Introduction
In the United States, colorectal cancer (CRC) is a
leading cause of cancer-related deaths (1). The diagnosis of CRC is based on the
tumor-node-metastasis (TNM) stage, a system that has limitations
due to varying genetic and epigenetic backgrounds. Biological
markers can improve early detection and guide clinicians in
subsequent therapies.
Trefoil factor (TFF) proteins include family members
TFF1, TFF2, and TFF3, which are characterized by the presence of at
least one 40-amino acid protein domain defining a three clover-leaf
structure termed the trefoil motif (2). TFF3 is a small, 9-kDa, stable protein
expressed in epithelia of the trachea, lungs, salivary glands, and
in the small intestine (3). In the
gastrointestinal (GI) tract, TFF3 is expressed in goblet cells of
the small and large intestines (4)
and is secreted, together with mucus, by mucus-secreting cells
(3,5). TFF3 promotes normal cell migration and
maintains colonic epithelial homeostasis (6,7).
TFF3 is involved in tumorigenesis and the
progression of various solid tumors (8–16). The
function of this protein in CRCs, however, remains unclear. It has
been suggested that patients with high TFF3 tumor levels have a
lower survival rate than those with lower expression (17). In addition, higher tumor expression
of TFF3 correlates with lymph node metastasis (LNM), i.e., a more
advanced stage (17). Furthermore,
high TFF3 levels in serum are associated with poor tumor
differentiation and a more advanced clinical TNM stage (18). By contrast, expression of TFF3 mRNA,
analyzed by real-time quantitative PCR (RT-PCR), does not differ
for paired CRCs and normal colonic mucosa (19). However, TFF3 transcripts are
elevated in CRCs with LNM compared with non-LNM tumors (19). As assessed by immunohistochemistry
(IHC), TFF3 expression in CRCs with LNM is elevated relative to
that in non-LNM CRCs (19).
Nevertheless, IHC of TFF3 in normal colonic mucosa and CRCs shows
no correlation of TFF3 expression with patient sex, cancer
differentiation status, or cancer stage (19).
Due to the conflicting findings related to TFF3,
further clarification is needed to elucidate the clinical value of
TFF3 as a marker of aggressive disease. Therefore, in the present
study, we analyzed TFF3 expression levels at the RNA and protein
levels in publicly available databases and validated its protein
expression in our collection of CRCs and their matching normal
tissues. Additionally, correlations between TFF3 expression,
molecular (expression of TP53), clinical and pathological
characteristics of patients (including patient survival) were
assessed.
Materials and methods
Bioinformatics analysis
The bioinformatics portal UALCAN (http://ualcan.path.uab.edu) was used to access TFF3
RNA and protein levels in normal colon and rectum tissue and in
CRCs of patients. This resource for expression analysis uses data
from The Cancer Gene Atlas (TCGA) (transcriptome by RNA sequencing)
(20) and the Clinical Proteomic
Tumor Analysis Consortium (CPTAC) Confirmatory/Discovery datasets
(proteomics by mass-spectrometry) (21). We checked for under-expressed genes
in TP53 mutant CRCs by use of heat-maps, which demonstrated
that TFF3 was one of the 25 genes having low expression in
TP53 mutant cancers as compared to TP53-wild-type tumors. RNA data
are expressed as transcripts per million and protein data as
Z-values, representative of standard deviations from the median
across samples for the given cancer type. Log2 spectral count ratio
values from CPTAC were first normalized within each sample profile,
then normalized across samples.
Patients and tissue samples
The population of this study was derived from the
University of Mississippi Medical Center (UMMC), Department of
Pathology research database. All tissue specimens (collected
between 2006 and 2016) were obtained at the time of surgery and had
complete clinicopathological data. The tissue samples were
de-identified and assigned a study number. Clinical and
pathological characteristics of the study subjects are provided in
Table I. These data include sex,
race, TNM stage, histological grade, evidence of LNM, surgical
margins, survival times, and status. Tumor and adjacent normal
colonic tissues from patients routinely obtained during surgery
were included in this study. A total of 96 cases were assessed by
board-certified pathologists (CS and VS). At the time of surgery,
patients were staged according to the guidelines of the American
Joint Committee on Cancer. The median follow-up for the 96 patients
was 5.4 years (range 0.1–10.3 years). All procedures of this study
involving human materials were approved by the UMMC Institutional
Review Board approval and performed according to the ethical
standards with the Declaration of Helsinki.
 | Table I.Clinicopathological characteristics
of the CRC patients. |
Table I.
Clinicopathological characteristics
of the CRC patients.
| Characteristic | Data |
|---|
| Age, years, mean
(range) | 59.2 (23–87) |
| Sex, n (%) |
|
|
Male | 50 (52.1) |
|
Female | 46 (47.9) |
| Race/ethnicity, n
(%) |
|
|
African-Americans | 56 (58.3) |
|
Non-Hispanic Whites | 40 (41.7) |
| Site, n (%) |
|
|
Colon | 62 (64.6) |
|
Rectum | 34 (35.4) |
| TNM stage, n
(%) |
|
| I | 11 (11.4) |
| II | 30 (31.3) |
|
III | 35 (36.5) |
| IV | 20 (20.8 |
| Histological grade,
n (%) |
|
|
Well-differentiated | 6
(6.3) |
|
Moderately differentiated | 78 (81.3) |
| Poorly
differentiated | 7
(7.3) |
|
Unknown | 5 (5.1%) |
| Lymph node
metastasis, n (%) |
|
|
Negative | 36 (37.5) |
|
Positive | 50 (52.1) |
|
Unknown | 10 (10.4) |
| Surgical margins, n
(%) |
|
|
Negative | 74 (77.1) |
|
Positive | 18 (18.8) |
|
Unknown | 4
(4.1) |
|
Follow-up time (years), median
(range) | 5.4 (0.1–10.3) |
Construction of tissue
microarrays
Tissue microarrays (TMA) were created using tumor
stage-matched CRC tissues. For each patient, representative
formalin-fixed paraffin-embedded (FFPE) tissue blocks, consisting
of a normal block and a tumor block were selected, giving a total
of 192 samples for TMA construction. Selection of the FFPE blocks
was accomplished on the basis of verified histological features,
which then were topographically correlated with the corresponding
paraffin blocks by pathologists. Cylindrical cores (2-mm) from
selected sites of the primary FFPE block were transferred to
composite paraffin blocks to construct the TMA using a Beecher MTA1
Manual Tissue Arrayer (Beecher Instruments). The resulting TMA
composite blocks were then sectioned at 5-µm thickness for IHC
staining and analysis.
Immunohistochemistry
IHC was performed on the FFPE tissue samples using
ABC Kits (Vector Laboratories Inc.) following the manufacturer's
instructions. Slides with the TMA sections were placed in a 60°C
oven for 1 h to allow the tissues to adhere. The sections were
deparaffinized in xylene, rehydrated with graded ethanol, and
washed with PBS, followed by antigen retrieval (Vector Laboratories
Inc., #H-3300, citrate-based antigen unmasking solution) with
citrate buffer (pH 6.0) for 20 min. Then, slides were incubated
with 3% hydrogen peroxide for 10 min to inactivate the endogenous
peroxidases, rinsed with PBS for 10 min, and incubated for 12 min
with protein blocking solution (Dako #X0590). Using mouse
Vectastain Elite ABC kits (Vector Laboratories, Inc.), blocking
serum was prepared using normal serum, and blocking of the tissue
sections was performed for 1 h at room temperature. Next, the
slides were incubated with blocking serum and primary antibody anti
human-TFF3 (mouse monoclonal diluted 1/25; cat # MAB4407, R&D
Systems) overnight at 4°C. Following extensive washing,
antigen-antibody complexes were detected using Vectastain Elite ABC
kits (Vector Laboratories, Inc.) according to the manufacturer's
protocol. By use of the ABC kits, anti-mouse IgG biotinylated
secondary antibody was prepared with blocking serum and incubated
for 30 min, followed by incubation with ABC Reagents A and B for
another 30 min. For color development, sections were processed with
3,3-diaminobenzidine peroxidase substrate kits (Vector
Laboratories, Inc.). Sections were then counterstained in Gill's
hematoxylin and dehydrated in ascending grades of ethanol before
clearing in xylene and being mounted under coverslips using
Cytoseal™ XYL (Thermo Fisher Scientific, Inc.; #83124). Subcellular
localizations of TFF3 were examined by a pathologist, defined as
cytoplasmic/membranous or globular staining, and scored.
Immunostaining evaluation
Evaluation of the IHC TMA was accomplished by two
independent evaluators blinded for specific diagnosis or prognosis
for each individual case. Tumor cells showing cytoplasm stained in
brown were considered positive. To provide a semi-quantitative
assessment of the expression of TFF3 in each core, colonic
epithelial cells were individually scored from 0–3 for the
intensity of immunostaining and 1–3 for the area of immunostaining.
The product of intensity and area was used as the combined
intensity score, which ranged from 0–9, with 0 defining no
expression and 9 defining high expression. Values are expressed as
median (interquartile range). To assess the association between
TFF3 expression and clinical features in the CRC cases, patients
were divided into two groups, with low and high TFF3 tumor
expression, based on the optimal cutoff point calculated as the
value with the most significant log-rank test split (4.5 for
combined intensity score).
Statistical analysis
Data were analyzed using SPSS software, version 13.0
(SPSS Inc.) and SAS 9.4 (SAS Inc.). The difference in TFF3 gene or
protein expression between normal tissue and tumor tissue or for
any other pairwise comparison obtained using bioinformatics
analyzes was evaluated by Student's t-test (for comparisons between
two groups), or one-way ANOVA followed by Dunnett's multiple
comparisons (when three or more groups were compared). Pairwise
comparisons were always relative to normal tissue. Pearson's
correlation coefficient (r) was used to evaluate association
between variables. For IHC data, differences were compared by
Mann-Whitney U test for non-matched data or Wilcoxon matched-pairs
signed rank test. Two-sided P-values were determined via Chi-square
or Fisher's exact tests for categorical variables. Overall survival
was analyzed by the Kaplan-Meier method with the use of the
log-rank test to compare survival of groups. For all analyses, the
level of significance was set at P<0.05.
Results
Bioinformatics analyses of RNA
expression of TFF3 in the CRC tissues
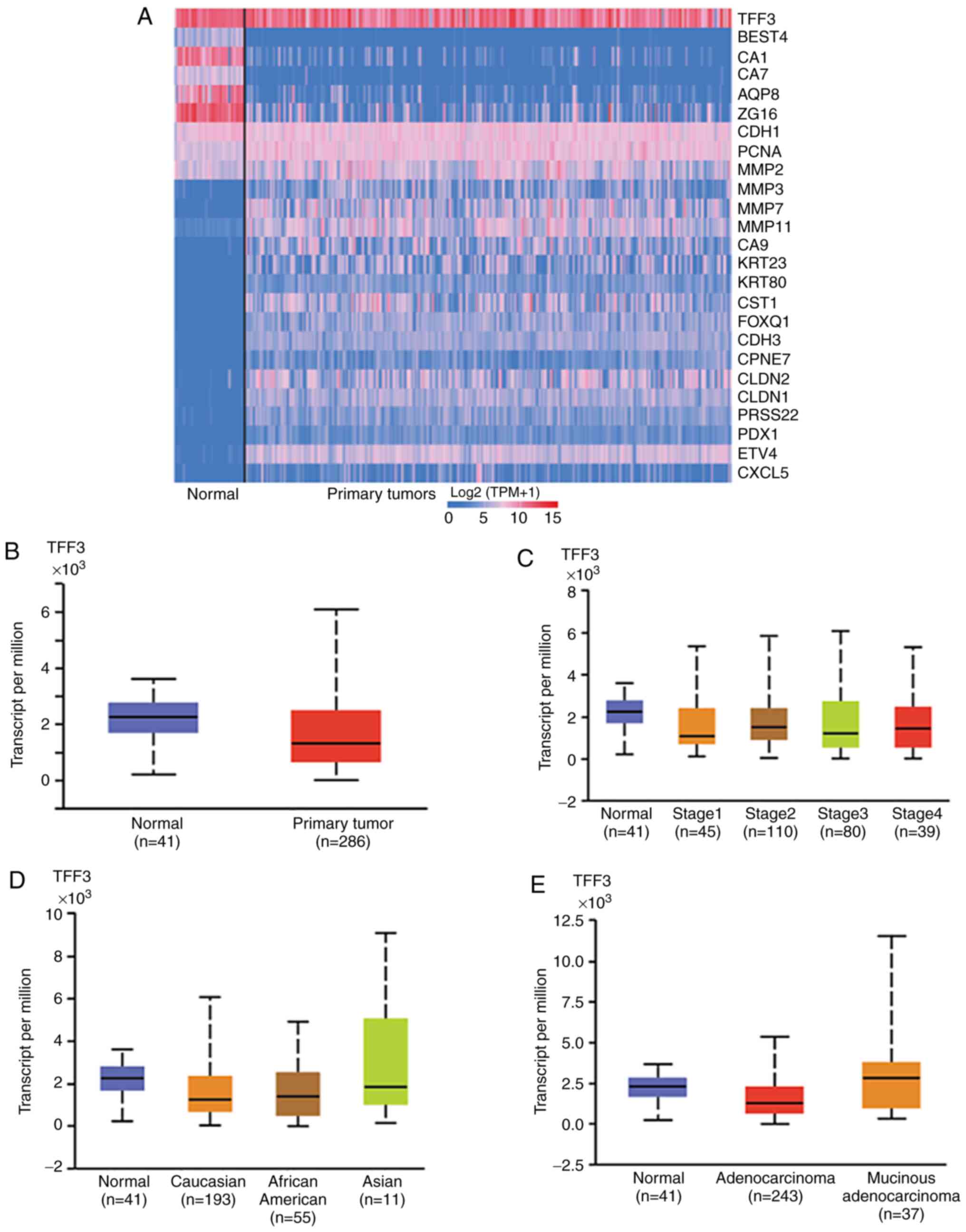
Using UALCAN we generated an interactive heat-map of
differentially expressed genes in normal tissue or CRCs and
included TFF3 as a query gene. The heat-map demonstrated
differential expression of various genes, including TFF3, in normal
and CRC tissues (Fig. 1A). Further,
as determined with the UALCAN database, mRNA data for CRCs
suggested TFF3 overexpression [NS (not significant), P=0.72] in
normal (n=41) as compared to CRC tissues (n=286) (Fig. 1B). Data mining for different
pathologic stages [stage 1 (n=45), stage 2 (n=110), stage 3 (n=80),
and stage 4 (n=39)] suggested lower TFF3 expression in CRCs as
compared to normal colon (n=41), irrespective of the stage (NS,
P=0.88) (Fig. 1C). Moreover,
UALCAN-acquired TCGA data showed lower expression of TFF3 in tumors
relative to normal colonic tissues irrespective of patient race
[Caucasian (n=193), African-American (n=55), and Asian (n=11)]
(Fig. 1D); however, race-related
values were not statistically different (P=0.56). A similar trend
was observed for tumor histologic types [adenocarcinoma (n=243) and
mucinous adenocarcinoma (n=37)] (Fig.
1E, P=0.053), nodal status [N0 (n=166), N1 (n=70), and N2
(n=47)] (Fig. S1A, P=0.77),
patient sex [male (n=156) vs. female (n=127)] (Fig. S1B, P=0.51), and age [21–40 years
(n=12), 41–60 years (n=90), 61–80 years (n=149), and 81–100 years
(n=32)] (Fig. S1C, P=0.53).
Bioinformatics CPTAC analyses of
protein expression of TFF3 in normal colonic and tumor tissues and
correlation with tumor and patient characteristics
UALCAN bioinformatics analysis was used to analyze
protein levels of TFF3 in colonic tissues. The protein expression
data was obtained from the mass-spectrometry proteomic profiles,
generated by the Clinical Proteomic Tumor Analysis Consortium
(CPTAC). The results showed that the expression of TFF3 was high in
normal colonic tissue (n=100) and low in CRCs (n=97) (Fig. 2A and B) (P<0.0001). In addition,
there was high expression in uterine corpus endometrial carcinoma
(UCEC) (P=0.002), low expression in clear cell renal cell carcinoma
(P<0.001), but no difference in breast cancers (P=0.77) and
ovarian cancer (P=0.22) (Fig. 2A).
TFF3 expression was significantly lower (P<0.0001) in late-stage
CRCs [stage 3 (n=40); stage 4 (n=8)] compared to early stages
[stage 1 (n=10); stage 2 (n=39)], suggesting a role for TFF3 in
tumor suppression (Fig. 2C).
Expression was low, particularly for adenocarcinoma (n=77), but
also for mucinous adenocarcinoma (n=19), as compared to normal
tissue, P<0.0001 (Fig. 2D).
Furthermore, TFF3 expression was low when tumors of Caucasian
(n=71), African-American (n=7), and Asian (n=16) CRC patients
(P<0.0001) (Fig. 2E) were
compared to normal tissue. Next, we found downregulation of TFF3 in
CRCs of patients for both sexes [male (n=41) vs. female (n=56),
P<0.0001] (Fig. 2F) and for age
groups [21–40 years (n=3), 41–60 years (n=31), 61–80 years (n=53),
and 81–100 years (n=7), P<0.0001] (Fig. 2G). These data showed downregulation
of TFF3 protein expression in CRCs as compared to normal colon
irrespective of the tumor stage; histologic type; and patient race,
sex, and age.
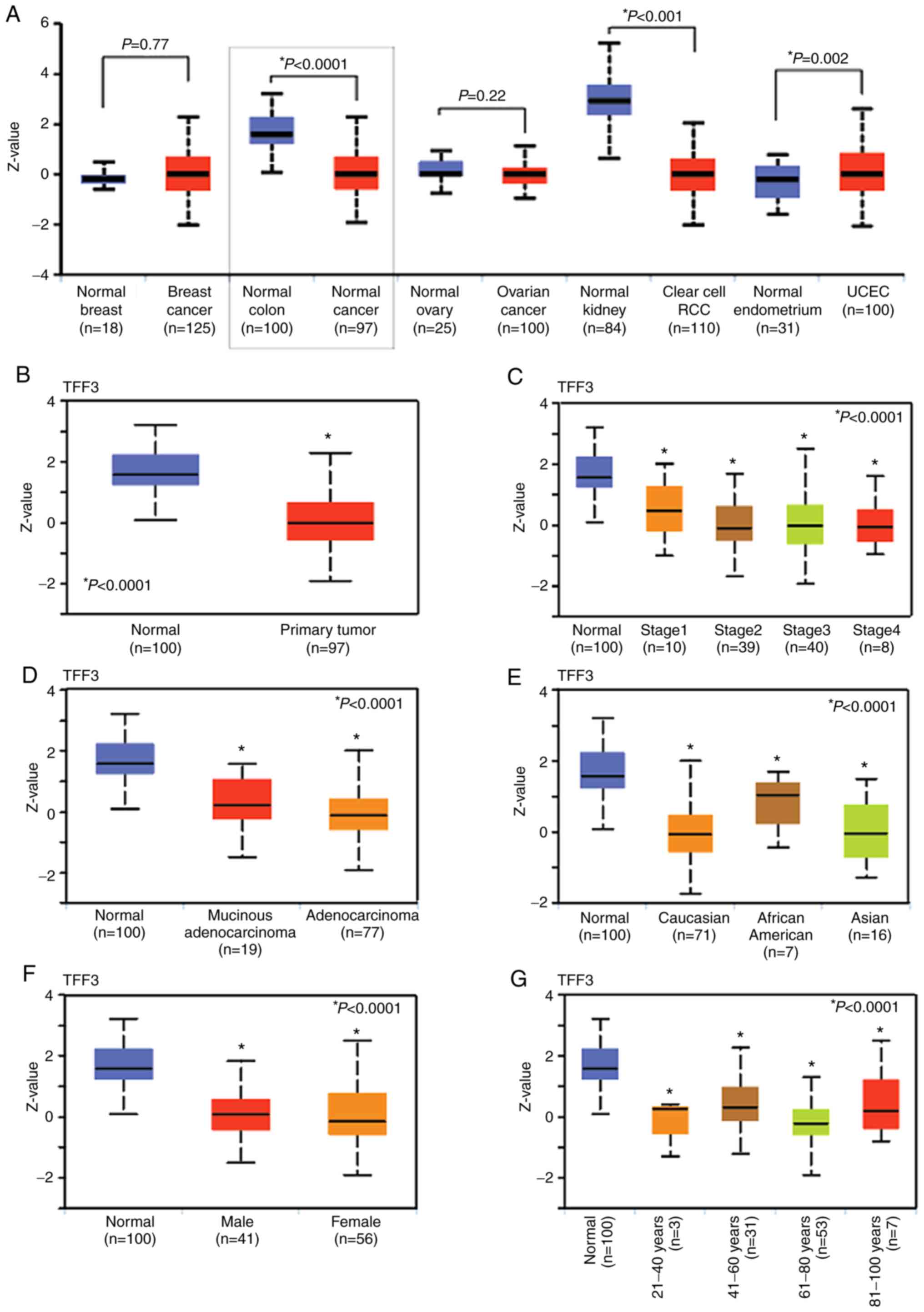 | Figure 2.Protein expression of TFF3 in CRC
tissues. (A) The graphs show the pan-cancer subtype for various
cancers. Z-values represent standard deviations from the median
across samples for the given cancer type. Log2 spectral count ratio
values from CPTAC were first normalized within each sample profile,
and then normalized across samples (Student's t-test). (B)
Box-whisker plots showing the protein levels of TFF3 in normal
tissue and tumors (Student's t-test). (C) Plots showing
correlations between TFF3 protein expression with pathologic tumor
stages, (D) tumor histologic types, (E) patient race, (F) patient
sex, and (G) age (C-G, one-way ANOVA with Dunnett's multiple
comparisons test). Pairwise comparisons relative to normal tissue.
CRC, colorectal cancer; TFF3, trefoil factor 3; CPTAC, Clinical
Proteomic Tumor Analysis Consortium. UALCAN website that used
two-sided Students t-test provided P-values, indicated by asterisk
(*). P-value <0.05 was defined as statistical significant. |
Correlation of TFF3 RNA expression
with TP53-mutational status using bioinformatics
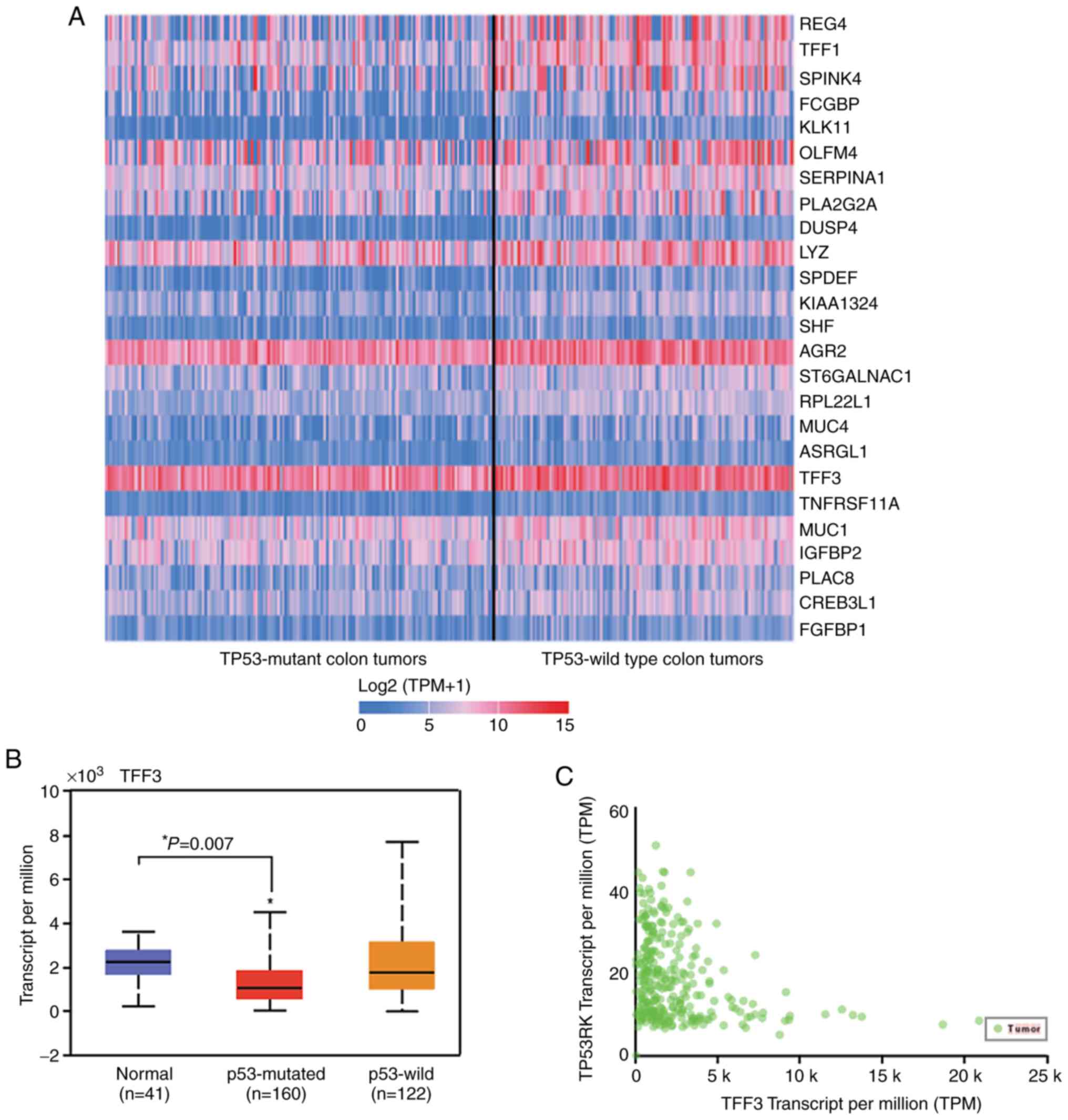
Since P53 mutations occur in 50–60% of CRCs, we
explored the correlation between TFF3 and p53 RNA expression and
generated an interactive heat-map using the UALCAN database
(Fig. 3A). The graph shows 27%
lower TFF3 RNA expression in TP53-mutant tumors (n=162)
(P=0.007) as compared to normal tissue (n=41). No significant
changes in transcripts of TFF3 were noted in TP53 wild-type tumors
(n=122), as compared to those observed in normal epithelium (n=41)
(Fig. 3B). UALCAN correlation
analysis showed an inverse correlation of TFF3 expression with TP53
regulating kinase (TP53RK) (Pearson correlation coefficient,
r=−0.32) (Fig. 3C).
Validation of bioinformatics findings
of TFF3 protein expression by immunohistochemical (IHC) profiling
of normal colonic and tumor tissue
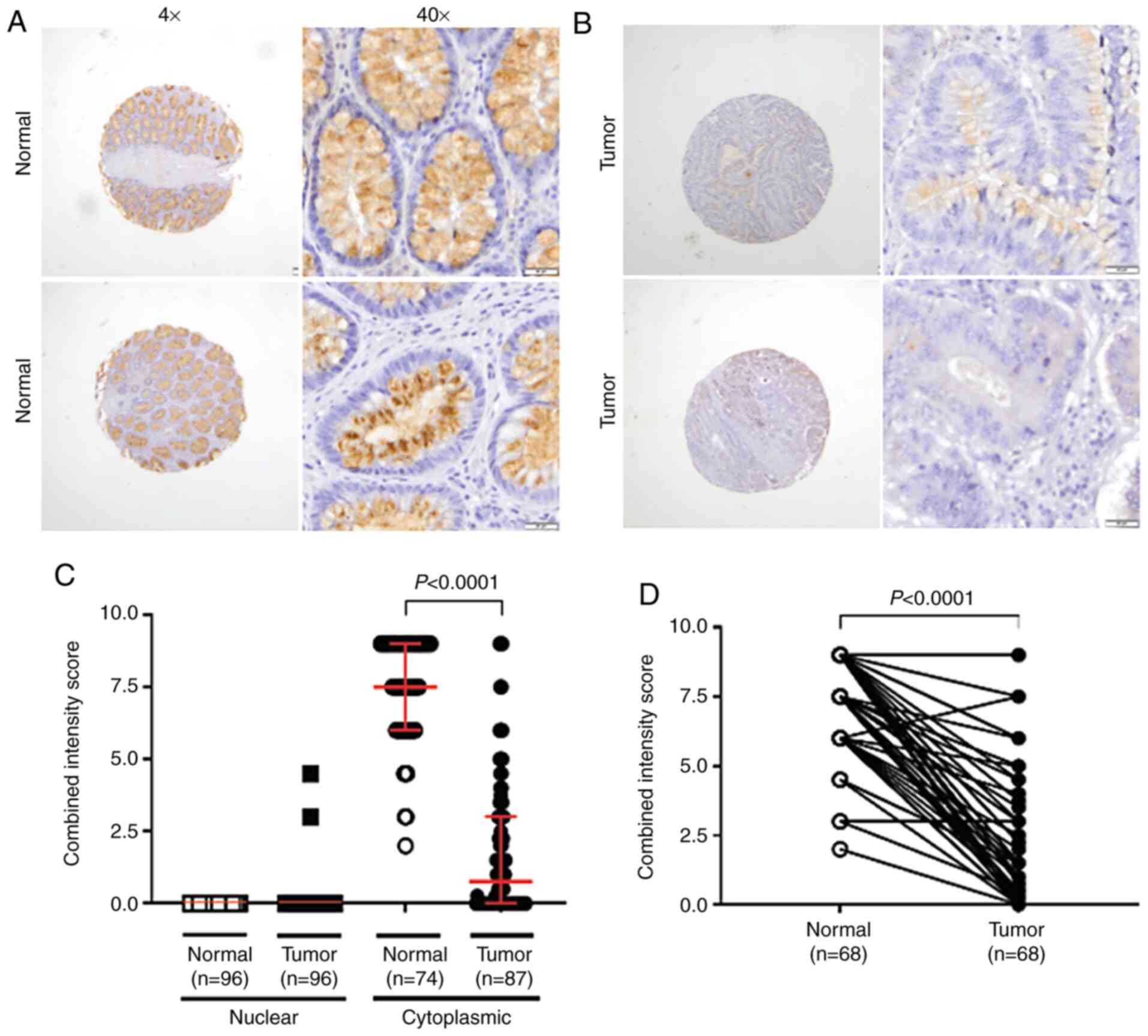
We evaluated TFF3 expression by IHC analysis of
normal tissues and CRCs. Positive staining was evident for 74
normal cores. In both the basal and luminal portions of colonic
crypts, cytoplasmic staining was present mainly in the supra- and
perinuclear cytoplasm of epithelial cells (Fig. 4A). In CRCs, although globular
staining was present in 2.1% (2 of 96) of specimens, TFF3 staining
was predominantly cytoplasmic, as noted in 71.9% (60 of 87) of the
positively stained cores. Mainly supra-nuclear (Fig. 4B), cytoplasmic TFF3 immunoreactivity
in CRCs [0.75 (3.0)] (Fig. 4C) was
lower by 90% (P<0.0001) relative to staining in normal tissues,
when independent samples were compared. Analysis of the cytoplasmic
immunostaining in normal samples revealed the absence of globular
TFF3 expression; the normal combined intensity score, however, was
7.5 (3.0) (Fig. 4C). Lower TFF3
expression was noted in 95.6% (65 of 68) of available normal-tumor
matching pairs (P<0.0001) (Fig.
4D).
Patients grouped by IHC expression of
TFF3 and association with clinicopathologic features
There was no significant association of TFF3
expression with patient sex (P=0.656), race/ethnicity (P=0.383),
tumor site (P=0.819), TNM stage (P=0.120), LNM (P=0.081), or
surgical margins (P=0.682) (Table
II). However, low TFF3 tumor immunoreactivity was associated
with moderately differentiated histological grade (P=0.026).
| Table II.Correlation of the clinicopathologic
findings with TFF3 expression in the CRC cases. |
Table II.
Correlation of the clinicopathologic
findings with TFF3 expression in the CRC cases.
| Characteristic | TFF3 low (score
≤4.75) | TFF3 high (score
>4.75) | χ2 or
Fisher's exact test P-value |
|---|
| Sex |
|
|
|
|
Male | 40 | 5 | 0.656 |
|
Female | 36 | 6 |
|
| Race/ethnicity |
|
|
|
|
African-Americans | 46 | 5 | 0.383 |
|
Non-Hispanic Caucasians | 30 | 6 |
|
| Site |
|
|
|
|
Colon | 31 | 29 | 0.819 |
|
Rectum | 13 | 14 |
|
| TNM stage |
|
|
|
| I | 9 | 2 | 0.120 |
| II | 21 | 6 |
|
|
III | 30 | 1 |
|
| IV | 16 | 2 |
|
| Histological
grade |
|
|
|
|
Well-differentiated | 2 | 2 | 0.026a |
|
Moderately differentiated | 64 | 7 |
|
| Poorly
differentiated | 5 | 2 |
|
| Lymph node
metastasis |
|
|
|
|
Negative | 25 | 7 | 0.081 |
|
Positive | 44 | 3 |
|
| Surgical
margins |
|
|
|
|
Negative | 57 | 10 | 0.682 |
|
Positive | 15 | 1 |
|
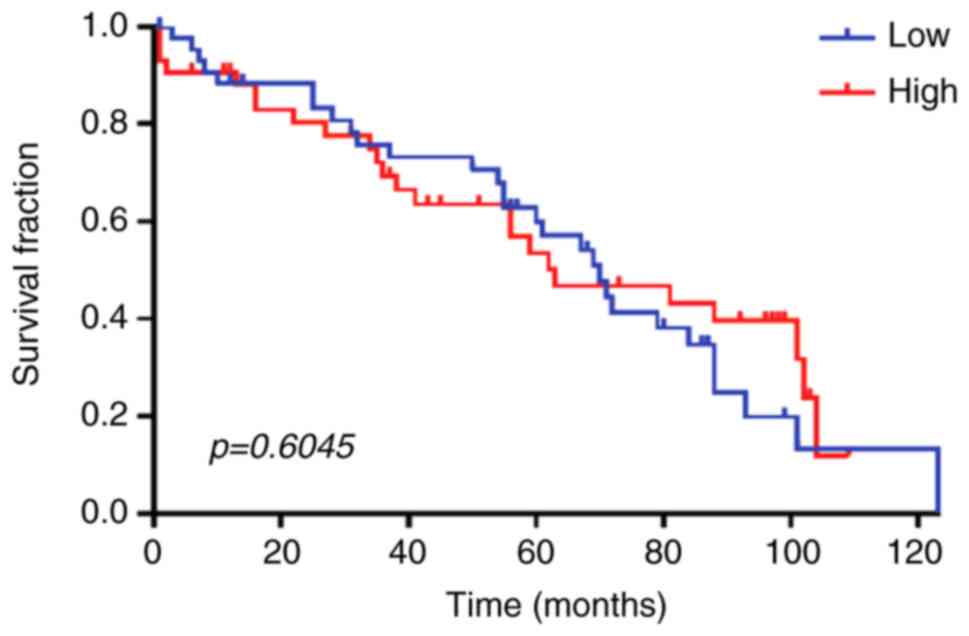
Survival analysis
There was no significant difference for high and low
IHC expression of TFF3 and overall survival (Fig. 5).
Discussion
Initiation and progression of CRC involves several
molecular alterations. Thus, finding new molecular targets remains
an essential milestone toward understanding the pathobiology and
progression of human cancers. Meta-analysis using available
web-tools to find molecular targets have helped cancer researchers
in achieving these milestones. By using UALCAN, a user-friendly
web-tool for analyzing cancer omics data from TCGA (RNA expression
by sequencing) and CPTAC (protein expression), the current study
established that TFF3 expression was significantly downregulated in
CRCs. Our study also validated, by IHC assays, low phenotypic
expression levels of TFF3 in CRCs as compared to normal tissue; the
expression was independent of pathologic tumor stage and histologic
type and patient race, age, or sex. In addition, the present study
showed, by bioinformatics analysis, that low levels of TFF3 RNA
expression were strongly associated with tumors exhibiting p53
mutations. Collectively, our data showed that TFF3 is downregulated
in CRCs and indicate that loss of TFF3 could be involved in the
pathogenesis and progression of the disease.
TFF proteins maintain GI mucosal homeostasis in
response to mechanical and/or chemical mucosal injury (22–26).
Through anti-apoptotic effects, TFFs protect epithelia from death
and promote cell migration (6,9,27,28).
TFFs are involved in the development and progression of various
types of cancer (8–10,12–14,16),
including CRC (17–19). The role of TFF3 in the pathogenesis
of CRC, however, remains unclear. Previously studied in different
malignancies, a discrepancy was observed regarding protein and RNA
levels of TFF3. Interestingly, similar to our findings, two earlier
studies in CRC reported reduced TFF3 expression at RNA and protein
levels in tumors relative to normal epithelium (11,19).
Specifically, Huang et al (19) found higher mRNA of TFF3 in
metastatic lesions of CRCs than those CRCs confined to the
colorectum, which is in agreement with our data that mRNA levels of
TFF3 were increased in advanced CRC stage relative to low stage
tumors. Additionally, Huang et al demonstrated decreased
mRNA levels of TFF3 organ-confined CRCs relative to normal tissues.
However, this association was not statistically significant
(19). Moreover, our data obtained
from publicly available RNA (TCGA data) and protein expression
(proteomics data) of TFF3 (obtained by using UALCAN) agrees with
our findings. Our data using UALCAN as a tool to analyze RNA (TCGA
data) and protein expression (proteomics), agrees with the reports
showing organ-specific tumor expression of TFF3. Moreover, our
analysis reproduces the expression patterns for TFF3 and CRC
revealed by previous studies. Although different from some previous
findings, we are confident about the relevance of our results since
our validation strategy using the UALCAN expression platform,
queried for the CPTAC Confirmatory/Discovery dataset, revealed
lower TFF3 expression in tumors relative to normal epithelium,
similar to what we found in our tissue sample cohort. Collectively,
our data suggest that protein expression of TFF3, a modulator of
cell differentiation and glandular structure, is low in CRCs
relative to normal mucosa.
In CRCs, p53 signaling is frequently dysregulated
(29,30). Moreover, tumors with p53 mutations
are resistant to various therapies. The current bioinformatics
analysis showed that CRC tumors exhibiting p53 mutations had low
expression of TFF3 but that p53 wild-type tumors did not,
indicating an inverse relationship of p53-mutated CRCs with low
TFF3 expression. Additionally, UALCAN correlation analysis showed
an inverse correlation of TFF3 expression with TP53 regulating
kinase (TP53RK), suggesting a link between TFF3 and TP53. Indeed, a
recent study of retinoblastoma cells showed that TFF3
overexpression activates TP53 and that TP53 is a downstream target
of TFF3 signaling (31). Moreover,
the heat map data showed reduced transcripts of TFF3 in
TP53-mutated CRCs, suggest a functional interactome linking
the signaling pathways which relate the expression of these two
molecules. Thus, future research is warranted focusing on
establishing the molecular basis of the functional interaction
between TFF3 and TP53 in CRC and would provide tools to molecularly
categorize histologic types (e.g., mucinous tumors), known to have
high expression of TFF3. Such multi-molecular classifiers could add
prognostic value to that offered by traditional single-molecule
classifiers.
Concerning the association between TFF3 expression
and clinicopathological variables, we did not find a correlation
between tumor expression of TFF3 and survival, even upon
stratification by clinicopathological variables. Since we did not
have a separate validation cohort for our IHC study, we performed
survival analyses based on mRNA of TFF3. We utilized two data
mining portals: UALCAN (TCGA dataset) and prognostics database
ProGeneV2 (32). For ProGenV2
analysis we used datasets: GSE28814, GSE17536, GSE17537, GSE12945,
GSE16125, GSE24551, GSE28722, GSE30378, GSE41258, GSE29621,
GSE38832, and GSE39582. In none of the studied datasets,
statistically significant association between expression of TFF3
and survival was found (data not shown). These results demonstrate
concordance between the UALCAN and ProGeneV2 platforms, and suggest
lack of prognostic value of TFF3 transcripts to anticipate survival
in CRC. Future study in a large CRC tissue cohort, with extended
follow-up, may provide the prognostic value of TFF3 in CRC. Our
findings add to the complexity related to the prognostic value of
TFF3 in CRC. For example, Yusup et al found poor overall
survival of CRC patients with high TFF3 expression relative to
those with low TFF3 expression (17). Similarly, there was lower survival
of patients with CRCs positive for TFF3 in comparison to those with
CRCs negative for TFF3 (33). In
addition, in the cited studies, higher TFF3 expression was found in
cancer tissue relative to corresponding normal mucosa. We, on the
contrary, found lower expression of TFF3 in CRCs relative to normal
mucosa. Despite the differences and the need of further
investigation, we and others have support to propose that, in
tumors with low or lack of expression of TFF3, epithelial
restitution and wound healing effects mediated by this protein, as
seen in normal mucosa, would not be prevalent. Under these
conditions, low TFF3 in the tumor may not help to maintain
epithelial integrity, as occurs in non-tumor tissue (34). Appropriate exploration of the
molecules related with CRC tumorigenesis or survival will help to
test this hypothesis. Although our findings differ with most of
those in the literature (17,33)
and suggest that tumor expression of TFF3 is not a prognostic
factor for poor survival of patients with CRC, this matter is an
issue for debate.
The limitations of our study include its
retrospective nature as well as its small sample size. Furthermore,
the results require validation in larger, independent cohorts. It
would be valuable to determine the prognostic value of serum TFF3,
previously determined to be associated with poor tumor
differentiation and clinical TNM stage (18).
In summary, our findings provide evidence that TFF3,
a factor involved in cell migration and integrity of the GI mucosa,
is downregulated in CRCs relative to normal epithelium and that it
may be involved in disease progression. We believe that relevance
of our findings is high due to similar patterns of low TFF3
expression in tumors identified in large, publicly available omics
databases. However, the prognostic value of TFF3 in CRCs is an
issue needing further research.
Supplementary Material
Supporting Data
Acknowledgements
We are grateful to Elizabeth Tarsi, Tara Craft,
Eldrin Bhanat, Jaswinder Kaur, and Joy King for establishing and
maintaining the databases, and to Jesus Monico and Lisa Sullivan
for establishing preparatory TMAs. We also thank Richard Summers,
Srinivasan Vijayakumar, and Roy Duhe (UMMC) for their continued
support. Anne Dautenhahn Martin and Jennifer Reneker at UMMC, and
Donald Hill at the University of Alabama at Birmingham edited the
manuscript.
Funding
This study was supported in part by the Office of
Research and Sponsored Programs, University of Mississippi Medical
Center (CRG and IE); the University of Mississippi School of
Medicine Medical Student Research Program (LF); Coordination for
the Improvement of the Higher Education Personnel (CAPES)
foundation, scholarship #13603-13-2 (MJS), and the impact funds
from School of Medicine and the Department of Pathology, University
of Alabama at Birmingham (UM).
Availability of data and materials
The data supporting the findings reported in this
study are available from the corresponding author upon reasonable
request.
Authors' contributions
IE, SA, AR, VS, CS, MS, LF, TP, XZ, WSO, SB, and SAD
contributed to the conceptualization of the research concept,
performing the experiments, formal analyses, and writing the
original draft. CL, UM, and CRG contributed to the
conceptualization of the research concept, study design,
supervision, reviewing and editing the original draft, and funding
acquisition. All authors read and approved the manuscript and agree
to be accountable for all aspects of the research in ensuring that
the accuracy or integrity of any part of the work are appropriately
investigated and resolved.
Ethics approval and consent for
publication
The UMMC Institutional Review Board approved the
study and all authors have given consent for publication. Written
informed consent was obtained from all of the patients.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2020. CA Cancer J Clin. 70:7–30. 2020. View Article : Google Scholar
|
|
2
|
Thim L: A new family of growth factor-like
peptides. ‘Trefoil’ disulphide loop structures as a common feature
in breast cancer associated peptide (pS2), pancreatic spasmolytic
polypeptide (PSP), and frog skin peptides (spasmolysins). FEBS
Lett. 250:85–90. 1989. View Article : Google Scholar
|
|
3
|
Madsen J, Nielsen O, Tornøe I, Thim L and
Holmskov U: Tissue localization of human trefoil factors 1, 2, and
3. J Histochem Cytochem. 55:505–513. 2007. View Article : Google Scholar
|
|
4
|
Podolsky DK, Lynch-Devaney K, Stow JL,
Oates P, Murgue B, DeBeaumont M, Sands BE and Mahida YR:
Identification of human intestinal trefoil factor. Goblet
cell-specific expression of a peptide targeted for apical
secretion. J Biol Chem. 268:6694–6702. 1993.
|
|
5
|
Xiao P, Ling H, Lan G, Liu J, Hu H and
Yang R: Trefoil factors: Gastrointestinal-Specific proteins
associated with gastric cancer. Clin Chim Acta. 450:127–134. 2015.
View Article : Google Scholar
|
|
6
|
Taupin D and Podolsky DK: Trefoil factors:
Initiators of mucosal healing. Nat Rev Mol Cell Biol. 4:721–732.
2003. View
Article : Google Scholar
|
|
7
|
Hernandez C, Santamatilde E, McCreath KJ,
Cervera AM, Diez I, Ortiz-Masia D, Martínez N, Calatayud S,
Esplugues JV and Barrachina MD: Induction of trefoil factor (TFF)1,
TFF2 and TFF3 by hypoxia is mediated by hypoxia inducible factor-1:
Implications for gastric mucosal healing. Br J Pharmacol.
156:262–272. 2009. View Article : Google Scholar
|
|
8
|
Samson MH: Quantitative measurements of
trefoil factor family peptides: Possibilities and pitfalls. Scand J
Clin Lab Invest. 73:193–202. 2013. View Article : Google Scholar
|
|
9
|
Aihara E, Engevik KA and Montrose MH:
Trefoil factor peptides and gastrointestinal function. Annu Rev
Physiol. 79:357–380. 2017. View Article : Google Scholar
|
|
10
|
Wong WM, Poulsom R and Wright NA: Trefoil
peptides. Gut. 44:890–895. 1999. View Article : Google Scholar
|
|
11
|
Babyatsky M, Lin J, Yio X, Chen A, Zhang
JY, Zheng Y, Twyman C, Bao X, Schwartz M, Thung S, et al: Trefoil
factor-3 expression in human colon cancer liver metastasis. Clin
Exp Metastasis. 26:143–151. 2009. View Article : Google Scholar
|
|
12
|
Garraway IP, Seligson D, Said J, Horvath S
and Reiter RE: Trefoil factor 3 is overexpressed in human prostate
cancer. Prostate. 61:209–214. 2004. View Article : Google Scholar
|
|
13
|
Kannan N, Kang J, Kong X, Tang J, Perry
JK, Mohankumar KM, Miller LD, Liu ET, Mertani HC, Zhu T, et al:
Trefoil factor 3 is oncogenic and mediates anti-estrogen resistance
in human mammary carcinoma. Neoplasia. 12:1041–1053. 2010.
View Article : Google Scholar
|
|
14
|
Kirikoshi H and Katoh M: Expression of
TFF1, TFF2 and TFF3 in gastric cancer. Int J Oncol. 21:655–659.
2002.
|
|
15
|
Kim WG, Kim JY and Park DY: Simple
classifiers for molecular subtypes of colorectal cancer. Arab J
Gastroenterol. 18:191–200. 2017. View Article : Google Scholar
|
|
16
|
Jahan R, Shah A, Kisling SG, Macha MA,
Thayer S, Batra SK and Kaur S: Odyssey of trefoil factors in
cancer: Diagnostic and therapeutic implications. Biochim Biophys
Acta Rev Cancer. 1873:1883622020. View Article : Google Scholar
|
|
17
|
Yusup A, Huji B, Fang C, Wang F, Dadihan
T, Wang HJ and Upur H: Expression of trefoil factors and TWIST1 in
colorectal cancer and their correlation with metastatic potential
and prognosis. World J Gastroenterol. 23:110–120. 2017. View Article : Google Scholar
|
|
18
|
Li Q, Wang K, Su C and Fang J: Serum
trefoil factor 3 as a protein biomarker for the diagnosis of
colorectal cancer. Technol Cancer Res Treat. 16:440–445. 2017.
View Article : Google Scholar
|
|
19
|
Huang YG, Li YF, Wang LP and Zhang Y:
Aberrant expression of trefoil factor 3 is associated with
colorectal carcinoma metastasis. J Cancer Res Ther. 9:376–380.
2013. View Article : Google Scholar
|
|
20
|
Chandrashekar DS, Bashel B, Balasubramanya
SA, Creighton CJ, Ponce-Rodriguez I, Chakravarthi B and Varambally
S: UALCAN: A portal for facilitating tumor subgroup gene expression
and survival analyses. Neoplasia. 19:649–658. 2017. View Article : Google Scholar
|
|
21
|
Chen F, Chandrashekar DS, Varambally S and
Creighton CJ: Pan-Cancer molecular subtypes revealed by
mass-spectrometry-based proteomic characterization of more than 500
human cancers. Nat Commun. 10:56792019. View Article : Google Scholar
|
|
22
|
Mashimo H, Wu DC, Podolsky DK and Fishman
MC: Impaired defense of intestinal mucosa in mice lacking
intestinal trefoil factor. Science. 274:262–265. 1996. View Article : Google Scholar
|
|
23
|
Farrell JJ, Taupin D, Koh TJ, Chen D, Zhao
CM, Podolsky DK and Wang TC: TFF2/SP-deficient mice show decreased
gastric proliferation, increased acid secretion, and increased
susceptibility to NSAID injury. J Clin Invest. 1091:193–204. 2002.
View Article : Google Scholar
|
|
24
|
Carrasco R, Pera M, May FE, Westley BR,
Martinez A and Morales L: Trefoil factor family peptide 3 prevents
the development and promotes healing of ischemia-reperfusion injury
in weanling rats. J Pediatr Surg. 39:1693–1700. 2004. View Article : Google Scholar
|
|
25
|
Serwin NM, Wisniewska M, Jesionowska A,
Skwirczyńska E, Marcinowska Z and Dołęgowska B: Serum levels of 12
renal function and injury markers in patients with
glomerulonephritis. Pol Arch Med Wewn. 126:483–493. 2016.
|
|
26
|
Schulze U, Hampel U, Sel S, Goecke TW,
Thäle V, Garreis F and Paulsen F: Fresh and cryopreserved amniotic
membrane secrete the trefoil factor family peptide 3 that is well
known to promote wound healing. Histochem Cell Biol. 138:243–250.
2012. View Article : Google Scholar
|
|
27
|
Taupin DR, Kinoshita K and Podolsky DK:
Intestinal trefoil factor confers colonic epithelial resistance to
apoptosis. Proc Natl Acad Sci USA. 97:799–804. 2000. View Article : Google Scholar
|
|
28
|
Kinoshita K, Taupin DR, Itoh H and
Podolsky DK: Distinct pathways of cell migration and antiapoptotic
response to epithelial injury: Structure-function analysis of human
intestinal trefoil factor. Mol Cell Biol. 20:4680–4690. 2000.
View Article : Google Scholar
|
|
29
|
Li XL, Zhou J, Chen ZR and Chng WJ: P53
mutations in colorectal cancer-molecular pathogenesis and
pharmacological reactivation. World J Gastroenterol. 21:84–93.
2015. View Article : Google Scholar
|
|
30
|
Manne U, Myers RB, Moron C, Poczatek RB,
Dillard S, Weiss H, Brown D, Srivastava S and Grizzle WE:
Prognostic significance of bcl-2 expression and p53 nuclear
accumulation in colorectal adenocarcinoma. Int J Cancer.
74:346–358. 1997. View Article : Google Scholar
|
|
31
|
Busch M, Klein S, Große-Kreul J, Scheiner
O, Metz K, Stephan H and Dünker N: P53, miR-34a and EMP1-newly
identified targets of TFF3 signaling in Y79 retinoblastoma cells.
Int J Mol Sci. 20:41292019. View Article : Google Scholar
|
|
32
|
Goswami CP and Nakshatri H: PROGgeneV2:
Enhancements on the existing database. BMC Cancer. 14:9702014.
View Article : Google Scholar
|
|
33
|
Morito K, Nakamura J, Kitajima Y, Kai K,
Tanaka T, Kubo H, Miyake S and Noshiro H: The value of trefoil
factor 3 expression in predicting the longterm outcome and early
recurrence of colorectal cancer. Int J Oncol. 46:563–568. 2015.
View Article : Google Scholar
|
|
34
|
Scholven J, Taras D, Sharbati S, Schön J,
Gabler C, Huber O, zum Büschenfelde DM, Blin N and Einspanier R:
Intestinal expression of TFF and related genes during postnatal
development in a piglet probiotic trial. Cell Physiol Biochem.
23:143–156. 2009. View Article : Google Scholar
|