Introduction
Based on recent global cancer statistics, 295,414
patients were newly diagnosed with epithelial ovarian carcinoma
(EOC) and 184,799 patients died of this tumor worldwide in 2018
(1). Thus, EOC is a leading cause of
mortality in women among all gynecologic cancers (2). Since EOC commonly remains asymptomatic,
in clinical practice it is known as a ‘silent killer’, and the
majority of patients present with widespread peritoneal metastases
at initial diagnosis. The oncologic outcome of EOC patients is
likely to be associated with the extent of peritoneal dissemination
(3–5).
Although complete clinical remission is achieved in about 80% of
patients who undergo aggressive surgery and systematic
chemotherapy, most of these clinical responders show recurrence
(6). Consequently, the oncologic
outcome of recurrent patients remains extremely poor (7,8).
Connective tissue growth factor (CTGF/CCN2) belongs
to a member of the CCN family (9).
CTGF has been reported to be involved in various aggressive tumor
properties, such as cell growth, migration, angiogenesis and
metastasis (10–13). Furthermore, according to prior
studies, CTGF expression is closely related to the acquisition of
chemoresistance to antineoplastic agents, including paclitaxel in
breast cancer (14), 5-FU in
colorectal cancer (15) and cisplatin
in osteosarcoma (16). Regarding EOC,
Wang et al revealed that the expression level of CTGF is
negatively correlated with the expression of miR-143 in tissue
samples, and that miR-143 exerts tumor-suppressing functions,
including, migration, invasion and cell proliferation by targeting
CTGF in vitro (17). However,
to the best of our knowledge, studies concerning the expression and
biological behavior of CTGF in relapsed EOC are limited.
We hypothesized that CTGF plays a central role in
both the chemoresistance and metastatic ability of EOC, and that
CTGF positivity may be a valuable predictor of a poor clinical
outcome in EOC patients. Here, we investigated the prognostic
impact of CTGF expression, and analyzed the functions of CTGF in
EOC cell progression.
Materials and methods
Cell culture
The EOC cell lines, ES-2, SKOV3, A2780, and OVCAR3,
were maintained in RPMI-1640 medium with 10% FBS and
penicillin/streptomycin. These cell lines were obtained from the
American Type Culture Collection (ATCC; Manassas, VA, USA) in
2012–2013. NOS2 and NOS3 cells, derived from serous EOC, were
established in our institute (18,19). These
cell lines were maintained in RPMI-1640 (Sigma-Aldrich; Merck KGaA)
supplemented with 10% fetal bovine serum (FBS) and
penicillin-streptomycin at 37°C in a humidified atmosphere of 5%
CO2. The NOS2TR and NOS3TR cells, established from
parental NOS2 and NOS3 cells, acquired chronic resistance to
paclitaxel (PTX) as previously described (20–22).
Inhibition of CTGF by small
interfering RNA (siRNA)
To generate CTGF-silenced cells, EOC cells were
transfected with either a pool of small interfering RNA (siRNA)
oligonucleotide-specific to human CTGF (final concentration, 30
pmol/l; assay ID s3709, cat. no. 4427038; Thermo Fisher Scientific,
Inc.) or control siRNA (Sigma-Aldrich; Merck KGaA) using
Invitrogen™ Lipofectamine™ RNAiMAX Transfection Regent (Thermo
Fisher Scientific, Inc.). The sequences for CTGF siRNA were as
follows: Sense, 5′-CCUAUCAAGUUUGAGCUUUTT-3′ and antisense,
5′-AAAGCUCAAACUUGAUAGGCT-3′. After overnight incubation at 37°C,
the culture medium was replaced with fresh complete medium
containing 10% FBS. Cells were harvested after 72 h and solubilized
for western blot analysis of CTGF silencing.
PTX chemosensitivity assay
The PTX chemosensitivity assay was performed as
described previously (23). Briefly,
cells were seeded in triplicate in 96-well plates at a density of
5,000 cells in a volume of 200 µl of culture media containing 10%
FBS. After incubation for 24 h at 37°C, the medium was replaced
with fresh medium with or without various concentrations of PTX
(Bristol Myers Squib, Tokyo, Japan). After an additional 72 h, cell
viability was assayed using the Cell Titer 96 Aqueous One Solution
Cell Proliferation Assay kit (Promega Corp., Tokyo, Japan).
In vitro migration assay
Cell migration was assayed in 24-well Transwell cell
culture chambers (Costar, Corning Inc., Corning, NY, USA). Cells
were suspended in the upper chamber at a final concentration of
1.0×106/ml in 200 µl of RPMI-1640 medium. In addition,
we examined the effect of siRNA transfection on the migration of
parental and PTX-resistant EOC cells. Cells transfected with siRNAs
were seeded in the upper chamber and allowed to migrate to the
fibronectin-coated lower surface for 20 h. The number of cells that
had migrated to the lower surface was counted to evaluate the
migration ability. Cells were seeded in 6-cm dishes in RPMI-1640
containing 10% FBS. After reaching 50% confluency, the medium was
replaced by fresh RPMI-1640 containing 10% FCS, and transfection
with siRNA (si-Ctrl and si-CTGF) was performed using Lipofectamine
RNAiMAX Transfection Regent. Forty-eight hours after transfection,
the cells were trypsinized and pelleted. Subsequently, the cells
were re-plated in the upper chambers of Transwell plates at a
density of 1.0×106/ml in 200 µl of RPMI-1640. The lower
chamber contained 700 µl of RPMI-1640 supplemented with 10% FBS.
The subsequent procedure was the same as described above. We
performed four individual experiments, and each assay was performed
in triplicate.
Western blot analysis
The western blot experimental procedure was
described previously (24). The
following primary antibodies were used: Anti-E-cadherin (cat. no.
3195, at a 1:1,000 dilution; Cell Signaling Technology),
anti-fibronectin (cat. no. sc-18825, at a 1:1,000 dilution; Santa
Cruz Biotechnology, Inc.), anti-vimentin (cat. no. 5741, at a
1:1,000 dilution; Cell Signaling Technology), and anti-CTGF (cat.
no. sc-365970, at a 1:1,000 dilution; Santa Cruz Biotechnology,
Inc.). The primary antibodies were washed in 0.05% Tween-20/PBS and
then incubated with horseradish peroxidase-conjugated secondary
antibody. Proteins were visualized using Amersham ELC Western
Blotting Detection Reagent (GE Healthcare Life Sciences). Bands
were visualized using ImageQuant LAS 4000 mini (GE Healthcare Life
Sciences).
RNA extraction and quantitative
real-time PCR
The procedure was previously described (25,26). Total
RNA was isolated using RNeasy Mini (Qiagen, Hilden, Germany). The
concentration of RNA was measured according to absorbance at 260
nm, and 0.5 mg of total RNA was reverse-transcribed using M-MLV
reverse transcriptase and a random primer using ReverTra Ace qPCR
RT Master Mix (Toyobo, Osaka, Japan) at 42°C for 60 min. Then, 1 µl
of the final cDNA solution was subjected to PCR using KOD DNA
polymerase (Toyobo). Amplification conditions were as follows:
Denaturation at 98°C for 2 min; 40 cycles at 98°C for 10 sec, 55°C
for 10 sec, and 68°C for 30 sec using LightCycler Nano (Roche
Diagnostics, Basel, Switzerland). GAPDH was used as an endogenous
control, relative expression was estimated using the comparative Cq
(2−ΔΔCq) method. The sequences of primers used for the
experiments were as follows: CTGF forward, 5′-TTCCAGAGCAGCTGCAAGTA
and reverse, 5′-GCCAAACGTGTCTTCCAGTC.
Cytokine stimulation
EOC cell lines were stimulated with recombinant
human TGF-β1 (10 ng/ml) (PeproTech, Inc., Rocky Hill, NJ, USA),
hepatocyte growth factor (HGF) (40 ng/ml) (PeproTech, Inc.) and
tumor necrosis factor α (TNF-α) (100 ng/ml) (R&D System,
Minneapolis, MN, USA) in RPMI-1640 medium supplemented with 10% FBS
for each incubation time.
Patients and immunohistochemical
staining
A total of 104 human EOC tissues were obtained from
patients who underwent surgical treatment at Nagoya University
Hospital between January 1994 and December 2010 after providing
informed consent. In regards to the histological types, we adopted
the World Health Organization (WHO) classification criteria
(27). The clinical stage was
assigned according to the International Federation of Gynecology
and Obstetrics (FIGO) staging system (28,29). This
study was approved by the Ethics Committee of Nagoya University
(Approval No. 2011-1234-2).
Formalin-fixed, paraffin-embedded tissue sections
were cut at a thickness of 4 µm. For heat-induced epitope
retrieval, deparaffinized sections in 0.01 M citrate buffer were
heated three times at 90°C for 5 min using a microwave oven.
Sections were incubated at 4°C for 12 h with primary antibody
(anti-goat-CTGF polyclonal, sc-14939, at a 1:100 dilution; Santa
Cruz Biotechnology, Inc.). The sections were rinsed and incubated
for 30 min with biotinylated anti-goat IgG antibody (Histofine
SAB-PO (goat) kit, cat. no. 414012; Nichirei Corp., Tokyo, Japan).
The immunoreactive staining was processed using the
peroxidase-anti-peroxidase method according to the manufacturer's
instructions (Dako, Hamburg, Germany). To detect the reaction,
3,3′-diaminobenzidine tetrachloride (DAB) chromogen solution was
used. After rinsing in water for 30 min, the sections were
counterstained with hematoxylin and then dehydrated. Finally, they
were mounted in mounting medium for examination.
Evaluation of immunohistochemical
staining
For evaluation of the results of immunohistochemical
staining, 10 fields for each specimen were selected and evaluated
with both low- (×100) and high- (×400) power microscopy (Axio
Imager A1, Carl Zeiss). Two investigators assessed the slides
without knowledge of the clinicopathologic features and were
blinded to each other's evaluation. The two investigators were in
agreement on all the slides examined. Based on the immunostaining
activity, a semiquantitative score was assigned according to the
intensity and area of the stained cells, as described previously
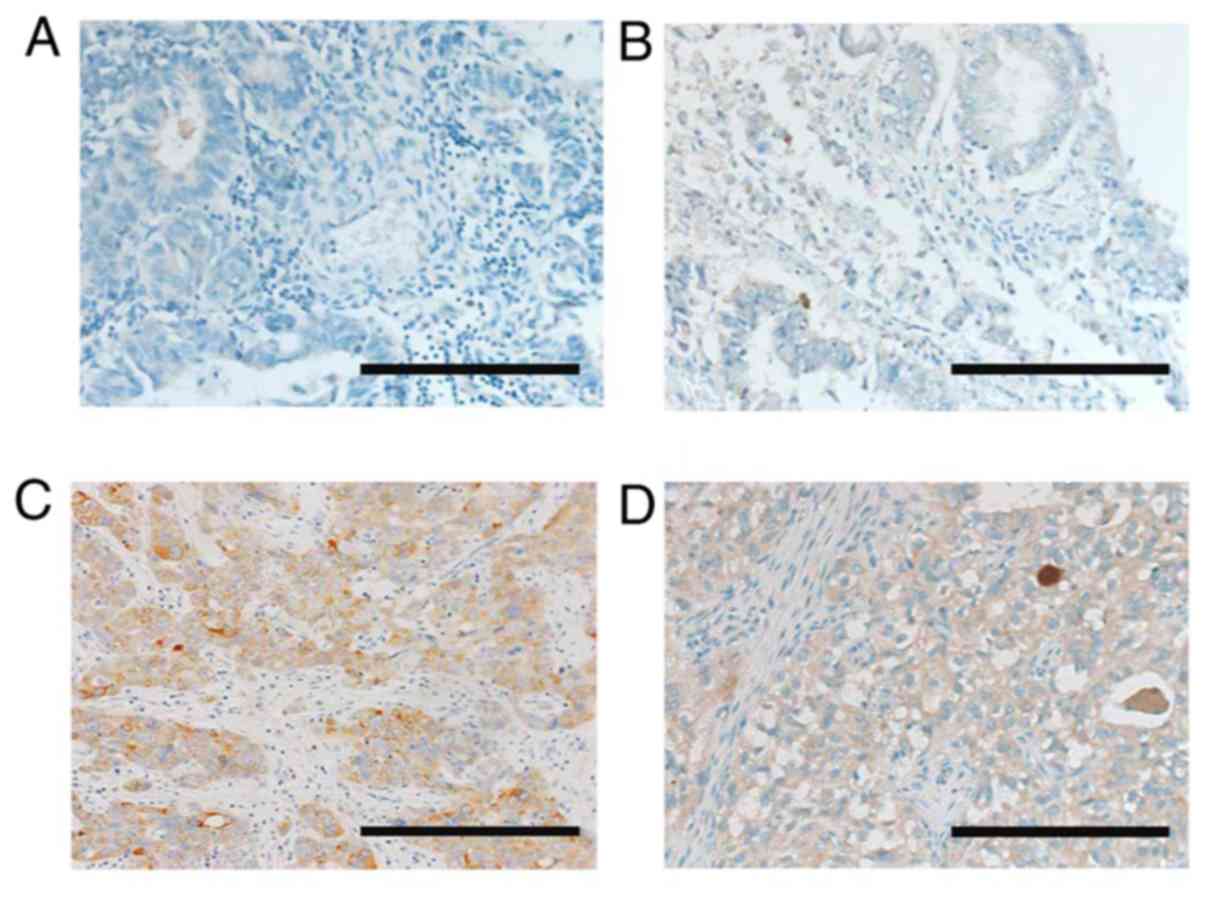
(30). For the evaluation of CTGF
expression, the staining intensity was scored as 0 (negative-weak),
1 (medium), 2 (strong), or 3 (very strong). The percentage of the
staining area was scored as 0 (0–10%), 1 (11–50%), and 2 (51–100%)
relative to the total tumor area. The sum of the staining intensity
and area scores was calculated as the final score (0–5) for CTGF.
Tumors with final scores of 0–1 and 2–5 were classified as showing
low and high expression, respectively.
Survival analyses
The distributions of the clinicopathologic factors
were assessed using the Chi-square test. The progression-free
survival (PFS) was defined as the time interval between the date of
surgery and date of the last follow-up or recurrence/progression.
The overall survival (OS) was defined as the time interval between
the date of surgery and date of the last follow-up or death from
any cause. The survival curves were compared employing the Log-rank
test. Survival analysis was conducted using the Kaplan-Meier
method. The prognostic significance of CTGF expression concerning
other clinicopathologic variables was assessed using univariable
and multivariable Cox's proportional hazard's analyses. All
statistical analyses were performed with JMP Pro version 10.0 (SAS
Institute, Japan). A P-value of <0.05 was considered indicative
of statistical significance.
Statistical analysis
All data are expressed as the mean ± SD. Data were
calculated from at least three independent experiments. The
significance of differences was analyzed by Student's t-test
or one-way analysis of variance (ANOVA) followed by Tukey's
post-hoc test. A P-value of <0.05 was considered indicative of
statistical significance.
Results
Patient characteristics
We initially examined CTGF expression and its
possible association with the prognostic outcome of EOC patients
employing an immunohistochemical experiment. Patient
characteristics are presented in Table
I. The median age was 54, ranging from 24–78 years. The
distributions of the FIGO stages were: 42.3% (44/104) stage I,
19.2% (20/104) stage II, 34.6% (36/104) stage III and 3.8% (4/104)
stage IV. Among all patients, pathological types were as follows:
34 (32.7%) with serous, 42 (40.4%) with clear-cell, 18 (17.3%) with
endometrioid, and 8 (7.7%) with mucinous carcinoma. One hundred and
one (97.1%) patients underwent postoperative chemotherapy. Three
patients did not receive postoperative chemotherapy due to their
severe complications or strong wishes. Among the 104 patients,
lower- and higher-level CTGF staining expressions were noted in 65
(62.5%) and 39 (37.5%) patients, respectively. Representative
images of various immunohistochemical intensities are presented in
Fig. 1. The distributions of the age,
stage, histological type, chemotherapy, and period of initial
treatment did not differ between the two groups Table I.
 | Table I.Association between the expression of
CTGF and clinicopathologic parameters of the EOC cases. |
Table I.
Association between the expression of
CTGF and clinicopathologic parameters of the EOC cases.
|
| CTGF
expression |
|
|---|
|
|
|
|
|---|
|
| Total | Low | High |
|
|---|
|
|
|
|
|
|
|---|
|
Characteristics | N | N | % | N | % | P-value |
|---|
| Total | 104 | 65 | 62.5 | 39 | 37.5 |
|
| Age (years) |
|
|
|
|
| 0.4617 |
|
≤50 | 38 | 22 | 33.8 | 16 | 41.0 |
|
|
>50 | 66 | 43 | 66.2 | 23 | 59.0 |
|
| FIGO stage |
|
|
|
|
| 0.138 |
| I | 44 | 31 | 47.7 | 13 | 33.3 |
|
| II | 20 | 14 | 21.5 | 6 | 15.4 |
|
|
III | 36 | 17 | 26.2 | 19 | 48.7 |
|
| IV | 4 | 3 | 4.6 | 1 | 2.6 |
|
| Histological type
(WHO) |
|
|
|
|
| 0.2283 |
|
Serous | 34 | 18 | 27.7 | 16 | 41.0 |
|
|
Clear-cell | 42 | 27 | 41.5 | 15 | 38.5 |
|
|
Endometroid | 18 | 12 | 18.5 | 6 | 15.4 |
|
|
Mucinous | 8 | 7 | 10.8 | 1 | 2.6 |
|
| Mixed
type | 1 | 1 | 1.5 | 0 | 0.0 |
|
|
Adenocarcinoma | 1 | 0 | 0.0 | 1 | 2.6 |
|
| Chemotherapy |
|
|
|
|
| 0.3367 |
|
None | 3 | 3 | 4.6 | 0 | 0.0 |
|
|
Platinum-based | 7 | 5 | 7.7 | 2 | 5.1 |
|
| Taxane
plus platinum | 94 | 57 | 87.7 | 37 | 94.9 |
|
| Period of initial
treatment |
|
|
|
|
| 0.5496 |
| Before
2005 | 33 | 22 | 33.8 | 11 | 28.2 |
|
| After
2006 | 71 | 43 | 66.2 | 28 | 71.8 |
|
Clinical outcome based on CTGF
expression
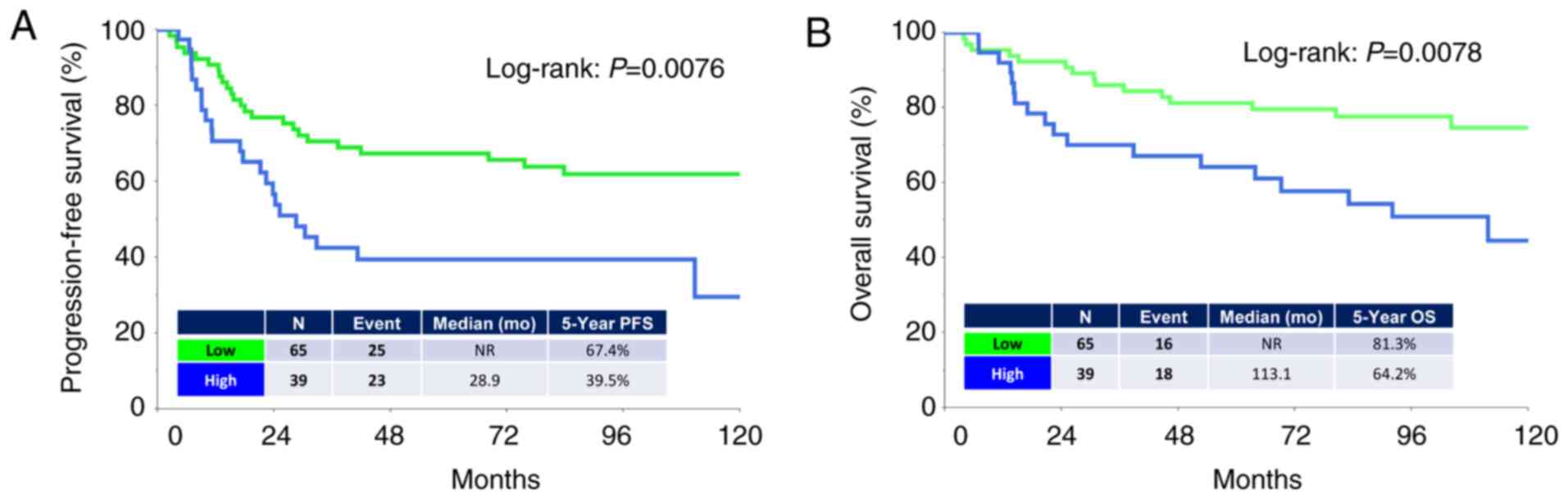
The median (range) follow-up duration was 93.6
(3.8–284.4) months in all patients. During the observation period,
48 (46.1%) patients experienced recurrence and 34 (32.7%) succumbed
to the disease. The median times to recurrence and death were 17.2
and 26.0 months, respectively. The five-year PFS and OS rates of
all patients were 57.4 and 75.1%, respectively. Patients in the
higher-level CTGF group showed poorer PFS and OS rates than those
in the lower-level group [PFS (log-rank: P=0.0076, and OS
(log-rank: P=0.0078), respectively] (Fig.
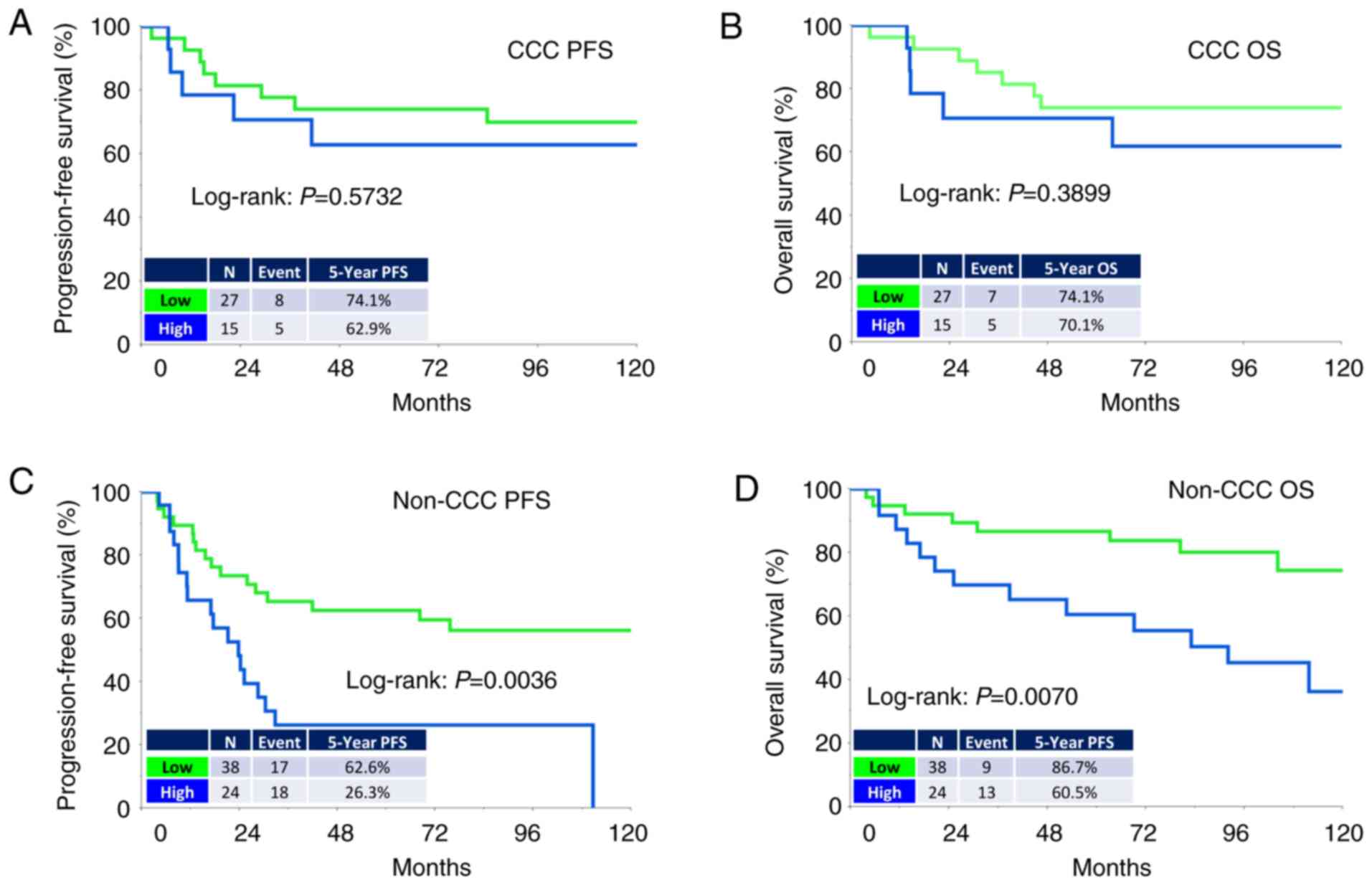
2A and B). Analysis of those with clear-cell carcinoma (CCC)
revealed no significant difference in PFS or OS between the two
groups (Fig. 3A and B). In contrast,
analysis of those with a non-clear-cell (non-CCC) histology
revealed that CTGF expression was significantly correlated with
poorer long-term survival (PFS: P=0.0036, OS: P=0.0070) (Fig. 3C and D).
Univariate and multivariate
analyses
We next conducted univariate and multivariate Cox
proportional analyses regarding PFS/OS, FIGO stage (I vs. II–IV),
age (≤50 vs. >50 years), histological type (non-clear-cell vs.
clear-cell), chemotherapy (taxane plus platinum vs. other
chemotherapy or none), period of initial treatment (before 2005 vs.
after 2006), and CTGF immunoreactivity (low vs. high) (Table SI). Based on univariate analysis, the
FIGO stage, histological type, and CTGF expression were significant
prognostic indicators of a poorer PFS. We evaluated the age, stage,
histological type and CTGF expressions in multivariate analysis.
This analysis demonstrated that the CTGF expression was a
significantly independent predictor of a poorer OS and PFS [OS:
Hazard ratio (HR): 2.141, 95% confidence interval (CI): 1.077–4.296
(P=0.0300); PFS: HR (high vs. low): 1.837, 95% CI: 1.023–3.289
(P=0.0418)].
Involvement of CTGF expression in the
tumor-promoting effect
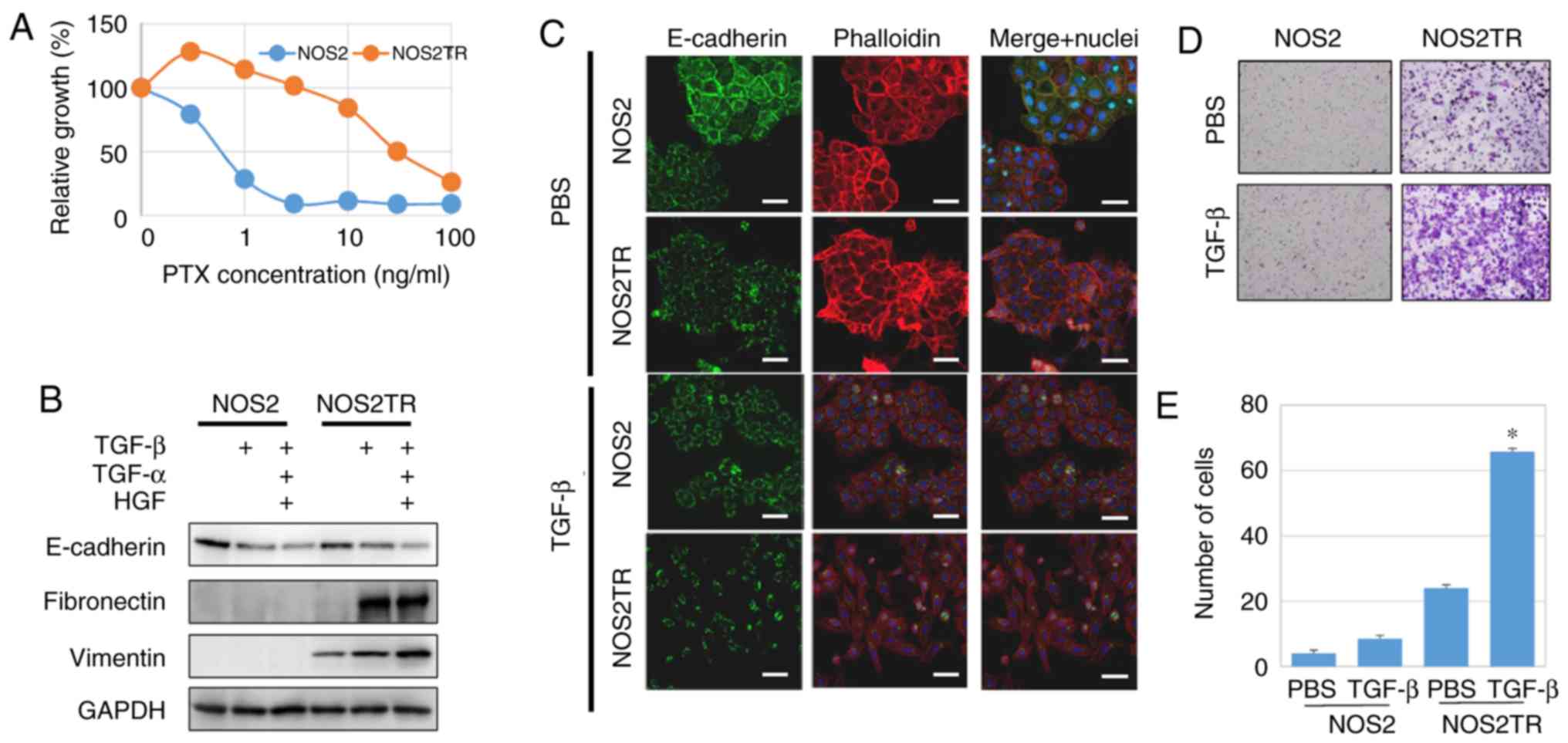
Subsequently, we examined the role of CTGF in the
malignant properties of EOC in vitro. Previously, we
generated PTX-resistant cell lines using parental EOC cells (NOS2).
We treated these cells for months with stepwisely increasing
concentrations of PTX and finally generated highly PTX-resistant
NOS2TR cells (Fig. 4A). The NOS2TR
cells displayed a spindle-shaped morphology with looser cell-cell
adhesion. Transforming growth factor (TGF)-β as well as hepatocyte
growth factor (HGF) and tumor necrosis factor (TNF)-α play an
important role in the dissemination of ovarian cancer, stimulating
tumor invasion and metastasis of tumor cells (31–33). When
in the presence of TGF-β, the morphology of NOS2TR cells showed a
more mesenchymal cell shape with decreased E-cadherin and increased
vimentin expressions, compared with the parental NOS2 cells
(Fig. 4B and C). Furthermore, the
addition of TGF-β to NOS2TR cells significantly increased the
migratory potential compared with that noted in the parental NOS2
cells (Fig. 4D and E)
(P<0.05).
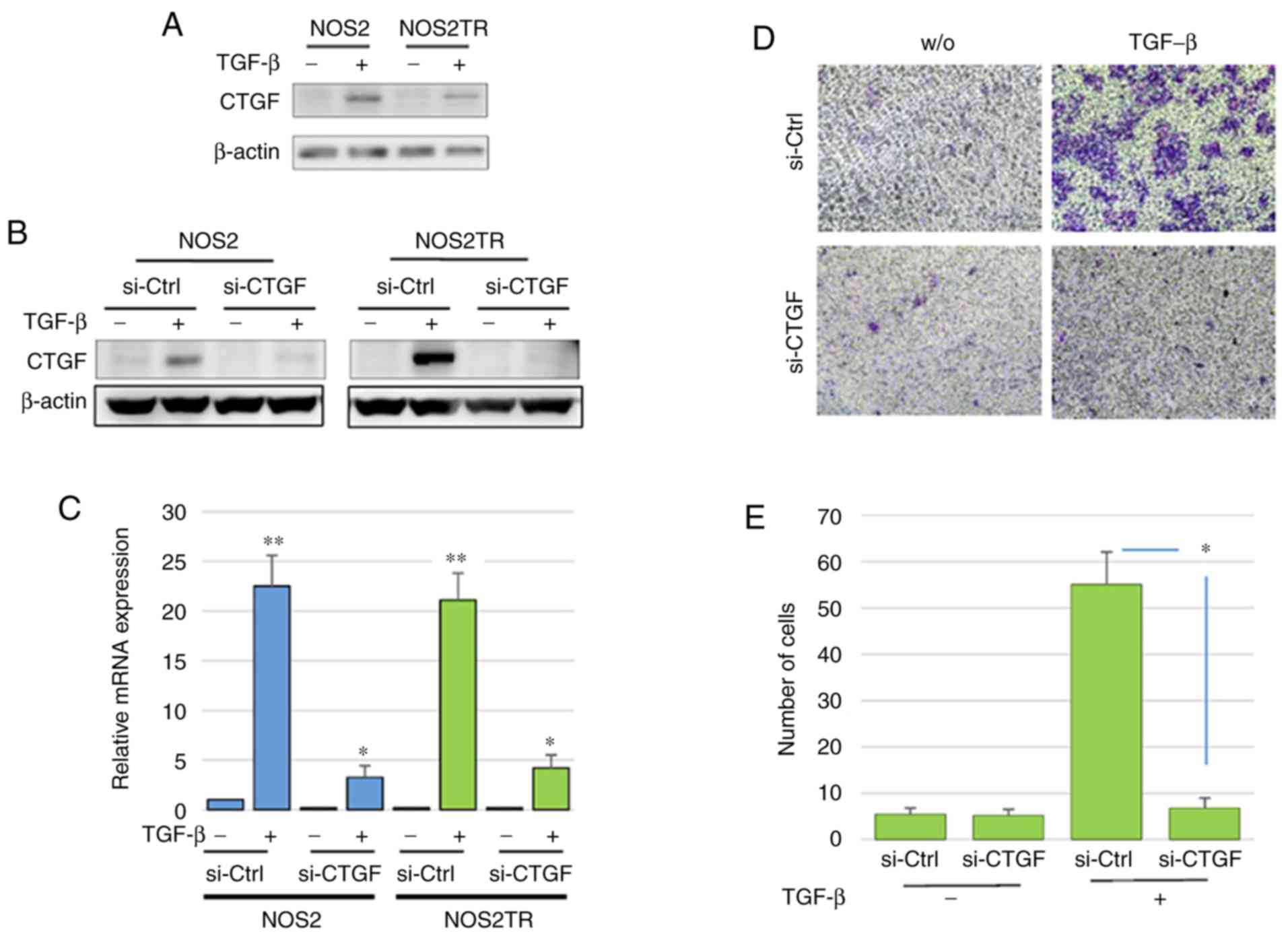
We further explored the role of CTGF in the
malignant properties of EOC using several in vitro
experiments. We first investigated the expression of CTGF in
various EOC cell lines. CTGF was expressed in ES-2 cells; however,
a lower level of expression of CTGF was observed in the SKOV3,
A2780, OVCAR, NOS2, and NOS2TR cells. The addition of TGF-β induced
the upregulation of CTGF expression in both the NOS2 and NOS2TR
cell lines (Fig. 5A). However, the
expression of CTGF following the addition of TGF-β was more
markedly increased in the NOS2TR than in the NOS2 cells. These
results suggest that TGF-β generated in the microenvironment
through cell-to-cell communication may contribute to the
enhancement of CTGF, leading to the acquisition of the chronic
chemoresistance/metastatic potential of EOC. Thus, we next examined
whether the acquired PTX-resistance of NOS2TR depended on the
upregulation of CTGF. Using specific si-RNA of CTGF, we confirmed
that the enhanced expression of CTGF in both cell lines was
completely blocked at the protein and transcriptional levels
(Fig. 5B and C). As shown in Fig. 5D, the enhanced migratory potential
induced by the addition of TGF-β was completely inhibited in the
CTGF-depleted NOS2TR cells. In contrast, in control
siRNA-transfected NOS2TR cells, we did not observe such an
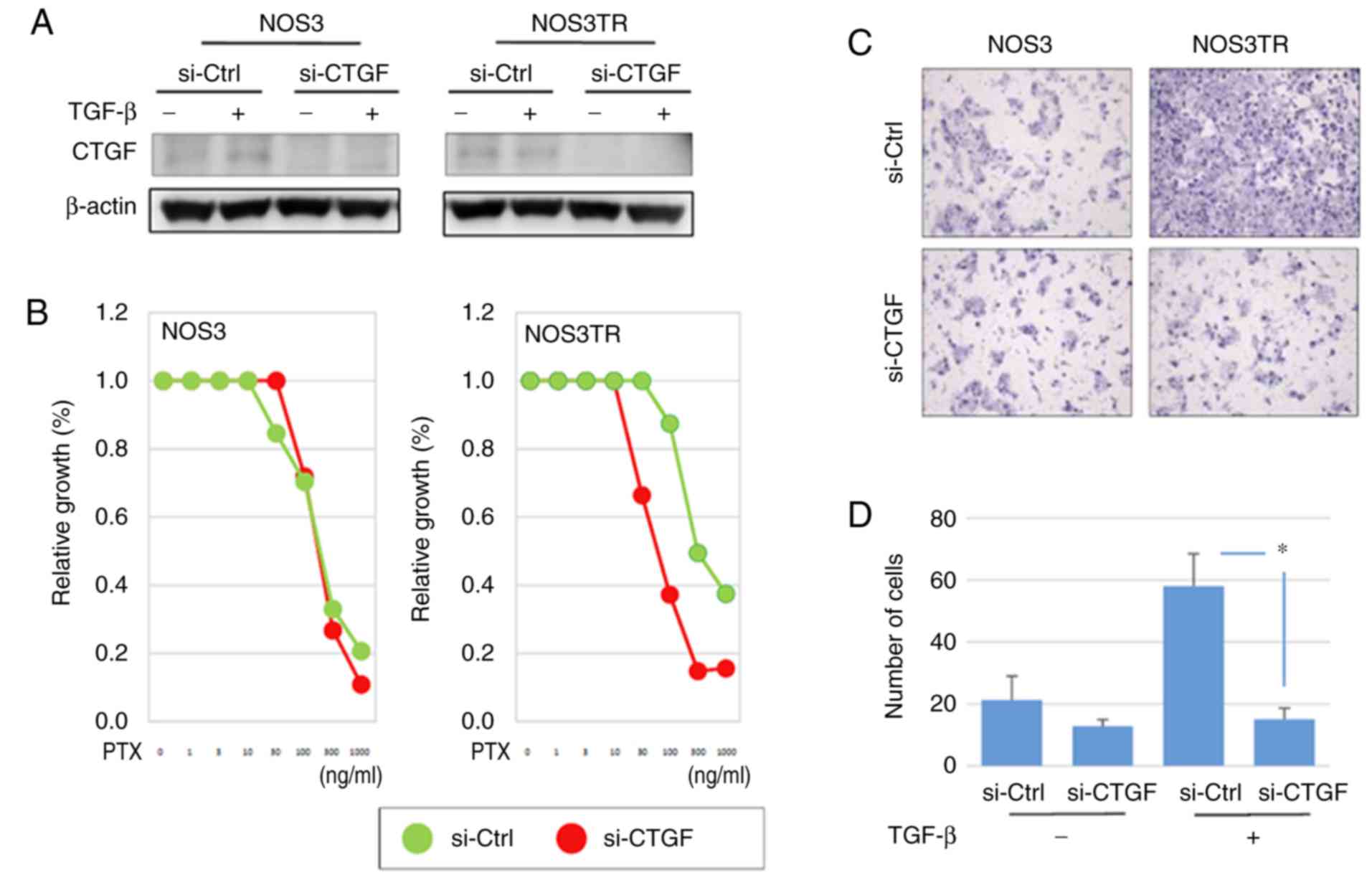
inhibitory effect (Fig. 5E). We
subsequently investigated whether CTGF is associated with the
chemoresistance-promoting effect in vitro. The NOS3TR cells,
another type of chronic PTX-resistant EOC cell line, transfected
with siRNAs (si-CTGF) were assessed by the PTX-sensitivity assay as
described above. In NOS3TR cells, the silencing of CTGF expression
led to restoration of the PTX sensitivity (Fig. 6A and B). Furthermore, we confirmed
that the TGF-β-dependent migration-promoting effect was completely
inhibited in CTGF-depleted NOS3TR cells, as observed in NOS3 cells
(Fig. 6C and D) (P=0.05).
Discussion
In the present study, we initially revealed that
connective tissue growth factor (CTGF) expression was significantly
correlated with a poorer prognostic outcome in epithelial ovarian
carcinoma (EOC) patients. Indeed, those with higher-level CTGF
expression demonstrated poorer OS and PFS rates than those with
lower-level expression. Moreover, multivariate analyses showed that
higher-level CTGF expression was an independent prognostic
indicator of poorer survival in those cases. Various studies have
revealed positive associations among CTGF expression, aggressive
features, and a poor oncologic outcome in patients with a number of
solid and hematological malignancies, including pre-B acute
lymphoblastic leukemia, gallbladder cancer, pancreatic carcinoma
and esophageal squamous cell carcinoma (34–37). Wang
et al demonstrated that CTGF expression was negatively
associated with the response to chemotherapy in breast cancer
patients who received neoadjuvant chemotherapy, and its cellular
overexpression resulted in resistance to doxorubicin- and
paclitaxel-induced apoptosis by the upregulation of Bcl-xL and
cellular inhibitor of apoptosis protein 1 (cIAP1) (38). Mao et al reported that the
expression of CTGF was significantly upregulated in clinical
tissues of gastric carcinoma patients, and the overexpression of
CTGF in gastric carcinoma cells promoted their migratory capability
in vitro and significantly increased tumor metastasis in
nude mice (39). Furthermore, the
downregulation of pancreatic tumor cells was found to lead to
markedly reduced growth on soft agar and in a murine subcutaneous
implantation model, and CTGF expression and secretion were found to
be increased in hypoxic pancreatic tumors (35). The current findings are consistent
with these results. However, in the present study, although
patients with a non-clear-cell histology and similar prognostic
tendencies were observed, analysis of those with clear-cell
carcinoma (CCC) revealed no significant difference between the low
and high CTGF expression groups. Indeed, EOC consists of
heterogeneous histological types with a different tumor biology.
CCC patients in general display a lower response rate to
platinum-based compounds, leading to intrinsic chemoresistance
(40,41). Thus, it is likely that chemoresistance
of this tumor is based on a CTGF-independent mechanism. Indeed,
earlier studies did not refer to the effect of CTGF expression on a
variety of histological types of EOC tumors. In a future study,
this observation should be verified.
A possible explanation of the poor survival in
patients with higher-level CTGF expression may be the enhanced
metastatic potential and chronic chemoresistance of this tumor. Our
previous study revealed that chronic PTX resistance induced more
marked mesenchymal hallmarks, including the switch of an epithelial
to a fibroblast-like morphology, upregulation of
epithelial-mesenchymal-transition-related biomarkers, and the
enhancement of motile capabilities (20). In the present study, the silencing of
CTGF significantly restored PTX susceptibility and reduced
invasiveness/motility in cells chronically resistant to PTX. This
suggests that the development/maintenance of both the
PTX-resistance and metastatic ability of these cells were
attributable to CTGF expression. A previous study showed that the
expression of CTGF was upregulated in human osteosarcoma cells
after treatment with cisplatin, and CTGF overexpression induced
enhanced resistance to cisplatin-mediated cell apoptosis through
upregulations of Bcl-xL and surviving (16). Yang et al demonstrated that the
overexpression of CTGF enhanced resistance to 5-FU-induced cell
apoptosis. They also reported that downregulation of the expression
of CTGF promoted the curative effect of chemotherapy and blocked
the cell cycle in the G1 phase (15).
Moreover, the expression of CTGF was found to be associated with
increased resistance to PTX-mediated cell apoptosis through the
upregulation of survivin and the AMP-activated protein kinase
(AMPK)-dependent nuclear factor κB pathway (42). In the treatment of EOC patients,
acquired or intrinsic chemoresistance is a major clinical cause of
a poor prognosis. The present study demonstrated that CTGF plays a
central role in the chemoresistance of EOC cells.
As well as tumor cells, stromal-cell derived CTGF
expression can exert tumor-promoting effects, such as proliferation
and invasion in glioma as well as pancreatic and prostate cancer
(43–45). Yang et al demonstrated that
stromal expression of CTGF induced significant increases in
microvessel density and xenograft tumor growth, suggesting that
this molecule is one of the key regulators of angiogenesis in the
tumor-reactive stromal microenvironment as a downstream mediator of
TGF-β1 (45). Similarly, according to
a recent study by Kim et al, immunohistochemical analyses of
high-grade serous ovarian tumors revealed that the highest level of
tumor stromal CTGF expression was correlated with the poorest
prognosis (46). Based on the
molecular signature in a subset of high-grade serous ovarian cancer
(HGSOC) samples that was primarily driven by a high stromal
response, CTGF was overexpressed in the stroma of these tumors in
association with a poor oncologic outcome (47). In our current analyses, we assessed
the CTGF immunoactivity in tumorous tissues. Indeed, CTGF may
function in the stromal cells as a metastasis-promoting factor
through tumor-stromal interaction. Considering the CTGF expression
as a molecular target of epithelial ovarian cancer (EOC) with
aggressive behavior, this substance plays an important role in not
only stromal-cancer communication but also the multidisciplinary
functions of tumor cells, including the development of
chemoresistance and metastatic potential.
The TGF-β signaling pathways are crucial regulators
of the multiple steps of the tumor microenvironment associated with
EMT (48–50). TGF-β was found to lead to a
long-lasting upregulation of CTGF mRNA and protein expression in
mouse and human proximal tubular epithelial cell lines (51). Tsai et al reported that CTGF is
an essential downstream mediator of TGF-β1-induced extracellular
matrix production and myofibroblast transdifferentiation in Graves'
orbital fibroblasts (52). Our
previous study demonstrated that TGF-β is generated by EOC cells,
which was synergistically upregulated under co-culture conditions
with human mesothelial cells (23).
In the present study, it was demonstrated that TGF-β stimulation
led to an increase in CTGF expression. Furthermore, it was revealed
that TGF-β-induced migratory potential and restoration of PTX
sensitivity were completely inhibited in CTGF-silenced
PTX-chemoresistant cells. Thus, there may be a close link between
the enhanced metastatic potential and PTX resistance of EOC via the
TGF-β/CTGF axis. However, in the present study, we did not conduct
relevant experiments regarding CTGF overexpression. We consider
that this was one of the critical limitations of the present
investigation. We hope to verify the significance of CTGF
overexpression in a future investigation. Overall, we consider CTGF
to be a valuable biomarker and effective therapeutic target for
EOC. Therefore, CTGF may be a therapeutic candidate for modulating
the PTX sensitivity of EOC.
In summary, we identified CTGF as a prognostic
indicator of and therapeutic target for EOC, particularly in
non-clear-cell carcinoma. An unfavorable outcome in patients with
higher-level CTGF expression may be due to the increased metastatic
capability and chemoresistance of EOC. However, the detailed
functions of CTGF remain unclear. We hope that the further
mechanistic elucidation of CTGF will contribute to improving
treatment for EOC patients by adding criteria for the
administration of systematic therapy in the future.
Supplementary Material
Supporting Data
Acknowledgements
We sincerely thank Mrs. M. Sugiyama (research
technician at Nagoya University, Graduate School of Medicine) for
advice on the in vitro experiments.
Funding
This study was supported by JSPS (Japan Society for
the Promotion of Science) KAKENHI Grants-in-Aid for Scientific
Research (grant nos. 17H04338 and 16K15704).
Availability of data and materials
The datasets used during the present study are
available from the corresponding author upon reasonable
request.
Authors' contributions
AS and HK carried out the data analysis and
interpretation and writing of the manuscript. ST, SS, YI, KN, JS,
KN and NY carried out the data collection. FK supervised the
research and was responsible for the funding. All authors read and
approved the manuscript and agree to be accountable for all aspects
of the research in ensuring that the accuracy or integrity of any
part of the work are appropriately investigated and resolved.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Nagoya University (Approval No. 2011-1234-2).
Patient consent for publication
Not applicable.
Competing interests
All authors declare that there are no competing
interests, and no financial or personal relationships with other
people or organizations that could inappropriately influence this
work.
Glossary
Abbreviations
Abbreviations:
|
EOC
|
epithelial ovarian cancer
|
|
HGSOC
|
high-grade serous ovarian cancer
|
|
CTGF
|
connective tissue growth factor
|
|
PFS
|
progression-free survival
|
|
OS
|
overall survival
|
|
FIGO
|
International Federation of Gynecology
and Obstetrics
|
References
|
1
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Brun JL, Feyler A, Chene G, Saurel J, Brun
G and Hocke C: Long-term results and prognostic factors in patients
with epithelial ovarian cancer. Gynecol Oncol. 78:21–27. 2000.
View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Thiery JP: Epithelial-mesenchymal
transitions in tumour progression. Nat Rev Cancer. 2:442–454. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Boyer B, Valles AM and Edme N: Induction
and regulation of epithelial-mesenchymal transitions. Biochem
Pharmacol. 60:1091–1099. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Vernon AE and LaBonne C: Tumor metastasis:
A new twist on epithelial-mesenchymal transitions. Curr Biol.
14:R719–R721. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Eisenkop SM, Friedman RL and Wang HJ:
Complete cytoreductive surgery is feasible and maximizes survival
in patients with advanced epithelial ovarian cancer: A prospective
study. Gynecol Oncol. 69:103–108. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kajiyama H, Mizuno M, Shibata K, Kawai M,
Nagasaka T and Kikkawa F: Extremely poor postrecurrence oncological
outcome for patients with recurrent mucinous ovarian cancer. Int J
Clin Oncol. 19:121–126. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Kajiyama H, Shibata K, Mizuno M, Umezu T,
Suzuki S, Yamamoto E, Fujiwara S, Kawai M, Nagasaka T and Kikkawa
F: Long-term clinical outcome of patients with recurrent epithelial
ovarian carcinoma: Is it the same for each histological type? Int J
Gynecol Cancer. 22:394–399. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Brigstock DR, Goldschmeding R, Katsube KI,
Lam SC, Lau LF, Lyons K, Naus C, Perbal B, Riser B, Takigawa M and
Yeger H: Proposal for a unified CCN nomenclature. Mol Pathol.
56:127–128. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Brigstock DR: The connective tissue growth
factor/cysteine-rich 61/nephroblastoma overexpressed (CCN) family.
Endocr Rev. 20:189–206. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Leask A and Abraham DJ: All in the CCN
family: Essential matricellular signaling modulators emerge from
the bunker. J Cell Sci. 119:4803–4810. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Tsai HC, Su HL, Huang CY, Fong YC, Hsu CJ
and Tang CH: CTGF increases matrix metalloproteinases expression
and subsequently promotes tumor metastasis in human osteosarcoma
through down-regulating miR-519d. Oncotarget. 5:3800–3812. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Han Q, Zhang HY, Zhong BL, Wang XJ, Zhang
B and Chen H: MicroRNA-145 inhibits cell migration and invasion and
regulates epithelial-mesenchymal transition (EMT) by targeting
connective tissue growth factor (CTGF) in esophageal squamous cell
carcinoma. Med Sci Monit. 22:3925–3934. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Lai D, Ho KC, Hao Y and Yang X: Taxol
resistance in breast cancer cells is mediated by the hippo pathway
component TAZ and its downstream transcriptional targets Cyr61 and
CTGF. Cancer Res. 71:2728–2738. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Yang K, Gao K, Hu G, Wen Y, Lin C and Li
X: CTGF enhances resistance to 5-FU-mediating cell apoptosis
through FAK/MEK/ERK signal pathway in colorectal cancer. Onco
Targets Ther. 9:7285–7295. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Tsai HC, Huang CY, Su HL and Tang CH: CCN2
enhances resistance to cisplatin-mediating cell apoptosis in human
osteosarcoma. PLoS One. 9:e901592014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang L, He J, Xu H, Xu L and Li N: MiR-143
targets CTGF and exerts tumor-suppressing functions in epithelial
ovarian cancer. Am J Transl Res. 8:2716–2726. 2016.PubMed/NCBI
|
|
18
|
Kajiyama H, Kikkawa F, Suzuki T, Shibata
K, Ino K and Mizutani S: Prolonged survival and decreased invasive
activity attributable to dipeptidyl peptidase IV overexpression in
ovarian carcinoma. Cancer Res. 62:2753–2757. 2002.PubMed/NCBI
|
|
19
|
Kajiyama H, Shibata K, Ino K, Mizutani S,
Nawa A and Kikkawa F: The expression of dipeptidyl peptidase IV
(DPPIV/CD26) is associated with enhanced chemosensitivity to
paclitaxel in epithelial ovarian carcinoma cells. Cancer Sci.
101:347–354. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Kajiyama H, Shibata K, Terauchi M,
Yamashita M, Ino K, Nawa A and Kikkawa F: Chemoresistance to
paclitaxel induces epithelial-mesenchymal transition and enhances
metastatic potential for epithelial ovarian carcinoma cells. Int J
Oncol. 31:277–283. 2007.PubMed/NCBI
|
|
21
|
Maeda O, Shibata K, Hosono S, Fujiwara S,
Kajiyama H, Ino K, Nawa A, Tamakoshi K and Kikkawa F: Spectrin αII
and βII tetramers contribute to platinum anticancer drug resistance
in ovarian serous adenocarcinoma. Int J Cancer. 130:113–121. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Utsumi F, Kajiyama H, Nakamura K, Tanaka
H, Mizuno M, Ishikawa K, Kondo H, Kano H, Hori M and Kikkawa F:
Effect of indirect nonequilibrium atmospheric pressure plasma on
anti-proliferative activity against chronic chemo-resistant ovarian
cancer cells in vitro and in vivo. PLoS One. 8:e815762013.
View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sakata J, Utsumi F, Suzuki S, Niimi K,
Yamamoto E, Shibata K, Senga T, Kikkawa F and Kajiyama H:
Inhibition of ZEB1 leads to inversion of metastatic characteristics
and restoration of paclitaxel sensitivity of chronic chemoresistant
ovarian carcinoma cells. Oncotarget. 8:99482–99494. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hosono S, Kajiyama H, Terauchi M, Shibata
K, Ino K, Nawa A and Kikkawa F: Expression of Twist increases the
risk for recurrence and for poor survival in epithelial ovarian
carcinoma patients. Br J Cancer. 96:314–320. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Sugiyama K, Kajiyama H, Shibata K, Yuan H,
Kikkawa F and Senga T: Expression of the miR200 family of microRNAs
in mesothelial cells suppresses the dissemination of ovarian cancer
cells. Mol Cancer Ther. 13:2081–2091. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Kurman RJ, Carcangiu ML, Herrington CS and
Young RH: WHO Classification of Tumours of Female Reproductive
OrgansFourth. IARC Press; 2014
|
|
28
|
Zeppernick F and Meinhold-Heerlein I: The
new FIGO staging system for ovarian, fallopian tube, and primary
peritoneal cancer. Arch Gynecol Obstet. 290:839–842. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Chen VW, Ruiz B, Killeen JL, Coté TR, Wu
XC and Correa CN: Pathology and classification of ovarian tumors.
Cancer 97 (10 Suppl). S2631–S2642. 2003. View Article : Google Scholar
|
|
30
|
Sakata J, Kajiyama H, Suzuki S, Utsumi F,
Niimi K, Sekiya R, Shibata K, Senga T and Kikkawa F: Impact of
positive ZEB1 expression in patients with epithelial ovarian
carcinoma as an oncologic outcome-predicting indicator. Oncol Lett.
14:4287–4293. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Lau TS, Chan LK, Wong EC, Hui CW, Sneddon
K, Cheung TH, Yim SF, Lee JH, Yeung CS, Chung TK and Kwong J: A
loop of cancer-stroma-cancer interaction promotes peritoneal
metastasis of ovarian cancer via TNFα-TGFα-EGFR. Oncogene.
36:3576–3587. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Nakamura M, Ono YJ, Kanemura M, Tanaka T,
Hayashi M, Terai Y and Ohmichi M: Hepatocyte growth factor secreted
by ovarian cancer cells stimulates peritoneal implantation via the
mesothelial-mesenchymal transition of the peritoneum. Gynecol
Oncol. 139:345–354. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Wei W, Kong B, Yang Q and Qu X: Hepatocyte
growth factor enhances ovarian cancer cell invasion through
downregulation of thrombospondin-1. Cancer Biol Ther. 9:79–87.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Alvarez H, Corvalan A, Roa JC, Argani P,
Murillo F, Edwards J, Beaty R, Feldmann G, Hong SM, Mullendore M,
et al: Serial analysis of gene expression identifies connective
tissue growth factor expression as a prognostic biomarker in
gallbladder cancer. Clin Cancer Res. 14:2631–2638. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Bennewith KL, Huang X, Ham CM, Graves EE,
Erler JT, Kambham N, Feazell J, Yang GP, Koong A and Giaccia AJ:
The role of tumor cell-derived connective tissue growth factor
(CTGF/CCN2) in pancreatic tumor growth. Cancer Res. 69:775–784.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Boag JM, Beesley AH, Firth MJ, Freitas JR,
Ford J, Brigstock DR, de Klerk NH and Kees UR: High expression of
connective tissue growth factor in pre-B acute lymphoblastic
leukaemia. Br J Haematol. 138:740–748. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Li LY, Li EM, Wu ZY, Huang X, Shen JH, Xu
XE, Wu JY, Huang Q and Xu LY: Connective tissue growth factor
expression in precancerous lesions of human esophageal epithelium
and prognostic significance in esophageal squamous cell carcinoma.
Dis Esophagus. 24:337–345. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Wang MY, Chen PS, Prakash E, Hsu HC, Huang
HY, Lin MT, Chang KJ and Kuo ML: Connective tissue growth factor
confers drug resistance in breast cancer through concomitant
up-regulation of Bcl-xL and cIAP1. Cancer Res. 69:3482–3491. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Mao Z, Ma X, Rong Y, Cui L, Wang X, Wu W,
Zhang J and Jin D: Connective tissue growth factor enhances the
migration of gastric cancer through downregulation of E-cadherin
via the NF-kB pathway. Cancer Sci. 102:104–110. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Sugiyama T, Kamura T, Kigawa J, Terakawa
N, Kikuchi Y, Kita T, Suzuki M, Sato I and Taguchi K: Clinical
characteristics of clear cell carcinoma of the ovary: A distinct
histologic type with poor prognosis and resistance to
platinum-based chemotherapy. Cancer. 88:2584–2589. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Shimada M, Kigawa J, Ohishi Y, Yasuda M,
Suzuki M, Hiura M, Nishimura R, Tabata T, Sugiyama T and Kaku T:
Clinicopathological characteristics of mucinous adenocarcinoma of
the ovary. Gynecol Oncol. 113:331–334. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Tsai HC, Huang CY, Su HL and Tang CH: CTGF
increases drug resistance to paclitaxel by upregulating survivin
expression in human osteosarcoma cells. Biochim Biophys Acta.
1843:846–854. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Edwards LA, Woolard K, Son MJ, Li A, Lee
J, Ene C, Mantey SA, Maric D, Song H, Belova G, et al: Effect of
brain- and tumor-derived connective tissue growth factor on glioma
invasion. J Natl Cancer Inst. 103:1162–1178. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Eguchi D, Ikenaga N, Ohuchida K, Kozono S,
Cui L, Fujiwara K, Fujino M, Ohtsuka T, Mizumoto K and Tanaka M:
Hypoxia enhances the interaction between pancreatic stellate cells
and cancer cells via increased secretion of connective tissue
growth factor. J Surg Res. 181:225–233. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Yang F, Tuxhorn JA, Ressler SJ, McAlhany
SJ, Dang TD and Rowley DR: Stromal expression of connective tissue
growth factor promotes angiogenesis and prostate cancer
tumorigenesis. Cancer Res. 65:8887–8895. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Kim HC, Ji W, Kim MY, Colby TV, Jang SJ,
Lee CK, Han SB and Kim DS: Interstitial pneumonia related to
undifferentiated connective tissue disease: Pathologic pattern and
prognosis. Chest. 147:165–172. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Tothill RW, Tinker AV, George J, Brown R,
Fox SB, Lade S, Johnson DS, Trivett MK, Etemadmoghadam D, Locandro
B, et al: Novel molecular subtypes of serous and endometrioid
ovarian cancer linked to clinical outcome. Clin Cancer Res.
14:5198–5208. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Crosas-Molist E, Bertran E and Fabregat I:
Cross-Talk Between TGF-β and NADPH oxidases during liver fibrosis
and hepatocarcinogenesis. Curr Pharm Des. 21:5964–5976. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Dhanasekaran R, Nakamura I, Hu C, Chen G,
Oseini AM, Seven ES, Miamen AG, Moser CD, Zhou W, van Kuppevelt TH,
et al: Activation of the transforming growth factor-β/SMAD
transcriptional pathway underlies a novel tumor-promoting role of
sulfatase 1 in hepatocellular carcinoma. Hepatology. 61:1269–1283.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Liu J, Chen S, Wang W, Ning BF, Chen F,
Shen W, Ding J, Chen W, Xie WF and Zhang X: Cancer-associated
fibroblasts promote hepatocellular carcinoma metastasis through
chemokine-activated hedgehog and TGF-β pathways. Cancer Lett.
379:49–59. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Kroening S, Solomovitch S, Sachs M,
Wullich B and Goppelt-Struebe M: Regulation of connective tissue
growth factor (CTGF) by hepatocyte growth factor in human tubular
epithelial cells. Nephrol Dial Transplant. 24:755–762. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Tsai CC, Wu SB, Kau HC and Wei YH:
Essential role of connective tissue growth factor (CTGF) in
transforming growth factor-β1 (TGF-β1)-induced myofibroblast
transdifferentiation from Graves' orbital fibroblasts. Sci Rep.
8:72762018. View Article : Google Scholar : PubMed/NCBI
|