Introduction
Activated leukocyte cell adhesion molecule (ALCAM),
also designated CD166, is a member of the immunoglobulin
superfamily. ALCAM is a cell adhesion molecule expressed by
epithelial cells in several organs and is involved in
embryogenesis, angiogenesis, hematopoiesis (1), immune response (2) and, of course, cell adhesion (3). Cell adhesion molecules can be involved
in tumor cell-tumor cell adhesion, tumor cell-endothelial cell
adhesion and tumor cell-matrix adhesion, which are all essential
during primary tumor formation or metastasis at different
times.
The initial studies that identified a role for ALCAM
in human malignancies were performed in melanoma (4,5). Over
the last decade, alterations in ALCAM expression have been
described in several other malignancies including bladder (6), colorectal (7), esophageal squamous cell (8), pancreatic (9), oral squamous cell (10) and ovarian cancer (11), neuroblastoma (12), prostate (13) and breast cancer (14,15).
These data suggest that ALCAM expression is increased in some
tumors and downregulated in others. An association between high
ALCAM expression and unfavorable prognosis has been shown for
colorectal (7), pancreatic
(9) and esophageal squamous cell
cancer (8), and neuroblastoma
(12). As a membrane protein, ALCAM
also represents a potential target for therapy, which has already
been successfully targeted by human recombinant single-chain
antibody in breast cancer cells (16).
For breast cancer, ALCAM expression data are
contradictory. Some studies revealed an increased ALCAM expression
to be associated with poor prognosis (15,17) or
lymph node metastasis and local recurrence (18), while others found a decreased ALCAM
expression to be linked to a poorer clinical course (14,19,20).
One explanation for these conflicting data potentially lies in the
relatively small number of breast cancer cases included in those
studies, ranging from 56 to 347 (14,15,17,21).
The aim of the present study was to clarify the prevalence and
prognostic role of ALCAM expression in breast cancer using a
pre-existing large-scale tissue microarray (TMA) including more
than 2,000 breast cancer samples. Our data demonstrate a strong
link between reduced membranous ALCAM expression and adverse
phenotype and poor prognosis in breast cancer.
Materials and methods
Breast cancer TMA
The pre-existing TMA used for the purpose of the
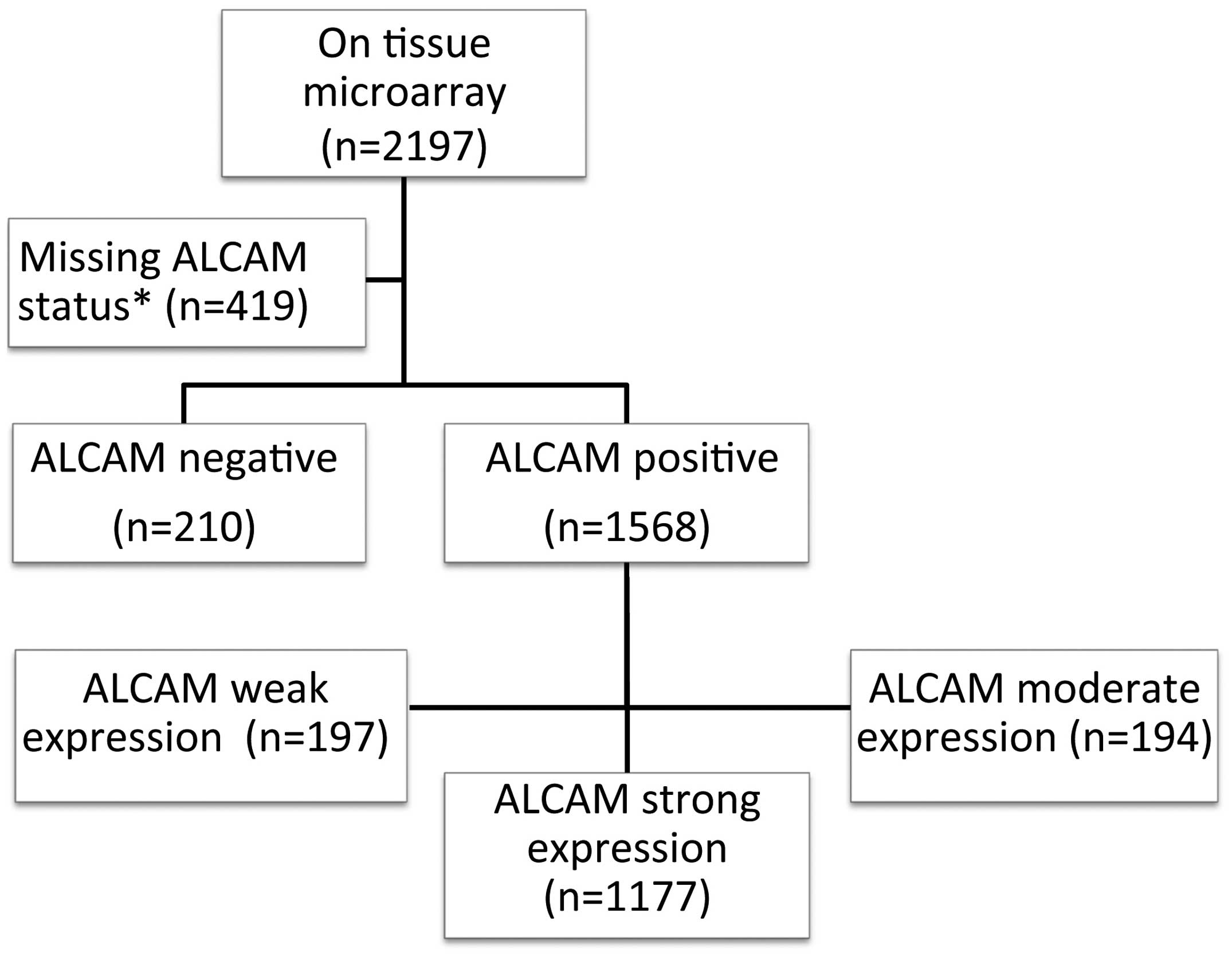
present study has been described in detail previously (22). In brief, the TMA contained a total
of 2,197 human breast cancer samples from paraffin-embedded tissue
specimens fixed in 4% neutral buffered formalin. The median patient
age was 62 years (range, 26–101). The use of the specimens and data
for research purposes was approved by the local Ethics Committee of
the University of Basel. Survival data were either obtained from
the cancer registry of Basel or collected from the patient
attending physicians. At the end of the present study, there were
2,194 patients with overall survival data (710 patients with, and
1,484 without event) and 943 with disease-specific data (204
patients with, and 739 without event) (Fig. 1). The mean follow-up time was 68
months (range, 1–176). Tumor size and nodal status were obtained
from the primary pathology reports. All slides from the tumors were
reviewed by specialized pathologists to define the histologic grade
according to Elston and Ellis (23)
and the tumor type according to the WHO classification (WHO 2012).
Four micrometer sections of the TMA blocks were transferred to an
adhesive-coated slide system (Instrumedics Inc., Hackensack, NJ,
USA) for immunohistochemical analyses. Evaluation of ALCAM
expression status was in accordance with the reporting
recommendations for tumor marker prognostic studies (REMARK)
guidelines (24).
Immunohistochemistry (IHC)
Freshly cut TMA sections were stained on one day in
a single experiment. High-temperature pretreatment of slides was
carried out in an autoclave in citrate buffer, pH 7.8 for 5 min.
Immunostaining for ALCAM was performed using a monoclonal antibody
(clone: MOG/07, 1:450; Novocastra). The EnVision system (Dako) was
used to visualize the immunostaining. Tissue with known positivity
was used as positive control and tonsil lymphocytes were used as
negative controls. All samples were evaluated by one of the authors
(E.B.). The staining intensity (scored on a scale of 0 to 3+) and
the proportion of positive tumor cells was recorded for each tissue
spot. Only membranous staining was evaluated since cytoplasmic
staining, if present, was always linked with stronger membranous
staining. Based on these values, a final IHC result was calculated
according to the following criteria: negative, in case of no
staining at all, and positive, subclassified as weak, moderate and
strong (weak, 1+ staining intensity in ≤70% positive tumor cells or
2+ staining intensity in ≤30% positive tumor cells; moderate, 1+
staining intensity in >70% tumor cells, 2+ in >30% but ≤70%
positive tumor cells or 3+ in ≤30% positive tumor cells; strong, 2+
>70% or 3+ >30% positive tumor cells). Data on the
immunohistochemical expression of Ki67, ER and PR were available
from previous studies (22,25). In these studies, the Allred score
was utilized for the evaluation of ER/PR staining. The percentage
of Ki67-positive tumor cell nuclei was registered as Ki67 labeling
index (LI).
Statistical analysis
Contingency table analysis and Chi-square test were
used to study the relationship between IHC results and
clinicopathological variables. Kaplan-Meier plots were used to
estimate disease-specific and overall survival and the statistical
significance was determined by the log-rank test. Cox proportional
hazard model with stepwise selection of the covariates was used to
determine the parameters with greatest influence on patient
survival. In exploratory analysis, p-values <0.05 were
considered to indicate a statistically significant difference.
Results
ALCAM expression
ALCAM immunostaining was interpretable in 1,778
(80.9%) of the 2,197 arrayed tissue spots on the TMA. Analysis
failures were either due to the absence of tissue on the TMA or
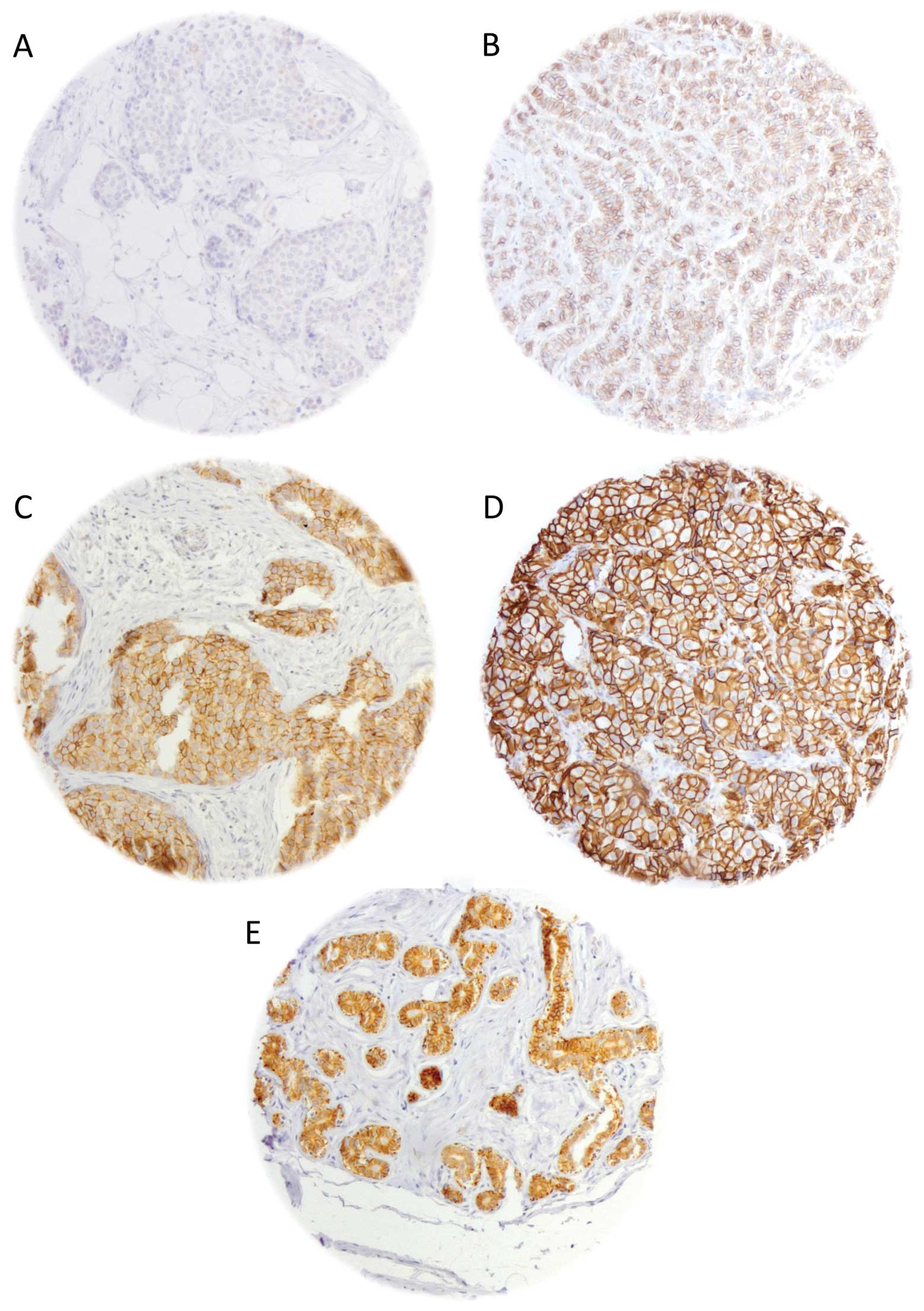
lack of unequivocal tumor cells in the arrayed sample. ALCAM
immunostaining always showed strong membrane predominance in our
tissues. Although varying degree of cytoplasmic staining was
sometimes observed, this was always associated with a much higher
staining level at the membranes. Membranous ALCAM staining was
observed in 1,568 (88.2%) of the informative cases. Staining was
considered weak in 197 (11.1%), moderate in 194 (10.9%) and strong
in 1,177 (66.2%) tumors. ALCAM immunostaining was absent in 210
(11.8%) cases. Representative images of ALCAM staining in breast
cancers are shown in Fig. 2.
ALCAM expression and tumor phenotype
ALCAM staining levels were comparable (60–90% with
strong staining) in most different histological subtypes except
from medullary cancers, which showed a significantly lower fraction
of strongly ALCAM-positive tumors [36%, as compared to 66% in
ductal carcinomas/invasive cancer of no special type (NST); WHO
2012] (p<0.0001). Reduced ALCAM staining was significantly
associated with advanced tumor size (p=0.0017) and unfavorable
tumor grade (p<0.0001). ALCAM staining levels were unrelated to
nodal status (p=0.098). In ductal carcinomas (NST), the largest
histologically defined subgroup, the associations with tumor
phenotype were similar; loss of ALCAM expression was significantly
linked to advanced tumor size (p=0.0015) and higher tumor grade
(p<0.0001). No significant association was found between ALCAM
staining levels and nodal status in the ductal (NST) subgroup
(p=0.045).
Cell proliferation was previously determined
immunohistochemically by using the Ki67 LI (22). An inverse relationship was found
between ALCAM staining and cell proliferation; the average Ki67 LI
increased from 26.3% in 1,011 cancers with strong ALCAM staining to
33.1% in 181 tumors lacking detectable ALCAM expression
(p<0.0001; Table I). Reduced
ALCAM immunostaining was further linked to negative ER and PR
status (p<0.0001 each). All results are summarized in Table II.
 | Table ICorrelation between ALCAM expression
levels and Ki67 LI. |
Table I
Correlation between ALCAM expression
levels and Ki67 LI.
| ALCAM score | n | Ki67 LI (mean) | P-value |
|---|
| Negative | 181 | 33.1 | <0.0001 |
| Weak | 170 | 30.1 | |
| Moderate | 160 | 27.5 | |
| Strong | 1,011 | 26.3 | |
| Table IIPathological characteristics of the
analyzed breast cancers included in the TMA in correlation with the
ALCAM IHC results. |
Table II
Pathological characteristics of the
analyzed breast cancers included in the TMA in correlation with the
ALCAM IHC results.
| ALCAM IHC
results |
|---|
|
|
|---|
| N (analyzable) | Negative (%) | Weak (%) | Moderate (%) | Strong (%) | P-value |
|---|
| Histology | | | | | | <0.0001b |
| All cancers | 1,778 | 11.8 | 11.1 | 10.9 | 66.2 | |
| Ductal
carcinomaa | 1,259 | 11.76 | 10.48 | 11.28 | 66.48 | |
| Lobular
carcinoma | 236 | 7.2 | 10.59 | 12.71 | 69.49 | |
| Medullary
carcinoma | 47 | 40.43 | 14.89 | 8.51 | 36.17 | |
| Tubular
carcinoma | 44 | 4.55 | 4.55 | 2.27 | 88.64 | |
| Mucinous
carcinoma | 51 | 7.84 | 23.53 | 7.84 | 60.78 | |
| Other rare
types | 141 | 13.48 | 14.18 | 9.22 | 63.12 | |
| pT Category | | | | | | 0.0017 |
| pT1 | 614 | 8.63 | 9.61 | 9.93 | 71.82 | |
| pT2 | 852 | 13.38 | 12.44 | 10.21 | 63.97 | |
| pT3 | 100 | 13 | 10 | 9 | 68 | |
| pT4 | 204 | 13.73 | 10.78 | 18.14 | 57.35 | |
| pN Category | | | | | | 0.098 |
| pN0 | 744 | 12.1 | 12.63 | 10.35 | 64.92 | |
| pN1 | 637 | 10.83 | 9.89 | 11.62 | 67.66 | |
| pN2 | 97 | 19.59 | 11.34 | 14.43 | 54.64 | |
| Histological
gradec | | | | | | <0.0001 |
| G1 | 418 | 5.98 | 11 | 10.77 | 72.25 | |
| G2 | 684 | 8.04 | 9.5 | 10.53 | 71.93 | |
| G3 | 553 | 20.43 | 13.56 | 11.03 | 54.97 | |
| ER status | | | | | | <0.0001 |
| Negative | 392 | 26.5 | 14.5 | 7.4 | 51.5 | |
| Positive | 1,303 | 7.1 | 10.1 | 12.0 | 70.8 | |
| PR status | | | | | | <0.0001 |
| Negative | 1,070 | 14.2 | 12.6 | 10.2 | 63.0 | |
| Positive | 571 | 6.7 | 8.6 | 12.3 | 71.5 | |
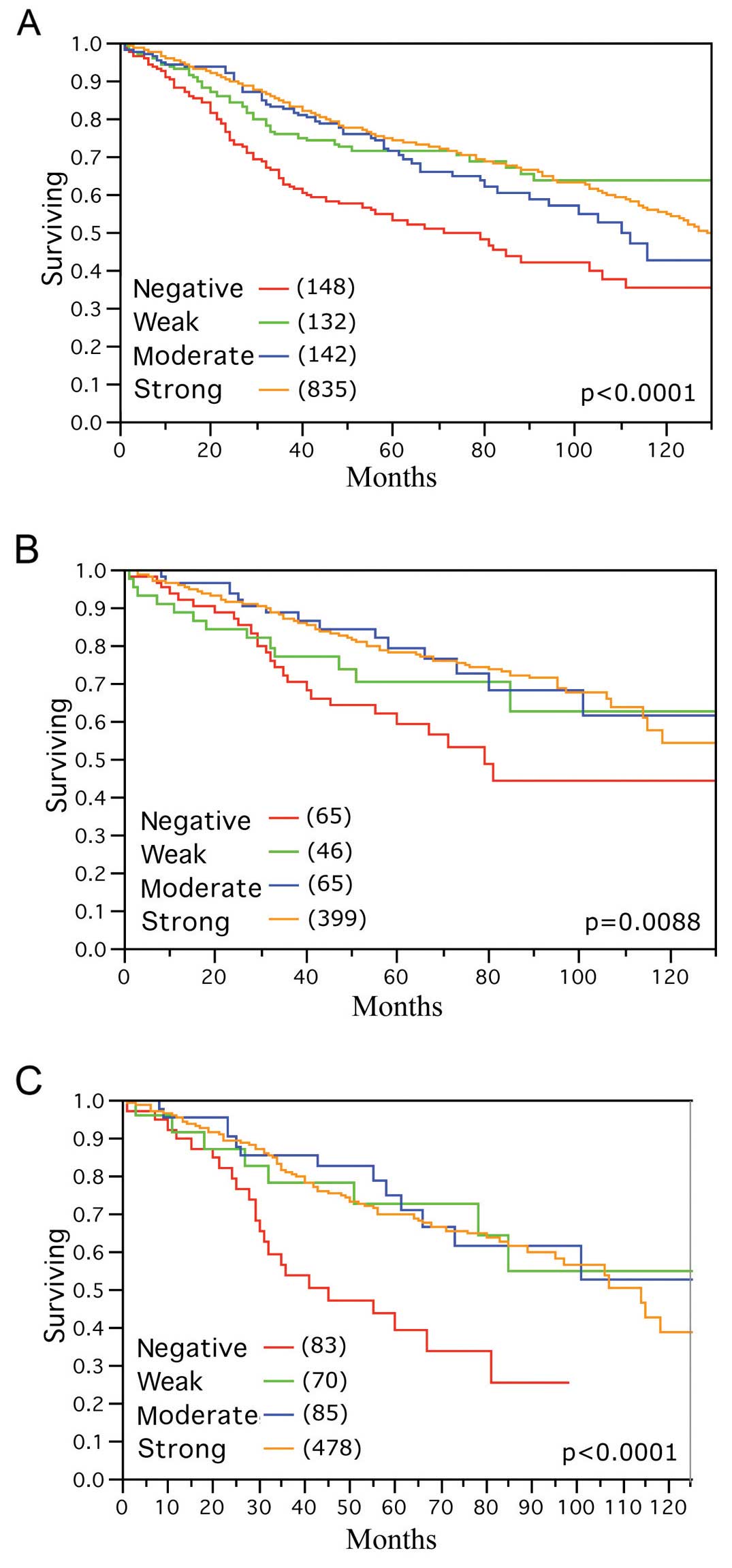
ALCAM expression as prognostic factor for
survival
Survival analysis revealed a highly significant
relationship between loss of ALCAM expression and poor overall
(p<0.0001; Fig. 3A) as well as
disease-specific patient survival (p=0.0088; Fig. 3B). This association also held true
in the subset of nodal positive breast cancers (p<0.0001;
Fig. 3C). An additional analysis in
a subset of 202 breast cancer patients who had received tamoxifen
monotherapy revealed no significant association between ALCAM
expression and survival data (p=0.2447; data not shown). Separate
analyses were also performed for subgroups with alternative
treatment information. In the subgroup of 63 breast cancer patients
who were treated by chemotherapy alone, the relationship between
ALCAM expression and outcome was retained (p=0.0212; data not
shown). In the 69 patients with combined treatment of chemotherapy
and tamoxifen, there was no significant impact of ALCAM expression
on survival (p=0.2486; data not shown).
A multivariate analysis including tumor size, nodal
status and histological grade did not suggest that ALCAM expression
is an independent prognostic marker in our patient cohort (Table III).
| Table IIICOX proportional hazard multivariate
analysis (tumor specific). |
Table III
COX proportional hazard multivariate
analysis (tumor specific).
| Disease-specific
survival |
|---|
|
|
|---|
| HR (95% CI) | P-value |
|---|
| ALCAM
expression | | 0.3349 |
| Negative vs.
weak | 1.4 (1.0–2.1) | |
| Weak vs.
moderate | 0.9 (0.4–1.5) | |
| Moderate vs.
strong | 0.9 (0.5–1.3) | |
| Size (pT) | | 0.008 |
| pT1 vs. pT2 | 0.8 (0.6–1.2) | |
| pT2 vs. pT3 | 1.0 (0.7–1.4) | |
| pT3 vs. pT4 | 0.7 (0.3–1.1) | |
| Nodal status | | <0.0001 |
| pN0 vs. pN1 | 0.3 (0.2–0.4) | |
| pN1 vs. pN2 | 1.0 (0.8–1.3) | |
| Grade | | <0.0001 |
| G1 vs. G2 | 0.6 (0.4–0.9) | |
| G2 vs. G3 | 0.8 (0.6–1.1) | |
Discussion
In the present study, more than 1,700 breast cancers
were successfully analyzed for ALCAM expression. The results
suggest that high ALCAM expression is a common feature of normal
and cancerous breast epithelial cells and that its loss is linked
to tumor progression, rapid cell proliferation and shortened
survival.
A comparison with normal breast tissue revealed that
ALCAM expression is high in normal breast epithelium but is reduced
or lost in a fraction of cancers. This observation is in line with
earlier data from King et al (14) and Kilic et al (26) describing that high levels of ALCAM
expression are typically seen in normal breast epithelium. These
findings suggest that high levels of ALCAM expression represent a
physiological situation. ALCAM expression was found to be retained
at high frequency and high levels in breast cancer in the present
study. A total of 88.2% of our cancers had detectable expression
including 66.2% with ‘strong’ expression according to our scoring
criteria. This high frequency is consistent with data from several
earlier studies. Burkhardt et al (15), for example, found 75%
ALCAM-expressing cancers among 160 analyzed cases. Ihnen et
al (27) showed that 95% of
their 162 breast cancers were ALCAM-positive, while Hein et
al (17) demonstrated 79%
ALCAM-expressing breast cancers in their cohort comprising 347
cases. Another study analyzing 84 cases found 96% of the tested
breast cancers to be ALCAM-positive (28).
In the present study, a significant association
between lost ALCAM expression and an adverse clinical course was
observed. This finding is in line with several of the earlier
studies analyzing ALCAM expression in breast cancer (14,19,20).
Based on the known function of ALCAM as a cell adhesion molecule,
it appears possible that loss of such a protein would result in
more adverse cancer cell behavior due to a facilitated tissue
infiltration, and, accordingly, a higher likelihood for developing
metastases. However, several other studies came to different
conclusions. For example, Piao et al (18) found high membranous ALCAM expression
to be statistically correlated with a worse clinical course and
high cytoplasmic staining with local recurrence. Hein et al
(17) found high ALCAM expression
linked to shorter overall survival compared to patients with
low/moderate ALCAM scores, while ALCAM-negative tumors had an
intermediate position. Burkhardt et al (15) reported that strong cytoplasmic ALCAM
expression was significantly associated with earlier disease
progression, while there was no correlation between membranous
ALCAM expression and clinicopathological data. Ihnen et al
(27) also failed to find an
association of ALCAM protein or mRNA expression with histological
type, grading or stage in a series of 162 breast cancers. It may be
that some of these contradictory data are due to the relatively
small patient cohorts analyzed, ranging from 56 to 347 (14,15,17,18,21,27).
The different methods used in those studies could be an additional
source explaining these conflicting results. For example, some
studies estimated levels of ALCAM using western blotting (26,27),
while others performed real-time PCR (14) or IHC (15,17,27–29).
A variable role of ALCAM expression in patient
prognosis depending on the therapies applied could also contribute
to variable results between studies evaluating the prognostic role
of ALCAM expression in breast cancer. A predictive role of ALCAM
expression has indeed been suggested. Ihnen et al (27) found high ALCAM mRNA expression to be
positively correlated with long overall survival in patients
treated with adjuvant chemotherapy in a series of 162 patients. In
contrast, patients with high ALCAM mRNA expression who did not
receive chemotherapy tended to have a poorer prognosis in their
study. In our patient cohort, the number of patients with complete
treatment information was quite limited. The small cohort with
treatment information did not enable us to show an unequivocal or
strong relationship between ALCAM expression and survival. Even in
the subgroup treated by chemotherapy alone, where the survival
differences reached statistical significance, the absolute
differences were only minimal.
Prediction of prognosis is of high relevance in
breast cancer. An increasing number of patients undergo prognostic
evaluation by multiparameter gene expression tests, such as
Oncotype DX™ (30,31). These tests are considered to be able
to reduce unnecessary adjuvant chemotherapy, Oncotype DX™, for
example, by evaluating the expression levels of 21 genes and
thereby generating a recurrence score of low, intermediate or high
risk, which supports the decision on giving adjuvant chemotherapy
or not. Data have shown that the recurrence score was low in 48% of
the first 20,050 tested patients and in this group there is
minimal, if any, benefit from adjuvant chemotherapy (32,33).
On the other hand, current knowledge indicates that approximately
up to 77% of breast cancer patients may be exposed to chemotherapy
toxicity and costs with little or no clinical benefit (34). Given the remaining ~30% of
‘unnecessary’ chemotherapies, these existing tests are still far
from ideal. It is highly likely that existing gene tests will soon
be replaced by next generation testing. Based on our data, ALCAM
expression analysis may be a component of future prognostic breast
cancer tests.
Another potential relevance of ALCAM expression in
breast cancer, is its membranous expression, which automatically
makes ALCAM a potential therapeutic target. Wiiger et al
(16) described a human recombinant
single-chain antibody targeting ALCAM that was able to inhibit
cancer cell invasion in vitro and in vivo tumor
growth. Furthermore, Roth et al (35) described an internalizing single
chain antibody that targets ALCAM in prostate cancer cells and
immunoliposomes using this antibody were developed in order to
deliver liposomal drugs to prostate cancer cells (35). These cell line experiments
illustrate that ALCAM may be of interest not only as a classical
membranous target structure for antibody therapy, but also as an
internalizing epitope for intracellular delivery of liposomal
drugs.
In summary, our data demonstrate that significant
levels of membranous ALCAM expression occur in most breast cancers.
This makes breast cancer a suitable target for anti-ALCAM therapies
once these become available. Moreover, reduced ALCAM expression was
strongly linked to adverse clinical features, making ALCAM a
candidate biomarker for next generation prognostic multigene panels
in breast cancer.
Acknowledgements
The authors acknowledge the technical support of
Christina Koop.
References
|
1
|
Ohneda O, Ohneda K, Arai F, et al: ALCAM
(CD166): its role in hematopoietic and endothelial development.
Blood. 98:2134–2142. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Masedunskas A, King JA, Tan F, et al:
Activated leukocyte cell adhesion molecule is a component of the
endothelial junction involved in transendothelial monocyte
migration. FEBS Lett. 580:2637–2645. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Swart GW: Activated leukocyte cell
adhesion molecule (CD166/ ALCAM): developmental and mechanistic
aspects of cell clustering and cell migration. Eur J Cell Biol.
81:313–321. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Degen WG, van Kempen LC, Gijzen EG, et al:
MEMD, a new cell adhesion molecule in metastasizing human melanoma
cell lines, is identical to ALCAM (activated leukocyte cell
adhesion molecule). Am J Pathol. 152:805–813. 1998.PubMed/NCBI
|
|
5
|
van Kempen LC, van den Oord JJ, van Muijen
GN, Weidle UH, Bloemers HP and Swart GW: Activated leukocyte cell
adhesion molecule/CD166, a marker of tumor progression in primary
malignant melanoma of the skin. Am J Pathol. 156:769–774.
2000.PubMed/NCBI
|
|
6
|
Tomita K, van Bokhoven A, Jansen C, et al:
Activated leukocyte cell adhesion molecule (ALCAM) expression is
associated with a poor prognosis for bladder cancer patients.
UroOncology. 3:121–129. 2003. View Article : Google Scholar
|
|
7
|
Weichert W, Knösel T, Bellach J, Dietel M
and Kristiansen G: ALCAM/CD166 is overexpressed in colorectal
carcinoma and correlates with shortened patient survival. J Clin
Pathol. 57:1160–1164. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Verma A, Shukla NK, Deo SV, Gupta SD and
Ralhan R: MEMD/ ALCAM: a potential marker for tumor invasion and
nodal metastasis in esophageal squamous cell carcinoma. Oncology.
68:462–470. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kahlert C, Weber H, Mogler C, et al:
Increased expression of ALCAM/CD166 in pancreatic cancer is an
independent prognostic marker for poor survival and early tumour
relapse. Br J Cancer. 101:457–464. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sawhney M, Matta A, Macha MA, et al:
Cytoplasmic accumulation of activated leukocyte cell adhesion
molecule is a predictor of disease progression and reduced survival
in oral cancer patients. Int J Cancer. 124:2098–2105. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mezzanzanica D, Fabbi M, Bagnoli M, et al:
Subcellular localization of activated leukocyte cell adhesion
molecule is a molecular predictor of survival in ovarian carcinoma
patients. Clin Cancer Res. 14:1726–1733. 2008. View Article : Google Scholar
|
|
12
|
Corrias MV, Gambini C, Gregorio A, et al:
Different subcellular localization of ALCAM molecules in
neuroblastoma: association with relapse. Cell Oncol. 32:77–86.
2010.PubMed/NCBI
|
|
13
|
Tomita K, van Bokhoven A, Jansen CF,
Bussemakers MJ and Schalken JA: Coordinate recruitment of
E-cadherin and ALCAM to cell-cell contacts by α-catenin. Biochem
Biophys Res Commun. 267:870–874. 2000.PubMed/NCBI
|
|
14
|
King JA, Ofori-Acquah SF, Stevens T,
Al-Mehdi AB, Fodstad O and Jiang WG: Activated leukocyte cell
adhesion molecule in breast cancer: prognostic indicator. Breast
Cancer Res. 6:R478–R487. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Burkhardt M, Mayordomo E, Winzer KJ, et
al: Cytoplasmic overexpression of ALCAM is prognostic of disease
progression in breast cancer. J Clin Pathol. 59:403–409. 2006.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Wiiger MT, Gehrken HB, Fodstad Ø,
Maelandsmo GM and Andersson Y: A novel human recombinant
single-chain antibody targeting CD166/ALCAM inhibits cancer cell
invasion in vitro and in vivo tumour growth. Cancer Immunol
Immunother. 59:1665–1674. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Hein S, Muller V, Kohler N, et al:
Biologic role of activated leukocyte cell adhesion molecule
overexpression in breast cancer cell lines and clinical tumor
tissue. Breast Cancer Res Treat. 129:347–360. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Piao D, Jiang T, Liu G, Wang B, Xu J and
Zhu A: Clinical implications of activated leukocyte cell adhesion
molecule expression in breast cancer. Mol Biol Rep. 39:661–668.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Davies S and Jiang WG: ALCAM, activated
leukocyte cell adhesion molecule, influences the aggressive nature
of breast cancer cells, a potential connection to bone metastasis.
Anti-cancer Res. 30:1163–1168. 2010.
|
|
20
|
Milde-Langosch K, Janke S, Wagner I, et
al: Role of Fra-2 in breast cancer: influence on tumor cell
invasion and motility. Breast Cancer Res Treat. 107:337–347. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Jezierska A, Matysiak W and Motyl T:
ALCAM/CD166 protects breast cancer cells against apoptosis and
autophagy. Med Sci Monit. 12:BR263–BR273. 2006.PubMed/NCBI
|
|
22
|
Ruiz C, Seibt S, Al Kuraya K, et al:
Tissue microarrays for comparing molecular features with
proliferation activity in breast cancer. Int J Cancer.
118:2190–2194. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Elston CW and Ellis IO: Pathological
prognostic factors in breast cancer. I The value of histological
grade in breast cancer: experience from a large study with
long-term follow-up. Histopathology. 19:403–410. 1991. View Article : Google Scholar
|
|
24
|
McShane LM, Altman DG, Sauerbrei W, Taube
SE, Gion M and Clark GM; Statistics Subcommittee of NCI-EORTC
Working Group on Cancer Diagnostics. REporting recommendations for
tumor MARKer prognostic studies (REMARK). Breast Cancer Res Treat.
100:229–235. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Al-Kuraya K, Schraml P, Torhorst J, et al:
Prognostic relevance of gene amplifications and coamplifications in
breast cancer. Cancer Res. 64:8534–8540. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kilic E, Milde-Langosch K, Müller V, Wirtz
R and Ihnen M: Expression of activated leukocyte cell adhesion
molecule in breast cancer. Predictability of the response to
taxane-free chemotherapy. Pathologe. 29(Suppl 2): S347–S352.
2008.(In German).
|
|
27
|
Ihnen M, Müller V, Wirtz RM, et al:
Predictive impact of activated leukocyte cell adhesion molecule
(ALCAM/CD166) in breast cancer. Breast Cancer Res Treat.
112:419–427. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Ihnen M, Köhler N, Kersten JF, et al:
Expression levels of activated leukocyte cell adhesion molecule
(ALCAM/CD166) in primary breast carcinoma and distant breast cancer
metastases. Dis Markers. 28:71–78. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
King JA, Tan F, Mbeunkui F, et al:
Mechanisms of transcriptional regulation and prognostic
significance of activated leukocyte cell adhesion molecule in
cancer. Mol Cancer. 9:2662010. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Paik S, Shak S, Tang G, et al: A multigene
assay to predict recurrence of tamoxifen-treated, node-negative
breast cancer. N Engl J Med. 351:2817–2826. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Glas AM, Floore A, Delahaye LJ, et al:
Converting a breast cancer microarray signature into a
high-throughput diagnostic test. BMC Genomics. 7:2782006.
View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Paik S, Tang G, Shak S, et al: Gene
expression and benefit of chemotherapy in women with node-negative,
estrogen receptor-positive breast cancer. J Clin Oncol.
24:3726–3734. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Sparano JA and Paik S: Development of the
21-gene assay and its application in clinical practice and clinical
trials. J Clin Oncol. 26:721–728. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Carlson JJ and Roth JA: The impact of the
Oncotype Dx breast cancer assay in clinical practice: a systematic
review and meta-analysis. Breast Cancer Res Treat. 141:13–22. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Roth A, Drummond DC, Conrad F, et al:
Anti-CD166 single chain antibody-mediated intracellular delivery of
liposomal drugs to prostate cancer cells. Mol Cancer Ther.
6:2737–2746. 2007. View Article : Google Scholar : PubMed/NCBI
|