Introduction
Manumycin A is a natural antibiotic isolated from
Streptomyces parvulus with various biological activities
that can act as a competitive Ras farnesyltransferase inhibitor or
irreversible inhibitor of neutral sphingomyelinase. Manumycin A as
a single agent and also in two- or triple-drug combinations showed
in vitro and in vivo anticancer activity based on its
cytotoxic, antiproliferative, proapoptotic, proautophagic,
antiangiogenic and antimetastatic properties in various
experimental models of fibrosarcoma (1), pancreatic (2) and anaplastic thyroid cancer (3), glioma (4), lymphoma (5) and others. Manumycin A has been shown
to be effective against aggressive and therapy-resistant
triple-negative breast cancer (6).
However, in addition to its anticancer properties, manumycin A also
exerts beneficial effects on atherosclerosis (7) and immunomodulatory properties
including modification of pro-inflammatory responses in glioma and
non-glioma tumor cells through abrogation of IL-1β-induced HIF-1α
activation in tumor cells (8),
suppression of interferon-γ and tumor necrosis factor-α in
BALB/c-mice (9) and downregulation
of mRNA for IL-6, TLR-8, IL-1β and inhibition of IL-1β, IL-6 and
IL-8 production in human monocytes (10).
Immodin [also known as DLE or transfer factor (TF)]
is a leukocyte immunomodulator and represents dialyzable leukocyte
extracts (DLEs) released from disintegrated blood leukocytes of
healthy human donors which are able to transfer cell-mediated
immunity from sensitized donors to naive recipients. The benefits
of TF were discovered ~50 years ago and the clinical experience is
based on the extensive research conducted by numerous groups
worldwide (11,12). DLE or TF preparations have been
reported as beneficial in a broad spectrum of pathologies caused by
microbial agents (13; reviewed in ref. 14) and in various diseases including
allergies, rhinitis (15), asthma
and atopic dermatitis (16), also
sepsis (17) and rheumatoid
arthritis (18). In the context of
cancer therapy, DLE was found to be effective as an adjuvant to
chemotherapy in patients with osteosarcoma (19), non-small cell lung (20,21)
and breast cancer (22), in
experimental glioma (23), and DLE
improved survival in patients with bronchogenic carcinoma (24) and prostate cancer (25). In regard to cancer, the mechanisms
that underlie the immunomodulatory effects of DLE have not been
elucidated.
The key steps in breast tumor progression, including
cellular transformation, proliferation, tumor cell survival and
angiogenesis, can be mediated by components of the hemostatic
system (26). Platelets as part of
the circulatory system play a fundamental role in maintaining
hemostasis. However, in addition to this role, they are also
important factors in inflammation, atherosclerosis and cancer
dissemination. Complex interactions between tumor cells and
circulating platelets play an important role in cancer growth and
dissemination (27). Platelets
guard tumor cells from immune elimination and promote their arrest
at the endothelium (28). The
growing tumor can enhance the production and activation of
platelets, thereby potentially creating a positive feedback loop to
fuel tumor growth (29). In
addition, a tumor produces high levels of cytokines and growth
factors known to promote tumor growth and metastasis and these
factors can be sequestered in and released by platelets (30). These pro-tumorigenic effects make
platelets a rational target for anticancer therapy.
The other components of the circulatory system,
neutrophils and eosinophils, are essential parts of innate
immunity. However, in addition to their important role in fighting
infections and inflammation, they play a critical role in the
development of effective antitumor immunity (31). The infiltration of neutrophils
and/or eosinophils in colorectal and primary small cell esophageal
carcinoma was found to be associated with a good prognosis and
enhanced survival of patients (32–34).
Studies using in vivo models reported that tumor-homing
neutrophils and/or eosinophils were essential for tumor rejection
by initiation of changes in the tumor microenvironment (35–37).
In the present study, we used a strongly immunogenic
4T1 mouse model as a well characterized system to replicate stage
IV breast cancer for evaluation of the antitumor potential of a
novel combination of the natural drug manumycin A and the
immunomodulator Immodin.
Materials and methods
Ethical approval
The State Veterinary and Food Administration of the
Slovak Republic approved the experimental protocol (no.
4296/12-221e), and the animals were handled and sacrificed in a
humane manner in accordance with the guidelines established by the
relevant commission.
Reagents
Manumycin A and Immodin were purchased from
Sigma-Aldrich (St. Louis, MO, USA) and IMUNA PHARM (Šarišské
Michaľany, Slovakia), respectively. The drugs were freshly prepared
on the day of use. Immodin was prepared by dissolving the
lyophilized dialysate of 200×106 leukocytes in water for
injection. Manumycin A was resuspended in vehiculum (1% Cremophor
oil in deionized water; Sigma-Aldrich) to reach the concentration
of 0.5 mg/ml.
Cell line
4T1 mouse mammary carcinoma cell line was purchased
from the American Type Culture Collection (ATCC; Rockville, MD,
USA). Cells were maintained in RPMI-1640 medium enriched with 5 mM
glutamate and 10% heat non-inactivated fetal bovine serum (FBS)
(both from Thermo Fisher Scientific, Waltham, MA, USA) and
maintained in a humidified incubator at 37°C in an atmosphere of 5%
CO2. Media were gentamicin- and antiobiotic-free.
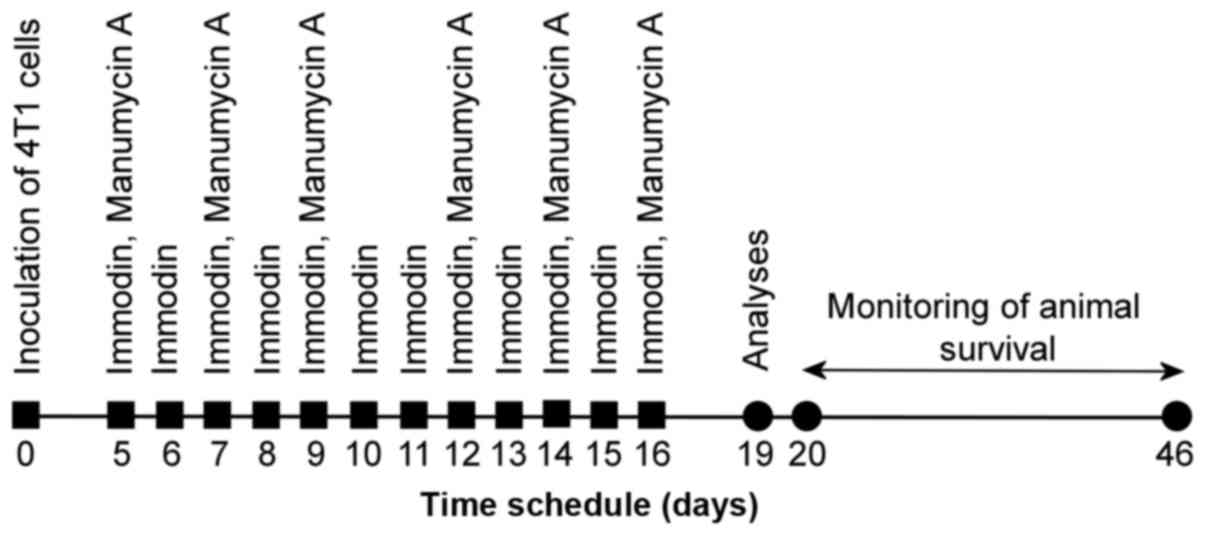
Animal model, cancer cell inoculation
and experimental design/drug treatment
Female BALB/c mice (Velaz, Prague, Czech Republic)
at 10 weeks of age were used in the experiments. The animals were
adapted to standard vivarium conditions with temperature 22±2°C,
relative humidity 45–60%, artificial regimen (L/D 12:12 h). During
the experiment, the animals were fed with a standard MP-OŠ-06 diet
(Biofer, Veľký Šariš, Slovakia) and water ad libitum. Mouse
mammary adenocarcinoma 4T1 cells (1×105 cells/mouse)
were inoculated subcutaneously in the abdominal mammary gland of
syngeneic BALB/c mice on day 0. The growth of tumors was monitored
from the third day after 4T1 cell inoculation and the size of
palpated tumors for each mouse individually was recorded. Animals
were randomized into 6 experimental groups (25 animals/group):
untreated control (C); Immodin-treated (IM); tumor control (4T1);
4T1 treated with Immodin (4T1 + IM); 4T1 treated with manumycin A
(4T1 + MANU); 4T1 treated with Immodin and manumycin A (4T1 + IM +
MANU). Drug administration was initiated on day 5 after cell
inoculation corresponding to the onset of palpable tumors. Immodin
was administered intraperitoneally to mice 12 times at the
concentration of 0.05 IU/mouse alone or along with manumycin A
administered perorally at the dose of 100 µg/mouse (6 times, every
second day) after the onset of palpable tumors. Seventy-two hours
after the final Immodin and/or manumycin A administration, 10
animals from each group were sacrificed by cervical dislocation
under anesthesia. Details of the experimental scheme are shown in
Fig. 1.
Tumor weight, tumor volume and animal
survival
During the autopsy of 10 mice/group, each primary
tumor was isolated, measured and weighed on digital scales and 5 of
the tumors were processed for histological analysis. The volume (V)
of tumors was calculated based on its diameters S1 and
S2 (S1<S2) using the formula V
= π × (S1)2 × S2/12. The remaining
15 animals/group were used for the evaluation of the survival of
the animals by recording the number of dead animals each day.
Starting the day after analysis, the survival times of 15
animals/group were reported as the percentage of animals surviving
the following 27 days. Animals in this experiment were sacrificed
when moribund. On day 28, the surviving mice were euthanized by
cervical dislocation. Survival data were analyzed by the program
MedCalc (http://www.medcalc.org/manual/kaplan-meier.php) as
well as by GraphPad Prism software (version 5.01) (GraphPad
Software, Inc., San Diego, CA, USA) and are presented in the
Kaplan-Meier survival curves.
Blood and serum analysis
Blood samples were collected shortly before cervical
dislocation by retro-orbital bleeding in 1-ml
K3EDTA-containing tubes, 2-ml heparin-containing tubes
and 2-ml serum collection tubes and stored at 4°C. Samples with
whole blood in K3EDTA tubes (both from Sarstedt,
Nümbrecht, Germany) were analyzed using an automated veterinary
hematology analyzer (Mindray BC 2800VET; Mindray, Shenzhen, China).
Refrigerated samples were warmed to room temperature (RT) for 30
min before analysis. Plasma/serum tubes were placed on ice, blood
for serum collection was allowed to clot for at least 30 min and
subsequently both tubes were centrifuged at 2,400 × g at 4°C for 15
min. Serum samples were stored at 4°C and biochemical analyses were
performed over 2 consecutive days using an automated clinical
chemistry analyzer (ELLIPSE; AMS SpA, Rome, Italy) according to the
manufacturer's instructions.
Leukocyte differential count
Air-dried smears of blood were stained with
May-Grünwald/Giemsa stain and scanned using a light microscope
(Leica DM500; Leica, Wetzlar, Germany) at a magnification of ×1,000
using oil immersion following standard routines. In each
microscopic field, the leukocytes were classified as lymphocytes,
monocytes, eosinophils, neutrophils and basophils. In each smear,
we counted 150–200 leukocytes/sample/mouse/group. The mean cell
numbers were calculated after scoring smears from 10 mice/group.
The neutrophil-lymphocyte ratio (NLR) was calculated from the white
cell differential count.
Flow cytometric analysis of leukocyte
phagocytic activity
The phagocytic activity of blood monocytes and
neutrophils was quantitatively determined using a commercial test
kit (FagoFlowEx kit; EXBIO, Praha, Czech Republic) which is based
on the ingestion of FITC-labeled Escherichia coli (E.
coli) bacteria by phagocytes. Briefly, 100 µl of heparinized
whole blood was incubated at 37°C for 10 min with 20 µl E.
coli bacteria that were opsonized with immunoglobulin and
complement and fluorescein (FITC)-labeled. Control samples were
incubated in an ice bath. Phagocytosis was stopped by placing the
sample on ice and adding a solution that quenches the FITC
fluorescence of surface bound bacteria, leaving the fluorescence of
internalized particles unaltered. After two washing steps,
erythrocytes were lysed by adding a BD FACS lysing solution
(Becton-Dickinson Biosciences, San Jose, CA, USA) and incubating
for 20 min at RT, followed by an additional washing. A DNA staining
solution was added prior to flow cytometric analysis, to exclude
aggregation artefacts of bacteria or cells. Samples were kept on
ice, and analyzed within 30 min of preparation using a BD
FACSCanto™ flow cytometer (Becton-Dickinson Biosciences) and
analyzed by BD FACSDiva™ software. Fluorescence measurements were
carried out using a 488 nm blue excitation laser. Bacteria were
excluded using the red fluorescence histogram (FL2) where
leukocytes have higher DNA content as compared to bacteria.
Neutrophils and monocytes were gated separately on FSC vs. SSC dot
plot and their green fluorescence histograms (FL1) were analyzed.
The results are expressed as a percentage.
Histological analysis of tumor
sections
Tumors isolated from 5 animals from each
experimental group were fixed in 4% paraformaldehyde in
phosphate-buffered saline (PBS) (pH 7.2) for 24 h at 4°C, washed in
tap water for 5 h and processed for preparation of paraffin
sections according to the standard protocol. Tumors were embedded
in low melting paraffin (Paraplast; Sigma-Aldrich) and the sections
(7-µm thick) were used for a set of staining procedures. Using the
standard protocol, some slides were stained with Mayer's
hematoxylin/eosin and other slides were used to localize
granulocytes after modified Sirius red staining protocol originally
described by Llewellyn (38).
Briefly, dehydrated sections were placed in Harris hematoxylin (pH
≤5.0) for 3 min, were rinsed in running tap water and briefly
immersed in 100% ethanol. This nuclear staining was followed by the
staining of eosinophilic granules by alkaline Sirius red stain
(without sodium chloride, pH 8.5) (Sigma-Aldrich), in which slides
were immersed for 1 h. After rinsing the slides in tap water for 5
min, sections were dehydrated in a set of graded alcohols and
cleared in HistoChoice clearing solution (Amresco, Solon, OH, USA).
Finally, sections were mounted into permanent medium HistoChoice
mounting fluid (Amresco). After staining, granules of eosinophils
were observed as bright red, whereas granules of neutrophils were
not visible and both cell types could also be discriminated by the
shape of nuclei stained dark blue. The morphometric analysis of
both cell types was carried out at a magnification of ×1,000 using
Olympus Microscope BX51 and a digital analysis imaging system
‘Analysis Docu’ (Soft Imaging Systems 3.0; Prague, Czech Republic).
After analysis of an average 30 screen fields on the sections of
individual tumors the mean number of counted cells for each section
was calculated for 0.1 mm2 of tissue area. Finally, the
mean number of the cells recorded for the sections of tumors from 5
mice were calculated showing data for 0.1 mm2.
Statistical analyses
All results were analyzed using GraphPad Prism
software (version 5.01) for normal distribution. All data were
examined for normal distribution and then the appropriate tests
were applied. Statistical differences between groups were analyzed
using ANOVA followed by Tukey's post hoc test or ANOVA
(Kruskal-Wallis test) followed by pairwise multiple comparison
procedures (Dunn's method) or Mann-Whitney rank-sum test. For
Kaplan-Meier survival analysis, a log-rank (Mantel-Cox) test was
applied. All differences were considered statistically significant
at P<0.05. For ethical reasons, when possible and appropriate,
different tissues, organs and whole blood samples from one animal
were used for several measurements (i.e., samples for determination
of different parameters in whole blood were obtained from the same
animals).
Results
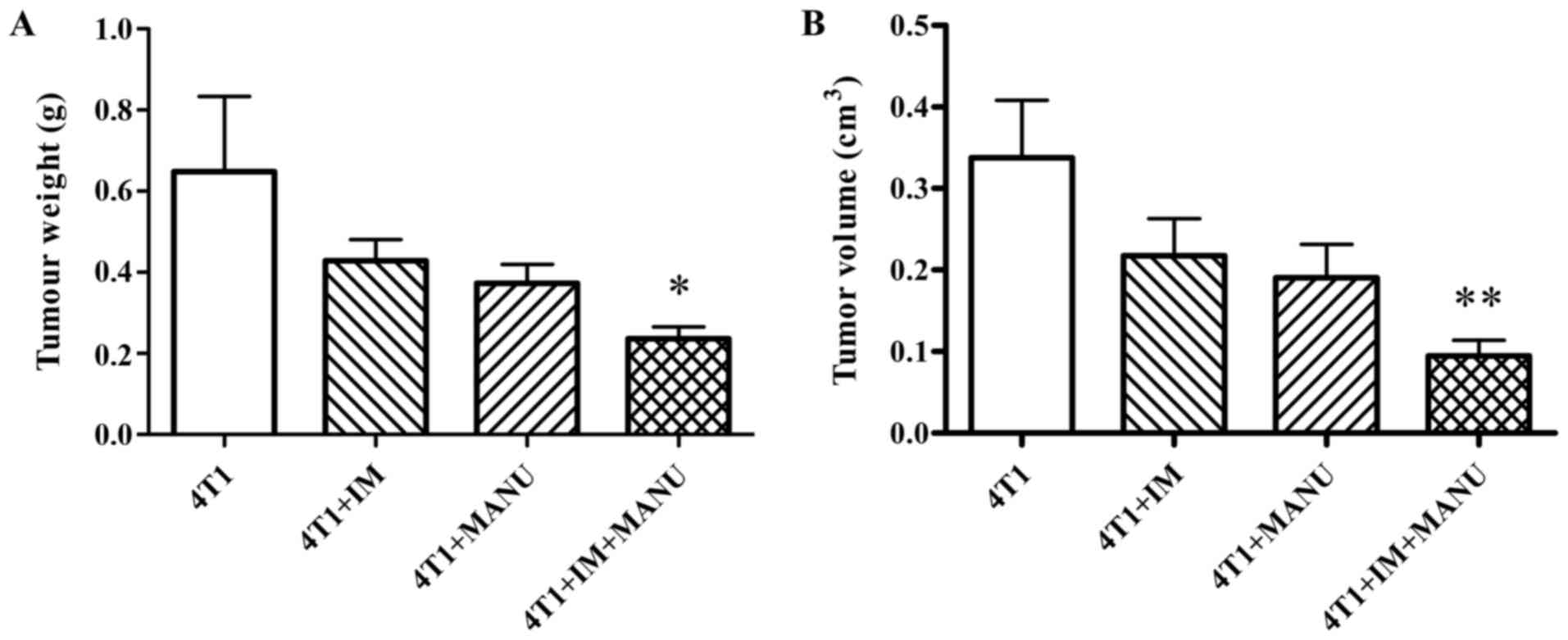
Tumor weight and tumor volume
Single agent treatments with Immodin and manumycin A
resulted in a non-significant decrease in tumor weight and volume
compared to the untreated 4T1 group. The combination treatment more
efficiently reduced the tumor weight (P<0.01; Fig. 2A) and volume (P<0.05; Fig. 2B) compared to the untreated 4T1
group.
Animal survival
Every experimental group of tumor-bearing mice had a
decreased survival compared to the survival noted in the control
and Immodin group (P<0.0001). All the treatments prolonged the
survival of the tumor-bearing mice compared to that of the
untreated 4T1 group (P<0.0001), but the most pronounced effect
was observed after combined therapy. The Kaplan-Meier curves for
all treatment groups showing the percentage of animals surviving
vs. time are presented in Fig.
3.
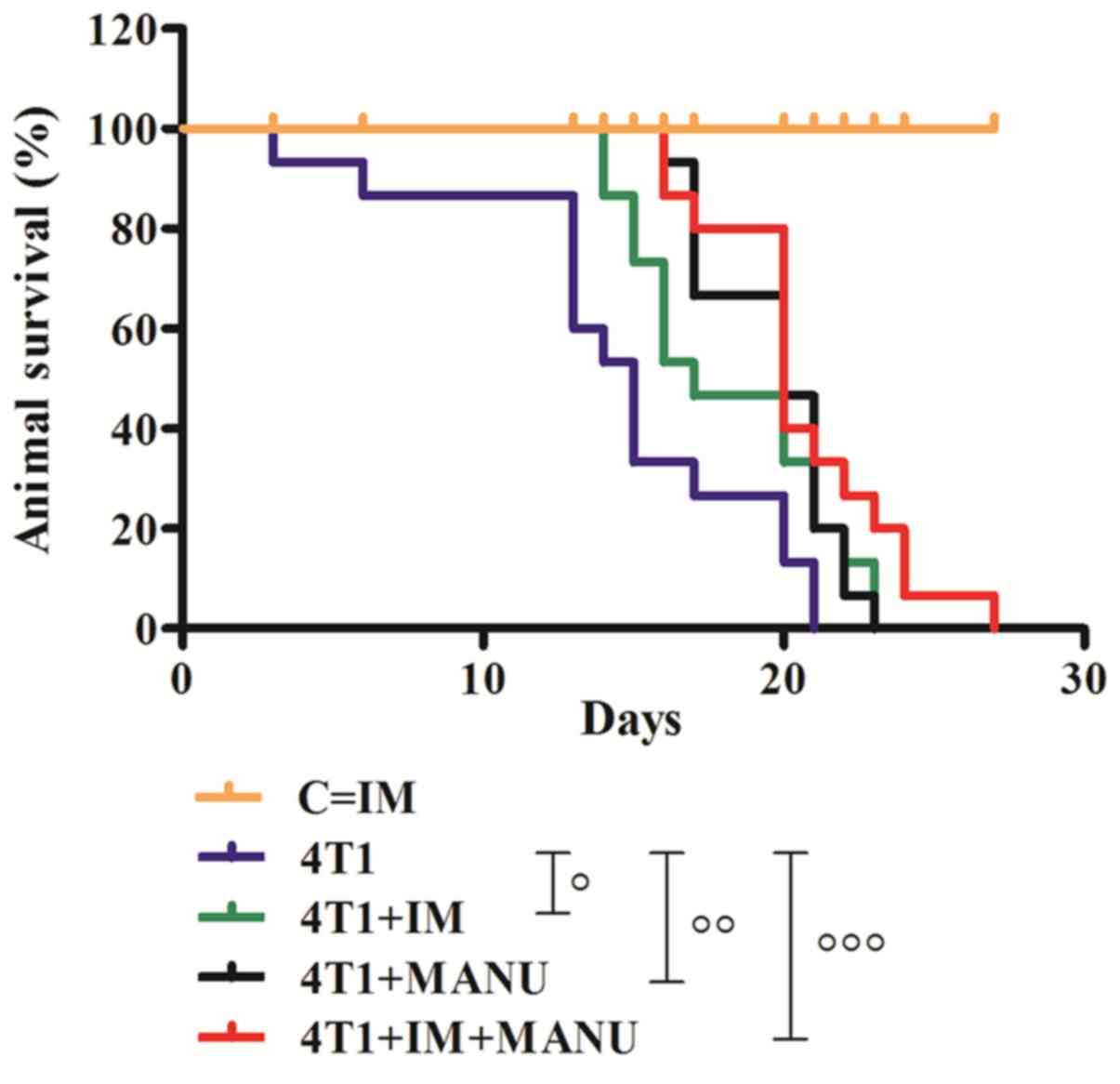 | Figure 3.Effect of the treatments on animal
survival. Kaplan-Meier survival curves (n=15) were compared using
log-rank test (Mantel-Cox); P=0.0312 (4T1 vs. 4T1 + IM), P=0.0019
(4T1 vs. 4T1 + MANU), P<0.0007 (4T1 vs. 4T1 + IM + MANU);
○P<0.05, ○○P<0.01,
○○○P<0.001). C, untreated control; IM, Immodin
treatment; 4T1, tumor control; 4T1 + IM, 4T1 treated with Immodin;
4T1 + MANU, 4T1 treated with manumycin A; 4T1 + IM + MANU, 4T1
treated with Immodin and manumycin A. |
Hematological parameters
The number (both the percentage and count) of
monocytes was significantly increased in the untreated as well as
this number in the treated 4T1 groups compared to the control
(P<0.001 for 4T1 and 4T1 + IM; P<0.01 for 4T1 + MANU;
P<0.05 for 4T1 + IM + MANU). While the monocyte count was
significantly decreased after treatment with the drug combination
when compared to the count noted in the untreated 4T1 group
(P<0.05), the percentage of monocytes was not significantly
different between the untreated and treated 4T1 groups. The
platelet count was significantly increased in the 4T1 group
compared to that in the untreated control (P<0.05). The combined
treatment prevented this increase; the platelet count in this group
was significantly decreased compared to the count in the untreated
4T1 group (P<0.01) and the count reached the level similar to
that of the control group. In addition, the platelet count
decreased following single treatments compared to the count in the
untreated 4T1 group, although these differences were not
significant. There was also a significant increase in plateletcrit
(PCT) in the 4T1 group compared to that in the control (P<0.01).
Treatment with manumycin A (P<0.05) or the drug combination
(P<0.001) caused a decrease in plateletcrit compared to that in
the untreated 4T1 group. While the percentage of peripheral blood
lymphocytes decreased in all 4T1 groups compared to the control
(P<0.001), the lymphocyte count was elevated in these groups
compared to the count noted in the control (P<0.01). Comparison
of the number or percentage of granulocytes and lymphocytes
revealed a reversal of granulocyte-lymphocyte ratio in the
tumor-bearing mice, with an 18- and 3-fold increase in the number
and percentage of granulocytes. In addition, almost all
hematological parameters in the 4T1 group showed a significant
difference compared to the control (increase in red blood cell
parameters RBC, HCT, HGB, RDW, MCHC and MCH) but neither the single
nor the combination treatment affected these changes (Table I).
 | Table I.Effect of the treatments on
hematological parameters. |
Table I.
Effect of the treatments on
hematological parameters.
|
| C | IM | 4T1 | 4T1 + IM | 4T1 + MANU | 4T1 + IM +
MANU |
|---|
| Total WBCs
(×109/l) | 6.19±0.47 | 14.33±2.66 |
31.34±9.37a |
43.10±6.00c |
35.50±6.79b |
31.38±2.51b |
| Monocytes
(×109/l) | 0.17±0.03 | 0.88±0.26 |
2.32±0.46c |
1.85±0.19c |
1.58±0.20b |
1.13±0.08a,d |
| Monocytes (%) | 2.79±0.25 | 2.70±0.14 |
4.92±0.34c |
4.20±0.39a |
4.14±2.6a |
4.10±0.35a |
| Lymphocytes
(×109/l) | 4.74±0.38 | 9.23±1.71 |
13.72±2.43b |
11.84±1.11b | 9.2±1.25 | 10.3±0.82 |
| Lymphocytes
(%) | 76.63±2.04 | 69.25±4.78 |
38.00±6.47c |
29.74±2.65c |
32.63±4.62c |
34.28±0.61c |
| Granulocytes
(×109/l) | 1.3±0.16 | 4.21±1.15 |
22.88±8.53b |
30.23±5.14c |
24.34±5.12b |
19.50±1.62a |
| Granulocytes
(%) | 20.59±1.82 | 27.69±3.97 |
65.10±6.90c |
71.14±3.98c |
65.97±4.67c |
60.11±1.90c |
| Platelets
(×109/l) | 377.0±24.25 | 399.8±53.96 |
631.6±73.14a | 586.2±54.22 | 431.2±52.07 |
321.6±42.14e |
| PCT (%) | 0.32±0.02 | 0.36±0.03 |
0.50±0.05b | 0.41±0.03 |
0.33±0.04d |
0.23±0.03f |
| PDW | 16.54±0.09 | 16.41±0.11 | 16.12±0.08 | 16.14±0.09 | 16.11±0.13 | 16.19±0.18 |
| RBC
(×1012/l) | 10.78±0.23 | 12.36±0.43 |
13.73±0.51c |
12.69±0.4a |
12.94±0.57a |
13.04±0.40b |
| HCT (%) | 58.31±1.37 | 67.81±2.40 |
73.66±2.56a | 69.54±2.53 | 63.90±6.17 | 70.99±2.10 |
| HGB (g/dl) | 17.49±0.46 |
21.23±0.71a |
23.04±1.01c |
21.27±0.75a |
21.62±1.04a |
22.01±0.62b |
| MCV (fl) | 54.1±0.32 | 54.9±0.39 | 53.70±0.26 | 54.77±0.47 | 53.92±0.45 | 54.47±0.36 |
| RDW (%) | 15.03±0.11 | 14.97±0.15 |
15.74±0.13a |
15.98±0.15c |
15.67±0.16a |
15.80±0.09b |
| MCHC (g/l) | 299.29±1.97 |
312.71±1.85b |
311.86±3.51b | 305.57±1.65 |
309.71±2.24a |
309.71±1.78a |
| MCH (pg) | 16.14±0.11 |
17.13±0.11c |
16.71±0.16a | 16.67±0.09 | 16.66±0.14 |
16.83±0.12b |
| MPV (fl) | 8.10±0.23 | 8.03±0.19 | 7.51±0.12 | 7.51±0.10 | 7.69±0.18 | 7.76±0.15 |
Biochemical parameters
Analysis of biochemical parameters revealed a
significant decrease in the serum concentration of total
cholesterol (P<0.05), LDL-cholesterol (P<0.05),
HDL-cholesterol (P<0.01), triglycerides (P<0.001) and total
proteins in the untreated 4T1 group compared to these values in the
control (P<0.001). All the treatments resulted in a significant
decrease in serum concentration of LDL-cholesterol compared to both
the control (P<0.001 for all treated groups) and 4T1 group
(P<0.05 for 4T1 + IM and 4T1 + MANU; P<0.01 for 4T1 + IM +
MANU). The combined treatment prevented the decrease in serum
concentration of HDL-cholesterol which was significantly increased
compared to that in the 4T1 group (P<0.05) reaching a value
similar to that of the control group. The serum concentration of
total proteins was increased in the 4T1 + MANU (P<0.05) and 4T1
+ IM + MANU (P<0.05) groups compared to the serum concentration
in the 4T1 group (Table II). There
were no significant changes in the levels of urea and creatinine or
liver transaminases AST, ALP and ALT between the treated and
untreated 4T1 groups (data not shown).
| Table II.Effect of the treatments on
biochemical parameters in serum. |
Table II.
Effect of the treatments on
biochemical parameters in serum.
|
| C | IM | 4T1 | 4T1 + IM | 4T1 + MANU | 4T1 + IM +
MANU |
|---|
| Total cholesterol
(mmol/l) | 4.41±0.12 | 4.00±0.09 |
3.53±0.26a |
3.63±0.16a | 3.80±0.17 | 3.90±0.10 |
| LDL-cholesterol
(mmol/l) | 2.64±0.03 |
2.38±0.03c |
2.54±0.00a |
2.44±0.03c,d |
2.44±0.02c,d |
2.43±0.01c,e |
| HDL-cholesterol
(mmol/l) | 2.26±0.06 | 2.15±0.08 |
1.68±0.15b |
1.81±0.02b | 1.88±0.10 |
2.11±0.06d |
| Triglyceride
(mmol/l) | 2.99±0.00 |
2.08±0.09c |
2.09±0.08c |
2.28±0.09c |
2.10±0.06c |
1.90±0.02c |
| Total protein
(g/l) | 51.30±0.10 | 46.90±1.10 |
42.05±0.18c |
45.33±0.54b |
45.93±1.21b,d |
46.35±0.63a,d |
Leukocyte differential count
Evaluation of the white blood cell differential
counts revealed a marked increase in the number of neutrophils
(70.43±6.47 vs. 18.00±1.88; P<0.001) accompanied by a decreased
number of lymphocytes (27.71±8.06 vs. 73.07±2.51; P<0.001) and
eosinophils (0.36±0.28 vs. 1.50±0.27; P<0.05) in the 4T1 group
compared to these numbers in the control group. The number of
monocytes was not significantly different between the tested
groups. The basophile counts were 1±1 and are not shown in Table III. The NLR calculated from the
white cell differential count revealed a 14-fold increase in NLR in
the 4T1 group compared to that of the control (3.56±1.28 vs.
0.25±0.03; P<0.001). None of the therapies affected this
ratio.
| Table III.Effect of the treatments on white
blood cell differential leukocyte count. |
Table III.
Effect of the treatments on white
blood cell differential leukocyte count.
|
| C | IM | 4T1 | 4T1 + IM | 4T1 + MANU | 4T1 + IM +
MANU |
|---|
| Neutrophils
(band) | 0.36±0.18 | 0.71±0.24 | 0.21±0.10 | 0.14±0.09 | 0.36±0.14 | 0.43±0.17 |
| Neutrophils
(segment) | 18.00±1.88 | 23.21±2.21 |
70.43±6.47c |
75.64±3.25c |
72.43±4.86c |
68.43±2.77c |
| Lymphocytes | 73.07±2.51 | 67.29±2.14 |
27.71±8.06c |
16.71±2.98c |
17.57±3.82c |
22.36±2.30c |
| Eosinophils | 1.50±0.27 | 1.21±0.26 |
0.36±0.28a |
0.29±0.29a |
0.36±0.09a |
0.21±0.15b |
| Monocytes | 7.41±1.60 | 7.50±0.44 | 10.17±0.98 | 9.25±1.16 | 8.08±1.39 | 9.33±1.63 |
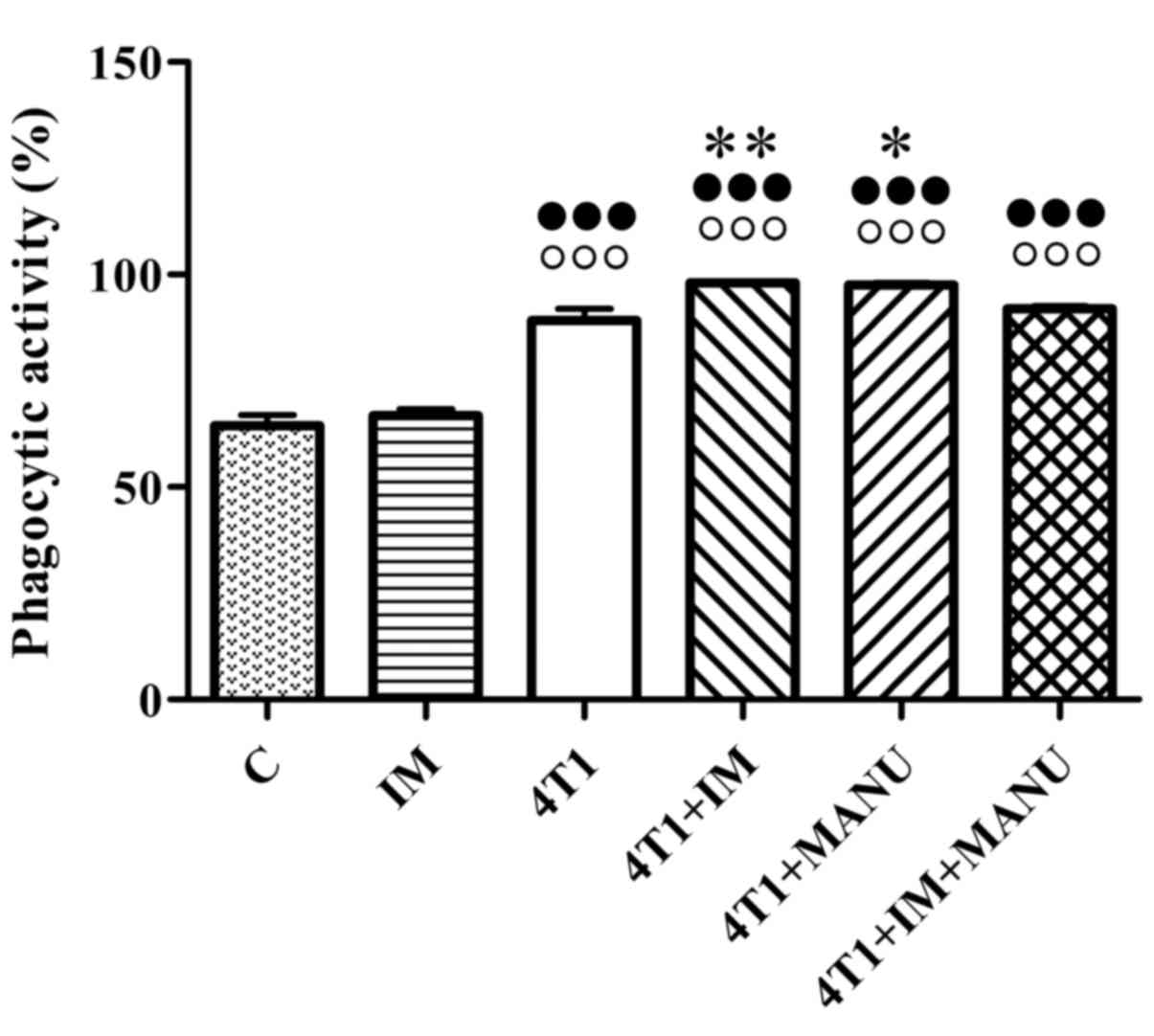
Phagocytic activity
Analysis of phagocytic activity of peripheral blood
monocytes and neutrophils revealed a significant increase in the
percentage of phagocytosing cells in all 4T1 groups compared to the
controls (P<0.001). Administration of Immodin or manumycin A to
the 4T1 group enhanced the phagocytic activity compared to the
activity in the untreated 4T1 group (P<0.01 for IM; P<0.05
for MANU). The phagocytic activity in the 4T1 + IM + MANU group was
not significantly different from the untreated 4T1 group. Due to
the same trend of phagocytic activity of monocytes and neutrophils,
we decided to demonstrate the total phagocytic activity (Fig. 4).
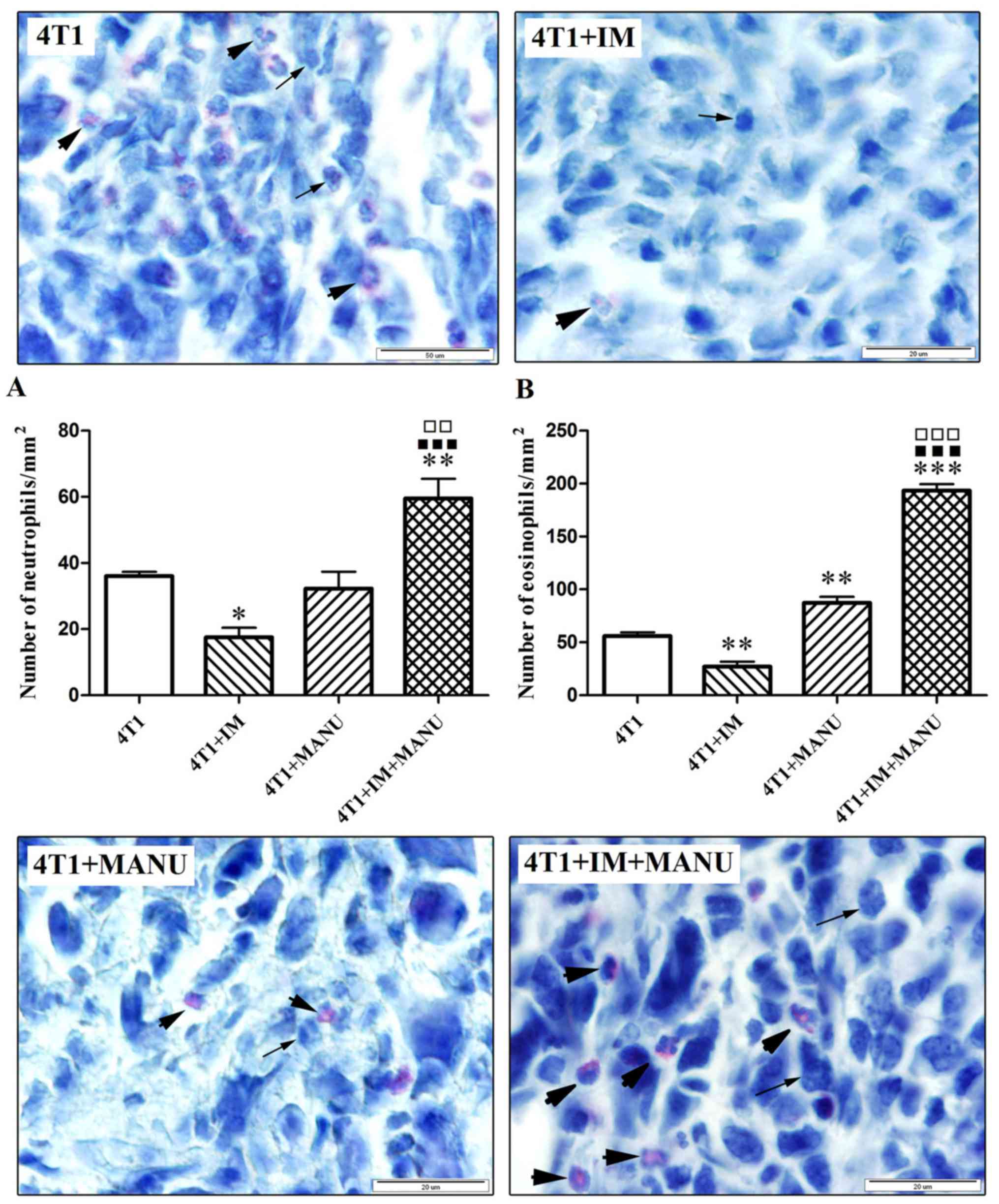
Neutrophils and eosinophils in primary
tumor tissue
Histological analysis of tumor tissue revealed an
increased infiltration of neutrophils (Fig. 5A) and eosinophils (Fig. 5B) in primary tumors of the animals
treated with the drug combination. The number of neutrophils was
significantly higher in the 4T1 + IM + MANU group in comparison
with all the other groups (P<0.05 for 4T1 and 4T1 + MANU;
P<0.001 for 4T1 + IM). The number of eosinophils was
significantly higher in the 4T1 + MANU group in comparison with the
4T1 group (P<0.01) and in the 4T1 + IM + MANU group in
comparison with all other groups (P<0.001).
Discussion
In the present study, we reported on the markedly
reduced tumor growth and prolonged survival of 4T1 tumor-bearing
mice receiving the combination treatment of manumycin A and
Immodin. Since cancer-associated inflammation is a key determinant
of disease progression and the inflammatory response involves
systemic alterations, whole blood cell analyses were carried out to
reveal alterations in the hematological profile in both untreated
and treated tumor-bearing mice. Our results showed that almost all
hematological parameters were affected by the tumor presence.
Regarding leukocytes, an elevated white blood cell count including
both the number of monocytes and granulocytes as well as an
increased count of lymphocytes were detected in the peripheral
blood of the tumor-bearing mice (number means both the absolute
count and percentage). These changes indicate 4T1 cell-triggered
activation of an inflammatory response involving systemic
alterations. However, besides monocytes, none of the parameters
were affected by the treatments. Monocyte counts dropped
significantly after the combination treatment but were still
slightly higher than in the control. On the basis of our complete
results showing an antitumor effect of the combination treatment,
we speculated that it may be caused by the recruitment of
circulating monocytes from the blood into a tumor and their
differentiation into M1-like macrophages with pro-inflammatory,
cytotoxic and antitumor properties (39–41).
The analysis of the white blood cell differential
counts revealed that the most abundant circulating blood leukocytes
in the 4T1-bearing mice were neutrophils. In the same cancer model,
circulating neutrophil numbers continuously increased with tumor
progression (42). Increasing
levels of WBC and neutrophils as a result of progressive increase
in extramedullary hematopoiesis in the spleen and the liver were
observed by week 2 after 4T1 tumor inoculation (43). Regarding granulocytes and
lymphocytes, our results are partially in agreement with a report
on leukemoid reaction caused by 4T1. Whereas DuPre' and Hunter
(44) observed a profound
granulocytosis associated with a decrease in peripheral blood
lymphocytes as the percentage of total leukocytes and constant
numbers of lymphocytes in 4T1 tumor-bearing mice (by day 15
post-tumor transplant vs. by day 19 post-tumor transplant in the
present study), our results demonstrated an elevated number of
granulocytes associated with a strong decrease in the percentage of
peripheral blood lymphocytes and elevated lymphocyte counts.
Despite the fact that the lymphocyte counts were higher in
tumor-bearing mice compared to the control, comparison of the
number or percentage of both the granulocytes and lymphocytes
revealed a reversal of the granulocyte-lymphocyte ratio (G/L) in
the tumor-bearing mice. It has been reported that with the
progression of cancer, the proportion of granulocytes increases in
peripheral blood and the G/L ratio is associated with tumor
progression and shorter survival (45). The high levels of granulocyte
colony-stimulating factor (G-CSF) protein in the serum of
tumor-bearing mice suggests that this factor is responsible for the
increase in granulocytes (44).
Absolute lymphocyte counts can be considered a biomarker of immune
status in the presence of a malignancy (46). The rapid growth observed during the
first two weeks after the inoculation of tumor cells was followed
by regression of growth between weeks 2 and 4 associated with
necrosis and infiltration of leukocytes (43). Our findings demonstrate the
increased infiltration of primary tumors with neutrophils and
eosinophils. Based on the inhibitory effect of the combination
treatment on tumor growth and prolonged survival of animals, we
assume the antitumor potential of granulocytes which has been
reported in several studies. Carretero et al (37) demonstrated an essential role of
tumor-homing eosinophils in tumor eradication and survival.
Antitumor effect of Virulizin® was associated with the
recruitment of eosinophils into tumors (47). Tumor-infiltrating neutrophils played
an essential role in establishment of antitumor immunity following
PDT (48), in stimulation of an
antitumor response in early-stage human lung cancer (49) and acted as potential mediators of
zoledronate-induced antitumor activity (50).
Injection of the 4T1 mammary carcinoma cell line
into BALB/c mice was found to induce a large increase in peripheral
blood neutrophils that correlated with tumor growth (51). Numerous pre-clinical and clinical
studies have demonstrated the association between the increased
number of circulating neutrophils and tumor progression (52–54).
The high neutrophil-lymphocyte ratio (NLR), one of the peripheral
blood-derived indicators of the systemic inflammatory response, was
found to be associated with adverse survival in many solid tumors
including breast cancer (55–59).
Our data also showed an increased neutrophil counts accompanied by
a decreased number of lymphocytes and high levels of NLR in
tumor-bearing mice. Notably, despite the fact that these changes
were not modified by the treatments, they were not associated with
tumor progression.
The evaluation of phagocytosis as a key mechanism of
the innate immune response revealed an increased phagocytic
activity of peripheral blood leukocytes in all tumor-bearing mice
with a profound increase in mice treated with single manumycin A or
Immodin indicating the activation of phagocytic capacity of
leukocytes in the presence of the tumor and its further
potentiation by single treatments. It has been revealed that the
phagocytic capacity of leukocytes is significantly activated in the
presence of a pathological process in the organism and this
activation is much more evident in cancer patients than in patients
with non-malignant disorders. In contrast, surgery,
chemoradiotherapy (60) and
chemotherapy (61) caused a
significant decrease in the phagocytosis of peripheral blood
neutrophils in breast cancer and macrophages in oral cancer
(62), thus interfering with the
defense reactions. In this regard, it is important that none of the
treatments negatively affected the phagocytic function, since it
has been suggested that such therapeutical procedures must be
chosen which do not interfere with the course of defense reactions
(63).
Furthermore, we observed a high number of platelets
and elevated plateletcrit in the untreated tumor-bearing mice. The
PDW and MPV were unchanged in all experimental groups. The same
alterations in platelet parameters have been documented in patients
with colorectal cancer (64).
Notably, both the platelet counts and plateletcrit returned to the
normal range in the tumor-bearing mice treated with the combination
of manumycin A and Immodin indicating its marked antiplatelet
action. This is of great importance since an elevated blood
platelet count correlates with poor survival and prognosis in a
large variety of cancers including breast cancer (65–69).
There is evidence for the positive antitumor effect of circulating
platelet reduction. Lowering platelet counts in various
experimental and clinical models decreased tumor lung invasion
(70,71), inhibited gastric and ovarian tumor
growth (72,73), prevented or delayed the development
of hepatocellular carcinoma (74)
and resulted in better survival of patients with head and neck
squamous cell carcinoma (75).
Stone et al (73) suggested
the existence of a paracrine circuit wherein increased production
of thrombopoietic cytokines in tumor and host tissue leads to
paraneoplastic thrombocytosis, which fuels tumor growth. In their
study anti-interleukin (IL)-6 antibody treatment significantly
reduced platelet counts in tumor-bearing mice and in patients with
epithelial ovarian cancer. An increased plasma IL-6 in patients
with metastatic prostate carcinoma was found to be correlated with
tumor burden (76). It has been
reported that the presence of a tumor increases both tumor- and
host-derived IL-6 in plasma and significant amounts of IL-6 are
stored in platelets (30).
Recently, it has been observed that manumycin A decreased
interleukin levels involved in various types of malignancies in
colorectal adenocarcinoma Caco-2 cells (77) and downregulated the mRNA for IL-6
and inhibited IL-6 production in TNF-α stimulated human monocytic
leukemia THP-1 cells and peripheral blood monocytes (10). Based on these data, we speculated
that the antiplatelet effect of single manumycin A or the
combination treatment may involve the inhibition of IL-6.
In the present study, we further demonstrated that
the red blood cell markers were also affected by the tumor showing
an increase in RBC, HCT, HGB, RDW, MCHC and MCH. All of these
parameters were increased in the tumor-bearing mice. We suppose
that these changes which were unaffected by either treatment, may
be a consequence of tumor-stimulated stress erythropoiesis in the
spleen. According to a recent study, 4T1 tumor development is
associated with the suppression of medullar erythropoiesis by
GCS-F, whereas tumor stress promotes erythropoiesis in the spleen.
The average spleen weight and splenocyte numbers started to
increase one week after 4T1 tumor cell implantation (78). Our results also showed a significant
increase in mean spleen weight in tumor-bearing mice which was
slightly suppressed by the combination treatment (data not shown).
Yilmaz et al (79) suggested
that the increase in RDW is the result of complex factors,
including inflammation, oxidative stress and the immune
response.
Alterations in cholesterol metabolism including
decreased total serum cholesterol, LDL-cholesterol, HDL-cholesterol
and triglycerides have been documented as a preclinical or
consequential effect of some types of cancer (80,81).
In contrast, an inverse relationship has been demonstrated between
HDL cholesterol and cancer risk (82–84).
Low HDL-cholesterol levels may simply be a reflection of chronic
conditions that increase inflammation and insulin resistance, which
may directly influence atherosclerosis and carcinogenesis (85). Our results showed the ability of the
combination treatment to decrease LDL-cholesterol and also to
restore the concentration of HDL-cholesterol and the total protein
content in tumor-bearing mice indicating the positive effect of the
treatment on cholesterol and protein metabolism as part of its
anticancer action. These results are in accordance with the data
from another study, which showed a decrease in LDL-cholesterol in
quercetin-treated S-180-bearing mice, whereas the HDL-cholesterol
increased compared with levels in the S-180-bearing mice (86).
In summary, our results revealed the most potent
antitumor effect of the novel combination of manumycin A and
Immodin in a 4T1 breast carcinoma mouse model demonstrated by
reduced tumor growth and prolonged survival associated with strong
antiplatelet effect and enhanced granulocyte infiltration in the
primary tumor indicating that various mechanisms are involved in
the antitumor activity of the combination treatment.
Acknowledgements
The present study was supported by the ASFEU Project
(with ITMS code no. 26220220157) supported by the operating program
‘Research and Development’ funded by the European Fund for Regional
Development (Slovakia) (0.7), and also by the Project SK0021,
co-financed through the EEA financial mechanism, the Norwegian
Financial Mechanism and the State Budget of the Slovak Republic
(0.3). The authors are grateful to Dr Zuzana Jendželovská, Dr Lenka
Hurtuková, Jana Vargová, Barbora Fecková and Slávka Štibraná for
assistance with the technical procedures.
References
|
1
|
Hara M, Akasaka K, Akinaga S, Okabe M,
Nakano H, Gomez R, Wood D, Uh M and Tamanoi F: Identification of
Ras farnesyltransferase inhibitors by microbial screening. Proc
Natl Acad Sci USA. 90:2281–2285. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ito T, Kawata S, Tamura S, Igura T, Nagase
T, Miyagawa JI, Yamazaki E, Ishiguro H and Matasuzawa Y:
Suppression of human pancreatic cancer growth in BALB/c nude mice
by manumycin, a farnesyl:protein transferase inhibitor. Jpn J
Cancer Res. 87:113–116. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
She M and Jim Yeung SC: Combining a matrix
metalloproteinase inhibitor, a farnesyltransferase inhibitor, and a
taxane improves survival in an anaplastic thyroid cancer model.
Cancer Lett. 238:197–201. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Dixit D, Sharma V, Ghosh S, Koul N, Mishra
PK and Sen E: Manumycin inhibits STAT3, telomerase activity, and
growth of glioma cells by elevating intracellular reactive oxygen
species generation. Free Radic Biol Med. 47:364–374. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sears KT, Daino H and Carey GB: Reactive
oxygen species-dependent destruction of MEK and Akt in Manumycin
stimulated death of lymphoid tumor and myeloma cell lines. Int J
Cancer. 122:1496–1505. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Singha PK, Pandeswara S, Venkatachalam MA
and Saikumar P: Manumycin A inhibits triple-negative breast cancer
growth through LC3-mediated cytoplasmic vacuolation death. Cell
Death Dis. 4:e4572013. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Sugita M, Sugita H and Kaneki M:
Farnesyltransferase inhibitor, Manumycin A, prevents
atherosclerosis development and reduces oxidative stress in
apolipoprotein E-deficient mice. Arterioscler Thromb Vasc Biol.
27:1390–1395. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Sharma V, Shaheen SS, Dixit D and Sen E:
Farnesyltransferase inhibitor manumycin targets IL1β-Ras-HIF-1α
axis in tumor cells of diverse origin. Inflammation. 35:516–519.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Saha B and Nandi D: Farnesyltransferase
inhibitors reduce Ras activation and ameliorate
acetaminophen-induced liver injury in mice. Hepatology.
50:1547–1557. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Cecrdlova E, Petrickova K, Kolesar L,
Petricek M, Sekerkova A, Svachova V and Striz I: Manumycin A
downregulates release of proinflammatory cytokines from TNF alpha
stimulated human monocytes. Immunol Lett. 169:8–14. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Berrón-Pérez R, Chávez-Sánchez R,
Estrada-García I, Espinosa-Padilla S, Cortez-Gómez R,
Serrano-Miranda E, Ondarza-Aguilera R, Pérez-Tapia M, Olvera B
Pineda, Jiménez-Martínez Mdel C, et al: Indications, usage, and
dosage of the transfer factor. Rev Alerg Mex. 54:134–139.
2007.PubMed/NCBI
|
|
12
|
Arnaudov A and Kostova Z: Dialysable
leukocyte extracts in immunotherapy. Biotechnol Biotechnol Equip.
29:1017–1023. 2015. View Article : Google Scholar
|
|
13
|
Cherenko SO, Reva ОA, Rekalova OM,
Kibizova NI, Yasir SG and Matvienko YO: Immunotherapy with
leukocyte immunomodulator dialysate in patients with
multidrug-resistant tuberculosis. Asthma and Allergies. 3:13–20.
2013.
|
|
14
|
Viza D, Fudenberg HH, Palareti A, Ablashi
D, De Vinci C and Pizza G: Transfer factor: An overlooked potential
for the prevention and treatment of infectious diseases. Folia
Biol. 59:53–67. 2013.
|
|
15
|
Homberg TA, Lara RI, Pérez-Tapia SM and
Jiménez Martínez MDC: Dialyzable leukocyte extracts as adjuvant
treatment for allergic rhinitis. World Allergy Organ J. 7:(Suppl
1). P52014. View Article : Google Scholar
|
|
16
|
Gómez Vera J, Chávez Sánchez R, Flores
Sandoval G, Orea Solano M, López Tiro JJ, Santiago Santos AD,
Espinosa Padilla S, Espinosa Rosales F, Huerta J, Ortega Martell
JA, et al: Transfer factor and allergy. Rev Alerg Mex. 57:208–214.
2010.PubMed/NCBI
|
|
17
|
Lokaj J, Pekarek J and Kuklinek P:
Leukocyte Dialysates and Transfer FactorMayer V and Borvác J:
Slovak Academy of Science; Bratislava: pp. 516–525. 1987
|
|
18
|
Georgescu C: Effect of long-term therapy
with transfer factor in rheumatoid arthritis. Med Interne.
23:135–140. 1985.PubMed/NCBI
|
|
19
|
Juarez PC: Effect of Transferon as an
adjuvant in the treatment of osteosarcoma (In Spanish) (unpublished
dissertation). National Polytechnic Institute; Mexico City:
2011
|
|
20
|
Pilotti V, Mastrorilli M, Pizza G, De
Vinci C, Busutti L, Palareti A, Gozzetti G and Cavallari A:
Transfer factor as an adjuvant to non-small cell lung cancer
(NSCLC) therapy. Biotherapy. 9:117–121. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Franco-Molina MA, Mendoza-Gamboa E,
Zapata-Benavides P, Vera-García ME, Castillo-Tello P, García de la
Fuente A, Mendoza RD, Garza RG, Támez-Guerra RS and
Rodríguez-Padilla C: IMMUNEPOTENT CRP (bovine dialyzable leukocyte
extract) adjuvant immunotherapy: A phase I study in non-small cell
lung cancer patients. Cytotherapy. 10:490–496. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Lara HH, Turrent LI, Garza-Treviño EN,
Tamez-Guerra R and Rodriguez-Padilla C: Clinical and immunological
assessment in breast cancer patients receiving anticancer therapy
and bovine dialyzable leukocyte extract as an adjuvant. Exp Ther
Med. 1:425–431. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pineda B, Estrada-Parra S, Pedraza-Medina
B, Rodriguez-Ropon A, Pérez R and Arrieta O: Interstitial transfer
factor as adjuvant immunotherapy for experimental glioma. J Exp
Clin Cancer Res. 24:575–583. 2005.PubMed/NCBI
|
|
24
|
Whyte RI, Schork MA, Sloan H, Orringer MB
and Kirsh MM: Adjuvant treatment using transfer factor for
bronchogenic carcinoma: Long-term follow-up. Ann Thorac Surg.
53:391–396. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Pizza G, De Vinci C, Cuzzocrea D, Menniti
D, Aiello E, Maver P, Corrado G, Romagnoli P, Dragoni E, LoConte G,
et al: A preliminary report on the use of transfer factor for
treating stage D3 hormone-unresponsive metastatic prostate cancer.
Biotherapy. 9:123–132. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Lal I, Dittus K and Holmes CE: Platelets,
coagulation and fibrinolysis in breast cancer progression. Breast
Cancer Res. 15:2072013. View
Article : Google Scholar : PubMed/NCBI
|
|
27
|
Bambace NM and Holmes CE: The platelet
contribution to cancer progression. J Thromb Haemost. 9:237–249.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Gay LJ and Felding-Habermann B:
Contribution of platelets to tumour metastasis. Nat Rev Cancer.
11:123–134. 2011. View
Article : Google Scholar : PubMed/NCBI
|
|
29
|
Lin RJ, Afshar-Kharghan V and Schafer AI:
Paraneoplastic thrombocytosis: The secrets of tumor self-promotion.
Blood. 124:184–187. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kerr BA, Miocinovic R, Smith AK, Klein EA
and Byzova TV: Comparison of tumor and microenvironment secretomes
in plasma and in platelets during prostate cancer growth in a
xenograft model. Neoplasia. 12:388–396. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Ostberg JR, Ertel BR and Lanphere JA: An
important role for granulocytes in the thermal regulation of colon
tumor growth. Immunol Invest. 34:259–272. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Fernández-Aceñero MJ, Galindo-Gallego M,
Sanz J and Aljama A: Prognostic influence of tumor-associated
eosinophilic infiltrate in colorectal carcinoma. Cancer.
88:1544–1548. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Klintrup K, Mäkinen JM, Kauppila S, Väre
PO, Melkko J, Tuominen H, Tuppurainen K, Mäkelä J, Karttunen TJ and
Mäkinen MJ: Inflammation and prognosis in colorectal cancer. Eur J
Cancer. 41:2645–2654. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Zhang Y, Ren H, Wang L, Ning Z, Zhuang Y,
Gan J, Chen S, Zhou D, Zhu H, Tan D, et al: Clinical impact of
tumor-infiltrating inflammatory cells in primary small cell
esophageal carcinoma. Int J Mol Sci. 15:9718–9734. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Tepper RI, Coffman RL and Leder P: An
eosinophil-dependent mechanism for the antitumor effect of
interleukin-4. Science. 257:548–551. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Giovarelli M, Cappello P, Forni G, Salcedo
T, Moore PA, LeFleur DW, Nardelli B, Di Carlo E, Lollini PL, Ruben
S, et al: Tumor rejection and immune memory elicited by locally
released LEC chemokine are associated with an impressive
recruitment of APCs, lymphocytes, and granulocytes. J Immunol.
164:3200–3206. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Carretero R, Sektioglu IM, Garbi N,
Salgado OC, Beckhove P and Hämmerling GJ: Eosinophils orchestrate
cancer rejection by normalizing tumor vessels and enhancing
infiltration of CD8+ T cells. Nat Immunol. 16:609–617.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Llewellyn BD: An improved Sirius red
method for amyloid. J Med Lab Technol. 27:308–309. 1970.PubMed/NCBI
|
|
39
|
Ma J, Liu L, Che G, Yu N, Dai F and You Z:
The M1 form of tumor-associated macrophages in non-small cell lung
cancer is positively associated with survival time. BMC Cancer.
10:1122010. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Pommier A, Audemard A, Durand A, Lengagne
R, Delpoux A, Martin B, Douguet L, Le Campion A, Kato M, Avril MF,
et al: Inflammatory monocytes are potent antitumor effectors
controlled by regulatory CD4+ T cells. Proc Natl Acad
Sci USA. 110:13085–13090. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Chanmee T, Ontong P, Konno K and Itano N:
Tumor-associated macrophages as major players in the tumor
microenvironment. Cancers. 6:1670–1690. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Sagiv JY, Michaeli J, Assi S, Mishalian I,
Kisos H, Levy L, Damti P, Lumbroso D, Polyansky L, Sionov RV, et
al: Phenotypic diversity and plasticity in circulating neutrophil
subpopulations in cancer. Cell Reports. 10:562–573. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Tao K, Fang M, Alroy J and Sahagian GG:
Imagable 4T1 model for the study of late stage breast cancer. BMC
Cancer. 8:2282008. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
DuPre' SA and Hunter KW Jr: Murine mammary
carcinoma 4T1 induces a leukemoid reaction with splenomegaly:
Association with tumor-derived growth factors. Exp Mol Pathol.
82:12–24. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Liu H and Tabuchi T, Takemura A, Kasuga T,
Motohashi G, Hiraishi K, Katano M, Nakada I, Ubukata H and Tabuchi
T: The granulocyte/lymphocyte ratio as an independent predictor of
tumour growth, metastasis and progression: Its clinical
applications. Mol Med Rep. 1:699–704. 2008.PubMed/NCBI
|
|
46
|
Rochet NM, Markovic SN and Porrata LF: The
role of complete blood cell count in prognosis-Watch this space!
Oncol Hematol Rev. 8:76–82. 2012. View Article : Google Scholar
|
|
47
|
Benatar T, Cao MY, Lee Y, Li H, Feng N, Gu
X, Lee V, Jin H, Wang M, Der S, et al: Virulizin induces production
of IL-17E to enhance antitumor activity by recruitment of
eosinophils into tumors. Cancer Immunol Immunother. 57:1757–1769.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Kousis PC, Henderson BW, Maier PG and
Gollnick SO: Photodynamic therapy enhancement of antitumor immunity
is regulated by neutrophils. Cancer Res. 67:10501–10510. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Eruslanov EB, Bhojnagarwala PS, Quatromoni
JG, Stephen TL, Ranganathan A, Deshpande C, Akimova T, Vachani A,
Litzky L, Hancock WW, et al: Tumor-associated neutrophils stimulate
T cell responses in early-stage human lung cancer. J Clin Invest.
124:5466–5480. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Mete S: Targeting tumor microenvironment
by zoledronate as a novel therapeutic approach in cancer
(dissertation). University of Zurich, Faculty of Science; Zurich:
2011
|
|
51
|
Demers M, Krause DS, Schatzberg D,
Martinod K, Voorhees JR, Fuchs TA, Scadden DT and Wagner DD:
Cancers predispose neutrophils to release extracellular DNA traps
that contribute to cancer-associated thrombosis. Proc Natl Acad Sci
USA. 109:13076–13081. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Schmidt H, Bastholt L, Geertsen P,
Christensen IJ, Larsen S, Gehl J and von der Maase H: Elevated
neutrophil and monocyte counts in peripheral blood are associated
with poor survival in patients with metastatic melanoma: A
prognostic model. Br J Cancer. 93:273–278. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Atzpodien J and Reitz M: Peripheral blood
neutrophils as independent immunologic predictor of response and
long-term survival upon immunotherapy in metastatic renal-cell
carcinoma. Cancer Biother Radiopharm. 23:129–134. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Coffelt SB, Kersten K, Doornebal CW,
Weiden J, Vrijland K, Hau CS, Verstegen NJ, Ciampricotti M,
Hawinkels LJ, Jonkers J, et al: IL-17-producing γδ T cells and
neutrophils conspire to promote breast cancer metastasis. Nature.
522:345–348. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Shimada H, Takiguchi N, Kainuma O, Soda H,
Ikeda A, Cho A, Miyazaki A, Gunji H, Yamamoto H and Nagata M: High
preoperative neutrophil-lymphocyte ratio predicts poor survival in
patients with gastric cancer. Gastric Cancer. 13:170–176. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Shibutani M, Maeda K, Nagahara H, Noda E,
Ohtani H, Nishiguchi Y and Hirakawa K: A high preoperative
neutrophil-to-lymphocyte ratio is associated with poor survival in
patients with colorectal cancer. Anticancer Res. 33:3291–3294.
2013.PubMed/NCBI
|
|
57
|
Chen J, Deng Q, Pan Y, He B, Ying H, Sun
H, Liu X and Wang S: Prognostic value of neutrophil-to-lymphocyte
ratio in breast cancer. FEBS Open Bio. 5:502–507. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Koh CH, Bhoo-Pathy N, Ng KL, Jabir RS, Tan
GH, See MH, Jamaris S and Taib NA: Utility of pre-treatment
neutrophil-lymphocyte ratio and platelet-lymphocyte ratio as
prognostic factors in breast cancer. Br J Cancer. 113:150–158.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Templeton AJ, McNamara MG, Šeruga B,
Vera-Badillo FE, Aneja P, Ocaña A, Leibowitz-Amit R, Sonpavde G,
Knox JJ, Tran B, et al: Prognostic role of neutrophil-to-lymphocyte
ratio in solid tumors: A systematic review and meta-analysis. J
Natl Cancer Inst. 106:dju1242014. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Ueta E, Osaki T, Yoneda K, Yamamoto T and
Umazume M: Influence of inductive chemoradiotherapy on salivary
polymorphonuclear leukocyte (SPMN) functions in oral cancer. J Oral
Pathol Med. 23:418–422. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Baskic D, Arsenijevic NN and Acimovic LD:
Monocyte phagocytic function in patients with breast cancer during
therapy. Meeting abstracts, 23rd Congress of the International
Association of Breast Cancer Research. 13–16 June; Dusseldorf,
Germany. http://breast-cancer-research.com/content/3/S1
|
|
62
|
Reshma K, Bharathi B, Rao AV, Dinesh M and
Vasudevan DM: Phagocytosis: A marker of decreased immune response
in radiation treated oral cancers. Biomed Res. 20:75–77. 2009.
|
|
63
|
Cron J and Jansa P: Role of phagocytic
cells in cancer. Folia Haematol Int Mag Klin Morphol Blutforsch.
108:481–527. 1981.PubMed/NCBI
|
|
64
|
Karagöz B, Bilgi O, Alacacioğlu A, Ozgün
A, Sayan O, Erikçi AA and Kandemir EG: Mean platelet volume
increase after tamoxifen, but not after anastrazole in adjuvant
therapy of breast cancer. Med Oncol. 27:199–202. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Taucher S, Salat A, Gnant M, Kwasny W,
Mlineritsch B, Menzel RC, Schmid M, Smola MG, Stierer M, Tausch C,
et al: Austrian Breast and Colorectal Cancer Study Group: Impact of
pretreatment thrombocytosis on survival in primary breast cancer.
Thromb Haemost. 89:1098–1106. 2003.PubMed/NCBI
|
|
66
|
Brockmann MA, Giese A, Mueller K, Kaba FJ,
Lohr F, Weiss C, Gottschalk S, Nolte I, Leppert J, Tuettenberg J,
et al: Preoperative thrombocytosis predicts poor survival in
patients with glioblastoma. Neuro Oncol. 9:335–342. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Lu CC, Chang KW, Chou FC, Cheng CY and Liu
CJ: Association of pretreatment thrombocytosis with disease
progression and survival in oral squamous cell carcinoma. Oral
Oncol. 43:283–288. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
68
|
Stravodimou A and Voutsadakis IA:
Pretreatment thrombocytosis as a prognostic factor in metastatic
breast cancer. Int J Breast Cancer. 2013:2895632013. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Digklia A and Voutsadakis IA:
Thrombocytosis as a prognostic marker in stage III and IV serous
ovarian cancer. Obstet Gynecol Sci. 57:457–463. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Gasic GJ, Gasic TB and Stewart CC:
Antimetastatic effects associated with platelet reduction. Proc
Natl Acad Sci USA. 61:46–52. 1968. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Li R, Ren M, Chen N, Luo M, Deng X, Xia J,
Yu G, Liu J, He B, Zhang X, et al: Presence of intratumoral
platelets is associated with tumor vessel structure and metastasis.
BMC Cancer. 14:1672014. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Mikami J, Kurokawa Y, Takahashi T,
Miyazaki Y, Yamasaki M, Miyata H, Nakajima K, Takiguchi S, Mori M
and Doki Y: Antitumor effect of antiplatelet agents in gastric
cancer cells: An in vivo and in vitro study. Gastric Cancer.
19:817–826. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Stone RL, Nick AM, McNeish IA, Balkwill F,
Han HD, Bottsford-Miller J, Rupairmoole R, Armaiz-Pena GN, Pecot
CV, Coward J, et al: Paraneoplastic thrombocytosis in ovarian
cancer. N Engl J Med. 366:610–618. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Sitia G, Aiolfi R, Di Lucia P, Mainetti M,
Fiocchi A, Mingozzi F, Esposito A, Ruggeri ZM, Chisari FV,
Iannacone M, et al: Antiplatelet therapy prevents hepatocellular
carcinoma and improves survival in a mouse model of chronic
hepatitis B. Proc Natl Acad Sci USA. 109:E2165–E2172. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Rachidi S, Wallace K, Day TA, Alberg AJ
and Li Z: Lower circulating platelet counts and antiplatelet
therapy independently predict better outcomes in patients with head
and neck squamous cell carcinoma. J Hematol Oncol. 7:652014.
View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Adler HL, McCurdy MA, Kattan MW, Timme TL,
Scardino PT and Thompson TC: Elevated levels of circulating
interleukin-6 and transforming growth factor-beta1 in patients with
metastatic prostatic carcinoma. J Urol. 161:182–187. 1999.
View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Petanidis S, Anestakis D, Argyraki M,
Hadzopoulou-Cladaras M and Salifoglou A: Differential expression of
IL-17, 22 and 23 in the progression of colorectal cancer in
patients with K-ras mutation: Ras signal inhibition and crosstalk
with GM-CSF and IFN-γ. PLoS One. 8:e736162013. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Liu M, Jin X, He X, Pan L, Zhang X and
Zhao Y: Macrophages support splenic erythropoiesis in 4T1
tumor-bearing mice. PLoS One. 10:e01219212015. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Yilmaz M, Cimilli G, Saritemur M, Demircan
F, Isaoglu U, Kisaoglu A and Emet M: Diagnostic accuracy of
neutrophil/lymphocyte ratio, red cell distribution width and
platelet distribution width in ovarian torsion. J Obstet Gynaecol.
36:218–222. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Kritchevsky SB and Kritchevsky D: Serum
cholesterol and cancer risk: An epidemiologic perspective. Annu Rev
Nutr. 12:391–416. 1992. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Hussein MA and Boshra SA: Antitumor and
structure antioxidant activity relationship of colchicine on
Ehrlich ascites carcinoma (EAC) in female mice. Int J Drug Deliv.
5:430–437. 2013.
|
|
82
|
Furberg AS, Jasienska G, Bjurstam N,
Torjesen PA, Emaus A, Lipson SF, Ellison PT and Thune I: Metabolic
and hormonal profiles: HDL cholesterol as a plausible biomarker of
breast cancer risk. The Norwegian EBBA Study. Cancer Epidemiol
Biomarkers Prev. 14:33–40. 2005.
|
|
83
|
Jafri H, Alsheikh-Ali AA and Karas RH:
Baseline and on-treatment high-density lipoprotein cholesterol and
the risk of cancer in randomized controlled trials of
lipid-altering therapy. J Am Coll Cardiol. 55:2846–2854. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
84
|
Touvier M, Fassier P, His M, Norat T, Chan
DS, Blacher J, Hercberg S, Galan P, Druesne-Pecollo N and
Latino-Martel P: Cholesterol and breast cancer risk: A systematic
review and meta-analysis of prospective studies. Br J Nutr.
114:347–357. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Robinson JG: Low high-density lipoprotein
cholesterol and chronic disease risk marker or causal? J Am Coll
Cardiol. 55:2855–2857. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
86
|
Ravichandran P, Elangovan V and
Govindasamy S: Chemopreventive effect of quercetin in
sarcoma-180-bearing mice. J Clin Biochem Nutr. 22:149–154. 1997.
View Article : Google Scholar
|