Introduction
Epithelial ovarian cancer (EOC) is the deadliest
gynecological malignancy since approximately 75% of ovarian cancer
cases present at an advanced stage when the disease has spread well
beyond the ovaries and the cancer involves the peritoneal cavity or
other organs (1). The cancer is
insidious; frequently initial symptoms occur only during the
advanced stage of the disease and are often related to the presence
of a grossly enlarged tumor and extensive ascites fluid (2).
According to a report of the American Joint
Committee on Cancer (AJCC), patients with stage III and IV EOC have
5-year relative survival rates of 33.5 and 17.9%. In contrast,
patients with stage I and II disease have 5-year relative survival
rates of 89.3 and 65.5%, respectively (3).
This disparity in survival between early and late
stage disease emphasizes the need to improve early detection and
diagnosis of EOC. Effective screening protocols are not currently
available, and risk assessment for the presence of EOC in women
with an ovarian cyst needs improvement.
The role of tumor biomarkers in the diagnosis and
follow-up of ovarian carcinoma is a controversial issue. During the
last several decades, several tumor markers have been detected in
the blood of patients with EOC, yet their sensitivities and
specificities for predicting this form of cancer appear no better
than those of mucin CA-125 alone (4,5).
The cancer antigen-125 (CA-125) is a glycoprotein
belonging to the family of mucins encoded by the gene MUC16. The
increased expression of this molecule is often associated with
benign gynecological pathologies, and with non-gynecological
conditions such as chronic liver disease, pancreatitis, kidney
disease and chronic inflammatory diseases (5,6).
Because of the poor sensitivity and specificity of CA-125, in
recent years, research has focused on the identification of new
biomarkers that can provide higher sensitivities and specificities.
Human epididymis protein 4 (HE4) has been recently accepted by the
US Food and Drug Administration (FDA) as a monitoring marker for
the management of patients with EOC. This new molecule, encoded by
the gene WFDC2, is a glycoprotein of 20–25 kDa initially identified
in the epithelium of the distal epididymis as a human protease
inhibitor. Moreover, it was found to be involved in the maturation
of sperm (7).
Several studies have demonstrated that HE4 is
increased in EOC but not in ovarian tissue under normal conditions
(8,9). Recently, it has been proposed that the
combined use of novel biomarkers such as HE4 and CA-125 improves
the sensitivity and specificity when compared with either biomarker
alone for the diagnosis and management of EOC (10–12).
Although several studies have focused on markers to facilitate the
early diagnosis of disease; it is just as important to identify
markers able to predict disease remission, response to therapy and,
in particular, early detection of disease relapse.
Recurrent EOC, unlike other solid tumors, tends to
present without accompanying symptoms and forms multiple small
implantations, particularly in the small intestine and mesentery,
which cannot be readily detected using conventional imaging
techniques (13,14).
Computed tomography (CT) has low sensitivity for
detecting disease recurrence, probably due to its inability to
detect small peritoneal implants and normal-sized lymph node
metastases (15,16). Moreover a number of patients with
disease relapse can present with normal CA-125 levels (15,17).
In the present study, we retrospectively
investigated the expression of two markers, CA-125 and HE4, as
indicators of relapse in EOC patients with recurrent disease in
combination with contrast-enhanced high-resolution multidetector
row computed tomography (CE CT) findings. Moreover, to improve the
management of these patients we evaluated a possible correlation
between HE4 levels and CE CT imaging results.
Materials and methods
Patients
All subjects included in the follow-up study were
patients referred to the Oncologic Unit A, of the Policlinico
Umberto I, Rome, Italy, from January 2009 to December 2011. Of the
total 21 women, 18 were in a postmenopausal state (age range 50–85
years, mean age 65.72±2.32) and 3 patients were in a premenopausal
state (age range 43–47; mean age 44.73±1.20). All patients had
advanced EOC (FIGO III/IV), and underwent surgery and adjuvant
chemotherapy, and were retrospectively selected for the assessment
of HE4 and CA-125 levels. Sixteen out of the 21 (76%) women were
affected by papillary serous carcinoma and 5 out of 21 (24%) were
affected by papillary serous carcinoma ‘poorly’ differentiated and
undifferentiated of grade G3/4. Each patient contributed 3 serum
samples drawn at 3-month intervals as follows: time interval I (1–3
months from surgery), time interval II (4–6 months from surgery),
time interval III (7–10 months from surgery).
Inclusion criteria for enrollment included that: all
patients had to show clinical remission after surgery and undergo
adjuvant chemotherapy. Nine out of the 21 women showed disease
relapse during the follow-up study (Group A), 12 out of 21 women
had stable disease during the follow-up study (Group B).
A written informed consent was obtained from all of
the patients prior to the collection of blood samples.
Sample collection
Serum samples were collected in a red-top vacutainer
following a standard protocol. Samples were clotted for 60–90 min,
and centrifuged for 10 min at 1,300 × g. The serum fractions were
aliquoted and stored at −80°C until analysis.
Measurements of the biomarkers
HE4
HE4 levels were determined using the HE4 EIA assay
(Fujirebio Diagnostics). The HE4 EIA is a solid phase,
non-competitive immunoassay based upon the direct ‘sandwich’
technique using 2 monoclonal antibodies, 2H5 and 3D8, directed
against 2 epitopes in the C-WFDC domain of HE4. Standard and
control/patient serum samples were incubated with biotinylated
anti-HE4 monoclonal antibody 2H5 aliquots in streptavidin-coated
microstrips. HE4 in standard or serum samples was adsorbed in the
streptavidin-coated microstrips by the biotinylated anti-HE4
monoclonal antibody during the incubation period. The strips were
then washed and incubated with HRP-labeled anti-HE4 monoclonal
antibody 3D8. After washing, buffered substrate/chromogen reagent
was added to each strip, and the enzyme reaction was able to
proceed. During the enzyme reaction, a blue color developed when
the antigen was present. The intensity of the color was directly
proportional to the amount of HE4 present in the samples. According
to the manufacturer’s indications, normal values of HE4 were
considered to be <150 pmol/l.
CA-125
CA-125 levels were evaluated by a one-step
‘sandwich’ radioimmunoassay (Radim, The Netherlands). Polystyrene
beads coated with the M11 capture antibody reacting with molecules
containing OC 125 reactive determinants were incubated with the
control or patient serum samples, standards, and tracer
(125I-labeled mouse monoclonal OC 125 antibody)
aliquots. The bound radioactivity observed was proportional to the
concentration of the OC 125 reactive determinant (antigen). Normal
levels of CA-125 were considered to be <35 U/ml.
Imaging
During the study period, 20 out of 21 patients
underwent at least two CE CT follow-ups with an time interval of ~6
months. For 2 out of 21 cases, a third CE CT was performed within 3
months from the previous one, due to a worsening in the patient
clinical conditions. The second CE CT generally was carried out
within the time interval II of the serum sampling. In 1 patient
(Group A) a second CE CT was not performed.
Contrast-enhanced high-resolution multidetector row
computed tomography (Somatom Sensation 64; Siemens Medical System,
Erlangen, Germany) was used to evaluate peritoneal carcinomatosis.
The parameters applied were as follows: 0.6×64 mm2
collimation, 3-mm section thickness, 250 effective mAs, 120 kVp and
0.8–1.5 mm reconstruction interval of coronal and sagittal images.
The CT scans were acquired in basal conditions and after
administration of contrast medium, cranio-caudally, from the dome
of the diaphragm to the pelvis. The images were post-processed
[multiplanar reconstruction (MPR) and maximum intensity projection
(MIP)] with reconstructions in sagittal and coronal plane sections
with a 1-mm interval to improve the anatomical analysis,
particularly of the surface lesions.
An intravenous injection of 20 mg of
butyl-scopolamine (Buscopan; Boehringer) was administered to all
patients to relax the bowel wall and reduce peristalsic bowel
movement before CT examinations. The patients were asked to ingest
1 liter of water in order to achieve optimal distension of the
stomach and of the bowel.
A dual phase protocol, arterial and venous phase,
after intravenous administration of contrast medium, was performed
in order to assess local tumor extent. Nonionic iodinated contrast
medium (350 mg I/ml Iomeron; Bracco, Milan, Italy) was administered
intravenously utilizing an automatic injector (Stellant DCT;
Medrad, Warrendale, PA, USA) at a rate of infusion of 3–3.5 ml/sec
for a total volume of 90–120 ml.
Parameters of tumor extension, i.e. peritoneal
carcinomatosis and lymph node dissemination, were evaluated
according to an arbitrary scoring classification as follows.
Peritoneal carcinomatosis: score 0, undetectable carcinomatosis;
score 1, single or multiple sites of micro-nodular implants (<1
cm) above or below the mesocolon; score 2, diffuse macro-nodular
implants (>1.5 cm) on the bowel surface or mesenterial implants,
and omental involvement with marked thickening (omental cake).
Lymph node dissemination: L0, lymph nodes 0.5–1 cm diameter; L1,
lymph nodes 1–1.5 cm; L2, lymph nodes 1.5–2.5 cm; L3, clusters of
lymph nodes >2.5 cm diameter.
Finally, we compared the two CE CT performed during
the study period for each patient in order to determine disease
progression, remission or stable disease.
Progression of disease was diagnosed when the
comparison between the two CE CT showed an increase in the score
(carcinomatosis and/or lymph node) or an increase in the size
and/or number by >20% of at least 3 implants of carcinomatosis
defined as target lesions.
Remission of disease was considered when there was
either a decrease in the score (carcinomatosis and/or lymph node),
or a decrease in the size and/or number by 30% of the target
lesions.
Stability was indicated when the disease did not
follow any of the parameters described above.
Statistical analysis
For each patient, the mean age ± SEM and the median
(range) of serum HE4 and CA-125 levels were determined. Box plots
were generated for each marker in Group A and B patients.
Statistically significant differences were assessed by the
nonparametric Mann-Whitney test for categorical variables using
MedCalc® v12.3.0 software. The level of statistical
significance was set at p<0.05.
Results
Biomarkers in the follow-up study
The concentrations of HE4 and CA-125, expressed as
median and range, measured in Group A and B within time intervals
I, II and III, are provided in Table
I.
 | Table ILevels of HE4 and CA-125 determined in
patients with disease relapse (Group A) and stable disease (Group
B) within 3 time ranges. |
Table I
Levels of HE4 and CA-125 determined in
patients with disease relapse (Group A) and stable disease (Group
B) within 3 time ranges.
| Group A (n=9), median
(range) | Group B (n=12),
median (range) |
|---|
|
|
|
|---|
| HE4 (pmol/l) | CA-125 (U/ml) | HE4 (pmol/l) | CA-125 (U/ml) |
|---|
| Time interval I | 120 (90–160)a | 15 (10–30) | 55.5 (40–135)a | 13 (8–56) |
| Time interval II | 165 (97–241)b | 20 (11–30)d | 63 (30–132)b | 11.5 (8–86)d |
| Time interval
III | 300 (137–806)c | 34 (12–170)e | 55 (30–126)c | 12 (8–170)e |
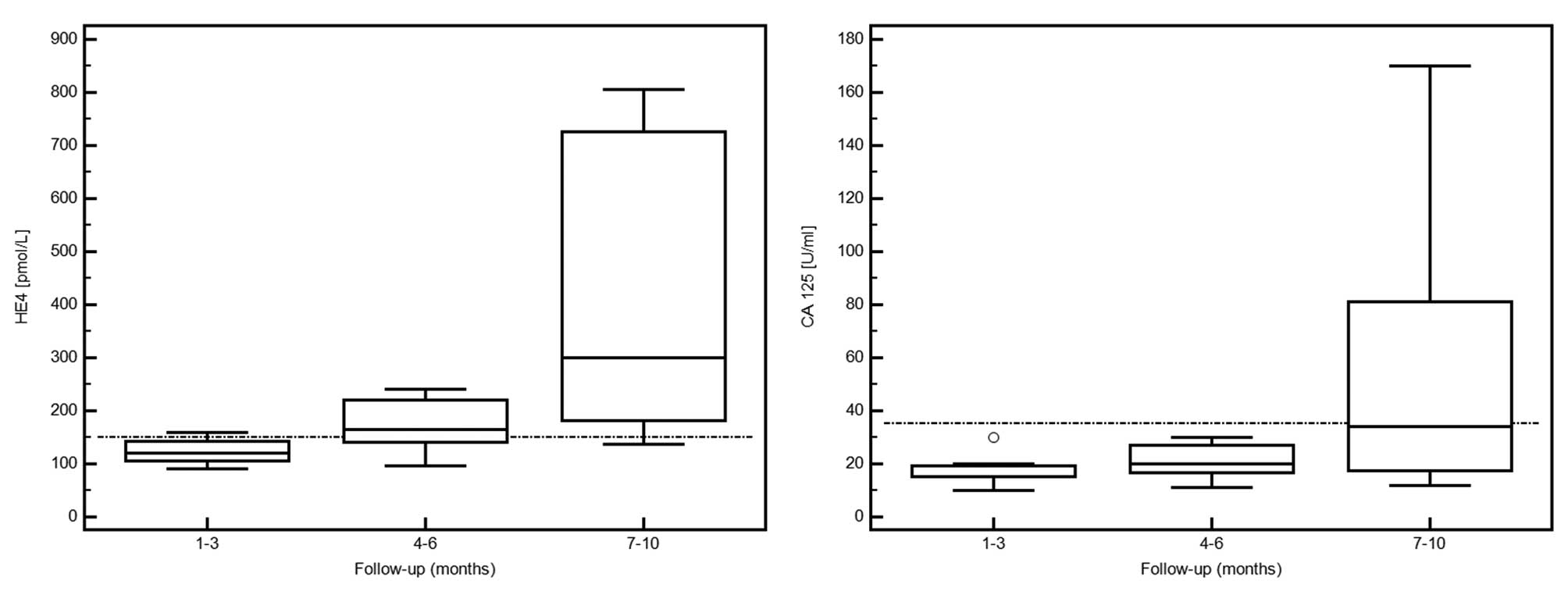
Group A
In the 9 patients who showed disease recurrence,
during the follow-up study, absolute concentrations of HE4 above
the threshold of positivity (150 pmol/l) were noted in 22, 78 and
89% of patients within time intervals I, II and III following
surgery, respectively.
We also observed that the serum levels of CA-125
were consistently below the threshold value (35 U/ml) during time
intervals I and II, while only 44% of patients had positive
absolute concentrations of the marker in the time interval III
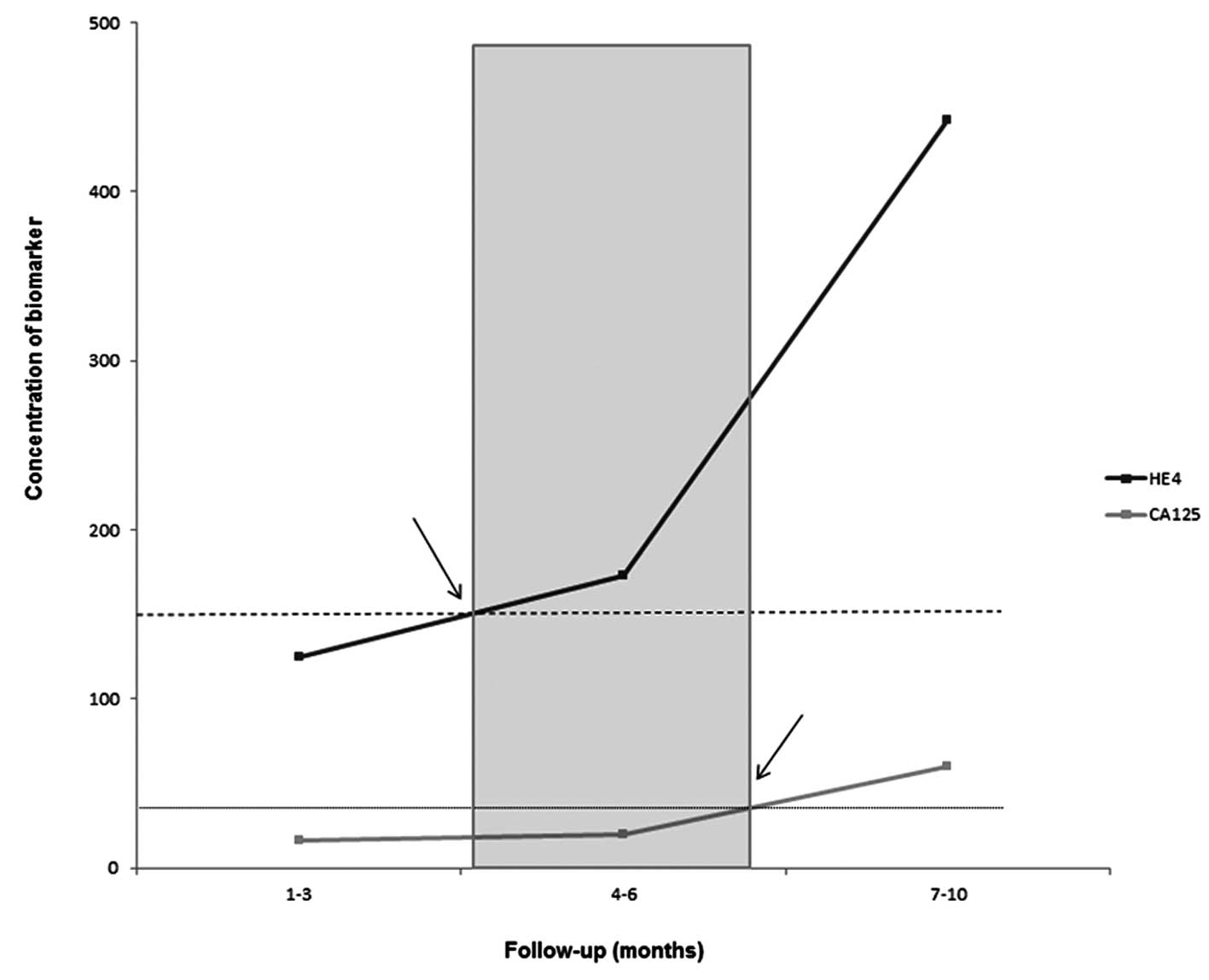
(Fig. 1). In these patients, the
increase in HE4 level above the cut-off preceded the rise of CA-125
~3 months. Furthermore, in the last time window, the mean increase
of HE4 was ~3-times the cut-off while the mean increase in CA-125
was ~1.5-times the value of positivity (Fig. 2).
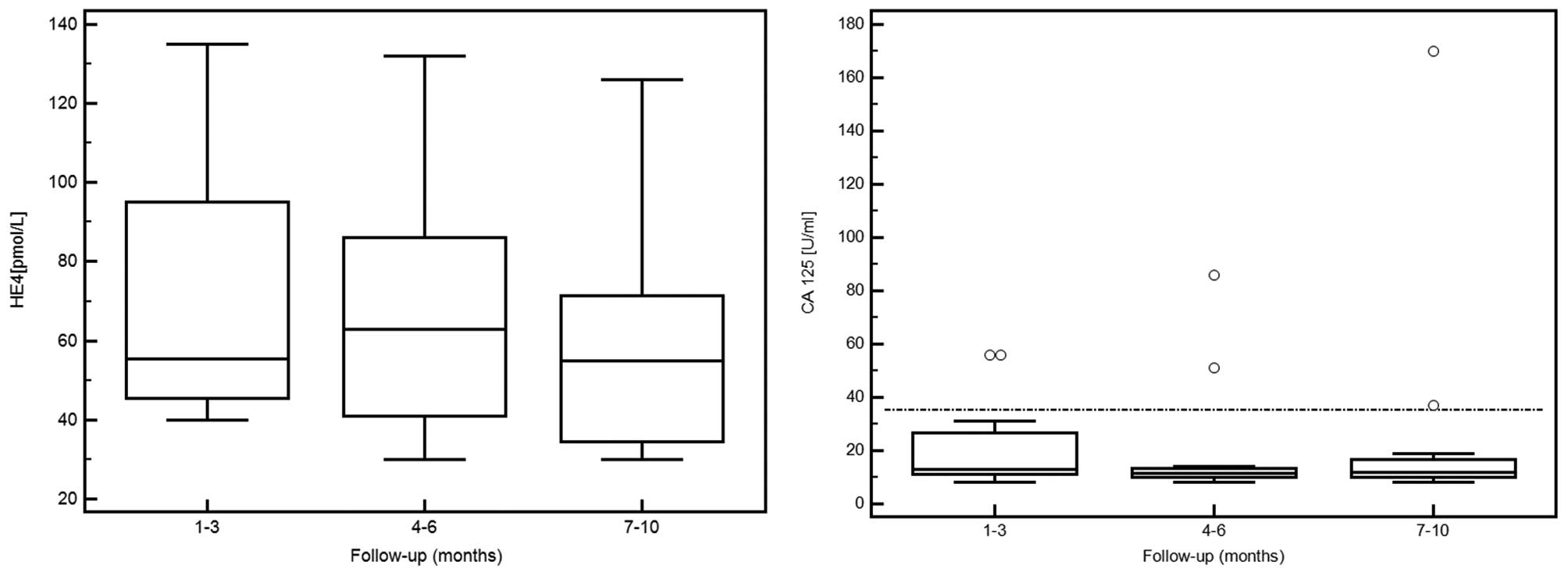
Group B
In the 12 patients who had stable disease, the HE4
concentrations were within the range of normality for all
determinations, while for CA-125, 6 positive values were present in
4 different patients (Fig. 3).
The median serum levels of HE4, drawn at 3-month
intervals, were significantly higher in Group A when compared with
values in Group B patients (time interval I: 120 vs. 55.5 pmol/l
p<0.002; time interval II: 165 vs. 63 pmol/l, p<0.0004; time
interval III: 300 vs. 55 pmol/l, p<0.0001). The median serum
levels of CA-125 measured between the 2 groups of women, were
statistically different only during time intervals II and III (20
vs. 11.5 U/ml, p<0.02 and 34 vs. 12 U/ml, p<0.02,
respectively).
Imaging in the follow-up study
Group A
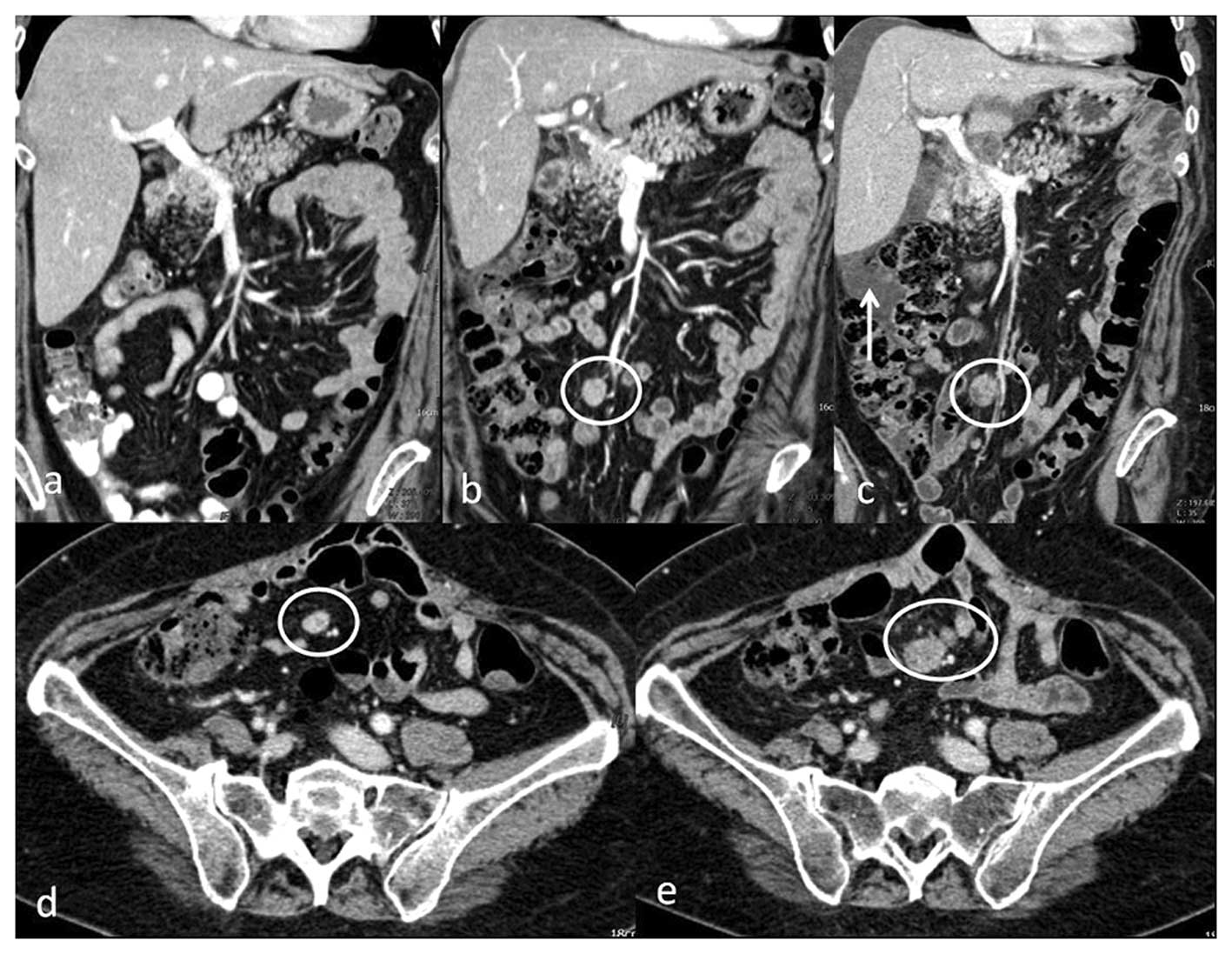
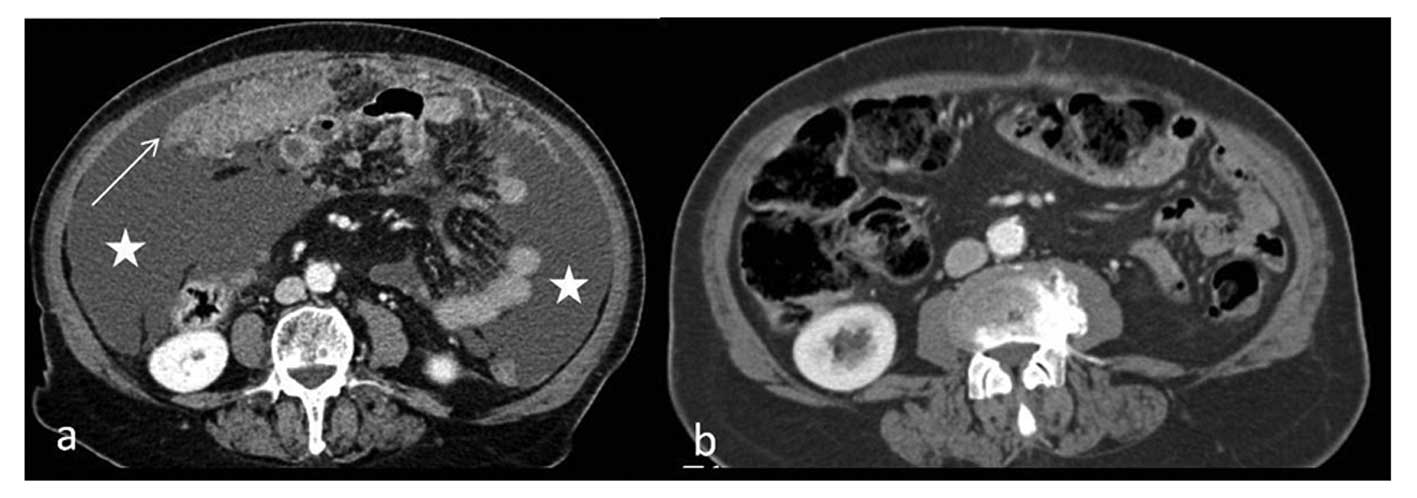
In 1 out of 9 patients in Group A, the first CT
showed no visible carcinomatosis (score 0) the second CE CT showed
the presence of multiple implants smaller than 1.5 mm (score 1).
Moreover, a worsening of clinical condition justified a third
examination (3 months after the second CT) which showed severe
progression of disease (score 2, lymph nodes 3) with associated
ascites (Fig. 4).
Six out of the 9 patients in Group A had an initial
condition (first CT) of score 1 and lymph nodes 1 or 2. In 5 out of
6 of these cases the second CE CT showed progressive disease with
an increased score both for carcinomatosis and lymph nodal disease.
The remaining case had stable disease at the second CE CT, while a
third examination was performed after a worsening condition, and
the CE CT determined disease progression as well.
Finally only 1 out of 9 patients, showed an initial
condition of score 2 and L2, which was determined to be L3 disease
at the second CE CT with increased size and number of
carcinomatosis implants.
Group B
In 10 out of 12 cases, the first CE CT showed no
visible carcinomatosis implants (score 0), and there was no image
worsening at the second CE CT during the follow-up.
In 2 out of 12 patients in Group B, the first CE CT
showed an initial condition of score 1 and lymph nodes 1; the
second CE CT showed a decrease in carcinomatosis implants which
were no longer visible (score 0) (Fig.
5).
Imaging and biomarkers
The evaluation of the imaging findings within time
interval II, which generally corresponded to the time of the second
CE CT, showed that Group A women presented with peritoneal
carcinomatosis and lymph node dissemination with various degrees of
disease progression. In particular, 6 out of 9 patients showed
elevated HE4 levels corresponding with widespread macro-nodular
implants (>1.5 cm) on the bowel or mesenterial surface (score 2)
and lymph nodal disease L2/L3.
The HE4 results of the Group B women were in
agreement with undetectable carcinomatosis (score 0), small lymph
node size without radiological significance (L1/L0). Furthermore,
CA-125 levels did not correlate with the different degrees of
carcinomatosis in both Group A and B.
Discussion
New and innovative approaches are needed for the
early detection of disease relapse in women affected by epithelial
ovarian cancer (EOC). Regardless of the development of new
treatments and therapies designed to improve the 5-year survival
rate, ovarian cancer still remains the deadliest type of cancer of
the female reproductive tract.
Biomarkers have great potential to serve as an
efficient screening tool for the early detection of ovarian cancer
(1). CA-125 is still the only tumor
marker recommended as a diagnostic or prognostic indicator and for
the monitoring of disease recurrence after surgery and adjuvant
chemotherapy (18–20). The major drawback of CA-125 is the
documented lack of specificity, as this marker may show levels
exceeding the 95th percentile of normal values in a significant
proportion of women with benign or malignant diseases (21). Accordingly, there have been many
efforts to improve the diagnostic performance of CA-125. Among
these, relevance has recently been given to HE4 which is one of the
most promising markers with improved sensitivity and specificity.
Moreover, for clinical management of patients affected by EOC, it
is of paramount importance to identify markers able to predict
early relapse of clinical disease during follow-up.
Numerous studies have shown that HE4 is able to
anticipate the relapse of disease compared to CA-125 (11,22).
Based on these data we conducted a retrospective follow-up study of
10 months. We enrolled 21 patients diagnosed with ovarian cancer
stages FIGO III/IV, who underwent medical or surgical treatment. Of
great importance from the clinical point of view, are the results
obtained in 9 out of 21 patients who exhibited disease recurrence
during the study period. In particular, during time interval II
(4–6 months following surgery) 78% of the patients had positive
values for HE4 while, at the same time, none showed alteration in
serum CA-125. It is important to note that the positivity for
CA-125 shown in 44% of patients occurred only during the last time
window of our study (7–10 months). Therefore, we conclude that, in
case of disease recurrence, increased levels of HE4 may precede an
elevation in CA-125 by ~3 months.
Our results are in agreement with literature data
which suggest that the biomarker CA-125 cannot reliably detect
small tumor masses <8 cm3(23). Thus, CA-125 is not suitable as an
indicator for the presence of microscopic minimal residual disease
following radical surgery and/or chemotherapy (24).
Furthermore, a randomized (EORTC 55955) trial showed
that there is no survival benefit for early treatment based on
increased CA-125 levels alone (25,26).
This may agree with the evidence suggesting that this marker is
increased when the disease is already widespread.
In the present study, we used CE CT to assess the
recurrence of disease, and correlated the findings with tumor
progression or stable disease with serum levels of the
biomarkers.
In the last decade, several studies have
demonstrated the important role of CE CT as an investigation of
choice in both pre-operative staging and follow-up (27), due to the short time taken, the good
cost-effective ratio and the widespread availability of the
technique.
It is widely accepted that, in preoperative staging,
CE CT allows confirmation of the presence of a malignant adnexal
mass, as well as allows the determination of the extent of the
disease. Both features are crucial for treatment planning.
Moreover, CE CT has proven to be useful for assessment of the
treatment response, and to diagnose disease recurrence. In this
regard CE CT was demonstrated to have a sensitivity of 85–95% in
the detection of disease recurrence (28).
However, it is necessary to specify that several
studies are currently comparing the use of CE CT and PET/CT as
surveillance tools for recurrent disease. In fact, the main
limitation of CE CT is the reduced sensitivity (~50%) for the
detection of peritoneal implants <10 mm (28), or for the differentiation of these
from fibrous residual after treatment. However, there are no
reliable data which favor PET/CT rather than CE CT and vice versa
(29).
In light of these data, it is necessary to combine
imaging data with clinical data, such as serial measurements of
tumor biomarkers for an early detection of recurrent disease. In
the present study, regarding disease recurrence or stable disease,
CE CT findings correlated with the serum level of HE4. In
particular, evaluation of the imaging results during time interval
II (4–6 months following surgery) showed a significant correlation
with high levels of HE4 in 6 out of 9 patients with recurrent
disease. Moreover the HE4 results of the women with stable disease
correlated with undetectable carcinomatosis (score 0) and with
small lymph node size without radiological significance
(L1/L0).
These data indicate that HE4 is superior to CA-125
for estimating the extent of peritoneal carcinomatosis and that it
correlates with tumor burden in all surgically treated patients
(30–32).
In conclusion, this follow-up study supports the
hypothesis that HE4 may be an early biomarker for the recurrence of
EOC and that the HE4 serum levels, combined with CE CT imaging,
could improve the monitoring management of women affected by this
tumor. However, it could have enormous benefits on patient life. In
fact, this may justify the use of this marker for a strict
follow-up rather than excessive use of CE CT imaging, which may be
needed in case of a positive value, considering the side-effects
due to ionizing radiation and injection of contrast medium
associated with this technique. It is obvious that our findings
warrant further validation.
Acknowledgements
The authors are thankful to Giuseppina Gennarini,
Barbara Colaprisca and Silvestra Tudini for their excellent
technical assistance.
References
|
1
|
Kobayashi E, Ueda Y, Matsuzaki S, Yokoyama
T, Kimura T, Yoshino K, Fujita M, Kimura T and Enomoto T:
Biomarkers for screening, diagnosis, and monitoring of ovarian
cancer. Cancer Epidemiol Biomarkers Prev. 21:1902–1912. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Berek JS, Crum C and Friedlander M: Cancer
of the ovary, fallopian tube, and peritoneum. Int J Gynaecol
Obstet. 119(Suppl 2): S118–S129. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Husseinzadeh N: Status of tumor markers in
epithelial ovarian cancer has there been any progress? A review
Gynecol Oncol. 120:152–157. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Rosen DG, Wang L, Atkinson JN, Yu Y, Lu
KH, Diamandis EP, Hellstrom I, Mok SC, Liu J and Bast RC Jr:
Potential markers that complement expression of CA125 in epithelial
ovarian cancer. Gynecol Oncol. 99:267–277. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Bast RC Jr, Badgwell D, Lu Z, et al: New
tumor markers: CA125 and beyond. Int J Gynecol Cancer. 15(Suppl 3):
274–281. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Medeiros LR, Rosa DD, da Rosa MI, et al:
Accuracy of CA 125 in the diagnosis of ovarian tumors: a
quantitative systematic review. Eur J Obstet Gynecol Reprod Biol.
142:99–105. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kirchhoff C: Molecular characterization of
epididymal proteins. Rev Reprod. 3:86–95. 1998. View Article : Google Scholar
|
|
8
|
Galgano MT, Hampton GM and Frierson HF Jr:
Comprehensive analysis of HE4 expression in normal and malignant
human tissues. Mod Pathol. 19:847–853. 2006.PubMed/NCBI
|
|
9
|
Hellström I, Raycraft J, Hayden-Ledbetter
M, et al: The HE4 (WFDC2) protein is a biomarker for ovarian
carcinoma. Cancer Res. 63:3695–3700. 2003.PubMed/NCBI
|
|
10
|
Li J, Dowdy S, Tipton T, Podratz K, Lu WG,
Xie X and Jiang SW: HE4 as a biomarker for ovarian and endometrial
cancer management. Expert Rev Mol Diagn. 9:555–566. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Anastasi E, Marchei GG, Viggiani V, et al:
HE4: a new potential early biomarker for the recurrence of ovarian
cancer. Tumour Biol. 31:113–119. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Moore RG and Maclaughlan S: Current
clinical use of biomarkers for epithelial ovarian cancer. Curr Opin
Oncol. 22:492–497. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Tempany CM, Zou KH, Silverman SG, Brown
DL, Kurtz AB and McNeil BJ: Staging of advanced ovarian cancer:
comparison of imaging modalities - report from the Radiological
Diagnostic Oncology Group. Radiology. 215:761–767. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Gronlund B, Høgdall C, Hilden J, Engelholm
SA, Høgdall EV and Hansen HH: Should CA-125 response criteria be
preferred to Response Evaluation Criteria In Solid Tumors (RECIST)
for prognostication during second-line chemotherapy of ovarian
carcinoma? J Clin Oncol. 22:4051–4058. 2004. View Article : Google Scholar
|
|
15
|
Gu P, Pan LL, Wu SQ, et al: CA 125, PET
alone, PET-CT, CT and MRI in diagnosing recurrent ovarian
carcinoma: a systematic review and meta-analysis. Eur J Radiol.
71:164–174. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Togashi K: Ovarian cancer: the clinical
role of US, CT, and MRI. Eur Radiol. 13(Suppl 4): L87–L104. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Goonewardene TI, Hall MR and Rustin GJ:
Management of asymptomatic patients on follow-up for ovarian cancer
with rising CA-125 concentrations. Lancet Oncol. 8:813–821. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Aebi S and Castiglione M; ESMO Guidelines
Working Group. Newly and relapsed epithelial ovarian carcinoma:
ESMO clinical recommendations for diagnosis, treatment and
follow-up. Ann Oncol. 20(Suppl 4): 21–23. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Sturgeon CM, Duffy MJ, Stenman U-H, et al:
National Academy of Clinical Biochemistry laboratory medicine
practice guidelines for use of tumor markers in testicular,
prostate, colorectal, breast, and ovarian cancers. Clin Chem.
54:e11–e79. 2008. View Article : Google Scholar
|
|
20
|
Bast RC Jr: Status of tumor markers in
ovarian cancer screening. J Clin Oncol. 21(Suppl 10): s200–s205.
2003. View Article : Google Scholar
|
|
21
|
Moore RG, Jaube-Raughley M, Brown AK, et
al: Comparison of a novel multiple marker assay vs. the Risk of
Malignancy Index for the prediction of epithelial ovarian cancer in
patients with a pelvic mass. Am J Obstet Gynecol. 203:e1–e6. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Schummer M, Drescher C, Forrest R, Gough
S, Thorpe J, Hellström I, Hellström KE and Urban N: Evaluation of
ovarian cancer remission markers HE4, MMP7 and Mesothelin by
comparison to the established marker CA125. Gynecol Oncol.
125:65–69. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hori SS and Gambhir SS: Mathematical model
identifies blood biomarker-based early cancer detection strategies
and limitations. Sci Transl Med. 3:109ra1162011.PubMed/NCBI
|
|
24
|
Häfner N, Nicolaus K, Weiss S, Frey M,
Diebolder H, Rengsberger M, Dürst M and Runnebaum IB:
p53-autoantibody may be more sensitive than CA-125 in monitoring
microscopic and macroscopic residual disease after primary therapy
for epithelial ovarian cancer. J Cancer Res Clin Oncol.
139:1207–1210. 2013.PubMed/NCBI
|
|
25
|
Rustin GJ: Follow-up with CA125 after
primary therapy of advanced ovarian cancer has major implications
for treatment outcome and trial performances and should not be
routinely performed. Ann Oncol. 22(Suppl 8): viii45–iii48. 2011.
View Article : Google Scholar
|
|
26
|
Rustin GJ, van der Burg ME, Griffin CL, et
al: Early versus delayed treatment of relapsed ovarian cancer (MRC
OV05/EORTC 55955): a randomised trial. Lancet. 376:1155–1163. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Forstner R, Sala E, Kinkel K and Spencer
JA; European Society of Urogenital Radiology. ESUR guidelines:
ovarian cancer staging and follow-up. Eur Radiol. 20:2773–2780.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Coakley FV, Choi PH, Gougoutas CA, Pothuri
B, Venkatraman E, Chi D, Bergman A and Hricak H: Peritoneal
metastases: detection with spiral CT in patients with ovarian
cancer. Radiology. 223:495–499. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sala E, Kataoka M, Pandit-Taskar N, Ishill
N, Mironov S, Moskowitz CS, Mironov O, Collins MA, Chi DS, Larson S
and Hricak H: Recurrent ovarian cancer: use of contrast-enhanced CT
and PET/CT to accurately localize tumor recurrence and to predict
patients’ survival. Radiology. 257:125–134. 2010.PubMed/NCBI
|
|
30
|
Diniz Bizzo SM, Meira DD, Lima JM, da
Mororó JS, Casali-da-Rocha JC and Ornellas MH: Peritoneal VEGF
burden as a predictor of cytoreductive surgery outcome in women
with epithelial ovarian cancer. Int J Gynaecol Obstet. 109:113–117.
2010.PubMed/NCBI
|
|
31
|
Kang S: The role of neoadjuvant
chemotherapy in ovarian cancer patients with extensive tumor
burden. J Gynecol Oncol. 22:299–300. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Midulla C, Manganaro L, Longo F, Viggiani
V, Frati L, Granato T and Anastasi E: HE4 combined with MDCT
imaging is a good marker in the evaluation of disease extension in
advanced epithelial ovarian carcinoma. Tumour Biol. 33:1291–1298.
2012. View Article : Google Scholar : PubMed/NCBI
|