Introduction
Liver cancer is one of the most prevalent types of
cancer worldwide, and was the seventh most frequently diagnosed
cancer and the second leading cause of cancer-associated deaths in
2018 (1), with 841,000 new cases and
781,000 relevant deaths, accounting for 4.7% and 8.2% of all cancer
cases and deaths worldwide, respectively (2). Although liver resection has curative
potential for patients with early-staged liver cancer, the majority
of patients are diagnosed with intermediate-to-advanced staged
cancer due to the often asymptomatic onset of the disease (3). For patients with unresectable liver
cancer, prolonging the survival and maintaining the quality of life
is paramount. Transcatheter arterial chemoembolization (TACE) is a
locoregional therapy that not only blocks the tumor blood supply
through the use of an embolization agent but also infiltrates the
tumor tissue resulting in a high concentration of the
chemotherapeutic agent specifically within the tumor tissue. TACE
is widely utilized to treat patients with unresectable liver cancer
due to its favorable efficacy and tolerable side effects (4). Traditionally, the drug carriers in
conventional TACE (cTACE) consist of lipiodol, a gelatin sponge,
particles and other compounds, which fail to stably release
chemotherapeutic agents and embolize target arteries accurately and
completely (5). During the past
decade, microspheres, a novel drug carrier, have been developed and
have become increasingly popular with regard to TACE (6). Compared with conventional drug carriers,
microspheres can be used to achieve more sustained drug release,
which prolongs the antitumor efficacy of the chemotherapeutic
agents (7,8). In addition, microspheres block feeding
arteries more accurately and completely than those of conventional
drug carriers, leading to improved tumor necrosis effects and
reduced chemotherapeutic side effects (9). Due to the advantages of microspheres
over conventional drug carriers, microspheres are being
increasingly used in TACE.
In recent years, several microsphere products have
become commercially available in China, including CalliSphere beads
(CBs) (Jiangsu Hengrui Medicine Co. Ltd.), DC beads (BTG) and
HepaSphere (Merit Medical) (8,10,11). Among these, CBs are the first
microsphere product independently developed by a local Chinese
pharmaceutical company (12). CBs are
made of polyvinyl alcohol, which is hydrophilic, nontoxic,
biocompatible and nonabsorbable (12,13).
Clinical studies have revealed favorable efficiency and safety of
CBs in treating patients with liver cancer (14,15).
Considering that China has a large number of patients who suffer
from liver cancer, accounting for ~50% of the estimated number of
liver cancer patients worldwide, CBs may be used to promising
effect in China.
Arsenic trioxide (ATO), an inorganic compound which
is known for its hypertoxicity in the ancient world, has been
approved for treating acute promyelocytic leukemia (APL) by the
American Food and Drug Administration in 2000 due to its anti-APL
properties (16). Previously, ATO was
demonstrated to exhibit effects on stem cell and metastasis in HCC.
For example, a noteworthy study revealed the potent antitumor
effects of the combination of ATO and sorafenib through a
TRAIL-dependent pathway in Huh7 and freshly-isolated HCC cells
(17). Another study revealed that
low a dose of ATO was sufficient to suppress vasculogenic mimicry
in hepatoblastoma without cell apoptosis (18). Furthermore, ATO has been demonstrated
to reduce liver cancer stem cells and metastasis by targeting a
serum response factor/minichromosome maintenance protein 7 complex
(19). Recently, ATO was also
revealed to be efficient for treatment of patients with liver
cancer and is used as a palliative treatment in patients with
advanced liver cancer in China (20).
Considering that systemic chemotherapy of ATO can result in severe
adverse events (such as convulsions, cardiovascular problems and
kidney failure), in the present study, it was hypothesized that
ATO-eluting microspheres for TACE may be a promising strategy to
maximize the antitumor activity of ATO while minimizing the
systemic toxicity (21). To the best
of our knowledge, there are no studies examining the use of
ATO-eluting microspheres and assessing their antitumor efficacy.
Therefore, the aim of the present study was to investigate the ATO
loading and releasing efficiencies of CBs, and to further explore
the anticancer activity of ATO-eluting CBs in liver cancer cells
and its pharmacokinetics, treatment efficacy as well as safety in a
rabbit model of liver cancer.
Materials and methods
Study design
The present was divided into three parts. In the
first part, the ATO loading and releasing efficiencies of CBs were
evaluated in vitro. In the second part, comparisons of cell
viability, invasion, apoptosis and expression of vascular
endothelial growth factor (VEGF) and matrix metalloproteinase 9
(MMP-9) in liver cancer cell lines (HepG2 and MHCC97H) were
performed by administrating liver cancer cells with ATO-eluting CBs
(CBATO group) or ATO solution (ATO group). In the third part,
comparisons of ATO concentrations in plasma, tumor tissue and
normal liver parenchyma, as well as macroscopic findings of liver
tissue were performed between the CBATO group and the cTACE group
in an animal model of liver cancer.
Preparation of CB and ATO
solution
CBs (100–300 µm) were purchased from Jiangsu Hengrui
Medicine Co., Ltd., and ATO was purchased from Shanghai LoyMed
Pharma Co., Ltd. The ATO solution (10 mg/ml) was prepared as
follows: 60 mg ATO powder was added to 6 ml glucose solution (5%)
and then mixed vigorously.
Evaluation of ATO loading efficiency
in CBs
A total of 1 g CB (without water) was added to the 6
ml ATO solution (10 mg/ml), and the mixture was vibrated carefully
for 1 sec; 50 µl solution was removed from the mixture every 10 min
for 60 min after vibration and centrifuged at 6660 × g for 5 min.
Subsequently, 2 ml solution was obtained after the upper layer was
diluted 100-fold, and the arsenic concentration was determined
using the silver diethyldithiocarbamate method, according to a
previously published study (22)
followed by spectrophotometry (y=0.0713×-0.013,
R2=0.9985; n=3), and the concentration of ATO was
calculated. The amount of ATO in CBs was equivalent to the total
amount subtracted from the solution. The experiment was replicated
3 times and the mean value and standard deviation of ATO
concentrations were measured, and an ATO loading curve was
drawn.
Evaluation of ATO releasing efficiency
in CBs
ATO-eluting CBs were placed on a flow cell of the
Pharmacopeia flow-through apparatus 4 (CE6; Sotax), the pump flow
rate was set at 5 ml/min and the releasing medium was 50 ml PBS
(Gibco; Thermo Fisher Scientific, Inc.). From the releasing medium,
4 ml PBS was obtained after 30 min, 1, 2, 4, 8, 12, 24 and 48 h
after the start of release, and the ATO concentration was
determined as aforementioned. The experiment was replicated 3
times, the mean value and standard deviation of ATO concentrations
were measured, and the ATO releasing curve was drawn.
Cell culture
Human liver cancer cell lines, HepG2 and MHCC97H,
(donated by Wuhan Union Hospital of Huazhong University of Science
and Technology) were cultured in DMEM (Invitrogen; Thermo Fisher
Scientific, Inc.) supplemented with 10% FBS (Gibco; Thermo Fisher
Scientific, Inc.), 100 U/ml and 100 µg/ml streptomycin (both from
North China Pharmaceuticals Co., Ltd.) at 37°C in a humidified
incubator with 5% CO2. In vitro experiments were performed
under sterile conditions.
Assessment of cell viability
Cell viability was performed using a Cell Counting
Kit-8 (CCK-8) assay (Dojindo Molecular Technologies, Inc.). HepG2
cells (authenticated by STR profiling) and MHCC97H cells were
seeded into a 96-well plate (2×104 cells/well), and 200
µl medium containing 0, 5, 10, 15 or 20 ng/ml (1 ng/ml ATO, ~0.5
µmol/l ATO) ATO-eluting CBs or ATO solution were added to the
wells. Subsequently, CCK-8 reagent was added to each well after 0,
12, 24, 48 or 72 h, and the plate was incubated for a further 4 h
at 37°C. The absorbance was measured at 450 nm with an automatic
microplate reader.
Assessment of cell invasion
Cell invasion was determined using a Transwell assay
(Corning, Inc.). Briefly, 2×104 cells (100 µl) in 0.5%
BSA-medium was added to the upper chamber of the Transwell insert
(A 24-well cell culture plate; a polycarbonate filter membrane with
a diameter of 6.5 mm was at the bottom of the chamber; micropore
diameter of 8.0 µm) which had been pre-coated with 50 µl Matrigel
(BD Biosciences), and 600 µl medium containing 10% FBS was added to
the lower chamber. After incubation at 37°C for 12 h, ATO-eluting
CBs or ATO solution were added to the medium to a final ATO
concentration of 0, 5, 10, 15 or 20 ng/ml, and the cells were
incubated for a further 48 h. Subsequently, the cells on the upper
surface of the filter were removed by wiping, and the cells which
had adhered to the undersurface of the filter were fixed in 4% of
paraformaldehyde for 30 min at 4°C, stained with 0.5% crystal
violet (Sigma-Aldrich; Merck KGaA) at 23°C for 10 min and imaged
using a light microscope; 3 fields (×100) of view were randomly
selected for cell counting, and the mean value of the cell count
was calculated.
Assessment of apoptosis
Cell apoptosis was analyzed using an Annexin
V/propidium iodide (AV/PI) assay. Briefly, liver cancer cells were
seeded in a 6-well plate (5×105 cells/well) and then
incubated (at 37°C, 5% CO2) for 24 h. Subsequently, 2 ml medium
containing 0, 5, 10, 15 or 20 ng/ml ATO-eluting CBs or ATO solution
were added to the wells, and incubated (at 37°C, 5% CO2) for a
further 24 or 48 h. Following incubation, cells were resuspended in
400 µl binding buffer, and 5 µl AV-FITC (BD Biosciences) and 5 µl
PI (BD Biosciences) was added. The mixture was incubated (~2-8°C in
the dark) for 15 min and the proportion of apoptotic cells was
analyzed using a flow cytometer and software (FlowJo 7.6.1 BD;
FlowJo, LLC).
Reverse transcription-quantitative
(RT-q) PCR
Liver cancer cells were seeded in a 6-well plate
(5×105 cells/well), and 2 ml medium containing 0, 5, 10,
15 or 20 ng/ml ATO-eluting CBs or ATO solution were added to the
wells, and incubated for 24 or 48 h. Following treatment, total RNA
was extracted from cells using TRIzol® reagent
(Invitrogen; Thermo Fisher Scientific, Inc.) and
reverse-transcribed to cDNA using PrimeScript™ RT reagent kit
(Takara Bio, Inc.). qPCR was performed using a QuantiNova
SYBR-Green PCR kit (Qiagen GmbH) and the mRNA expression levels of
VEGF and MMP-9 were determined using the 2−ΔΔCq method
(23). GAPDH was used as an internal
reference. The sequences of the primers used were: VEGF forward,
5′-TGTCTAATGCCCTGGAGCCT-3′ and reverse,
5′-GCTTGTCACATCTGCAAGTACG-3′; MMP9 forward,
5′-CGGTTTGGAAACGCAGATGG-3′ and reverse, 5′-TGGGTGTAGAGTCTCTCGCT-3′;
and GADPH forward, 5′-TGGAAGGACTCATGACCACA-3′ and reverse,
5′-TTCAGCTCAGGGATGACCTT-3′.
Western blotting
Liver cancer cells were seeded in a 6-well plate
(5×105 cells/well), and 2 ml medium containing 0, 5, 10,
15 or 20 ng/ml ATO-eluting CBs or ATO solution were added to the
wells, and incubated for 24 or 48 h. Total protein was extracted
using RIPA lysis and extraction buffer (Thermo Fisher Scientific,
Inc.), and the concentration was determined using a BCA kit (Thermo
Fisher Scientific, Inc.). Protein samples (40 µg) were loaded on an
8% SDS-gel, resolved using SDS-PAGE and transferred to
polyvinylidene fluoride membranes (EMD Millipore). After blocking
(the PVDF membranes were immersed and blocked with the TBST sealant
containing 5% skimmed milk powder and stored at 37°C for 2 h), the
membranes were incubated overnight at 4°C with anti-VEGF (1:1,000;
product code ab32152; Abcam) or anti-MMP-9 (1:1,000; product code
ab76003; Abcam) primary antibodies. The dilutions for both the
antibodies were performed using 5% BSA. Subsequently, the membranes
were incubated with horseradish peroxidase-conjugated secondary
antibody goat anti-rabbit IgG-HRP (1:5,000; product code ab6721;
Abcam) at 37°C for 2 h. Signals were visualized using Pierce
enhanced chemiluminescence Western Blotting Substrate (Thermo
Fisher Scientific, Inc.). Anti-β-actin (1:5,000; product code
ab227387; Abcam) was used as the loading control. The ImageJ
software (1.8.0; National Institutes of Health) was used for
densitometric analysis.
Preparation of animal models with VX2
liver cancer
All the procedures on animals were approved by the
Institutional Animal Care and Use Committee at our institution
(Ethics and Scientific Trial Committee of the First Affiliated
Hospital of Zhengzhou University), and the experiments were
performed in accordance with institutional guidelines. Adult male
New Zealand white rabbits (water ad libitum and regular diets)
(n=100; weighing 3.5–4.1 kg) raised at a temperature of ~20-27°C, a
humidity greater than 60%, an airflow value not exceeding 0.2
m/sec, a ventilation frequency of ~10–20 times/h, a 12-h light/dark
cycle and an indoor noise controlled within 60 dB, were obtained
from Henan Experimental Animal Center and active VX2 tumors were
implanted into these rabbits under aseptic conditions. In this
study, all VX2 models were transplanted with a single tumor. Then,
a CT scan was performed 15 days after surgery in the CBATO, CB,
cTACE and control groups. The general procedure of implantation was
as follows: Rabbits were anesthetized with a mixture of
acepromazine [2.5 mg/kg, intramuscularly (i.m.); Sage Chemical Co.,
Ltd.] and ketamine hydrochloride (44 mg/kg, i.m.; Jiuxu
Pharmaceutical Co., Ltd.), and the anesthetization was maintained
using sodium pentobarbital. Subsequently, the abdomen was shaved
and prepared for aseptic procedures, and the left lateral lobe of
the liver was exposed after a small incision was made. The fresh
VX2 tumor was harvested from carriers, minced and inoculated into
the liver. Finally, the abdomen was closed in layers to complete
the operation. After the surgery, the rabbits were fed for 14 days
to ensure the growth of the VX2 tumors, and then contrast-enhanced
computed tomography was used to examine the location and size of
the tumor in each rabbit. The eligible rabbits were selected for
further experiments. The study was approved from The Scientific
Research and Clinical Trial Ethics Committee of the First
Affiliated Hospital of Zhengzhou University (No. Scientific
research-2017-03).
Treatments
A total of 24 rabbit models were deemed suitable for
further use, and were randomly divided into the CBATO (n=12) and
cTACE group (n=12). The CBATO group received TACE using ATO-eluting
CBs (100–300 µm; Jiangsu Hengrui Medicine Co. Ltd.; 0.5 mg/kg ATO),
and the cTACE group received TACE using ATO/lipiodol emulsion (0.5
mg/kg ATO). The general TACE procedure was as follows: Rabbits were
anesthetized as aforementioned, then the right femoral artery was
exposed, and a 4-F sheath (Cook, Inc.) was placed into the artery.
Subsequently, a 4-F catheter (Cook, Inc.) was inserted into the
hepatic artery to identify its anatomy, and a 2.7-F coaxial
microcatheter (Cook, Inc.) was catheterized into the left hepatic
artery; the ATO-eluting CBs or ATO/lipiodol emulsion was injected
into the target artery. After treatment, the catheters were
removed, the artery was ligated, and the rabbits were fed for
another 14 days.
Determination of ATO concentration in
plasma
Whole blood was obtained after 0.17, 0.33, 0.67, 1,
3, 6, 12, 24 and 72 h after surgery, and the ATO concentration was
determined by liquid chromatography-mass spectrometry.
Gross observation of the liver, histopathological
examination of the tumor tissue and determination of ATO
concentration in tissues. From both groups, 4 rabbits were
euthanized (under deep anesthesia by slow injection of a lethal
dose (100 mg/kg of body weight of sodium pentobarbital
intravenously) after 1, 7 or 14 days following the surgery, and
gross observation of the liver was performed after 1 or 7 days
following the surgery. Subsequently, tumor tissue samples from all
rabbits were obtained and dissected into two equal halves. One half
was fixed with formalin at 23°C for 24 h, mounted on slices and
stained with hematoxylin and eosin at 23°C for 5 min, and
histopathologically examined. The other half was used to determine
the ATO concentrations using liquid chromatography-mass
spectrometry. Additionally, the normal liver parenchyma was also
obtained after euthanasia and the ATO concentration was determined
using liquid chromatography-mass spectrometry as well.
Euthanasia of the experimental
rabbits
According to the American Veterinary Medical
Association Guidelines for the Euthanasia of Animals: 2013 Edition
(24), in order to reduce the pain of
the experimental rabbits, the experimental animals received ear
marginal vein rapid injection of sodium pentobarbital (100 mg/kg),
for euthanization; after injection of the drug, the vital signs of
the experimental rabbits were checked every 2 min until no
heartbeat, no spontaneous breathing for 2–3 min or no blink reflex
was observed. In order to decrease the pain and stress, all animals
were euthanized under deep anesthesia by slow injection of a lethal
dose of sodium pentobarbital intravenously, and provided with soft
music to terminate their lives in a painless environment. After
euthanasia, the rabbits were wrapped and placed on ice temporarily
and then harmless treatment was performed. The whole euthanasia
process performed was not observed by other experimental rabbits
(24).
Statistical analysis
Data are presented as the mean ± standard deviation.
Comparisons between two groups were determined using an unpaired
Students t-test, and comparisons between different concentrations
within a group were performed using a one-way ANOVA followed by a
post hoc Tukeys test. Statistical analysis was performed in SPSS
version 13.0 (SPSS, Inc.), and GraphPad Prism version 6.0 (GraphPad
Software, Inc.) was used to plot the graphs. P<0.05 was
considered to indicate a statistically significant difference.
Results
ATO loading and releasing efficiencies
of CBs
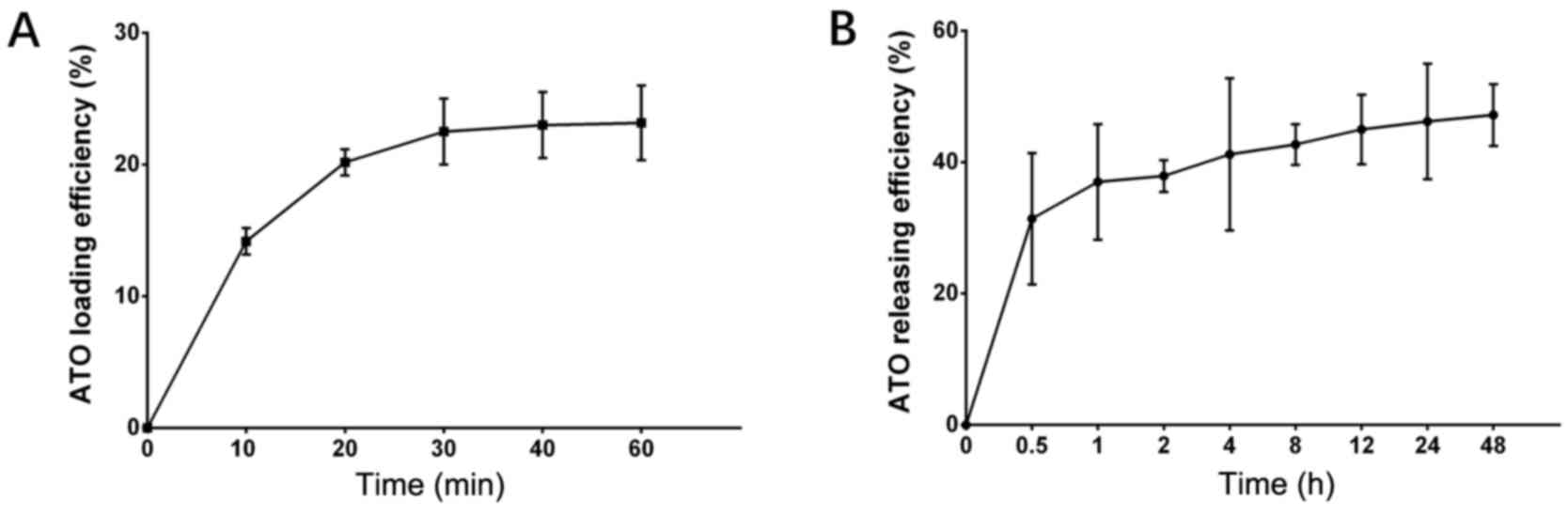
The amount of ATO loaded by CBs increased with time
within the first 40 min, and the optimal loading efficiency was
23.0±2.5% (Fig. 1A). In addition, the
ATO release curve revealed that CBs rapidly released substantial
ATO during the first 30 min (up to 31.40±10.0%), then slowly
released ATO within the latter 48 h (47.20±4.70%) (Fig. 1B). These data indicated that ATO
loading and releasing efficiencies of CBs were acceptable.
Comparison of cell viability between
the CBATO group and ATO group in liver cancer cells
To evaluate the anti-liver cancer activities of
ATO-eluting CBs, cell viability between the CBATO group and the ATO
group was compared. Cell viability was suppressed by ATO in a
dose-dependent manner both in the CBATO group (all P<0.05) and
ATO group (all P<0.05) at each time-point in HepG2 cells
(Fig. 2A-D) and in MHCC97H cells
(Fig. 2E-H). For comparison of cell
viability between the CBATO group and the ATO group, there was no
difference between the two groups after 24 h (P>0.05; Fig. 2A), 48 h (P>0.05; Fig. 2B) or 72 h (P>0.05; Fig. 2C) at each concentration, but cell
viability was decreased in the CBATO group after 96 h (P<0.05;
Fig. 2D) compared with the ATO group
at an ATO concentration of 20 ng/ml in the HepG2 cells. The cell
viability in MHCC97H cells was similar between the two groups after
24 h (P>0.05; Fig. 2E) and 48 h
(P>0.05; Fig. 2F) at each
concentration, whereas after 72 h (P<0.05; Fig. 2G) and 96 h (P<0.05; Fig. 2H), viability in the CBATO group was
reduced compared with the ATO group at an ATO concentration of 10
ng/ml. These data indicated that, to some extent, ATO-eluting CBs
suppressed the cell viability compared with ATO solution in liver
cancer cells.
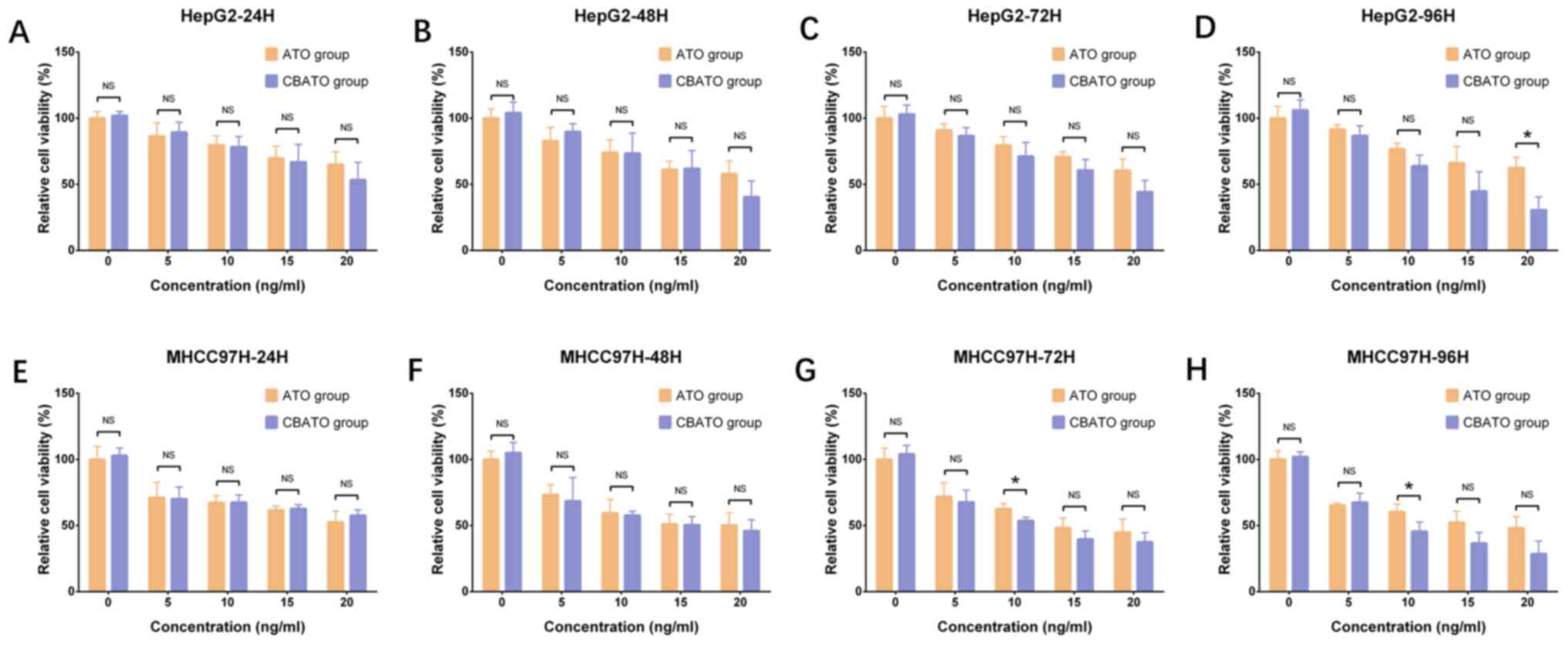 | Figure 2.Cell viability in the CBATO and ATO
groups in liver cancer cells. Cell viability in HepG2 cells at (A)
24, (B) 48, (C) 72 and (D) 96 h between the CBATO group and ATO
group. Cell viability in MHCC97H cells at (E) 24, (F) 48, (G) 72
and (H) 96 h between the CBATO and ATO groups. Comparison between
the CBATO and ATO groups was determined by t-test, P<0.05 was
considered as significant. *P<0.05. Comparison among various
concentrations within a group was determined by one-way ANOVA
followed by multiple comparisons test (Tukeys test), P<0.05 was
considered as significant, the statistical significance was not
presented in the figure but described in the Result section. ATO,
arsenic trioxide; CBs, CalliSphere beads; NS, no significance. |
Comparison of invasion between the
CBATO group and ATO group in liver cancer cells
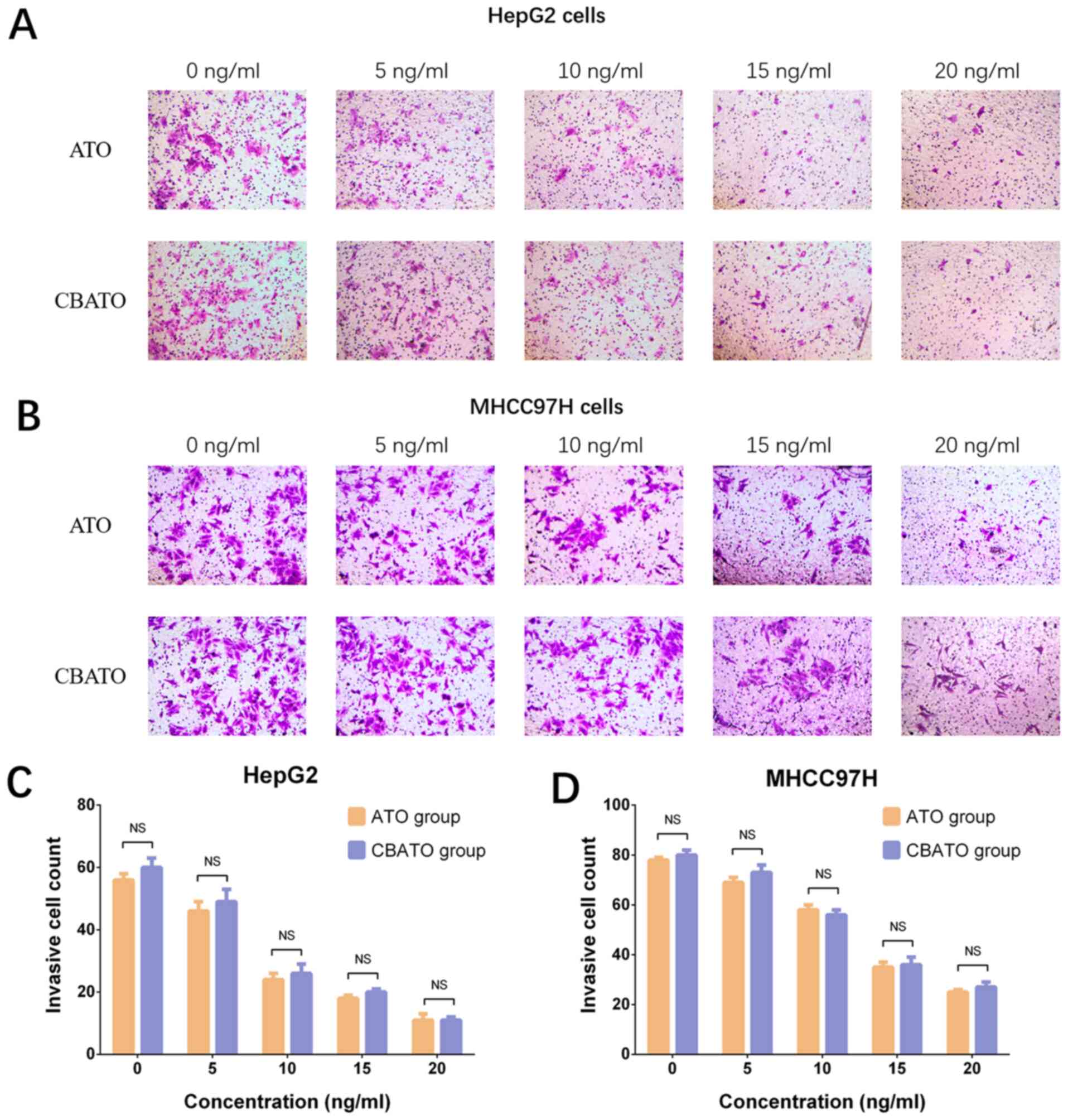
In HepG2 (Fig. 3A and
C) and MHCC97H (Fig. 3B and D)
cells, invasion was reduced by ATO in a dose-independent manner in
both the CBATO group (P<0.05) and the ATO group (P<0.05)
after 48 h compared with the control. There was no difference in
invasion between the CBATO group and the ATO group at each
concentration (all P>0.05; Fig. 3C and
D), indicating that ATO-eluting CBs did not affect cell
invasion compared with ATO solution in liver cancer cells.
Comparison of cell apoptosis between
the CBATO group and ATO group in liver cancer cells
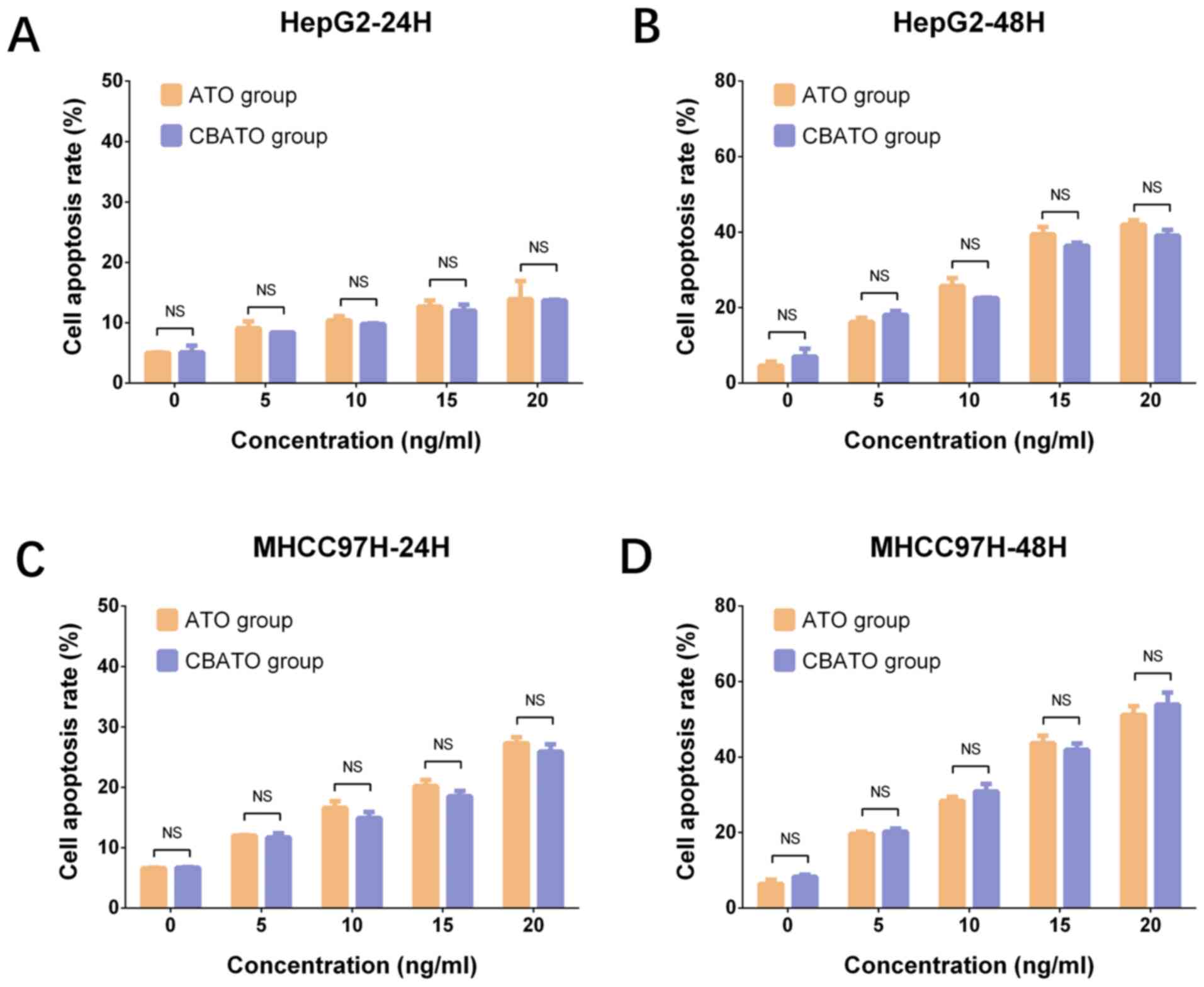
In HepG2 (all P<0.05; Fig. 4A and B) and MHCC97H (all P<0.05;
Fig. 4C and D) cells, the cell
apoptosis rate was increased by ATO in a dose-dependent manner both
in the CBATO group and the ATO group after 24 and 48 h. The
apoptosis rate was similar between the CBATO group and the ATO
group at each concentration after 24 h (all P>0.05) and 48 h
(all P>0.05), indicating that ATO-eluting CBs did not affect
cell apoptosis compared with ATO solution in liver cancer
cells.
Comparison of VEGF mRNA and protein
expression levels between the CBATO group and ATO group in liver
cancer cells
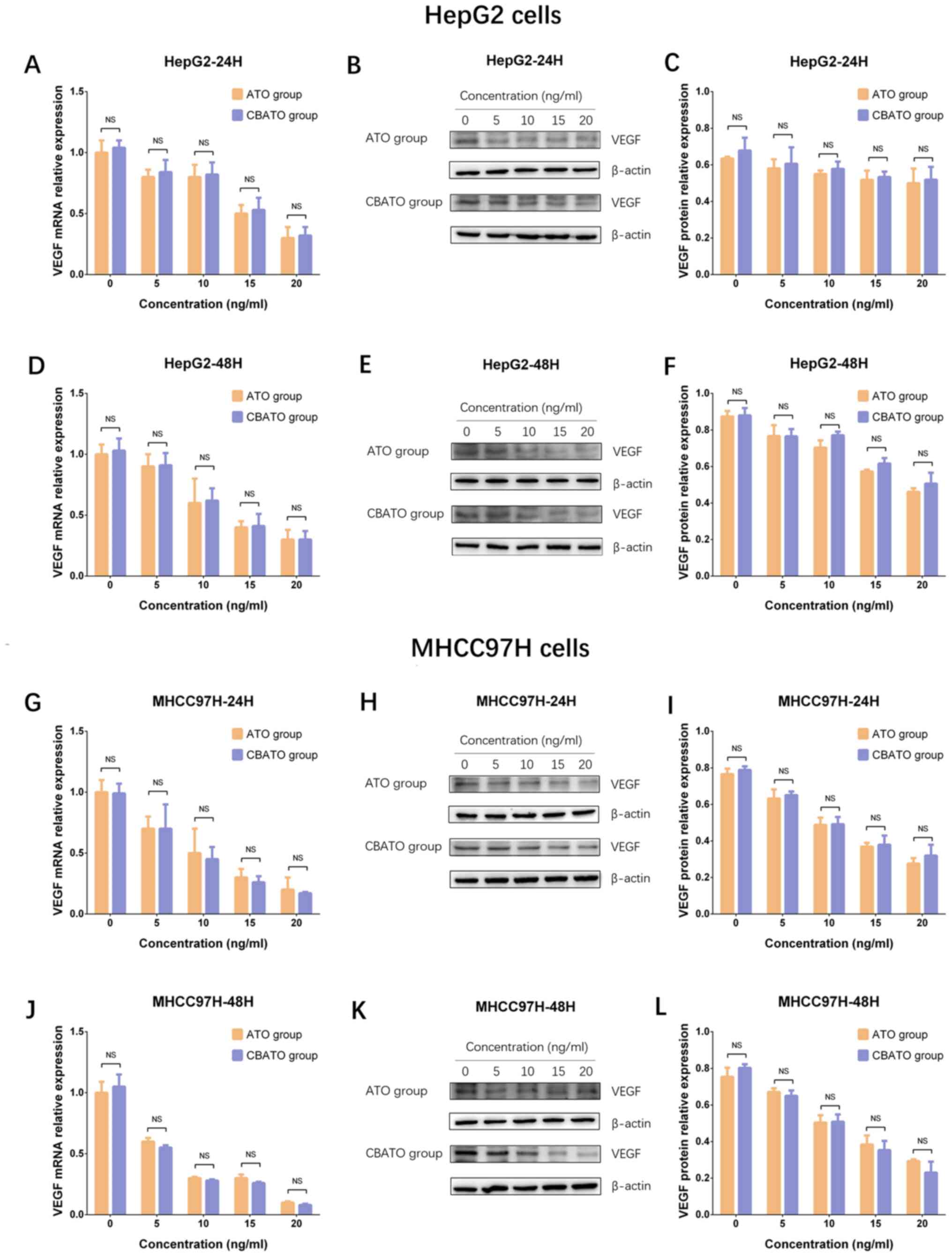
As VEGF is reported to serve an important role in
promoting growth and invasion of liver cancer cells, the VEGF mRNA
and protein expression levels between the CBATO group and TACE
group were measured to assess the impact of ATO-eluting CBs on
liver cancer cell growth and invasion (25,26). The
results revealed that VEGF mRNA and protein expression levels were
decreased by ATO in a dose-dependent manner in the CBATO group (all
P<0.05) and ATO group (all P<0.05) after 24 h (Fig. 5A-C) and 48 h (Fig. 5D-F) in HepG2 cells. There was no
difference in VEGF mRNA or protein expression levels between the
two groups after 24 or 48 h in HepG2 cells (all P>0.05). In
MHCC97H cells, VEGF expression also decreased in a similar manner
between the two groups compared with HepG2 cells (Fig. 5G-L). These data indicated that ATO
inhibited VEGF expression in liver cancer cells, while ATO-eluting
CBs had no impact on the inhibitory effect of ATO.
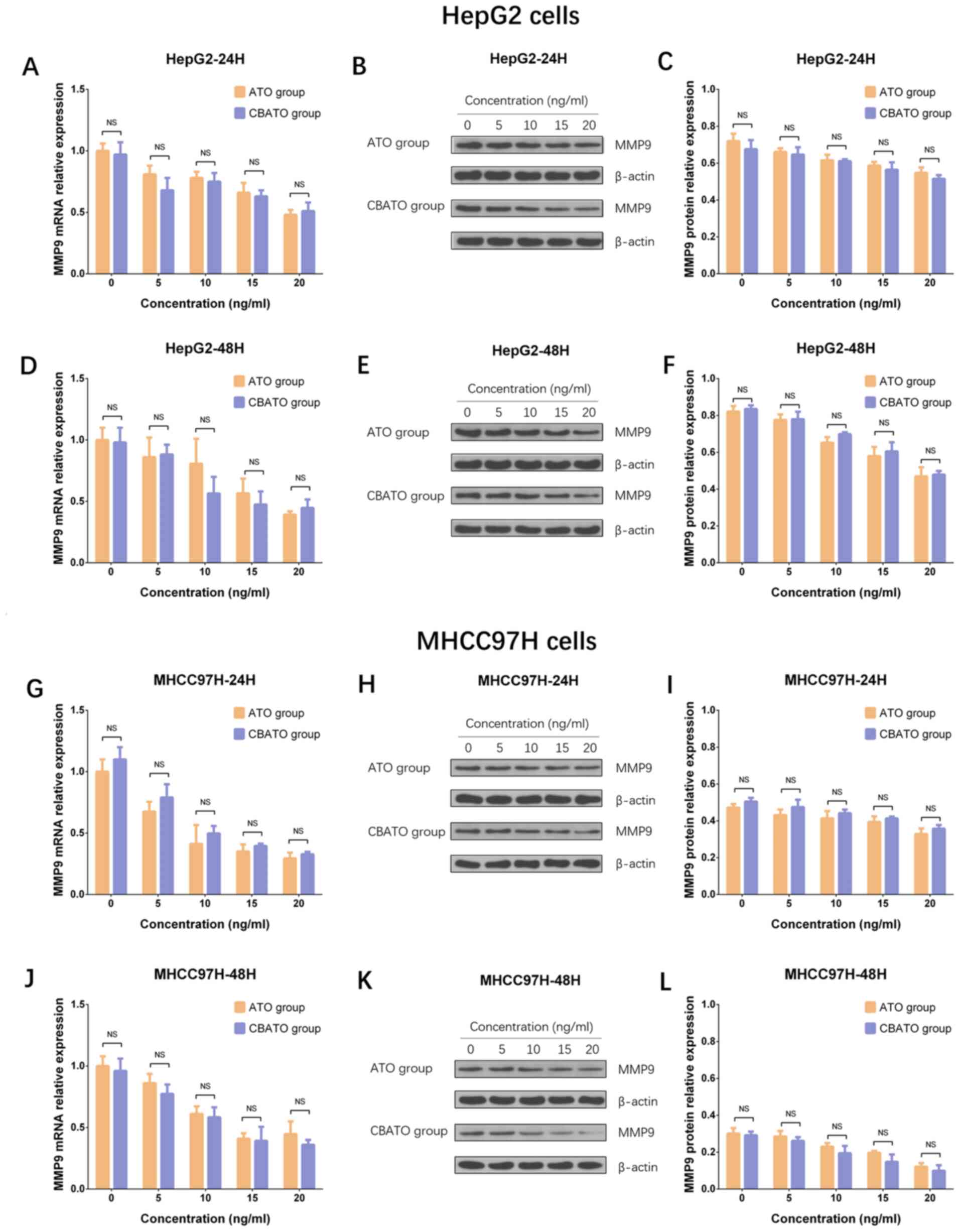
Comparison of MMP9 mRNA and protein
expression levels between the CBATO group and ATO group in liver
cancer cells
MMP9 expression levels were compared between the
CBATO group and the TACE group, and the results revealed that MMP9
mRNA and protein expression levels were decreased in an ATO
dose-dependent manner both in the CBATO group (all P<0.05) and
ATO group (all P<0.05) after 24 h (Fig. 6A-C) and 48 h (Fig. 6D-F) in HepG2 cells. However, there was
no difference in MMP9 mRNA or protein expression levels observed
between the two groups after 24 or 48 h in HepG2 cells (all
P>0.05). In MHCC97H cells, MMP9 expression was reduced in a
similar manner between the two groups compared with HepG2 cells
(Fig. 6G-L). These results indicated
that ATO suppressed MMP9 expression in liver cancer cells, while
ATO-eluting CBs did not affect the suppressive effect.
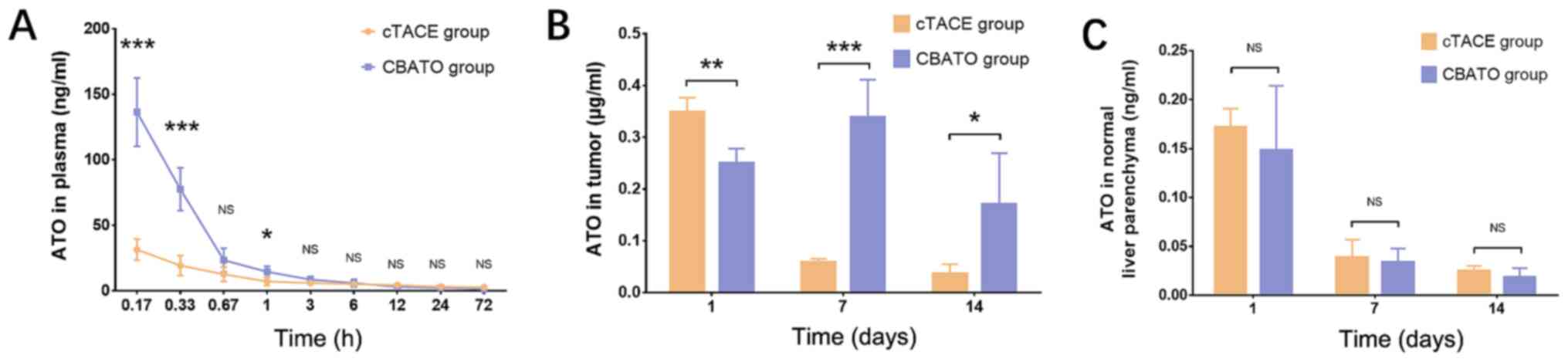
Comparison of ATO concentrations in
plasma, tumor tissue and normal liver parenchyma between the CBATO
group and cTACE group
ATO concentration in the plasma was higher in the
CBATO group compared with the cTACE group after 0.17 h
(P<0.001), 0.33 h (P<0.001) and 1 h (P<0.05) after surgery
(Fig. 7A). ATO concentration in the
tumor tissue was lower after 1 day (P<0.01) but higher after
days 7 (P<0.001) and 14 (P<0.05) in the CBATO group compared
with the cTACE group (Fig. 7B). The
ATO concentration in the normal liver parenchyma was similar
between the two groups after 1 (P>0.05), 7 (P>0.05) and 14
days (P>0.05) after the surgery (Fig.
7C). These data indicated that ATO-eluting CBs increased the
ATO plasma concentration whilst maximizing ATO tumor concentration
compared with the ATO/lipiodol emulsion when using TACE in a rabbit
model of liver cancer.
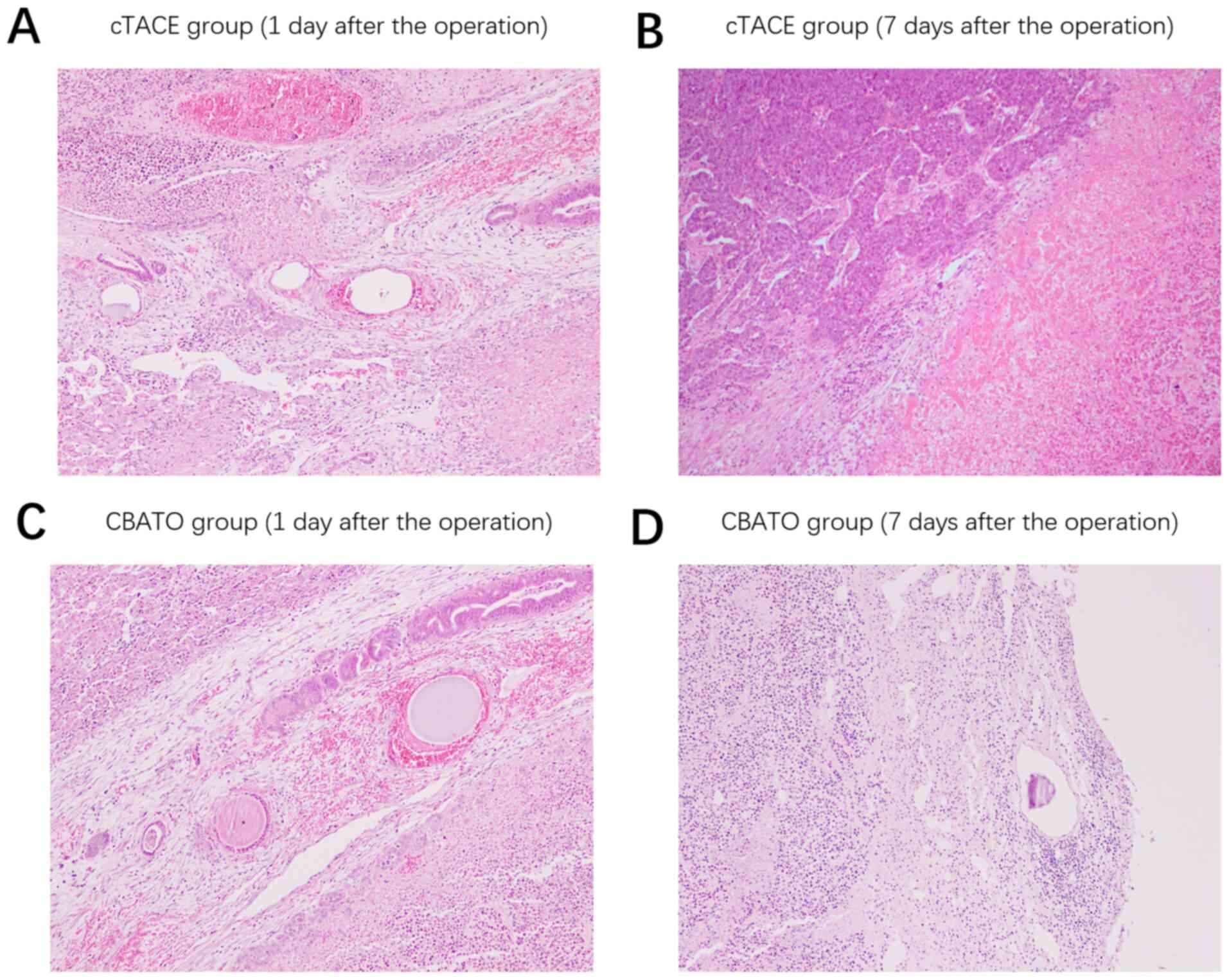
Comparison of histopathological
findings in tumor tissue between the CBATO group and cTACE
group
Following the surgery, on the 1st day,
thrombosis in the vascular lumen, a substantial number of
erythrocytes in the vascular wall and necrotic cancer cells in the
perivascular areas were observed both in the cTACE group (Fig. 8A) and the CBATO group (Fig. 8C). After the 7th day, there
was substantial increase in new cancer cells around the necrotic
cancer cells in the cTACE group (Fig.
8B); whereas there were a large number of necrotic cancer cells
and inflammatory cells in the perivascular areas in the CBATO
group, and no new cancer cells were observed (Fig. 8D), indicating that ATO-eluting CBs had
better treatment efficacy compared with ATO/lipiodol emulsion in
the TACE treatment of liver cancer.
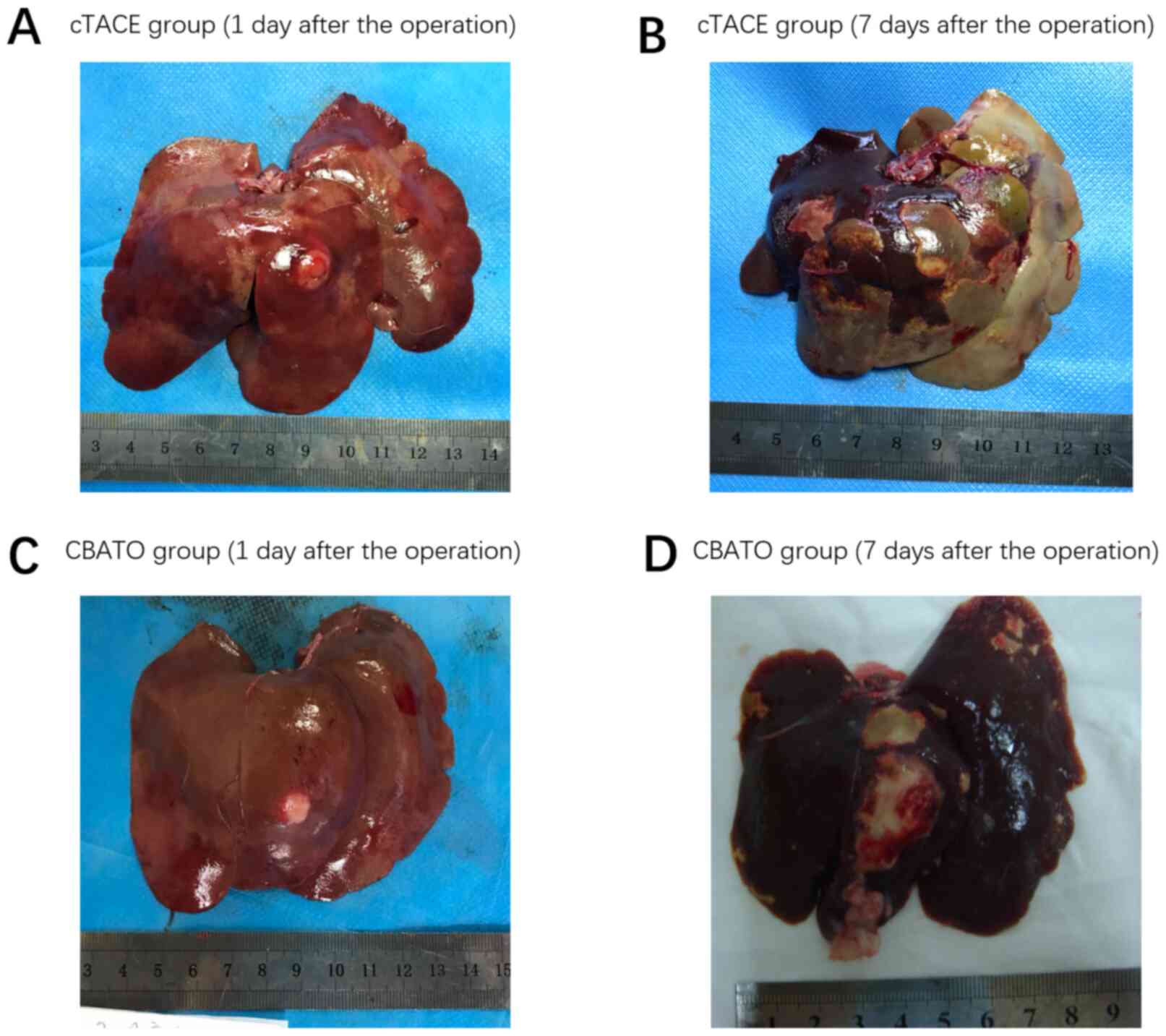
Comparison of macroscopic findings on
rabbit liver between the CBATO group and cTACE group
Following the surgery, on the 1st day, ATO-eluting
CBs (Fig. 9C) had a greater effect on
reduction of extensive necrosis and fibrosis radiologically
compared with cTACE (Fig. 9A). After
the 7th day, ATO-eluting CBs (Fig.
9D) had less effect on necrosis of tumor tissues and normal
liver parenchyma compared with cTACE (Fig. 9B), indicating that ATO-eluting CBs
reduced the toxicity on normal liver parenchyma compared with the
ATO/lipiodol emulsion. In this study, all VX2 models were
transplanted with a single tumor. Then, a CT scan was performed 15
days after surgery in the CBATO, CB, cTACE and control groups, and
the tumor maximum length diameter was 10.6±0.93, 11.0±0.78,
10.7±0.71 and 10.8±0.85 mm, respectively.
Discussion
Drug-eluting bead-TACE (DEB-TACE) has been
extensively used as an interventional therapy for patients with
unresectable liver cancer in recent years owing to its favorable
treatment efficacy and moderate adverse events (27). In DEB-TACE, microspheres are reported
to be superior to conventional drug carriers/embolization agents
(such as lipiodol). For instance, a meta-analysis revealed that
microspheres provided improved tumor response, survival and fewer
adverse events compared with lipiodol in the treatment of advanced
liver cancer patients (28). In
addition, several animal studies have demonstrated that
microspheres block tumor blood supply more completely and release
chemotherapeutic agents more consistently compared with lipiodol,
which results in a lower concentration of chemotherapeutic agents
in the plasma and normal tissues, and a higher concentration in
tumor tissue; this subsequently results in improved antitumoral
efficacy and reduced adverse events (7,8). Due to
the favorable efficacy and safety of microspheres such as CBs, they
are increasingly being used in DEB-TACE-mediated treatment of liver
cancer.
ATO is an effective chemotherapeutic agent which
exhibits powerful cytotoxicity in liver cancer cells via multiple
pathways. For example, a previous study revealed that ATO
stimulates cell cycle arrest in liver cancer cells (HepG2 and
SMMC7721 cell lines) via directly targeting a tumor suppressor gene
phosphatase and tensin homologue deleted on chromosome 10 (29). Additionally, ATO was revealed to
substantially increase reactive oxygen species (ROS) levels,
resulting in cell apoptosis in liver cancer cells (HepG2), and
suppressing the ROS levels reversed the apoptosis caused by ATO
(30). ATO was also revealed to
inhibit liver cancer tumorigenesis via suppression of VEGF and
metalloprotease expression (31–33). These
studies confirm the favorable anti-liver cancer properties of ATO.
However, the clinical application of ATO in treating liver cancer
patients has been strictly restricted due to its severe systemic
toxicity. In view that DEB-TACE reduces the circulating
concentration while increasing the intratumoral concentration of
chemotherapeutic drugs, it is hypothesized that ATO-eluting
microspheres may enhance the efficiency and tolerance of ATO.
However, information concerning the feasibility, treatment efficacy
and safety of ATO-eluting microspheres in DEB-TACE treatment of
liver cancer is limited.
In the present study, the in vitro ATO
loading and releasing efficiencies of CBs (100–300 µm) was
evaluated, and it was revealed that ATO was loaded by CBs in a
sustainable manner with an optimal loading efficiency of 23.0±2.5%,
which was relatively lower compared with two previous studies. In a
previous study, both doxorubicin and irinotecan achieved loading
within 40 min using DC beads (500–700 µm) and HepaSphere (400–600
µm) (34). In another study, >99%
of doxorubicin was loaded within 1 h using DC beads (100- 300 µm),
LifePearl (200 µm), HepaSphere (30–60 µm) and Tandem (100 µm)
(35). Possible reasons for the
discrepancy may be: i) The previous studies utilized doxorubicin or
irinotecan as a loading agent, which may form strong ionic
interaction with microspheres. The interaction between ATO and
microspheres may be weaker compared with the interaction between
doxorubicin or irinotecan and microspheres, thereby resulting in a
lower loading efficiency. ii) Microspheres are made of different
materials (such as sulfonate-modified polyvinyl alcohol or sodium
acrylate-modified polyvinyl alcohol), which may influence the
interaction between ATO and microspheres, as well. iii) Different
solutions (such as saline and deionized water) may also affect the
loading efficiency. In the present study, it was observed that CBs
released ATO in a rapid manner within the first 30 min
(31.40±10.0%) then released ATO in a prolonged manner for the
following 48 h (47.20±4.70%), which was also relatively different
from previous studies, possibly due to the aforementioned reasons.
In brief, the present study revealed that ATO could be loaded and
released by CBs favorably.
As ATO exhibits favorable efficacy in liver cancer
patients, and CBs exhibited acceptable ATO loading and releasing
efficiencies, it is hypothesized that ATO-eluting CBs has a good
efficacy for treating liver cancer. However, the in vitro
anti-liver cancer activity of ATO-eluting CBs has not been
demonstrated until now, to the best of our knowledge. Therefore,
cell viability, the apoptosis rate and invasive cell count were
compared by treating liver cancer cells with ATO-eluting CBs or ATO
solution, and it was revealed that ATO-eluting CBs reduced cell
viability to some extent and did not affect invasive cell count or
the apoptosis rate compared with ATO solution in liver cancer
cells. Additionally, liver cancer cells treated with ATO-eluting
CBs or ATO solution exhibited downregulated VEGF and MMP9
expression to a similar degree, both of which are reported to
promote cell invasion (25,26). The results of the present study
indicated that ATO loaded by CBs exhibited slightly improved
efficacy in suppressing liver cancer progression compared with the
ATO solution, which may be due to the fact that CBs surrounded the
liver cancer cells, which caused a large ATO concentration gradient
between the extra-cell matrix and cytoplasm, thereby facilitating
the diffusion of ATO into liver cancer cells to exert its cytotoxic
effects.
The pharmacokinetics or efficacy of chemotherapeutic
agents by microspheres or conventional drug carriers/embolization
agents have been compared in several animal studies (7,8,36). One noteworthy study revealed that
doxorubicin-loaded HepaSphere has a lower doxorubicin concentration
in plasma (within 24 h) while a higher concentration in tumor
tissue (over 14 days) compared with doxorubicin-loaded lipiodol
following TACE treatment in a rabbit model of liver cancer
(37). Another study revealed that
both doxorubicin and its metabolite doxorubicinol plasma
concentrations were lower, whereas the doxorubicin concentration in
tumor tissue was higher after being released by DC beads compared
with lipiodol in a rabbit model of liver cancer (36). Additionally, in the previous study, it
was also revealed that complete necrosis of tumor tissue was
achieved after 7 days of doxorubicin-eluting DC bead
chemoembolization, but only partial necrosis of tumor tissue was
achieved using the doxorubicin/lipiodol emulsion chemoembolization
(36). These animal studies revealed
that several microspheres are superior to conventional drug
carriers/embolization agents regarding drug pharmacokinetics and
treatment efficacy. However, the in vivo ATO
pharmacokinetics, efficacy and safety of ATO-eluting CBs are still
unclear. Therefore, the ATO pharmacokinetics, tumor necrosis
efficacy and safety following chemo-embolizing with ATO-eluting CBs
or ATO/lipiodol emulsion in a rabbit VX2 liver cancer model were
evaluated. The results revealed that the ATO concentration in
plasma was higher, whereas ATO concentration in tumor tissue was
higher after chemoembolization of ATO-eluting CBs compared with
ATO/lipiodol emulsion, suggesting that ATO-eluting CBs exhibited
improved ATO pharmacokinetics compared with ATO/lipiodol emulsion.
Probable reasons for these results include: i) Lipiodol may
circulate with blood, leading to a higher ATO concentration in
plasma and a lower ATO concentration in tumor tissue. ii) CBs
released ATO in a more sustainable manner compared with lipiodol,
which may contribute to its accumulation in tumor tissue and a
decreased metabolism speed, thereby increasing its tumor
concentration and decreasing its plasma concentration.
Additionally, it was revealed that ATO-eluting CBs enhanced tumor
necrosis compared with ATO/lipiodol emulsion at day 7 after the
surgery, indicating that ATO-eluting CBs had improved efficacy
compared with ATO/lipiodol emulsion (probably due to the higher ATO
concentration in tumor tissue after chemoembolizing with
ATO-eluting CBs compared with ATO/lipiodol emulsion). Notably,
gross observations on liver tissue revealed that ATO-eluting CBs
decreased necrosis of normal liver parenchyma compared with
ATO/lipiodol emulsion, which may be due to the fact that
ATO/lipiodol emulsion can spread to the normal liver parenchyma,
thereby causing necrosis of normal liver parenchyma or lipiodol
itself exhibited cytotoxic effects on normal liver cells. However,
there was no major difference between soluble and
microsphere-loaded ATO in vitro, whereas the use of
microspheres resulted in a more sustained release of ATO in the
tumor mass (although the initial peak was somewhat lower), the
difference of the impact of ATO-eluting CBs on liver cancer between
in vivo and in vitro may due to the fact that
specifics of release are considerably more complicated in
vivo compared with in vitro. Thus, further studies are
required in which the tumor cells should initially be incubated in
ATO-CBs or a slightly higher concentration of ATO, followed by a
wash-out, and subsequently a new incubation of ATO-CBs or ATO at a
markedly lower concentration.
In summary, CBs present with acceptable ATO loading
and releasing efficiencies. Additionally, ATO-eluting CBs exhibited
superior anticancer properties in liver cancer cells, and improved
pharmacokinetics, treatment efficacy and milder liver toxicity of
ATO compared with the ATO/lipiodol emulsion in the TACE treatment
of the rabbit model of liver cancer.
Acknowledgements
Not applicable.
Funding
The present study was supported by the National
Natural Science Foundation of China (grant nos. 81401494 and
U2004119).
Availability of data and materials
The datasets used and analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors contributions
XD and GZ were the main contributors to the research
design, and XH reviewed and revised the study for important
intellectual content. In the present study, XD and JR were mainly
responsible for the drug loading and release experiments of arsenic
trioxide microspheres. XD was mainly responsible for exploration of
the dispensing process and dosage of arsenic trioxide loading in
drug-carrying microspheres. XH designed the drug loading and
release experiments of arsenic trioxide microspheres. JR was mainly
responsible for the in vitro experiments assessing the
effects of arsenic trioxide microspheres on hepatocellular
carcinoma cells. HL was mainly responsible for the establishment of
the rabbit VX2 liver tumor model and gradually improved the CT
enhanced detection method for the rabbit VX2 liver tumor. PC was
mainly responsible for the implementation of TACE treatment in a
rabbit VX2 liver tumor model. SJ completed the collection of blood
and tissue samples. MW completed the serum (tissue) sample
pretreatment and drug concentration detection. SJ and MW jointly
completed the analysis and interpretation of the data. In addition,
HL, GZ and PC completed the drafting of the manuscipt. All authors
read and approved the final manuscript.
Ethics approval and consent to
participate
The study was approved from The Scientific Research
and Clinical Trial Ethics Committee of the First Affiliated
Hospital of Zhengzhou University (No. Scientific research-2017-03).
All the procedures on animals were approved by the Institutional
Animal Care and Use Committee at our institution (Ethics and
Scientific Trial Committee of the First Affiliated Hospital of
Zhengzhou University), and the experiments were performed in
accordance with institutional guidelines.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
Glossary
Abbreviations
Abbreviations:
|
ATO
|
arsenic trioxide
|
|
CBs
|
CalliSphere beads
|
|
TACE
|
transhepatic arterial
chemoembolization
|
|
cTACE
|
conventional TACE
|
|
PBS
|
phosphate-buffered saline
|
|
CCK-8
|
Cell Counting Kit-8
|
|
qPCR
|
quantitative polymerase chain
reaction
|
References
|
1
|
Siegel RL, Miller KD and Jemal A: Cancer
statistics, 2018. CA Cancer J Clin. 68:7–30. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Bray F, Ferlay J, Soerjomataram I, Siegel
RL, Torre LA and Jemal A: Global cancer statistics 2018: GLOBOCAN
estimates of incidence and mortality worldwide for 36 cancers in
185 countries. CA Cancer J Clin. 68:394–424. 2018. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
El-Serag HB: Hepatocellular carcinoma. N
Engl J Med. 365:1118–1127. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Jang JH, Lee JW, Hong JT and Jin YJ:
Transarterial chemoembolization for hepatocellular carcinoma: An
evidence-based review of its place in therapy. J Hepatocell
Carcinoma. 2:123–129. 2015.PubMed/NCBI
|
|
5
|
Liu YS, Ou MC, Tsai YS, Lin XZ, Wang CK,
Tsai HM and Chuang MT: Transarterial chemoembolization using
gelatin sponges or microspheres plus lipiodol-doxorubicin versus
doxorubicin-loaded beads for the treatment of hepatocellular
carcinoma. Korean J Radiol. 16:125–132. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xie F, Zang J, Guo X, Xu F, Shen R, Yan L,
Yang J and He J: Comparison of transcatheter arterial
chemoembolization and microsphere embolization for treatment of
unresectable hepatocellular carcinoma: A meta-analysis. J Cancer
Res Clin Oncol. 138:455–462. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zhang S, Huang C, Li Z, Yang Y, Bao T,
Chen H, Zou Y and Song L: Comparison of pharmacokinetics and drug
release in tissues after transarterial chemoembolization with
doxorubicin using diverse lipiodol emulsions and CalliSpheres Beads
in rabbit livers. Drug Deliv. 24:1011–1017. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Lee KH, Liapi EA, Cornell C, Reb P, Buijs
M, Vossen JA, Ventura VP and Geschwind JF: Doxorubicin-loaded
QuadraSphere microspheres: Plasma pharmacokinetics and intratumoral
drug concentration in an animal model of liver cancer. Cardiovasc
Intervent Radiol. 33:576–582. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ni JY, Xu LF, Wang WD, Sun HL and Chen YT:
Conventional transarterial chemoembolization vs microsphere
embolization in hepatocellular carcinoma: A meta-analysis. World J
Gastroenterol. 20:17206–17217. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Zhang X, Zhou J, Zhu DD, Huang J, Sun JH,
Li TF, Shi CS, Sun ZC, Hou QM, Peng ZY, et al: CalliSpheres(R)
drug-eluting beads (DEB) transarterial chemoembolization (TACE) is
equally efficient and safe in liver cancer patients with different
times of previous conventional TACE treatments: a result from CTILC
study. Clin Transl Oncol. 21:167–177. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Yamaguchi T, Seki T, Komemushi A, Suwa K,
Tsuda R, Inokuchi R, Murata M, Yuki M, Harima Y and Okazaki K:
Acute necrotizing pancreatitis as a fatal complication following DC
Bead transcatheter arterial chemoembolization for hepatocellular
carcinoma: A case report and review of the literature. Mol Clin
Oncol. 9:403–407. 2018.PubMed/NCBI
|
|
12
|
Guan YS, He Q, Jin Y and Yao F:
Development of CalliSpheres® embolic microspheres.
Zhonghua Gan Zang Bing Za Zhi. 24:549–551. 2016.(In Chinese).
PubMed/NCBI
|
|
13
|
Chen G, Zhang D, Ying Y, Wang Z, Tao W,
Zhu H, Zhang J and Peng Z: Clinical investigation on transarterial
chemoembolization with indigenous drug-eluting beads in treatment
of unresectable hepatocellular carcinoma. Zhejiang Da Xue Xue Bao
Yi Xue Ban. 46:44–51. 2017.(In Chinese). PubMed/NCBI
|
|
14
|
Wu B, Zhou J, Ling G, Zhu D and Long Q:
CalliSpheres drug-eluting beads versus lipiodol transarterial
chemoembolization in the treatment of hepatocellular carcinoma: A
short-term efficacy and safety study. World J Surg Oncol.
16:692018. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Zhou GH, Han J, Sun JH, Zhang YL, Zhou TY,
Nie CH, Zhu TY, Chen SQ, Wang BQ, Yu ZN, et al: Efficacy and safety
profile of drug-eluting beads transarterial chemoembolization by
CalliSpheres® beads in Chinese hepatocellular carcinoma
patients. BMC Cancer. 18:6442018. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Cohen MH, Hirschfeld S, Flamm Honig S,
Ibrahim A, Johnson JR, OLeary JJ, White RM, Williams GA and Pazdur
R: Drug approval summaries: Arsenic trioxide, tamoxifen citrate,
anastrazole, paclitaxel, bexarotene. Oncologist. 6:4–11. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Wang L, Min Z, Wang X, Hu M, Song D, Ren
Z, Cheng Y and Wang Y: Arsenic trioxide and sorafenib combination
therapy for human hepatocellular carcinoma functions via
up-regulation of TNF-related apoptosis-inducing ligand. Oncol Lett.
16:3341–3350. 2018.PubMed/NCBI
|
|
18
|
Zhang F, Zhang CM, Li S, Wang KK, Guo BB,
Fu Y, Liu LY, Zhang Y, Jiang HY and Wu CJ: Low dosage of arsenic
trioxide inhibits vasculogenic mimicry in hepatoblastoma without
cell apoptosis. Mol Med Rep. 17:1573–1582. 2018.PubMed/NCBI
|
|
19
|
Wang HY, Zhang B, Zhou JN, Wang DX, Xu YC,
Zeng Q, Jia YL, Xi JF, Nan X, He LJ, et al: Arsenic trioxide
inhibits liver cancer stem cells and metastasis by targeting
SRF/MCM7 complex. Cell Death Dis. 10:4532019. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Qiu Y, Dai Y, Zhang C, Yang Y, Jin M, Shan
W, Shen J, Lu M, Tang Z, Ju L, et al: Arsenic trioxide reverses the
chemoresistance in hepatocellular carcinoma: A targeted
intervention of 14-3-3eta/NF-kappaB feedback loop. J Exp Clin
Cancer Res. 37:3212018. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Song P, Hai Y, Ma W, Zhao L, Wang X, Xie
Q, Li Y, Wu Z, Li Y and Li H: Arsenic trioxide combined with
transarterial chemoembolization for unresectable primary hepatic
carcinoma: A systematic review and meta-analysis. Medicine
(Baltimore). 97:e06132018. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Schiavone EL and Torrado OA: Determination
of arsenic in water by the silver diethyldithiocarbamate method.
Rev Sanid Milit Argent. 66:251–263. 1967.(In Spanish). PubMed/NCBI
|
|
23
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) Method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cima G: AVMA Guidelines for the Euthanasia
of Animal. Javma - Journal of the American Veterinary Medical
Association. (2013 edition). 242:715–716. 2013.
|
|
25
|
Sharma BK, Srinivasan R, Chawla YK and
Chakraborti A: Vascular endothelial growth factor: Evidence for
autocrine signaling in hepatocellular carcinoma cell lines
affecting invasion. Indian J Cancer. 53:542–547. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Zhou L, Wang DS, Li QJ, Sun W, Zhang Y and
Dou KF: Downregulation of the Notch signaling pathway inhibits
hepatocellular carcinoma cell invasion by inactivation of matrix
metalloproteinase-2 and −9 and vascular endothelial growth factor.
Oncol Rep. 28:874–882. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Nouri YM, Kim JH, Yoon HK, Ko HK, Shin JH
and Gwon DI: Update on transarterial chemoembolization with
drug-eluting microspheres for hepatocellular carcinoma. Korean J
Radiol. 20:34–49. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Huang K, Zhou Q, Wang R, Cheng D and Ma Y:
Doxorubicin-eluting beads versus conventional transarterial
chemoembolization for the treatment of hepatocellular carcinoma. J
Gastroenterol Hepatol. 29:920–925. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Zhang X, Jia S, Yang S and Yang Y, Yang T
and Yang Y: Arsenic trioxide induces G2/M arrest in hepatocellular
carcinoma cells by increasing the tumor suppressor PTEN expression.
J Cell Biochem. 113:3528–3535. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Jiang L, Wang L, Chen L, Cai GH, Ren QY,
Chen JZ, Shi HJ and Xie YH: As2O3 induces apoptosis in human
hepatocellular carcinoma HepG2 cells through a ROS-mediated
mitochondrial pathway and activation of caspases. Int J Clin Exp
Med. 8:2190–2196. 2015.PubMed/NCBI
|
|
31
|
Cui L, Gao B, Cao Z, Chen X, Zhang S and
Zhang W: Downregulation of B7-H4 in the MHCC97-H hepatocellular
carcinoma cell line by arsenic trioxide. Mol Med Rep. 13:2032–2038.
2016. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Yu H, Zhu GY, Xu RZ, Niu HZ, Lu Q, Li GZ,
Wang ZY, Zhang DS, Gu N and Teng GJ: Arterial embolization
hyperthermia using As2O3 nanoparticles in VX2 carcinoma-induced
liver tumors. PLoS One. 6:e179262011. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Tan B, Huang JF, Wei Q, Zhang H and Ni RZ:
Anti-hepatoma effect of arsenic trioxide on experimental liver
cancer induced by 2-acetamidofluorene in rats. World J
Gastroenterol. 11:5938–5943. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Jordan O, Denys A, De Baere T, Boulens N
and Doelker E: Comparative study of chemoembolization loadable
beads: In vitro drug release and physical properties of DC bead and
hepasphere loaded with doxorubicin and irinotecan. J Vasc Interv
Radiol. 21:1084–1090. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
de Baere T, Plotkin S, Yu R, Sutter A, Wu
Y and Cruise GM: An in vitro evaluation of four types of
Drug-eluting microspheres loaded with doxorubicin. J Vasc Interv
Radiol. 27:1425–1431. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Hong K, Khwaja A, Liapi E, Torbenson MS,
Georgiades CS and Geschwind JF: New intra-arterial drug delivery
system for the treatment of liver cancer: preclinical assessment in
a rabbit model of liver cancer. Clin Cancer Res. 12:2563–2567.
2006. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Gupta S, Wright KC, Ensor J, Van Pelt CS,
Dixon KA and Kundra V: Hepatic arterial embolization with
doxorubicin-loaded superabsorbent polymer microspheres in a rabbit
liver tumor model. Cardiovasc Intervent Radiol. 34:1021–1030. 2011.
View Article : Google Scholar : PubMed/NCBI
|