Introduction
Hepatocellular carcinoma (HCC) is one of the most
common cancers worldwide, especially in Asia, with a high mortality
rate (1). It is challenging to
evaluate the prognosis of HCC patients. Based on molecular
profiling, several prognostic markers for HCC are used in the
clinic (2), but only a few genes
have been identified as useful.
Dual oxidase 1 (DUOX1) is a key phenotype of the
NADPH-oxidase (NOX) family, and the main function of this gene is
reactive oxygen species (ROS) production (3). DUOX1 is predominantly found in the
thyroid, where it is involved in the synthesis of thyroid hormones
(4). It is also highly expressed in
normal epithelial cells in the airway, pancreas, placenta,
prostate, testis and salivary gland (3,5).
Recent research indicates that DUOX1 may function as a selective
tumor-suppressor gene (TSG) during tumor initiation and
progression. In lung cancer cells, DUOX1 is frequently silenced by
its promoter hypermethylation (6).
In poorly differentiated follicular thyroid carcinoma, a high
expression of DUOX1 is associated with a reduced risk of death
(7). Moreover, our previous study
(8) found that DUOX1 expression is
also frequently decreased in most liver cancer cell lines and
primary HCC tissues compared to its expression in non-tumor
tissues, and silencing of DUOX1 gene expression is mediated by
promoter hypermethylation.
Reactive oxygen species (ROS), chemically reactive
molecules containing oxygen including oxygen ions and peroxides,
are the key mediators of cellular oxidative stress and redox
dysregulation involved in cancer initiation and progression
(9). For a long time, ROS were
considered oncogenic since they were implicated in cancer
progression and metastasis (9).
Increased ROS levels contribute to genetic instability and cancer
initiation and progression (10,11).
Thus, it is widely accepted that constitutively elevated levels of
cellular oxidative stress and dependence on mitogenic and
anti-apoptotic ROS signaling in cancer cells are involved in
carcinogenesis (12).
Paradoxically, apart from being involved in proliferative,
anti-apoptotic, metastatic and angiogenic signaling, ROS may also
exert cytotoxic and pro-apoptotic functions that would limit
tumorigenicity and malignant progression (13,14).
We previously reported that DUOX1 acts as a TSG to suppress tumor
cell growth through the induction of G2/M phase cell cycle arrest
and an increase in ROS generation (8). However, our previous research has not
identified associations between clinical outcomes and DUOX1
expression.
We hypothesized that DUOX1 could be used as a
pathological and prognostic biomarker for HCC patients. Therefore,
we investigated the expression of DUOX1 in a set of HCC specimens.
The results validated the relevance of DUOX1 expression to HCC
clinical outcomes.
Materials and methods
Patient cohort and specimens
Seventy-two patients (56 males and 16 females) from
Huashan Hospital (Shanghai, China) were included in this study. All
the patients underwent radical hepatic resection for HCC between
2008 and 2010. The age of the patients ranged from 16 to 84 years
[mean ± standard deviation (SD), 53.67±12.30 years]. The criteria
for radicality have been published (15). None of the patients in this study
received any preoperative chemotherapy or embolization therapy. The
tumor tissues and the adjacent non-tumor tissues were collected
from these patients above as frozen samples. The distance between
adjacent non-tumor tissue and tumor tissue boundary was 2 cm,
beyond which was regarded as distant normal tissue. The selected
tumor areas consisted of more than 80% tumor cells which was
confirmed by histologic examination. Classification of the tumor
stage using the Tumor-Node-Metastasis (TNM) stage was based on the
7th edition of the American Joint Committee on Cancer (AJCC) Cancer
Staging Manual (16).
Ethic statements
All patients were given informed consent for
obtaining the study specimens. Experiments and procedures were in
accordance with the Helsinki Declaration of 1975, and approved by
the Human Ethics Committee of Shanghai Fudan University.
Follow-up
Follow-up ended at death or June 1st, 2013,
whichever came first. Follow-up imaging was performed every 3–6
months for 2 years and then every 6–12 months. According to the
revised Response Evaluation Criteria in Solid Tumors (RECIST)
guidelines (version 1.1) (17), the
appearance of one or more new malignant lesions on multiphase
computed tomography (CT) scan or magnetic resonance (MR) imaging
denoted disease progression. Disease-free survival (DFS) was
defined as the time period from the date of surgical operation to
the first cancer recurrence (local or distant). Overall survival
(OAS) was calculated from the date of cancer resection to death or
the last contact.
RNA/DNA extraction and reverse
transcription
Total RNA and genomic DNA from the human tissue
samples were extracted using TRIzol reagent (Invitrogen) according
to the manufacturer's instructions, and their concentrations were
quantified by NanoDrop 1000 (NanoDrop, Wilmington, DE, USA). A
reverse transcription reaction was performed using 1 µg of
total RNA with the High Capacity cDNA Reverse Transcription kit
(SYBR qPCR RT Mix, FSQ-101; Toyobo).
Quantitative real-time PCR
The mRNA levels of DUOX1 were determined by
real-time PCR using SYBR Green Master Mix kit and ABI 7500
Real-Time PCR system (Applied Biosystems, Foster City, CA, USA).
Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) was used as an
internal control of RNA integrity. The 2−ΔΔct method was
used to analyze the relative changes in DUOX1 expression from the
real-time PCR experiments (18).
Real-time PCR was performed in triplicate. Primers used for DUOX1
were: DUOX1 forward, 5′-CCACCAGGAGTGGCATAAGT-3′ and reverse,
5′-CAGCTGACGGATGACTTGAA-3′ (110-bp product).
Statistical analysis
Kruskal-Wallis test was used to examine the
statistical differences among three groups or more. The
Mann-Whitney U-test was used to compare continuous variables
between two groups. The diagnostic performance of DUOX1 was
assessed by receiver operating characteristic (ROC) curve and the
area under the ROC curve (AUC). Survival curves were plotted using
the Kaplan-Meier method, and the statistical significance between
groups was determined by taking the log-rank test. Independent
variables predicting survival were evaluated by conducting a
multiple stepwise regression analysis with the Cox model. A simple
risk score was devised by using significant variables obtained from
the multiple stepwise Cox's regression analysis with P<0.05. The
discrimination capabilities of the simple risk score were also
presented by ROC curve and AUC. The optimal cut-off value was
determined to maximize the sum of the sensitivity and specificity.
All statistical tests were two-sided, and p-values <0.05 were
considered as statistically significant. The statistical analyses
were performed using SPSS version 21.0, MedCalc version 11.4 and
GraphPad Prism version 5.0.
Results
Correlation of DUOX1 expression and the
clinicopathological features
We enrolled 72 HCC patients in this study. The
median age of the liver cancer patients was 53.67 years (range,
16–84 years). The HCC patients were grouped according to tissue
type (tumor tissue vs. non-tumor tissue), HBsAg expression
(positive vs. negative), histological grade (grade 1, 2 and 3
groups), tumor stage (stage I, II, III and IV groups) and hepatic
cirrhosis (yes vs. no), respectively. We confirmed the difference
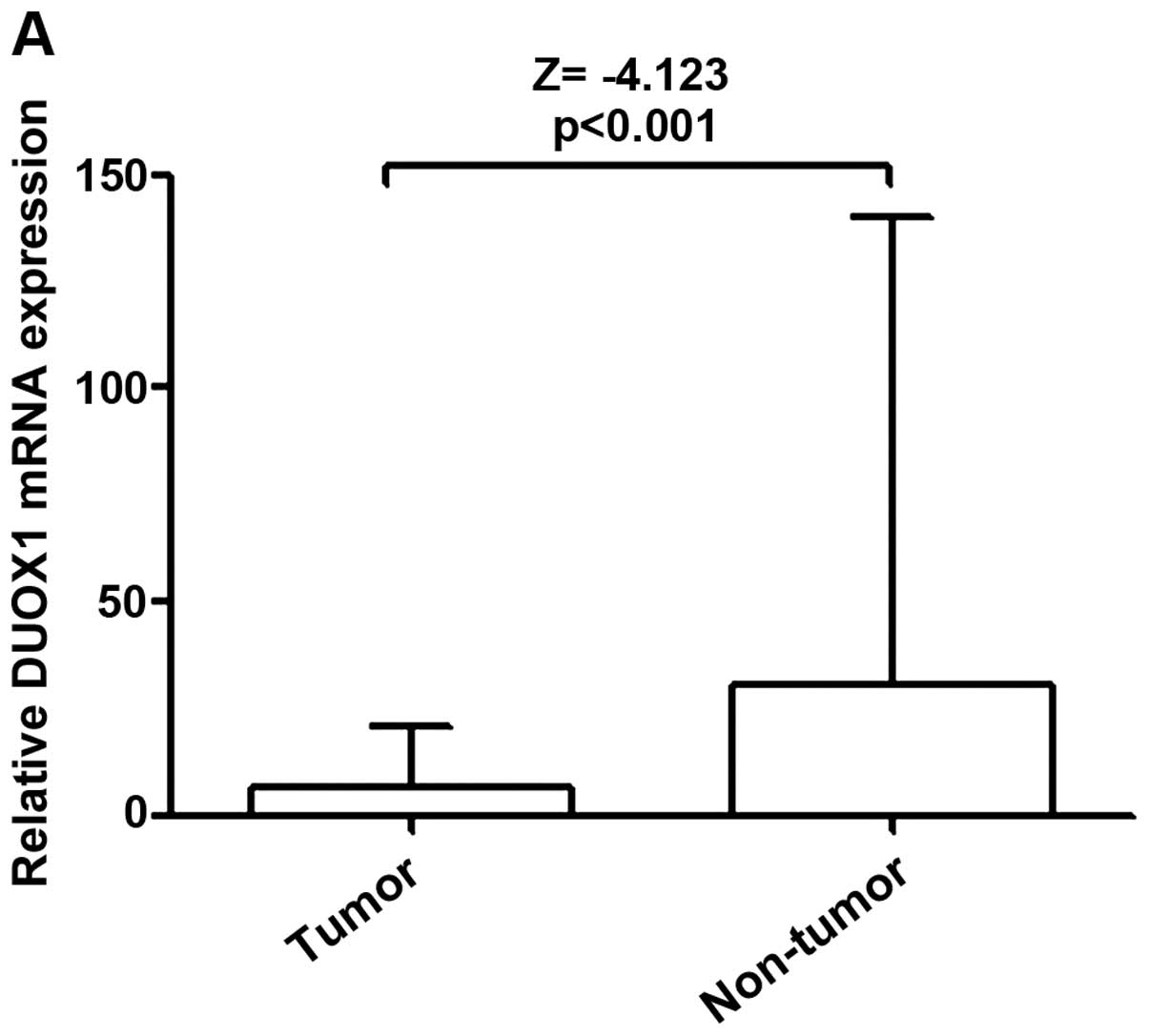
in DUOX1 expression in these groups (Fig. 1). DUOX1 mRNA expression was
significantly downregulated in the human primary HCC tissues when
compared with that in the adjacent non-tumor tissues (Fig. 1A). The expression of DUOX1 mRNA was
also significantly related to HBsAg expression (p=0.009, Fig. 1B) and hepatic cirrhosis (p=0.018,
Fig. 1E). Histological grade and
tumor stage were not correlated with DUOX1 mRNA levels (Fig. 1C and D).
Diagnostic performance of DUOX1 and
determination of the optimal cut-off value of DUOX1 mRNA
levels
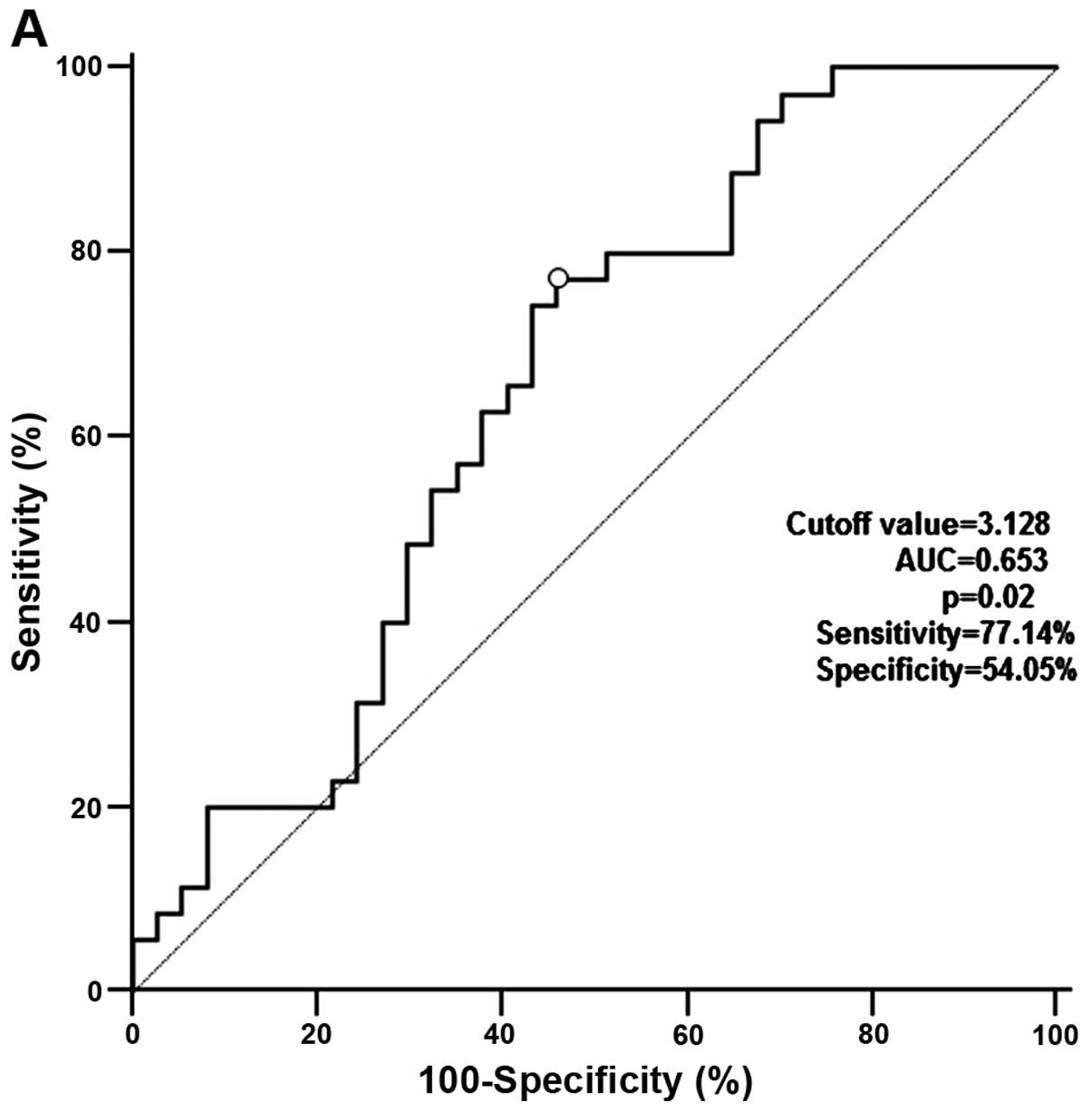
We considered death (yes vs. no) and recurrence (yes
vs. no) as final diagnosis separately; DUOX1 expression was
regarded as a diagnostic test. Then two ROC curves were plotted by
software MedCalc11.4 to evaluate the predictive efficacy of DUOX1
for HCC patient survival (Fig. 2).
The optimal cut-off values for DUOX1 expression were 3.128 and
3.468 according to the ROC curve for recurrence (Fig. 2A) and for death (Fig. 2B), respectively. Corresponding
diagnostic indices were as follows: sensitivity 77.14 and 77.78%,
specificity 54.05 and 62.96%, AUC 0.653 and 0.749. Based on the
optimal cut-off values for DUOX1 expression, patients were further
categorized into two groups to evaluate DFS (≥3.128, high
expression vs. <3.128, low expression) and OAS (≥3.468, high
expression vs. <3.468, low expression).
Relationship between disease-free
survival, overall survival and clinicopathological factors in the
HCC patients
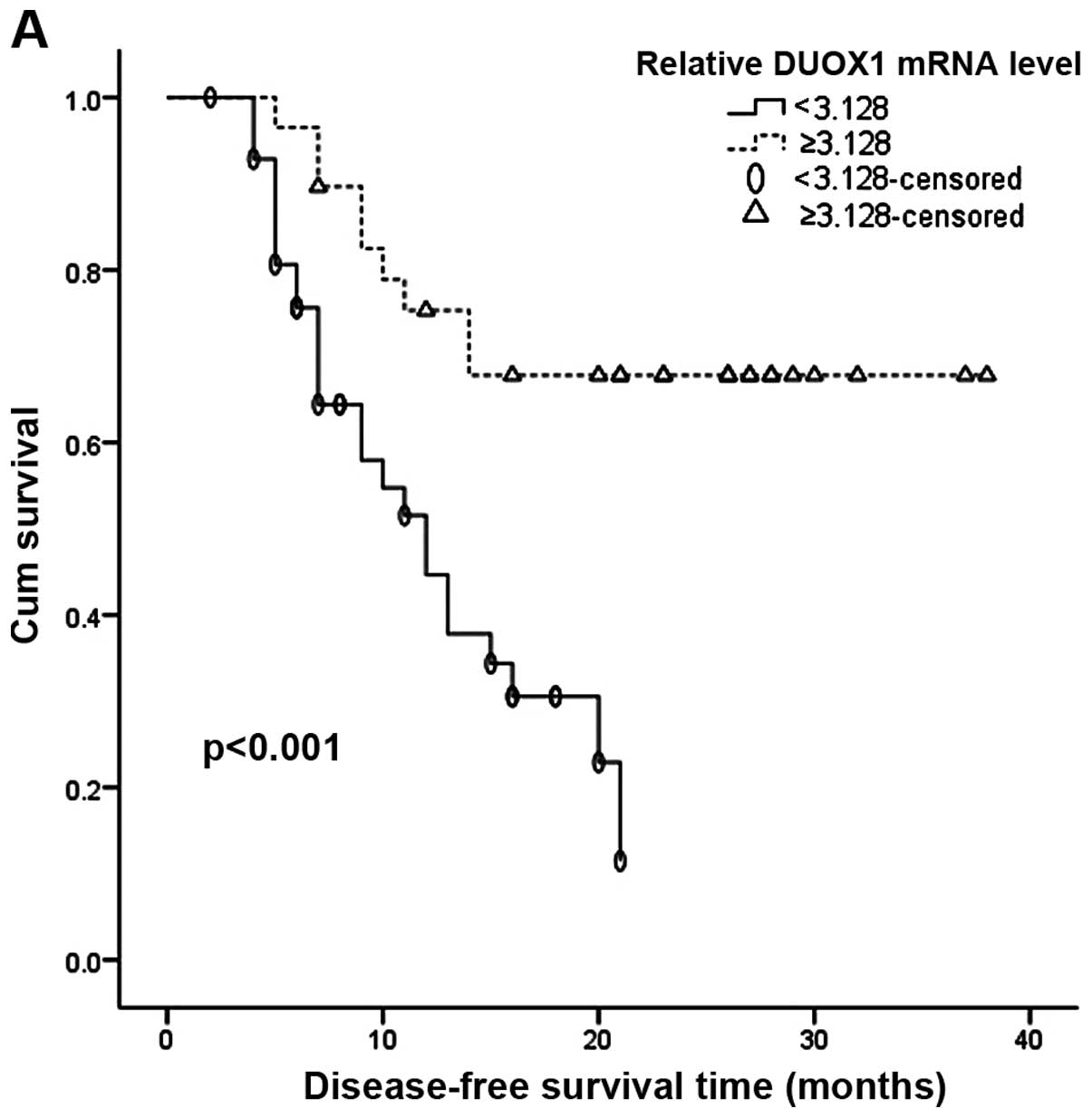
Subsequently, we used the Kaplan-Meier method to
further investigate the impact of clinical factors on DFS and OAS.
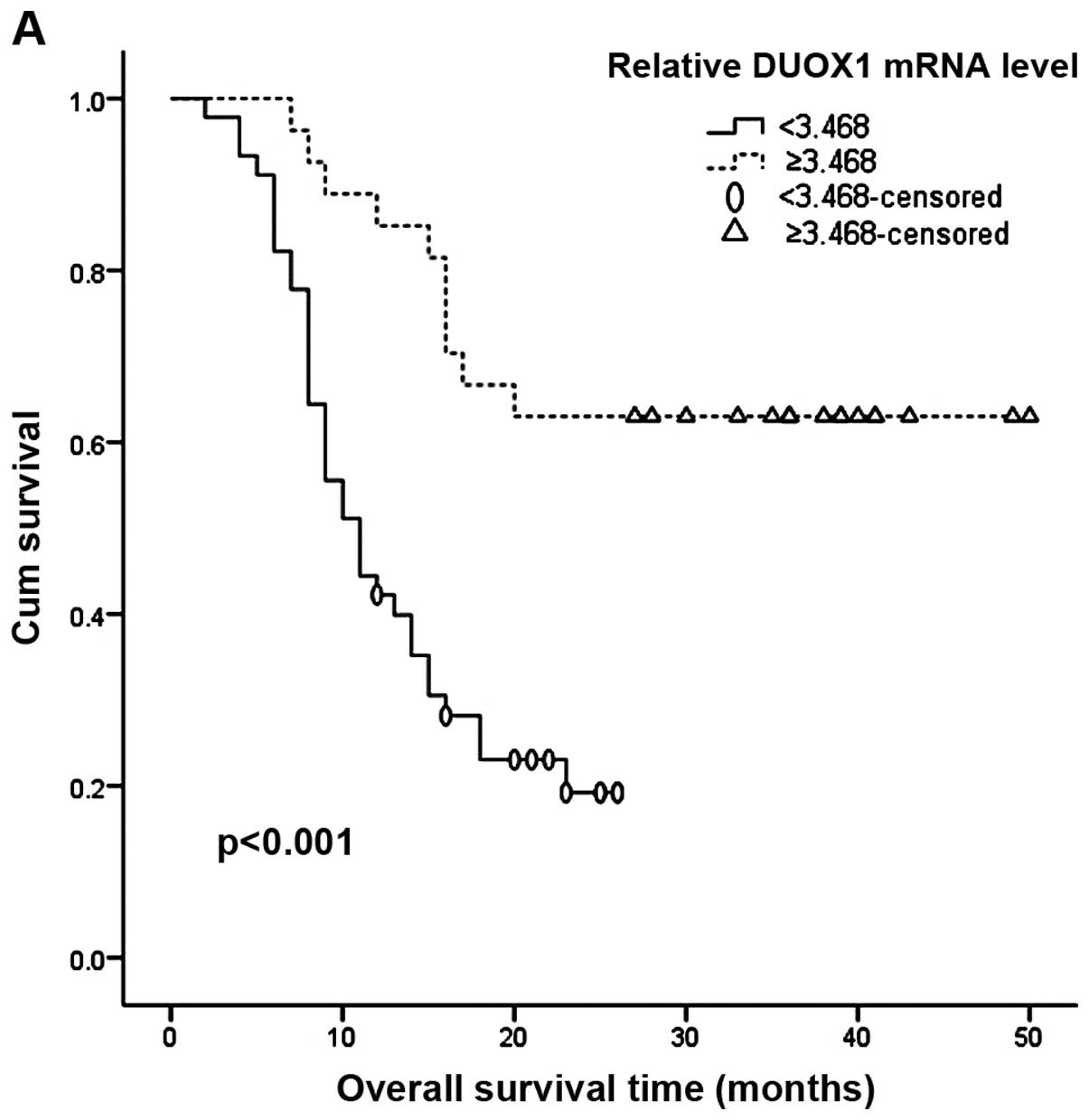
As shown in Figs. 3A and 4A, patients with high DUOX1 expression
tended to have prolonged DFS and OAS compared with those with low
DUOX1 expression. Figs. 3B and F
and 4B and F show that HBsAg
expression and age [60 years was taken as the cut-off value
according to Gokcan's et al (19)] were significantly correlated with
DFS and OAS. However, it is clear from Figs. 3D and E and 4D and E that intrahepatic metastasis was
correlated with OAS only and TNM stage seemed merely related to
DFS. Finally, histological grade had no correlation with DFS
(Fig. 3C) and OAS (Fig. 4C).
Univariate analysis and multivariate
analysis with Cox proportional hazards model
Furthermore, the univariate Cox's proportional
hazards model, in which the clinical factors such as gender, HBsAg,
tumor size [5 cm was considered as cut-off value according to
Hwang's et al (20)], age,
intrahepatic metastasis, histological grade, tumor stage, and DUOX1
expression were respectively included, showed that low expression
of DUOX1 was an independent prognostic factor for DFS (RR=3.65,
p=0.001) and OAS (RR=3.69, p<0.001) in hepatic carcinoma
patients (Table I). Notably, tumor
stage and HBsAg expression were merely correlated with DFS
(RR=2.10, p=0.030, and RR=8.82, p=0.032), and showed no association
with OAS. The results also showed that age was an independent
unfavorable prognostic factor for DFS and OAS (Table I).
 | Table IUnivariate analysis of prognostic
factors in patients with HCC as evaluated by disease-free survival
and overall survival. |
Table I
Univariate analysis of prognostic
factors in patients with HCC as evaluated by disease-free survival
and overall survival.
| Variable | Number | Disease-free survival
| Overall survival
|
|---|
| RR (95% CI) | β | P-value | RR (95% CI) | β | P-value |
|---|
| Gender | | | | | | | |
| Male | 56 | 1.11 (0.45–2.34) | 0.01 | 0.897 | 1.26 (0.61–2.62) | 0.228 | 0.542 |
| Female | 16 | Reference | | | Reference | | |
| HBsAg | | | | | | | |
| Positive | 62 | 8.82
(1.21–64.64) | 2.177 | 0.032 | 3.17
(0.98–10.24) | 1.153 | 0.054 |
| Negative | 10 | Reference | | | Reference | | |
| Age (years) | | | | | | | |
| <60 | 50 | Reference | | | Reference | | |
| ≥60 | 22 | 2.30
(1.01–5.29) | 0.834 | 0.049 | 2.31
(1.11–4.80) | 0.836 | 0.025 |
| Tumor size
(cm) | | | | | | | |
| <5 | 23 | Reference | | | Reference | | |
| ≥5 | 49 | 1.18
(0.58–2.36) | 0.162 | 0.65 | 1.06
(0.56–1.99) | 0.056 | 0.862 |
| Intrahepatic
metastasis | | | | | | | |
| Yes | 15 | 1.96
(0.91–4.20) | 0.673 | 0.084 | 1.92
(0.99–3.72) | 0.651 | 0.054 |
| No | 57 | Reference | | | Reference | | |
| Histological
grade | | | | | | | |
| 1 or 2 | 56 | Reference | | | Reference | | |
| 3 | 16 | 1.10
(0.50–2.43) | 0.099 | 0.805 | 1.10
(0.54–2.22) | 0.094 | 0.792 |
| Tumor stage | | | | | | | |
| I or II | 42 | Reference | | | Reference | | |
| III or IV | 30 | 2.10
(1.07–4.16) | 0.743 | 0.03 | 1.73
(0.96–3.11) | 0.548 | 0.067 |
| DUOX1 mRNA
level | | | | | | | |
| DFS OAS | DFS OAS | | | | | | |
| <3.128
<3.468 | 43 45 | 3.65
(1.67–7.96) | 1.294 | 0.001 | 3.69
(1.81–7.54) | 1.307 | <0.001 |
| ≥3.128 ≥3.468 | 29 27 | Reference | | | Reference | | |
The multivariable analysis including the significant
prognostic factors in the univariate analysis for DFS and OAS after
radical resection for HCC is summarized in Tables II and III. The expression of DUOX1 was found to
be one of the independent risk factors in the multivariable
analysis for DFS (p=0.002, RR=3.67; Table II) and OAS (p<0.001, RR=4.63;
Table III). Age and intrahepatic
metastasis were also significantly correlated with DFS (Table II) and OAS (Table III), while elderly age appeared to
have a more significant impact on DFS (≥60 years vs. <60 years,
RR=3.86, p=0.007) and OAS (≥60 years vs. <60 years, RR=4.55,
p=0.001).
| Table IIMultivariate analysis of prognostic
factors in patients with HCC as evaluated by disease-free
survival. |
Table II
Multivariate analysis of prognostic
factors in patients with HCC as evaluated by disease-free
survival.
| Parameter | β | RR | 95% CI | P-value |
|---|
| Relative DUOX1 mRNA
level (<3.128 vs. ≥3.128) | 1.300 | 3.67 | 1.59–8.45 | 0.002 |
| Age (≥60 vs. <60
years) | 1.351 | 3.86 | 1.44–10.36 | 0.007 |
| Intrahepatic
metastasis (yes vs. no) | 0.894 | 2.45 | 1.08–6.17 | 0.046 |
| TNM stage (III or
IV vs. I or II) | 0.833 | 2.30 | 0.95–5.58 | 0.065 |
| HBsAg (positive vs.
negative) | 1.287 | 3.62 | 0.43–30.21 | 0.234 |
| Histological grade
(3 vs. 1 or 2) | 0.324 | 1.38 | 0.59–3.26 | 0.459 |
| Gender (male vs.
female) | 0.397 | 1.49 | 0.62–3.55 | 0.372 |
| Tumor size (≥5
vs.<5 cm) | 0.246 | 1.28 | 0.53–3.11 | 0.587 |
| Table IIIMultivariate analysis of prognostic
factors in patients with HCC as evaluated by overall survival. |
Table III
Multivariate analysis of prognostic
factors in patients with HCC as evaluated by overall survival.
| Parameters | β | RR | 95% CI | P-value |
|---|
| Relative DUOX1 mRNA
level (<3.468 vs. ≥3.468) | 1.532 | 4.63 | 2.04–10.51 | <0.001 |
| Age (≥60 vs. <60
years) | 1.515 | 4.55 | 1.90–10.88 | 0.001 |
| Intrahepatic
metastasis (yes vs. no) | 1.132 | 3.10 | 1.30–7.40 | 0.011 |
| TNM stage (III or
IV vs. I or II) | 0.180 | 1.19 | 0.58–2.48 | 0.629 |
| HBsAg (positive vs.
negative) | 0.311 | 1.37 | 0.34–5.47 | 0.661 |
| Histological grade
(3 vs. 1 or 2) | 0.124 | 1.13 | 0.53–2.41 | 0.747 |
| Gender (male vs.
female) | 0.241 | 1.27 | 0.57–2.84 | 0.555 |
| Tumor size (≥5 vs.
<5 cm) | 0.022 | 1.02 | 0.48–2.19 | 0.955 |
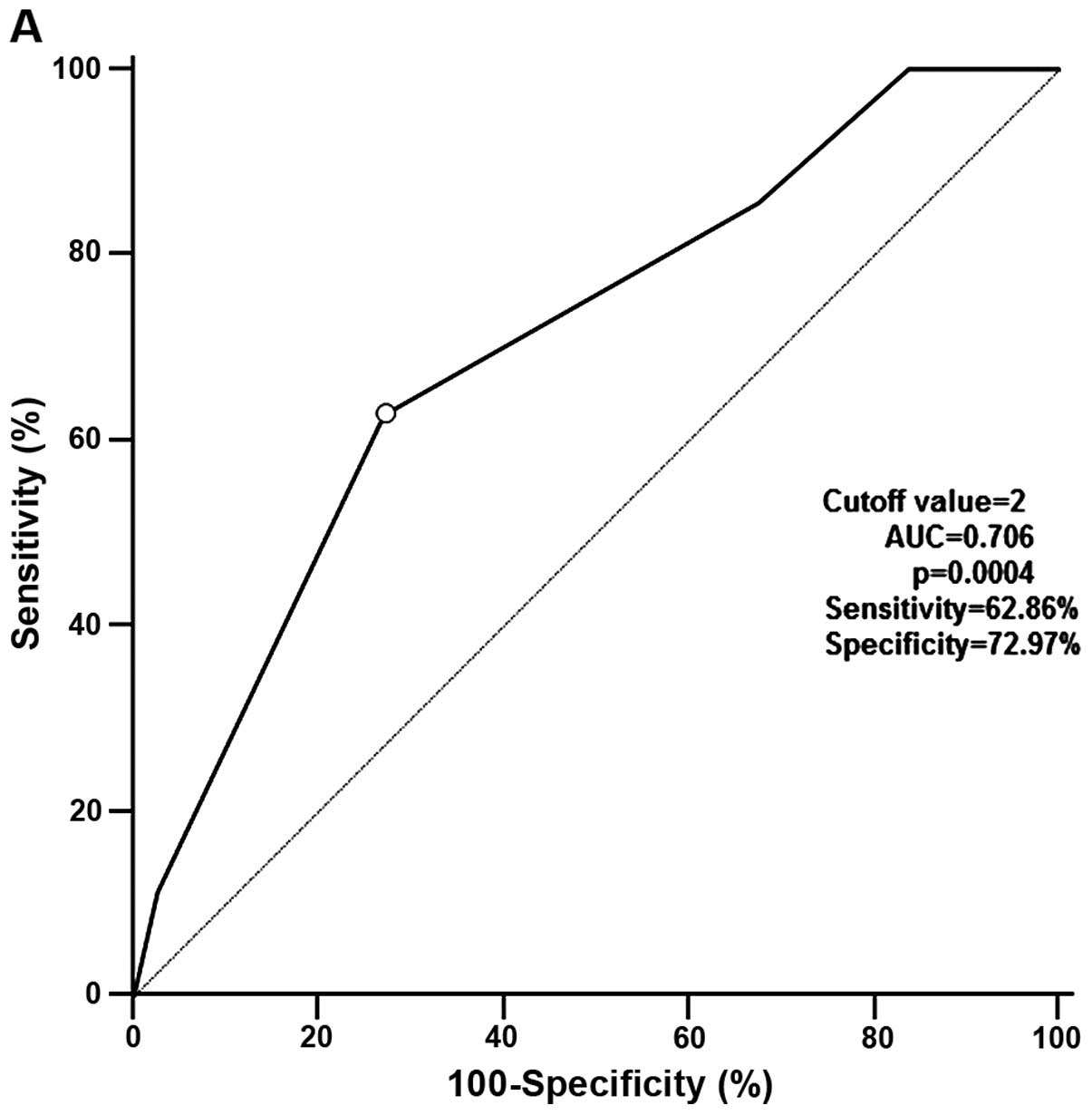
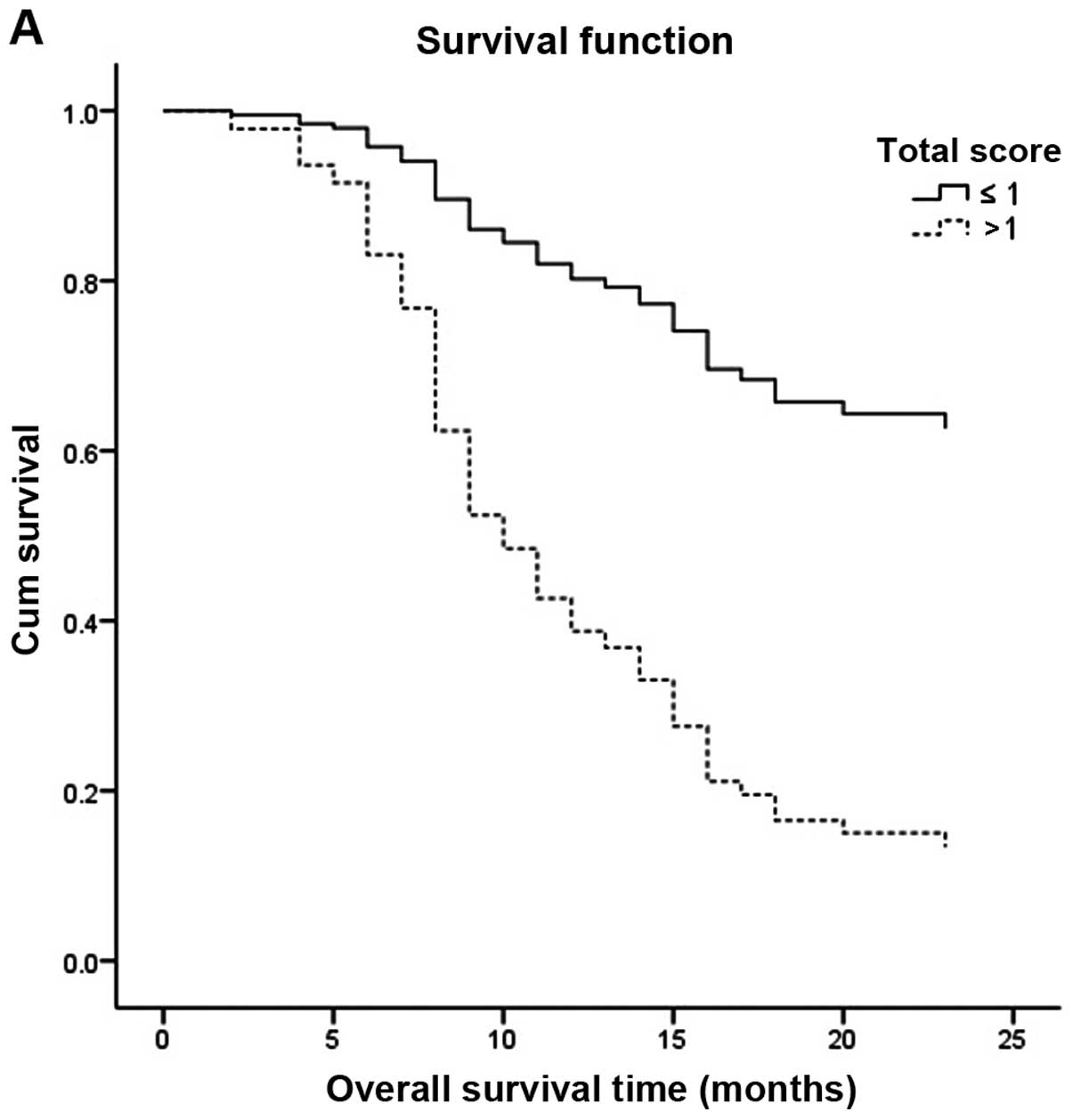
A simple risk score for predicting HCC
patient prognosis
A simple risk score was then devised by using
significant variables in the Cox model with P<0.05. The score is
the weighted sum of those variables for which the weights were
defined as the quotient (rounded to the nearest integer) of the
corresponding estimated coefficients from a Cox's regression
analysis divided by the smallest regression coefficient in the same
Cox model (Tables IV and V). The total score ranging from 0 to 4 was
used to predict DFS. OAS was predicted by the total score ranging
from 0 to 3. HCC patients were divided into two groups by the
endpoint of DFS (recurrence: yes or no) or endpoint of OAS (death:
yes or no), and the total score was considered as a diagnostic
test. Then two ROC curves were performed by software MedCalc11.4
(Fig. 5). The optimal cut-off
points of the two ROC curves were score 1 (OAS prediction score,
Fig. 5B) and score 2 (DFS
prediction score, Fig. 5A)
separately. For clinical and informative application, the patients
were further categorized into two risk groups to evaluate DFS
(total score ≤2 vs. total score >2) and OAS (total score ≤1 vs.
total score >1). From Fig. 6, it
was determined that patients whose total score was more than 2 were
more likely to relapse and patients with a total score more than 1
were apt to succumb to the disease than patients whose score was
less than 2 and 1. By applying the cut-off point of the two ROC
curves, the sensitivity and specificity to predict the death of
liver cancer patients after surgery were 73.33 and 7.78%, and to
predict the recurrence of HCC patients after operation were 62.86
and 72.97%. The AUC of the ROC curve for DFS was 0.706 (Fig. 5A) and for OAS was 0.798 (Fig. 5B).
| Table IVComponents of the disease-free
survival prediction score. |
Table IV
Components of the disease-free
survival prediction score.
| Factors | Score (rounded to
the nearest integer) | Score origin |
|---|
| DUOX1 mRNA
level | | |
| ≥3.128 | 0 | |
| <3.128 | 1 | 1.300/0.894 |
| Age (years) | | |
| <60 | 0 | |
| ≥60 | 2 | 1.351/0.894 |
| Intrahepatic
metastasis | | |
| No | 0 | |
| Yes | 1 | 0.894/0.894 |
| Table VComponents of the overall survival
prediction score. |
Table V
Components of the overall survival
prediction score.
| Factors | Score (rounded to
the nearest integer) | Score origin |
|---|
| DUOX1 mRNA
level | | |
| ≥3.468 | 0 | |
| <3.468 | 1 | 1.532/1.132 |
| Age (years) | | |
| <60 | 0 | |
| ≥60 | 1 | 1.515/1.132 |
| Intrahepatic
metastasis | | |
| No | 0 | |
| Yes | 1 | 1.132/1.132 |
Discussion
Generally, the increase in ROS production in
epithelial cells is mainly attributed to mitochondrial superoxide
production (21). However,
coordinated expression of DUOX1 and its maturation factor DUOXA1 in
some epithelial cancer cells suggests that the intracellular level
of ROS (superoxide and hydrogen peroxide) in epithelial cells may
be partially controlled by the dual oxidases (5). Regardless of the role of ROS in cancer
initiation and progression, a recent report linked intracellular
ROS accumulation to the establishment of senescence, connecting ROS
to tumor suppression (22). This is
in contrast to the well-described tumor-promoting ROS activities
which have been implicated in enhanced cell proliferation and
metastasis. Moreover, it has been demonstrated that cisplatin
apoptogenicity depends on the formation of ROS and occurs
independently of nuclear DNA damage, suggesting that apoptogenic
oxidative stress is the crucial mechanism of cisplatin-induced
cancer cell death (23). Moreover,
our previous study also demonstrated that DUOX1 exerted cytotoxic
and pro-apoptotic functions and suppressed tumorigenicity and
malignant progression by enhancing the production of intracellular
ROS (8).
It has been well established that cell cycle
checkpoints are important control mechanisms in maintaining tissue
homeostasis and one of the checkpoints, the G2/M checkpoint blocks
the entry into mitosis when DNA is damaged (24). Based on our previous research, the
liver cancer cell growth suppression induced by ectopic DUOX1
expression seemed to be caused by increasing G2/M phase cell number
(8), which implied that DUOX1
suppressed tumor cell growth through inducing G2/M phase cell cycle
arrest. Furthermore, in a previous study, we verified that DUOX1
was frequently silenced by promoter hypermethylation in most liver
cancer cell lines and primary HCC tissues, which suggest that
epigenetic inactivation of DUOX1 is an important factor in the
tumorigenesis of liver cancers (8).
Regrettably, the associations between prognosis of liver cancer
patients and DUOX1 expression were not identified in our previous
research.
In the present study, we found that the DUOX1 mRNA
expression was significantly decreased in the majority of primary
HCCs that we examined compared with that in the non-tumor liver
tissues (Fig. 1A). This result was
consistent with our previous report. We further investigated the
correlations between DUOX1 expression and clinicopathologic
features of the liver cancer cases. DUOX1 expression was
significantly correlated with HBsAg expression and hepatic
cirrhosis (Fig. 1B and E). Notably,
DUOX1 expression had no correlation with histological grade and
tumor stage (Fig. 1C and D). Then
two ROC curves of DUOX1 expression to predict DFS and OAS were
performed. In terms of predicting DFS, the area under the ROC curve
(AUC) was 0.653 for the DUOX1 mRNA level, and corresponding
diagnostic index including sensitivity was 77.14% and specificity
was 54.05% (Fig. 2A). ROC analysis
also identified the DUOX1 mRNA level as a predictive factor for OAS
(AUC, 0.749; p=0.0001; sensitivity, 77.78; specificity, 62.96%)
(Fig. 2B). Thus, we can conclude
that DUOX1 is an efficient biomarker for HCC prognosis. We only
measured the DUOX1 expression level in tissue and neglected
expression of DUOX1 in the serum, which hindered the further study
of the predictive efficacy of DUOX1 for HCC patient survival.
Further survival analysis with Kaplan-Meier method
indicated that patients with high DUOX1 expression (≥3.128) had a
longer DFS compared to the patients with low expression of DUOX1
(<3.128) (Fig. 3A). Similarly,
Fig. 4A shows that a high DUOX1
level (≥3.468) was also correlated with longer OAS compared with
the low DUOX1 level counterpart (<3.468). The HBsAg level and
age were also significantly correlated with DFS (Fig. 3B and F) and OAS (Fig. 4B and F) according to the
Kaplan-Meier analysis. Yet, intrahepatic metastasis was correlated
with OAS only and TNM stage seemed merely related to DFS (Figs. 3D and E and 4D and E). More confusingly, univariate Cox
regression analysis demonstrated that tumor stage and the HBsAg
level all were merely correlated to DFS, and showed no association
with OAS (Table I). Therefore, we
speculated that interference may exist among these variables above.
Fortunately, the influence of age and DUOX1 level on prognosis
according to Table I corresponded
to the study with Kaplan-Meier analysis.
In the present study, the univariate analysis with
Kaplan-Meier method and Cox model was firstly chosen to detect
important factors that may affect the prognosis of HCC patients,
but the results according to these two methods had some
contradictions. Thus, a multivariate analysis was needed to be
performed to identify the authenticity and validity of the
prognostic factors detected from the univariate analysis.
Ultimately, we screened the prognostic factors, DUOX1 expression,
age and intrahepatic metastasis, for DFS (Table II) and OAS (Table III). The data illustrated that the
hazard ratios of DUOX1 expression for DFS and OAS were respectively
3.67 (p=0.002) and 4.63 (p<0.001), indicating that the group
with lower DUOX1 expression may have an ~3.67-fold risk of liver
cancer relapse and a 4.63-fold risk of death. Nevertheless, the Cox
regression analysis suggested that tumor stage, histological grade,
gender and tumor size were not correlated with DFS and OAS, which
is in conflict with other research (25). The reason leading to the difference
between this research and other studies may be the small sample
size. In our present study, only 72 HCC patients were included,
which could hide the statistical significance of some variables in
the Cox regression analysis.
In order to research the impact of DUOX1 in more
detail expression, age and intrahepatic metastasis on DFS and OAS,
we developed a simple score composed of three variables to predict
the risk of HCC relapse and death after tumor resection. Patients
with prediction score of ≤2 vs. >2 had a distinctly different
risk of HCC relapse and with a total score of ≤1 vs. >1 had a
significantly different risk of HCC patient overall survival.
Notably, patients with a total score ≤2 had a low risk of HCC
recurrence and with total score ≤1 had a low risk for mortality
(Fig. 6). Identification of patient
risk for their prognosis could initiate an individualized
surveillance program for HCC patients after tumor resection.
Tumor occurrence and development can be considered
as the accumulation of gene mutations and epigenetic modifications.
The predominant consequence of this accumulation is the activation
of proto-oncogenes or silencing of tumor-suppressor genes (26). Consistent with previous reports that
DUOX1 can inhibit the occurrence or development of malignant tumors
through various mechanisms (3,6), our
results showed that the expression of DUOX1 in liver non-tumor
tissue was significant higher than that in liver malignant tumor
tissues. More importantly, we found that the patients with higher
DUOX1 expression had better cumulative survival. These results
together indicate that DUOX1 acts as a tumor suppressor in the
development of hepatic carcinoma and could well be considered as a
novel biomarker for prognosis and therapy in liver cancer. The
scoring system including DUOX1 in this study can provide evidence
to predict the recurrence and death of HCC patients after tumor
resection.
In summary, this study generated valuable evidence
that the high expression of DUOX1 in HCC leads to a better
prognosis in terms of both DFS and OAS after radical resection.
DUOX1 can be a useful predictor of survival in HCC patients.
Moreover, the scoring system including DUOX1 acts as a predictive
model first used in our study to predict HCC patient survival and
this predictive model can be a potential prognostic tool for liver
cancer patients.
Acknowledgments
We thank Dr Zhang Hao for providing the hepatoma
samples from the 72 patients.
References
|
1
|
Yang JD and Roberts LR: Hepatocellular
carcinoma: A global view. Nat Rev Gastroenterol Hepatol. 7:448–458.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Sakamoto M: Early HCC: Diagnosis and
molecular markers. J Gastroenterol. 44(Suppl 19): 108–111. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Roy K, Wu Y, Meitzler JL, Juhasz A, Liu H,
Jiang G, Lu J, Antony S and Doroshow JH: NADPH oxidases and cancer.
Clin Sci (Lond). 128:863–875. 2015. View Article : Google Scholar
|
|
4
|
De Deken X, Wang D, Many MC, Costagliola
S, Libert F, Vassart G, Dumont JE and Miot F: Cloning of two human
thyroid cDNAs encoding new members of the NADPH oxidase family. J
Biol Chem. 275:23227–23233. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Fischer H: Mechanisms and function of DUOX
in epithelia of the lung. Antioxid Redox Signal. 11:2453–2465.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Luxen S, Belinsky SA and Knaus UG:
Silencing of DUOX NADPH oxidases by promoter hypermethylation in
lung cancer. Cancer Res. 68:1037–1045. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Pulcrano M, Boukheris H, Talbot M, Caillou
B, Dupuy C, Virion A, De Vathaire F and Schlumberger M: Poorly
differentiated follicular thyroid carcinoma: Prognostic factors and
relevance of histological classification. Thyroid. 17:639–646.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Ling Q, Shi W, Huang C, Zheng J, Cheng Q,
Yu K, Chen S, Zhang H, Li N and Chen M: Epigenetic silencing of
dual oxidase 1 by promoter hypermethylation in human hepatocellular
carcinoma. Am J Cancer Res. 4:508–517. 2014.PubMed/NCBI
|
|
9
|
Tong L, Chuang CC, Wu S and Zuo L:
Reactive oxygen species in redox cancer therapy. Cancer Lett.
367:18–25. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Sablina AA, Budanov AV, Ilyinskaya GV,
Agapova LS, Kravchenko JE and Chumakov PM: The antioxidant function
of the p53 tumor suppressor. Nat Med. 11:1306–1313. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
D'Autréaux B and Toledano MB: ROS as
signalling molecules: Mechanisms that generate specificity in ROS
homeostasis. Nat Rev Mol Cell Biol. 8:813–824. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Bhattacharyya S and Saha J: Tumour,
oxidative stress and host t cell response: Cementing the dominance.
Scand J Immunol. 82:477–488. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cabello CM, Bair WB III and Wondrak GT:
Experimental therapeutics: Targeting the redox Achilles heel of
cancer. Curr Opin Investig Drugs. 8:1022–1037. 2007.PubMed/NCBI
|
|
14
|
Fruehauf JP and Meyskens FL Jr: Reactive
oxygen species: A breath of life or death? Clin Cancer Res.
13:789–794. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Nagasue N, Kohno H, Chang YC, Taniura H,
Yamanoi A, Uchida M, Kimoto T, Takemoto Y, Nakamura T and Yukaya H:
Liver resection for hepatocellular carcinoma. Results of 229
consecutive patients during 11 years. Ann Surg. 217:375–384. 1993.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Edge SB and Compton CC: The American Joint
Committee on Cancer: The 7th edition of the AJCC cancer staging
manual and the future of TNM. Ann Surg Oncol. 17:1471–1474. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Eisenhauer EA, Therasse P, Bogaerts J,
Schwartz LH, Sargent D, Ford R, Dancey J, Arbuck S, Gwyther S,
Mooney M, et al: New response evaluation criteria in solid tumours:
Revised RECIST guideline (version 1.1). Eur J Cancer. 45:228–247.
2009. View Article : Google Scholar
|
|
18
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-delta delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar
|
|
19
|
Gokcan H, Savaş N, Oztuna D, Moray G,
Boyvat F and Haberal M: Predictors of survival in hepatocellular
carcinoma patients. Ann Transplant. 20:596–603. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Hwang S, Lee YJ, Kim KH, Ahn CS, Moon DB,
Ha TY, Song GW, Jung DH and Lee SG: The impact of tumor size on
long-term survival outcomes after resection of solitary
hepatocellular carcinoma: Single-institution experience with 2558
patients. J Gastrointest Surg. 19:1281–1290. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Nickel A, Kohlhaas M and Maack C:
Mitochondrial reactive oxygen species production and elimination. J
Mol Cell Cardiol. 73:26–33. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Ramsey MR and Sharpless NE: ROS as a
tumour suppressor? Nat Cell Biol. 8:1213–1215. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Berndtsson M, Hägg M, Panaretakis T,
Havelka AM, Shoshan MC and Linder S: Acute apoptosis by cisplatin
requires induction of reactive oxygen species but is not associated
with damage to nuclear DNA. Int J Cancer. 120:175–180. 2007.
View Article : Google Scholar
|
|
24
|
Taylor WR and Stark GR: Regulation of the
G2/M transition by p53. Oncogene. 20:1803–1815. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Kao WY, Chao Y, Chang CC, Li CP, Su CW,
Huo TI, Huang YH, Chang YJ, Lin HC and Wu JC: Prognosis of
early-stage hepatocellular carcinoma: The clinical implications of
substages of Barcelona Clinic Liver Cancer System based on a cohort
of 1265 patients. Medicine (Baltimore). 94:e19292015. View Article : Google Scholar
|
|
26
|
Hahn WC and Weinberg RA: Rules for making
human tumor cells. N Engl J Med. 347:1593–1603. 2002. View Article : Google Scholar : PubMed/NCBI
|