Introduction
Bladder cancer is a common disease worldwide. At any
point in time 2.7 million people have a history of bladder cancer
(1). Most cases of bladder cancer
are non-muscle invasive at initial diagnosis (2). In non-muscle-invasive bladder cancer
(NMIBC), ~75% of patients present with stage pTa, pT1 or carcinoma
in situ (CIS) lesions (3).
Generally, NMIBC prognosis is good, although 30–80% cases may show
recurrence, with 1–45% progressing to muscle invasion within 5
years (3–5). Consequently, NMIBC is a chronic
disease with varying oncologic outcomes requiring frequent
follow-up and repeated treatments with cystoscopy, making the cost
per patient from diagnosis to death the highest of all cancers
(6,7).
Recent diagnostic methods combined with
state-of-the-art technology have been introduced in cystoscopy to
collect real-time in vivo histological images of the bladder
mucosa for diagnosis (8), and
endoscopic molecular imaging can detect molecular changes in
diseased cells within the mucosa. This discipline has great
potential to improve medicine via detection of diseases in early
stages (9,10). Application of molecular imaging to
endoscopy for the diagnosis and treatment of cancer may increase
the efficiency of endoscopic screening and surveillance. An
important advantage of performing molecular imaging of the mucosa
is the opportunity to apply exogenous probes (11). Several different classes of probe
technology have been developed to perform molecular imaging,
including antibodies, antibody fragments, peptides, nanoparticles
and activatable probes (12,13).
Peptide-based delivery of compounds has numerous
advantages over other delivery systems. Peptides are smaller in
size and penetrate more efficiently into tissue compared to
antibodies. In addition, peptides are synthesized by automated
techniques with low production costs, which makes them even more
popular (14). Two cyclic bladder
cancer-homing peptides have been identified to date. The first
peptide, CSNRDARRC, was discovered after screening a phage display
peptide library on bladder cancer cells (15). The second one is PLZ4 (CQDGRMGFC),
which was identified by screening a one-bead-one-compound
combinatorial library on bladder cancer (16). PLZ4 not only selectively binds to
bladder cancer cell lines but also to primary bladder cancer cells
from patients, and not to normal urothelial cells (17). However, the CSNRDARRC and PLZ4
peptides were screened from muscle-invasive bladder cancer cell
lines [HT-1376, 5637 (HTB-9), SCaBER, TCCSUP (HTB-5)], whereas ~75%
of all patients with bladder cancer present with NMIBC at follow-up
with cystoscopy.
The most commonly used cystoscopy, white light
cystoscopy (WLC), has several shortcomings. Carcinomas in
situ are difficult to visualize and distinguish from benign
inflammatory lesions (18), and
WLC-guided transurethral resection of NMIBC underscores the
shortcomings of WLC in the diagnosis of papillary lesions:
inadequate visualization of all tumors that may be present; diffuse
tumor borders may result in missed or incompletely resected lesions
(19). Therefore, with NMIBC in
particular, tumor-homing peptides are very important for
cystoscopic optical molecular imaging to visualize residual tumors
and carcinomas in situ.
The phage display technology is based on the ability
to express foreign polypeptides as fusions to capsid proteins on
the surface of bacteriophages; it was first described in 1985 by
Smith (20). Phage display has
successfully selected peptides specific for molecular signatures or
biomarkers in tumor tissue and vasculature. In vitro
screening involving the binding of phages to cultured cells has
identified peptides specific to tumor cells, such as bladder and
lung tumor cells. In vivo screening after intravenous
administration of phage libraries has identified peptides that home
to diverse pathologic tissues such as cancer and tumor blood
vessels. In the present study, we identified a bladder tumor
cell-binding peptide using in vivo screening of a
phage-display peptide library.
Materials and methods
Cell lines
The non-muscle-invasive bladder tumor cell line
BIU-87 (Chinese human superficial bladder cancer cell line) was
kindly provided by Dr Zhou Liqun (Institute of Urology, Peking
University, Beijing, China) (21–23).
The other bladder tumor T24, E–J and 5637 cell lines were purchased
from the Shanghai Ouro Biological Science and Technology Co., Ltd.
(Shanghai, China). The cell lines SMMC-7721 (human hepatoma), SiHa
(human cervical cancer), KC (human kidney cancer) and MCF-7 (human
breast cancer) were provided by Shanxi Medical Center of Scientific
Research (Taiyuan, China). BIU-87, T24, E–J, 5637, KC and SMMC-7721
cells were cultured in RPMI-1640 medium; MCF-7 and SiHa cells were
cultured in high-glucose Dulbecco's modified Eagle's medium (DMEM).
Each medium was supplemented with 10% fetal bovine serum (FBS)
containing 1% penicillin and streptomycin. Cells were grown at 37°C
in 5% CO2.
Animals
All animal experiments were conducted according to
the guidelines of the Laboratory Animals Ethics Committee of Shanxi
Medical University. BALB/c nu/nu nude male mice (4–6 weeks) were
purchased from Hunan SJA Laboratory Animal Co. Ltd. (Hunan, China).
The model was established as previously reported (24,25)
with some modifications. Briefly, a mixture of BIU-87 tumor cells
(1×107) and basement membrane extract (Matrigel; 200
μl; BD Biosciences, San Jose, CA, USA) was subcutaneously
injected into the forelimb armpits. Visible tumors were formed
after ~15 days.
In vivo phage display biopanning
The Ph.D.-C7C Phage Display Peptide Library kit
containing E. coli host strain ER2738 was purchased from New
England Biolabs (Beverly, MA, USA). Tumor-bearing mice were
intravenously injected with 2×1011 plaque forming units
(PFUs) of phage peptide library via the tail vein. After 15 min,
mice were sacrificed and perfused by injection of 50 ml 0.9% normal
saline through the heart to wash unbound phages. Then, a portion of
the tumor and control tissues (liver, kidney, lung and muscle) were
harvested and preserved with 4% formaldehyde. The tumors were
manually homogenized and washed with 10× Tris-buffered saline
containing 0.1% Tween-20 (0.1% TBST) to remove non-specifically
bound phages. Cell membrane-bound phages were eluted with 1 ml of
elution buffer (0.2 M glycine-HCl, pH 2.2, 1 mg/ml BSA) for 10 min
on ice, and neutralized with 150 μl of 1 M Tris-HCl (pH
9.0). After centrifugation, the supernatant was collected, and the
cells in the precipitate were washed once with phosphate-buffered
saline (PBS)-BSA and lysed with 0.1% Triton X-100 for 2 h at room
temperature. Thus, the internalized phages contained in the cell
lysate were recovered. A total of 10 μl eluted phage was
titrated on agar plates in the presence of IPTG/X-gel (1 mg/l) and
tetracycline (40 mg/ml). The remaining phages were amplified by
ER2738 bacteria at 37°C for 4.5 h, and injected into tumor-bearing
mice to repeat the above procedures. The entire biopanning process
was repeated three rounds. At the end of the third round, the phage
solution was eluted and titrated on LB/IPTG/X-gel plates. Then,
phage clones were randomly selected, and the inserted DNA sequence
was determined using the primer: 5′-CCCTCATAGTTAGCGTAACG-3′ (New
England Biolabs). All peptide library DNA was sequenced using a DNA
sequencer following previous protocols (26).
Immunohistochemical staining with
phage
In vivo phage localization assays were
performed as previously described (27,28).
Tumor and control tissues (liver, kidney, lung and muscle),
extracted from tumor-bearing mice and preserved in 4%
paraformaldehyde were paraffin-embedded and 4-μm sections
were obtained. After deparaffinization, the sections were rinsed
(3×5 min) in PBST (0.01 M PBS, 0.05% Tween-20; pH 7.4), and blocked
with 3% hydrogen peroxide-methanol at room temperature for
endogenous peroxidase quenching. The sections were then incubated
with blocking buffer (10% normal goat serum) at room temperature
for 30 min, followed by overnight incubation at 4°C with rabbit
anti-M13 bacteriophage antibody diluted in PBS (1:200). Next, the
sections were rinsed in PBST (3×5 min) and incubated for 30 min at
37°C with goat anti-rabbit IgG (1:50). Detection was carried out
with 3,3′-diaminobenzidine (DAB) at room temperature in the dark
for 5 min. Counterstaining was performed with hematoxylin. Sections
were finally dehydrated, cleared and mounted with neutral resin.
For the blank control group, the same steps described above were
followed, but the anti-M13 bacteriophage antibody was replaced by
PBS. A ScanScope digital pathology scanning system (Aperio
Technologies, Vista, CA, USA) was used to analyze the binding of
the phage peptide to tissues.
Cell enzyme-linked immunosorbent
assay
After the third round of in vivo screening,
30 blue single colonies were randomly picked from the phage titer
plates. Each single colony was amplified, and 1×1010 PFU
of each colony were stored at 4°C until enzyme-linked immunosorbent
assay (ELISA) detection.
BIU-87 and iMBT cells (normal human bladder
epithelial cells) were plated at a density of 1×104
cells/well in a 96-well plate and incubated at 37°C in 5%
CO2 for 24 h. Subsequently, the cells were washed and
fixed with 4% paraformaldehyde for 15 min at room temperature.
After incubation with 3% H2O2 (100
μl/well) at 37°C for 30 min, the plates were washed 3 times
with PBS, and the wells were blocked with 200 ml of 5% BSA for 30
min at 37°C. The phages (1×1010 PFU/well) were added to
BIU-87 or iMBT cells and incubated at 37°C for 1-2 h. The plates
were then washed 3 times with TBST before addition of 100 μl
HRP-anti-M13 mAb (1:5,000) for 1 h at 37°C. After washing 3 times
with 0.05% TBST, 3,3′,5,5′-tetramethylbenzidine (TMB) was added at
room temperature for 30 min. The reaction was terminated by the
addition of 50 μl of 2 M H2SO4.
Subsequently, the plates were read on an automated ELISA plate
reader at 450 nm. Unrelated phages with equal titers were added to
the wells in place of selected phage clones to serve as negative
controls. Selectivity was determined using the following formula:
Selectivity = [BIU-87 (OD450 - OD450negative
control)]/[normal human bladder epithelial cells (OD450 -
OD450negative control)]. Those with affinity ≥2 were
considered positive clones; those with the highest binding
affinities had their amino acid sequences analyzed.
Peptide synthesis
The CSSPIGRHC (NYZL1) and control CRIGSPHSC
(svNYZL1) peptides were synthesized (Chinese Peptide Co., Hangzhou,
China) using the standard solid-phase fluorenylmethyloxycarbonyl
chloride chemistry. The products were purified to a minimum purity
of 98% by high-performance liquid chromatography (HPLC). The
sequence and structure of each peptide were characterized by mass
spectrometry. FITC-conjugated CSSPIGRHC and FITC-conjugated
CRIGSPHSC (negative control) were also synthesized in the same
manner.
Binding of a fluorescent peptide to
cultured and exfoliated cells in the urine
The non-muscle-invasive bladder tumor BIU-87 cells
(n=1×105) were plated in glass-bottom dishes (35 mm;
GBD-35-15; NEST) and cultured for 24 h. The cells were washed 3
times with PBS and fixed with 4% paraformaldehyde at room
temperature for 20 min. After cells were blocked with 2% BSA for 1
h, the FITC-NYZL1 and FITC-svNYZL1 peptides, respectively, were
added for 1, 4 or 12 h at 37°C. After 3 washes,
4′,6-diamidino-2-phenylindole (DAPI) was used to stain the nuclei
for 5 min at room temperature and examined for fluorescence by
laser scanning confocal microscopy (Olympus FluoView FV1000;
Olympus, Tokyo, Japan). Meanwhile, the other bladder tumor cell
lines, i.e. T24, E–J and 5637 as well as KC, SMMC-7721, SiHa and
MCF-7 cells were further assessed by fluorescence microscopy using
a procedure similar to that described above. FITC-conjugated
synthetic NYZL1 peptides were incubated with the cells for 12 h at
37°C. FITC-svNYZL1 peptides were used as negative controls. Mean
cellular fluorescence intensity of 5 fields (up, down, left, right
and middle) was used for statistical analysis. The percentage of
positive (peptide bound) cells was calculated by dividing the
number of green fluorescent cells with that of DAPI-stained cells
in 5 high-power fields.
Urine samples were collected from 66 bladder cancer
patients hospitalized in The First Hospital of Shanxi Medical
University from August 2014 to January 2015. Of these patients, 9
had Ta disease, 22 T1 disease, 21
T2 disease and 14 T3–4 disease as determined
by pathological analyses. Meanwhile, 12 cystitis patients and 24
healthy individuals with similar ages were selected as controls.
Exfoliated cells were obtained from 200 ml of second morning
voiding urine from patients with BCa and healthy adults. Urine
samples were processed immediately after collection. After
centrifugation for 10 min (1,300 rpm), the sediment was fixed with
4% paraformaldehyde at room temperature for 30 min. Then, cells
were smeared in the Laser confocal culture dish. The FITC-NYZL1 (5
μmol/l) and FITC-svNYZL1 (5 μmol/l) peptides were
incubated with the cells for 1 h at 4°C. After 3 washes, DAPI was
used to stain the nuclei for 5 min at room temperature and examined
for fluorescence by laser scanning confocal microscopy. Data
analysis was carried out as described for cultured cells above.
Competitive experiment
The non-muscle-invasive bladder tumor BIU-87 cells
(n=1×106) were divided into 6 tubes for the 2 groups.
NYZL-1 non-tagged and NYZL 1 FITC-tagged solutions both contained
the peptides at 5 mg/ml. Experimental details are listed in
Table I. BIU-87 cells were treated
with various probes, followed by staining in the dark for 30 min;
after two PBS washes, cells were fixed with 2% PFA, resuspended and
assessed on a FACS analyzer. Experiments were repeated 3 times.
 | Table INYZL1 probe competitive assay. |
Table I
NYZL1 probe competitive assay.
| NYZL1
| NYZL1-FITC
|
|---|
| 2 μl | 5 μl | 10 μl | 2 μl | 5 μl | 10 μl |
|---|
| BIU-87 cells | | | | | | |
| Competitive
group | + | + | + | + | + | + |
| Control group | | − | | + | + | + |
Peptide binding on human tissues
Peptide-based immunofluorescent histochemistry was
performed to validate peptide binding to human bladder cancer.
Frozen sections of human bladder cancer and adjacent normal
appearing bladder mucosa tissues were performed according to the
procedures described above. Fresh frozen sections were blocked with
PBS/1% BSA at 37°C for 30 min, incubated with 100 μmol/l
FITC-NYZL1 or FITC-svNYZL1 (negative control) at 4°C for 1 h, and
washed with PBS. After counterstaining of cells with DAPI,
fluorescent images of tissue slides were acquired under a
fluorescence microscope.
Tumor homing of the NYZL1 peptide in
vivo
To test the tumor-homing ability, FITC-NYZL1 or
FITC-svNYZL1 (210 μg) was injected into the tail vein of
human BIU-87 tumor-bearing mice. After 24 h, mice were anesthetized
and transcardially perfused with physiological saline to remove
blood and unbound peptides. Tumors and control organs were excised
and frozen in tissue-freezing medium (Jung Tissue Freezing Medium;
Leica Microsystems, Wetzlar, Germany), cut into 6-μm
sections and arrayed on slides. The slides were then fixed with 4%
paraformaldehyde for 20 min at 4°C, stained with DAPI for 8 min at
room temperature and examined for fluorescence by laser scanning
confocal microscopy (Olympus FluoView FV1000). Quantification of
imaging data was accomplished using Image-Pro Plus 7.0 (Media
Cybernetics, Bethesda, MD, USA).
Whole-organ imaging
For whole-organ imaging (29), tumor-bearing mice were intravenously
injected with 200 μl of 720 μM fluorescein-conjugated
peptide (FITC-NYZL1 or FITC-svNYZL1). After 30 min, 1, 2, 4, 8 and
12 h, the mice were anesthetized and transcardially perfused with
physiological saline to remove unbound peptides; tumors and organs
were excised for examination. Organ imaging was performed under
blue light using a multispectral fluorescence in vivo
molecular imaging system (S-0010A; Science, Taiyuan, China).
Statistical analysis
All quantitative data are mean ± standard error of
the mean (SEM). According to normality test results, data were
compared using one-way analysis of variance (ANOVA) followed by LSD
post hoc test. Two-tailed P<0.05 was considered statistically
significant; adjusted P-values were used among subgroup
comparisons. All statistical analyses were performed with SPSS 17.0
(IBM, Armonk, NY, USA) for Windows.
Results
Specific binding ability of the phages to
BIU-87 bladder tumor tissue in vivo
To obtain the tumor-homing peptides by in
vivo phage display biopanning against human bladder tumor
cells, phage recovery from xenograft tumor tissues was assessed
after every round of biopanning. The numbers of phages specifically
binding to the tumor gradually increased: phage recovery rates were
1.324×10−5, 2.526×10−5 and
5.738×10−3 PFU/g in the first, second and third rounds,
respectively (Table II). After the
third round of screening, the numbers of phages that bound to the
tumor tissue were enriched ~4.334×102-fold compared to
the first round.
| Table IIEnrichment rate of phage screening
in vivo. |
Table II
Enrichment rate of phage screening
in vivo.
| Panning round | Tumor weight
(g) | Selected phage
(input PFU) | Eluted phage
(output PFU) | Phage recovery rate
[(output/input)/g] |
|---|
| 1 | 0.37 |
3.0×1010 |
8.0×105 |
1.324×10−5 |
| 2 | 0.38 |
1.0×1010 |
4.8×105 |
2.526×10−5 |
| 3 | 0.61 |
2.0×108 |
3.5×105 |
5.738×10−3 |
After the third round of screening, we randomly
selected 30 phage clones for ELISA. The results showed 24 phage
clones with selective binding to BIU-87 cells compared with normal
bladder cells (affinity ≥2.0), including 10 individual phage clones
with higher binding activity (affinity >6.0), which were
isolated and sequenced. After translation into corresponding
peptide sequences, eight phage clones displayed a predominant
CSSPIGRHC motif; one displayed the CTMSNLKGC motif and another the
CNNVLSQMC peptide motif. We used ExPASy/ProtParam and NCBI/BLAST
databases to further analyze the CSSPIGRHC peptide. This motif had
no homology with known genes and proteins. Thus, the CSSPIGRHC
peptide is a new peptide sequence specifically binding to BIU-87
cells. This peptide (CSSPIGRHC) was named NYZL1 and synthesized for
further testing. Since BIU-87 cells are Chinese human superficial
bladder cancer cells, the present study is the first to explore the
selected NYZL1 peptide with specific binding to Chinese bladder
cancer.
To evaluate the specificity of phage clones for
tumor homing, we compared the tissue distribution among the tumor,
liver, kidney, lung, bladder and muscle tissues in each round of
screening by immunohistochemistry. Phage peptides were enriched in
tumor tissues and increased with each round of screening in
vivo (Fig. 1B–D). The majority
of phage clones preferentially bound to tumors rather than control
tissues after the third screening (Fig.
1D–I). Various non-specific adsorption phages were observed in
the liver and kidney tissues, perhaps since the phages were
metabolized mainly by the liver and kidneys (Fig. 1G and H). Only few phages binding to
bladder, lung and muscle tissues were obtained after the third
screening (Fig. 1E, F and I).
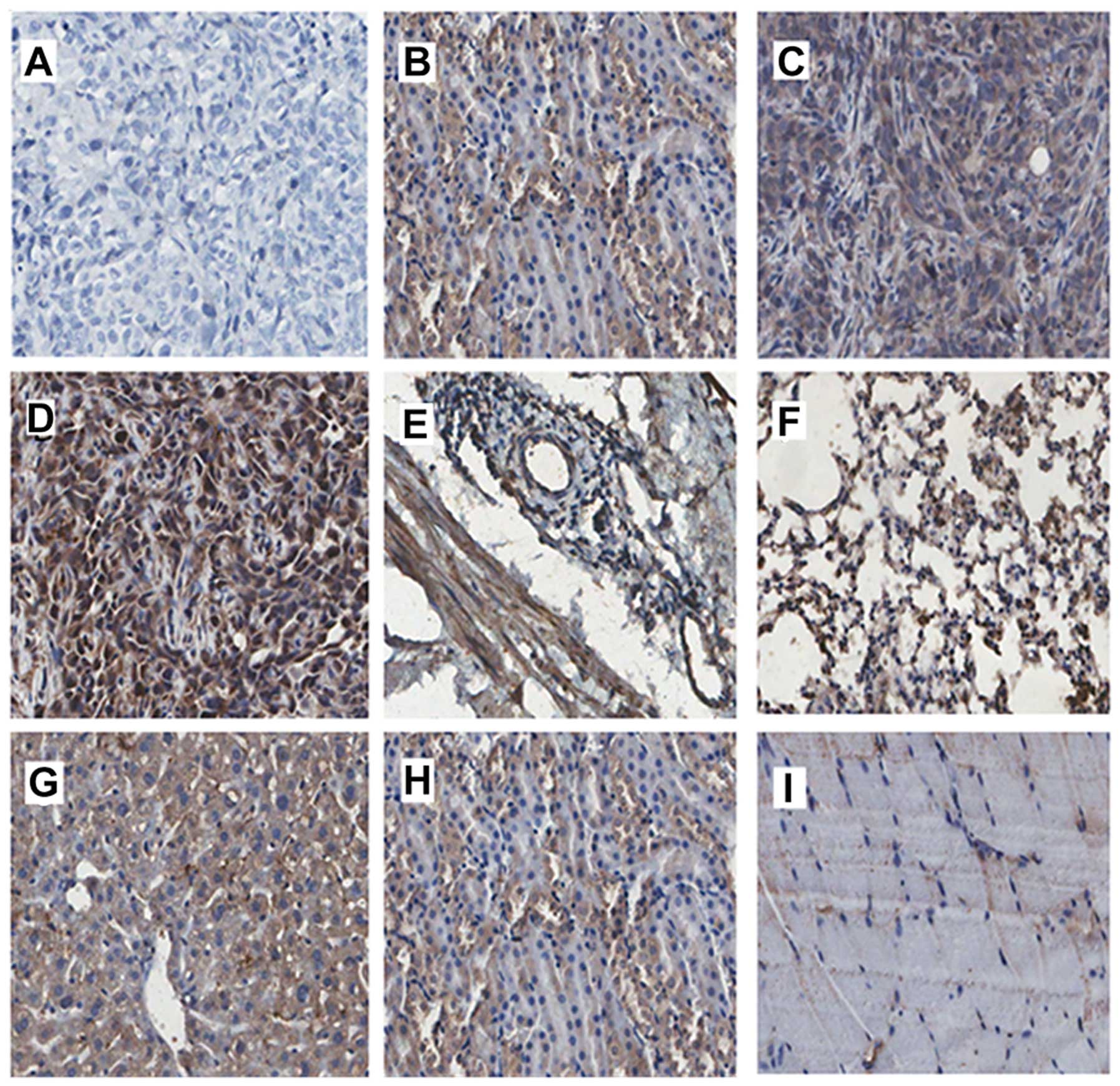 | Figure 1In vivo phage localization
assays by phage immunostaining. Phage immunostaining confirms a
significant difference in the binding rate and specificity between
tumor and normal tissues (bladder mucosa, liver, kidney, lung and
muscle). The phage binding rate was increased in tumor tissues with
increasing screening round. (A) Tumor tissue in the control group.
(B–D) First, second and third screening of phage tumor tissue
sections. (E–I) Control tissues from the third round (E, bladder;
F, lung; G, liver; H, kidney; and I, muscle) (magnification, ×200;
Aperio ScanScope). |
NYZL1 specifically binds to BIU-87
bladder cancer cells in vitro
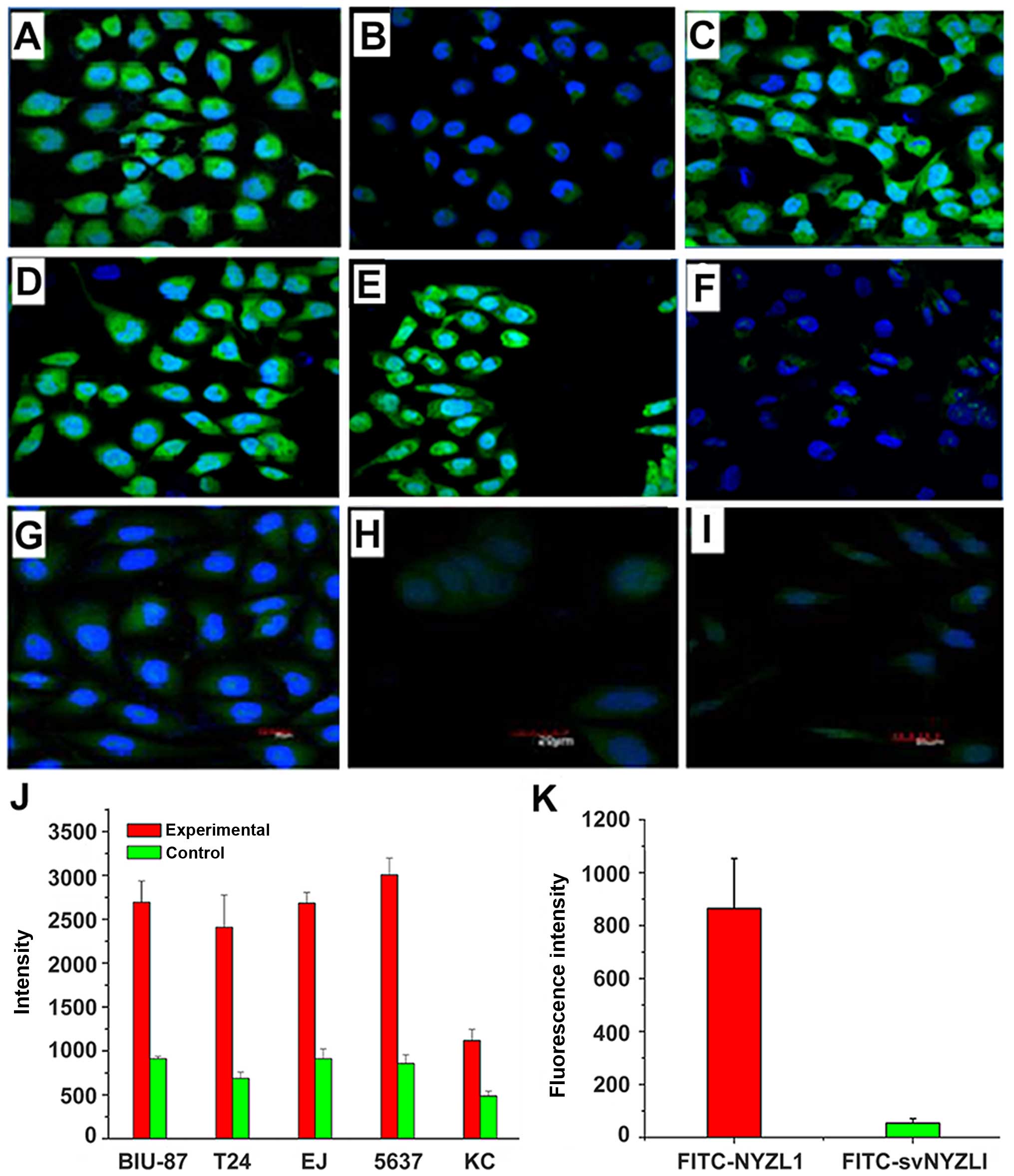
To further verify the specific binding of NYZL1 to
bladder cancer cells, whole cell binding assay was performed in
vitro. The NYZL1 peptide was synthesized and conjugated with
green fluorescent FITC at its amino terminus. Several bladder
cancer cell lines (BIU-87, T24, E–J and 5637) were selected and
other tumor cells (KC, SMMC-7721, SiHa and MCF-7) were used as
controls. Immunofluorescence analysis demonstrated that the
FITC-conjugated NYZL1 peptide strongly bound to BIU-87, T24, E–J
and 5637 bladder cancer cells, compared with the control KC,
SMMC-7721, SiHa and MCF-7 cells (Fig.
2; Table III). The FITC-NYZL1
peptide bound to BIU-87 cells with a similar strength compared to
the other bladder cancer T24, E–J, 5637 cells (Fig. 2A–J). Meanwhile, the negative control
FITC-svNYZL1 (the control peptide, CRIGSPHSC, is a scrambled
variant of NYZL1, named svNYZL1) was used to determine whether
peptide NYZL1 binds to BIU-87 bladder cancer cells in vitro.
Fluorescein imaging revealed that NYZL1 specifically bound to
BIU-87 bladder cancer cells. By contrast, no positive fluorescence
was detected in the FITC-svNYZL1 peptide group (Fig. 2K). These results revealed that
binding of the NYZL1 peptide to other types of tumor cells was
relatively weak compared to that to bladder tumor cells. Next,
binding of the NYZL1 peptide to BIU-87 cells vs. different types of
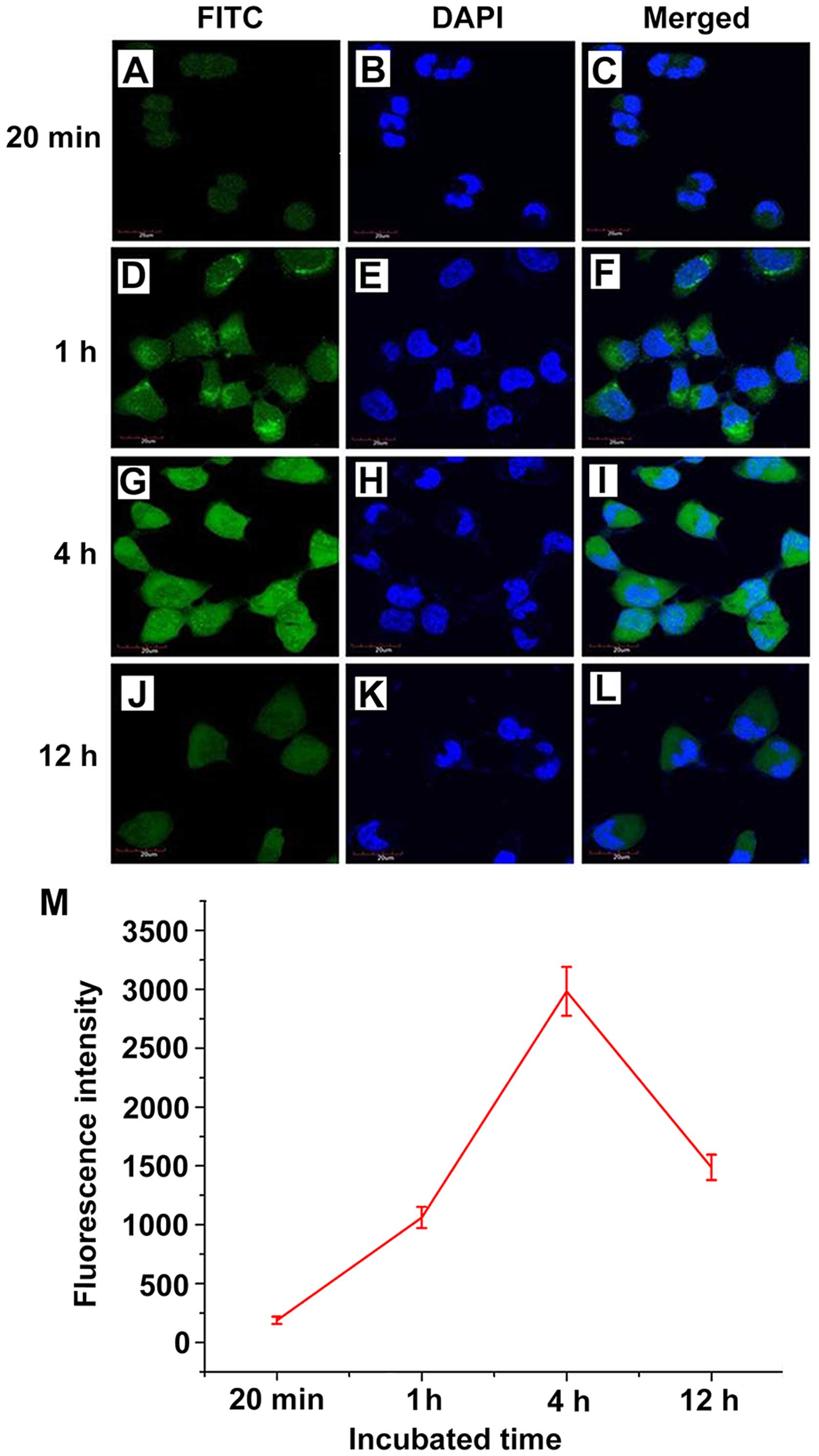
tumor cells was measured by flow cytometry. Cellular fluorescence
intensity in confocal images in the experimental (FITC-NYZL1)
groups was measured at 20 min, 1, 4 and 12 h. Notably, the
FITC-NYZL1 peptide bound to bladder cancer cells in a
time-dependent manner. FITC-NYZL1 bound to BIU-87 cell cytoplasm at
20 min (Fig. 3A–C). After a 1-h
incubation, fluorescein staining was not only detected in the
cytoplasm, but also partially appeared in the nucleoplasm (Fig. 3D–F). After a 4-h incubation,
fluorescein staining in the cytoplasm was significantly increased,
with punctiform accumulation in the nucleus (Fig. 3G–I). After a 12-h incubation,
fluorescein staining in the cytoplasm and nucleus gradually
decreased (Fig. 3J–L).
| Table IIIAverage fluorescence values of
fluorescent probe FITC-NYZL1 binding to different cancer cell
lines. |
Table III
Average fluorescence values of
fluorescent probe FITC-NYZL1 binding to different cancer cell
lines.
| Cell lines | No. of samples | Average
fluorescence value (mean ± SEM) | W-value
(Shapiro-Wilk test) |
|---|
| BIU-87a | 10 |
3660.254±184.532 | 0.927 |
| SMMC-7721 | 10 |
1138.822±127.238 | 0.892 |
| MCF-7 | 10 |
720.534±178.783 | 0.924 |
| SiHa | 10 | 615.094±98.903 | 0.936 |
Competitive experiment
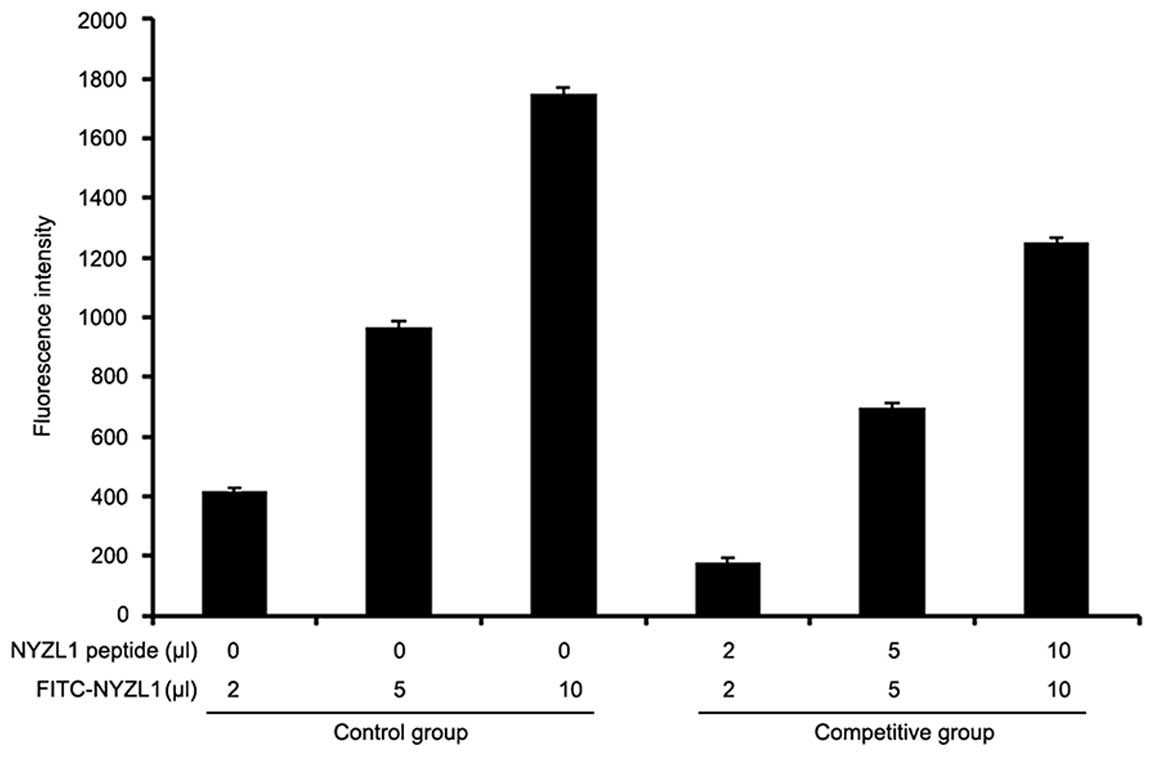
Specificity of the NYZL1 target was assessed by a
competitive assay, using FITC-NYZL1 and the NYZL1 peptide (5 mg/ml)
to co-treat BIU-87 cells. Fluorescence intensity of normal
untreated BIU-87 cells was 15.24±5.1; after treatment of BIU-87
cells with 2, 5 and 10 μl of FITC-NYZL1 alone, fluorescence
intensities of 416.00±13.2, 966.85±20.2 and 1751.45±16.4 were
obtained, respectively, indicating a dose-dependent increase in
fluorescence intensity. Meanwhile, BIU-87 cells co-treated with
FITC-NYZL1 and NYZL1 peptides resulted in reduced fluorescence
intensities of 180.45±12.4, 696.30±16.3, 1253.24±11.5, for 2 5 and
10 μl of FITC-NYZL1, respectively, which were significantly
different compared with the control group (P<0.05) (Fig. 4). These results indicated that the
NYZL1 peptide blocked the binding sites of BIU-87 cells for
NYZL1-FITC.
Detection of exfoliated cells in urine
samples from bladder cancer patients
Next, we examined whether the target peptide could
bind to cells in the urine from bladder cancer patients. The
fluorescent NYZL1 peptide bound to exfoliated cells from urine
sample of bladder cancer patients, unlike the control peptide
FITC-svNYZL1 (Fig. 5A and B).
Little fluorescence by peptide binding was detected with exfoliated
cells from control urine samples of a cystitis patient and a
healthy individual (Fig. 5C and D,
respectively). The percentages of positive peptide bound cells were
relatively high in all urine samples from cancer patients, with
10–48% (mean, 30%) in Ta, 33–78% (mean, 57%) in T1, 58–87% (mean,
73%) in T2, and 71–93% (mean, 85%) in T3–4 stage tumors.
In contrast, fewer positive cells were found in urine samples from
patients with inflammation (0–10%; mean, 6.5%) and healthy
individuals (0–5%; mean, 3%) (Fig.
5E). The binding rates of the FITC-NYZL1 peptide in urine
exfoliated cells showed overt differences in various stages of
cancer; the higher the stage, the higher the specific binding rate.
These findings suggested that the CSNRDARRC peptide is capable of
distinguishing malignant cells from cells that exfoliate from
bladder tumors, inflammatory lesions or normal tissues.
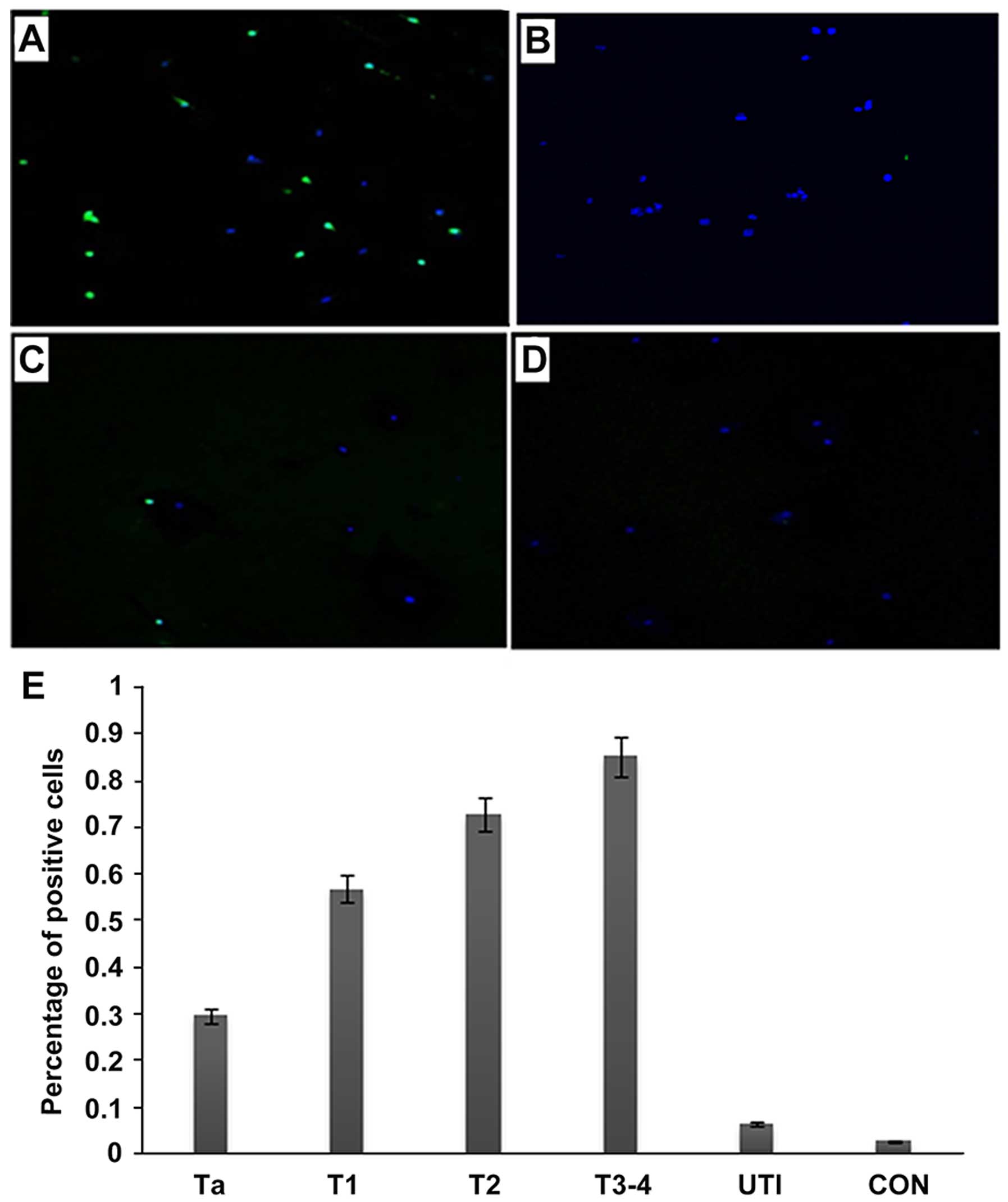 | Figure 5Detection of bladder tumor cells in
the urine with the NYZL1 peptide. Urinary cells were collected from
urine samples of bladder cancer (A and B), cystitis (C) and healthy
control (D) patients. Cells were incubated at 4°C for 1 h with 5
μmol/l solutions of the FITC-NYZL1 peptide (A, C and D) or
FITC-svNYZL1 (B), washed and stained with DAPI for counterstaining,
and assessed by laser scanning confocal microscopy. Images are
merged for the fluorescent peptide and DAPI staining.
Magnification, ×200. (E) A bar graph of tumor or control vs.
percentage of positive cells. Numbers in the vertical axis
represent percentage of positive cells. Ta-T3-4, bladder tumors;
UTI, urinary tract infection; CON, healthy control. The average
intensities (integrated intensity per unit area) of fluorescence in
the tumor and control groups, respectively, were calculated. |
Selective binding of the NYZL1 peptide to
human bladder tumor tissues
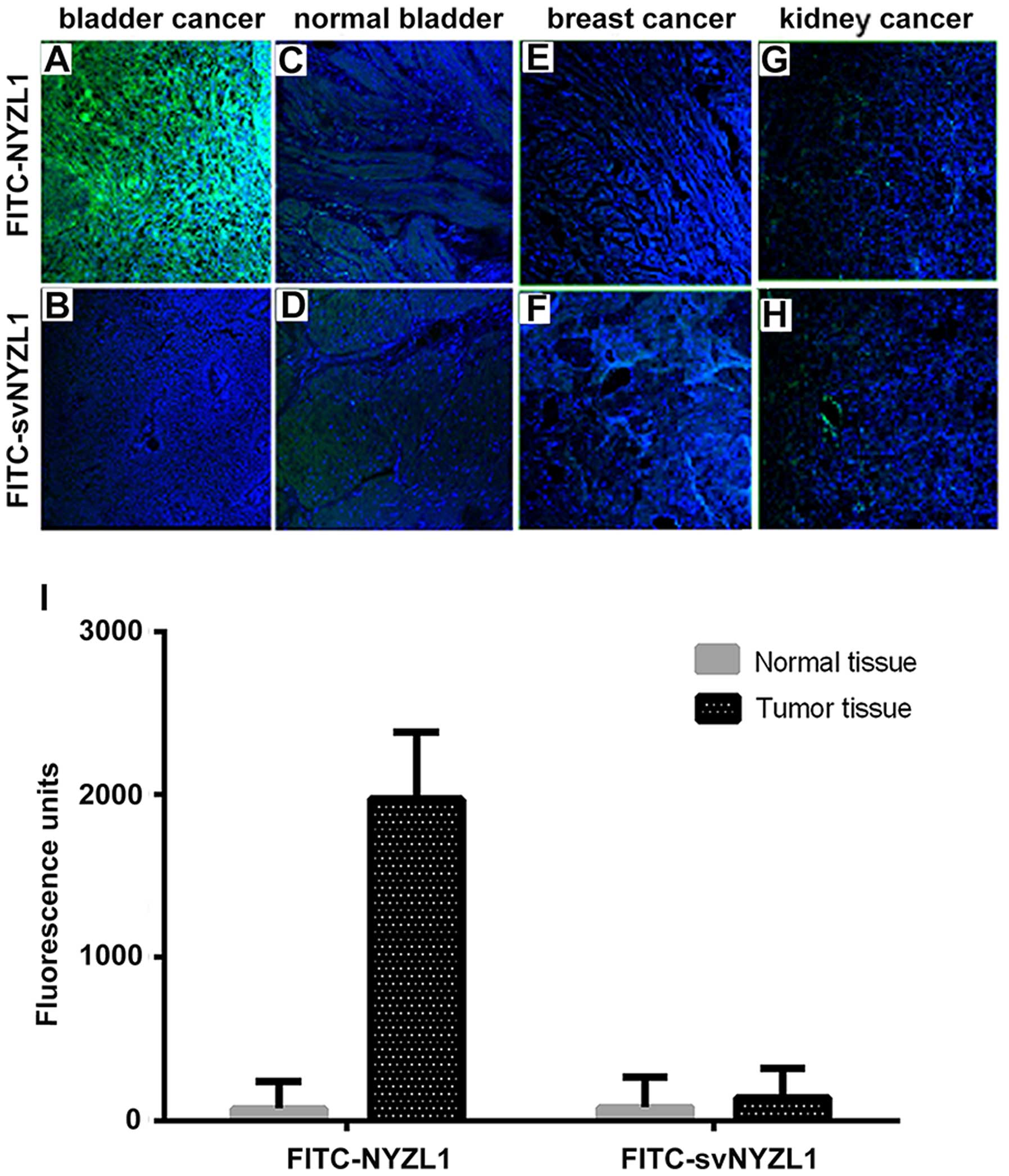
As shown in Fig. 6A,
the synthetic FITC-NYZL1 peptide selectively bound to the primary
bladder cancer tissue. Meanwhile, the scrambled control peptide
FITC-svNYZL1 did not bind significantly to the tumor tissue
(Fig. 6B). In contrast, limited
binding of the FITC-NYZL1 peptide to the adjacent normal bladder
tissue was observed (Fig. 6C).
Quantification of fluorescence intensities in 5 primary bladder
tumor and three normal bladder tissue specimens showed that NYZL1
bound to tumor tissues with a greater strength compared with normal
tissues (Fig. 6I). In addition, the
NYZL1 peptide did not bind to breast and kidney cancer specimens
(Fig. 6E and G), suggesting the
tumor-type specificity of the NYZL1 peptide.
Homing ability of the NYZL1 peptide in
vivo
It was important to determine whether the NYZL1
peptide homes to bladder tumors, allowing in vivo detection
and imaging. FITC-NYZL1 (210 μg) was injected via tail vein
into mice carrying BIU-87 xenograft tumors at 0.8–1.0 cm in
diameter. Tumor tissues and control organs were then excised and
processed for frozen sectioning at 24 h after injection of the
peptide. Immunofluorescence showed that the FITC-NYZL1 peptide
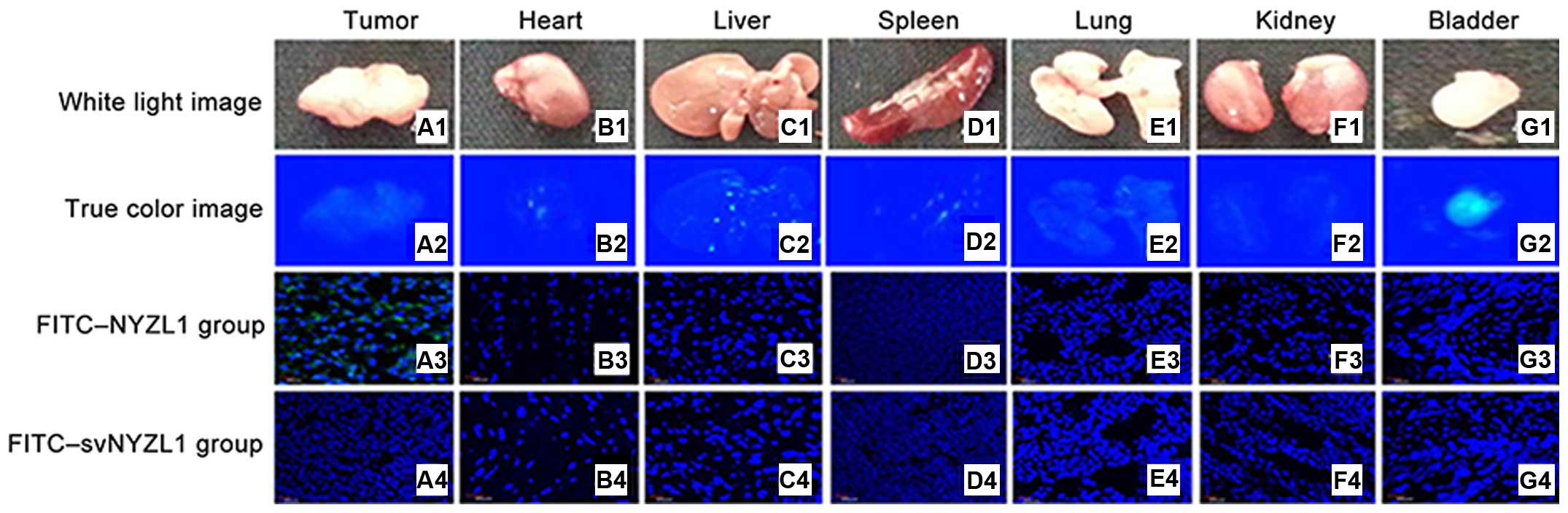
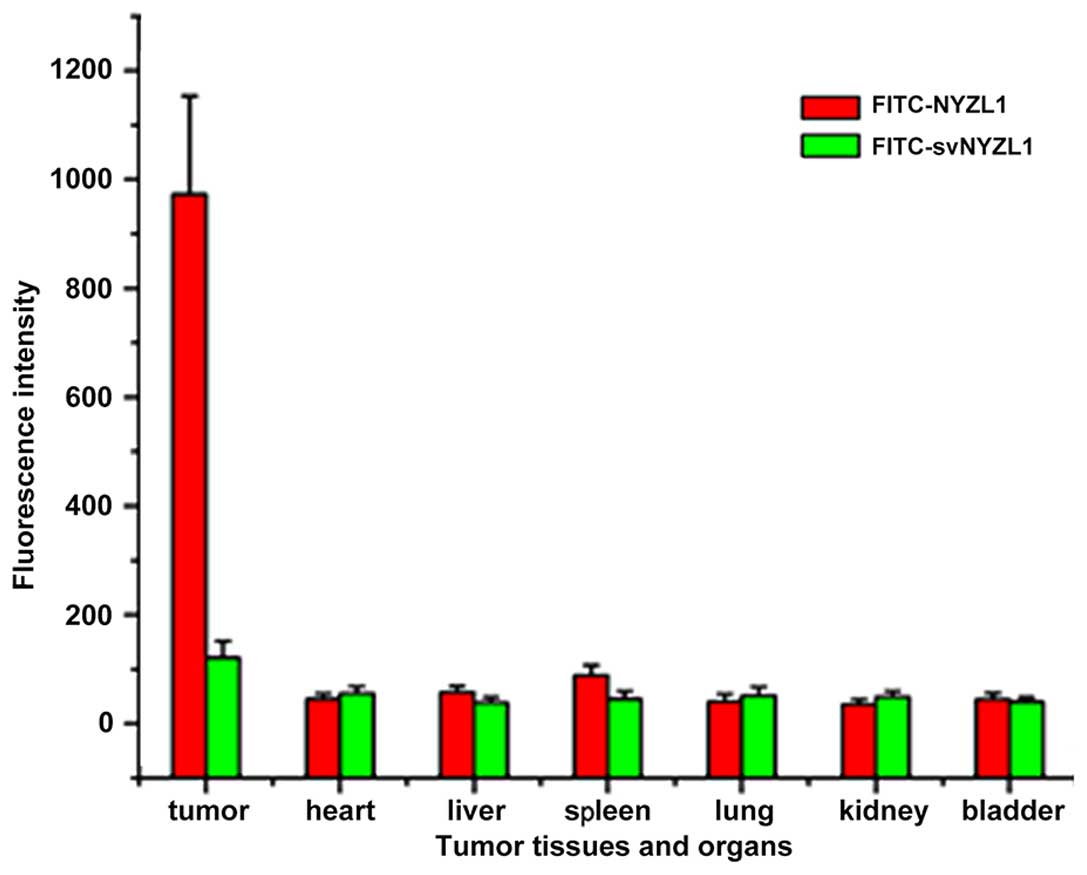
homed to the bladder tumor tissue (Fig.
7A3), but not to other organs such as the bladder, kidney,
heart, lung, liver and spleen (Figs.
7 and 8) of tumor-bearing rats.
By contrast, the scrambled control FITC-svNYZL1 peptide was not
detected in the tumor tissue (Fig.
7A4). These results confirmed that the NYZL1 peptide
specifically homed to bladder tumor tissues.
The NYZL1 peptide delivers fluorescein to
tumor tissues for imaging detection
To determine whether FITC-NYZL1 accumulated in tumor
tissues and can be visualized at the organ level, FITC-NYZL1 or
FITC-svNYZL1 was injected intravenously into mice harboring human
bladder tumor xenografts.
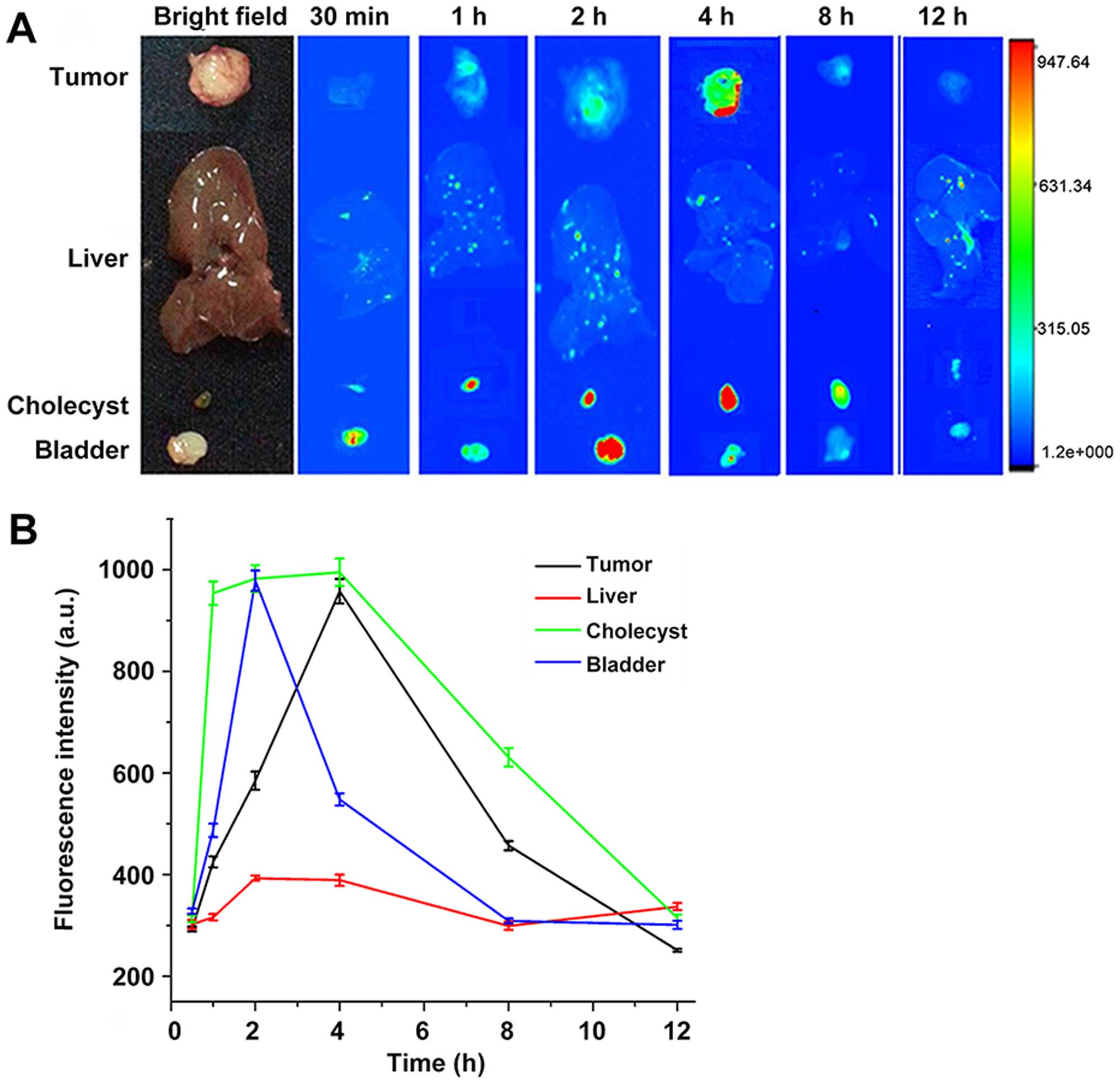
Various tissues and organs, including the implanted
tumor, heart, liver, spleen, lung, kidney, and bladder were
collected at 30 min, 1, 2, 4, 8 and 12 h after peptide injection.
The isolated tissues and organs were examined by fluorescence
microscopy in real-time to trace the fluorescent probe. At first a
portion of the FITC-NYZL1 probe was found in the gallbladder as a
result of metabolism by the liver; at this time, the liver and
gallbladder showed fluorescent signals. Meanwhile, another portion
of the FITC-NYZL1 probe was excreted with urine via the kidneys and
bladder. The remaining portion was concentrated in the targeted
tumor through blood circulation. As a result, fluorescent signals
were found in the bladder and gallbladder soon after probe
injection, and decreased overtime with gradual excretion.
Meanwhile, fluorescence intensity in tumor tissues increased
gradually: it peaked at 4–6 h, before decreasing from the 8 h time
point. The FITC-NYZL1 probe had almost disappeared at 12 h after
injection (Fig. 9A and B).
Considering the presence of fluorescence in tumor cells despite the
lack of signals at the organ and tissue levels, it can be inferred
that NYZL1 shuttled the fluorescent dye to the designated tumor
cells and specifically bound to the target tumor. Fluorescent
microscopy results showed that the fluorescent signal was sustained
for over 24 h at the molecular level, even when it disappeared at
the tissue level. In addition, normal tissues and other organs were
negative for fluorescence. Taken together, these findings confirmed
the homing and binding affinity of the FITC-NYZL1 probe in bladder
tumor cells.
Discussion
In the present study, we used a bladder tumor model
established in BALB/c nude mice by subcutaneous transplantation of
human NMIBC BIU-87 cells for in vivo biopanning of the phage
display library. We isolated a cyclic 7 amino acid peptide
(CSSPIGRHC, named NYZL1) that could specifically bind to the
xenograft bladder tumor. We also showed that the peptide could
recognize human bladder cancer cells, providing targeted delivery
of fluorochrome to the tumor tissue. These data indicated that this
peptide may be a new tool for optical molecular imaging diagnosis
of NMIBC.
Cyclic peptides show better biological activity
compared to their linear counterparts due to conformational
rigidity (30). Indeed, the
rigidity of cyclic peptides decreases the entropy term of the Gibbs
free energy, therefore allowing the enhanced binding toward target
molecules, or receptor selectivity. Another benefit from cyclic
structures is the resistance to hydrolysis by exopeptidases due to
the lack of both amino and carboxyl termini. Cyclic peptides can be
resistant even to endopeptidases, as the structure is less flexible
than linear peptides. Various cyclic peptides, though not all, can
cross the cell membrane. In the present study, we screened a cyclic
peptide (CSSPIGRHC) specifically binding to the human NMIBC cell
line BIU-87.
To successfully establish the xenograft bladder
tumor model in BALB/c mice, we used Matrigel, which significantly
promotes the formation and proliferation of tumor xenografts.
Bladder cancer tumors developed in all nude mice when BIU-87 cells
were injected along with Matrigel; this greatly optimized animal
utilization, reduced the experimental period, and provided an
efficient experimental method for modeling of non-muscle-invasive
bladder tumors. Matrigel was kept on ice before use, with
pre-cooled pipettes, tips and tubes used for Matrigel
preparation.
In vivo phage display panning has been
employed to isolate organ homing phages from peptide libraries. In
this method, first published by Pasqualini and Ruoslahti, phage
libraries are injected into the tail vein of mice (31). Shortly thereafter, mice are
sacrificed and the target organs removed. The organ-associated
phages are retrieved and amplified from the homogenized tissues and
the panning is repeated in another mouse. After 3-5 rounds of
panning, several peptide motifs are typically identified for a
given organ (32,33). Using the same technology, tumor
targeting peptides can be identified (34).
In the present study, we obtained a new peptide with
a cyclic structure and specific binding to bladder tumor cell lines
by in vivo phage display panning. This peptide exhibited
specific binding to human bladder cancer cells in culture and
tissues. The CSSPIGRHC phage preferential binding to cultured
BLU-87 human bladder cancer cells was validated by ELISA.
Fluorescence microscopy and AFM studies directly confirmed the
specificity of the NYZL1 peptide. Our results revealed that NYZL1
had stronger binding to BIU-87 cells compared with the other tumor
cells (kidney, breast and cervical cancer cells); however, this
peptide bound to BIU-87 cells with a similar binding strength as
the other bladder cancer cells studied, including T24, E–J and
5637. Fluorescent peptide overlay of tissue sections showed that
the NYZL1 peptide bound to human bladder cancer sections but not to
those of adjacent normal bladder or other tumor tissues. In
addition, NYZL1 peptide-labeled bladder-exfoliated cells were found
in urine samples from bladder cancer patients. These results
indicate that the NYZL1 peptide can distinguish tumor-adjacent
normal mucosa from bladder cancer, and is tumor type specific. This
peptide may be useful as a targeting moiety for selective delivery
of therapeutics, and constitutes a potential diagnostic probe for
the detection of NMIBC.
To confirm the specific homing of NYZL1, we injected
the FITC-NYZL1 probe into tumor-bearing mice. Immunofluorescence
analysis showed that the FITC-NYZL1 peptide homed to bladder tumor
tissues but not normal tissues in tumor-bearing rats. These results
confirmed that the NYZL1 peptide specifically homes to the bladder
tumor tissue. Furthermore, FITC-NYZL1 circulated throughout the
whole body after intravenous injection. A portion of the FITC-NYZL1
probe was transported to the gallbladder via liver metabolism, with
the liver and gallbladder showing fluorescent signals. Another
portion of the FITC-NYZL1 probe was excreted in the urine. The
remaining portion was concentrated in the targeted tumor. As a
result, fluorescent signals appeared in the bladder and gallbladder
soon after probe injection, decreasing overtime with gradual
excretion. Meanwhile, fluorescent intensity in tumor tissues
increased gradually, peaking at 4–6 h and decreasing from the 8 h
time point; almost no signal was found at 12 h after probe
injection (Fig. 5). Considering
that fluorescence of tumor cells was positive at the microscopic
level despite the lack of signal at the organ and tissue levels
(Fig. 4), it can be concluded that
NYZL1 transports the fluorescent dye to designated tumor cells and
specifically binds to the target tumor. Fluorescence microscopy
studies showed that the fluorescent signal was sustained for over
24 h at the molecular level even after it had disappeared at the
tissue level. In addition, normal tissues and organs showed no
fluorescent signals. Taken together, these studies confirmed the
specificity and binding affinity of the FITC-NYZL1 probe in
targeted tumor cells, with binding time more than 24 h.
We attempted to identify peptides specifically
targeting bladder tumors to guide optical molecular cystoscopic
imaging for diagnosis of tiny or residual tumors. One potential
application of such specific peptide homing to tumor vasculature is
to deliver toxins or pro-drug molecules as targeted therapeutic
agents to increase the efficacy of anticancer therapy and decrease
the undesired systemic side-effects in other tissues (14,35).
The peptide NYZL1 is very appropriate for labeling with
fluorophores for optical molecular cystoscopy diagnosis and
treatment of NMIBC.
In summary, we successfully applied the in
vivo phage display biopanning approach to identify the peptide
CSSPIGRHC (NYZL1), which targets bladder cancer. The present study
is the first to describe the NYZL1 peptide specifically binding to
Chinese bladder cancer. We demonstrated the specificity and homing
ability of NYZL1. Tumor homing peptide can be widely used in
diagnostic and therapeutic models by conjugating them with
anticancer drugs or imaging particles. The potential clinical
applications include tumor localization to guide transurethral
resection of bladder tumors, imaging detection, and targeted drug
delivery for noninvasive bladder cancer.
Acknowledgments
The present study was carried out as part of a study
on the ̔Diagnosis of bladder tumor by targeting peptide mediated
optical molecular imaging̓ (no. 81172444), supported by the
National Natural Science Foundation of China.
References
|
1
|
Ploeg M, Aben KK and Kiemeney LA: The
present and future burden of urinary bladder cancer in the world.
World J Urol. 27:289–293. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Babjuk M, Oosterlinck W, Sylvester R,
Kaasinen E, Böhle A and Palou-Redorta J: European Association of
Urology (EAU): EAU guidelines on non-muscle-invasive urothelial
carcinoma of the bladder. Eur Urol. 54:303–314. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kirkali Z, Chan T, Manoharan M, Algaba F,
Busch C, Cheng L, Kiemeney L, Kriegmair M, Montironi R, Murphy WM,
et al: Bladder cancer: Epidemiology, staging and grading, and
diagnosis. Urology. 66(Suppl 1): S4–S34. 2005. View Article : Google Scholar
|
|
4
|
Sylvester RJ, van der Meijden AP,
Oosterlinck W, Witjes JA, Bouffioux C, Denis L, Newling DW and
Kurth K: Predicting recurrence and progression in individual
patients with stage Ta T1 bladder cancer using EORTC risk tables: a
combined analysis of 2596 patients from seven EORTC trials. Eur
Urol. 49:466–477. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Hall MC, Chang SS, Dalbagni G, Pruthi RS,
Seigne JD, Skinner EC, Wolf JS Jr and Schellhammer PF: Guideline
for the management of nonmuscle invasive bladder cancer (stages Ta,
T1, and Tis): 2007 update. J Urol. 178:2314–2330. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Botteman MF, Pashos CL, Redaelli A, Laskin
B and Hauser R: The health economics of bladder cancer: A
comprehensive review of the published literature.
Pharmacoeconomics. 21:1315–1330. 2003. View Article : Google Scholar
|
|
7
|
Riley GF, Potosky AL, Lubitz JD and
Kessler LG: Medicare payments from diagnosis to death for elderly
cancer patients by stage at diagnosis. Med Care. 33:828–841. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Liu JJ, Droller MJ and Liao JC: New
optical imaging technologies for bladder cancer: Considerations and
perspectives. J Urol. 188:361–368. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Weissleder R: Molecular imaging in cancer.
Science. 312:1168–1171. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kwon YS, Cho YS, Yoon TJ, Kim HS and Choi
MG: Recent advances in targeted endoscopic imaging: Early detection
of gastrointestinal neoplasms. World J Gastrointest Endosc.
4:57–64. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Mahmood U and Wallace MB: Molecular
imaging in gastrointestinal disease. Gastroenterology. 132:11–14.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Cheng L, Davison DD, Adams J,
Lopez-Beltran A, Wang L, Montironi R and Zhang S: Biomarkers in
bladder cancer: Translational and clinical implications. Crit Rev
Oncol Hematol. 89:73–111. 2014. View Article : Google Scholar
|
|
13
|
Muguruma N, Miyamoto H, Okahisa T and
Takayama T: Endoscopic molecular imaging: Status and future
perspective. Clin Endosc. 46:603–610. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Vlieghe P, Lisowski V, Martinez J and
Khrestchatisky M: Synthetic therapeutic peptides: Science and
market. Drug Discov Today. 15:40–56. 2010. View Article : Google Scholar
|
|
15
|
Lee SM, Lee EJ, Hong HY, Kwon MK, Kwon TH,
Choi JY, Park RW, Kwon TG, Yoo ES, Yoon GS, et al: Targeting
bladder tumor cells in vivo and in the urine with a peptide
identified by phage display. Mol Cancer Res. 5:11–19. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Zhang H, Aina OH, Lam KS, de Vere White R,
Evans C, Henderson P, Lara PN, Wang X, Bassuk JA and Pan CX:
Identification of a bladder cancer-specific ligand using a
combinatorial chemistry approach. Urol Oncol. 30:635–645. 2012.
View Article : Google Scholar
|
|
17
|
Gautam A, Kapoor P, Chaudhary K, Kumar R
and Raghava GP and Raghava GP: Open Source Drug Discovery
Consortium: Tumor homing peptides as molecular probes for cancer
therapeutics, diagnostics and theranostics. Curr Med Chem.
21:2367–2391. 2014. View Article : Google Scholar
|
|
18
|
Babjuk M, Burger M, Zigeuner R, Shariat
SF, van Rhijn BW, Compérat E, Sylvester RJ, Kaasinen E, Böhle A,
Palou Redorta J, et al: European Association of Urology: EAU
guidelines on non-muscle-invasive urothelial carcinoma of the
bladder: Update 2013. Eur Urol. 64:639–653. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Geavlete B, Jecu M, Multescu R, Georgescu
D and Geavlete P: HAL blue-light cystoscopy in high-risk
nonmuscle-invasive bladder cancer - re-TURBT recurrence rates in a
prospective, randomized study. Urology. 76:664–669. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Smith GP: Filamentous fusion phage: Novel
expression vectors that display cloned antigens on the virion
surface. Science. 228:1315–1317. 1985. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Li M, Gu FL, Li WB, Song YS, Zhou AR and
Guo YL: Introduction of wild-type p53 gene downregulates the
expression of H-ras gene and suppresses the growth of bladder
cancer cells. Urol Res. 23:311–314. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhou HL, Zheng YJ, Cheng XZ, Lv YS, Gao R,
Mao HP and Chen Q: Intercellular transfer of P-glycoprotein from
the drug resistant human bladder cancer cell line BIU-87 does not
require cell-to-cell contact. J Urol. 190:1069–1075. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Chen J, Ou-Yang X, Gao J, Zhu J, He X and
Rong J: Knockdown of ribonuclease inhibitor expression with siRNA
in non-invasive bladder cancer cell line BIU-87 promotes growth and
metastasis potentials. Mol Cell Biochem. 349:83–95. 2011.
View Article : Google Scholar
|
|
24
|
Fridman R, Benton G, Aranoutova I,
Kleinman HK and Bonfil RD: Increased initiation and growth of tumor
cell lines, cancer stem cells and biopsy material in mice using
basement membrane matrix protein (Cultrex or Matrigel)
co-injection. Nat Protoc. 7:1138–1144. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Lewis MT, Landua JD, Adams HC III and
Medina D: A mystery wrapped in an enigma: Matrigel enhancement of
mammary cell growth and morphogenesis. J Mammary Gland Biol
Neoplasia. 17:99–101. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Green MR and Sambrook J: Molecular
Cloning: A Laboratory Manual. Cold Spring Harbor Laboratory Press;
New York: 2012
|
|
27
|
Koivistoinen A, Ilonen II, Punakivi K,
Räsänen JV, Helin H, Sihvo EI, Bergman M and Salo JA: A novel
peptide (Thx) homing to non-small cell lung cancer identified by ex
vivo phage display. Clin Transl Oncol. 15:492–498. 2013. View Article : Google Scholar
|
|
28
|
Zhang L, Giraudo E, Hoffman JA, Hanahan D
and Ruoslahti E: Lymphatic zip codes in premalignant lesions and
tumors. Cancer Res. 66:5696–5706. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Pilch J, Brown DM, Komatsu M, Järvinen TA,
Yang M, Peters D, Hoffman RM and Ruoslahti E: Peptides selected for
binding to clotted plasma accumulate in tumor stroma and wounds.
Proc Natl Acad Sci USA. 103:2800–2804. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Horton DA, Bourne GT and Smythe ML:
Exploring privileged structures: The combinatorial synthesis of
cyclic peptides. J Comput Aided Mol Des. 16:415–430. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Pasqualini R and Ruoslahti E: Organ
targeting in vivo using phage display peptide libraries. Nature.
380:364–366. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Essler M and Ruoslahti E: Molecular
specialization of breast vasculature: A breast-homing
phage-displayed peptide binds to aminopeptidase P in breast
vasculature. Proc Natl Acad Sci USA. 99:2252–2257. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Kolonin MG, Saha PK, Chan L, Pasqualini R
and Arap W: Reversal of obesity by targeted ablation of adipose
tissue. Nat Med. 10:625–632. 2004. View
Article : Google Scholar : PubMed/NCBI
|
|
34
|
Arap W, Pasqualini R and Ruoslahti E:
Cancer treatment by targeted drug delivery to tumor vasculature in
a mouse model. Science. 279:377–380. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Craik DJ, Fairlie DP, Liras S and Price D:
The future of peptide-based drugs. Chem Biol Drug Des. 81:136–147.
2013. View Article : Google Scholar
|