Introduction
Chimeric antigen receptors (CARs) are synthetic
receptors that retarget T cells to tumor cell surface antigens in
order to eliminate the targeted tumor cells (1). CD19 CAR-T cell therapy has led to
encouraging responses in patients with relapsed/refractory
B-lineage hematological malignancies, including leukemia, lymphoma
and myeloma (2–5). However, despite the marked clinical
response in various types of B-cell neoplasms, the efficacy of
CAR-T cell therapy against relapsed/refractory lymphoma has not yet
been established (6,7). There are several challenges to
overcome in the therapy of B-cell non-Hodgkin lymphoma (B-NHL) by
CD19 CAR-T cells. Challenges of the CAR-T cell therapy for
relapsed/refractory lymphoma include selection of target antigens,
management of toxicity and modulation of the tumor microenvironment
(8,9).
Blocking tumor immune evasion by targeting the
immune checkpoints has become a research focus in the treatment of
relapsed or refractory tumors (10). Programmed death-1 (PD-1)/programmed
death-ligand 1 (PD-L1) are the most important immune checkpoints
identified to date, and have introduced a modern era of cancer
immunotherapy (11). A significant
correlation between the level of PD-1 (expressed on T cells)/PD-L1
(expressed on tumor cells) and the immunosuppression of T cells has
been reported (12). Several
clinical trials have confirmed the effects and clinical application
value of PD-1/PD-L1 inhibitors (13–15).
The PD-1 expression on T cells or PD-L1 expression on tumor cells
may compromise the efficacy of CD19 CAR-T cell therapy. Therefore,
treatment with CD19 CAR-T cells in combination with PD-1 inhibitors
may overcome the immunosuppression of the PD-1/PD-L1 axis and
improve the therapeutic effect on relapsed/refractory B-NHL. In a
previously reported case, a PD-1 inhibitor was administered to a
patient with refractory diffuse large B-cell lymphoma (DLBCL) and
progressive disease on day 26 after therapy with CD19 CAR-T cells
(16). The patient exhibited a
clinically significant response, an expansion of CD19 CAR-T cells
and decreased expression of PD-1.
It was hypothesized that CD19 CAR-T cells from
patient T cells with high PD-1 expression in combination with a
PD-1 inhibitor may overcome the immunosuppression induced by the
PD-1 pathway. The aim of the present study was to improve the
therapeutic efficacy in relapsed or refractory B-lineage
hematological malignancies, particularly lymphoma.
Materials and methods
Primary cells, cell lines and PD-1
inhibitor
Informed consent was provided by 7 patients with
lymphoma and healthy donor agreed to participate in this experiment
within a clinical trial at the Department of Hematology at Tianjin
First Central Hospital (Tianjin, China) with autologous CAR-T 19
cells (ChiCTR-ONN-16009862; Tianjin First Central Hospital Medical
Ethics Committee). All animal procedures were approved by the
institutional animal and care use committee of Tianjin First
Central Hospital. Human T cells with high PD-1 expression were
derived from the peripheral blood of seven patients with lymphoma
(males:females, 3:4; age: 25–68 years old). PD-1 normal expression
of human T cells was isolated from the peripheral blood of seven
healthy donors (males:females, 1:6; age, 22–45 years old). Raji
lymphoma cell lines were obtained from the American Type Culture
Collection (Manassas, VA, USA) and were cultured in RPMI-1640
medium (Gibco; Thermo Fisher Scientific, Inc., Waltham, MA, USA)
containing 10–20% fetal bovine serum (Gibco; Thermo Fisher
Scientific, Inc.), 1% penicillin/streptomycin, 2 mmol/l
L-glutamine, and 1 mmol/l sodium pyruvate at 37°C in a humidified
incubator with a 4% CO2 atmosphere. The PD-1 inhibitor
used was OPDIVO (nivolumab).
Isolation of peripheral blood
mononuclear cells (PBMCs) and transduction of T cells
Ethical approval and informed consent were obtained.
Patients with lymphoma and healthy donors agreed to participate
this experiment as part of a clinical trial at the Department of
Hematology at Tianjin First Central Hospital with autologous CAR-T
19 cells (ChiCTR-ONN-16009862). PBMCs of 7 patients and healthy
donors were isolated from buffy coat by Ficoll density gradient
centrifugation (500 × g for 10 min at room temperature).
CD3+ T cells were selected by MACS using CD3 microbeads
(Miltenyi Biotec, Inc., Cambridge, MA, USA) from the PBMCs. Then,
CD3+ T cells were stimulated with anti-CD3/anti-CD28
mAb-coated Human T-Expander beads (cat. no. 11141D; Thermo Fisher
Scientific, Inc., Waltham, MA, USA) and cultured in T-cell medium
X–Vivo 15 (Lonza Group, Ltd., Basel, Switzerland) supplemented with
250 IU/ml interleukin-2 (IL-2; Proleukin®; Novartis
International AG, Basel, Switzerland) at 37°C in a humidified
incubator with a 4% CO2. The manufacturer's instructions
were followed and performed as described by Kochenderfer et
al (5). At 4 days after
isolation and culture, T cells (3×106) were transduced
with a lentiviral vector encoding CD19 CAR constructs (5 µg;
lenti-EF1a-CD19-2rd-CAR; Creative Biolabs, Inc., Shirley, NY, USA)
and cultured in media containing recombinant human IL-2 (30 U/ml).
After 12 days in culture, T cells were analyzed by flow cytometry
to detect the CD19 CAR-T expression.
Flow cytometry
Flow cytometric analysis of PBMCs was performed
using 2–5×106 total cells/condition. To quantify
transgene expression in transduced T cells, cells were isolated and
stained with antibodies (1:200) for 15 min at room temperature.
CD19 expression on lymphoma cells was determined using
anti-CD19-phycoerythrin (PE; 1:200; cat. no. 560992; Beckman
Coulter, Inc., Brea, CA, USA). CD3 expression on lymphoma cells was
analyzed using anti-CD3-allophycocyanin (1:200; cat. no. 561800;
Beckman Coulter, Inc.). The expression of PD-1 on CD3+ T
lymphoma cells was analyzed using anti-CD297-fluorescein
isothiocyanate (1:200; cat. no. 558694; Miltenyi Biotec, Inc.). To
assess phenotypes of CAR-T cells, data were analyzed based on gated
CAR+/GFP+ cells using BD AccuriC6 software
(BD Biosciences, San Jose, CA, USA).
CAR-19 T cell proliferation in
vitro
The proliferation of CD19 CAR-T cells was detected
using Cell Counting Kit-8 (CCK-8; Dojindo Molecular Technologies,
Inc., Kumamoto, Japan). CCK-8 was added to the medium and cultured
simultaneously. The absorbance at 450 nm was determined as the
blank control. Absorbance was detected using an enzyme standard
meter at 450 nm at 0, 24 and 48 h.
Cytotoxicity of Raji lymphoma cells in
vitro
Each group of CD19 CAR-T cells (4×105)
combined with a PD-1 inhibitor (36 µg/ml; Bristol-Myers Squibb, New
York, NY, USA) were co-cultured with Raji lymphoma cells
(1×105; or not co-cultured) at a 4:1 ratio for 48 h in
the absence of supplemented cytokines. CD19 CAR-T cells were
isolated from the co-culture by MACS using CD3 microbeads (as
described above). Cytotoxicity was detected using a lactate
dehydrogenase (LDH) cytotoxicity test kit (Dojindo Molecular
Technologies, Inc.) at 490 nm at 0, 24 and 48 h.
Cytokine release assays
Cytokine release assays to detect tumor necrosis
factor-α (TNF-α) and interferon-γ (IFN-γ) were detected using ELISA
kits (cat. nos. 555268 and 550612; BD Biosciences). The absorbance
detection value was detected at 450 nm at 0, 12, 24 and 48 h. The
level of IL-6 (cat. no. 200-06; Wuhan Merck Biotechnology Co.,
Ltd.) in the serum was detected by electrochemiluminescence
analysis.
PD-1 mRNA expression of T cells or
CAR-T cells
The expression of PD-1 mRNA in T cells or CAR-T
cells was detected by reverse transcription-quantitative polymerase
chain reaction (RT-qPCR) analysis. At 24 or 48 h after
treatment/co-culture, total RNA extracted from the cells using
TRIzol® reagent (Invitrogen; Thermo Fisher Scientific,
Inc.) was used as the template for all RT reactions. The cDNA was
synthesized with random priming from 10 µl total RNA with the aid
of the Revert Aid™ First Strand cDNA Synthesis kit (Fermentas;
Thermo Fisher Scientific, Inc.), following the manufacturer's
instructions. RT-qPCR was performed to characterize the mRNA levels
of specific genes using Fast SYBR-Green Master Mix (Applied
Biosystems; Thermo Fisher Scientific, Inc.) in a Biosystems StepOne
Real-Time PCR machine (Applied Biosystem; Thermo Fisher Scientific,
Inc.). Expression level of PD-1, normalized to GAPDH and relative
to a calibrator, was expressed as 2−ΔΔCq (fold
difference). The primers used in for qPCR experiments were as
follows: PD-1, forward 5′AGACGGAGTATGCCACCATT3′ and reverse
5′CACTGTGGGCATTGAGACAT3′; GAPDH, forward 5′-ATTCAACGGCACAGTCAAGG-3′
and reverse 5′-GCAGAAGGGGCGGAGATGA-3′.
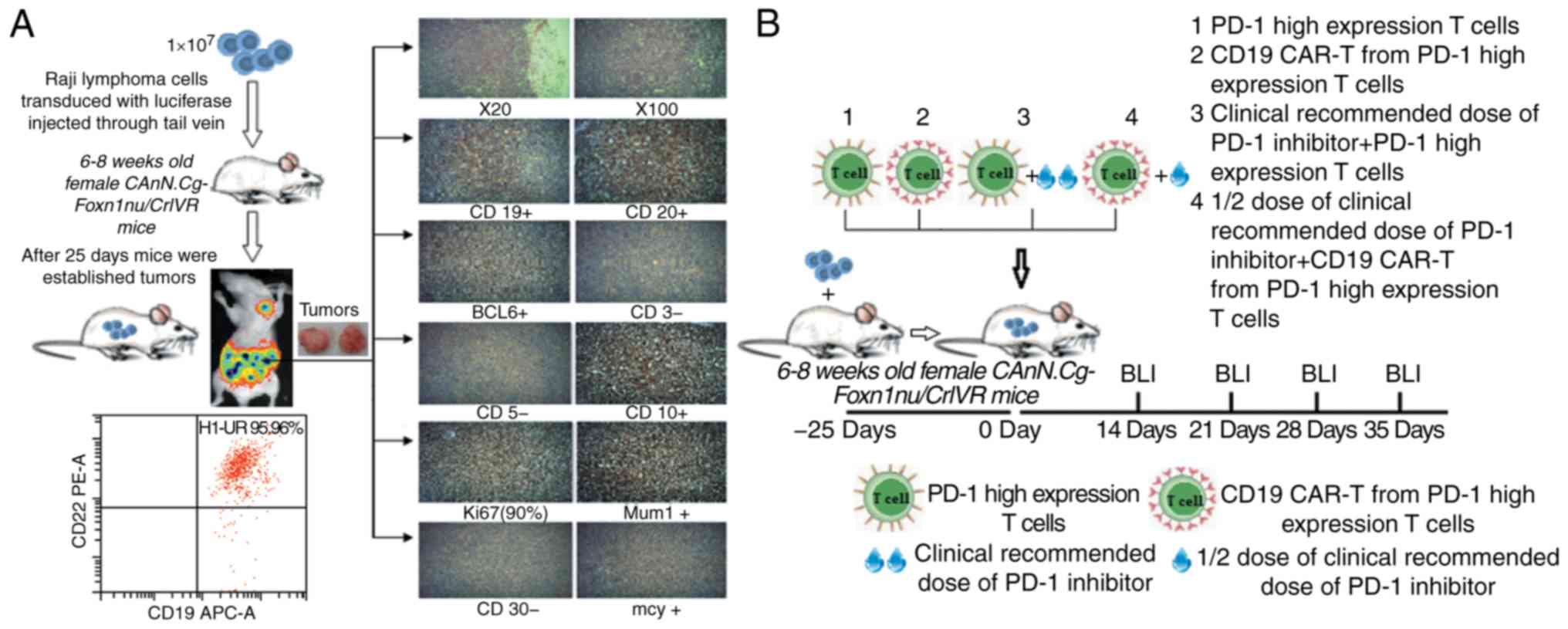
Mouse tumor models
In a lymphoma animal model, 6–8 week old female
CAnN.Cg-Foxn1nu/CrlVR (BALB/c) mice weighing 20±1.8 g (n=24;
Beijing Vitonlihua Experimental Animal Technology Co., Ltd.,
Beijing, China) were housed a rat facility with light and dark
cycle (10 h light and 14 h darkness each day) and access to food
and water. The room temperature was 26–28°C. They were injected
with 1×107 Raji lymphoma cells transduced with
luciferase (purchased from Shanghai Suer Biotechnology Co.) through
the tail vein. Mice were monitored for established tumors with
bioluminescent imaging using a multifunctional in vivo
imaging system. After 25 days, mice were randomized and treated
tail vein injection as follows: PD-1 high expression T cells from
lymphoma patient (5×106); transduced CD19 CAR-T cells
(5×106) from lymphoma patient (high expression PD-1);
PD-1 high expression T cells (5×106) with PD-1 inhibitor
(3 mg/kg) or CD19 CAR-T cells (5×106) from lymphoma
patient (high expression PD-1) with PD-1 inhibitor (1.5 mg/kg). At
14, 21, 28 and 35 days, mice were monitored with bioluminescent
imaging for disease progression following intraperitoneal injection
with luciferin (150 mg/kg). The peripheral blood was taken from the
tail vein of mice to analyze. The proportion of CD19 expression on
lymphoma cells and CD19 CAR-T cells in mice were analyzed by flow
cytometry.
Statistical analysis
SPSS 17.0 (SPSS, Inc., Chicago, IL, USA) statistical
software was used for statistical analysis. Data are expressed as
the mean ± standard error and analyzed by one-way ANOVA, with
Student-Newman-Keuls method used for pairwise comparison. P<0.05
was considered to indicate a statistically significant
difference.
Results
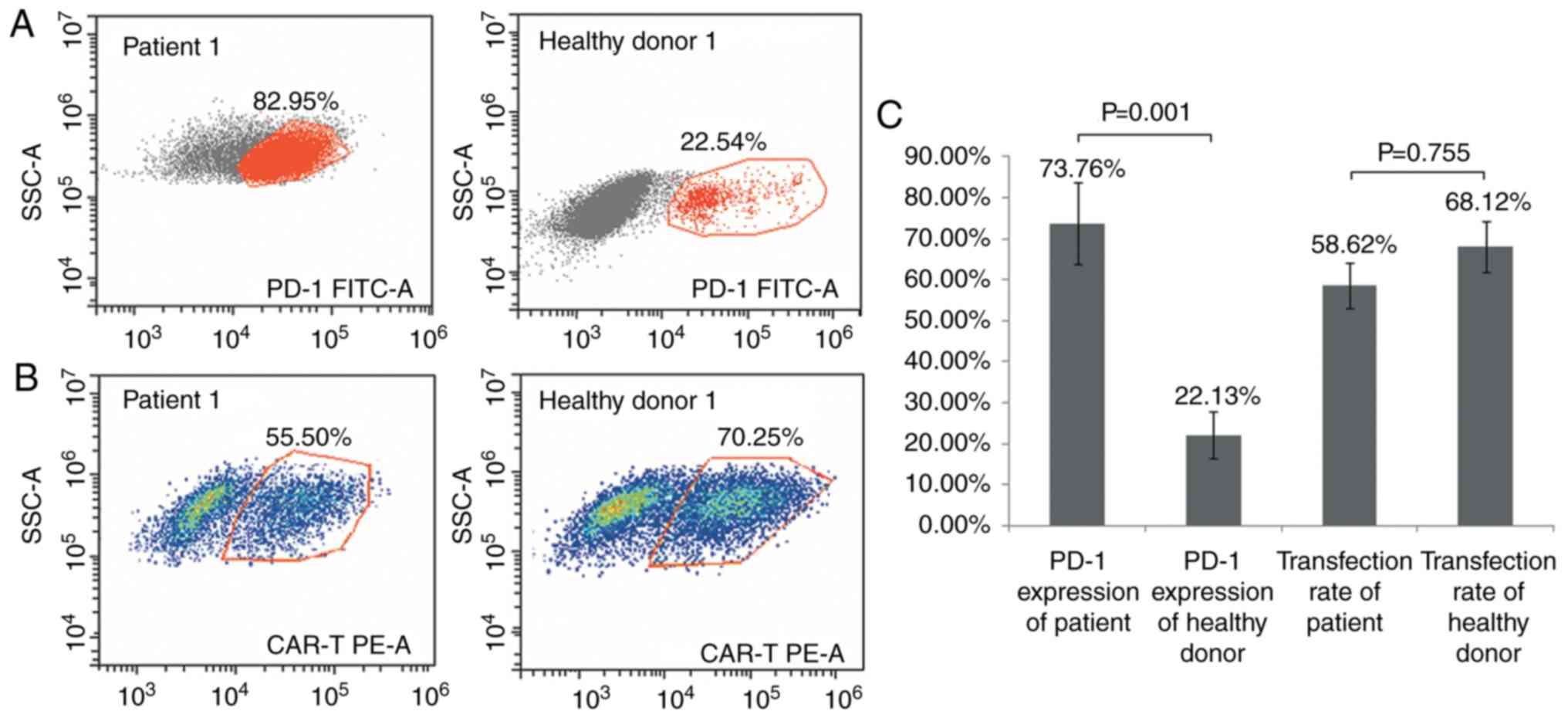
Transduction efficiency of CD19 CAR-T
cells from T cells with high PD-1 expression
The titer of CD19 CAR cell virus was
3×108 TU/ml. The mean expression of PD-1 on T cells from
the seven patients with lymphoma by flow cytometry was 73.76±9.89%
and the highest expression of PD-1 was 82.95% prior to
transduction. The mean transduction efficiency of T cells with high
PD-1 expression in the lymphoma patients was 58.62±5.58%. In
addition, the mean expression of PD-1 on the T cells of the seven
healthy donors was 22.13±5.74%, and the mean CD19 CAR transduction
efficiency was 68.12±6.26% (P=0.001; Fig. 1).
Effect of different doses of PD-1
inhibitor on the cytotoxicity of CD19 CAR-T cells
CD19 CAR-T cells produced from T cells with high
PD-1 expression were combined with72, 36 and 18 µg/ml PD-1
inhibitor and cultured in vitro. In addition, transduced
CD19 CAR-T cells from the healthy donors, CD19 CAR-T cells from T
cells with high PD-1 expression without PD-1 inhibitor, and the T
cells with high PD-1 expression combined with PD-1 inhibitor, were
used as the control groups. An LDH assay was used to determine
cytotoxicity. The cytotoxicity of CD19 CAR-T cells produced from T
cells with high PD-1 expression was lower than PD-1 inhibitor
treated CAR-T cells (high PD-1) and healthy donor CAR-T cells at 24
and 48 h after co-culture with Raji lymphoma cells. At 24 h after
co-culture with Raji lymphoma cells, there was no difference
between the cytotoxicity (LDH activity) of CD19 CAR-T cells from T
cells with high PD-1 expression combined with different doses of
PD-1 inhibitor, and those from the healthy donor CAR-T cells.
However, at 48 h after co-culture, the cytotoxicity of CD19 CAR-T
cells from T cells with high PD-1 expression combined with 18 µg/ml
PD-1 inhibitor was lower than all other groups of combined PD-1
inhibitor treatment and healthy donor CD19 CAR-T cells. The
cytotoxicity of CD19 CAR-T cells from T cells with high PD-1
expression combined with different doses of PD-1 inhibitor was
higher compared with that of T cells with high PD-1 expression
(Fig. 2A).
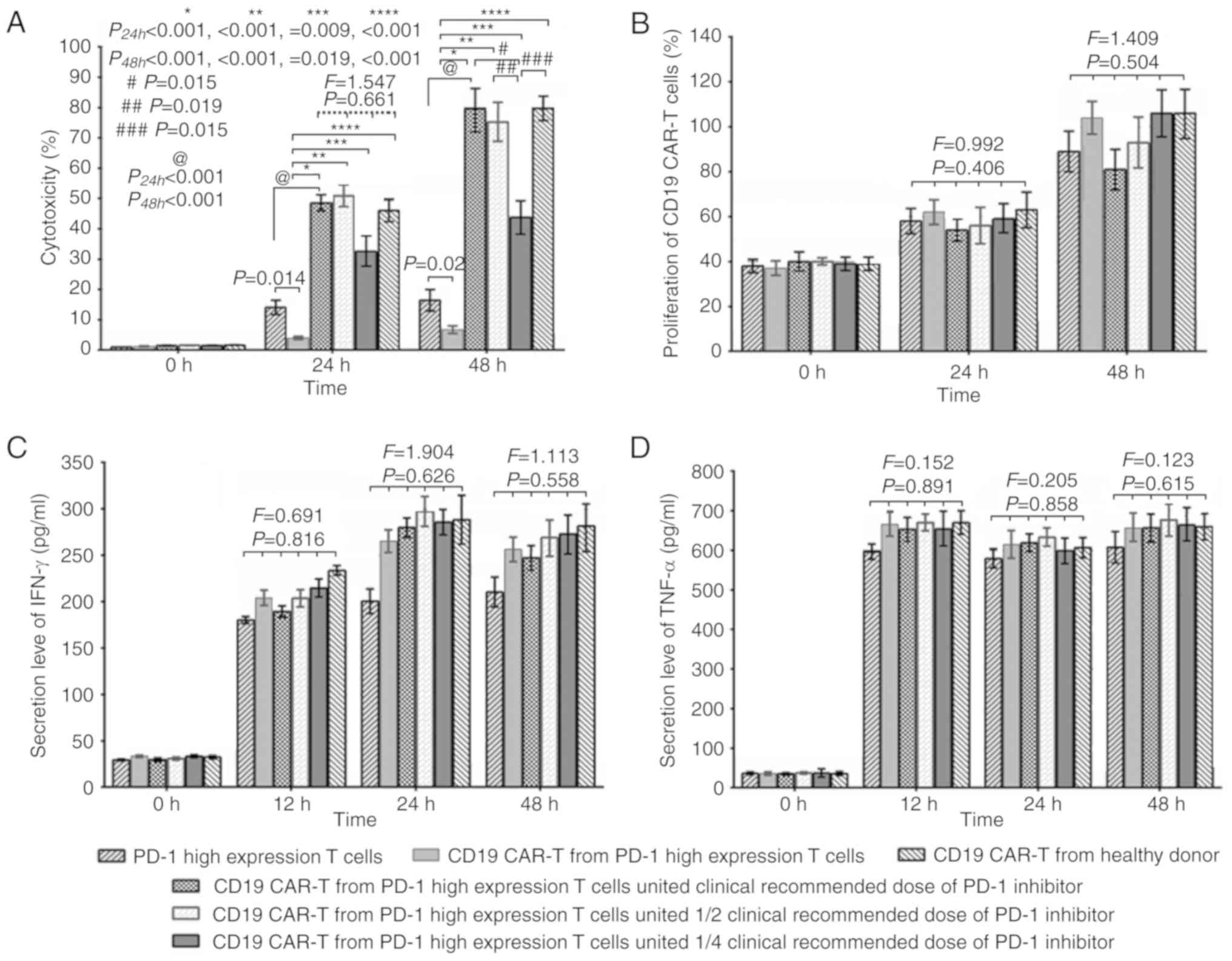 | Figure 2.(A) The cytotoxicity (LDH assay) of T
cells with high PD-1 expression transduced with CD19 CAR was lower
transduced cells from healthy donors and high PD-1 expression
transduced cells treated with PD-1 inhibitor at 24 and 48 h after
co-culture with Raji lymphoma cells (P24 h <0.001,
<0.001, =0.009, <0.001; P48 h <0.001,
<0.001, =0.019, <0.001). At 24 h after co-culture with Raji
lymphoma cells, there were no differences in the cytotoxicity (LDH
assay) of CD19 CAR-T cells from T cells with high PD-1 expression
combined with different doses of PD-1 inhibitor and those from
healthy donors (P=0.661). However, at 48 h after co-culture with
Raji lymphoma cells, the cytotoxicity (LDH assay) of CD19 CAR-T
cells from T cells with high PD-1 expression combined with 18 µg/ml
of PD-1 inhibitor was lower compared with the other high PD-1
combined treatment T cells (PD-1 inhibitor and CD19 CAR
transduction) and the CD19 CAR transduced healthy donor T cell
group (P=0.015, 0.019 and 0.015, respectively). (B-D) There were no
differences in (B) cell viability of CAR-T cells (isolated using
MACS CD3 Microbeads), or the (C) IFN-γ and (D) TNF-α secretion
level among all groups at each time point. CAR, chimeric antigen
receptor; PD-1, programmed death-1; IFN-γ, interferon-γ; TNF-α,
tumor necrosis factor-α. |
Effect of different doses of PD-1
inhibitor on the proliferation of CD19 CAR-T cells
CD19 CAR-T cells from T cells with high PD-1
expression co-cultured with Raji lymphoma cells were treated with
72, 36 and 18 µg/ml PD-1 inhibitor, and cultured in vitro.
CD19 CAR-T cells were isolated from the co-culture by MACS using
CD3 microbeads. There were no differences in the proliferation of
all groups at 24 and 48 h of culture (Fig. 2B).
Effect of different doses of PD-1
inhibitor on inflammatory factor secretion by CD19 CAR-T cells
CD19 CAR-T cells from T cells with high PD-1
expression co-cultured with Raji lymphoma cells were treated with
72, 36 and 18 µg/ml PD-1 inhibitor and cultured in vitro.
There were no differences in the IFN-γ and TNF-α secretion level
among the groups at 12, 24 and 48 h of culture (Fig. 2C and D).
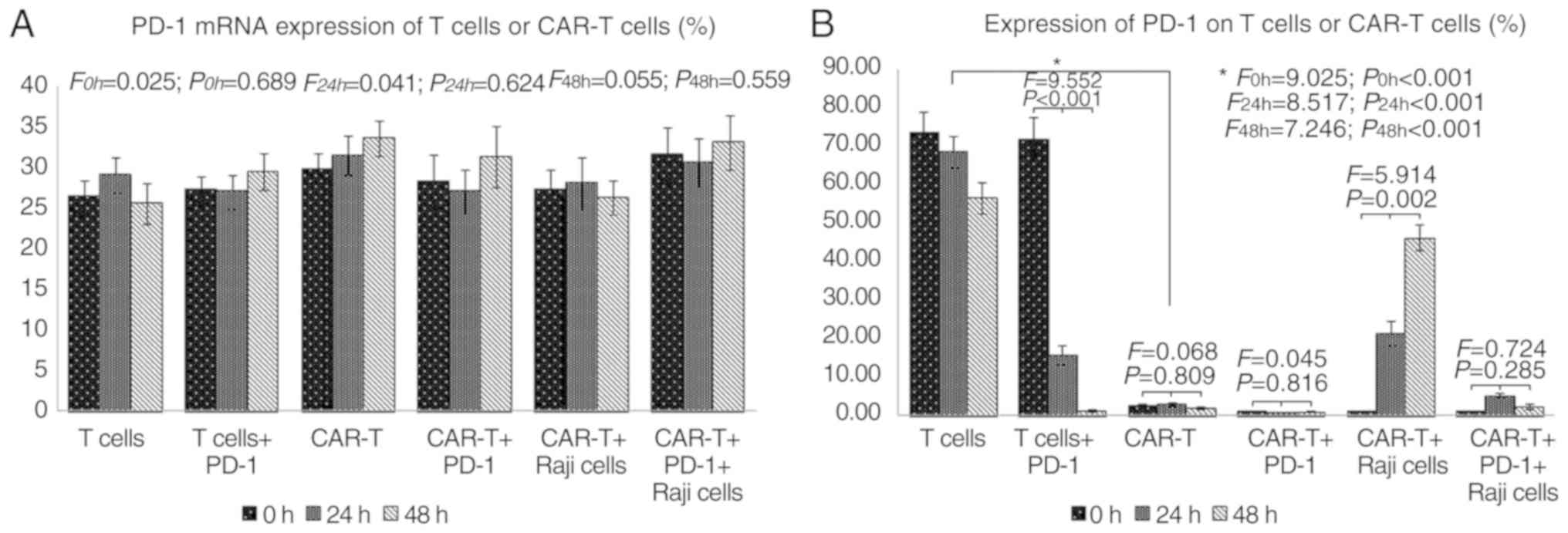
PD-1 expression and PD-1 mRNA
expression of T cells or CAR-T cells
T cells and mature CAR-T cells were used to
investigate the effect of PD-1 inhibitor on the PD-1 mRNA
expression and PD-1 expression of T cells or CAR-T cells. Following
culture in vitro for 48 h, data from T cells with high PD-1
expression with or without PD-1 inhibitor, CD19 CAR-T cells from
patient T cells with high PD-1 expression with or without PD-1
inhibitor, and Raji co-culture of CD19 CAR-T cells from patient T
cells with high PD-1 expression and tumor cells with or without
PD-1 inhibitor. There were no differences in the PD-1 mRNA
expression among different groups and at different time points
(Fig. 3A). The number of CD19 CAR-T
cells expressing PD-1 declined significantly after in vitro
culture, but it increased with the prolonged exposure time to Raji
cancer cells (Fig. 3B).
Effect of CD19 CAR-T cells combined
with different doses of PD-1 inhibitor in mice
After 25 days, tumor establishment in mice was
confirmed following intravenous injection of Raji lymphoma cells
(Fig. 4). Having demonstrated that
PD-1 inhibitor can reverse the low cytotoxicity of CD19 CAR-T cells
from patient T cells highly expressing PD-1 in vitro, the
synergistic effect of CAR-T cells and PD-1 inhibitor was
investigated in vivo. To lower the incidence of side-effects
of the PD-1 inhibitor in mice, a reduced dose of PD-1 inhibitor was
applied in combination with CAR-T cells. The mice were then
randomly allocated to receive patient T cells with high PD-1
expression, CAR-T cells from patient T cells with high PD-1
expression, patient T cells with high PD-1 expression combined
withPD-1 inhibitor, and CAR-T cells from patient T cells with high
PD-1 expression combined with 1/2 the clinical recommended dose of
PD-1 inhibitor (indicated as 1, 2, 3 and 4, respectively, in
Fig. 4).
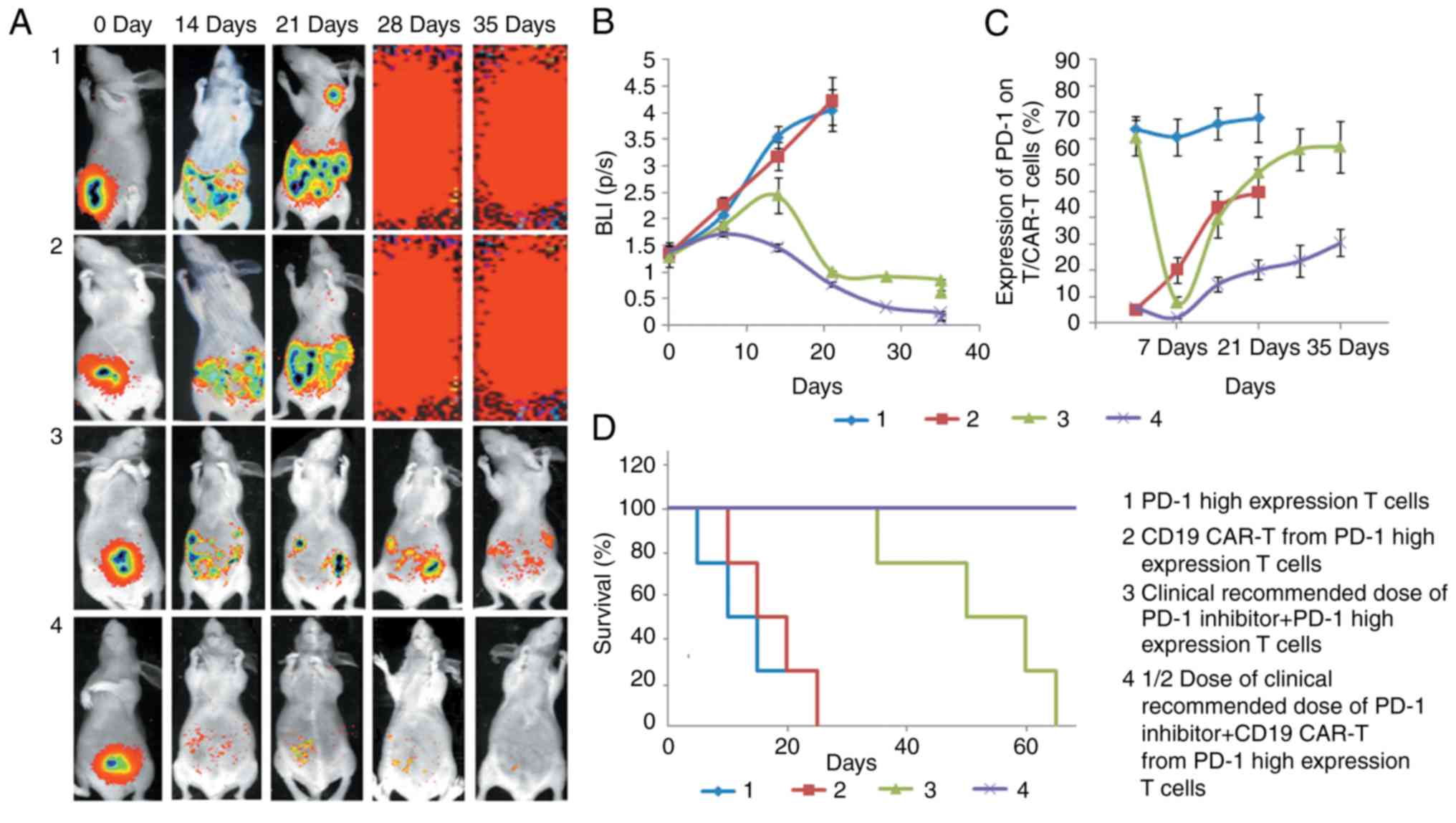
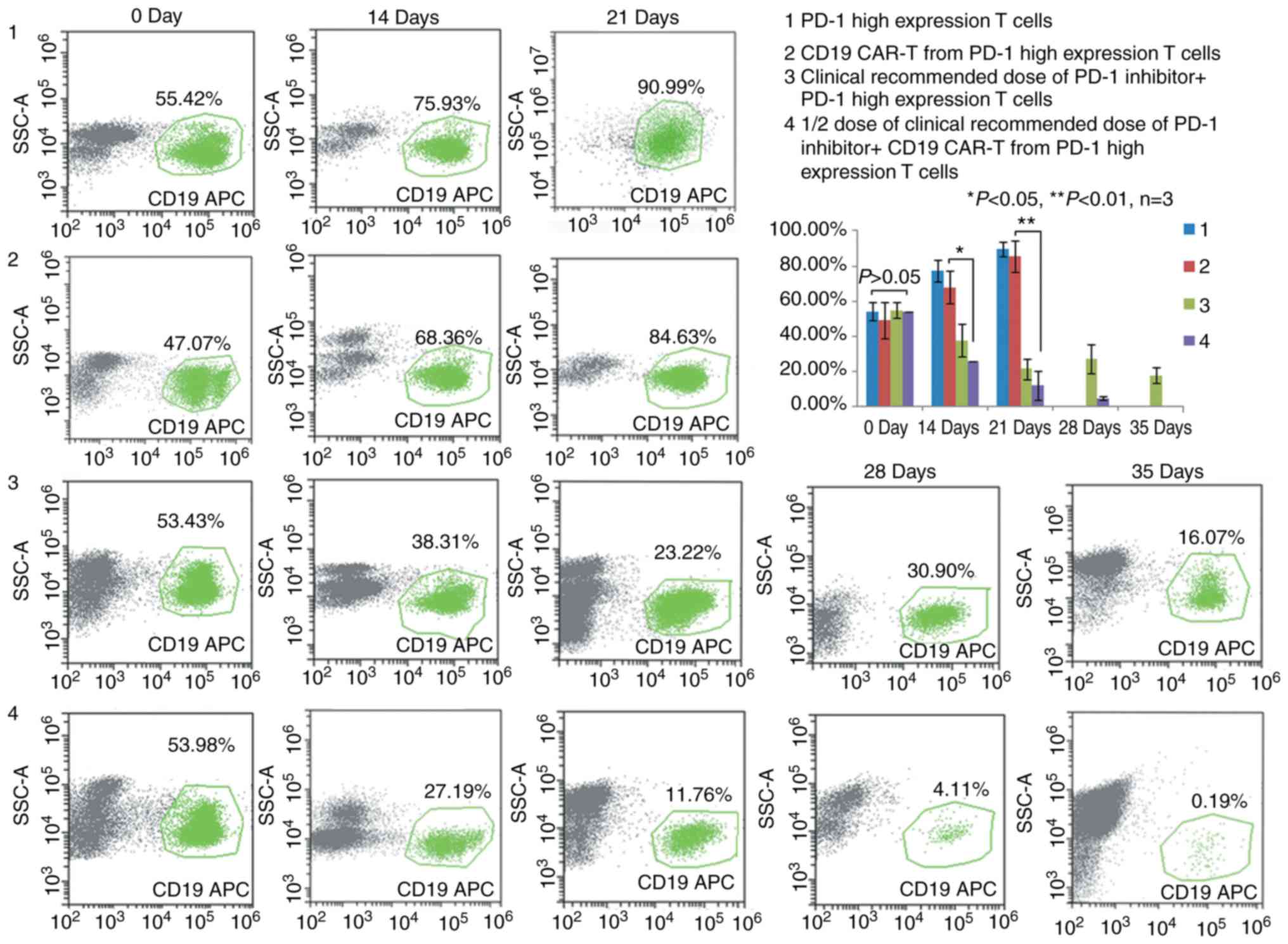
Mice treated with CAR-T cells from patient T cells
with high PD-1 expression combined with 1/2 the clinical
recommended dose of PD-1 inhibitor exhibited the fastest lymphoma
regression and the longest survival (Fig. 5). High tumor load was observed in
the lymphoma cells in the four groups of mice on day 0. Lymphoma
cells were reduced in the PD-1 inhibitor group and the CAR-T cells
combined with PD-1 inhibitor group. At 35 days after the injection
of CD19 CAR-T cells, the number of lymphoma cells in the CAR-T
cells combined with PD-1 inhibitor group was very low (Fig. 6).
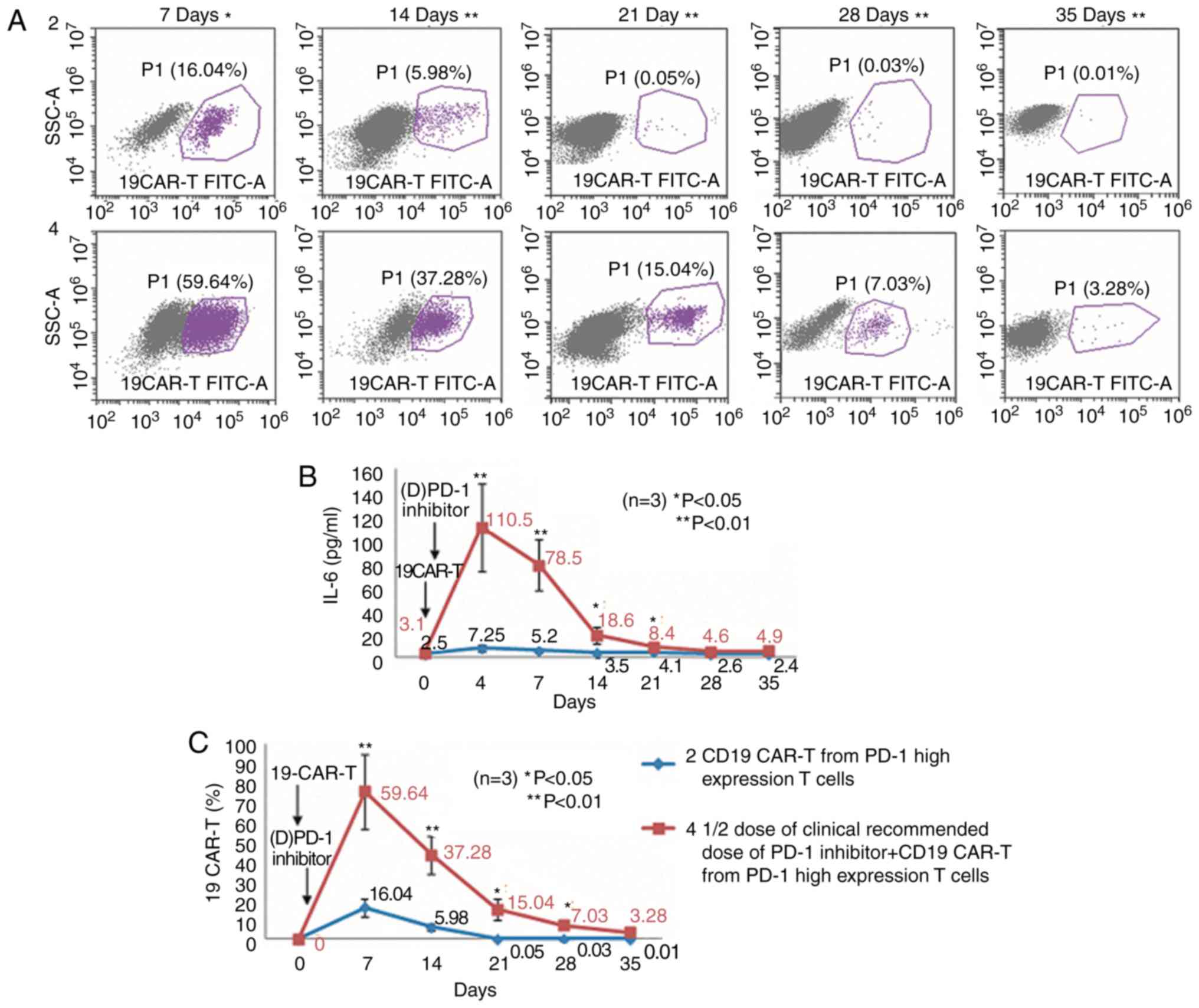
Mice treated with CAR-T cells combined with PD-1
inhibitor exhibited the highest ratio of CAR-T cells 7 days after
injection of CD19 CAR-T cells. PD-1 inhibitor promoted the
proliferation of CAR-T cells in mice. In addition, the IL-6 level
was the highest at 4 days after injection of CD19 CAR-T cells in
the combination therapy group (Fig.
7). However, no such results were observed in the CAR-T cells
without PD-1 inhibitor group. The body weight of mice in group 1
and 2 decreased by 3–6 g before death, but the weight loss of mice
was not significant in group 3 and 4 (data not shown).
Discussion
CAR-T cells can improve remission rates with a
favorable outcome for relapsed/refractory B-cell acute
lymphoblastic leukemia (ALL) (4,5,17,18)
and other B-lineage hematological malignancies (6,19). A
meta-analysis investigated the effect of CD19 CAR-T cells in 119
patients with refractory B-cell malignancies from 14 phase I
clinical trials (20). The overall
response rate to CD19 CAR-T cells was 73%. ALL patients had higher
response rates, but chronic lymphocytic leukemia and B-NHL patients
had comparatively lower response rates. CD19 CAR-T-cell therapy for
B-lineage hematological malignancies is associated with several
problems, including the insufficient activity of CAR-T cells
(21), as repeated antigen exposure
may result in CAR-T cell exhaustion. The resolution of this problem
requires novel strategies to enhance CAR-T cell function and
persistence (22).
The immunosuppressive pathways are promoted by the
combination of tumor cells expressing PD-L1 and T cells expressing
PD-1, preventing T cells from entering the tumor area or inducing
T-cell apoptosis, thereby blocking the effect of immunotherapy
mediated by T cells (4,23,24).
The marked upregulation of PD-1 expression on CAR-T cells results
in a reduction of the anti-tumor immune response and failure of
CAR-T cell therapy (25,26). These results were confirmed by our
experiments in vivo and in vitro. Checkpoint
inhibitors specifically blocking these immunosuppressive pathways
may improve the immune function of T cells. Thus, the
identification of PD-1 expression on T cells and PD-L1 expression
on tumor cells revolutionized cancer immunotherapy (10). The clinical use of these antibodies
is rapidly expanding as an approach to cancer therapy (11,27).
Although the effect of PD-1 inhibitor and PD-L1 inhibitor was
notable in the lymphoma cells, persistence was limited and the
majority of the patients cannot obtain a long-term benefit
(28).
It was hypothesized that the problem of exhausted
immune function of CAR-T cells may be overcome by combination with
a PD-1 inhibitor. Previous studies on combination therapy with
immune checkpoint inhibitors focused on solid tumors (29) and reports on hematological
malignancies demonstrated that PD-1 inhibitors enhanced CAR-T cell
activity (16). A previously
reported refractory DLBCL case achieved a clinically significant
response from a PD-1 inhibitor administered on day 26 after therapy
failure with CD19 CAR-T cells (16). However, if the CAR-T cells are
exhausted, the PD-1 inhibitor will not exert an optimal synergistic
effect. Seeking to improve therapeutic efficacy, we devised the
combination of CD19 CAR-T cells with PD-1 inhibitor
synchronously.
PD-1 inhibitor therapy is associated with several
possibly immune-related adverse events occurring in the nervous,
respiratory, hematological, circulatory and musculoskeletal systems
(30,31). The mechanism underlying PD-1
inhibitor-induced toxicity is unclear. Certain mechanisms of immune
checkpoint inhibitor-derived toxicity have been identified
(32,33), but further studies are required to
elucidate the molecular mechanisms of T cell-mediated side-effects.
Although these T cell-driven drug reactions are rare, they are
potentially fatal.
The side-effects of CAR-T cell therapy, such as
cytokine release syndrome, were also considered. It was
hypothesized that CD19 CAR-T cell therapy in combination with a
PD-1 inhibitor at a reduced dose may lower the risk of side-effects
and improve therapeutic efficacy. In the present study, patient T
cells with high PD-1 expression and CD19 CAR-T cells derived from T
cells with high PD-1 expression exerted almost no effect on
lymphoma cells. This phenomenon was replicated in the lymphoma
animal model. Therefore, CD19 CAR-T cells from patients with high
PD-1 expression were treated with different doses of PD-1 inhibitor
[clinically recommended dose (72 µg/ml), and one-half (36 µg/ml)
and one-quarter (18 µg/ml) of the clinical recommended dose) in
order to improve the activity of the devitalized CD19 CAR-T cells.
The analysis in vitro demonstrated, as expected, that 1/2
the clinical recommended dose of PD-1 inhibitor was able to
increase the anti-tumor activity of CD19 CAR-T cells from patients
with high PD-1 expression to the level of healthy donor CD19 CAR-T
cells; however, the lower dose (1/4 clinical recommended dose) did
not improve the activity of CD19 CAR-T cells.
The results were then verified in a lymphoma animal
model, in which the combination of CD19 CAR-T cells from patients
with high PD-1 expression and 1/2 the clinical recommended dose of
PD-1 inhibitor exerted satisfactory effects. The mice that received
combination therapy with inhibitor had a longer survival (>35
days) compared with the CD19 CAR-T cells from patients with high
PD-1 expression group. Of note, in the combination group, there was
a peak of the IL-6 level and CD19 CAR-T cell proportion following
injection of the PD-1 inhibitor. However, this phenomenon was not
observed in the CD19 CAR-T cells from patients with high PD-1
expression group. We intend to further investigate the side-effects
of this combined therapy in mice in future studies, including the
body weight changes, blood cell counts, transaminase levels and LDH
levels of mice. Moreover, histopathological changes of mice after
this combined therapy would also bee assessed.
The present study also investigated whether the PD-1
inhibitor affected the PD-1 mRNA expression in T cells or CAR-T
cells. No difference in the PD-1 mRNA expression was observed among
different T-cell or CAR-T-cell groups at different time points.
However, the number of CAR-T cells expressing PD-1 was markedly
reduced after in vitro culture. This may be associated with
cell proliferation in in vitro culture. However, at low
effector-target ratio, the PD-1 expression in CAR-T cells returned
to high levels with gradual prolongation of the co-culture time. In
the present study, the CD19 CAR-T cells from patients with high
PD-1 expression combined with 1/2 the clinical recommended dose of
PD-1 inhibitor prevented the increase in the expression of PD-1 in
CAR-T cells when they were exposed to tumor cells. These results
may contribute to the application of CD19 CAR-T cells for the
treatment of relapsed or refractory B-cell lymphoma.
Acknowledgements
Not applicable.
Funding
This study was supported by the Hospital Funding
Project (grant nos. CM201805).
Availability of data and materials
The datasets and certain material used and/or
analyzed during the present study are available from the
corresponding author on reasonable request.
Authors' contributions
Concept and design, QD; performed the experiments,
RZ; acquisition of data, YYJ and HBZ; analysis and interpretation
of data, JW and MFZ; writing, review and/or revision of manuscript,
RZ. All authors read and approved the manuscript and agree to be
accountable for all aspects of the research in ensuring that the
accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent to
participate
Ethical approval and informed consent were obtained.
Patients with lymphoma and healthy donors agreed to participate
this experiment as part of a clinical trial at the Department of
Hematology at Tianjin First Central (Tianjin, China) hospital with
autologous CAR-T 19 cells (ChiCTR-ONN-16009862). All animal
procedures were approved by the institutional animal and care use
committee of Tianjin First Central Hospital (Tianjin, China).
Patient consent for publication
All patients agreed to publication of this
paper.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Sadelain M, Brentjens R and Rivière I: The
basic principles of chimeric antigen receptor design. Cancer
Discov. 3:388–398. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brentjens RJ, Davila ML, Riviere I, Park
J, Wang X, Cowell LG, Bartido S, Stefanski J, Taylor C, Olszewska
M, et al: CD19-targeted T cells rapidly induce molecular remissions
in adults with chemotherapy-refractory acute lymphoblastic
leukemia. Sci Transl Med. 5:177ra1382013. View Article : Google Scholar
|
|
3
|
Grupp SA, Kalos M, Barrett D, Aplenc R,
Porter DL, Rheingold SR, Teachey DT, Chew A, Hauck B, Wright JF, et
al: Chimeric antigen receptor-modified T cells for acute lymphoid
leukemia. N Engl J Med. 368:1509–1518. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Davila ML, Riviere I, Wang X, Bartido S,
Park J, Curran K, Chung SS, Stefanski J, Borquez-Ojeda O, Olszewska
M, et al: Efficacy and toxicity management of 19-28z CAR T cell
therapy in B cell acute lymphoblastic leukemia. Sci Transl Med.
6:224ra1252014. View Article : Google Scholar
|
|
5
|
Kochenderfer JN, Dudley ME, Carpenter RO,
Kassim SH, Rose JJ, Telford WG, Hakim FT, Halverson DC, Fowler DH,
Hardy NM, et al: Donor-derived CD19-targeted T cells cause
regression of malignancy persisting after allogeneic hematopoietic
stem cell transplantation. Blood. 122:4129–4139. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Kochenderfer JN, Dudley ME, Kassim SH,
Somerville RP, Carpenter RO, Stetler-Stevenson M, Yang JC, Phan GQ,
Hughes MS, Sherry RM, et al: Chemotherapy-refractory diffuse large
B-cell lymphoma and indolent B-cell malignancies can be effectively
treated with autologous T cells expressing an anti-CD19 chimeric
antigen receptor. J Clin Oncol. 33:540–549. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Jolley B and Walker S: Chimeric antigen
receptor T-cell therapy for lymphomas. Hosp Pharm. 52:469–470.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Barrett DM, Singh N, Porter DL, Grupp SA
and June CH: Chimeric antigen receptor therapy for cancer. Annu Rev
Med. 65:333–347. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Bonifant CL, Jackson HJ, Brentjens RJ and
Curran KJ: Toxicity and management in CAR T-cell therapy. Mol Ther
Oncolytics. 3:160112016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Dong H, Strome SE, Salomao DR, Tamura H,
Hirano F, Flies DB, Roche PC, Lu J, Zhu G, Tamada K, et al:
Tumor-associated B7-H1 promotes T-cell apoptosis: A potential
mechanism of immune evasion. Nat Med. 8:793–800. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu K, Tan S, Chai Y, Chen D, Song H,
Zhang CW, Shi Y, Liu J, Tan W, Lyu J, et al: Structural basis of
anti-PD-L1 monoclonal antibody avelumab for tumor therapy. Cell
Res. 27:151–153. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Topalian SL, Hodi FS, Brahmer JR,
Gettinger SN, Smith DC, McDermott DF, Powderly JD, Carvajal RD,
Sosman JA, Atkins MB, et al: Safety, activity, and immune
correlates of anti-PD-1 antibody in cancer. N Engl J Med.
366:2443–2454. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hamid O, Robert C, Daud A, Hodi FS, Hwu
WJ, Kefford R, Wolchok JD, Hersey P, Joseph RW, Weber JS, et al:
Safety and tumor responses with lambrolizumab (anti-PD-1) in
melanoma. N Engl J Med. 369:134–144. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Wolchok JD, Kluger H, Callahan MK, Postow
MA, Rizvi NA, Lesokhin AM, Segal NH, Ariyan CE, Gordon RA, Reed K,
et al: Nivolumab plus ipilimumab in advanced melanoma. N Engl J
Med. 369:122–133. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Topalian SL, Sznol M, McDermott DF, Kluger
HM, Carvajal RD, Sharfman WH, Brahmer JR, Lawrence DP, Atkins MB,
Powderly JD, et al: Survival, durable tumor remission, and
long-term safety in patients with advanced melanoma receiving
nivolumab. J Clin Oncol. 32:1020–1030. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Chong EA, Melenhorst JJ, Lacey SF, Ambrose
DE, Gonzalez V, Levine BL, June CH and Schuster SJ: PD-1 blockade
modulates chimeric antigen receptor (CAR)-modified T cells:
Refueling the CAR. Blood. 129:1039–1041. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Maude SL, Frey N, Shaw PA, Aplenc R,
Barrett DM, Bunin NJ, Chew A, Gonzalez VE, Zheng Z, Lacey SF, et
al: Chimeric antigen receptor T cells for sustained remissions in
leukemia. N Engl J Med. 371:1507–1517. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Lee DW, Kochenderfer JN, Stetler-Stevenson
M, Cui YK, Delbrook C, Feldman SA, Fry TJ, Orentas R, Sabatino M,
Shah NN, et al: T cells expressing CD19 chimeric antigen receptors
for acute lymphoblastic leukaemia in children and young adults: A
phase 1 dose-escalation trial. Lancet. 385:517–528. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Batlevi CL, Matsuki E, Brentjens RJ and
Younes A: Novel immunotherapies in lymphoid malignancies. Nat Rev
Clin Oncol. 13:25–40. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Zhang T, Cao L, Xie J, Shi N, Zhang Z, Luo
Z, Yue D, Zhang Z, Wang L, Han W, et al: Chimeric antigen
receptor-modified T cells for treatment of B cell malignancies in
phase I clinical trials: A meta-analysis. Oncotarget.
6:33961–33971. 2015.PubMed/NCBI
|
|
21
|
Makita S, Yoshimura K and Tobinai K:
Clinical development of anti-CD19 chimeric antigen receptor T-cell
therapy for B-cell non-Hodgkin lymphoma. Cancer Sci. 108:1109–1118.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Chen N, Morello A, Tano Z and Adusumilli
PS: CAR T-cell intrinsic PD-1 checkpoint blockade: A two-in-one
approach for solid tumor immunotherapy. Oncoimmunology.
6:e12733022016. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Pardoll DM: The blockade of immune
checkpoints in cancer immunotherapy. Nat Rev Cancer. 12:252–264.
2012. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Jaspers JE and Brentjens RJ: Development
of CAR T cells designed to improve antitumor efficacy and safety.
Pharmacol Ther. 178:83–91. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Gargett T, Yu W, Dotti G, Yvon ES, Christo
SN, Hayball JD, Lewis ID, Brenner MK and Brown MP: GD2-specific CAR
T cells undergo potent activation and deletion following antigen
encounter but can be protected from activation-induced cell death
by PD-1 blockade. Mol Ther. 24:1135–1149. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Li S, Siriwon N, Zhang X, Yang S, Jin T,
He F, Kim YJ, Mac J, Lu Z, Wang S, et al: Enhanced cancer
immunotherapy by chimeric antigen receptor-modified T cells
engineered to secrete checkpoint inhibitors. Clin Cancer Res.
23:6982–6992. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Topalian SL, Drake CG and Pardoll DM:
Immune checkpoint blockade: A common denominator approach to cancer
therapy. Cancer Cell. 27:450–461. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Huang AC, Postow MA, Orlowski RJ, Mick R,
Bengsch B, Manne S, Xu W, Harmon S, Giles JR, Wenz B, et al: T-cell
invigoration to tumour burden ratio associated with anti-PD-1
response. Nature. 545:60–65. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
John LB, Kershaw MH and Darcy PK: Blockade
of PD-1 immunosuppression boosts CAR T-cell therapy.
Oncoimmunology. 2:e262862013. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Läubli H, Balmelli C, Bossard M, Pfister
O, Glatz K and Zippelius A: Acute heart failure due to autoimmune
myocarditis under pembrolizumab treatment for metastatic melanoma.
J Immunother Cancer. 3:112015. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Koelzer VH, Rothschild SI, Zihler D, Wicki
A, Willi B, Willi N, Voegeli M, Cathomas G, Zippelius A and Mertz
KD: Systemic inflammation in a melanoma patient treated with immune
checkpoint inhibitors-an autopsy study. J Immunother Cancer.
4:132016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Dubin K, Callahan MK, Ren B, Khanin R,
Viale A, Ling L, No D, Gobourne A, Littmann E, Huttenhower C, et
al: Intestinal microbiome analyses identify melanoma patients at
risk for checkpoint-blockade-induced colitis. Nat Commun.
7:103912016. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Iwama S, De Remigis A, Callahan MK, Slovin
SF, Wolchok JD and Caturegli P: Pituitary expression of CTLA-4
mediates hypophysitis secondary to administration of CTLA-4
blocking antibody. Sci Transl Med. 6:230ra2452014. View Article : Google Scholar
|