Introduction
Gastric cancer (GC) is one of the most prevalent
cancers in Japan and other East Asian countries (1). Although the 5-year survival rate of GC
patients with early stage in Japan is 97%, the recurrence rate
after surgery in GC patients with advanced stage is also high. In
particular, the 5-year survival rate at stage IV is around 10%. In
order to improve the prognosis, it is important to clarify the
biomarkers for the screening of GC patients in the high-risk group
of recurrence.
MicroRNAs (miRNAs) have been shown to be one of the
potential biomarkers for tumor diagnosis and prediction of
prognosis in various types of cancer (2,3). They
are small non-coding 23–35 nucleotide molecules, which
post-transcriptionally regulate the production of proteins from
their messenger RNAs (mRNAs) (3).
miRNAs play an important role in the process of cell proliferation,
differentiation, apoptosis and metastasis (2). It has been reported that miRNAs are
abnormally expressed in cancers and influence the initiation and
progression of cancer cells as oncogenes or tumor-suppressor genes
(4). In addition, miRNAs can be
detected not only in tissues, but also in body fluids such as
plasma, serum, urine, saliva and lactation milk. Many studies have
focused on cancer-derived miRNAs in the circulatory system of
cancer patients (5,6). These studies indicated that plasma
miRNAs may act as minimally invasive biomarkers for the diagnosis
and prognosis of GC patients (5–8).
Other studies have confirmed the existence of miRNAs
in a stable form within plasma/serum exosome. The exosomes, which
are extremely small at 40–150 nm, originate from the luminal
membranes of multivesicular bodies (9,10).
Released by the process of fusion with the cell membranes of
multivesicular bodies, these exosomes contain protein and
selectively packaged RNA, such as miRNA, and have the ability to
transfer these components to other cells (11,12).
Cancer patients often exhibit high concentrations of exosomes, and
if the exosomes contain intact miRNA, they have potential as
effective predictive and prognostic biomarkers (12–15).
At present, we have already reported that exosome miR-21 is a
useful biomarker for predicting the recurrence and prognosis of
lung and colorectal cancer (16,17).
However, few published studies have investigated the association
between the plasma exosomal miRNA expression and the prognosis of
GC patients at each tumor stage.
In the present study, we aimed to demonstrate the
potential of exosome-encapsulated miRNAs as predictive biomarkers
for recurrence and prognosis in GC patients at each tumor
stage.
Patients and methods
Study design
We selected recurrence specific exosomal miRNA by
microRNA micro-array analysis using the plasma exosomes collected
from stage I GC patients who had relapsed after surgery (n=3),
stage I GC patients who had not relapsed after surgery (n=3) and
healthy controls (n=3). Subsequently, we validated the selected
miRNA using the plasma exosomes collected from another 232 GC
patients and 20 healthy volunteers. The patients were studied
between November 2006 and December 2013 at Teikyo University
Hospital. The cancer stage was determined according to the TNM
classification (UICC). In the present study, 74 cases with stage I,
47 cases with stage II, 79 cases with stage III and 32 cases with
stage IV GC were included. The median follow-up period was 3.8
years (range, 0.4–10.6 years). The samples were collected before
the start of the treatment. The patients were treated with standard
treatment for GC patients. The study protocol conformed to the
guidelines of the ethics committee of the Teikyo University, and
was approved by the review board of the Teikyo University
(09-081-3). Written informed consent was obtained from the all
patients.
Patients follow-up
Post-operative follow-up was performed according to
the guidelines published by the Japanese Gastric Cancer Association
(18). Confirmation of recurrence
was required to evaluate imaging or pathological diagnosis. Testing
of the tumor markers (CEA and CA19-9), combined with a general
physical examination, were conducted every 3 months for 3 years and
then every 6 months for 5 years. Following surgery, computed
tomography was conducted once every 6 months for 5 years and then
every 6 or 12 months for up to 10 years. Gastroscopy was conducted
annually for a period of 5 years after surgery.
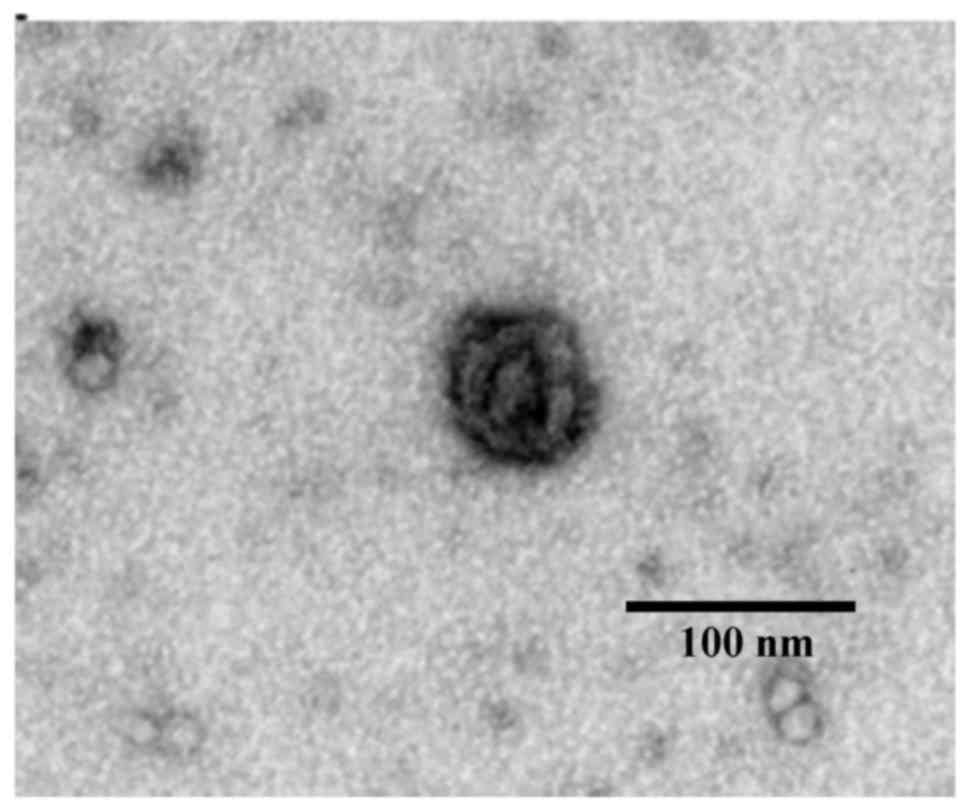
Purification of exosomes from plasma
and recognition by transmission electron microscopy
Plasma (1 ml) separated from blood was used for
microarray analysis and quantitative real-time reverse
transcription-PCR (qRT-PCR). The exosomes were separated by
ultracentrifugation (15,000 × g for 70 min) from the plasma, and
the isolated exosomes were recognized by transmission electron
microscopy using the electron microscope H-7600 (Hitachi
High-Technologies Corp., Tokyo, Japan) as previously described
(17).
Total RNA isolation from exosomes and
tissues
Total RNAs (including the miRNA) of exosomes were
isolated using the miRNeasy Serum/Plasma kit (Qiagen, Venlo, The
Netherlands) and total RNAs (including the miRNA) of tissues were
extracted using the miRNeasy Mini kit (Qiagen). Subsequent
extraction and cartridge work was performed according to the
manufacturer's protocol as previously described (17). The quality of extracted RNA was
assessed using an Agilent 2100 Bioanalyzer (Agilent Technologies,
Santa Clara, CA, USA).
miRNA microarray analysis
Examination of the exosomal miRNA expression
profiles was conducted with a 3D-Gene Human miRNA Oligo chip ver.20
(Toray Industries Inc. Tokyo, Japan). In total, 2,578 genes were
mounted in this chip. A 3D-Gene scanner (Toray) was used to scan
and analyze the fluorescence signals. All procedures were conducted
according to the manufacturer's protocol. The raw data for each
spot were normalized to the mean intensity of background signals
determined by all blank signal intensities at 95% confidence
intervals. Effective assessements were considered when the signal
intensity of both duplicate spots was >2SD of the background
signal intensity.
Quantitative real time-PCR (qRT-PCR)
for miRNAs of exosomes and tissues
By using qRT-PCR, the miRNA expression from the
plasma exosomes and tissues was examined. Synthesis of cDNA of
total RNA isolated from exosomes was conducted using TaqMan
microRNA primers specific for miR-23b and miR-16a (Thermo Fisher
Scientific Inc., Waltham, MA, USA), and TaqMan Micro-RNA Reverse
Transcription kit (Thermo Fisher Scientific). Since previous
research had reported that miR-16a was a reliable endogenous
control for miRNA analysis by qRT-PCR in human plasma samples, we
decided to use it as an internal control. TaqMan microRNA primers
specific for miR-23b and RNU6B and TaqMan Micro-RNA Reverse
Transcription kit (Thermo Fisher Scientific) were employed to
synthesize the cDNA of total RNA isolated from tissues. RNU6B was
selected as the internal control of tissue samples. qRT-PCR was
performed using TaqMan Universal PCR Master Mix (Thermo Fisher
Scientific) and LightCycler-480 (Roche Applied Science, Basel,
Switzerland) following the manufacturer's protocol. Each sample was
analyzed in duplicate. Relative quantification of miRNA expression
was calculated using the 2−ΔΔCT method as previously
described (17).
Statistical analysis
The data were expressed as the mean ± standard
deviation (SD). The cut-off value was set at 0.78, which is the
median of miR-23b. The relationship between the microRNA expression
and clinicopathological factors was analyzed using the Student's
t-test, the Chi-square test and ANOVA. Using the Kaplan-Meier
survival curves, overall survival (OS) and disease-free survival
(DFS) curves were analyzed, and the differences were estimated
using log-rank tests. Cox proportional hazard model was used to
estimate univariate and multivariate hazard ratios for OS and DFS.
Multivariate analysis was performed for factors that showed
significance in univariate analysis. All P-values are two-sided,
and P<0.05 was considered to indicate a statistically
significant difference. Statistical analyses were performed using
the JMP 9.0 software (SAS Institute, Inc., Cary, NC, USA).
Results
Exosome electron microscopic
image
To confirm the exosomes, we examined the
ultracentrifugation samples from the plasma of GC patients by
transmission electron microscopy. In this sample, we captured
images of round micro vesicles that had diameters of about 50–100
nm (Fig. 1).
Exosomal miRNA array analysis of GC
patients
To reveal the recurrence-predictor exosomal miRNA in
GC patients, microRNA array analysis was employed. In the present
study, plasma exosome samples were collected from stage I GC
patients who showed recurrence after surgery (recurrence group,
n=3), stage I GC patients who did not show any recurrence after
surgery (non-recurrence group, n=3) and a healthy control group
(n=3). The clinical backgrounds of these 6 GC patients and 3
healthy controls used for this analysis are listed in Table I. The recurrence sites of 3 patients
were liver. Table II demonstrates
the five markedly downregulated and upregulated exosomal miRNAs
after comparison of these samples. In these miRNAs, miR-23b
(MIMAT0000418) of the recurrence group displayed the most marked
change compared to that of the healthy control and non-recurrence
group. In the data for the upregulated miRNAs, fold changes were at
lower levels than those of the downregulated miRNAs. These results
led us to select miR-23b as a potential predictive marker in GC
patients.
 | Table I.Background of 6 GC patients and 3
healthy volunteers subjected to microRNA array analysis. |
Table I.
Background of 6 GC patients and 3
healthy volunteers subjected to microRNA array analysis.
| A, GC patients |
|---|
|
|---|
| Case no. | 1 | 2 | 3 | 4 | 5 | 6 |
|---|
| Age/Race | 61/Jpn. | 60/Jpn. | 66/Jpn. | 59/Jpn. | 72/Jpn. | 76/Jpn. |
| Sex | F | M | M | M | F | M |
| TNM stage | I | I | I | I | I | I |
| Recurrence
(location) | – | – | – | + (Liver) | + (Liver) | + Liver) |
| Tumor size
(cm) | 2.3 | 6.3 | 5.0 | 4.5 | 6.7 | 5.5 |
|
Differentiation | Mod | Mod | Por | Mod | Mod | Por |
| Tumor
differentiation | T2 | T2 | T2 | T2 | T2 | T2 |
| Lymph node
metastasis | n (−) | n (−) | n (−) | n (−) | n (−) | n (−) |
| Clinical
outcome | Survival | Survival | Survival | Death | Death | Death |
|
| B, Healthy
volunteers |
|
| No. | 1 | 2 | 3 |
|
|
|
|
| Age/race | 71/Jpn. | 62/Jpn. | 63/Jpn. |
|
|
|
| Sex | M | F | M |
|
|
|
| Table II.The 5 markedly downregulated and
upregulated miRNAs in plasma exosomes of stage I GC patients with
recurrence by miRNA array analysis. |
Table II.
The 5 markedly downregulated and
upregulated miRNAs in plasma exosomes of stage I GC patients with
recurrence by miRNA array analysis.
|
|
|
| Fold-change |
|
|
|
|
|
| Ranks | microRNA | MiRBase no. | Recurrent GC vs.
healthy controls | Recurrent GC vs.
non-recurrent GC |
|---|
| Downregulation |
| 1 | miR-23b-3p | MIMAT 0000418 | 0.30 | 0.35 |
| 2 | miR-3135b | MIMAT 0018985 | 0.33 | 0.52 |
| 3 | miR-6131 | MIMAT 0024615 | 0.35 | 0.55 |
| 4 | miR-6850-3p | MIMAT 0027601 | 0.38 | 0.60 |
| 5 | miR-187-5p | MIMAT 0004561 | 0.49 | 0.62 |
| Upregulation |
| 1 | miR-21-5p | MIMAT 0000076 | 2.58 | 2.15 |
| 2 | miR-106a-5p | MIMAT 0000103 | 2.54 | 2.13 |
| 3 | miR-221-3p | MIMAT 0000278 | 2.53 | 2.27 |
| 4 | miR-223-3p | MIMAT 0000280 | 2.53 | 2.17 |
| 5 | miR-6511a-5p | MIMAT 0025478 | 2.47 | 2.12 |
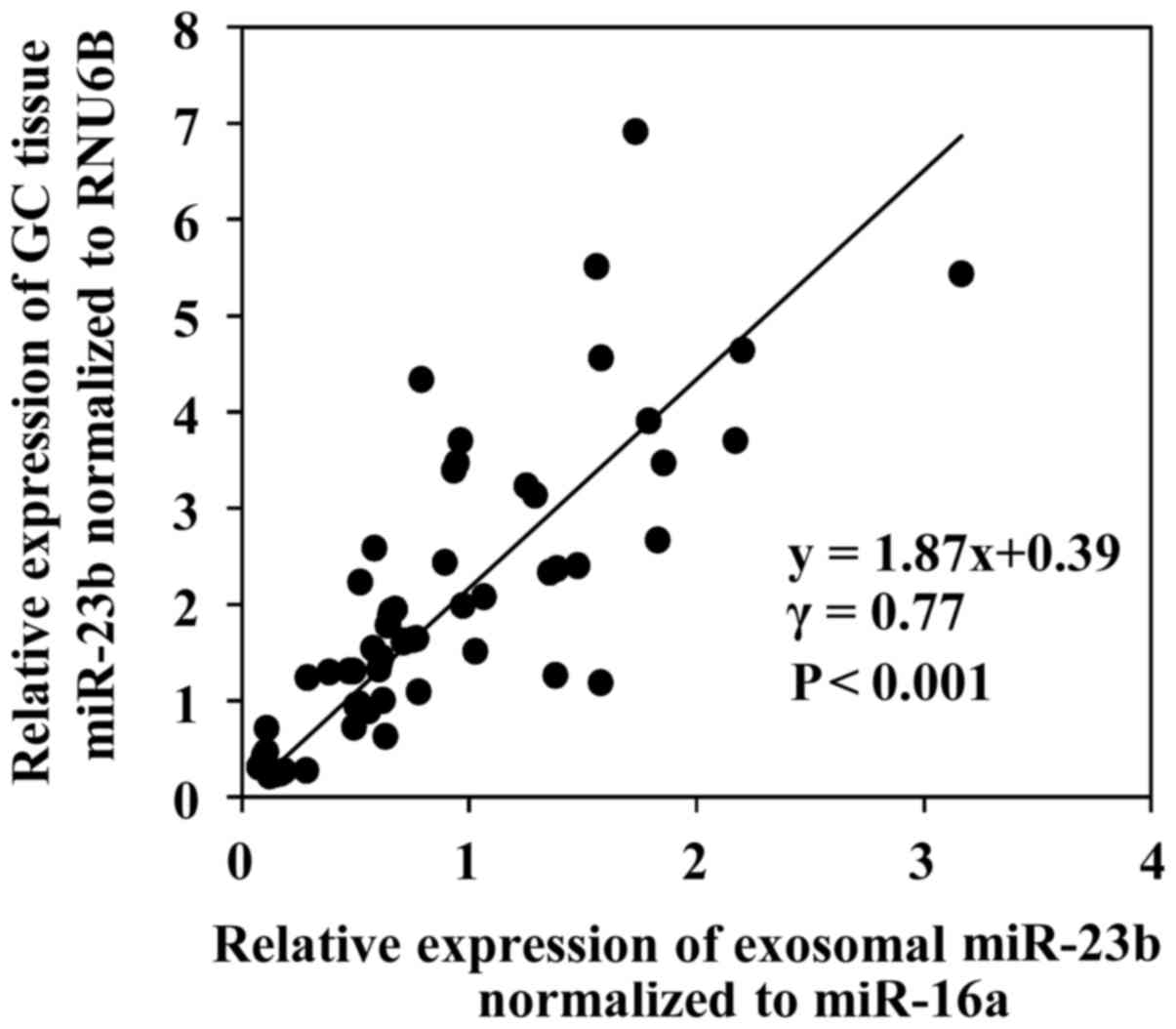
Expression of miR-23b in the GC
tissues and plasma exosomes
Expression of miR-23b was assessed by qRT-PCR in
plasma exosomal samples and primary tissues collected from GC
patients. First, we examined the correlation between exosomal
miR-23b levels and miR-23b expression in primary tumor tissues in
the same patients. Sixty patients with stage I (15 cases), stage II
(15 cases), stage III (15 cases) or stage IV (15 cases) GC were
subjected in this analysis. As displayed in Fig. 2, a positive significant correlation
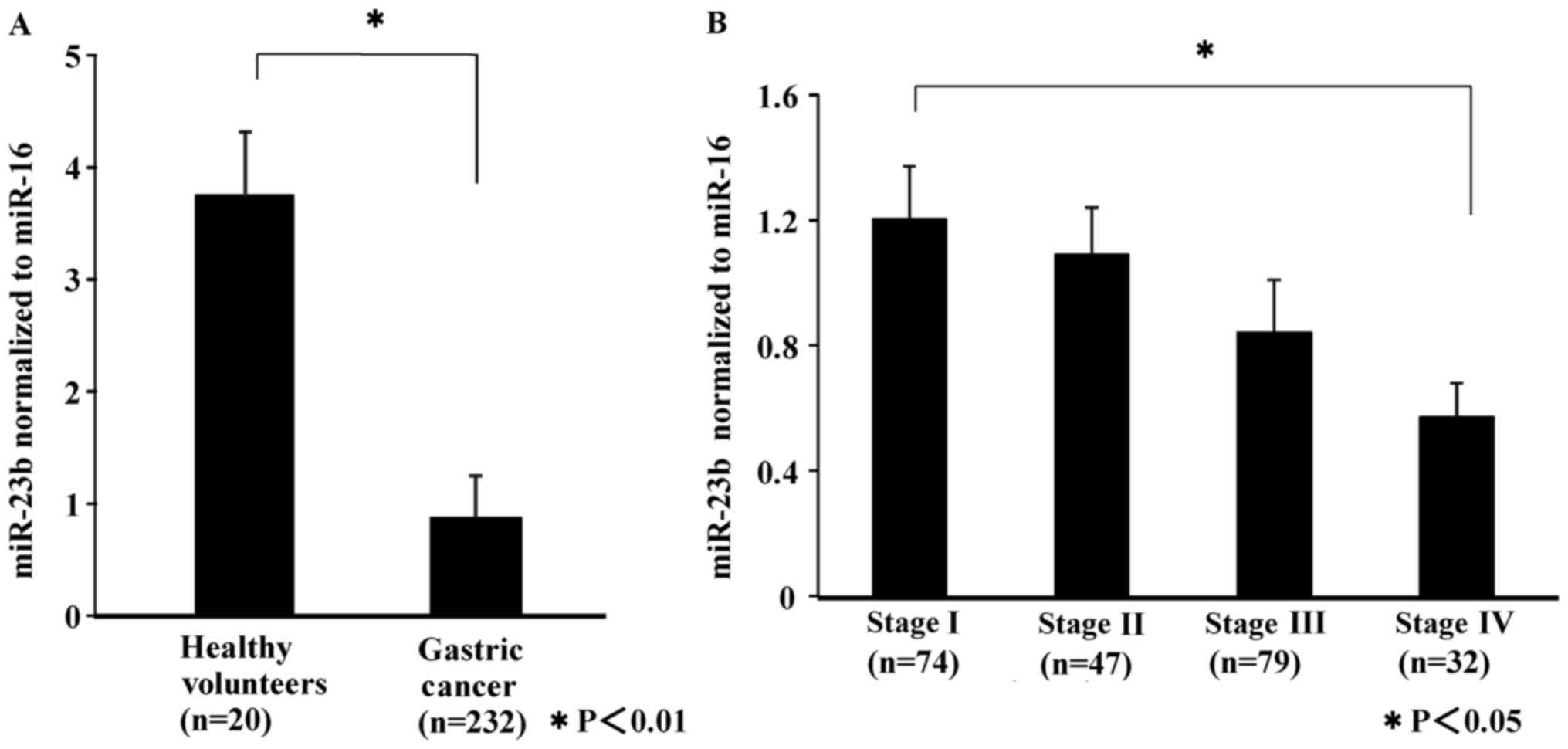
was demonstrated between them (P<0.01). Subsequenlty, exosomal
miR-23b levels from 232 patients with stage I (74 cases), stage II
(47 cases), stage III (79 cases) and stage IV (32 cases) GC and 20
healthy volunteers were compared. As displayed in Fig. 3A, exosomal miR-23b levels of GC
patients were significantly lower than those of the healthy
controls (P<0.01). Furthermore, with the progression of cancer,
exosomal miR-23b levels decreased (Fig.
3B). In stage IV patients, the miR-23b levels decreased
significantly (P<0.05).
Association between exosomal miR-23b
levels and clinicopathological factors
To evaluate the correlation between the expression
of exosomal miR-23b levels and the clinicopathological factors, 232
patients were divided into two groups, in which the expression of
exosomal miR-23b levels was either high or low (Table III). The cut-off level was
determined as the median of the miR-23a expression levels (0.78). A
statistically significant association was observed between the
miR-23b and the tumor size, depth of invasion, liver metastasis and
TNM stage.
| Table III.Relationship between the
clinicopathological factors of patients and the expression of
miR-23b. |
Table III.
Relationship between the
clinicopathological factors of patients and the expression of
miR-23b.
| Variables | miR-23b low
(n=100), n (%) | miR-23b high
(n=132), n (%) | P-value |
|---|
| Sex |
|
|
|
|
Male | 74 (74.0) | 91
(68.9) | 0.400 |
|
Female | 26 (26.0) | 41
(31.1) |
|
| Tumor size
(cm) |
|
|
|
|
<5 | 36 (36.0) | 68
(51.5) | 0.019 |
| ≥5 | 64 (64.0) | 64
(48.5) |
|
|
Differentiation |
|
|
|
|
Well/moderate | 60 (60.0) | 67
(50.8) | 0.161 |
|
Poor/other | 40 (40.0) | 65
(49.2) |
|
| Depth of
invasion |
|
|
|
|
pT1 | 21 (21.0) | 45
(34.1) | 0.029 |
|
≥pT2 | 79 (79.0) | 87
(65.9) |
|
| Lymphatic
invasion |
|
|
|
| Ly
(−) | 35 (35.0) | 64
(48.5) | 0.184 |
| Ly
(+) | 65 (65.0) | 68
(51.5) |
|
| Venous
invasion |
|
|
|
| V
(−) | 39 (39.0) | 58
(43.9) | 0.450 |
| V
(+) | 61 (61.0) | 74
(56.1) |
|
| Lymph node
metastasis |
|
|
|
| N
(−) | 35 (35.0) | 59
(44.7) | 0.136 |
| N
(+) | 65 (65.0) | 73
(55.3) |
|
| Liver
metastasis |
|
|
|
| H
(−) | 93 (93.0) | 130 (98.5) | 0.032 |
| H
(+) | 7
(7.0) | 2
(1.5) |
|
| Peritoneum
dissemination |
|
|
|
| P
(−) | 87 (87.0) | 121 (91.7) | 0.248 |
| P
(+) | 13 (13.0) | 11
(8.3) |
|
| Distant
metastasis |
|
|
|
| M
(−) | 93 (93.0) | 128 (95.5) | 0.282 |
| M
(+) | 7
(7.0) | 4
(4.5) |
|
| TNM stage |
|
|
|
| I | 24 (24.0) | 50
(37.9) | 0.034 |
| II | 22 (22.0) | 25
(18.9) |
|
|
III | 34 (34.0) | 45
(34.1) |
|
| IV | 20 (20.0) | 12
(9.1) |
|
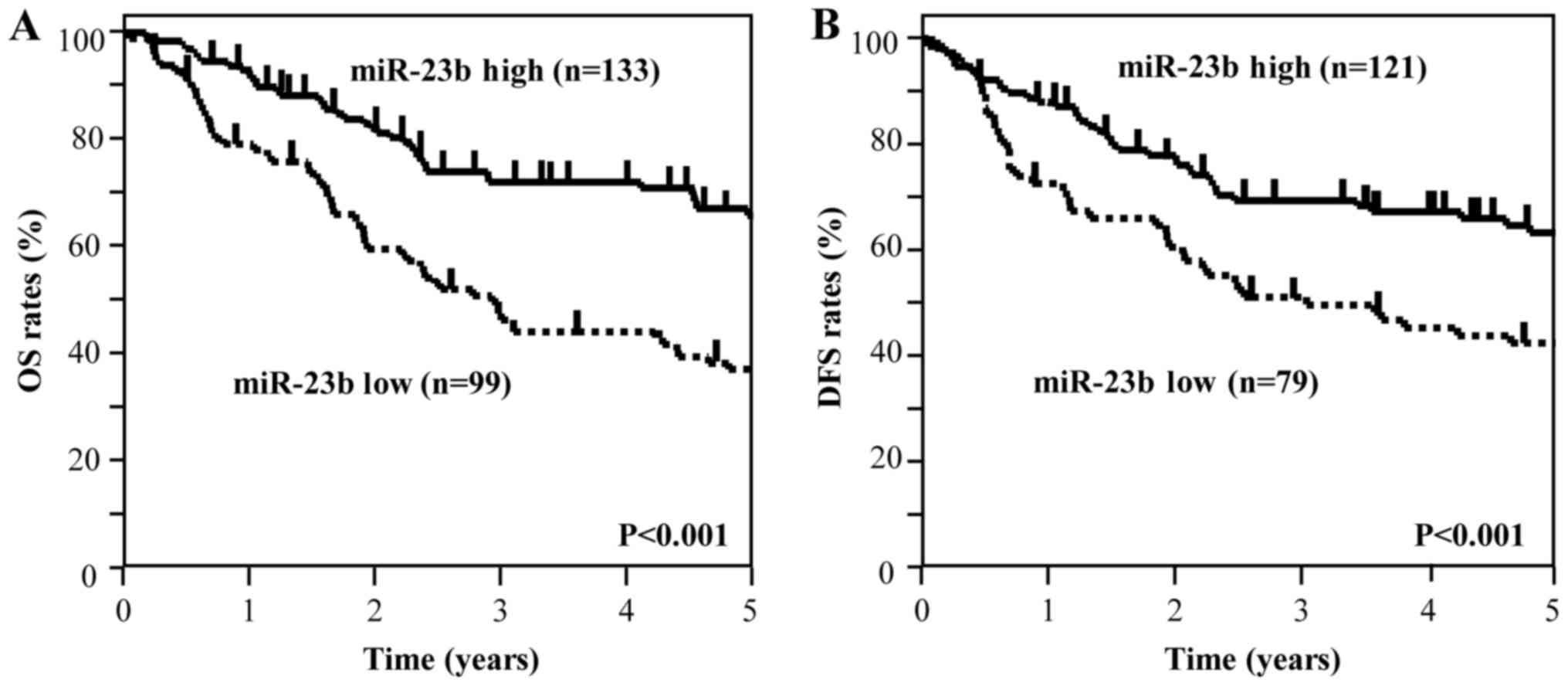
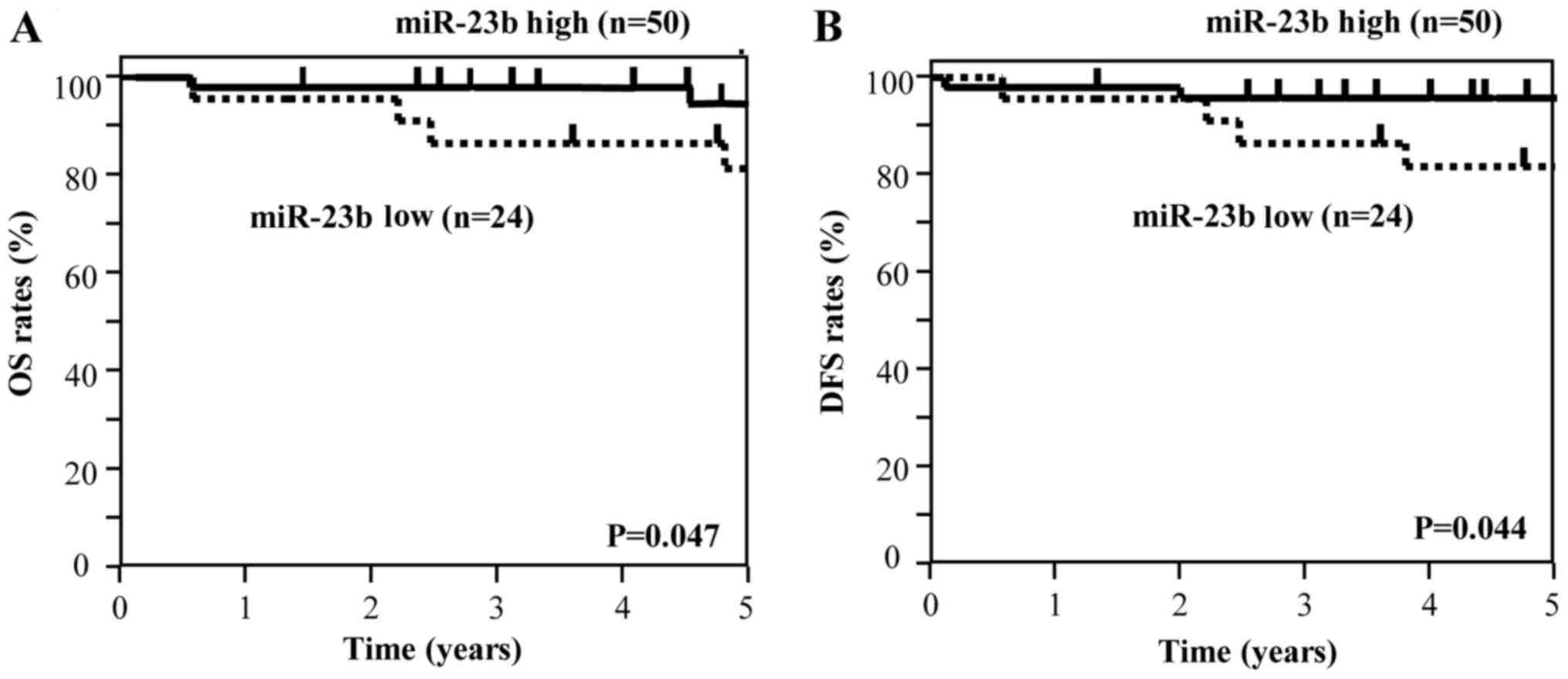
Kaplan-Meier OS and DFS survival
curves based on exosomal miR-23b levels
A comparison was made between the Kaplan-Meier OS
curves of all patients (n=232) and the DFS curves of patients who
had experienced curative surgery (n=200). In all patients, the low
miR-23b group exhibited a significantly worse OS than those in the
high miR-23b group (Fig. 4A). In
those patients who had undergone curative surgery, the low miR-23b
group showed a significantly worse DFS than those in the high
miR-23b group (Fig. 4B). An
analysis of the data at each stage revealed that, in patients with
stage I (n=74), the low miR-23b group showed a significantly worse
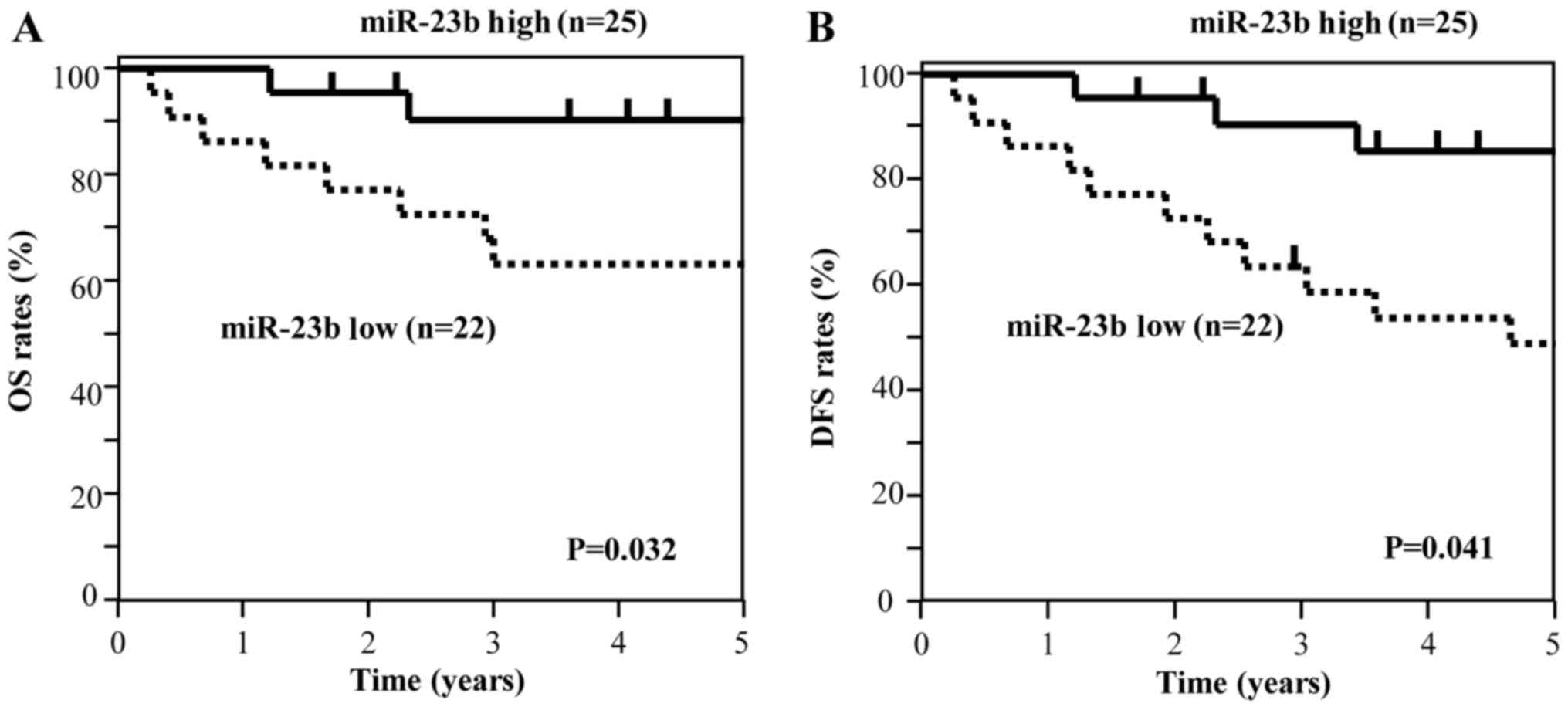
OS and DFS than those in the high miR-23b group (Fig. 5). In patients with stage II GC
(n=47), the low miR-23b group showed a significantly worse OS and
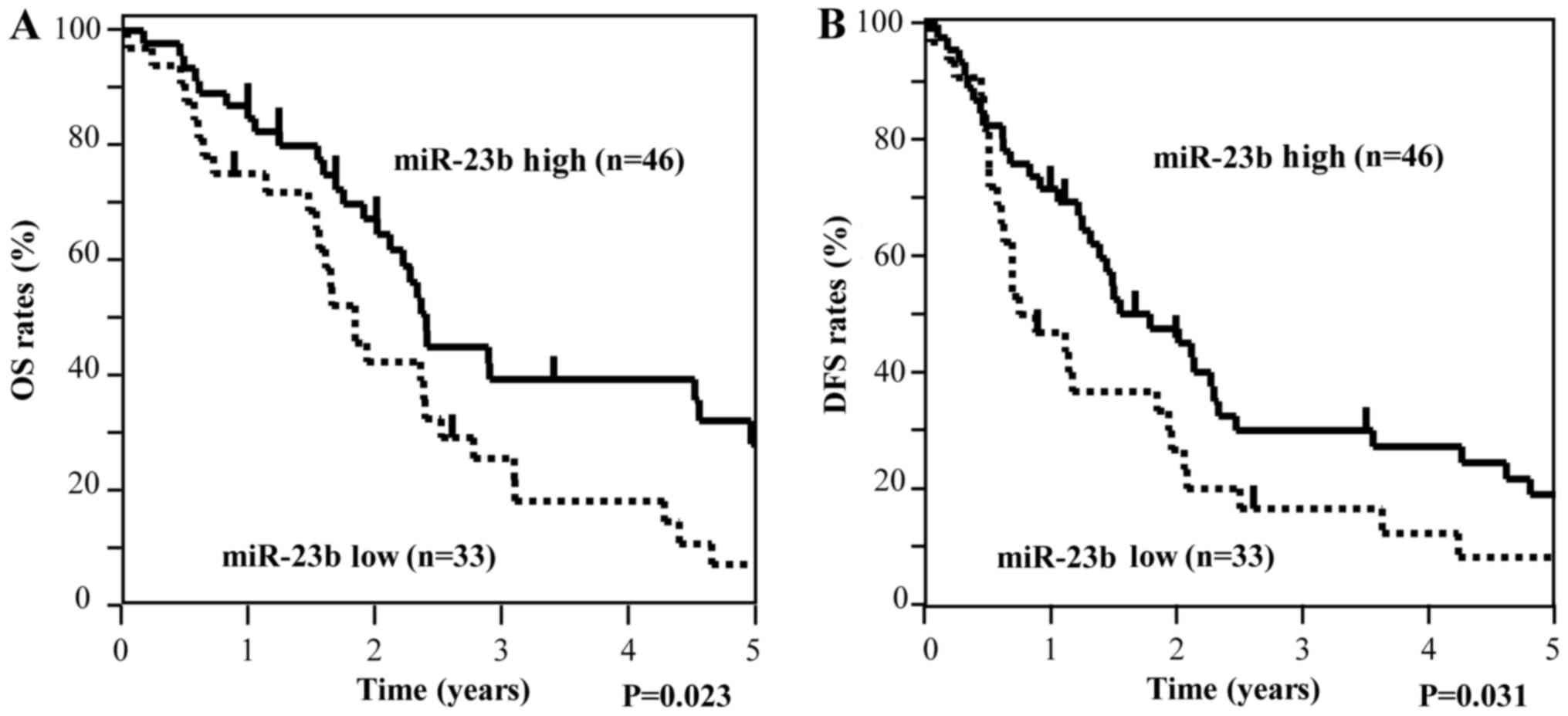
DFS than those in the high miR-23b group (Fig. 6). Among stage III GC patients
(n=79), the low miR-23b group had a significantly worse OS and DFS
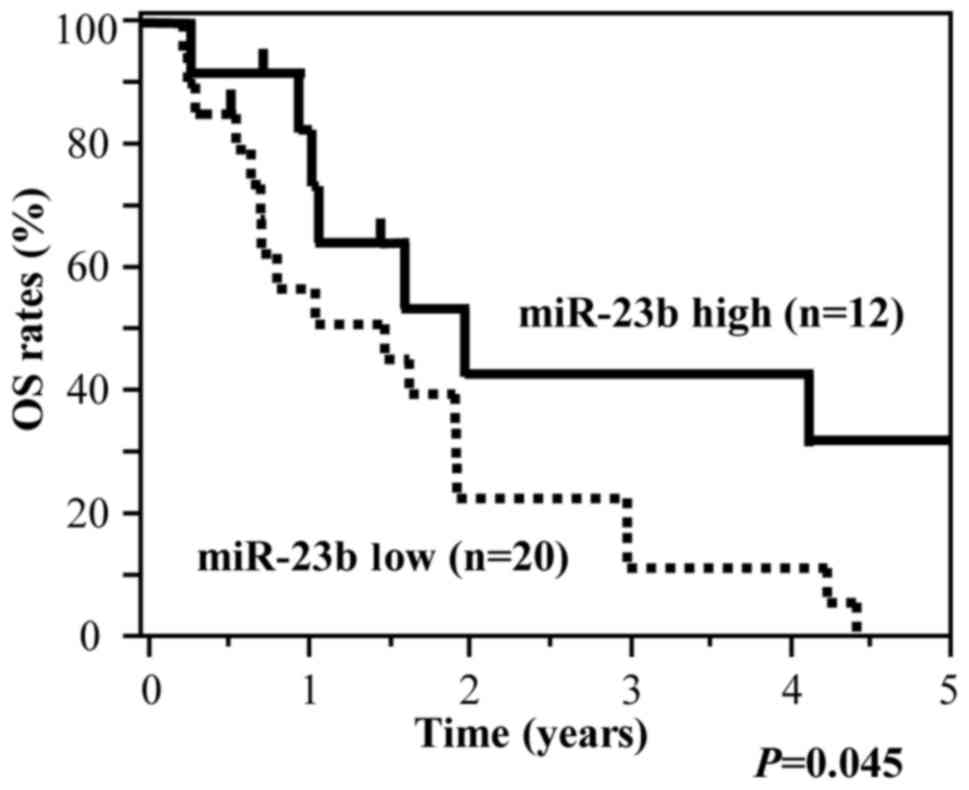
compared to the high miR-23b group (Fig. 7). As for GC patients at stage IV
(n=32), the low miR-23b group was observed to have significantly
worse OS than those in the high miR-23b group (Fig. 8). These data indicated that a low
expression of exosomal miR-23b correlated with recurrence and poor
prognosis in all stages.
Univariate and multivariate Cox
proportional hazard regression analysis for OS and DFS
Univariate and multivariate Cox analysis for OS and
DFS in GC patients was examined. Multivariate analysis was
performed for variables that showed significance in univariate
analysis. Table IV displays the
results of univariate and multivariate analysis for the OS of all
patients (n=232) and the DFS of those patients who had received
curative surgical procedures (n=200). In the multivariate analysis
for OS, depth of invasion, lymphatic invasion, liver metastasis,
peritoneum dissemination and exosomal miR-23b showed significance.
In the multivariate analysis for DFS, tumor size, depth of
invasion, lymph node metastasis and exosomal miR-23b showed
significance for DFS. We then considered the prognostic value of
these factors at each stage of tumor development. In the
multivariate analysis of patients with stage I GC, depth of
invasion and exosomal miR-23b demonstrated significance for both OS
and DFS (Table V). In the
multivariate analysis of patients with stage II GC, exosomal
miR-23b showed significance for OS and DFS (Table VI). In the multivariate analysis of
patients with stage III GC, exosomal miR-23b showed significance
for OS and DFS (Table VII). The
multivariate analysis at stage IV GC patients indicated that
exosomal miR-23b showed significance for OS (Table VIII). These results led us to
believe that plasma exosomal miR-23b levels were an independent
prognostic factor in GC patients of all four stages of tumor
development.
| Table IV.Univariate and multivariate Cox
analyses for OS in all patients and DFS in patients who had
undergone curative surgery. |
Table IV.
Univariate and multivariate Cox
analyses for OS in all patients and DFS in patients who had
undergone curative surgery.
| A, OS |
|---|
|
|---|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | RC | Hazard ratio (95%
CI) | P-value | RC | Hazard ratio (95%
CI) | P-value |
|---|
| Tumor size | 1.06 | 2.73
(1.79–4.25) | <0.001 | 0.447 | 1.56
(0.99–2.52) | 0.065 |
| Depth of
invasion | 2.69 | 7.74
(6.16–8.22) | <0.001 | 1.833 | 6.25
(2.07–9.14) | 0.001 |
| Lymph node
metastasis | 1.62 | 5.09
(3.12–8.17) | <0.001 | 0.284 | 1.32
(0.72–2.53) | 0.362 |
| Lymphatic
invasion | 1.36 | 3.89
(2.45–6.47) | <0.001 | 0.258 | 2.16
(1.20–3.99) |
0.010 |
| Venous
invasion | 1.17 | 3.22
(2.07–5.16) | <0.001 | 0.463 | 1.58
(0.94–2.77) |
0.080 |
| Histological
type | −0.13 | 0.87
(0.58–1.29) |
0.513 |
|
|
|
| Liver
metastasis | 1.78 | 5.94
(2.75–11.35) | <0.001 | 1.667 | 5.29
(1.92–12.42) | 0.003 |
| Peritoneum
dissemination | 1.18 | 3.27
(1.92–5.33) | <0.001 | 1.224 | 3.40
(1.80–6.07) | 0.001 |
| miR-23b | −0.83 | 0.45
(0.29–0.64) | <0.001 | −0.556 | 0.57
(0.37–0.78) | 0.011 |
|
| B, DFS |
|
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
Variables | RC | Hazard ratio
(95% CI) | P-value | RC | Hazard ratio
(95% CI) | P-value |
|
| Tumor size | 1.12 | 3.38
(2.14–5.49) | <0.001 | 0.557 | 1.74
(1.07–2.90) | 0.024 |
| Depth of
invasion | 2.76 | 5.79
(6.57–11.78) | <0.001 | 2.046 | 7.73
(2.52–13.87) | 0.001 |
| Lymph node
metastasis | 1.89 | 6.67
(3.88–12.34) | <0.001 | 0.671 | 1.95
(1.03–3.94) | 0.039 |
| Lymphatic
invasion | 1.45 | 4.24
(2.57–7.36) | 0.001 | 0.399 | 1.49
(0.86–2.69) | 0.154 |
| Venous
invasion | 1.59 | 4.91
(2.92–8.78) | 0.001 | 0.474 | 1.60
(0.92–2.97) | 0.096 |
| Histological
type | 0.12 | 1.13
(0.74–1.72) | 0.565 |
|
|
|
| miR-23b | −0.48 | 0.61
(0.40–0.75) | 0.023 | −0.43 | 0.64
(0.41–0.91) | 0.041 |
| Table V.Univariate and multivariate Cox
analyses for OS and DFS in patients with stage I GC. |
Table V.
Univariate and multivariate Cox
analyses for OS and DFS in patients with stage I GC.
| A, OS |
|---|
|
|---|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | RC | HR (95% CI) | P-value | RC | HR (95% CI) | P-value |
|---|
| Tumor size | −0.01 | 0.99
(0.14–4.62) | 0.994 |
|
|
|
|
Lymph-node metastasis | 0.71 | 2.04
(0.11–12.13) | 0.547 |
|
|
|
|
Lymphatic invasion | 0.72 | 2.05
(0.29–9.52) | 0.418 |
|
|
|
|
Vascular invasion | 1.37 | 3.92
(0.77–17.86) | 0.094 |
|
|
|
|
Histological type | 0.24 | 1.27
(0.28–6.46) | 0.752 |
|
|
|
| Depth
of invasion | 2.03 | 7.63
(1.68–18.79) | 0.010 | 2.00 | 7.41
(1.63–17.75) | 0.021 |
| miR-23b | −1.53 | 0.22
(0.02–0.87) | 0.032 | −1.49 | 0.22
(0.04–0.95) | 0.043 |
|
| B, DFS |
|
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
Variables | RC | HR (95%
CI) | P-value | RC | HR (95%
CI) | P-value |
|
| Tumor size | 0.01 | 1.01
(0.15–4.71) | 0.987 |
|
|
|
| Lymph-node
metastasis | 0.82 | 2.26
(0.12–13.30) | 0.493 |
|
|
|
| Lymphatic
invasion | 0.80 | 2.23
0.32–10.35) | 0.369 |
|
|
|
| Vascular
invasion | 1.38 | 3.97
(0.78–18.08) | 0.091 |
|
|
|
| Histological
type | 0.25 | 1.28
(0.28–6.50) | 0.746 |
|
|
|
| Depth of
invasion | 2.20 | 8.98
(1.98–15.62) | 0.016 | 2.15 | 8.57
(1.89–13.57) | 0.027 |
| miR-23b | −1.63 | 0.20
(0.03–0.81) | 0.037 | −1.58 | 0.21
(0.03–0.91) | 0.044 |
| Table VI.Univariate and multivariate Cox
analyses for OS and DFS in patients with stage II GC. |
Table VI.
Univariate and multivariate Cox
analyses for OS and DFS in patients with stage II GC.
| A, OS |
|---|
|
|---|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | RC | HR (95% CI) | P-value | RC | HR (95% CI) | P-value |
|---|
| Tumor size | 1.24 | 3.44
(1.17–11.40) | 0.029 | 1.07 | 2.90
(0.97–9.75) | 0.061 |
| Lymph-node
metastasis | −0.53 | 0.59
(0.20–1.74) | 0.333 |
|
|
|
| Lymphatic
invasion | −0.15 | 0.86
(0.29–3.15) | 0.806 |
|
|
|
| Vascular
invasion | 1.25 | 3.49
(0.68–63.54) | 0.153 |
|
|
|
| Histological
type | 0.78 | 2.19
(0.75–6.78) | 0.152 |
|
|
|
| Depth of
invasion | 2.04 | 8.77
(2.87–9.76) | 0.469 |
|
|
|
| miR-23b | −1.14 | 0.32
(0.07–0.78) | 0.025 | −1.25 | 0.39
(0.09–0.88) | 0.042 |
|
| B, DFS |
|
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
Variables | RC | HR (95%
CI) | P-value | RC | HR (95%
CI) | P-value |
|
| Tumor size | 1.21 | 3.37
(1.15–11.08) | 0.027 | 1.07 | 2.91
(0.98–9.63) | 0.057 |
| Lymph-node
metastasis | −0.39 | 0.67
(0.23–1.97) | 0.464 |
|
|
|
| Lymphatic
invasion | −0.13 | 0.88
(0.29–3.22) | 0.833 |
|
|
|
| Vascular
invasion | 1.40 | 4.04
(0.80–73.30) | 0.100 |
|
|
|
| Histological
type | 0.79 | 2.20
(0.76–6.74) | 0.144 |
|
|
|
| Depth of
invasion | 2.05 | 8.07
(2.31–8.87) | 0.393 |
|
|
|
| miR-23b | −1.37 | 0.26
(0.06–0.72) | 0.020 | −1.23 | 0.29
(0.07–0.91) | 0.040 |
| Table VII.Univariate and multivariate analyses
of the prognostic factors for OS in patients with stage III GC. |
Table VII.
Univariate and multivariate analyses
of the prognostic factors for OS in patients with stage III GC.
| A, OS |
|---|
|
|---|
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | RC | HR (95% CI) | P-value | RC | HR (95% CI) | P-value |
|---|
| Tumor size | −0.01 | 0.11
(0.54–0.91) | 0.045 | −2.21 | 0.19
(0.72–2.08) | 0.113 |
| Lymph-node
metastasis | −2.52 | 0.08
(0.01–1.52) | 0.080 |
|
|
|
| Lymphatic
invasion | 0.54 | 1.71
(0.79–4.48) | 0.186 |
|
|
|
| Vascular
invasion | 0.51 | 1.66
(0.82–3.83) | 0.164 |
|
|
|
| Histological
type | −0.26 | 0.77
(0.45–1.31) | 0.338 |
|
|
|
| Depth of
invasion | −1.17 | 0.31
(0.06–5.54) | 0.331 |
|
|
|
| miR-23b | −0.61 | 0.55
(0.32–0.73) | 0.026 | −0.58 | 0.56
(0.33–0.86) | 0.037 |
|
| B, DFS |
|
| Univariate
analysis | Multivariate
analysis |
|
|
|
|
|
Variables | RC | HR (95%
CI) | P-value | RC | HR (95%
CI) | P-value |
|
| Tumor size | −0.07 | 0.93
(0.54–1.73) | 0.819 |
|
|
|
| Lymph-node
metastasis | −1.53 | 0.22
(0.04–3.90) | 0.227 |
|
|
|
| Lymphatic
invasion | 0.56 | 1.74
(0.47–0.92) | 0.044 | 0.55 | 1.74
(0.87–2.01) | 0.126 |
| Vascular
invasion | 0.35 | 1.42
(0.77–2.88) | 0.273 |
|
|
|
| Histological
type | 0.74 | 3.01
(0.62–1.63) | 0.985 |
|
|
|
| Depth of
invasion | −0.24 | 0.79
(0.17–11.98) | 0.820 |
|
|
|
| miR-23b | −0.47 | 0.58
(0.38–0.81) | 0.038 | −0.47 | 0.62
(0.41–0.89) | 0.044 |
| Table VIII.Univariate and multivariate Cox
analyses for OS in patients with stage IV GC. |
Table VIII.
Univariate and multivariate Cox
analyses for OS in patients with stage IV GC.
|
| Univariate
analysis | Multivariate
analysis |
|---|
|
|
|
|
|---|
| Variables | RC | HR (95% CI) | P-value | RC | HR (95% CI) | P-value |
|---|
| Tumor size | −0.29 | 0.75
(0.32–1.94) | 0.524 |
|
|
|
| Lymph-node
metastasis | 1.31 | 3.71
(1.23–16.22) | 0.038 | 0.35 | 1.42
(0.27–8.30) | 0.679 |
| Lymphatic
invasion | 1.31 | 3.69
(1.47–11.25) | 0.044 | 0.95 | 2.58
(0.81–10.98) | 0.115 |
| Vascular
invasion | 0.72 | 2.06
(0.93–4.70) | 0.075 |
|
|
|
| Histological
type | 0.26 | 1.30
(0.50–3.04) | 0.566 |
|
|
|
| Depth of
invasion | −0.21 | 0.71
(0.27–9.78) | 0.780 |
|
|
|
| Peritoneum
dissemination | −0.54 | 0.58
(0.26–1.43) | 0.225 |
|
|
|
| Liver
metastasis | 0.68 | 1.98
(0.83–4.44) | 0.118 |
|
|
|
| miR-23b | −0.88 | 0.42
(0.16–0.87) | 0.030 | −0.38 | 0.68
(0.24–0.97) | 0.042 |
Discussion
In the present study, we demonstrated that plasma
exosomal miR-23b offers a great potential as a minimally invasive
predictive biomarker for recurrence and prognosis in GC patients.
Low expression of exosomal miR-23b indicated a poor prognosis for
OS in GC patients at stage I, II, III and IV as well as for DFS in
GC patients at stage I, II and III.
Recently, many studies have revealed that miRNAs are
stable in the exosomes and show promise as biomarkers. They are
minimally invasive in several types of cancers, including GC
(9,10). It is known that plasma exosome plays
an important role in cell-to-cell signaling (12–14).
In this study, firstly we selected a recurrence-predictor exosomal
miRNA using the miRNA microarray. miR-23b expressed the lowest
downregulation in stage I GC patients who showed recurrence after
surgery (recurrence group) compared with that of stage I GC
patients who did not show recurrence after surgery (non-recurrence
group) and healthy controls. We also examined the miRNA which
demonstrated upregulation in this miRNA microarray analysis.
However, differences between the recurrence, non-recurrence and
healthy control group were small. Therefore, we selected miR-23b as
a predictive biomarker for recurrence of GC patients.
miR-23b is a member of the miR-23b/27b/24 cluster
(9q22.32). Functionally, overexpression of miR-23b functions as a
tumor suppressor and it has been shown to inhibit migration,
proliferation, invasion and tumor growth in various cancers
(19–21). Zhuang et al (22) as well as Pellegrino et al
(23) have revealed that miR-23b is
a tumor-suppressor microRNA, and that low-expression level of
miR-23b was associated with metastasis in patients with breast and
colon cancer.
In the present study, we revealed that plasma
exosomal miR-23b levels of GC patients were significantly lower
than those of healthy individuals. These results indicated that
miR-23b may be useful in the diagnosis of GC patients. Using tumor
tissues, many researchers have demonstrated that the expression of
miR-23b wass significantly downregulated in prostate,
hepatocellular, bladder and colon cancer (19,24,25).
Using the plasma samples (but not exosomes), Kou et al
(26) reported that miR-23b was
significantly downregulated in colon cancer patients. Although
these studies did not use exosomes, the results obtained may
support our findings. In addition, our data revealed a significant
association between the exosomal miR-23b levels and the expression
of miR-23b in primary tumor tissues collected from the same
patients. Our results indicated that the tumor tissues may be the
source of plasma exosomal miR-23b. Furthermore, we evaluated the
relationship between exosomal miR-23b levels and the
clinicopathological factors of patients, and revealed that the
expression of miR-23b had a significant association with tumor
size, depth of invasion, liver metastasis and stage. In the present
study, miR-23b was selected by miRNA microarray analyses which were
performed between patients without recurrence (non-recurrence) and
patients with liver metastasis. Therefore, plasma miR-23b may have
shown a significant relationship with ‘liver metastasis’, not
‘peritoneal dissemination’ or ‘distant metastasis’. Using tissues
samples, but not exosomes, Ma et al (27) reported that miR-23b levels were
associated with lymph node metastasis, stage and depth of
invasion.
The prognostic value of plasma miR-23b levels has
been reported in patients with various types of cancer, but the
results remained controversial. Kou et al (26) reported that downregulation of
miR-23b in plasma was associated with poor prognosis in patients
with colorectal cancer. In contrast, Zhuang et al (22) reported that upregulation of plasma
miR-23b was associated with a poor prognosis of GC. In this study,
the low expression of plasma exosomal miR-23b was significantly
associated with poor overall survival and shorter recurrence-free
survival in GC patients. The instability of miRNA may be one of the
reasons for this controversy. Since miRNAs are preserved in an
intact form in exosomes, their stability as biomarkers may be
enhanced as a result (15–17). In the present study, we used plasma
exosome, and examined its usefulness as predictive biomarker for
recurrence and prognosis of GC patients at each tumor stage. Our
results demonstrated that low expression of exosomal miR-23b was
significantly associated with poor OS and shorter DFS in GC
patients with stage I, II, III and IV. Furthermore, we found that
exosomal miR-23b was a significant independent prognostic factor
for OS and DFS in GC patients with stage I, II and III and for OS
in patients with stage IV. To the best of our knowledge, no
previous study has clarified the prognostic value of exosomal
miR-23b as a biomarker in patients with GC at each tumor stage.
The current standard treatment of GC differs
according to stage. In Japan, the standard treatment for stage I is
endoscopic submucosal dissection or laparoscopic gastrectomy. For
patients with stage II and III (except SS/N0 patients), TS-1 is
administrated for one year after surgery (28,29).
Aggressive postoperative adjuvant chemotherapy, in the form of the
administration of capecitabine plus oxaliplatin, is performed in
the first half year after surgery for patients with stage III GC
(30). However, recurrent cases
exist in patients with stage I who underwent curative surgery and
in patients with stage II and III who completed postoperative
adjuvant chemotherapy. In order to improve prognosis, it is
important to clarify high-risk cases of recurrence at each tumor
stage. In our study, we revealed that exosomal miR-23b was useful
for the selection of GC patients at stage I, II and III who are at
high risk of recurrence.
One of the limitations of our study is that it was a
retrospective study. Therefore, a larger prospective study is
required to clarify the value of exosomal miR-23b. In addition, the
target gene of miR23b was not examined in our study. Previous
studies have reported Pyk2, Ywhaz, ATG12 and HMGB2 as target genes
for miR-23b (19,20,31,32).
We are planning to examine these issues in our next study.
In summary, this study has indicated that exosomal
miR-23b is a promising, minimally invasive biomarker for the
diagnosis, prediction of recurrence and prognosis of patients with
GC. Therefore, further development of this exosomal microRNA is
expected.
Acknowledgements
We thank Miss J Tamura for her excellent technical
assistance and all the members of the upper gastrointestinal group
for their clinical suggestions.
Funding
The present study was supported by a JSPS KAKENHI
(grant nos. JP15K10150 and 17K10608).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
HI conceived and designed the study. YK, HI and RF
wrote the manuscript. YK and HI performed the experiment. YK, YS,
DT, HM, YI, NS, TK and MH collected the clinical data. HI and RF
reviewed and edited the manuscript. All authors read and approved
the manuscript and agree to be accountable for all aspects of the
research in ensuring that the accuracy or integrity of any part of
the work are appropriately investigated and resolved.
Ethics approval and consent to
participate
The study protocol conformed to the guidelines of
the Teikyo University Ethics Committee and was approved by the
review board of Teikyo University (approval no. 09-081-3). Written
informed consent was obtained from all patients.
Consent for publication
Written informed consent was obtained from all
patients for the publication of their data.
Competing interests
The authors state that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
GC
|
gastric cancer
|
|
miRNA
|
microRNA
|
|
qRT-PCR
|
quantitative real-time reverse
transcription-PCR
|
References
|
1
|
Uemura N, Okamoto S, Yamamoto S, Matsumura
N, Yamaguchi S, Yamakido M, Taniyama K, Sasaki N and Schlemper RJ:
Helicobacter pylori infection and the development of gastric
cancer. N Engl J Med. 345:784–789. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Grady WM and Tewai M: The next thing in
prognostic molecular markers: microRNA signatures of cancer. Gut.
59:706–708. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yi R, Li Y, Wang FL, Miao G, Qi RM and
Zhao YY: MicroRNAs as diagnostic and prognostic biomarkers in
colorectal cancer. World J Gastrointest Oncol. 8:330–340. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Tsai MM, Wand CS, Tsai CY, Huang HW, Chi
HC, Lin YH, Lu PH and Lin KH: Potential diagnostic, prognostic and
therapeutic target microRNAs in human gastric cancer. Int J Mol
Sci. 17:E9452016. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Wang H, Wang L, Wu Z, Sun R, Jin H, Ma J,
Liu L, Ling R, Yi J, Wang L, et al: Three dysregulated microRNAs in
serum as novel biomarkers for gastric cancer screening. Med Oncol.
31:2982014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Tsujiura M, Komatsu S, Ichikawa D,
Shiozaki A, Konishi H, Takeshita H, Moriumura R, Nagata H,
Kawaguchi T, Hirajima S, et al: Circulating miR-18a in plasma
contributes to cancer detection and monitoring in patients with
gastric cancer. Gastric Cancer. 18:271–279. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Ma GJ, Gu RM, Zhu M, Wen X, Li JT, Zhang
YY, Zhang XM and Chen SQ: Plasma post-operative miR-21 expression
in the prognosis of gastric cancers. Asian Pac J Cancer Prev.
14:7551–7554. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Gorur A, Fidanci Balci S, Unal Dogruer N,
Ayaz L, Akbayir S, Yaroglu Yildirim H, Dirlik M, Serin MS and Tamer
L: Determination of plasma microRNA for early detection of gastric
cancer. Mol Biol Rep. 40:2091–2096. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Kowal J, Tkach M and Théry C: Biogenesis
and secretion of exosome. Curr Opin Cell Biol. 29:116–125. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Ge Q, Zhou Y, Lu J, Bai Y, Xie X and Lu Z:
miRNA in plasma exosome is stable under different storage
conditions. Molecules. 19:1567–1575. 2014. View Article : Google Scholar
|
|
11
|
Colombo M, Raposo G and Théry C:
Biogenesis, secretion and intercellular interactions of exosomes
and other extracellular vesicles. Ann Rev Cell Dev Biol.
30:255–289. 2014. View Article : Google Scholar
|
|
12
|
Kadota T, Yoshioka Y, Fujita Y, Kuwano K
and Ochiya T: Extracellular vesicles in lung cancer-From bench to
bedside. Semin Cell Dev Biol. 67:39–47. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Ogata-Kawata H, Izumiya M, Kurioka D,
Honma Y, Yamada Y, Furuta K, Gunji T, Ohta H, Okamoto H, Sonoda H,
et al: Circulating exosomal microRNAsas biomarkers of colon cancer.
PLoS One. 9:e929212014. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Hannafon BN and Ding WQ: Intercelluar
communication by exosome-derived microRNAs in cancer. Int J Mol
Sci. 14:14240–14269. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Tovar-Camargo OA, Toden S and Goel A:
Exosomal microRNA biomarkers: Emerging frontiers in colorectal and
other human cancers. Expert Rev Mol Diagn. 16:553–567. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Dejima H, Iinuma H, Kanaoka R, Matsutani N
and Kawamura K: Exosomal microRNA in plasma as a non-invasive
biomarker for the recurrence of non-small cell lung cancer. Oncol
Lett. 13:1256–1263. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Tsukamoto M, Iinuma H, Yagi T, Matsuda K
and Hashiguchi Y: Circulating exosomal MicroRNA-21 as a biomarker
in each tumor stage of colorectal cancer. Oncology. 92:360–370.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Japanese Gastric Cancer Association:
Japanese gastric cancer treatment guidelines 2014 (ver.4). Gastric
Cancer. 20:1–19. 2017. View Article : Google Scholar
|
|
19
|
Salvi A, Sabelli C, Moncini S, Venturin M,
Arici B, Riva P, Portolani N, Giulini SM, De Petro G and Barlati S:
MicroRNA-23b mediates urokinase and c-met downmodulation and a
decreased migration of human hepatocellular carcinoma cells. FEBS
J. 276:2966–2982. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Li W, Liu Z, Chen L, Zhou L and Yao Y:
MicroRNA-23b is an independent prognostic marker and suppresses
ovarian cancer progression by targeting runt-related transcription
factor-2. FEBS Lett. 588:1608–1615. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Loftus JC, Ross JT, Paquette KM, Paulino
VM, Nasser S, Yang Z, Kloss J, Kim S, Berens ME and Tran NJ: miRNA
expression profiling in migration glioblastoma cells: Regulation of
cell migration and invasion by miR-23b via targeting of Pyk2. PLoS
One. 7:e398182012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Zhang H, Hao Y, Yang J, Zhou Y, Li J, Yin
S, Sun C, Ma M, Huang Y and Xi JJ: Genome-wide functional screening
of miR-23b as a pleiotropic modulator suppressing cancer
metastasis. Nat Commun. 2:5542011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pellegrino L, Stebbing J, Braga VM,
Frampton AE, Jacob J, Buluwela L, Jiao LR, Periyasamy M, Madsen CD,
Caley MP, et al: miR-23b regulates cytoskeletal remodeling,
motility and metastasis by directly targeting multiple transcripts.
Nucleic Acids Res. 41:5400–5412. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Majid S, Dar AA, Saini S, Arora S,
Shahryari V, Zaman MS, Chang I, Yamamura S, Tanaka Y, Deng G and
Dahiya R: miR-23b represses proto-oncogene Src kinase and functions
as methylation-silenced tumor suppressor with diagnostic and
prognostic significance in prostate cancer. Cancer Res.
72:6435–6446. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Goto Y, Kojima S, Nishikawa R, Enokida H,
Chiyomaru T, Kinoshita T, Nakagawa M, Naya Y, Ichikawa T and Seki
N: The microRNA-23b/27b/24-1 cluster is a disease progression
marker and tumor suppressor in prostate cancer. Oncotarget.
5:7748–7759. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kou CH, Zhou T, Han XL, Zhuang HJ and Qian
HX: Downregulation of miR-23b in plasma is associated with poor
prognosis in patients with colorectal cancer. Oncol Lett.
12:4838–4844. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Ma G, Dai W, Sang A, Yang X and Gao C:
Upregulation of microRNA-23a/b promotes tumor progression and
confers poor prognosis in patients with gastric cancer. Int J Clin
Exp Pathol. 7:8833–8840. 2014.PubMed/NCBI
|
|
28
|
Sakuramoto S, Sasako M, Yamaguchi T,
Kinoshita T, Fujii M, Nashimoto A, Furukawa H, Nakajima T, Ohashi
Y, Imamura H, et al: Adjuvant chemotherapy for gastric cancer with
S-1, an oral fluoropyrimidine. N Engl J Med. 357:1810–1820. 2007.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Sasako M, Sakuramoto S, Katai H, Kinoshita
T, Furukawa H, Yamaguchi T, Nashimoto A, Fujii M, Nakajima T and
Ohashi Y: Five-year outcomes of a randomized phase III trial
comparing adjuvant chemotherapy with S-1 versus surgery alone in
stage II or III gastric cancer. J Clin Oncol. 29:4387–4393. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Bang YJ, Van Cutsem E, Feyereislova A,
Chung HC, Shen L, Sawaki A, Lordick F, Ohtsu A, Omuro Y, Satoh T,
et al: Trastuzumab in combination with chemotherapy versus
chemotherapy alone for treatment of HER2-positive advanced gastric
or gastro-oesophageal junction cancer (ToGA): A phase 3,
open-label, randomised controlled trial. Lancet. 376:687–697. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
An Y, Zhang Z, Shang Y, Jiang X, Dong J,
Yu P, Nie Y and Zhao Q: miR-23b-3p regulates the chemoresistance of
gastric cancer cells by targeting ATG12 and HMGB2. Cell Death Dis.
6:e17662015. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zaman MS, Thamminana S, Shahryari V,
Chiyomaru T, Deng G, Saini S, Majid S, Fukuhara S, Chang I, Arora
S, et al: Inhibition of PTEN gene expression by oncogenic
miR-23b-3p in renal cancer. PLoS One. 7:e502032012. View Article : Google Scholar : PubMed/NCBI
|