Introduction
Lung cancer is one of the most common malignant
tumors in the world, with non-small cell lung cancer (NSCLC)
accounting for 80–85% of all cases. Although many methods have been
developed for the treatment of NSCLC, such as surgical resection,
chemotherapy and radiotherapy, the prognosis of NSCLC remains poor
and the 5-year survival rate is only about 50% (1). In recent years, although many single
tumor biomarkers which may be predictive of response and prognosis,
including epidermal growth factor receptor (EGFR), the canonical
Wnt pathway and Notch3 have been developed, there is still lack of
specific and sensitive enough molecular biomarkers to accurately
predict the survival of NSCLC patients (2–4).
Rho guanine nucleotide exchange factor 5 (ARHGEF5)
is a member of guanine nucleotide exchange factors family (GEFs)
(5,6). Some studies have shown that ARHGEF5
can prompt the tumor metastasis and infiltration through its
effects on adhesion and cytoskeletal functions by activating Rho
GTPase (7,8). Debily et al(9) revealed that ARHGEF5 is overexpressed
in breast tumor, and might play a crucial role in breast tumor
progression. ARHGEF5 expression leads to altered growth properties
and tumorigenesis in mouse (5). Xie
et al(10) also showed that
ARHGEF5 mRNA levels were dramatically elevated in NSCLC cell lines
compared to normal lung tissue. However, the expression of ARHGEF5
in the lung cancer tissues is unknown.
Src, a member of the Src family of tyrosine kinases,
is a key regulator of cellular proliferation, survival, motility
and invasiveness (11). In NSCLC,
overexpression of Src has been shown to play an important role in
tumor development and metastases. ARHGEF5 is crucial for
Src-induced podosome formation (12). Overexpression of ARHGEF5 promotes
actin stress fiber remodeling through activating RhoA, and the
activation of RhoA or Cdc42 is required for Src-induced podosome
formation.
In light of the above mentioned considerations, we
examined the expression of ARHGEF5 and Src in resected NSCLC
tissues and evaluated the correlation between ARHGEF5 and Src.
Furthermore, we explored the relationship between the expression of
ARHGEF5 and Src and the prognosis of resected NSCLC patients.
Materials and methods
Patients and cell lines
Consecutive cohorts of NSCLC tumors resected from
193 NSCLC patients from July, 2010 to December, 2011 were analyzed.
Information on baseline demographics, clinicopathological
characteristics and surgical approach was collected after review of
clinical notes and histopathology reports. Patients who did not
receive a curative resection and had a previous history of cancer,
pre-surgical chemotherapy or radiotherapy were excluded. All
patients gave their written informed consent for participation in
this study. This study was approved by the Southwest Hospital
Ethics Committee. Another four NSCLC tissue samples as well as
their corresponding normal tissues adjacent to resection margins
from patients for western blot analysis were also obtained.
Normal human bronchus epithelial cell (HBE) and
NSCLC cells H322, SPC-1, H1650 (adenocarcinima) and H520 (squamous
cell) were obtained from Academy of Military Medical Science
(Beijing, China) and maintained in RPMI-1640 or DMEM (Trace,
Melbourne, Australia) supplemented with 10% fetal bovine serum
(FBS), 100 U/ml penicillin, and 100 μg/ml streptomycin at 37°C, in
a humid atmosphere of 5% CO2.
Tissue microarray
Tissue microarrays (TMAs) were constructed as
previously described (13).
Briefly, using the H&E sections as templates, representative
areas of each tumor were identified and marked on a section of the
donor block. Approximately 4 μm-thick (1.5-mm diameter) tissue
cylinders were punched from each donor paraffin block using a TMA
instrument (Beecher Instruments; Silver Spring, MD, USA). The donor
cores were placed into the corresponding recipient block holes that
were punched in advance using the same TMA instrument. To better
represent each case, two tumor and two normal tissue cores that
were located adjacent to the tumor were punched from each case.
After construction, recipient blocks were placed into an oven at
37°C for 20 min, rapidly removed, and pressed down by a slide for a
moment to flatten the surface. Serial 4 μm-thick sections were cut
with a Leica microtome (Leica Microsystems; Wetzlar, Germany) and
mounted onto polylysine-coated slides.
Immunohistochemistry
All tissue sections were routinely dewaxed,
rehydrated, and prepared for immunohistochemistry. Sodium citrate
buffer (pH 6.0) was used as an antigen retrieval solution, and the
sections were blocked with 5% BSA, and incubated with 1:50
polyclonal rabbit anti-ARHGEF5 (11379-1-AP, Proteintech Group),
1:50 polyclonal goat anti-Src antibody (AF3389, R&D) overnight.
The tissue sections were then incubated with secondary antibodies
and DAB reagent (Gene Tech, Shanghai, China), and counterstained
with hematoxylin, followed by dehydration and visualization with
3.3-diaminobenzidine (Gene Tech, Shanghai, China). Negative
controls were performed in each case by replacing the primary
antibody with PBS.
Expression of ARHGEF5 and Src was evaluated as the
percentage of positive cells in a specimen, and by staining
intensity as previously described (14). The percentage of positive cells was
evaluated quantitatively and scored as 0 for staining of ≤1% of
total cells counted, 1 for staining of 2–25%, 2 for staining of
26–50%, 3 for staining of 51–75%, and 4 for staining of >75% of
the cells examined. Intensity was graded as follows: 0, no signal;
1, weak; 2, moderate; and 3, strong staining. A total ‘staining
score’ of 0–12 was calculated and graded as negative (−, score
0–1), weak (+, score 2–4), moderate (++, score 5–8), or strong
(+++, score 9–12). The staining score was evaluated by two
experienced pathologists. Discrepant cases were reviewed in a
multi-head microscope and reported as a consensus.
Fluorescent immunohistochemistry
Immunofluorescent staining was conducted to localize
the expression of Src and ARHGEF5. The frozen surgically resected
sections from NSCLC patients were fixed for 20 min in 4%
paraformaldehyde. The lung tissues of patient were then rinsed 3
times with PBS for 5 min each time, and incubated in a
protein-blocking solution for 20 min at room temperature. After
incubation with the primary antibody against either human ARHGEF5
(1:50; 11379-1-AP, Proteintech Group) or human Src (1:50; AF3389,
R&D) overnight at 4°C, followed by incubation with the
secondary antibody (either myc-conjugated IgG, 1:50, Santa Cruz; or
Cy3-conjugated IgG, 1:50, Beyotime) at 37°C for 1 h, the cells and
lung tissue of patient were counterstained with Hoechst 33342 to
reveal the nuclei. Cells or slides without incubation primary
antibodies were served as negative controls. The cells or slides
were then analyzed by confocal laser scanning microscopy.
Western blot analysis
Tumor cells or cell lines were lysed in lysis
buffer: 50 mmol/l Tris-HCl (pH 8.0), 150 mmol/l NaCl, 0.5% NP40,
0.5% sodium deoxycholate, and Protease Inhibitor Cocktail Set III
(Calbiochem). The protein concentration was determined using a
Bio-Rad protein assay (Bio-Rad) with bovine serum albumin as
standard. Each lysate (10 μg) were resolved on 10–12% denaturing
polyacrylamide gels (with 3% polyacrylamide stacking gel) and
transferred electrophoretically onto a nitrocellulose membrane (GE
Healthcare Biosciences). After blocking with 5% nonfat dry milk in
TBST, the membrane was incubated with a rabbit polyclonal antihuman
ARHGEF5 antibody or a goat polyclonal antihuman Src antibody for 1
h at room temperature. Immunoreactive proteins were incubated with
horseradish peroxidase-conjugated mouse HRP-linked IgG antibody
(1:700 dilution in TBSTT with 2% dry milk) (GE Healthcare
Biosciences) for 1 h at room temperature. After washing with TBST,
the reactants were developed using the enhanced chemiluminescence
kit (GE Healthcare Biosciences).
Co-immunoprecipitation and immunoblot
analyses
The Co-immunoprecipitation analysis was performed as
previously described (15). In
briefly, H322 or H1650 cell lysate were immunoprecipitated
overnight with 3 μg of the Polyclonal Goat anti-Src antibody
(AF3389, R&D). Immunoprecipitates were collected on protein A/G
beads (30 μl per immunoprecipitation). Beads were washed three
times in lysis buffer, resuspended in 35 μl of Laemmli sample
buffer, and resolved on 7.5% SDS-polyacrylamide gels. Proteins were
transferred to nitrocellulose membranes (Protran; Schleicher and
Schuell), immunoblotted with the Polyclonal Rabbit anti-ARHGEF5
(11379-1-AP, Proteintech Group), and subjected to chemiluminescent
detection.
Statistical analysis
SPSS 18.0 (SPSS Inc., Chicago, IL, USA) was used to
perform the statistical analysis. Chi-square test and likelihood
ratio test were used to illustrate the significance of various
clinical characteristics. The χ2 test was used to assess
the association between clinical features and the expression of
biological factors. OS and the 95% confidence intervals (CIs) were
evaluated by the Kaplan-Meier method comparing the different groups
by log-rank test. The Cox proportional hazards model was used to
evaluate the prognostic role of each single studied parameter on
OS, in univariate and multivariate analyses. P-values were
considered statistically significant at <0.05.
Results
Clinical characteristics of the
patients
The patient clinical characteristics are summarized
according to the histologic types (Table I). A total of 193 NSCLC patients
(male, 145; female, 48; average age, 61.84 years; age range, 31–84)
were enrolled in this study, of which 99 cases were squamous cell
carcinoma (SCC) (51.30%) and 94 cases were adenocarcinomas (ADC)
(48.70%). Of the patients enrolled in the study, 83 cases (43.01%)
had tumor metastasis in the lymph nodes and 110 cases (56.99%) did
not (Table I).
 | Table ICharacteristics of the NSCLC
patients. |
Table I
Characteristics of the NSCLC
patients.
| Characteristics | Cases (%) |
|---|
| Histology |
| SCC | 99 (51.30) |
| ADC | 94 (48.70) |
| Age (years) |
| <60 | 70 (36.27) |
| ≥60 | 123 (63.73) |
| Gender |
| Male | 145 (75.13) |
| Female | 48 (24.87) |
| Pathologic Stage |
| I | 68 (35.23) |
| II | 61 (31.61) |
| III | 64 (33.16) |
| Tumor Grade |
| I | 15 (7.78) |
| II | 108 (55.96) |
| III | 70 (36.27) |
| Lymph node
metastasis |
| Positive | 83 (43.01) |
| Negative | 110 (56.99) |
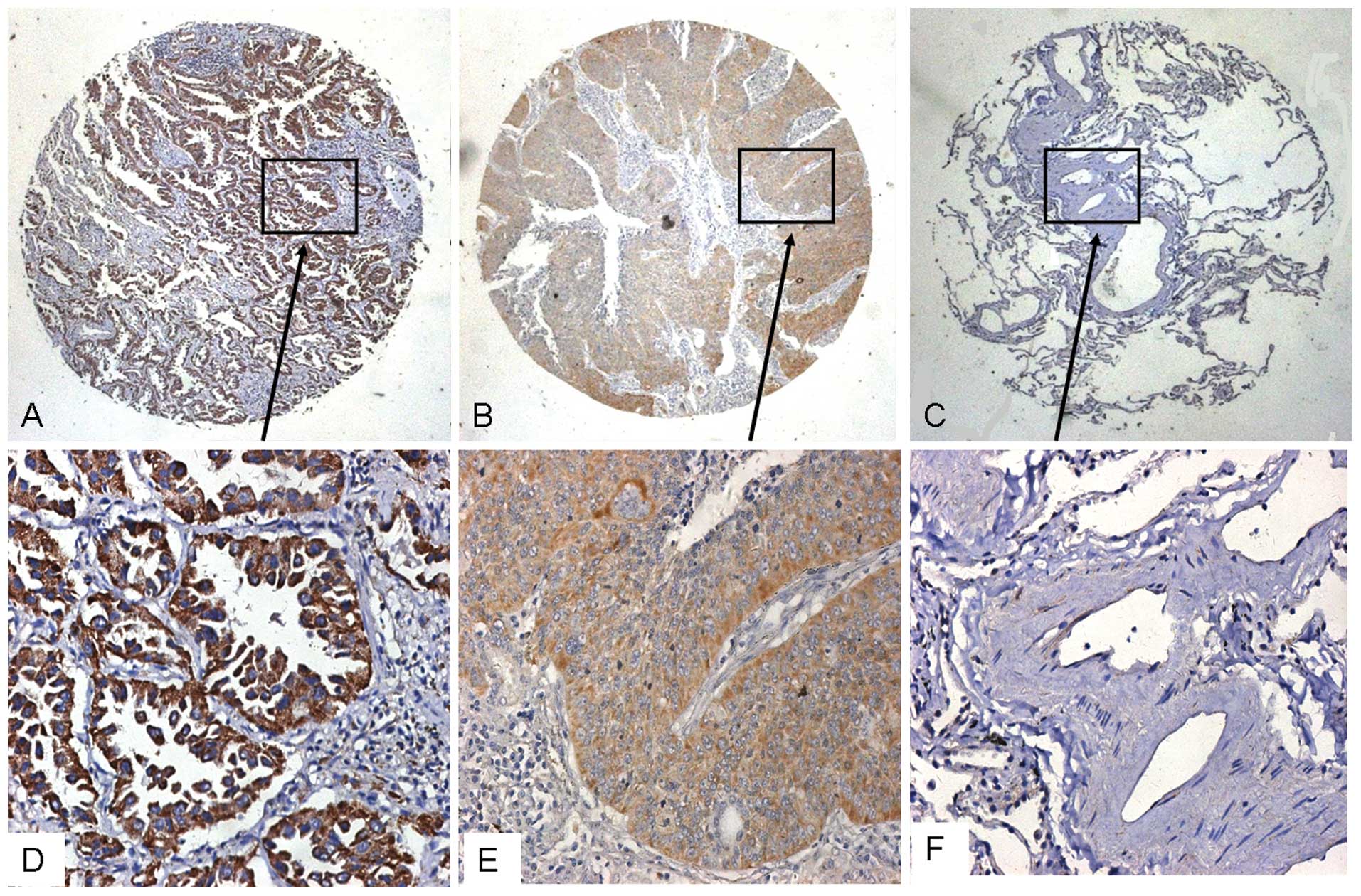
Expression of ARHGEF5 in NSCLC
As shown in Fig. 1,
ARHGEF5 expression was detected in the ADC and SCC tissues, but not
in the adjacent tissues. The ARHGEF5 was mainly located in the
cytoplasma of tumor cells. In all 193 cases, ARHGEF5 was positive
in 133 cases (68.91%) and negative in 60 cases (31.09%) (Table II). According to the histological
subtypes, ARHGEF5 was detected in 64 of 94 cases of ADC (68.09%)
and 69 of 99 cases of SCC (69.70%) (Table II). The level of ARHGEF5 in poorly
differentiated tumors was significantly higher than that in
moderately-to-well differentiated tumors (P=0.032, Table II). Younger patients (<60 years)
also exhibited higher ARHGEF5 expression than older ones (P=0.043,
Table II). Furthermore, the level
of ARHGEF5 was significantly associated with tumor stage (P=0.027,
Table II).
| Table IIRelationship between the clinical
characteristics and the expression of ARHGEF5. |
Table II
Relationship between the clinical
characteristics and the expression of ARHGEF5.
|
Characteristics | ARHGEF5 positive
cases (%) | ARHGEF5 negative
cases (%) | Total | P-value |
|---|
| Histology |
| SCC | 69 (69.70) | 30 | 99 | 0.931 |
| ADC | 64 (68.09) | 30 | 94 | |
| Gender |
| Male | 103 (71.03) | 42 | 145 | 0.299 |
| Female | 30 (62.5) | 18 | 48 | |
| Age (years) |
| ≥60 | 78 (63.41) | 45 | 123 | 0.043 |
| <60 | 55 (78.57) | 15 | 70 | |
|
Differentiation |
|
Well/moderately | 71 (57.72) | 52 | 123 | 0.032 |
| Poorly | 52 (74.29) | 18 | 70 | |
| Tumor stage |
| I | 39 (57.35) | 29 | 68 | 0.027 |
| II | 48 (78.69) | 13 | 61 | |
| III | 45 (70.31) | 19 | 64 | |
| Lymph node
metastasis |
| Yes | 60 (72.29) | 23 | 83 | 0.469 |
| No | 73 (66.36) | 37 | 110 | |
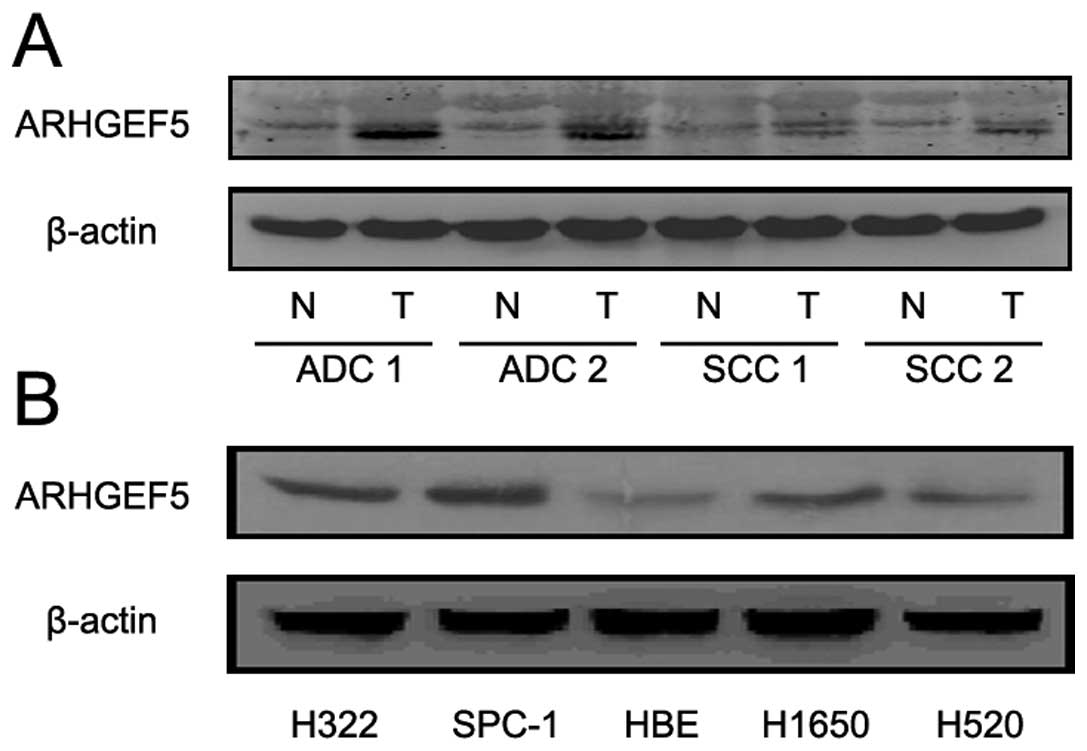
In addition, we examined the expression of ARHGEF5
in lung cancer tissues and NSCLC cell lines by western blotting.
The level of ARHGEF5 protein was obviously higher in tumor tissues
than in adjacent tissues (Fig. 2A).
Similar results were observed in NSCLC cell lines than in human
broncho-epithelial (HBE) cells (Fig.
2B).
Expression of Src in NSCLC
As shown in Table
III, among the 133 NSCLC patients with positive ARHGEF5
expression, 110 cases (56.99%) showed positive Src expression,
whereas 23 cases showed negative Src expression. In contrast, among
the 60 patients with negative ARHGEF5, 25 patients showed negative
Src expression, whereas 35 patients showed positive Src protein
expression. Among the 64 ADC patients with positive ARHGEF5
expression, 59 showed positive Src expression, whereas 5 patients
had negative Src expression. In contrast, among the 30 patients
with negative ARHGEF5, 12 patients showed negative Src expression,
whereas 18 patients had positive Src protein expression. A
significant correlation between ARHGEF5 and Src expression in NSCLC
(χ2=11.874, P=0.001) and in ADC (χ2=12.194,
P=0.000) was found. However, there was no correlation between
ARHGEF5 and Src expression in SCC.
| Table IIICorrelation between ARHGEF5 and Src
expression in the tumor tissues of NSCLC patients. |
Table III
Correlation between ARHGEF5 and Src
expression in the tumor tissues of NSCLC patients.
| Subtypes | Group | ARHGEF5 (+) | ARHGEF5 (−) | Total | P-value |
|---|
| NSCLC | Src (+) | 110 | 35 | 145 | 0.001 |
| Src (−) | 23 | 25 | 48 | |
| Total | 133 | 60 | 193 | |
| SCC | Src (+) | 50 | 17 | 67 | 0.107 |
| Src (−) | 18 | 14 | 32 | |
| Total | 68 | 31 | 99 | |
| ADC | Src (+) | 59 | 18 | 77 | 0.000 |
| Src (−) | 5 | 12 | 17 | |
| Total | 64 | 30 | 94 | |
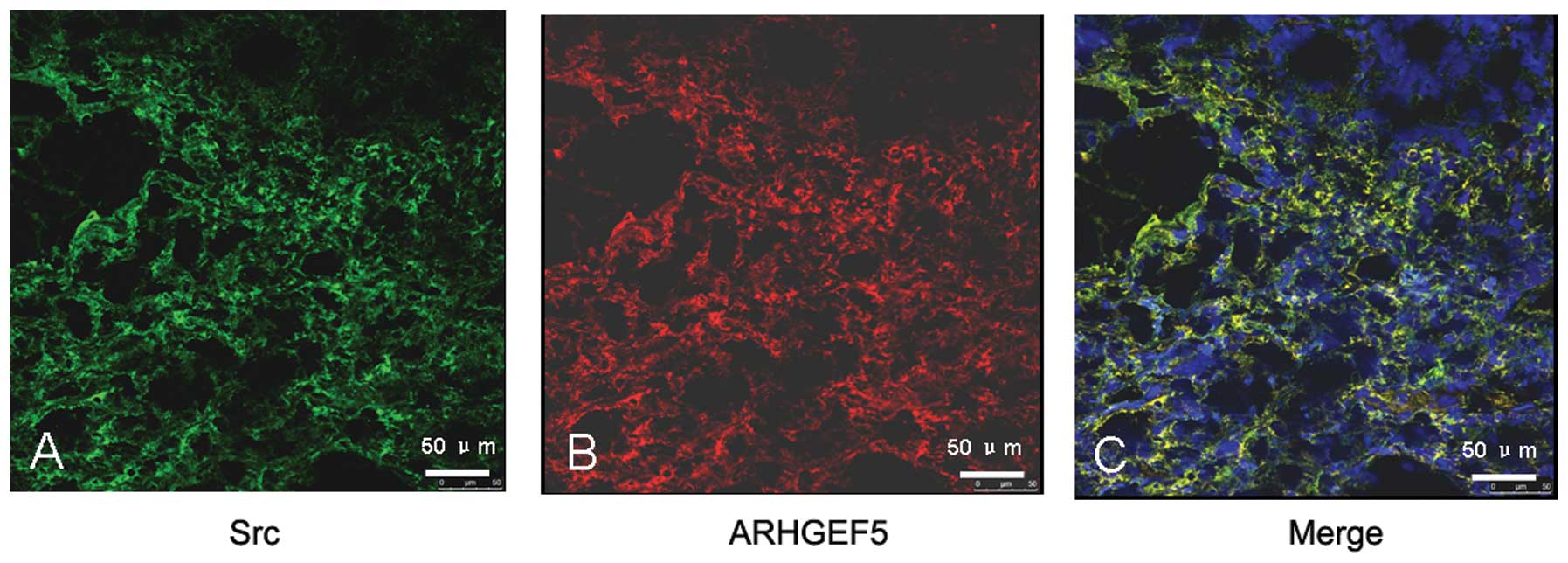
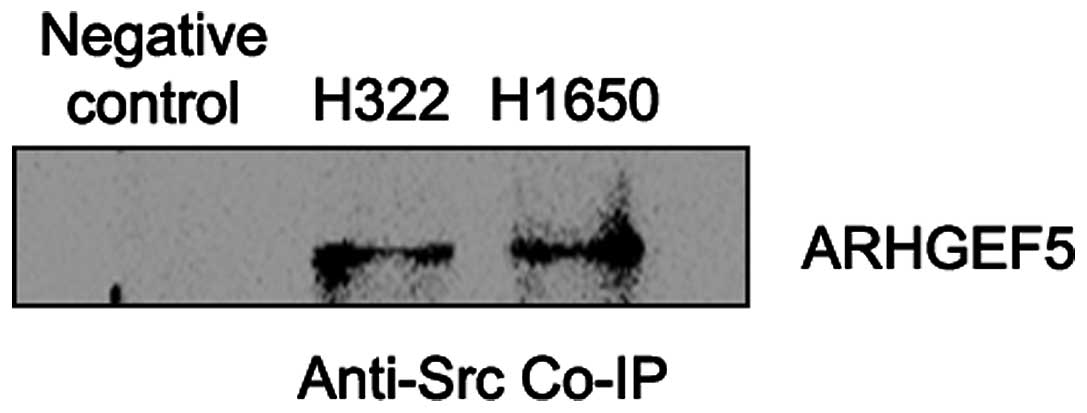
ARHGEF5 interacts with Src directly in
NSCLC
To confirm the interaction between ARHGEF5 and Src,
fluorescent immunohistochemistry and co-immunoprecipitation were
performed with the tumor tissues and lung cancer cell lines,
respectively. It was shown that ARHGEF5 and Src were co-expressed
in NSCLC patient tumor tissues (Fig.
3) and the interaction between Src and ARHGEF5 was revealed by
co-immunoprecipitation in NCI-H322 cells and NCI-H1650 cells
(Fig. 4).
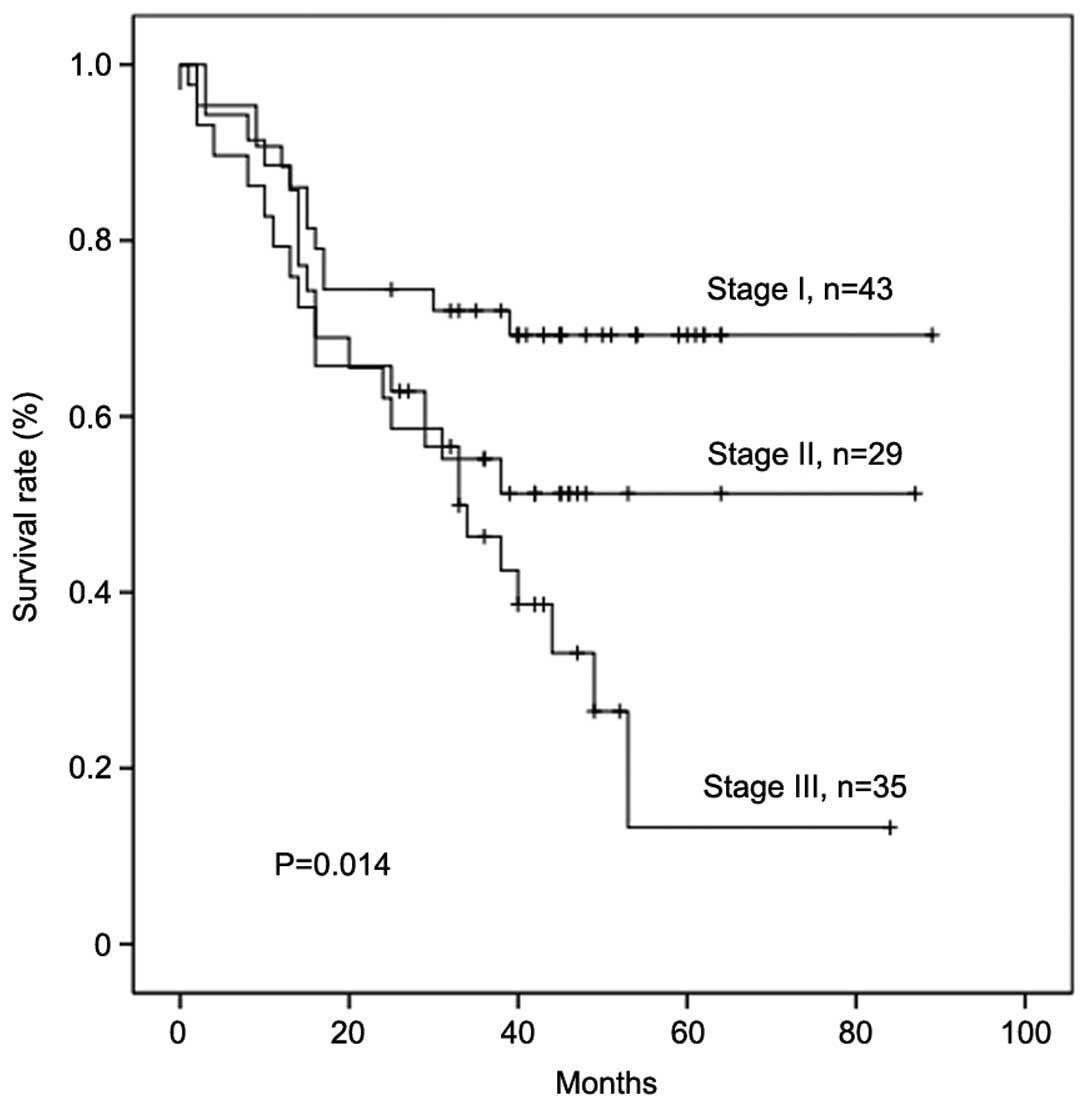
Survival analysis
A total of 107 patients completed the overall
survival (OS) follow-up and 86 patients were lost to follow-up. The
median follow-up time was 34.29 months. There was a significant
difference in the OS time of patients in different clinical stages
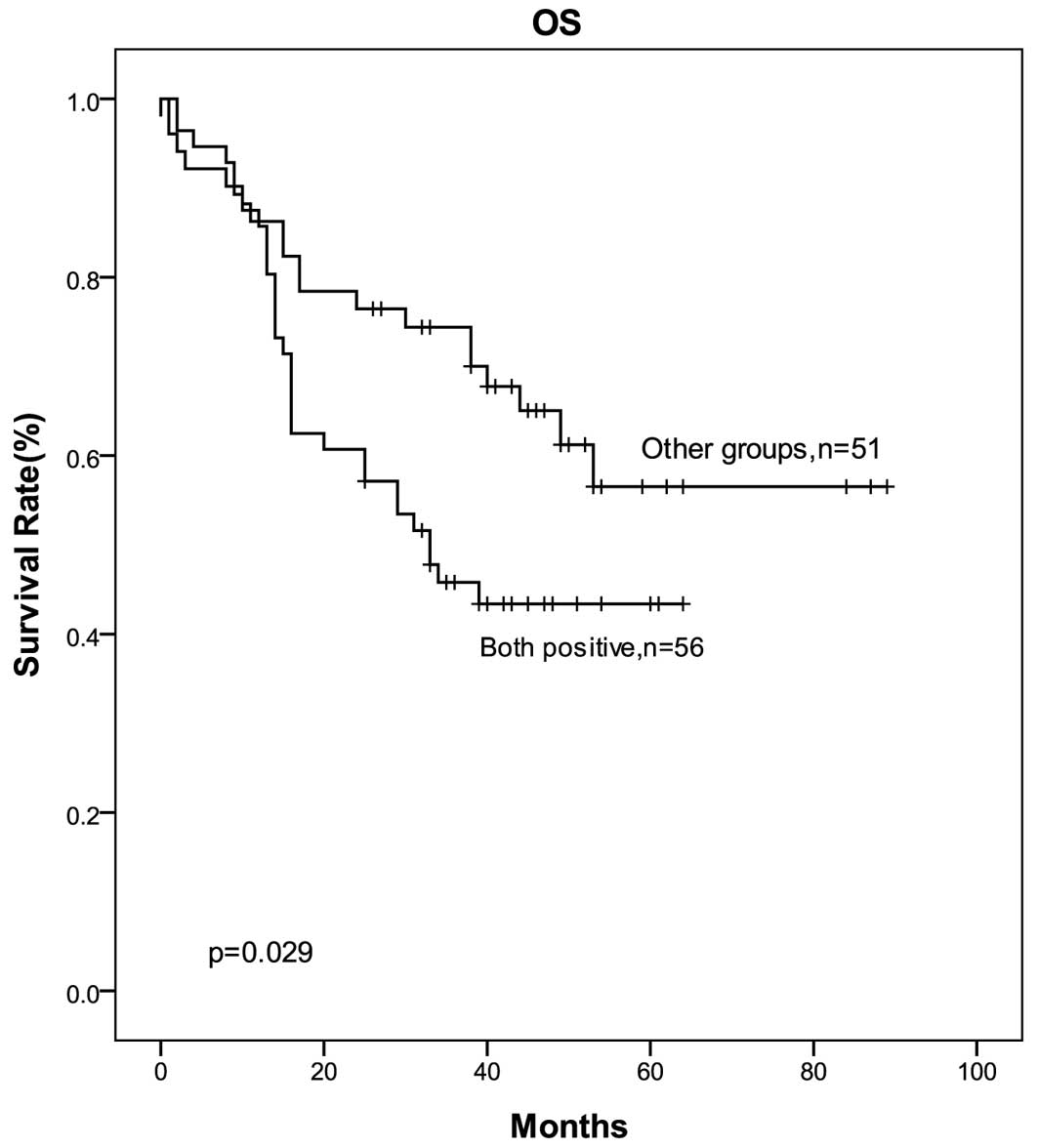
(Fig. 5). To further explore
whether there was a correlation between the co-expression of
ARHGEF5 and Src and OS time, the patients were stratified into 2
groups according to ARHGEF5 and Src expression: group 1,
ARHGEF5(+)/Src(+) patients (n=56); group 2, other patients (n=51).
The median survival times for group 1 and group 2 were 29.37 months
and 39.90 months, respectively. The patients in ARHGEF5(+)/Src(+)
group showed a worse OS compared with the other patients (29.37
months versus 39.90 months, P=0.029, Fig. 6).
Discussion
In the present study, we assessed the expression of
ARHGEF5 in NSCLC tissues and the possible correlation of ARHGEF5
and Src co-expression with the survival time of NSCLC patients. The
results revealed a significant increase of ARHGEF5 expression in
NSCLC tissues and cultured cell lines compared with in matched
adjacent tissues and HBE cells, respectively. Notably, an
interaction between ARHGEF5 and Src was detected in both NSCLC
tissues and cultured lung cancer cells. Among the cases completing
the OS follow-up, the patients with ARHGEF5(+)/Src(+) showed a
worse OS time compared with the other patients.
In the development and progression of human lung
cancer, many recent studies have revealed a link with the
deregulation of GEFs (16). The
expression of Rac1-GEF Tiam1 is higher in high-metastatic cells
than in low-metastatic cells, and downregulation of Tiam1 can
reduce the invasiveness of high-metastatic human giant-cell lung
cancer cells (17). ECT2, a member
of the human Dbl family GEFs, is overexpressed in the lung and
esophageal cancers. Furthermore, high level of ECT2 was found to be
associated with poor prognosis of lung cancer patients (18). Aberrant expression of Vav1 was found
in 42% of 78 lung cancer cell lines examined and 46% of 57 human
primary lung cancer specimens and the depletion of Vav1 expression
in H358 and H441 lung cancer cells resulted in the reduction of
colony formation in soft agar in vitro and tumor size in
nude mice (19,20). A recent study showed that Vav2- and
Vav3-deficiency reduced microvascular density, tumor cell growth
and survival in the transplanted B16 melanoma and Lewis lung
carcinoma models in vivo(21). In the present study, we showed that
ARHGEF5 was also highly expressed in the resected NSCLC tissues and
cultured lung cancer cell lines. In addition, we showed that
ARHGEF5 was closely correlated with age, tumor stage and
differentiation. It is well known that younger NSCLC patients
usually display a more aggressive disease course (22,23).
In the present study, we found that the expression of ARHGEF5 in
young patients (<60 years) was significantly higher than that in
older patients (>60 years). Since the tumor stage and
differentiation had a high correlation with the prognosis, the
level of ARHGEF5 might correlate with the prognosis of NSCLC
patients. Thus, the overexpression of ARHGEF5 in young patients may
be related to the aggressive disease course.
High levels of Src kinase activity, which can
promote tumor cell growth and differentiation (24,25)
have been observed in many cancer types, including lung cancer
(26–28). Src may stimulate tumorigenesis in
NSCLC in a variety of ways, such as the signal transducer and
activator of transcription 3 (STAT-3) and focal adhesion kinase
(FAK)-related pathways, both of which are involved in tumor
survival (29,30). Src activates the VEGF pathway via
STAT-3 (31) and in response to
hypoxia in human lung adenocarcinoma cells, thus increasing the
blood supply to the oxygen-starved tumor (32). In this study, we found that Src was
extensively expressed in NSCLC tissues. Then we further analyzed
the co-expression of ARHGEF5 and Src in SCC and ADC, the results
showed that the positive rate of ARHGEF5 and Src co-expression was
higher in ADC (62.77%) than in SCC (50.51%) and the expression of
ARHGEF5 was associated with the expression of Src ADC
(χ2=12.194, P=0.000), but not in SCC. Furthermore, it
has been reported that ARHGEF5 is able to be phosphorylated by Src
and then bound to Src to form a complex with Src and PI3K (12). Our results showed that there was a
dynamic interaction between ARHGEF5 and Src in the lung cancer
tissues and lung cancer cell lines, indicating that the Src-ARHGEF5
pathway may play a role in the tumorigenesis and development of ADC
rather than SCC.
To explore the clinical significance of
co-expression of ARHGEF5 and Src in patients with resected NSCLC,
we analyzed the correlation of ARHGEF5 and Src co-expression and
the OS in NSCLC patients. Noteworthy, we found patients with
ARHGEF5(+)/Src(+) had a significantly shorter OS than the other
patients. Therefore, ARHGEF5/Src can be considered a candidate
prognostic biomarker for patients with resected NSCLC. Furthermore,
activation of STAT-3 and FAK by Src is required for
anchorage-dependent and -independent cell growth in a range of
human tumors including NSCLC (30).
Therefore, Src, a cellular tyrosine kinase, offers a particularly
promising molecular target for anticancer therapy, as inhibition of
Src may lead to the inhibition of multiple signaling pathways, and
thereby the inhibition of tumor progress. However, although a
number of Src inhibitors are currently being investigated as
potential therapies for NSCLC, such as dasatinib (11,33),
the antitumor activity of Src inhibitors is limited. Thus, the
combination with other signal protein inhibitors is often needed
(34). In the present study, we
showed that ARHGEF5 was overexpressed in the lung cancer tissues
and correlated with tumor stage and differentiation. In addition,
co-expression of ARHGEF5 and Src was correlated with the prognosis
of NSCLC patients and there was an interaction between ARHGEF5 and
Src in the lung cancer tissues. These findings suggest that
inhibition of both Src and ARHGEF5 in NSCLC may be a promising
cancer therapy for patients with resected NSCLC.
In conclusion, our study found an obvious expression
of ARHGEF5 in the NSCLC tissues and lung cancer cell lines. The
expression of ARHGEF5 correlated with age, tumor stage and the
differentiation. In addition, Src was also expressed in the NSCLC
tissues, and co-expression of Src and ARHGEF5 correlated with
shorter OS time, indicating ARHGEF5/Src can be considered as a
prognostic biomarker and a therapeutic target for patients with
resected NSCLC.
Acknowledgements
This study was supported by the National Natural
Science Foundation of China (No. 81001045).
References
|
1
|
Goya T, Asamura H, Yoshimura H, et al:
Prognosis of 6644 resected non-small cell lung cancers in Japan: a
Japanese lung cancer registry study. Lung Cancer. 50:227–234. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Lee SY, Kim MJ, Jin G, et al: Somatic
mutations in epidermal growth factor receptor signaling pathway
genes in non-small cell lung cancers. J Thorac Oncol. 5:1734–1740.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Casas-Selves M, Kim J, Zhang Z, et al:
Tankyrase and the canonical Wnt pathway protect lung cancer cells
from EGFR inhibition. Cancer Res. 72:4154–4164. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Ye YZ, Zhang ZH, Fan XY, et al: Notch3
overexpression associates with poor prognosis in human
non-small-cell lung cancer. Med Oncol. 30:5952013. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Chan AM, McGovern ES, Catalano G, Fleming
TP and Miki T: Expression cDNA cloning of a novel oncogene with
sequence similarity to regulators of small GTP-binding proteins.
Oncogene. 9:1057–1063. 1994.PubMed/NCBI
|
|
6
|
Takai S, Chan AM, Yamada K and Miki T:
Assignment of the human TIM proto-oncogene to 7q33-->q35. Cancer
Genet Cytogenet. 83:87–89. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zheng Y: Dbl family guanine nucleotide
exchange factors. Trends Biochem Sci. 26:724–732. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Hart MJ, Eva A, Evans T, Aaronson SA and
Cerione RA: Catalysis of guanine nucleotide exchange on the CDC42Hs
protein by the dbl oncogene product. Nature. 354:311–314. 1991.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Debily MA, Camarca A, Ciullo M, et al:
Expression and molecular characterization of alternative
transcripts of the ARHGEF5/TIM oncogene specific for human breast
cancer. Hum Mol Genet. 13:323–334. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Xie X, Chang SW, Tatsumoto T, Chan AM and
Miki T: TIM, a Dbl-related protein, regulates cell shape and
cytoskeletal organization in a Rho-dependent manner. Cell Signal.
17:461–471. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Giaccone G and Zucali PA: Src as a
potential therapeutic target in non-small-cell lung cancer. Ann
Oncol. 19:1219–1223. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Kuroiwa M, Oneyama C, Nada S and Okada M:
The guanine nucleotide exchange factor Arhgef5 plays crucial roles
in Src-induced podosome formation. J Cell Sci. 124:1726–1738. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Li P, Zhang Z, Wang Q, et al: The ectopic
expression of IFN regulatory factor 4-binding protein is correlated
with the malignant behavior of human breast cancer cells. Int
Immunopharmacol. 9:1002–1009. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Maaser K, Daubler P, Barthel B, et al:
Oesophageal squamous cell neoplasia in head and neck cancer
patients: upregulation of COX-2 during carcinogenesis. Br J Cancer.
88:1217–1222. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Sharma SV, Oneyama C, Yamashita Y, et al:
UCS15A, a non-kinase inhibitor of Src signal transduction.
Oncogene. 20:2068–2079. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Lazer G and Katzav S: Guanine nucleotide
exchange factors for RhoGTPases: good therapeutic targets for
cancer therapy? Cell Signal. 23:969–979. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hou M, Tan L, Wang X and Zhu YS: Antisense
Tiam1 down-regulates the invasiveness of 95D cells in vitro. Acta
Biochim Biophys Sin. 36:537–540. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hirata D, Yamabuki T, Miki D, et al:
Involvement of epithelial cell transforming sequence-2 oncoantigen
in lung and esophageal cancer progression. Clin Cancer Res.
15:256–266. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Fernandez-Zapico ME, Gonzalez-Paz NC,
Weiss E, et al: Ectopic expression of VAV1 reveals an unexpected
role in pancreatic cancer tumorigenesis. Cancer Cell. 7:39–49.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lazer G, Idelchuk Y, Schapira V, Pikarsky
E and Katzav S: The haematopoietic specific signal transducer Vav1
is aberrantly expressed in lung cancer and plays a role in
tumourigenesis. J Pathol. 219:25–34. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Brantley-Sieders DM, Zhuang G, Vaught D,
et al: Host deficiency in Vav2/3 guanine nucleotide exchange
factors impairs tumor growth, survival, and angiogenesis in vivo.
Mol Cancer Res. 7:615–623. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Serrano-Olvera A and Gerson R: Age
associated survival rate in non small cell lung cancer. Gac Med
Mex. 145:27–35. 2009.(In Spanish).
|
|
23
|
Salmeron D, Chirlaque MD, Isabel
Izarzugaza M, et al: Lung cancer prognosis in Spain: the role of
histology, age and sex. Respir Med. 106:1301–1308. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Xu W, Allbritton N and Lawrence DS: SRC
kinase regulation in progressively invasive cancer. PLoS One.
7:e488672012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Budde RJ, Ke S and Levin VA: Activity of
pp60c-src in 60 different cell lines derived from human tumors.
Cancer Biochem Biophys. 14:171–175. 1994.PubMed/NCBI
|
|
26
|
Mazurenko NN, Kogan EA, Zborovskaya IB and
Kisseljov FL: Expression of pp60c-src in human small cell and
non-small cell lung carcinomas. Eur J Cancer. 28:372–377. 1992.
View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Masaki T, Igarashi K, Tokuda M, et al:
pp60c-src activation in lung adenocarcinoma. Eur J Cancer.
39:1447–1455. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Thomas SM and Brugge JS: Cellular
functions regulated by Src family kinases. Annu Rev Cell Dev Biol.
13:513–609. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Laird AD, Li G, Moss KG, et al: Src family
kinase activity is required for signal tranducer and activator of
transcription 3 and focal adhesion kinase phosphorylation and
vascular endothelial growth factor signaling in vivo and for
anchorage-dependent and -independent growth of human tumor cells.
Mol Cancer Ther. 2:461–469. 2003.
|
|
30
|
Song L, Turkson J, Karras JG, Jove R and
Haura EB: Activation of Stat3 by receptor tyrosine kinases and
cytokines regulates survival in human non-small cell carcinoma
cells. Oncogene. 22:4150–4165. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Eliceiri BP, Paul R, Schwartzberg PL, Hood
JD, Leng J and Cheresh DA: Selective requirement for Src kinases
during VEGF-induced angiogenesis and vascular permeability. Mol
Cell. 4:915–924. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Sato M, Tanaka T, Maeno T, et al:
Inducible expression of endothelial PAS domain protein-1 by hypoxia
in human lung adenocarcinoma A549 cells. Role of Src family
kinases-dependent pathway. Am J Respir Cell Mol Biol. 26:127–134.
2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Johnson FM, Bekele BN, Feng L, et al:
Phase II study of dasatinib in patients with advanced
non-small-cell lung cancer. J Clin Oncol. 28:4609–4615. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Haura EB, Tanvetyanon T, Chiappori A, et
al: Phase I/II study of the Src inhibitor dasatinib in combination
with erlotinib in advanced non-small-cell lung cancer. J Clin
Oncol. 28:1387–1394. 2010. View Article : Google Scholar : PubMed/NCBI
|