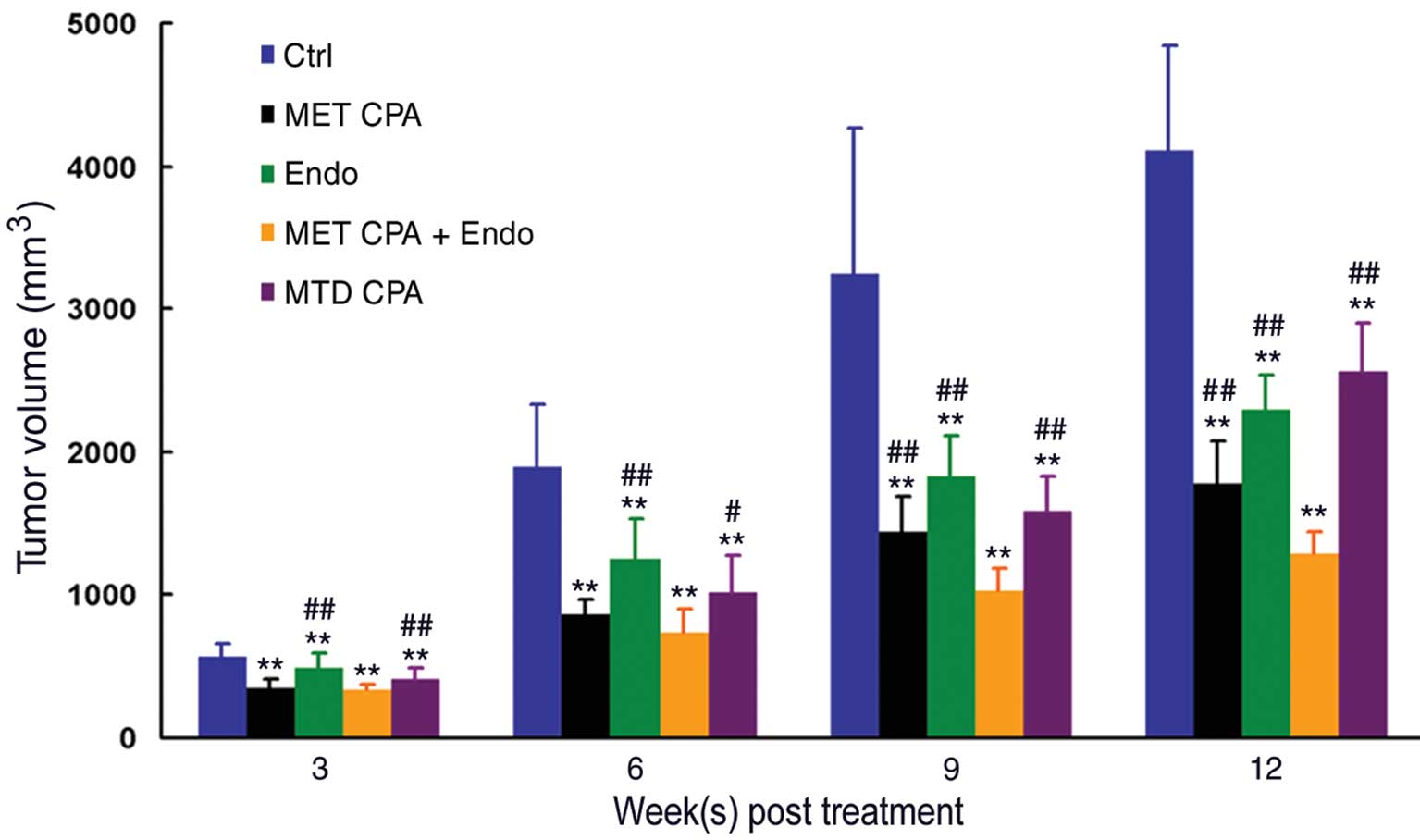
The growth of xenograft tumors in mice treated with
MET CPA alone, Endostar alone, MET CPA plus Endostar, or MTD CPA
alone is shown in Fig. 1. In
comparison with that in the controls, the tumor volumes in all
drug-treated groups of mice were significantly smaller (P<0.01),
indicating that treatment with either drug inhibited the growth of
xenograft tumors in vivo. More importantly, the tumor
volumes in the MET CPA + Endo group of mice were significantly less
than that in all other groups at 3, 6, 9 and 12 weeks
post-treatment, except that the difference between the MET CPA and
MET CPA + Endo group was not significant at 3 and 6 weeks
post-treatment (P>0.05). Collectively, these data indicated that
treatment with either drug inhibited the growth of xenograft
tumors, and that MET CPA combined with Endostar had the most robust
anti-tumor effect in this experimental model.
MET CPA combined with Endostar reduces
the frequency of peripheral blood CECs in the tumor-bearing
mice
The peripheral blood CECs is an excellent surrogate
marker for evaluation of vascular damage and neoangiogenesis, which
are involved in the growth and metastasis of cancer (15,16).
To understand whether alterations in vascular damage or
angiogenesis are involved in the delayed growth of xenograft tumors
conferred by MET CPA combined with Endostar, we first characterized
the frequency of peripheral blood CECs from mice of different
groups at 9 weeks post-treatment (Fig.
2). First, there was no significant difference in the total
numbers of blood nuclear cells among these groups of mice (data not
shown). Second, relatively high frequency of total and viable
peripheral blood CECs (0.53±0.09 and 0.35±0.08%, respectively) was
detected in the Ctrl group. Third, while treatment with MTD CPA
increased the frequency of both total and viable CECs in mice
(0.71±0.07 and 0.54±0.09%, respectively, P<0.01), treatment with
MET CPA or Endostar significantly reduced it (P<0.01).
Furthermore, the frequency of both total and viable CECs in the MET
CPA + Endo group of mice (0.19±0.05 and 0.07±0.03%, respectively)
was significantly lower than that in the other groups of mice (all
P<0.05). Collectively, these data indicated that MET CPA or
Endostar significantly decreased the frequency of peripheral blood
CECs and treatment with both further reduced it in mice.
MET CPA combined with Endostar reduces
the tumor-associated MVD
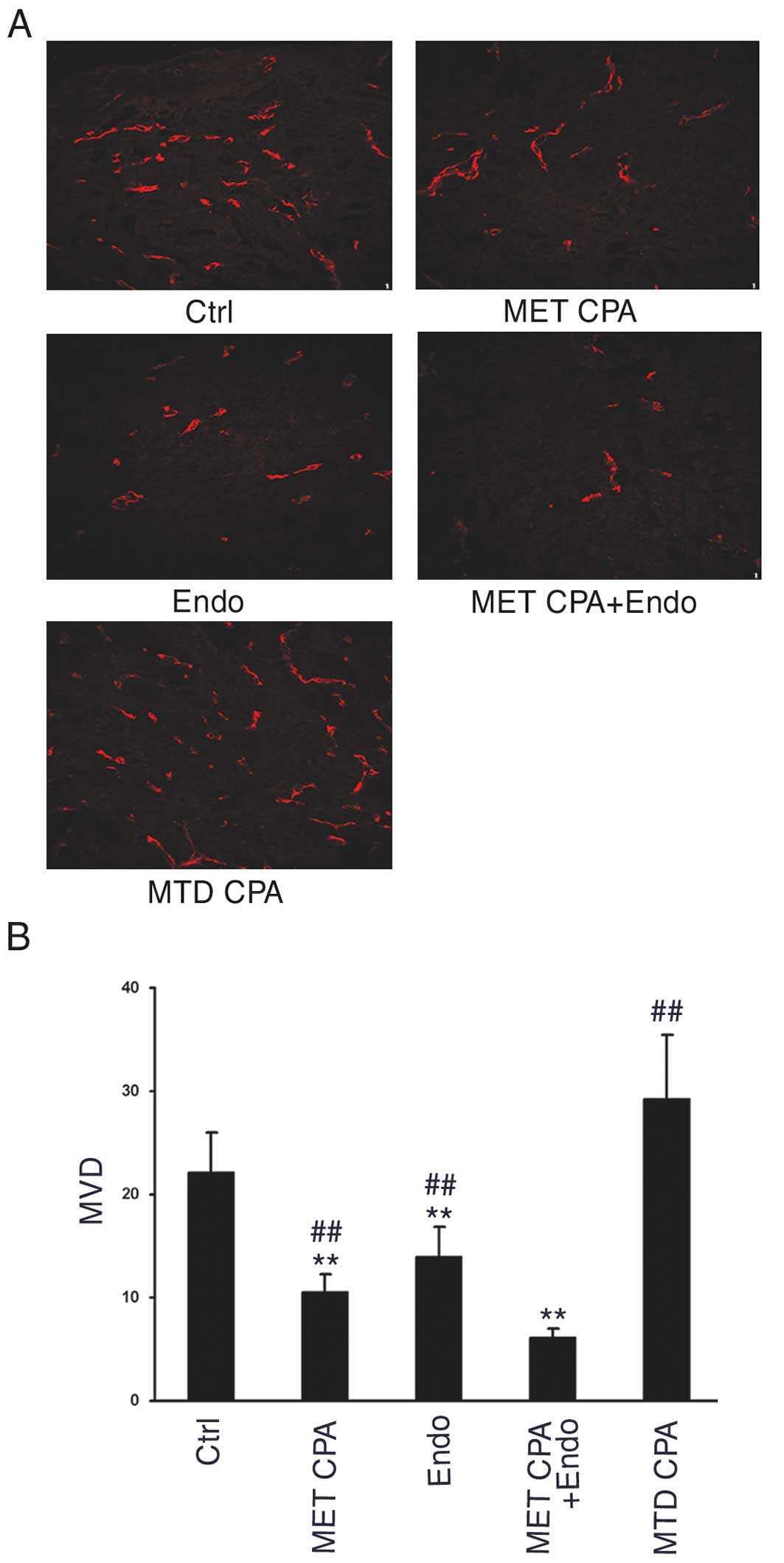
Next, we examined MVD in xenograft tumors by
immunofluorescence staining with antibody against CD31, a specific
marker of endothelial cells. As shown in Fig. 3, a high level of MVD was detected in
tumor tissues from the Ctrl and MTD CPA groups of mice, but
significantly lower value of MVD was observed in tumor tissues from
the MET CPA, Endo, and MET CPA + Endo groups of mice. Quantitative
analysis indicated that the value of MVD in the Ctrl group
(22.08±3.98) was similar to that in the MTD CPA group of mice
(29.29±6.11, P>0.05), both significantly greater than that in
the MET CPA (10.58±1.71) and Endo groups (14.04±2.86, P<0.01).
These data suggested that MET CPA or Endostar, but not MTD CPA,
significantly inhibited the formation of microvascular vessels in
xenograft tumors. Notably, the value of MVD in tumor tissues from
the MET CPA + Endo group of mice (6.08±0.96) was not only
significantly less than that in the Ctrl and MTD CPA groups of
mice, but also significantly less than that in the MET CPA or Endo
groups (P<0.01 vs. other groups). Thus, MET CPA plus Endostar
could further mitigate the tumor growth-induced microvassel
angiogenesis in mice.
MET CPA combined with Endostar reduces
pericyte coverage in xenograft tumors
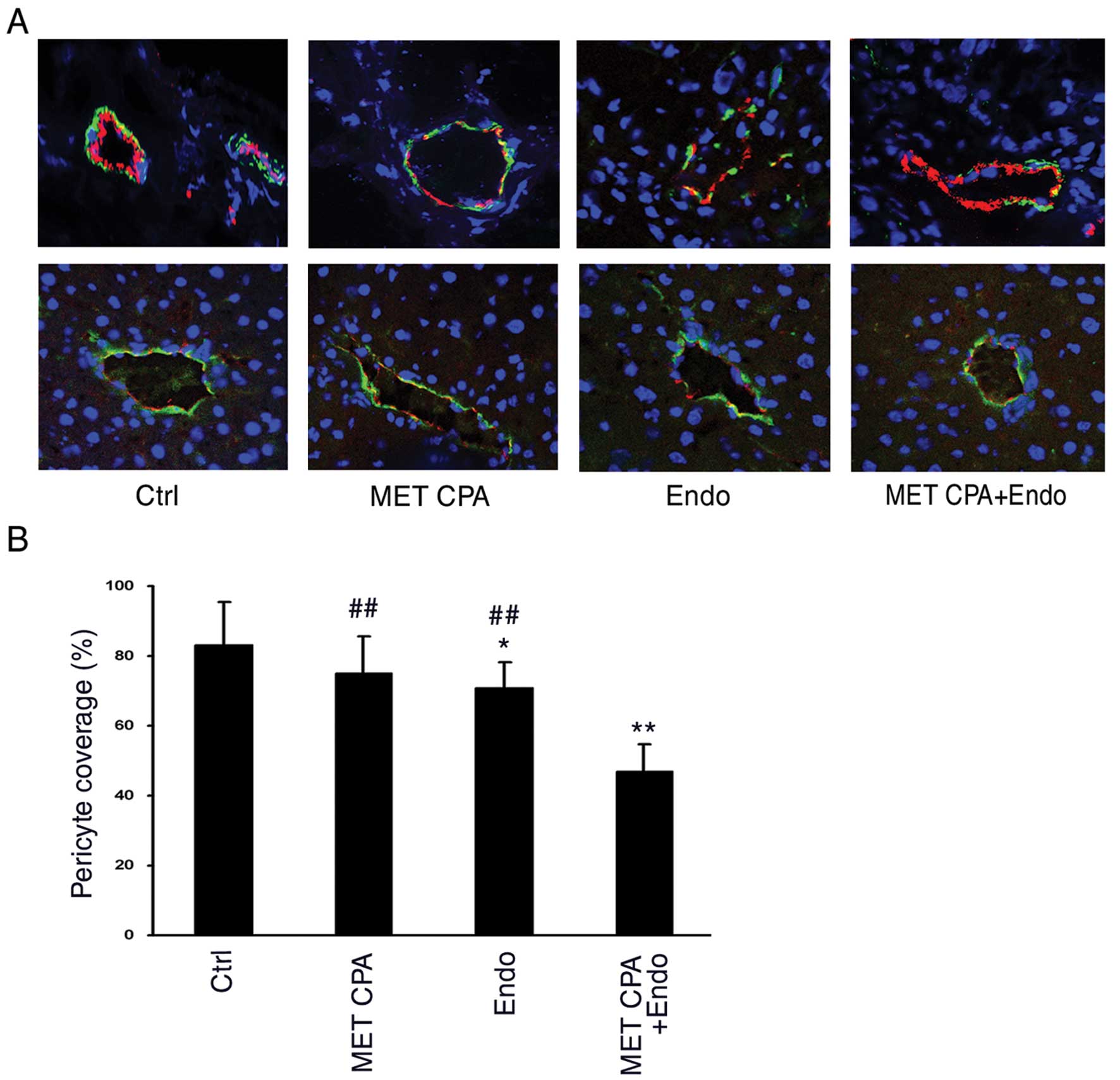
Given that pericytes can modulate multiple behaviors
of endothelial cells, we assessed pericyte coverage as a measure of
tumor angiogenesis by immunofluorescence staining of tumor tissue
sections with antibody against NG2, a specific marker of pericytes.
As illustrated in Fig. 4, the value
of pericyte coverage was 83.26±12.26% in the Ctrl group of mice,
similar to that detected in the MET CPA group of mice
(75.10±10.71%), indicating that treatment with MET CPA alone did
not dramatically alter pericyte coverage (P>0.05, Fig. 4A, upper panels and B). However, the
value of pericyte coverage in the Endo group of mice (71.16±7.31%)
was significantly less than that in the Ctrl group (P<0.05).
More interestingly, the value of pericyte coverage in the MET CPA +
Endo group of mice was further reduced to 46.77±7.66%, as compared
with that in other groups (P<0.01). In contrast, the
dissociation of pericytes from endothelial cells and the
differences in pericyte coverage from different treatments were not
detected in livers of mice (Fig.
4A, lower panels), suggesting that anti-angiogenic effect only
occurred in the tumor but not in normal tissue. These data further
indicate that MET CPA plus Endostar inhibits neoangiogenesis in the
tumors, which may contribute to the inhibition of tumor growth in
mice.
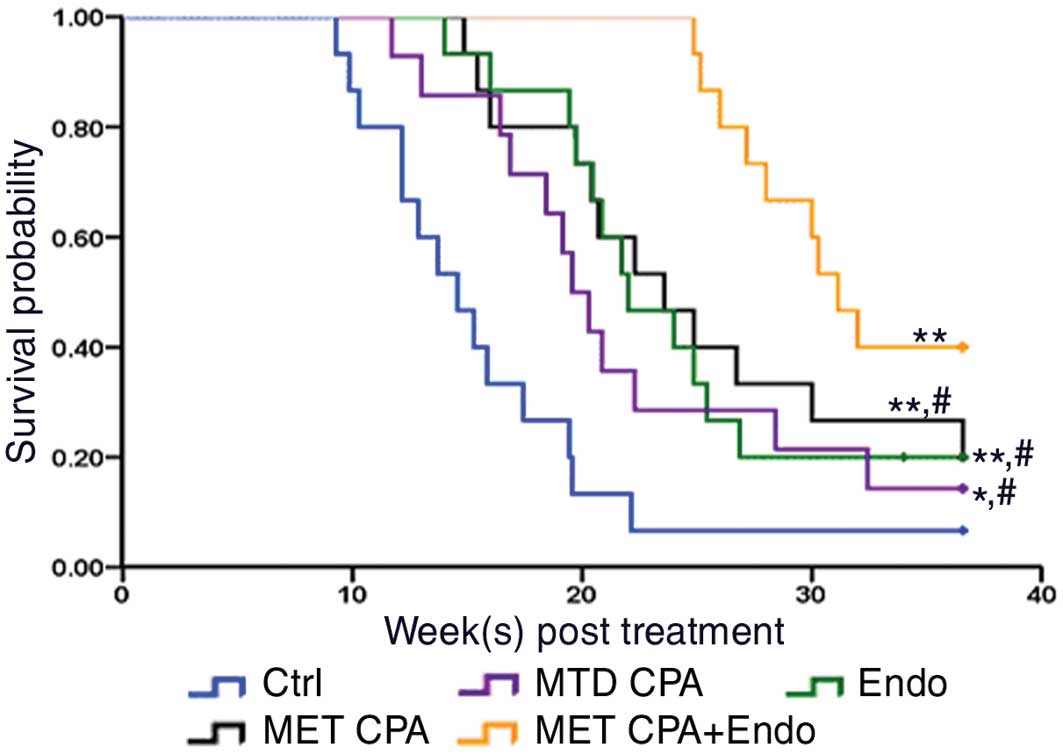
MET CPA combined with Endostar prolongs
survival of tumor-bearing mice
Finally, we examined the impact of different
treatments on survival of tumor-bearing mice. Consistent with the
alterations in tumor burden, mice in the Ctrl group survived a
shorter period with a median survival time of 14.57 weeks (Fig. 5). In contrast, mice in the MET CPA,
Endo, and MTD CPA groups survived significantly longer with a
median survival time of 23.57, 22.00 and 19.56 weeks, respectively
(P<0.05 vs. control group). More importantly, mice in the MET
CPA + Endo group survived much longer with a median time of 31.14
weeks (P<0.05 vs. other groups). These data clearly demonstrated
that MET CPA combined with Endostar further prolonged survival of
tumor-bearing mice.
Discussion
Here we report that the combination of MET CPA and
Endostar exhibits enhanced anti-tumor effects with respect to the
growth of xenograft tumors and survival of tumor-bearing mice.
Mechanistically, combined treatment further reduced the frequency
of total and viable peripheral blood CECs, the value of MVD, and
pericyte coverages in xenograft tumors derived from NSCLC. The
activities on tumor-associated angiogenesis may contribute to
anti-tumor effects as conferred by MET CPA combined with
Endostar.
Angiogenesis plays a critical role in continuous
tumor growth and tumor dissemination, involving in extensive
crosstalk among tumor cells, vascular endothelial cells, stromal
cells and pericytes (17). This
process is associated with the alterations on the cellular level
both locally within the tumor and systematically in the blood
circulation. It starts with pericyte-endothelial cell dissociation,
followed by proliferation and invasion of endothelial cells,
formation of endothelial tubulogenesis and vascular stabilization
(18). Consequently, an increased
MVD and pericyte coverage are often observed in tumors with a high
level of angiogenesis and correlated with unfavorable
clinicopathologic parameters (19).
Systemically, at least two distinct populations of CECs have been
identified: bone marrow-derived circulating endothelial progenitor
cells (CEPs,
CD45−CD146+CD34+CD133+),
and mature CECs
(CD45−CD146+CD34+CD133−)
(20). They constitute a rare
population of circulating blood cells under physiological
condition, but they dramatically increase in response to vascular
damage in pathological situations. The frequency of peripheral
blood CECs has been considered a useful surrogate marker for
angiogenesis in tumor progression (21,22).
Furthermore, growing evidence suggests that alterations in the
frequency of peripheral blood CECs and their viability are
correlated with the therapeutic responses to angiogenesis inhibitor
in cancer patients (23–25). Therefore, measurements of peripheral
blood CECs, together with MVD and pericyte coverage in the tumors,
are valuable for uncovering the role of anti-angiogenic drugs.
In the present study, we examined the impact of MET
CPA and/or Endostar on the peripheral blood CECs, MVD and pericyte
coverage in tumor-bearing mice. We found that in the control group,
peripheral CECs constituted ~0.50% of circulating blood cells,
nearly 70% of which were viable CECs, and concomitantly, higher
levels of MVD and pericyte coverage were detected in xenograft
tumors. In contrast, MET CPA or Endostar significantly reduced the
frequency of peripheral blood total and viable CECs and the value
of MVD; Endostar also considerably inhibited pericyte coverage in
xenograft tumors. More importantly, MET CPA combined with Endostar
further reduced the frequency of peripheral blood total and viable
CECs, the value of MVD, and pericyte coverage. These data indicate
that the combination of MET CAP with Endostar lead to more potent
inhibition of neoangiogenesis in the tumors, which may contribute
to the inhibition of tumor growth in mice. Interestingly, when we
examined pericyte coverage in liver tissues form tumor-bearing mice
we found that there was no significant difference in pericyte
coverage among the different treatment groups, suggesting that MET
CPA or Endostar predominantly affects angiogenesis in tumor
tissues. In addition, the levels of angiogenesis in xenograft
tumors appear to be negatively associated with the length of
survival periods in different groups of mice.
Notably, we found that treatment with MTD CPA
effectively inhibited the growth of xenograft tumors, but enhanced
peripheral blood CECs in mice, which is consistent with the role of
MTD cytotoxic chemotherapy in inducing endothelial damage (26). By contrast, when administered on a
metronomic schedule, CPA not only inhibited the growth of tumors,
but also reduced the frequency of peripheral blood CECs in mice,
with a further reduced level when combined with Endostar. The
increased level of CECs may contribute to the repair of damaged
vasculature after MTD chemotherapy and the decreased level of CECs
suppress the repair and recovery of tumor vasculature which is
indispensable to tumor growth and metastasis. As to the underlying
mechanism for the opposite effects of MTD CPA and MET CPA on CECs
level, a possible explanation is their inverse effects on the
mobilization and viability of CEPs. Mice treated with MTD CPA
experienced a robust CEPs mobilization a few days after the end of
drug administration, while the CEPs numbers and viability in mice
treated with MET CPA was sustained at a very low level for a much
prolonged period (13,14).
Endostar has been demonstrated to antagonize the
VEGF-mediated signaling in vascular endothelial cells (27), and in these cells, MET CPA markedly
increases the level of thrombospondin 1 (28), which is a well known endogenous
inhibitor of angiogenesis. The combination of Endostar and MET CPA
may inhibit the angiogenesis and growth of tumors. Indeed, in the
present study, the combination of MET CPA and Endostar resulted in
robust anti-tumor effects through enhanced inhibition of
tumor-associated angiogenesis. Our data are consistent with
findings from other studies (12,23),
and support the notion that MET chemotherapy combined with an
angiogenesis inhibitor is a better strategy for the treatment of
cancers (29). Conceivably, this
therapeutic strategy can be moved from bench to bedside,
particularly for a maintenance therapy after efficient first-line
chemotherapy on patients with advanced NSCLC, to achieve
sustainable tumor control and a longer progression-free survival
(30).
In conclusion, our results indicate that MET CPA
combined with Endostar results in enhanced anti-tumor and
anti-angiogenic effects in a xenograft model of human lung cancer.
These findings may aid in the design of clinical trials to
investigate the efficacy of metronomic chemotherapy combined with
an angiogenesis inhibitor for patients with advanced NSCLC, which
may serve as a promising treatment strategy.
Acknowledgements
We gratefully thank Boqing Li in the Department of
Anhui Key Laboratory of Infection and Immunity (Bengbu Medical
College) for his help in performing flow cytometry; and Jing Zhang
in the Department of Bioscience (Bengbu Medical College) for his
technical help in confocal microscopy.
References
|
1
|
Jemal A, Bray F, Center MM, Ferlay J, Ward
E and Forman D: Global cancer statistics. CA Cancer J Clin.
61:69–90. 2011. View Article : Google Scholar
|
|
2
|
Parkin DM, Bray F, Ferlay J and Pisani P:
Global cancer statistics, 2002. CA Cancer J Clin. 55:74–108. 2005.
View Article : Google Scholar
|
|
3
|
Goffin J, Lacchetti C, Ellis PM, Ung YC
and Evans WK: First-line systemic chemotherapy in the treatment of
advanced non-small cell lung cancer: a systematic review. J Thorac
Oncol. 5:260–274. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Felip E, Cedrés S, Checa E and Martinez P:
How to integrate current knowledge in selecting patients for first
line in NSCLC? Ann Oncol. 21(Suppl 7): 230–233. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Thatcher N and Heighway J: Maintenance and
consolidation therapy in patients with unresectable stage III/IV
non-small cell lung cancer. Oncologist. 15:1034–1042. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kerbel RS and Kamen BA: The
anti-angiogenic basis of metronomic chemotherapy. Nat Rev Cancer.
4:423–436. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pasquier E, Kavallaris M and Andre N:
Metronomic chemotherapy: new rationale for new directions. Nat Rev
Clin Oncol. 7:455–465. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Man S, Bocci G, Francia G, Green SK, Jothy
S, Hanahan D, Bohlen P, Hicklin DJ, Bergers G and Kerbel RS:
Antitumor effects in mice of low-dose (metronomic) cyclophosphamide
administered continuously through the drinking water. Cancer Res.
62:2731–2735. 2002.PubMed/NCBI
|
|
9
|
Kong DS, Lee JI, Kim WS, Son MJ, Lim do H,
Kim ST, Park K, Kim JH, Eoh W and Nam DH: A pilot study of
metronomic temozolomide treatment in patients with recurrent
temozolomide-refractory glioblastoma. Oncol Rep. 16:1117–1121.
2006.PubMed/NCBI
|
|
10
|
Song HF, Liu XW, Zhang HN, Zhu BZ, Yuan
SJ, Liu SY and Tang ZM: Pharmacokinetics of His-tag recombinant
human endostatin in Rhesus monkeys. Acta Pharmacol Sin. 26:124–128.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jia H and Kling J: China offers
alternative gateway for experimental drugs. Nat Biotechnol.
24:117–118. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Pietras K and Hanahan D: A multitargeted,
metronomic, and maximum-tolerated dose ‘chemo-switch’ regimen is
antiangiogenic, producing objective responses and survival benefit
in a mouse model of cancer. J Clin Oncol. 23:939–952. 2005.
|
|
13
|
Bertolini F, Paul S, Mancuso P,
Monestiroli S, Gobbi A, Shaked Y and Kerbel RS: Maximum tolerable
dose and low-dose metronomic chemotherapy have opposite effects on
the mobilization and viability of circulating endothelial
progenitor cells. Cancer Res. 63:4342–4346. 2003.PubMed/NCBI
|
|
14
|
Goon PK, Lip GY, Stonelake PS and Blann
AD: Circulating endothelial cells and circulating progenitor cells
in breast cancer: relationship to endothelial
damage/dysfunction/apoptosis, clinicopathologic factors, and the
Nottingham Prognostic Index. Neoplasia. 11:771–779. 2009.
|
|
15
|
Goon PK, Lip GY, Boos CJ, Stonelake PS and
Blann AD: Circulating endothelial cells, endothelial progenitor
cells, and endothelial microparticles in cancer. Neoplasia.
8:79–88. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Mancuso P, Calleri A, Cassi C, Gobbi A,
Capillo M, Pruneri G, Martinelli G and Bertolini F: Circulating
endothelial cells as a novel marker of angiogenesis. Adv Exp Med
Biol. 522:83–97. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Folkman J: Angiogenesis: an organizing
principle for drug discovery? Nat Rev Drug Discov. 6:273–286. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Raza A, Franklin MJ and Dudek AZ:
Pericytes and vessel maturation during tumor angiogenesis and
metastasis. Am J Hematol. 85:593–598. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Miyata Y, Kanda S, Ohba K, Nomata K,
Hayashida Y, Eguchi J, Hayashi T and Kanetake H: Lymphangiogenesis
and angiogenesis in bladder cancer: prognostic implications and
regulation by vascular endothelial growth factors-A, -C, and -D.
Clin Cancer Res. 12:800–806. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mariucci S, Rovati B, Bencardino K,
Manzoni M and Danova M: Flow cytometric detection of circulating
endothelial cells and endothelial progenitor cells in healthy
subjects. Int J Lab Hematol. 32:E40–E48. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Martin-Padura I and Bertolini F:
Circulating endothelial cells as biomarkers for angiogenesis in
tumor progression. Front Biosci (Schol Ed). 1:304–318. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Bertolini F, Shaked Y, Mancuso P and
Kerbel RS: The multifaceted circulating endothelial cell in cancer:
towards marker and target identification. Nat Rev Cancer.
6:835–845. 2006. View
Article : Google Scholar : PubMed/NCBI
|
|
23
|
Dellapasqua S, Bertolini F, Bagnardi V,
Campagnoli E, Scarano E, Torrisi R, Shaked Y, Mancuso P, Goldhirsch
A, Rocca A, Pietri E and Colleoni M: Metronomic cyclophosphamide
and capecitabine combined with bevacizumab in advanced breast
cancer. J Clin Oncol. 26:4899–4905. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Furstenberger G, von Moos R, Lucas R,
Thurlimann B, Senn HJ, Hamacher J and Boneberg EM: Circulating
endothelial cells and angiogenic serum factors during neoadjuvant
chemotherapy of primary breast cancer. Br J Cancer. 94:524–531.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Zhang H, Vakil V, Braunstein M, Smith EL,
Maroney J, Chen L, Dai K, Berenson JR, Hussain MM, Klueppelberg U,
Norin AJ, Akman HO, Ozçelik T and Batuman OA: Circulating
endothelial progenitor cells in multiple myeloma: implications and
significance. Blood. 105:3286–3294. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Laquente B, Vinals F and Germa JR:
Metronomic chemotherapy: an antiangiogenic scheduling. Clin Transl
Oncol. 9:93–98. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ling Y, Yang Y, Lu N, You QD, Wang S, Gao
Y, Chen Y and Guo QL: Endostar, a novel recombinant human
endostatin, exerts antiangiogenic effect via blocking VEGF-induced
tyrosine phosphorylation of KDR/Flk-1 of endothelial cells. Biochem
Biophys Res Commun. 361:79–84. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Bocci G, Francia G, Man S, Lawler J and
Kerbel RS: Thrombospondin 1, a mediator of the antiangiogenic
effects of low-dose metronomic chemotherapy. Proc Natl Acad Sci
USA. 100:12917–12922. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Murray A, Little SJ, Stanley P, Maraveyas
A and Cawkwell L: Sorafenib enhances the in vitro anti-endothelial
effects of low dose (metronomic) chemotherapy. Oncol Rep.
24:1049–1058. 2010.PubMed/NCBI
|
|
30
|
Fidias P and Novello S: Strategies for
prolonged therapy in patients with advanced non-small-cell lung
cancer. J Clin Oncol. 28:5116–5123. 2010. View Article : Google Scholar : PubMed/NCBI
|