Introduction
Advanced prostate cancer requires androgen for
growth and usually responds to androgen deprivation therapy
(1–4). The disease progresses, however, due to
the development of mechanisms of resistance to an
androgen-independent state (also referred to as
castration-resistant or hormone-refractory) (5,6).
Additional therapies such as chemotherapy and newer antiandrogens
are only temporarily effective (7,8).
Therefore, novel and less toxic approaches for delaying the
progression of prostate cancer to androgen independence or delaying
the need to start such additional therapies would change the
treatment paradigm for managing prostate cancer and be of great
benefit for patients.
Atorvastatin is a widely used statin drug for
lowering cholesterol (9,10). Celecoxib is a selective
cyclooxygenase-2 (COX-2) inhibitor. Previous studies investigating
either statin drugs (including atorvastatin) or celecoxib have
found that they have anti-prostate cancer activity (11–16).
However, the effects of these two drugs in combination on prostate
cancer progression to androgen independence have not yet been
studied. Our previous study found that administration of a
combination of atorvastatin and celecoxib was more effective than
either agent alone for inhibiting azoxymethane-induced colon
carcinogenesis in rats (17). More
recently we found that atorvastatin and celecoxib in combination
synergistically inhibited the growth and induced apoptosis in
cultured prostate cancer cells. This combination inhibited the
progression of androgen-dependent LNCaP tumors to androgen
independence and the growth of androgen-independent PC-3 prostate
tumors in SCID mice more effectively than either agent alone
(18,19). Based on our preclinical studies, we
have a phase II clinical trial underway to determine whether a
combination of atorvastatin and celecoxib can stabilize or decrease
a previously rising PSA in prostate cancer patients who developed
biochemical relapse after surgery or radiation therapy. Due to the
beneficial effects, the study has now been expanded into a national
trial involving multiple cancer centers (NCT01220973). Although our
previous in vitro cell culture and in vivo animal
experiments showed that atorvastatin in combination with celecoxib
inhibited androgen-independent growth of prostate cancer cells, the
mechanisms for the effect are not clear. Since increased
interleukin (IL)-6 has been associated with progression of
androgen-dependent prostate cancer to androgen independence
(20–26), we hypothesized that atorvastatin and
celecoxib in combination would strongly inhibit the increased
formation of IL-6 that occurs during the formation of
androgen-independent LNCaP prostate tumors and that this inhibition
would lead to the suppression of prostate cancer growth.
In the present study, we determined the effect of
atorvastatin and celecoxib administration alone or in combination
on IL-6 levels in androgen-dependent prostate cancer LNCaP cells
grown in androgen-deficient medium. We found that culturing LNCaP
cells in androgen-depleted (AD) medium increased the levels of IL-6
and survivin, and treatment of these cells with atorvastatin in
combination with celecoxib inhibited the increase in IL-6 and
survivin. In animal experiments, we found that IL-6 expression was
increased in androgen-independent LNCaP tumors. Treatment of the
mice with atorvastatin or celecoxib alone inhibited the increase in
IL-6 and survivin as LNCaP tumors became androgen-independent, and
treatment of the mice with a combination of celecoxib and
atorvastatin resulted in a much stronger inhibition.
Materials and methods
Cells and reagents
LNCaP cells were obtained from the American Type
Culture Collection (ATCC, Rockville, MD, USA). Atorvastatin and
celecoxib were provided by the National Cancer Institute’s
Repository. Propylene glycol, polysorbate 80, benzyl alcohol,
ethanol and dimethyl sulfoxide (DMSO) were purchased from Sigma
(St. Louis, MO, USA). Matrigel was obtained from BD Biosciences
(Bedford, MA, USA). RPMI-1640 tissue culture medium,
penicillin-streptomycin, L-glutamine and fetal bovine serum (FBS)
were from Gibco-BRL (Grand Island, NY, USA). Charcoal-stripped FBS
was purchased from HyClone Inc. (Logan, UT, USA). LNCaP cells were
maintained in RPMI-1640 culture medium containing 10% FBS that was
supplemented with penicillin (100 U/ml)-streptomycin (100 μg/ml)
and L-glutamine (300 μg/ml). Atorvastatin and celecoxib were
dissolved in DMSO, and the final concentration of DMSO in all
experiments was 0.2%. In experiments with AD medium,
charcoal-stripped FBS was used to replace the regular FBS in the
cell culture medium.
Determination of the number of viable
cells
The number of viable cells after each treatment was
determined using a hemacytometer under a light microscope (Nikon
Optiphot, Japan). Cell viability was determined by the trypan blue
exclusion assay, which was conducted by mixing 80 μl of the cell
suspension and 20 μl of 0.4% trypan blue solution for 2 min. Blue
cells were counted as dead cells and the cells that did not absorb
dye were counted as live cells.
Morphological assessment of apoptotic
cells
Apoptosis was determined by morphological assessment
of cells stained with propidium iodide (27). Briefly, cytospin slides were
prepared after each experiment, and cells were fixed with
acetone/methanol (1:1) for 10 min at room temperature, followed by
10 min with propidium iodide staining (1 μg/ml in PBS) and analyzed
using a fluorescence microscope (Nikon Eclipse TE200, Japan).
Apoptotic cells were identified by classical morphological features
including nuclear condensation, cell shrinkage and formation of
apoptotic bodies (27). At least
200 cells were counted in each sample, and the percentage of
apoptotic cells was determined.
Western blotting
An antibody against survivin (AB3610) was obtained
from the Millipore Co. (Billerica, MA, USA). The western blot
analysis was performed as described in detail in our previous
publication (28). The extent of
protein loading was determined by blotting for β-actin, and the
levels of survivin in the western blotting were analyzed by optical
density measurement and normalized for β-actin to obtain the
relative density (RD) for the control and cells treated with
atorvastatin and/or celecoxib.
Progression of androgen-dependent
prostate LNCaP tumors to androgen independence in immunodeficient
mice
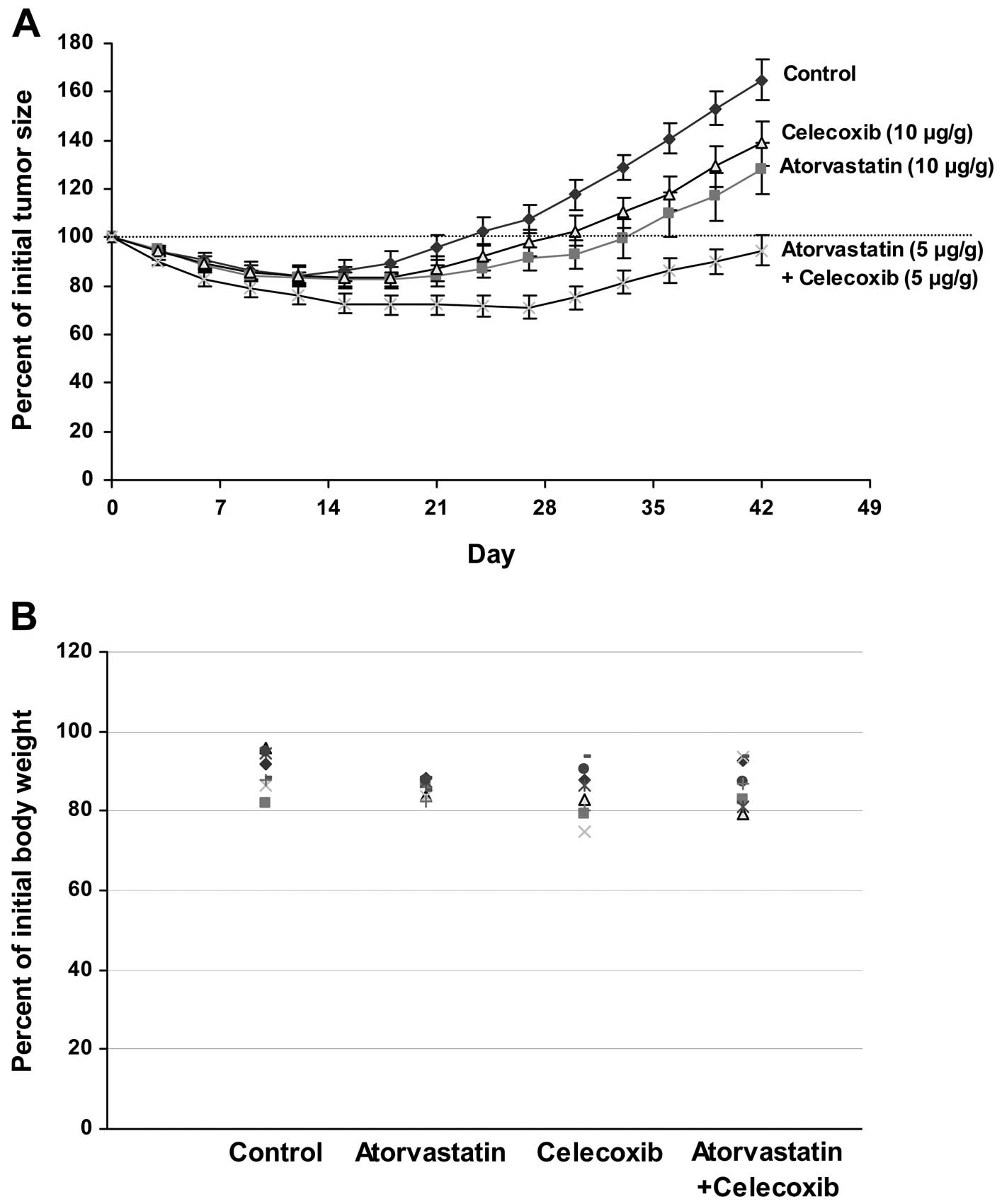
Male SCID mice with androgen-dependent LNCaP tumors
were surgically castrated and injected with vehicle (5 μl/g body
weight), atorvastatin (10 μg/g body weight), celecoxib (10 μg/g
body weight) or atorvastatin (5 μg/g body weight) + celecoxib (5
μg/g body weight) once a day for 42 days as described in detail in
our previous publication (18). The
animal experiment was carried out under an Institutional Animal
Care and Use Committee (IACUC)-approved protocol.
Immunostaining
An immunoperoxidase staining method (29) was used to determine the level of
IL-6 in LNCaP cells and the level of IL-6 and survivin in LNCaP
tumors. Briefly, cytospin slides of LNCaP cells or paraffin
sections of LNCaP tumors were incubated with either anti-IL-6
(AF-206-NA; R&D Systems, San Diego, CA, USA) or anti-survivin
(AB3610) antibody for 1 h at room temperature. The sections and
cytospin slides were then incubated with a biotinylated secondary
antibody for 30 min followed by incubation with conjugated-avidin
solution (Elite ABC kit purchased from Vector Laboratories) for 30
min. Color development was achieved by incubation with 0.02%
3,3′-diaminobenzidine tetrahydrochloride containing 0.02% hydrogen
peroxide for 10 min at room temperature.
Statistical analyses
The analysis of variance (ANOVA) method with the
Tukey-Kramer test (30) was used
for the comparison of growth inhibition and apoptosis. The
potential synergistic effect of atorvastatin and celecoxib was
assessed by the isobole method (31), using the equation Ac/Ae + Bc/Be =
combination index (CI); where Ac and Bc represent the concentration
of drug A and drug B used in the combination, and Ae and Be
represent the concentration of drug A and B that produced the same
magnitude of effect when administered alone. If CI is <1, then
the drugs are considered to act synergistically. If the CI is >1
or =1, then the drugs act in an antagonistic or additive manner,
respectively.
Results
Effects of atorvastatin and celecoxib on
growth and apoptosis in cultured prostate cancer LNCaP cells
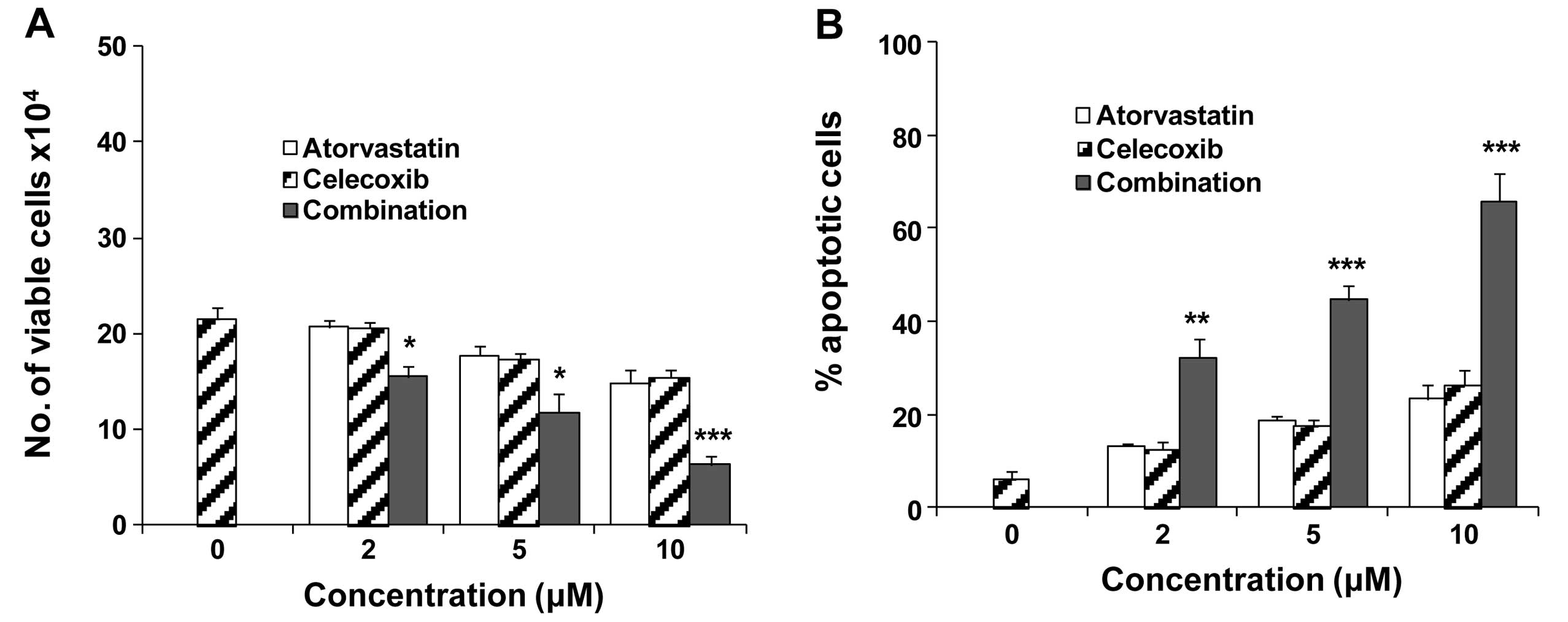
We determined the effects of atorvastatin and
celecoxib alone or in combination on growth and apoptosis in LNCaP
cells cultured in AD medium. LNCaP cells were cultured in AD medium
and treated with different concentrations of atorvastatin and
celecoxib alone or in combination for 96 h. Cell growth was
determined by counting the number of viable cells (Fig. 1A). As shown in Fig. 1A, treatment of LNCaP cells with
atorvastatin and celecoxib in combination had a stronger inhibitory
effect on cell growth than either drug alone. The CI (31) for IC50 was 0.81
indicating a synergistic effect when the cells were treated with a
combination of atorvastatin and celecoxib. Apoptosis in LNCaP cells
treated with atorvastatin and/or celecoxib was determined by
morphological assessment (Fig. 1B).
As shown in Fig. 1B, atorvastatin
and celecoxib in combination had a stronger stimulatory effect on
apoptosis than either drug alone. Indeed the apoptotic response
following treatment with 2 μM of each drug in combination was
greater than that for 10 μM of atorvastatin or celecoxib alone
(Fig. 1B). The CI for 50% apoptosis
was calculated as 0.56 indicating synergy.
Effects of atorvastatin and celecoxib
alone or in combination on the levels of IL-6 and survivin in
cultured LNCaP cells
Due to the important role of IL-6 in prostate cancer
progression (20–26), we determined the effect of
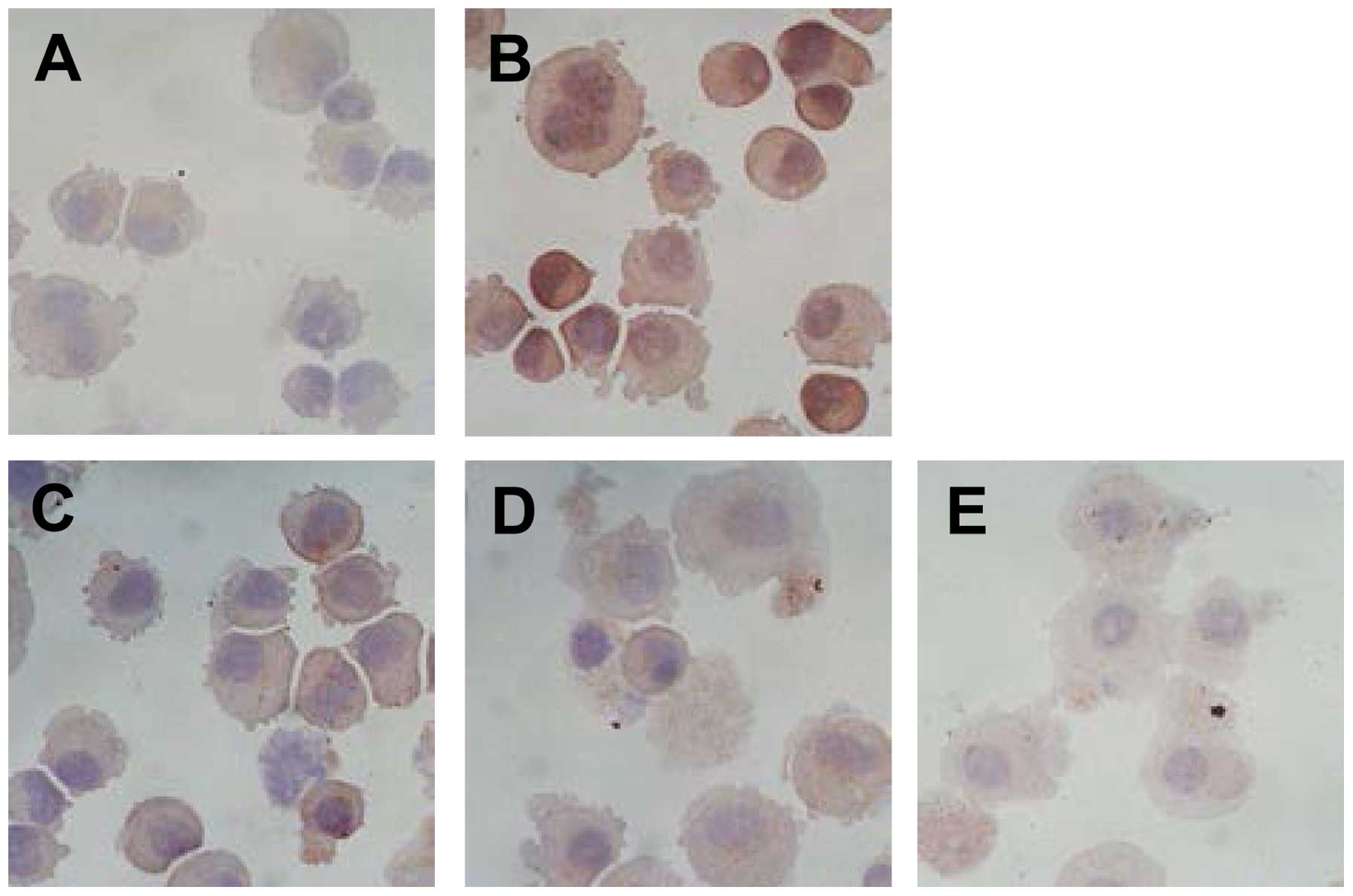
atorvastatin and/or celecoxib on this cytokine. As shown in
Fig. 2, culturing LNCaP cells in AD
medium increased the level of IL-6. Treatment of the cells in AD
medium with a combination of atorvastatin and celecoxib had a more
potent effect for inhibiting the increase in IL-6 than either drug
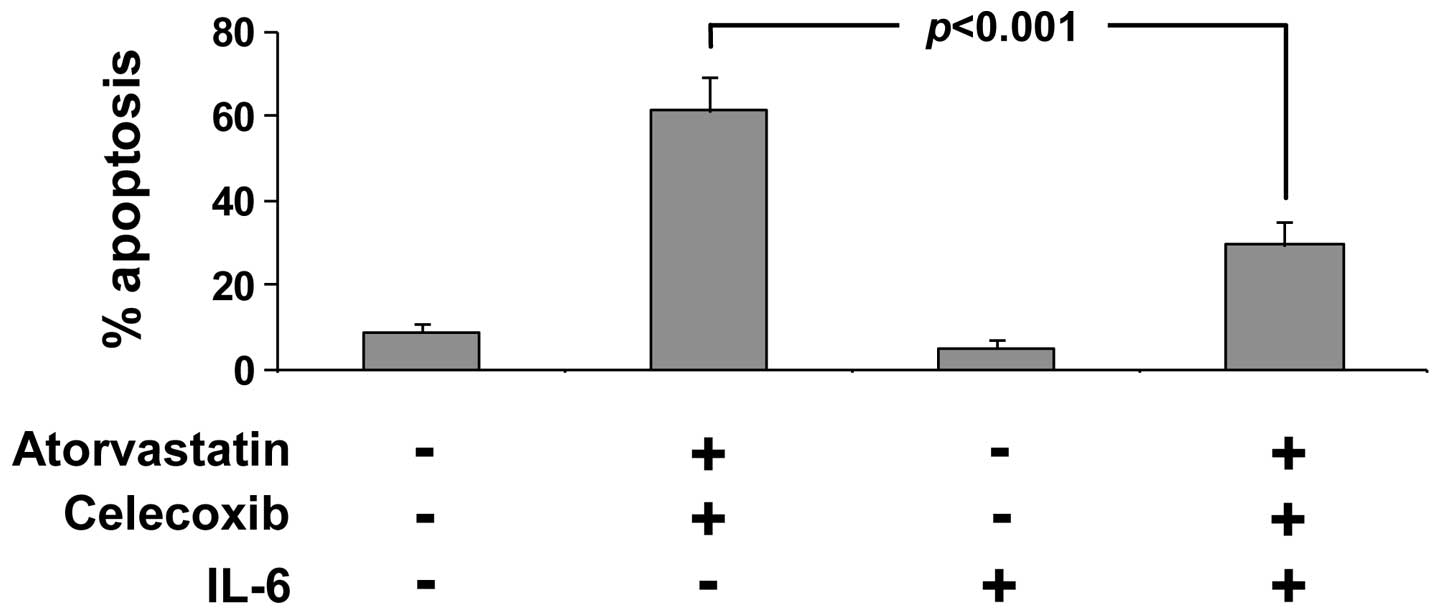
alone (Fig. 2). To further evaluate
the role of IL-6 in apoptosis induction by atorvastatin and
celecoxib, we determined whether addition of recombinant IL-6 may
abrogate the stimulatory effect of atorvastatin and celecoxib on
apoptosis. In these experiments, LNCaP cells were treated with a
combination of atorvastatin and celecoxib in the presence or
absence of recombinant IL-6. We found that addition of recombinant
IL-6 significantly decreased the combined effect of atorvastatin
and celecoxib on apoptosis in the LNCaP cells cultured in AD medium
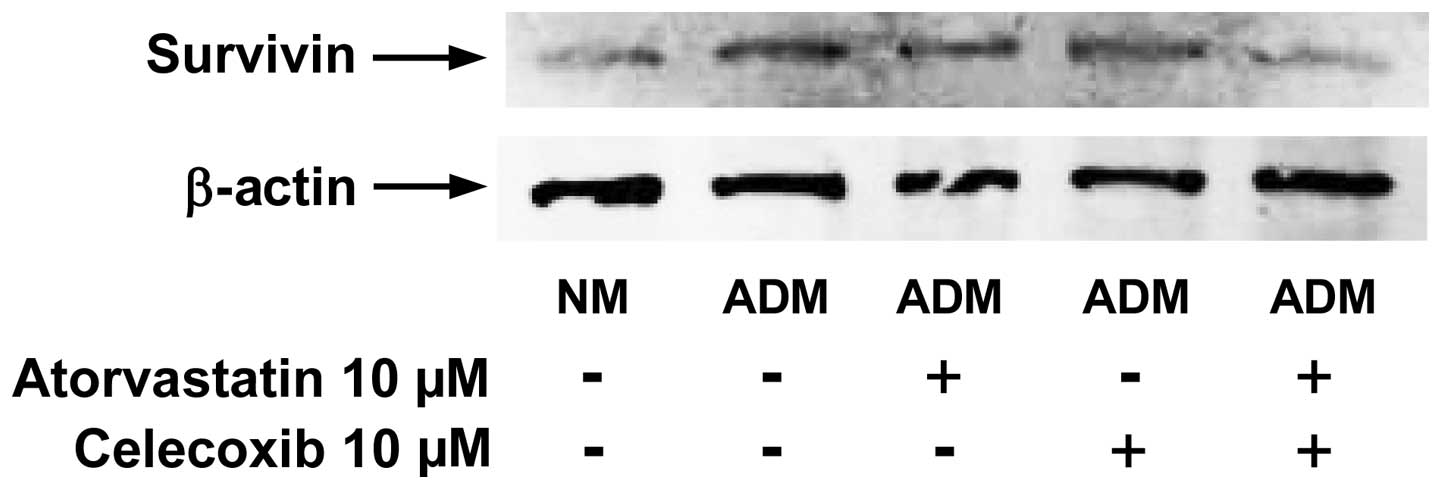
(Fig. 3). In additional
experiments, the effects of atorvastatin and/or celecoxib on the
level of survivin were determined using western blot analysis. We
found that culturing the LNCaP cells in AD medium increased the
level of survivin, and treatment of the cells with a combination of
atorvastatin and celecoxib strongly inhibited the increase in the
level of this protein (Fig. 4).
Effect of atorvastatin and celecoxib
treatment on the level of IL-6 and survivin in LNCaP tumors in
castrated mice as they progress from a state of androgen-dependence
to androgen-independence
To assess the effect of atorvastatin and celecoxib
in vivo, we studied the effect of each agent alone and in
combination on LNCaP xenograft tumors in SCID mice. We found that
treatment with a combination of atorvastatin and celecoxib strongly
inhibited the progression of androgen-dependent LNCaP tumors to
androgen independence when compared to the vehicle treatment only
or either agent alone (Fig.
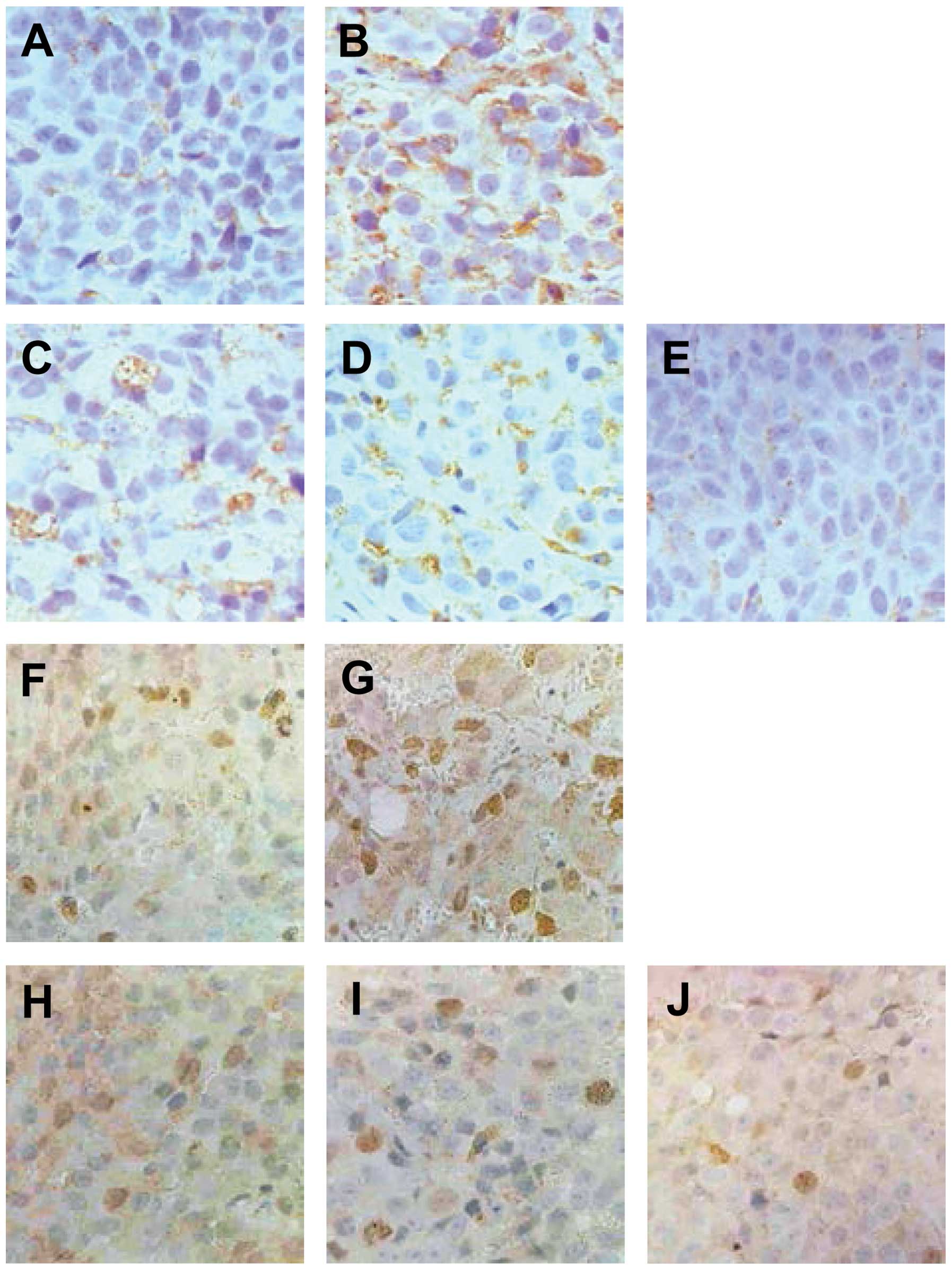
5)(18). In the present study,
the levels of IL-6 and survivin in LNCaP tumors as they became
androgen-independent were determined using immunohistochemistry. We
found that androgen-dependent LNCaP tumors (before castration) had
low levels of IL-6 (Fig. 6A) and
survivin (Fig. 6F). Increased
levels of IL-6 (Fig. 6B) and
survivin (Fig. 6G) were observed in
androgen-independent tumors (42 days after castration). Treatment
of the mice with atorvastatin alone caused a modest decrease in
IL-6 (Fig. 6C) and survivin
(Fig. 6H). Treatment of the mice
with celecoxib alone also resulted in a moderate decrease in IL-6
(Fig. 6D) and survivin (Fig. 6I). However, treatment with a
combination of celecoxib and atorvastatin resulted in a much
stronger inhibition of the increased level of IL-6 (Fig. 6E) and survivin (Fig. 6J) in LNCaP tumors of the castrated
mice.
Discussion
In previous studies, we found that administration of
atorvastatin and celecoxib in combination had a strong inhibitory
effect on the progression of androgen-dependent LNCaP tumors to
androgen-independence in castrated SCID mice, and combined drug
treatment also inhibited the growth of androgen-independent
prostate cancer PC-3 tumors (18,19).
In the present study, we demonstrated that atorvastatin and
celecoxib in combination strongly inhibited the formation of IL-6
in LNCaP cells grown in androgen-deficient medium as well as in
LNCaP tumors as they became androgen-independent in castrated SCID
mice. IL-6 is a pleiotropic cytokine originally identified as a
regulator of immune and inflammatory responses (32), and evidence has been accumulating
that IL-6 may also play an important role in prostate cancer
progression to an androgen-independent state (24,25).
Increased serum levels of IL-6 in prostate cancer patients were
found to be associated with androgen-independence and metastatic
disease (33,34), and overexpression of IL-6 was
associated with protection of LNCaP cells from apoptosis during
androgen depletion (26). Recent
studies have shown that IL-6 can activate AR signaling in the
absence of androgen (21–23).
In an in vitro study, we found that the level
of IL-6 in LNCaP cells was increased after the cells were cultured
in androgen-depleted medium. During androgen deprivation therapy,
survival and proliferation of prostate cancer cells in the absence
of androgen can occur and are important during the development of
androgen-independence. Since IL-6 was shown to activate AR
signaling (21–23), increased levels of IL-6 during
androgen deprivation may enhance the survival and proliferation of
prostate cancer cells. In the present study, we found that a
combination of atorvastatin and celecoxib inhibited growth and
stimulated apoptosis in LNCaP cells cultured in androgen-depleted
(AD) medium, and their effects were associated with a decrease in
IL-6 levels. Moreover, addition of recombinant IL-6 partially
abrogated the effect of atorvastatin and celecoxib on apoptosis
stimulation in LNCaP cells indicating that a decreased IL-6 level
is important for the effect of atorvastatin and celecoxib. In
vivo, we found that IL-6 expression was increased in
androgen-independent LNCaP tumors. Treatment of the mice with
atorvastatin or celecoxib alone resulted in a decrease in the level
of IL-6 in the androgen-independent LNCaP tumors. The combination
of atorvastatin and celecoxib caused a stronger inhibitory effect
on the IL-6 level than either drug alone. The present study
indicates that progression of androgen-dependent LNCaP tumors to
androgen independence is associated with an increase in IL-6 and
that treatment with atorvastatin and celecoxib inhibited the
increased tumor level of IL-6.
Survivin is a member of the inhibitor of apoptosis
(IAP) gene family, and is involved in the control of mitotic
progression and inhibition of apoptosis (35). In prostate cancer, overexpression of
survivin has been associated with increased cancer aggressiveness
and reduced patient survival (36).
Survivin is a downstream target of the signal transducer and
activator of transcription 3 (Stat3) that can be activated by IL-6
in prostate cancer (21,26,37).
In the present study, we found that treatment with atorvastatin and
celecoxib in combination markedly decreased the levels of IL-6 and
survivin in cultured LNCaP cells in AD medium as well as in LNCaP
xenograft tumors in castrated SCID mice. Our studies indicate that
the effects of atorvastatin in combination with celecoxib on
prostate cancer LNCaP cells are associated with inhibition of the
IL-6 signaling pathway.
In summary, we demonstrated in the present study
that atorvastatin and celecoxib in combination strongly decreased
the levels of IL-6 and survivin in cultured LNCaP cells grown in AD
medium and in LNCaP xenograft tumors in castrated SCID mice.
Addition of IL-6 partially abrogated the apoptosis-inducing effect
of atorvastatin and celecoxib in LNCaP cells. This result indicates
that the effect of a combined treatment of atorvastatin and
celecoxib on apoptosis is mediated, at least in part, by inhibition
of the formation of IL-6. The present study suggests that the IL-6
signaling pathway may be a useful target for the prevention of
androgen-dependent prostate cancer progression to
androgen-independence.
Acknowledgements
The present study was supported by funds from the
Cancer Institute of New Jersey (CCSG P30-CA072720 R.S.D.), the
Chinese National Science Foundation grants (nos. 81272452 and
21272043), and the Foundation for Distinguished Young Talent in
High Education of Guangdong (LYM11055). The authors thank Ms.
Annette Dionisio for her excellent help in the preparation of this
manuscript.
References
|
1
|
Loblaw DA, Virgo KS, Nam R, Somerfield MR,
Ben-Josef E, Mendelson DS, Middleton R, Sharp SA, Smith TJ, Talcott
J, Taplin M, Vogelzang NJ, Wade JL III, Bennett CL and Scher HI;
American Society of Clinical Oncology. Initial hormonal management
of androgen-sensitive metastatic, recurrent, or progressive
prostate cancer: 2006 update of an American Society of Clinical
Oncology practice guideline. J Clin Oncol. 25:1596–1605. 2007.
View Article : Google Scholar
|
|
2
|
Devlin HL and Mudryj M: Progression of
prostate cancer: multiple pathways to androgen independence. Cancer
Lett. 274:177–186. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
So A, Gleave M, Hurtado-Col A and Nelson
C: Mechanisms of the development of androgen independence in
prostate cancer. World J Urol. 23:1–9. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Schröder FH: Progress in understanding
androgen-independent prostate cancer (AIPC): a review of potential
endocrine-mediated mechanisms. Eur Urol. 53:1129–1137. 2008.
|
|
5
|
Chi KN, Bjartell A, Dearnaley D, Saad F,
Schröder FH, Sternberg C, Tombal B and Visakorpi T:
Castration-resistant prostate cancer: from new pathophysiology to
new treatment targets. Eur Urol. 56:594–605. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Pilat MJ, Kamradt JM and Pienta KJ:
Hormone resistance in prostate cancer. Cancer Metastasis Rev.
17:373–381. 1999. View Article : Google Scholar
|
|
7
|
Stein MN, Goodin S and Dipaola RS:
Abiraterone in prostate cancer: a new angle to an old problem. Clin
Cancer Res. 18:1848–1854. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Seruga B and Tannock IF:
Chemotherapy-based treatment for castration-resistant prostate
cancer. J Clin Oncol. 29:3686–3694. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Farnier M and Davignon J: Current and
future treatment of hyperlipidemia: the role of statins. Am J
Cardiol. 82:3J–10J. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Malhotra HS and Goa KL: Atorvastatin: an
updated review of its pharmacological properties and use in
dyslipidaemia. Drugs. 61:1835–1881. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Jacobs EJ, Rodriguez C, Bain EB, Wang Y,
Thun MJ and Calle EE: Cholesterol-lowering drugs and advanced
prostate cancer incidence in a large U.S. cohort. Cancer Epidemiol
Biomarkers Prev. 16:2213–2217. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Flick ED, Habel LA, Chan KA, et al: Statin
use and risk of prostate cancer in the California Men’s Health
Study cohort. Cancer Epidemiol Biomarkers Prev. 16:2218–2225.
2007.
|
|
13
|
Hamilton RJ, Banez LL, Aronson WJ, Terris
MK, Platz EA, Kane CJ, Presti JC Jr, Amling CL and Freedland SJ:
Statin medication use and the risk of biochemical recurrence after
radical prostatectomy: results from the Shared Equal Access
Regional Cancer Hospital (SEARCH) Database. Cancer. 116:3389–3398.
2010. View Article : Google Scholar
|
|
14
|
Abedinpour P, Baron VT, Welsh J and
Borgström P: Regression of prostate tumors upon combination of
hormone ablation therapy and celecoxib in vivo. Prostate.
71:813–823. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Dandekar DS, Lopez M, Carey RI and
Lokeshwar BL: Cyclooxygenase-2 inhibitor celecoxib augments
chemotherapeutic drug-induced apoptosis by enhancing activation of
caspase-3 and -9 in prostate cancer cells. Int J Cancer.
115:484–492. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Harris RE: Cyclooxygenase-2 (cox-2)
blockade in the chemoprevention of cancers of the colon, breast,
prostate, and lung. Inflammopharmacology. 17:55–67. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Reddy BS, Wang CX, Kong AN, Khor TO, Zheng
X, Steele VE, Kopelovich L and Rao CV: Prevention of
azoxymethane-induced colon cancer by combination of low doses of
atorvastatin, aspirin, and celecoxib in F 344 rats. Cancer Res.
66:4542–4546. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Zheng X, Cui XX, Gao Z, Zhao Y, Lin Y,
Shih WJ, Huang MT, Liu Y, Rabson A, Reddy B, Yang CS and Conney AH:
Atorvastatin and celecoxib in combination inhibits the progression
of androgen-dependent LNCaP xenograft prostate tumors to androgen
independence. Cancer Prev Res. 3:114–124. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Zheng X, Cui XX, Avila GE, Huang MT, Liu
Y, Patel J, Kong AN, Paulino R, Shih WJ, Lin Y, Rabson AB, Reddy BS
and Conney AH: Atorvastatin and celecoxib inhibit prostate PC-3
tumors in immunodeficient mice. Clin Cancer Res. 13:5480–5487.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hammacher A, Thompson EW and Williams ED:
Interleukin-6 is a potent inducer of S100P, which is up-regulated
in androgen-refractory and metastatic prostate cancer. Int J
Biochem Cell Biol. 37:442–450. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Chen T, Wang LH and Farrar WL: Interleukin
6 activates androgen receptor-mediated gene expression through a
signal transducer and activator of transcription 3-dependent
pathway in LNCaP prostate cancer cells. Cancer Res. 60:2132–2135.
2000.
|
|
22
|
Kim O, Jiang T, Xie Y, Guo Z, Chen H and
Qiu Y: Synergism of cytoplasmic kinases in IL6-induced
ligand-independent activation of androgen receptor in prostate
cancer cells. Oncogene. 23:1838–1844. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gazi MH, Gong A, Donkena KV and Young CY:
Sodium selenite inhibits interleukin-6-mediated androgen receptor
activation in prostate cancer cells via upregulation of
c-Jun. Clin Chim Acta. 380:145–150. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Smith PC, Hobisch A, Lin DL, Culig Z and
Keller ET: Interleukin-6 and prostate cancer progression. Cytokine
Growth Factor Rev. 12:33–40. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Malinowska K, Neuwirt H, Cavarretta IT,
Bektic J, Steiner H, Dietrich H, Moser PL, Fuchs D, Hobisch A and
Culig Z: Interleukin-6 stimulation of growth of prostate cancer in
vitro and in vivo through activation of the androgen receptor.
Endocr Relat Cancer. 16:155–169. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lee SO, Lou W, Johnson CS, Trump DL and
Gao AC: Interleukin-6 protects LNCaP cells from apoptosis induced
by androgen deprivation through the Stat3 pathway. Prostate.
60:178–186. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Wei X, Du ZY, Cui XX, Verano M, Mo RQ,
Tang ZK, Conney AH, Zheng X and Zhang K: Effects of cyclohexanone
analogues of curcumin on growth, apoptosis and NF-κB activity in
PC-3 human prostate cancer cells. Oncol Lett. 4:279–284. 2012.
|
|
28
|
Zheng X, Chang RL, Cui XX, Avila GE,
Hebbar V, Garzotto M, Shih WJ, Lin Y, Lu SE, Rabson AB, Kong AN and
Conney AH: Effects of 12-O-tetradecanoylphorbol-13-acetate
(TPA) in combination with paclitaxel (Taxol) on prostate Cancer
LNCaP cells cultured in vitro or grown as xenograft tumors in
immunodeficient mice. Clin Cancer Res. 12:3444–3451. 2006.
|
|
29
|
Zheng X, Cui XX, Huang MT, Liu Y, Wagner
GC, Lin Y, Shih WJ, Lee MJ, Yang CS and Conney AH: Inhibition of
progression of androgen-dependent prostate LNCaP tumors to androgen
independence in SCID mice by oral caffeine and voluntary exercise.
Nutr Cancer. 64:1029–1037. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Hsu JC: Comparisons: Theory and Methods.
Chapman and Hall; New York, NY: 1996, View Article : Google Scholar
|
|
31
|
Zhao L, Wientjes MG and Au JL: Evaluation
of combination chemotherapy: integration of nonlinear regression,
curve shift, isobologram, and combination index analyses. Clin
Cancer Res. 10:7994–8004. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Hirano T: The biology of interleukin-6.
Chem Immunol. 51:153–180. 1992. View Article : Google Scholar
|
|
33
|
Michalaki V, Syrigos K, Charles P and
Waxman J: Serum levels of IL-6 and TNF-α correlate with
clinicopathological features and patient survival in patients with
prostate cancer. Br J Cancer. 90:2312–2316. 2004.
|
|
34
|
Nakashima J, Tachibana M, Horiguchi Y, Oya
M, Ohigashi T, Asakura H and Murai M: Serum interleukin 6 as a
prognostic factor in patients with prostate cancer. Clin Cancer
Res. 6:2702–2706. 2000.PubMed/NCBI
|
|
35
|
Altieri DC: Targeting survivin in cancer.
Cancer Lett. 332:225–228. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Shariat SF, Lotan Y, Saboorian H, Khoddami
SM, Roehrborn CG, Slawin KM and Ashfaq R: Survivin expression is
associated with features of biologically aggressive prostate
carcinoma. Cancer. 100:751–757. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Costantino L and Barlocco D: STAT 3 as a
target for cancer drug discovery. Curr Med Chem. 15:834–843. 2008.
View Article : Google Scholar : PubMed/NCBI
|