Introduction
Nasopharyngeal carcinoma (NPC) is an aggressive
malignancy of the head and neck closely associated with
Epstein-Barr virus (EBV) infection (1), characterized by notable geographical
variation. It is particularly prevalent in East and Southeast Asia,
with southern China being a high-incidence region (2). Among the pathological subtypes,
EBV-associated non-keratinizing squamous cell carcinoma accounts
for >95% of cases in endemic areas (3), making it the primary focus of clinical
treatment. In 2022, >120,000 new cases and >70,000 deaths
were reported globally (4).
Although the incidence of NPC has gradually declined worldwide over
the past few decades, and the 5-year overall survival (OS) rate for
early-stage patients has reached 94.0% (5), the deep anatomical location and
non-specific clinical manifestations of the disease often result in
the majority of patients being diagnosed at an advanced stage. This
leads to poor prognosis, with recurrence and distant metastasis
being the leading causes of death. NPC is relatively sensitive to
radiotherapy and chemotherapy, with a combination of synchronous
chemoradiotherapy (CRT) being the standard treatment modality.
However, some patients still experience local recurrence or distant
metastasis due to radiation resistance, chemotherapy resistance or
other factors. The rate of distant metastasis in newly diagnosed
patients with NPC is 6–15%, and ~20% of patients with
non-metastatic NPC will eventually experience recurrence or
metastasis after definitive treatment (6,7). In
recent years, the gemcitabine + cisplatin (GP) regimen has been
recommended by major guidelines as the first-line standard
treatment for recurrent and metastatic NPC (8). However, its clinical efficacy remains
limited, with median progression-free survival (mPFS) and median OS
(mOS) of only 7.0 and 22.1 months, respectively (6,9).
Recently, the clinical breakthrough of immune checkpoint inhibitors
(ICIs) and the precise development of targeted therapies have
transformed the treatment landscape for NPC (10–13),
offering the potential for survival improvement. Combined
therapeutic strategies, particularly immunotherapy in combination
with targeted therapy or chemotherapy, have demonstrated
substantial synergistic potential, emerging as a key area of
research in the field. However, existing reviews primarily focus on
the clinical data of individual treatment modalities, offering
limited in-depth analysis of the synergistic mechanisms underlying
combination therapies. Furthermore, there is a lack of
comprehensive integration of the latest clinical evidence, such as
bispecific antibodies, antibody-drug conjugates (ADCs) and the
translational challenges associated with their clinical
application. The present review systematically summarized the
breakthroughs in basic research, clinical evidence progress and
translational application challenges in the fields of targeted
therapy and immunotherapy for recurrent/metastatic NPC (R/M-NPC),
with a focus on innovative combination therapies, providing novel
ideas and approaches for the effective treatment of R/M-NPC in
clinical practice.
Immunotherapy
Tumor immunotherapy is a novel strategy that aims to
control and eliminate tumor cells by activating or maintaining
immune cycles and restoring normal antitumor immune responses. In
recent years, with the in-depth understanding of tumor immunology
and breakthroughs in immune regulation technologies, immunotherapy
has become a key pillar in the comprehensive treatment of NPC
(14). At present, immunotherapy
for NPC mainly focuses on immune checkpoint blockade therapies
(such as PD-1/PD-L1 inhibitors), adoptive immune cell therapy (such
as EBV-targeted CAR-T cells), cytotoxic T lymphocyte antigens,
therapeutic vaccines [peptide vaccines targeting EBV latent
membrane proteins (LMPs)] and immune modulation strategies. These
approaches function by reshaping the antitumor immune responses of
the body and overcoming tumor immune escape mechanisms,
demonstrating notable efficacy in the translational treatment of
R/M-NPC and locally advanced NPC.
PD-1/PD-L1 inhibitors
PD-1 is a membrane-bound receptor primarily
expressed on the surface of immune cells such as T cells and B
cells. It plays a crucial role in inhibiting T cell-mediated
inflammatory responses and modulating cellular reactions to
maintain immune homeostasis and promote self-tolerance. PD-L1, the
ligand for PD-1, is predominantly found on the surface of tumor
cells, certain immune cells and some non-immune cells. The
interaction between PD-1 and PD-L1 leads to the downregulation of
CD8+ T lymphocyte and CD4+ T lymphocyte
activity via the PD-1/PD-L1 pathway, inhibiting their proliferation
and ultimately suppressing their effector function within the tumor
microenvironment (TME) (15). This
results in diminished immune-mediated tumor cell elimination and
facilitates immune evasion by the tumor.
PD-1 inhibitors primarily exert their antitumor
effects by blocking the PD-1/PD-L1 signaling pathway, thereby
reactivating T cell-mediated antitumor immunity. On one hand, PD-1
inhibitors specifically bind to the PD-1 molecules on the surface
of T cells via their antigen-binding fragments (Fig. 1). By occupying the ligand-binding
site of PD-1, these inhibitors prevent the interaction between PD-1
and PD-L1 on tumor cells, thereby disrupting the inhibitory signals
transmitted through this pathway. On the other hand, once the
inhibitory signals are removed, activated T cells regain
proliferative capacity and secrete large amounts of cytokines such
as IFN-γ and TNF-α, which directly attack tumor cells. Furthermore,
activated T cells can also stimulate other immune cells, leading to
a broader immune response aimed at eradicating tumor cells.
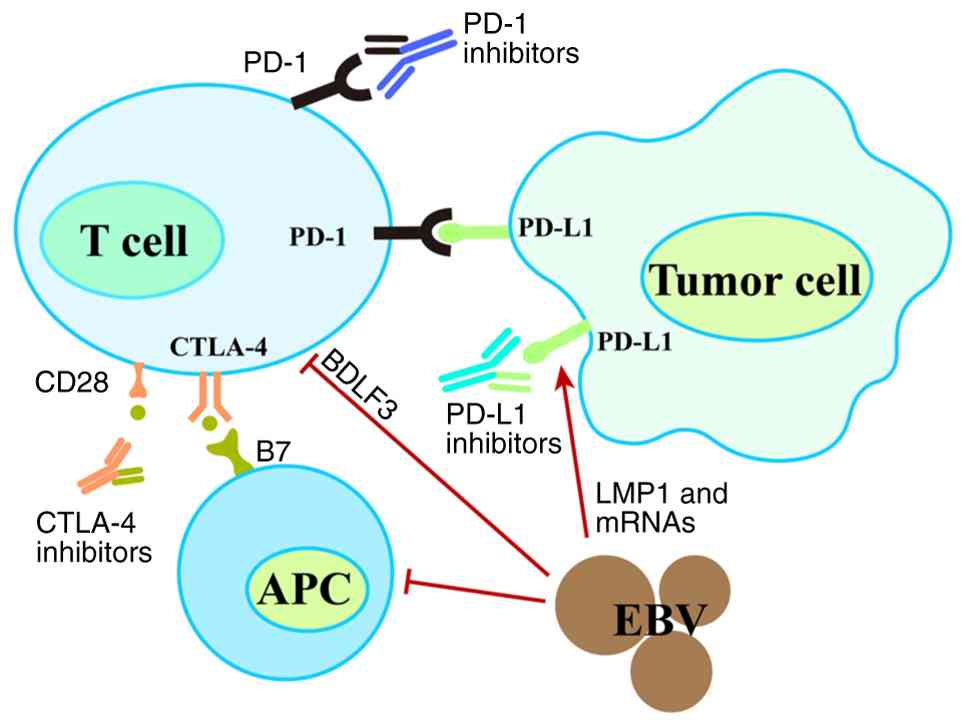 | Figure 1.PD-1 binds to PD-L1, and through the
PD-1/PD-L1 pathway, it reduces T lymphocyte activity and inhibits
their proliferation, thereby suppressing the functional role of T
lymphocytes in the tumor microenvironment. PD-1 inhibitors, by
specifically recognizing and binding to PD-1 molecules on the
surface of T cells via their antigen-binding fragment, and PD-L1
inhibitors, which bind to PD-L1 molecules on tumor cells, both
disrupt the inhibitory signals transmitted through this pathway,
thereby restoring the ability of T cells to kill tumor cells.
CTLA-4 inhibitors bind to CTLA-4 on T cells, blocking the
interaction between CTLA-4 and its ligand B7, thereby enhancing T
cell activation and proliferation. The EBV can use BDLF3, which
interferes with antigen presentation by both MHC-I and MHC-II,
limiting T cell-mediated immune recognition. Viral proteins such as
LMP1 and microRNAs induce PD-L1 expression, which binds to PD-1 on
T cells, reducing their antitumor and antiviral responses. CTLA-4,
cytotoxic T lymphocyte antigen 4; APC, antigen-presenting cell;
EBV, Epstein-Barr virus; PD-(L)1, programmed cell death (ligand)
protein type 1. |
Toripalimab
Toripalimab is a recombinant humanized PD-1
monoclonal antibody, which was approved in China in 2021 and later
by the US Food and Drug Administration and European Medicines
Agency for the treatment of R/M-NPC. Multiple studies have
demonstrated the promising application of toripalimab in locally
advanced or R/M-NPC. A Phase II clinical trial investigating
toripalimab in combination with concurrent CRT during the
neoadjuvant and adjuvant phases for locally advanced NPC found
that, compared with the placebo group receiving only CRT, the
toripalimab combination group showed higher 2-year PFS (16). This suggests that early intervention
with immunotherapy may reduce the risk of recurrence by activating
antitumor immunity. This approach offers a novel immuno-enhancing
strategy for patients with locally advanced NPC. In R/M-NPC, a
Phase III trial (JUPITER-02) with 3-year survival follow-up showed
that the mPFS for the toripalimab combined with gemcitabine and
cisplatin (GP regimen) group was 21.4 months, extending by 13.2
months (21.4 vs. 8.2 months) (17).
This result directly facilitated its approval by regulatory
agencies in the U.S., China and Europe, establishing immune
combination chemotherapy as the first-line standard treatment for
R/M-NPC.
Camrelizumab
Camrelizumab is a humanized high-affinity anti-PD-1
immunoglobulin G4-k monoclonal antibody that has shown promising
clinical potential in locally advanced or R/M-NPC. The Chinese
Society of Clinical Oncology guidelines have approved camrelizumab
in combination with chemotherapy as first-line treatment. In the
Phase III CAPTAIN-1st study, adding camrelizumab to cisplatin and
gemcitabine notably extended the PFS (9.7 vs. 6.9 months) (18). The key mechanism of action lies in
the inhibition of myeloid-derived suppressor cells (MDSCs),
promotion of dendritic cell (DC) maturation and reduction of the
immunosuppressive TME, which enhances the release of tumor antigens
and provides additional recognition targets for
camrelizumab-activated T cells, thereby augmenting antitumor
efficacy. Furthermore, in the context of locally advanced NPC, the
DIPPER study demonstrated that, after a median follow-up of 39
months, camrelizumab combined with the GP chemotherapy regimen
exhibited superior antitumor activity and safety compared with GP
chemotherapy alone (19). Compared
with traditional concurrent CRT, this combination enhances tumor
cell sensitivity to radiation while avoiding the risk of severe
hematologic toxicity and radiation-induced mucositis, offering a
safer treatment option for elderly patients or those with
comorbidities who are intolerant to high-intensity therapies.
Tislelizumab
Tislelizumab is a humanized IgG4 anti-PD-1
monoclonal antibody that has demonstrated promising antitumor
efficacy across a variety of malignancies. It has been approved in
China for the treatment of multiple cancer types (20). In a Phase III trial (RATIONALE 309)
evaluating its efficacy in untreated R/M NPC (21), the combination of tislelizumab with
gemcitabine and cisplatin was compared with placebo with
gemcitabine and cisplatin. In an interim analysis, the combination
of tislelizumab and chemotherapy significantly prolonged PFS
compared with placebo with chemotherapy. Furthermore, after
progression, second-line therapy results demonstrated favorable
trends for both PFS and OS in the tislelizumab combination group
vs. the placebo group. The aforementioned study suggested that the
combination of tislelizumab with chemotherapy substantially reduces
the risk of disease progression or death, with a tolerable safety
profile, offering the potential for maximum clinical benefit to
patients.
Sintilimab
Sintilimab is a highly selective, fully humanized
anti-PD-1 monoclonal antibody that has shown efficacy in various
solid tumors (22). A recent Phase
III clinical trial in China (23)
found that in patients with locally advanced NPC, sintilimab
combined with chemotherapy resulted in a higher PFS rate compared
with the standard treatment group. However, the sintilimab group
also exhibited a higher incidence of grade 3–4 adverse events.
Therefore, further trials with longer follow-up are required to
validate the efficacy and safety profile of sintilimab.
Additionally, considerable gaps remain in the clinical exploration
of sintilimab, with its indications currently limited to locally
advanced NPC. Efficacy data in R/M-NPC are sparse, with only
small-sample Phase II single-arm studies available. In addition,
there is a lack of head-to-head comparisons with the standard GP
regimen or other PD-1 inhibitors.
Nivolumab
Nivolumab is a humanized IgG4 monoclonal antibody
that inhibits the PD-1 receptor on T cells, preventing its
interaction with PD-L1. In the treatment of R/M-NPC, nivolumab has
demonstrated considerable activity, with a superior 1-year OS rate
compared with historical data from similar populations (24). A study has shown that nivolumab
offers a novel treatment option for patients with
platinum-resistant R/M-NPC, with a high disease control rate (DCR)
and manageable safety profile (25). However, existing data mainly consist
of single-arm trials with small sample sizes, making it difficult
to exclude baseline differences in patient characteristics that may
influence survival benefits. As such, the real-world efficacy of
nivolumab in R/M-NPC requires further validation through larger
cohort studies. A recent Phase II trial with long-term follow-up
data has shown that nivolumab, in combination with induction
chemotherapy and radiotherapy, provides effective antitumor
activity with lower toxicity, offering a new combination strategy
for locally advanced NPC treatment (26).
Pembrolizumab
Pembrolizumab is a humanized monoclonal IgG4
antibody that binds to the PD-1 receptor and effectively blocks its
interaction with the ligand. Pembrolizumab shows promise in NPC
treatment. In the Phase Ib KEYNOTE-028 study, which primarily
targeted patients with multiple prior treatment failures,
pembrolizumab demonstrated preliminary antitumor activity (27), providing a novel potential treatment
option for patients that are chemotherapy-resistant. By contrast,
in the Phase III KEYNOTE-122, which focused on patients with
R/M-NPC who had failed platinum-based chemotherapy, pembrolizumab
monotherapy did not show a significant difference in efficacy
compared with single-agent chemotherapy (28). The differences in the efficacy
results between these two studies can largely be attributed to
variations in the study populations and sample sizes. KEYNOTE-028
included patients who had failed multiple lines of treatment, with
a small sample size of just 27 patients, and its survival benefits
lack confirmation from large-scale real-world data. By contrast,
KEYNOTE-122 was a Phase III confirmatory trial with a sample size
of 233 patients, covering a broader clinical population with
increased heterogeneity. The results of KEYNOTE-122 are therefore
more reflective of the real-world clinical scenario and offer a
more accurate assessment of the general efficacy of
pembrolizumab.
KL-A167
KL-A167 is an innovative, humanized anti-PD-L1
monoclonal antibody developed in China. It has been approved by the
National Medical Products Administration for treating patients with
R/M-NPC who have failed second-line chemotherapy or beyond. Through
targeted mutation technology for Fc segment optimization, KL-A167
eliminates ADCC and CDC effects, providing advantages such as
higher stability and reduced immune evasion. A Phase II study
showed that in patients with R/M-NPC who had received multiple
lines of treatment and had a high tumor burden (43.9% liver with
metastasis, 31.8% with ≥3 lines of chemotherapy failure), KL-A167
monotherapy achieved an overall response rate (ORR) of 26.5%, with
a mPFS of 2.8 months and OS of 16.2 months, while maintaining a
favorable safety profile (29). A
recent secondary analysis of the aforementioned study (30,31)
revealed that patients with non-liver metastasis had significantly
longer PFS and OS compared with patients with liver metastasis.
This finding is noteworthy, as patients with liver metastasis
typically have a lower response rate to immunotherapy. However,
these studies remain in the preliminary validation phase, with the
existing Phase II design being a single-arm trial lacking
head-to-head comparison with standard later-line treatments. This
limits the ability to definitively determine its relative efficacy
advantage. Furthermore, the small sample size may lead to an
overestimation of efficacy. A Phase III study is currently underway
and will provide further data for validation.
PD-1/PD-L1 inhibitors, when used as monotherapy or
in combination with chemotherapy, CRT or as adjuvant treatment in
R/M-NPC, have shown notable improvements in ORR, PFS and OS, with
manageable safety profiles. The clinical trial results related to
PD-1/PD-L1 inhibitors are shown in Table I. PD-1/PD-L1 inhibitors are
progressively becoming central to the treatment of NPC, and
combination strategies have substantially improved prognosis.
 | Table I.List of Phase II/III clinical trials
for immunotherapy in NPC. |
Table I.
List of Phase II/III clinical trials
for immunotherapy in NPC.
| First author/s,
year | Drug (year) | Targets | Study design | Disease
setting | n | Outcomes | Phase | (Refs.) |
|---|
| Yang et al,
2021 | Camrelizumab | PD-1 | Randomized,
doubleblind, camrelizumab vs. placebo in combination with
gemcitabine and cisplatin | Untreated
R/M-NPC | 343 (camrelizumab
group, n=134) | Camrelizumab group
mPFS, 9.7 months; placebo group mPFS, 6.9 months; HR, 0.54 | III | (18) |
| Yang et al,
2023 | Tislelizumab | PD-1 | Multicenter;
Tislelizumab plus chemotherapy as first-line treatment | R/M NPC | 263 (Tislelizumab
group, n=131) | Median follow-up,
15.5 months, Tislelizumab group mPFS, 9.6 months, ORR 69.5%;
placebo group mPFS, 7.4 months; placebo-chemotherapy, ORR
55.3% | III | (21) |
| Chan et al,
2023 | Pembrolizumab | PD-1 | Open-label,
randomized, pembrolizumab monotherapy vs. chemotherapy | Platinum-pretreated
R/M-NPC | 233 (pembrolizumab
group, n=117) | Pembrolizumab
median OS, 17.2 months; chemotherapy median OS, 15.3 months; HR,
0.9 | III | (28) |
| Liu et al,
2024 | Sintilimab | PD-1 | Multicenter,
open-label, parallel-group, randomized, controlled,
induction-concurrent chemoradiotherapy with or without
sintilimab | Non-metastatic
stage III–IVa locoregionally advanced NPC | 425 (sintilimab
group, n=210) | Event-free
survival | III was higher in
the sintilimab group (36-month rate, 86 vs. 76%) | (23) |
| Liu et al,
2024 | Toripalimab | PD-1 | Randomized,
single-center, double-blind, placebo-controlled | Untreated stage III
or IVa NPC | 150 (toripalimab
group, n=100) | Median follow-up
for PFS, 37.8 months; 2-year PFS for toripalimab group, 92.0%;
2-year PFS for placebo group, 74.0%; HR, 0.40 | II | (16) |
| Xu et al,
2025 | Nivolumab | PD-1 | Multicenter,
nivolumab combined with induction chemotherapy and
radiotherapy | Stage III and IVa
NPC | 178 | Median follow-up,
43 months; 3-year failure-free survival, 88.5%; 3-year OS,
97.9% | II | (26) |
| Shi et al,
2023 | KL-A167 (2022) | PD-L1 | Multicenter,
single-arm | R/M-NPC, failed at
least two lines of chemotherapy | 153 | ORR, 26.5%; DCR,
56.8%; mPFS, 2.8 months; median OS, 16.2 months | II | (29) |
| Li et al,
2025; Li et al, 2025 | KL-A167 (2025) | PD-L1 | Multicenter,
single-arm, a secondary analysis of R/M-NPC patients treated with
KL-A167 | R/M-NPC, failed at
least two lines of chemotherapy | 153 | mPFS (72 vs. 144
days) and OS (730 vs. 305 days) were significantly longer for
patients with non-liver metastases. | II | (30,31) |
| Jiang et al,
2025 | Cadonilimab
(2025) | PD-1 and
CTLA-4 | Single-arm,
open-label, plus TPC chemotherapy (NAB-paclitaxel, cisplatin or
lobaplatin and capecitabine) | RM-NPC, failed at
least one line of chemotherapy and anti-PD-1 immunotherapy | 25 | ORR, 68%; median
DOR, 9.1 months; mPFS, 10.6 months; 12-month OS, 75.6% | II | (36) |
Cytotoxic T lymphocyte antigen 4 (CTLA-4)
inhibitors
CTLA-4 is a crucial inhibitory ligand found on
effector T cells. The binding of CD28 typically promotes T cell
activation and proliferation (Fig.
1). After T cell activation, the expression of CTLA-4
increases, and it suppresses T cell effector functions by
inhibiting CD28 receptor signaling, thereby regulating the immune
response (32). The inhibitory
signals of CTLA-4 are transmitted through the binding of B7-1
(CD80) and B7-2 (CD86) to antigen-presenting cells. In addition to
blocking co-stimulation, CTLA-4 is also critical for T cell
proliferation and NK-based cytotoxic functions. Therefore, by
blocking CTLA-4 with high-affinity anti-CTLA-4 antibodies, CTLA-4
signaling can be inhibited, which enhances T cell-mediated
elimination of cancer cells, promotes T cell activation and
improves immune responses against cancer (33).
Ipilimumab, an anti-CTLA-4 antibody, can bind to
CTLA-4 and block its interaction with its ligands, CD80/CD86,
thereby enhancing T cell activation and proliferation. A study has
shown that ipilimumab, in combination with nivolumab, also exhibits
activity in patients with R/M-NPC who have previously received
first-line combination chemotherapy (34). Subsequent studies revealed that
ipilimumab treatment led to increased expression of PD-L1/PD-L2 in
tumors and greater T cell infiltration, along with reduced stromal
and malignant cell components (35). This suggests that ipilimumab may
induce remodeling of the tumor and immune microenvironment,
potentially enhancing the effectiveness of subsequent anti-PD-1
therapy.
PD-1/CTLA-4 bispecific antibody
Cadonilimab is a symmetric tetravalent bispecific
antibody that targets both PD-1 and CTLA-4. In a prospective study,
cadonilimab combined with TPC chemotherapy demonstrated significant
antitumor activity in patients with RM-NPC (36). Another study reported encouraging
results, showing improved ORR and PFS in patients with
chemotherapy-refractory R/M-NPC (37). Recent research highlights that the
combination of cadonilimab and chemotherapy outperformed previous
dual ICI neoadjuvant studies (38).
These findings suggest that the combination of bispecific
antibodies with chemotherapy may offer a potential advantage in
enhancing tumor response rates. This breakthrough indicates that
the synergistic efficacy of bispecific antibodies may surpass that
of dual-agent combinations, providing a novel direction for
improving therapeutic outcomes in locally advanced patients.
Although existing data highlight the potential of cadonilimab
across various treatment settings, as a novel bispecific antibody,
its long-term efficacy, stability and safety profile require
further validation through large-scale clinical trials.
Adoptive cell immunotherapy
As most NPC cases are EBV-positive, targeting EBV
antigens expressed in NPC has become a method to improve the
prognosis of patients with advanced disease. The viral antigens
expressed in NPC can induce specific T lymphocyte responses
(39), producing EBV-specific
cytotoxic T lymphocytes (EBV-CTLs) that are highly specific. The
approach of extracting active immune cells from the body of the
patient, followed by ex vivo screening and expansion, before
applying them clinically is known as EBV-CTL therapy. Previous
clinical trials have demonstrated that EBV-CTL therapy can offer
clinical benefits (40,41). The VANCE trial in Singapore
evaluated the efficacy of EBV-CTL in R/M EBV-positive NPC, with
results showing no significant difference in mOS between the group
receiving sequential infusion of autologous EBV-CTLs after
first-line gemcitabine plus carboplatin (GC) chemotherapy and the
group receiving GC chemotherapy alone (25.0 vs. 24.9 months).
Although no survival advantage was observed, the VANCE trial still
lays the foundation for further exploration of EBV-CTL therapy.
Further clinical trials are expected in the future to further
investigate the potential of EBV-CTL in the treatment of NPC
(42).
Chimeric antigen receptor (CAR)-T cell therapy is an
immunotherapy that involves genetically modifying the T cells of
patients to express synthetic receptors termed CARs, which include
both antigen recognition domains and intracellular signaling
domains (43,44). These CAR-T cells can specifically
target tumor-associated antigens through scFv, eliminating tumor
cells by producing inflammatory cytokines and achieving
long-lasting antitumor activity. As a highly promising innovative
therapy, CAR-T cell therapy has opened novel therapeutic avenues
for NPC, particularly in cases of recurrence or metastasis
refractory to conventional treatments. Clinical translational
research on its application in NPC is currently underway.
NK cells, a key component of the immune system, play
a crucial role in tumor immune surveillance (45) by eliminating tumor cells in an
antigen-independent manner. NK cells induce apoptosis through the
expression of death ligands (such as TNF-α, FasL and TRAIL) and
regulate immunity by producing cytokines and chemokines (including
IFN-γ, IL-10, CCL3, CCL4 and CCL5). Higher NK cell activity is
associated with reduced carcinogenic viral infections and increased
survival rates. A Phase I study (46) of expanded NK cells combined with
cetuximab for the treatment of R/M-NPC showed that, among seven
treated patients, four had stable disease and three experienced
progression. The disease PFS of three patients who received two NK
cell treatments were 12, 13 and 19 months, respectively. Research
on this combinatory strategy remains in its early stages, with
current data being limited in scope and lacking controlled designs.
Its efficacy in R/M-NPC remains to be further validated through
larger, controlled studies. Nevertheless, the preliminary results
obtained thus far have laid an important foundation for future
exploration in this field.
Although adoptive cell immunotherapy has shown
certain efficacy in cancer treatment, challenges remain regarding
treatment-related toxicity and persistence. In CAR-T cell therapy,
functional impairments and T cell exhaustion are notable obstacles,
primarily due to the reduced vitality and short duration of some T
cells, insufficient infiltration of effective sites and the impact
of the immunosuppressive TME (47).
EBV-specific CAR-T and TIL therapies offer promising breakthrough
approaches for refractory NPC, targeting high-risk or recurrent
patient populations. These therapies are currently in the clinical
advancement phase, and more innovative strategies may emerge in the
future.
Tumor vaccines
Virus-associated antigens are preferable targets,
and EBV-positive NPC cells can express LMP and EBV nuclear antigen
1 (48). EBV antigens can directly
regulate the expression of PD-L1. EBV-encoded LMPs (LMP1 and LMP2)
induce high PD-L1 expression on tumor cells (Fig. 1), thereby directly inhibiting T cell
cytotoxicity. Furthermore, EBV antigen stimulation of tumor cells
and cells within the TME promotes the secretion of
anti-inflammatory cytokines such as IL-10 and TGF-β, which suppress
pro-inflammatory responses and foster an immunosuppressive
phenotype. Based on this mechanism, activating EBV-specific T cell
responses through tumor vaccines can not only directly eliminate
tumor cells expressing EBV antigens, but also induce long-lasting
immune memory to prevent tumor relapse. DCs have the ability to
present tumor antigens and can load multiple antigen-encoding mRNA
constructs to efficiently activate T cells. DC vaccines have shown
variable efficacy in the treatment of various malignancies,
possibly related to interactions with other therapeutic agents and
the functionality of bone marrow and lymphocytes (49). At present, research on DC vaccines
is limited, and more clinical trials are needed to define their
therapeutic efficacy.
The lipid-based LMP2-mRNA vaccine is a therapeutic
vaccine for NPC. A preclinical study has shown that mice treated
with three doses of the vaccine significantly suppressed tumor
growth in models expressing LMP2, demonstrating its potential in
combating NPC (50). A newly
developed LMP2-mRNA lipid nanoparticle (C2@mLMP2) can be delivered to
tumor-draining lymph nodes, inducing an increase in T cells. A
study has observed that C2@mLMP2, in
combination with αPD-1, exhibits strong synergistic antitumor
effects (51).
Although mRNA vaccines can trigger antigen-specific
T cell responses, therapeutic vaccination alone cannot achieve
potent tumor suppression. A recent study found (52) that the combination of mRNA vaccines
and NK cell therapy has demonstrated significant synergistic
effects in humanized NPC mouse models. This combination not only
leads to sustained inhibition and eradication of tumor cells, but
also effectively enhances the infiltration efficiency of human T
cells and NK cells into the TME, boosting their antitumor immune
functions. Therefore, combining therapeutic vaccination with NK
cell therapy is a promising strategy for treating EBV-positive NPC.
However, the efficacy and safety of this approach still require
further exploration in subsequent studies.
RNA vaccines for tumor therapy face numerous
challenges in the clinical translation process (53). The inherent characteristics of
tumors, including the development of resistance and immune evasion
mechanisms, notably impact treatment efficacy. Practical obstacles
also remain, such as the difficulty in determining optimal
individualized dosing regimens, defining suitable patient
populations, accurately quantifying tumor cells and addressing
technical issues such as the prolonged vaccine production timeline.
Currently, tumor mRNA vaccines remain in the early stages of
clinical development, with preliminary studies showing promising
immunogenicity and potential survival benefits. However, due to the
suppressive TME and inefficient antigen presentation, monotherapy
has shown limited efficacy. Therefore, combination therapy is
considered a key strategy to enhance therapeutic outcomes. Future
research should focus on the development of personalized tumor mRNA
vaccines and the exploration of novel immunoadjuvants. Notably, the
long-term efficacy of both monotherapy and combination therapy with
mRNA vaccines still requires validation through large-scale,
well-designed clinical trials.
Targeted therapy
In recent years, the rapid development of molecular
biology and tumor immunology has made targeted therapy a key pillar
of the comprehensive treatment of NPC (14). Currently, targeted therapies for NPC
focus on several core targets, including epidermal growth factor
receptor (EGFR), vascular endothelial growth factor (VEGF) and its
receptor (VEGFR), EBV-related antigens, as well as abnormally
activated signaling pathways such as PI3K/AKT/mTOR. Through diverse
treatment approaches, such as small molecule inhibitors and
monoclonal antibodies, targeted therapy precisely interferes with
key biological processes such as tumor cell proliferation,
angiogenesis and immune evasion. These advancements have notably
improved the quality of life and prognosis of patients. The
clinical trial results related to targeted therapy for NPC are
shown in Table II.
| Table II.List of Phase II/III clinical trials
for targeted therapy in NPC. |
Table II.
List of Phase II/III clinical trials
for targeted therapy in NPC.
| First author/s,
year | Drug | Targets | Study Design | Disease
setting | n | Outcomes | Phase | (Refs.) |
|---|
| Chan et al,
2005 | Cetuximab | EGFR | Multicenter,
open-label, single-arm | Refractory
R/M-NPC | 60 | ORR, 11.7%; mPFS,
81 days; median OS, 233 days | II | (59) |
| Chua et al,
2008 | Gefitinib | EGFR | Single-center | R/M-NPC, failed at
least 2 lines of chemotherapy | 19 | mPFS, 4 months;
median OS, 16 months | II | (78) |
| Jin et al,
2013 | Endostar | VEGF | Endostar combined
with gemcitabine-cisplatin chemotherapy | M-NPC | 30 | Median follow-up,
13.1 months; mPFS, 19.4 months; 1-year PFS rate, 69.8%; ORR, 85.7%;
OS, 90.2% | II | (93) |
| Li et al,
2020 | Endostar | VEGF | Randomized,
controlled, multicenter, standard chemoradiation with or without
Endostar | Locally advanced
NPC | 114 (Endostar
group, n=56) | 5-year OS, 73.2%;
PFS, 80.1%; FFS, 91.0%; control group, no significant difference
was found | II | (94) |
| Xu et al,
2022 | Endostar | VEGF | Randomized, open,
multicenter, Endostar combined with PF and IMRT | Locally advanced
NPC | 83 (Endostar group,
n=41) | Endostar group
showed significantly prolonged PFS by ~4 months, no significant
difference in the median overall survival was shown | II | (95) |
| Xu et al,
2024 | MRG003 | EGFR | MRG003 combined
with pucotenlimab | R/M-NPC, failed
firstline platinum-based therapy | 30 | Median follow-up
time, 4.2 months; cORR, 66.7%; DCR, 93.3%; 6-month PFS rate, 76.2%;
6-month DOR rate, 83.3% | II | (68) |
| Han et al,
2025 | Becotatug vedotin
(MRG003) | EGFR | Randomized,
controlled, multicenter, open-label, Becotatug vedotin vs.
chemotherapy | R/M-NPC, failed ≥2
lines of systemic chemotherapy and PD-(L)1 inhibitor | 173 (MRG003,
n=86) | By 30 June 2024,
ORR with MRG003 compared with chemotherapy was 30.2 vs. 11.5%; mPFS
was 5.8 vs. 2.8 months; as of 30 December 2024, the updated mOS was
17.1 vs. 12.0 months | II | (69) |
| Yang et al,
2025 | Izalontamab
brengitecan | EGFR and HER3 | Multicenter,
randomized, open-label | R/M-NPC, at least
to 2 standard therapies, including at least one platinum-containing
regimen and PD-1/PD-L1 inhibitors | 386 (iza- bren
group, n=191) | Median follow-up,
7.66 months; iza-bren ORR, 54.6%; chemotherapy, 27.0%; overall
survival data were not mature at data cut-off | III | (72) |
Notably, multi-target combination therapies and
precision medicine models based on genetic testing are driving NPC
targeted therapy toward more efficient and individualized
treatments. This novel approach presents a new avenue of
investigation for overcoming this challenging disease.
EGFR pathway
EGFR is a transmembrane glycoprotein that belongs to
the receptor tyrosine kinase ErbB family, which includes ErbB-1
(EGFR), ErbB-2 (HER2/neu), ErbB-3 (HER3) and ErbB-4 (HER4)
(54). By binding with ligands,
EGFR activates intracellular signaling pathways, such as PI3K/Akt
and MAPK, to regulate cell proliferation, differentiation, survival
and migration (55). In numerous
tumors, EGFR is abnormally activated due to overexpression or
genetic mutations, promoting tumor initiation and progression. EGFR
is overexpressed in ~80% of NPC cases, enhancing tumor cell
proliferation and metastasis (56).
EGFR plays a crucial inhibitory role in tumor immune regulation. On
one hand, activation of EGFR reduces the secretion of key
pro-inflammatory cytokines, such as IL-2 and IFN-γ, by T cells,
while simultaneously promoting tumor cells to strengthen their
immunosuppressive phenotype, thereby directly weakening the
antitumor immune response of the body. On the other hand, EGFR can
upregulate the surface expression of PD-L1 on tumor cells via ERK,
AKT-mTOR and STAT signaling pathways, further enhancing the
inhibitory activity of the PD-1/PD-L1 immune checkpoint and
ultimately reducing the clinical efficacy of ICIs in tumor
treatment (57).
EGFR inhibitors can directly suppress tumor cell
proliferation. Their mechanism involves competitively inhibiting
the binding of extracellular ligands to EGFR after binding to EGFR,
blocking the intracellular activation of EGFR, and thereby
inhibiting the activation of downstream pathways related to cell
proliferation, adhesion and angiogenesis, caused by EGFR
activation. This results in the suppression of tumor cell growth
(58), achieving antitumor effects.
Currently, EGFR inhibitors used for NPC treatment in clinical
practice and research include cetuximab, nimotuzumab, MRG003 and
BL-B01D1.
Cetuximab
Cetuximab is a monoclonal antibody that binds to
EGFR and has been used for treating EBV-related NPC. A Phase II
study in R/M-NPC demonstrated that the combination of cetuximab and
carboplatin achieved an ORR of 11.7% and a DCR of 60%. Notably,
only 31.7% of patients experienced treatment-related toxicities,
confirming the efficacy of the combination in disease control for
relapsed or metastatic NPC and its acceptable safety profile in the
later-line setting (59). In
locally advanced NPC, the combination of cetuximab and cisplatin
with intensity-modulated radiation therapy (IMRT) is also expected
to improve survival rates in patients with NPC (60). However, a recent study (61) found that the overexpression of the
complement regulatory protein CD55 in EBV-associated NPC cells
suppressed ADCC activity, thus reducing the efficacy of cetuximab.
This explains why some patients exhibit poor therapeutic outcomes
and provides a direction for overcoming resistance whereby
downregulating CD55 expression or combining with complement
inhibitors may restore the ADCC effect of cetuximab, offering a new
target for precision-targeted therapy.
Nimotuzumab
Nimotuzumab is a humanized monoclonal antibody
targeting EGFR, which inhibits tumor cell proliferation and
promotes apoptosis. Several clinical studies have reported clinical
benefits of nimotuzumab combined with chemotherapy vs. chemotherapy
alone as first-line treatment for R/M-NPC (62–64). A
recent Phase II clinical study on nimotuzumab combined with
docetaxel and cisplatin as first-line therapy for patients with
R/M-NPC (65) found that the ORR
and DCR were 65.4 and 90.4%, respectively. The majority of adverse
events were grade 1–2. Grade 3/4 adverse events were primarily
hematologic toxicities, including neutropenia and leukopenia.
Overall, these were manageable, with no unexpected severe adverse
reactions observed. These findings suggest promising efficacy,
along with satisfactory tolerability and safety profiles, providing
a potential treatment option for first-line therapy in R/M-NPC that
balances both efficacy and safety.
Becotatug vedotin
Becotatug vedotin (MRG003) is China's first
EGFR-targeted ADC. It consists of an anti-EGFR humanized monoclonal
antibody conjugated with the cytotoxic drug monomethyl auristatin E
via a cleavable linker VC. In 2022, results from a non-randomized
clinical trial (66) indicated that
MRG003 demonstrated controllable safety characteristics and
promising antitumor activity in patients with EGFR-positive NPC and
SCCHN (Squamous Cell Carcinoma of the Head and Neck). A 2023 study
further highlighted that MRG003 exhibited satisfactory
tolerability, manageable safety and showed promising efficacy in
patients with 2nd/3rd-line recurrent/metastatic SCCHN who had
failed prior platinum-based and PD-1/L1 inhibitor treatments
(67). A Phase II clinical study
presented at the 2024 European Society for Medical Oncology Asia
Annual Meeting (68) showed that
among 30 patients, two achieved complete remission, 18 achieved
partial remission and eight had stable disease, with a DCR of
93.3%. The 6-month PFS was 76.2 and 83.3% of patients had a
duration of remission lasting >6 months.
At the 2025 American Society of Clinical Oncology
Annual Meeting (69), the results
of a Phase IIb clinical study of the EGFR ADC MRG003 for treating
advanced NPC were presented. The study involved patients with
R/M-NPC who had failed at least two lines of systemic chemotherapy
and PD-L1 inhibitor treatment. Patients were randomly assigned to
receive MRG003 or chemotherapy (capecitabine or docetaxel). As of
June 30, 2024, the ORR in the MRG003 group was significantly
superior to that of the chemotherapy group, with a marked reduction
in the risk of disease progression and a substantial improvement in
PFS. In addition, a clear trend toward survival benefit was
observed in OS, particularly after excluding the interference of
crossover treatments, where this advantage became even more
pronounced. These results indicate that MRG003 has shown a trend
toward survival benefit.
BL-B01D1
BL-B01D1 is the first EGFR-HER3 bispecific ADC,
designed to specifically bind to EGFR or HER3 on the surface of
tumor cells. In a Phase I clinical trial (70), BL-B01D1 showed preliminary antitumor
activity and acceptable safety in patients with extensively treated
advanced solid tumors. A study in 2024 found that BL-B01D1
monotherapy achieved an ORR of 54% in NPC (71). Recently, the Phase III clinical
trial of the EGFR/HER3 bispecific ADC, izalontamab brengitecan
(iza-bren; BL-B01D1) for NPC (study code: BL-B01D1-303) met its
primary endpoint in an interim analysis, making it the first
bispecific ADC drug to complete phase III studies worldwide. The
results showed that, compared with chemotherapy, iza-bren
significantly improved the ORR in patients with R/M-NPC, with a
manageable safety profile. These findings suggest that BL-B01D1 may
represent a novel therapeutic direction for this patient population
(72).
In addition to directly inhibiting tumor cell
proliferation, EGFR inhibitors can also influence the tumor immune
microenvironment [including increased expression of MHC class I
(73) and class II molecules
(74) on tumor cells], thereby
enhancing tumor antigen presentation. Due to these effects, EGFR
inhibitors can transform an immunosuppressive TME into an
immune-activated one, notably improving the effectiveness of
immunotherapies. Some studies suggest (75,76)
that EGFR-driven tumors may also induce the expression of PD-L1,
which, when bound to PD-1, increases inhibitory signals. This may
lead to the suppression of CD8+ T cells expressing PD-1
receptors, hindering their immune response against tumor cells.
Given these effects, combining anti-PD-L1 antibodies with EGFR
inhibitors for NPC is a promising strategy.
EGFR-TKIs
EGFR-TKIs achieve targeted therapy by blocking the
binding of ATP to the intracellular tyrosine kinase domain of EGFR.
Gefitinib, a first-generation EGFR-TKI, a small molecule inhibitor,
has been shown to exhibit intrinsic resistance in most NPC cell
lines (77). A Phase II study
reported that none of the patients with recurrent or metastatic NPC
achieved clinical remission after gefitinib treatment, thus it is
not recommended for use in NPC outside of clinical trials (78). However, other studies have suggested
that EGFR-TKI treatment may increase PD-L1 expression in immune
cells, making them more responsive to subsequent ICIs, indicating
that EGFR-TKI treatment may influence the TME and produce favorable
effects on ICI efficacy (79,80).
Anti-angiogenesis pathway
VEGF is a growth factor with angiogenic activity
that promotes mitosis and inhibits apoptosis in endothelial cells,
increases vascular permeability and facilitates cell migration. Due
to these effects, VEGF plays a crucial role in regulating both
normal and pathological angiogenesis processes. Studies have shown
that VEGF plays an essential role in the molecular pathogenesis of
tumor growth and metastasis (81).
VEGF-induced abnormal vascular structures compromise tumor vessel
integrity, making it difficult for T cells and DCs to infiltrate
tumor tissue. Additionally, VEGF can directly inhibit DC
maturation, reducing the presentation of tumor antigens to T cells
and hindering the initiation of immune responses. It also promotes
the expression of PD-L1 and recruits MDSCs, thereby exacerbating
immune evasion (82) and reducing
the efficacy of checkpoint inhibitors. Various angiogenesis
inhibitors are available for treating different types of advanced
solid tumors. Numerous current treatment approaches target one or
more VEGF subtypes, VEGF receptors or signaling pathways (83). Bevacizumab is an anti-VEGF-A drug,
and the first humanized anti-angiogenic antibody approved for the
treatment of colorectal cancer. Bevacizumab is now widely used for
the treatment of NPC. A meta-analysis has shown that, among
multiple clinical studies included, bevacizumab was the most
effective treatment for achieving partial response in NPC (80.6%),
followed by standard cancer treatments (57%), cetuximab (51.5%),
nimotuzumab (31.2%) and Endostar (29.7%) (84).
In addition to its direct role in angiogenesis and
tumor growth, VEGF can also induce immune suppression within the
TME (85). It can suppress T-cell
function, increase the recruitment of regulatory T cells (Tregs)
and MDSCs, and inhibit the differentiation and activation of DCs.
When VEGF levels are elevated within the TME, it further stimulates
the proliferation of MDSCs and Tregs, increases VEGFR expression
and inhibits T-cell activity via VEGF/VEGFR signaling. This change
in the TME can, to some extent, enhance the effectiveness of
immunotherapy. A preclinical study demonstrated that anti-VEGF
therapy could improve the effectiveness of anti-PD-L1 treatment by
improving vascular conditions. Simultaneously, anti-PD-1 or
anti-PD-L1 therapies could also make anti-angiogenesis therapies
more sensitive and extend their therapeutic effects (86). Furthermore, some studies have shown
that, in various models, the use of bispecific anti-angiogenesis
therapy could promote T-cell extravasation from tumor vessels
(87,88). It could also reduce inhibitory
factors on innate immune cells or those derived from innate immune
cells, promoting the establishment and development of antitumor
immunity, thus enhancing the activity of anti-PD-L1 treatment
(89).
Similarities between the EGFR and VEGF
pathways
Although the EGFR and VEGF pathways target different
molecules, they share key overlaps in regulating tumor immune
evasion and the TME. Both pathways activate downstream PI3K and ERK
signaling (Fig. 2), leading to
upregulation of immune checkpoint molecules such as PD-L1 on tumor
cells. Additionally, both pathways induce tumor cells to secrete
factors such as IL-10 and TGF-β, which recruit Tregs, MDSCs and M2
macrophages, thereby promoting immune suppression within the TME
and facilitating immune evasion. Furthermore, there is
cross-activation between the two pathways, whereby the EGFR pathway
can indirectly promote VEGF transcription through downstream
signals, while VEGF pathway activation can enhance EGFR
phosphorylation, collectively driving tumor angiogenesis and immune
evasion.
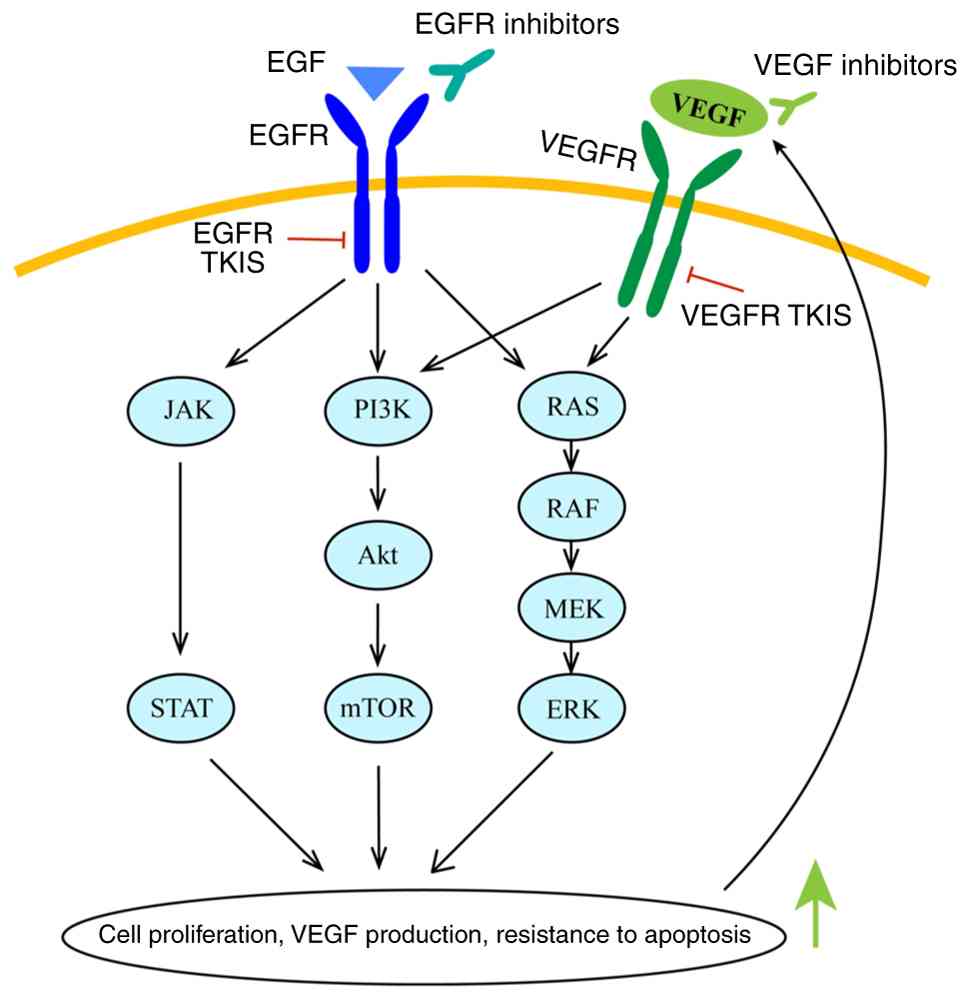 | Figure 2.Upon activation by EGF, EGFR promotes
cell proliferation, VEGF production and anti-apoptotic activity
through the JAK/STAT, PI3K/Akt/mTOR and RAS/RAF/MEK/ERK pathways.
VEGF activates VEGFR and shares these downstream signals. EGFR
inhibitors/TKIs can block EGFR activation, while VEGF
inhibitors/VEGFR TKIs inhibit the interaction between VEGF and
VEGFR. The combination of these inhibitors can simultaneously block
the upstream signaling of both pathways, synergistically
suppressing tumor progression and delaying resistance. EGF,
epidermal growth factor; EGFR, epidermal growth factor receptor;
VEGF, vascular endothelial growth factor; VEGFR, vascular
endothelial growth factor receptor; TKIs, tyrosine kinase
inhibitors. |
Recombinant human endostatin
Endostar is a recombinant human endostatin that
directly inhibits endothelial cell proliferation and suppresses
tumor development through multiple targets, thus exerting its
antitumor effects. These targets include VEGF, VEGFR-2 and
platelet-derived growth factor receptor (90). Additionally, Endostar notably
increases the percentage of basal membrane and pericyte coverage.
It normalizes the tumor vasculature by reducing interstitial fluid
pressure and vascular permeability, which in turn reduces tumor
hypoxia and alters the vascular physiology within the tumor.
Alleviating tumor hypoxia and improving vascular delivery may
enhance the cytotoxic effects of chemotherapy drugs and ionizing
radiation (91,92). Several Phase II clinical trials have
confirmed that Endostar combined with chemotherapy is a safe and
effective treatment for NPC and head and neck squamous cell
carcinoma (93,94). The latest study indicated that, in
patients with locally advanced NPC, Endostar combined with
cisplatin and 5-fluorouracil chemotherapy and sequential IMRT
significantly improved PFS (Endostar group, 25.6 months; control
group without Endostar, 21.4 months) (95). The combination of Endostar and
immunotherapy may be a promising strategy for treating NPC,
although further investigation is required.
Combination strategies: Immunotherapy plus
targeted therapy
The combination of immunotherapy and targeted
therapy represents a key breakthrough in the treatment of malignant
tumors, with both modalities synergistically reshaping the
antitumor immune response to enhance clinical benefits. Targeted
therapies, such as anti-angiogenic agents, remodel tumor
vasculature, improve oxygen supply and reduce PD-L1 expression,
while also inhibiting the functions of immunosuppressive cells such
as Tregs and MDSCs, and downregulating immune checkpoint molecules.
Additionally, targeted therapies induce tumor metabolic stress,
recruit CD8+ T cells and NK cells, and enhance their
cytotoxic activity, thus creating a favorable environment for
immunotherapy. Immunotherapy, in turn, strengthens the antigen
presentation induced by tumor immunogenic cell death through
targeted drugs, complementing the cytotoxic effects of targeted
therapies. It also induces stem cell-like memory T cells, enabling
long-term tumor control. Together, these treatments reduce
resistance, with immunotherapy clearing targeted-resistant cells
and targeted therapy restoring exhausted T cell function. This
combined approach inhibits tumor immune evasion and modulates the
cytokine network, further reducing the risk of resistance.
Numerous clinical studies have confirmed the
clinical value of this immunotherapy-targeted therapy combination
strategy (Table III). For
example, a recent Phase II study demonstrated that the combination
of toripalimab and anlotinib in the treatment of R/M-NPC achieved a
notable ORR of 37.5% and a DCR of 85.0%, with favorable
tolerability. The study also indicated that the response of plasma
circulating tumor DNA (ctDNA) correlates with efficacy, and ctDNA
may serve as a potential biomarker for predicting the treatment
response of this combination regimen (96). Several clinical trials have shown
promising treatment outcomes for the combination of camrelizumab
and apatinib in NPC. A Phase II study in 2023 (97) demonstrated notable disease control
in patients with platinum-resistant R/M-NPC, with survival benefits
even in those resistant to PD-1 inhibitors. Another Phase II study
in the same year (98) demonstrated
that the combination of camrelizumab and apatinib in patients with
R/M-NPC resulted in a median follow-up duration of 16 months, with
an ORR of 38.5%, a DCR of 61.5%, a mPFS of 6 months and a mOS of 14
months, indicating promising antitumor activity and manageable
toxicity. In 2024, a study further combined this regimen with
chemotherapy in patients with N3-stage NPC, achieving excellent
control of distant metastasis, with the safety profile remaining
within acceptable limits (99). A
recent study involving pembrolizumab, with or without bevacizumab
(100), directly confirmed the
advantage of combination therapy, with the ORR significantly higher
in the pembrolizumab and bevacizumab group compared with
pembrolizumab monotherapy, clearly demonstrating the synergistic
effect of anti-angiogenic drugs and PD-1 inhibitors. Additionally,
the combination of PD-1 inhibitors with other targeted therapies
has shown population-specific benefits. Toripalimab combined with
GFH018 (101) in previously
treated patients with R/M-NPC resulted in an ORR of 26.1%, a DCR of
43.5%, a mPFS of 2.0 months and a median duration of response of
7.6 months. Notably, patients who had not been previously treated
with ICIs exhibited significantly improved efficacy, with
substantial improvements in ORR, DCR and PFS, while even
ICI-treated patients achieved some disease control. Overall, the
toxicity was manageable, and there was persistent antitumor
activity.
| Table III.List of Phase II/III clinical trials
for immunotherapy combined with targeted therapy in NPC. |
Table III.
List of Phase II/III clinical trials
for immunotherapy combined with targeted therapy in NPC.
| First author/s,
year | Drugs | Targets | Study design | Disease
setting | n | Outcomes | Phase | (Refs.) |
|---|
| Yuan et al,
2023 | Camrelizumab and
apatinib | PD-1 and
VEGFR2 | Single-arm,
camrelizumab plus apatinib | R/M-NPC,
platinum-resistant and PD-1 inhibitor resistant | 72 | Platinum-resistant,
median follow-up time, 23.3 months; mPFS, 12.6 months; 1-year OS,
82.5%; mOS, NA; PD-1 inhibitor resistant ORR, 34.3%; mPFS, 4.5
months; mOS, 16.2 months; 1-year OS, 68.8% | II | (97) |
| Mo et al,
2023 | Camrelizumab and
apatinib | PD-1 and
VEGFR2 | Multicenter,
open-label, single-arm, apatinib combined with camrelizumab | R/M-NPC, at least
to 1 standard therapy | 26 | Median follow-up
duration, 16 months; ORR, 38.5%; DCR, 61.5%; mPFS, 6 months; mOS,
14 months | II | (98) |
| Liang et al,
2024 | Camrelizumab and
apatinib | PD-1 and
VEGFR2 | Open-label,
single-arm, camrelizumab and apatinib plus chemoradiotherapy | Stage N3 NPC | 49 | Both 1- and 2-year
DMFS rates, 98.0%; 2-year FFS, 95.9%; OS, 98.0%. | II | (99) |
| Zhang et al,
2024 | Toripalimab and
anlotinib | PD-1 and VEGFR | Multicenter,
single-arm, toripalimab plus anlotinib | R/M-NPC | 40 | Median follow-up,
17.4 months; mPFS, 9.5 months; 1-year OS, 73.3% | II | (96) |
| Chong et al,
2025 | Pembrolizumab and
bevacizumab | PD-1 and VEGF | Randomized,
open-label, pembrolizumab with or without bevacizumab | R/M-NPC | 48 | Bevacizumab and
pembrolizumab group ORR, 58.3%; pembrolizumab group ORR,
12.5%. | II | (100) |
| Tang et al,
2025 | Toripalimab and
GFH018 | PD-1 and
TGFβRI | Multinational,
open-label and single-arm, GFH018 and toripalimab combination
therapy | R/M-NPC, at least
to 1 standard therapy | 46 | ORR, 26.1%; DCR,
43.5%; mPFS, 2.0 months; median DOR, 7.6 months; without prior ICI
treatment: ORR 40%, DCR 60%, mPFS 9.0 months, median DOR was not
reached; previously exposed to ICIs: ORR 9.5%, DCR 23.8% | Ib/II | (101) |
In summary, the trend towards combining
immunotherapy and targeted therapy in NPC is clear. The synergistic
action between PD-1 inhibitors and anti-angiogenic drugs can
effectively improve disease control, with notable population
heterogeneity in treatment efficacy. The exploration of biomarkers,
such as ctDNA, holds promise for the precise selection of patients
who may benefit. This combined strategy not only overcomes the
efficacy limitations of monotherapy but also expands the research
direction for precision treatment in NPC, providing personalized
therapeutic options for patients with different clinical
profiles.
Future directions
NPC, a malignancy with notable geographic
clustering, exhibits highly heterogeneous biological behavior and
is closely related to EBV infection, epigenetic changes and
abnormal molecular signaling pathways. Precision-targeted
strategies based on tumor cell surface receptors (such as EGFR),
key angiogenesis factors (such as VEGF) and virus-associated
antigens have become an important direction to overcome the
limitations of traditional chemotherapy and radiotherapy.
Additionally, the deconstruction of the immune-suppressive network
in the TME provides a key entry point for immunotherapy. Therefore,
integrating tumor pathological classification
(keratinizing/non-keratinizing), EBV viral load, molecular markers
and immune infiltration characteristics is the core prerequisite
for achieving precision treatment.
In the field of targeted therapy, monoclonal
antibodies targeting EGFR (such as nimotuzumab) combined with
chemotherapy and radiotherapy have become the standard treatment
for locally advanced NPC, notably improving local control rates.
Anti-angiogenesis agents (such as bevacizumab) exhibit efficacy in
delaying disease progression in recurrent and metastatic patients
by blocking the VEGF pathway. In terms of immunotherapy, PD-1
inhibitors play a key role in activating T cell responses triggered
by EBV-associated tumor antigens. Single-agent or combination
therapies with chemotherapy or anti-angiogenesis agents have
demonstrated nearly a 30% improvement in ORRs compared with
traditional chemotherapy, particularly in patients that are
PD-L1-positive (CPS ≥10) or have a high tumor mutation burden. Some
of these regimens have already been recommended in international
guidelines.
However, current treatments still face several
challenges. Firstly, targeted therapies often encounter resistance
due to compensatory activation of the EGFR pathway, tumor vascular
heterogeneity and other issues. In addition, immunotherapy is only
effective for ~40% of patients, and EBV-mediated immune escape and
regulatory T cell infiltration in the TME may weaken efficacy. A
promising development is the combination of targeted therapy with
immunotherapy. For example, EGFR inhibitors can enhance T cell
eliminating activity by downregulating PD-L1 expression, while the
combination of CTLA-4 inhibitors and PD-1 inhibitors has shown
synergistic antitumor effects in clinical studies by dual
checkpoint blockade.
Future clinical research is likely to focus more on
the comprehensive analysis of genomics, viral immunology and
dynamic changes in the immune microenvironment, strengthening the
development of novel immunotherapies targeting EBV-specific
antigens and tumor stem cell targets, and screening biomarkers to
identify the patient population that would benefit most. With the
clinical application of various immune inhibitors and the
continuous development of novel therapeutic targets, clinical
translation of cutting-edge technologies such as bispecific
antibodies and adoptive cell therapy, NPC treatment is hypothesized
to move from the current model of personalized targeted and
immunotherapy towards a combination of targeted immunotherapy.
Ultimately, this may lead to a new era of precise targeting and
immune modulation in NPC therapy.
Conclusion
Current research has demonstrated notable progress
in the development and application of targeted therapy and
immunotherapy for NPC. Molecular-targeted drugs targeting key
pathways such as EGFR and VEGF/VEGFR, as well as ICIs targeting
PD-1/PD-L1 or CTLA-4, have shown clinically meaningful efficacy and
controllable safety in the treatment of locally advanced and
R/M-NPC. The combination of these novel therapies with standard CRT
is changing the treatment landscape.
However, numerous challenges remain. Primary and
acquired resistance to targeted therapy and immunotherapy limit the
long-term effectiveness of these treatments, with only ~40% of
patients achieving notable benefit from ICIs. There is an urgent
need for predictive biomarkers beyond PD-L1 expression (CPS) and
tumor mutational burden to improve identification of the
appropriate patient populations. Although prospects are promising,
numerous new approaches still need to be further validated in
large-scale, randomized phase III trials.
In conclusion, the era of precision oncology for NPC
is rapidly advancing, with the successful integration of targeted
therapy and immunotherapy. With strong guidance from reliable
biomarkers and individualized based on tumor biology, these
strategies may offer new opportunities to improve survival outcomes
for patients with NPC at various stages.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
Not applicable.
Authors' contributions
ZY and HL wrote this manuscript. MC, LZ and MG
collected information, revised the manuscript finally and provided
some critical suggestions. RY provided general supervision and gave
final approval of the manuscript. All authors read and approved the
final version of the manuscript. Data authentication is not
applicable.
Ethics approval and consent to
participate
Not applicable.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Wang HY, Chang YL, To KF, Hwang JS, Mai
HQ, Feng YF, Chang ET, Wang CP, Kam MK, Cheah SL, et al: A new
prognostic histopathologic classification of nasopharyngeal
carcinoma. Chin J Cancer. 35:412016. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Chua MLK, Wee JTS, Hui EP and Chan ATC:
Nasopharyngeal carcinoma. Lancet. 387:1012–1024. 2016. View Article : Google Scholar
|
|
3
|
Chen YP, Chan ATC, Le QT, Blanchard P, Sun
Y and Ma J: Nasopharyngeal carcinoma. Lancet. 394:64–80. 2019.
View Article : Google Scholar
|
|
4
|
Filho AM, Laversanne M, Ferlay J, Colombet
M, Piñeros M, Znaor A, Parkin DM, Soerjomataram I and Bray F: The
GLOBOCAN 2022 cancer estimates: Data sources, methods, and a
snapshot of the cancer burden worldwide. Int J Cancer.
156:1336–1346. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Jen CW, Tsai YC, Wu JS, Chen PL, Yen JH,
Chuang WK and Cheng SHC: Prognostic classification for patients
with nasopharyngeal carcinoma based on American Joint Committee on
cancer staging system T and N categories. Ther Radiol Oncol.
4:22020. View Article : Google Scholar
|
|
6
|
Zhang L, Huang Y, Hong S, Yang Y, Yu G,
Jia J, Peng P, Wu X, Lin Q, Xi X, et al: Gemcitabine plus cisplatin
versus fluorouracil plus cisplatin in recurrent or metastatic
nasopharyngeal carcinoma: A multicentre, randomised, open-label,
phase 3 trial. Lancet. 388:1883–1892. 2016. View Article : Google Scholar
|
|
7
|
Lee AWM, Ng WT, Chan JYW, Corry J, Mäkitie
A, Mendenhall WM, Rinaldo A, Rodrigo JP, Saba NF, Strojan P, et al:
Management of locally recurrent nasopharyngeal carcinoma. Cancer
Treat Rev. 79:1018902019. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bossi P, Chan AT, Licitra L, Trama A,
Orlandi E, Hui EP, Halámková J, Mattheis S, Baujat B, Hardillo J,
et al: Nasopharyngeal carcinoma: ESMO-EURACAN clinical practice
guidelines for diagnosis, treatment and follow-up†. Ann Oncol.
32:452–465. 2021. View Article : Google Scholar
|
|
9
|
Hong S, Zhang Y, Yu G, Peng P, Peng J, Jia
J, Wu X, Huang Y, Yang Y, Lin Q, et al: Gemcitabine plus cisplatin
versus fluorouracil plus cisplatin as first-line therapy for
recurrent or metastatic nasopharyngeal carcinoma: Final overall
survival analysis of GEM20110714 phase III study. J Clin Oncol.
39:3273–3282. 2021. View Article : Google Scholar
|
|
10
|
Chen P, Liu B, Xia X, Huang P and Zhao J:
Current progress in immunotherapy of nasopharyngeal carcinoma. Am J
Cancer Res. 13:1140–1147. 2023.PubMed/NCBI
|
|
11
|
Liu X, Shen H, Zhang L, Huang W, Zhang S
and Zhang B: Immunotherapy for recurrent or metastatic
nasopharyngeal carcinoma. NPJ Precis Oncol. 8:1012024. View Article : Google Scholar
|
|
12
|
Kang Y, He W, Ren C, Qiao J, Guo Q, Hu J,
Xu H, Jiang X and Wang L: Advances in targeted therapy mainly based
on signal pathways for nasopharyngeal carcinoma. Signal Transduct
Target Ther. 5:2452020. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Kang Y, He W, Ren C, Qiao J, Guo Q, Hu J,
Xu H, Jiang X and Wang L: Correction: Advances in targeted therapy
mainly based on signal pathways for nasopharyngeal carcinoma.
Signal Transduct Target Ther. 5:2652020. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Kim J, Lee Y, Kim S and Park JC: Novel
therapeutic development for nasopharyngeal carcinoma. Curr Oncol.
32:4792025. View Article : Google Scholar
|
|
15
|
Morad G, Helmink BA, Sharma P and Wargo
JA: Hallmarks of response, resistance, and toxicity to immune
checkpoint blockade. Cell. 184:5309–5337. 2021. View Article : Google Scholar
|
|
16
|
Liu SL, Li XY, Yang JH, Wen DX, Guo SS,
Liu LT, Li YF, Luo MJ, Xie SY, Liang YJ, et al: Neoadjuvant and
adjuvant toripalimab for locoregionally advanced nasopharyngeal
carcinoma: A randomised, single-centre, double-blind,
placebo-controlled, phase 2 trial. Lancet Oncol. 25:1563–1575.
2024. View Article : Google Scholar
|
|
17
|
Mai HQ, Chen QY, Chen D, Hu C, Yang K, Wen
J, Li J, Shi Y, Jin F, Xu R, et al: Toripalimab plus chemotherapy
for recurrent or metastatic nasopharyngeal carcinoma: The
JUPITER-02 randomized clinical trial. JAMA. 330:1961–1970. 2023.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Yang Y, Qu S, Li J, Hu C, Xu M, Li W, Zhou
T, Shen L, Wu H, Lang J, et al: Camrelizumab versus placebo in
combination with gemcitabine and cisplatin as first-line treatment
for recurrent or metastatic nasopharyngeal carcinoma (CAPTAIN-1st):
A multicentre, randomised, double-blind, phase 3 trial. Lancet
Oncol. 22:1162–1174. 2021. View Article : Google Scholar
|
|
19
|
Liang YL, Liu X, Shen LF, Hu GY, Zou GR,
Zhang N, Chen CB, Chen XZ, Zhu XD, Yuan YW, et al: Adjuvant PD-1
blockade with camrelizumab for nasopharyngeal carcinoma: The DIPPER
randomized clinical trial. JAMA. 333:1589–1598. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Lee A and Keam SJ: Tislelizumab: First
approval. Drugs. 80:617–624. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Yang Y, Pan J, Wang H, Zhao Y, Qu S, Chen
N, Chen X, Sun Y, He X, Hu C, et al: Tislelizumab plus chemotherapy
as first-line treatment for recurrent or metastatic nasopharyngeal
cancer: A multicenter phase 3 trial (RATIONALE-309). Cancer Cell.
41:1061–1072.e4. 2023. View Article : Google Scholar
|
|
22
|
Lu Z, Wang J, Shu Y, Liu L, Kong L, Yang
L, Wang B, Sun G, Ji Y, Cao G, et al: Sintilimab versus placebo in
combination with chemotherapy as first line treatment for locally
advanced or metastatic oesophageal squamous cell carcinoma
(ORIENT-15): Multicentre, randomised, double blind, phase 3 trial.
BMJ. 377:e0687142022. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu X, Zhang Y, Yang KY, Zhang N, Jin F,
Zou GR, Zhu XD, Xie FY, Liang XY, Li WF, et al:
Induction-concurrent chemoradiotherapy with or without sintilimab
in patients with locoregionally advanced nasopharyngeal carcinoma
in China (CONTINUUM): A multicentre, open-label, parallel-group,
randomised, controlled, phase 3 trial. Lancet. 403:2720–2731. 2024.
View Article : Google Scholar
|
|
24
|
Ma BBY, Lim WT, Goh BC, Hui EP, Lo KW,
Pettinger A, Foster NR, Riess JW, Agulnik M, Chang AYC, et al:
Antitumor activity of nivolumab in recurrent and metastatic
nasopharyngeal carcinoma: An international, multicenter study of
the Mayo clinic phase 2 consortium (NCI-9742). J Clin Oncol.
36:1412–1418. 2018. View Article : Google Scholar
|
|
25
|
Jung HA, Park KU, Cho S, Lim J, Lee KW,
Hong MH, Yun T, An HJ, Park WY, Pereira S, et al: A phase II study
of nivolumab plus gemcitabine in patients with recurrent or
metastatic nasopharyngeal carcinoma (KCSG HN17-11). Clin Cancer
Res. 28:4240–4247. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Xu C, Zhou GQ, Li WF, Hu DS, Chen XZ, Lin
SJ, Jin F, Huang XQ, Peng G, Huang J, et al: Nivolumab combined
with induction chemotherapy and radiotherapy in nasopharyngeal
carcinoma: A multicenter phase 2 PLATINUM trial. Cancer Cell.
43:925–936.e4. 2025. View Article : Google Scholar
|
|
27
|
Hsu C, Lee SH, Ejadi S, Even C, Cohen RB,
Le Tourneau C, Mehnert JM, Algazi A, van Brummelen EMJ, Saraf S, et
al: Safety and antitumor activity of pembrolizumab in patients with
programmed death-ligand 1-positive nasopharyngeal carcinoma:
Results of the KEYNOTE-028 study. J Clin Oncol. 35:4050–4056. 2017.
View Article : Google Scholar
|
|
28
|
Chan ATC, Lee VHF, Hong RL, Ahn MJ, Chong
WQ, Kim SB, Ho GF, Caguioa PB, Ngamphaiboon N, Ho C, et al:
Pembrolizumab monotherapy versus chemotherapy in
platinum-pretreated, recurrent or metastatic nasopharyngeal cancer
(KEYNOTE-122): An open-label, randomized, phase III trial. Ann
Oncol. 34:251–261. 2023. View Article : Google Scholar
|
|
29
|
Shi Y, Qin X, Peng X, Zeng A, Li J, Chen
C, Qiu S, Pan S, Zheng Y, Cai J, et al: Efficacy and safety of
KL-A167 in previously treated recurrent or metastatic
nasopharyngeal carcinoma: A multicenter, single-arm, phase 2 study.
Lancet Reg Health West Pac. 31:1006172022.
|
|
30
|
Li Y, Min Y, Wei Z, Liu Z, Pei Y, Yang Y,
Gao K, Song G, Xu S, He S, et al: Metastatic sites of baseline as
predictors in recurrent or metastatic nasopharyngeal carinoma
treated with PD-L1 inhibitor: A secondary analysis of multicenter,
single-arm, phase II study (KL-A167). Cancer Immunol Immunother.
74:722025. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Li Y, Min Y, Wei Z, Liu Z, Pei Y, Yang Y,
Gao K, Song G, Xu S, He S, et al: Correction: Metastatic sites of
baseline as predictors in recurrent or metastatic nasopharyngeal
carinoma treated with PD-L1 inhibitor: A secondary analysis of
multicenter, single-arm, phase II study (KL-A167). Cancer Immunol
Immunother. 74:3222025. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Zhang H, Dai Z, Wu W, Wang Z, Zhang N,
Zhang L, Zeng WJ, Liu Z and Cheng Q: Regulatory mechanisms of
immune checkpoints PD-L1 and CTLA-4 in cancer. J Exp Clin Cancer
Res. 40:1842021. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Rowshanravan B, Halliday N and Sansom DM:
CTLA-4: A moving target in immunotherapy. Blood. 131:58–67. 2018.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Lim DWT, Kao HF, Suteja L, Li CH, Quah HS,
Tan DSW, Tan SH, Tan EH, Tan WL, Lee JN, et al: Clinical efficacy
and biomarker analysis of dual PD-1/CTLA-4 blockade in
recurrent/metastatic EBV-associated nasopharyngeal carcinoma. Nat
Commun. 14:27812023. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Ma Y, Zhou H, Luo F, Zhang Y, Zhu C, Li W,
Huang Z, Zhao J, Xue J, Zhao Y, et al: Remodeling the tumor-immune
microenvironment by anti-CTLA4 blockade enhanced subsequent
anti-PD-1 efficacy in advanced nasopharyngeal carcinoma. NPJ Precis
Oncol. 8:652024. View Article : Google Scholar
|
|
36
|
Jiang Y, Bei W, Wang L, Lu N, Xu C, Liang
H, Ke L, Ye Y, He S, Dong S, et al: Efficacy and safety of
cadonilimab (PD-1/CTLA-4 bispecific) in combination with
chemotherapy in anti-PD-1-resistant recurrent or metastatic
nasopharyngeal carcinoma: A single-arm, open-label, phase 2 trial.
BMC Med. 23:1522025. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Chen QY, Guo SS, Luo Y, Qu S, Wu DH, Chen
XZ, Chen DP, Qin XT, Lin Q, Jin F, et al: Efficacy and safety of
cadonilimab in previously treated recurrent or metastatic
nasopharyngeal carcinoma(COMPASSION-06): A phase II multicenter
study. Oral Oncol. 151:1067232024. View Article : Google Scholar
|
|
38
|
Cao F, Li Y, Fang Q, Lin R, Zhao Z, Xu P,
Yan H, Zhang X, Jiang K, Zhou J, et al: Cadonilimab (a PD-1/CTLA-4
bispecific antibody) plus neoadjuvant chemotherapy in locally
advanced head and neck squamous cell carcinoma: A phase II clinical
trial. Clin Cancer Res. 31:3876–3885. 2025. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Meij P, Leen A, Rickinson AB, Verkoeijen
S, Vervoort MBHJ, Bloemena E and Middeldorp JM: Identification and
prevalence of CD8(+) T-cell responses directed against Epstein-Barr
virus-encoded latent membrane protein 1 and latent membrane protein
2. Int J Cancer. 99:93–99. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Comoli P, Pedrazzoli P, Maccario R, Basso
S, Carminati O, Labirio M, Schiavo R, Secondino S, Frasson C,
Perotti C, et al: Cell therapy of stage IV nasopharyngeal carcinoma
with autologous Epstein-Barr virus-targeted cytotoxic T
lymphocytes. J Clin Oncol. 23:8942–8949. 2005. View Article : Google Scholar
|
|
41
|
Chia WK, Teo M, Wang WW, Lee B, Ang SF,
Tai WM, Chee CL, Ng J, Kan R, Lim WT, et al: Adoptive T-cell
transfer and chemotherapy in the first-line treatment of metastatic
and/or locally recurrent nasopharyngeal carcinoma. Mol Ther.
22:132–139. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Toh HC, Yang MH, Wang HM, Hsieh CY,
Chitapanarux I, Ho KF, Hong RL, Ang MK, Colevas AD, Sirachainan E,
et al: Gemcitabine, carboplatin, and Epstein-Barr virus-specific
autologous cytotoxic T lymphocytes for recurrent or metastatic
nasopharyngeal carcinoma: VANCE, an international randomized phase
III trial. Ann Oncol. 35:1181–1190. 2024. View Article : Google Scholar
|
|
43
|
Looi CK, Loo EM, Lim HC, Chew YL, Chin KY,
Cheah SC, Goh BH and Mai CW: Revolutionizing the treatment for
nasopharyngeal cancer: The impact, challenges and strategies of
stem cell and genetically engineered cell therapies. Front Immunol.
15:14845352024. View Article : Google Scholar
|
|
44
|
Jackson HJ, Rafiq S and Brentjens RJ:
Driving CAR T-cells forward. Nat Rev Clin Oncol. 13:370–383. 2016.
View Article : Google Scholar
|
|
45
|
Zhang H, Yang L, Wang T and Li Z: NK
cell-based tumor immunotherapy. Bioact Mater. 31:63–86.
2023.PubMed/NCBI
|
|
46
|
Lim CM, Liou A, Poon M, Koh LP, Tan LK,
Loh KS, Petersson BF, Ting E, Campana D, Goh BC and Shimasaki N:
Phase I study of expanded natural killer cells in combination with
cetuximab for recurrent/metastatic nasopharyngeal carcinoma. Cancer
Immunol Immunother. 71:2277–2286. 2022. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Pan K, Farrukh H, Chittepu VCSR, Xu H, Pan
CX and Zhu Z: CAR race to cancer immunotherapy: From CAR T, CAR NK
to CAR macrophage therapy. J Exp Clin Cancer Res. 41:1192022.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Liao Y, Yan J, Beri NR, Giulino-Roth L,
Cesarman E and Gewurz BE: Germinal center cytokine driven
epigenetic control of Epstein-Barr virus latency gene expression.
PLoS Pathog. 20:e10119392024. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Sayour EJ, Boczkowski D, Mitchell DA and
Nair SK: Cancer mRNA vaccines: Clinical advances and future
opportunities. Nat Rev Clin Oncol. 21:489–500. 2024. View Article : Google Scholar
|
|
50
|
Guo M, Duan X, Peng X, Jin Z, Huang H,
Xiao W, Zheng Q, Deng Y, Fan N, Chen K and Song X: A lipid-based
LMP2-mRNA vaccine to treat nasopharyngeal carcinoma. Nano Res.
16:5357–5367. 2023. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Xiang Y, Tian M, Huang J, Li Y, Li G, Li
X, Jiang Z, Song X and Ma X: LMP2-mRNA lipid nanoparticle
sensitizes EBV-related tumors to anti-PD-1 therapy by reversing T
cell exhaustion. J Nanobiotechnology. 21:3242023. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Huang K, Lin XJ, Hu JC, Xia TY, Xu FP,
Huang JD and Zhou N: Epstein-Barr virus mRNA vaccine synergizes
with NK cells to enhance nasopharyngeal carcinoma eradication in
humanized mice. Mol Ther Oncol. 33:2009862025. View Article : Google Scholar
|
|
53
|
Li H, Min L, Du H, Wei X and Tong A:
Cancer mRNA vaccines: Clinical application progress and challenges.
Cancer Lett. 625:2177522025. View Article : Google Scholar
|
|
54
|
Liu Q, Yu S, Zhao W, Qin S, Chu Q and Wu
K: EGFR-TKIs resistance via EGFR-independent signaling pathways.
Mol Cancer. 17:532018. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Roskoski R Jr: Small molecule inhibitors
targeting the EGFR/ErbB family of protein-tyrosine kinases in human
cancers. Pharmacol Res. 139:395–411. 2019. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
London M and Gallo E: Epidermal growth
factor receptor (EGFR) involvement in epithelial-derived cancers
and its current antibody-based immunotherapies. Cell Biol Int.
44:1267–1282. 2020. View Article : Google Scholar
|
|
57
|
Li X, Lian Z, Wang S, Xing L and Yu J:
Interactions between EGFR and PD-1/PD-L1 pathway: Implications for
treatment of NSCLC. Cancer Lett. 418:1–9. 2018. View Article : Google Scholar
|
|
58
|
Hong X, Wang G, Xu G, Shi W, Wang T, Rong
Z and Mo C: Prognostic value of EGFR and p-EGFR in nasopharyngeal
carcinoma: A systematic review and meta-analysis. Medicine
(Baltimore). 101:e285072022. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Chan ATC, Hsu MM, Goh BC, Hui EP, Liu TW,
Millward MJ, Hong RL, Whang-Peng J, Ma BBY, To KF, et al:
Multicenter, phase II study of cetuximab in combination with
carboplatin in patients with recurrent or metastatic nasopharyngeal
carcinoma. J Clin Oncol. 23:3568–3576. 2005. View Article : Google Scholar
|
|
60
|
Ma BBY, Kam MKM, Leung SF, Hui EP, King
AD, Chan SL, Mo F, Loong H, Yu BKH, Ahuja A and Chan ATC: A phase
II study of concurrent cetuximab-cisplatin and intensity-modulated
radiotherapy in locoregionally advanced nasopharyngeal carcinoma.
Ann Oncol. 23:1287–1292. 2012. View Article : Google Scholar
|
|
61
|
Zhu Q, Duan XB, Hu H, You R, Xia TL, Yu T,
Xiang T and Chen MY: EBV-induced upregulation of CD55 reduces the
efficacy of cetuximab treatment in nasopharyngeal carcinoma. J
Transl Med. 22:11112024. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Qu L, Wang JH, Du JX, Kang P, Niu XQ and
Yin LZ: Use of nimotuzumab combined with cisplatin in treatment of
nasopharyngeal carcinoma and its effect on expressions of VEGF and
MMP-2. Clin Transl Oncol. 23:1342–1349. 2021. View Article : Google Scholar
|
|
63
|
Zhu Y, Yang S, Zhou S, Yang J, Qin Y, Gui
L, Shi Y and He X: Nimotuzumab plus platinum-based chemotherapy
versus platinum-based chemotherapy alone in patients with recurrent
or metastatic nasopharyngeal carcinoma. Ther Adv Med Oncol.
12:17588359209537382020. View Article : Google Scholar
|
|
64
|
Zhao C, Miao J, Shen G, Li J, Shi M, Zhang
N, Hu G, Chen X, Hu X, Wu S, et al: Anti-epidermal growth factor
receptor (EGFR) monoclonal antibody combined with cisplatin and
5-fluorouracil in patients with metastatic nasopharyngeal carcinoma
after radical radiotherapy: A multicentre, open-label, phase II
clinical trial. Ann Oncol. 30:637–643. 2019. View Article : Google Scholar
|
|
65
|
Zou Q, Cao Y, Lai Y, Fang Y, Zhang Y, Liu
P, Lu L, Wu H, Huang T, Su N, et al: Nimotuzumab combined with
docetaxel and cisplatin as first-line treatment for patients with
recurrent or metastatic nasopharyngeal carcinoma: A multicenter,
phase 2 trial. BMC Med. 23:2642025. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Qiu MZ, Zhang Y, Guo Y, Guo W, Nian W,
Liao W, Xu Z, Zhang W, Zhao HY, Wei X, et al: Evaluation of safety
of treatment with anti-epidermal growth factor receptor antibody
drug conjugate MRG003 in patients with advanced solid tumors: A
phase 1 nonrandomized clinical trial. JAMA Oncol. 8:1042–1046.
2022. View Article : Google Scholar
|
|
67
|
Xue L, Han Y, Zhang Q, Li X, Fang M, Zhong
L, Wang S, Liu Y, Zhang S and Guo Y: 939P Efficacy and safety of a
novel anti-EGFR ADC MRG003 in recurrent or metastatic squamous cell
carcinoma of the head and neck patients. Ann Oncol. 34 (Suppl
2):S5902023. View Article : Google Scholar
|
|
68
|
Xu RH, Ruan D, Han F, Zhou Y, Wang F, Tang
LQ, Li Z, Chen C, Lin J, Liu F, et al: 402O Preliminary results of
phase II study to evaluate safety and efficacy of combination
pucotenlimab with epidermal growth factor receptor-ADC (EGFR-ADC)
MRG003 in recurrent or metastatic nasopharyngeal carcinoma
(R/M-NPC). Ann Oncol. 35 (Suppl 4):S15542024. View Article : Google Scholar
|
|
69
|
Han F, Wang X, Xiang Y, Tang LQ, Qu S, Shu
X, Zhang P, Qiu S, Zhou Y, Guo Y, et al: Becotatug vedotin vs.
chemotherapy in pre-heavily treated advanced nasopharyngeal
carcinoma: A randomized, controlled, multicenter, open-label study.
J Clin Oncol. 43 (17 Suppl):LBA60052025. View Article : Google Scholar
|
|
70
|
Ma Y, Huang Y, Zhao Y, Zhao S, Xue J, Yang
Y, Fang W, Guo Y, Han Y, Yang K, et al: BL-B01D1, a first-in-class
EGFR-HER3 bispecific antibody-drug conjugate, in patients with
locally advanced or metastatic solid tumours: A first-in-human,
open-label, multicentre, phase 1 study. Lancet Oncol. 25:901–911.
2024. View Article : Google Scholar
|
|
71
|
Jiménez-Labaig P, Rullan A, Hernando-Calvo
A, Llop S, Bhide S, O'Leary B, Braña I and Harrington KJ: A
systematic review of antibody-drug conjugates and bispecific
antibodies in head and neck squamous cell carcinoma and
nasopharyngeal carcinoma: Charting the course of future therapies.
Cancer Treat Rev. 128:1027722024. View Article : Google Scholar
|
|
72
|
Yang Y, Zhou H, Tang L, Qiu S, Han Y, Ji
D, Chen X, Lei F, Qu S, Deng B, et al: Izalontamab brengitecan, an
EGFR and HER3 bispecific antibody-drug conjugate, versus
chemotherapy in heavily pretreated recurrent or metastatic
nasopharyngeal carcinoma: A multicentre, randomised, open-label,
phase 3 study in China. Lancet. 406:2235–2243. 2025. View Article : Google Scholar
|
|
73
|
Wang H, Fan S, Zhan Y, Xu Y, Du Y, Luo J,
Zang H, Peng S and Wang W: Targeting EGFR-binding protein SLC7A11
enhancing antitumor immunity of T cells via inducing MHC-I antigen
presentation in nasopharyngeal carcinoma. C Cell Death Dis.
16:212025. View Article : Google Scholar
|
|
74
|
Pollack BP: EGFR inhibitors, MHC
expression and immune responses: Can EGFR inhibitors be used as
immune response modifiers? Oncoimmunology. 1:71–74. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
75
|
Akbay EA, Koyama S, Carretero J, Altabef
A, Tchaicha JH, Christensen CL, Mikse OR, Cherniack AD, Beauchamp
EM, Pugh TJ, et al: Activation of the PD-1 pathway contributes to
immune escape in EGFR-driven lung tumors. Cancer Discov.
3:1355–1363. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Madeddu C, Donisi C, Liscia N, Lai E,
Scartozzi M and Macciò A: EGFR-mutated non-small cell lung cancer
and resistance to immunotherapy: Role of the tumor
microenvironment. Int J Mol Sci. 23:64892022. View Article : Google Scholar
|
|
77
|
Ma BBY, Lui VWY, Poon FF, Wong SCC, To KF,
Wong E, Chen H, Lo KW, Tao Q, Chan ATC, et al: Preclinical activity
of gefitinib in non-keratinizing nasopharyngeal carcinoma cell
lines and biomarkers of response. Invest New Drugs. 28:326–333.
2010. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Chua DT, Wei WI, Wong MP, Sham JS,
Nicholls J and Au GK: Phase II study of gefitinib for the treatment
of recurrent and metastatic nasopharyngeal carcinoma. Head Neck.
30:863–867. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Isomoto K, Haratani K, Hayashi H, Shimizu
S, Tomida S, Niwa T, Yokoyama T, Fukuda Y, Chiba Y, Kato R, et al:
Impact of EGFR-TKI treatment on the tumor immune microenvironment
in EGFR mutation-positive non-small cell lung cancer. Clin Cancer
Res. 26:2037–2046. 2020. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Peng S, Wang R, Zhang X, Ma Y, Zhong L, Li
K, Nishiyama A, Arai S, Yano S and Wang W: EGFR-TKI resistance
promotes immune escape in lung cancer via increased PD-L1
expression. Mol Cancer. 18:1652019. View Article : Google Scholar : PubMed/NCBI
|
|
81
|
Ferrara N: VEGF and intraocular
neovascularization: From discovery to therapy. Transl Vis Sci
Technol. 5:102016. View Article : Google Scholar
|
|
82
|
Ghalehbandi S, Yuzugulen J, Pranjol MZI
and Pourgholami MH: The role of VEGF in cancer-induced angiogenesis
and research progress of drugs targeting VEGF. Eur J Pharmacol.
949:1755862023. View Article : Google Scholar
|
|
83
|
Apte RS, Chen DS and Ferrara N: VEGF in
signaling and disease: Beyond discovery and development. Cell.
176:1248–1264. 2019. View Article : Google Scholar
|
|
84
|
Htet H, Anaghan JRJ, Jaiprakash H, Burud
IAS, Subramaniam T, Iezhitsa I and Agarwal R: Efficacy and safety
of molecular targeted therapies in nasopharyngeal carcinoma: A
network meta-analysis. BMC Cancer. 25:1102025. View Article : Google Scholar : PubMed/NCBI
|
|
85
|
Yang J, Yan J and Liu B: Targeting
VEGF/VEGFR to modulate antitumor immunity. Front Immunol.
9:9782018. View Article : Google Scholar
|
|
86
|
Allen E, Jabouille A, Rivera LB,
Lodewijckx I, Missiaen R, Steri V, Feyen K, Tawney J, Hanahan D,
Michael IP and Bergers G: Combined antiangiogenic and anti-PD-L1
therapy stimulates tumor immunity through HEV formation. Sci Transl
Med. 9:eaak96792017. View Article : Google Scholar : PubMed/NCBI
|
|
87
|
Zhang L, Lin Y, Hu L, Wang Y, Hu C,
Shangguan X, Tang S, Chen J, Hu P, Chen ZS, et al: Transient
intracellular expression of PD-L1 and VEGFR2 bispecific nanobody in
cancer cells inspires long-term T cell activation and infiltration
to combat tumor and inhibit cancer metastasis. Mol Cancer.
24:1192025. View Article : Google Scholar : PubMed/NCBI
|
|
88
|
Hack SP, Zhu AX and Wang Y: Augmenting
anticancer immunity through combined targeting of angiogenic and
PD-1/PD-L1 pathways: Challenges and opportunities. Front Immunol.
11:5988772020. View Article : Google Scholar
|
|
89
|
Schmittnaegel M, Rigamonti N, Kadioglu E,
Cassará A, Wyser Rmili C, Kiialainen A, Kienast Y, Mueller HJ, Ooi
CH, Laoui D and De Palma M: Dual angiopoietin-2 and VEGFA
inhibition elicits antitumor immunity that is enhanced by PD-1
checkpoint blockade. Sci Transl Med. 9:eaak96702017. View Article : Google Scholar : PubMed/NCBI
|
|
90
|
Ling Y, Yang Y, Lu N, You QD, Wang S, Gao
Y, Chen Y and Guo QL: Endostar, a novel recombinant human
endostatin, exerts antiangiogenic effect via blocking VEGF-induced
tyrosine phosphorylation of KDR/Flk-1 of endothelial cells. Biochem
Biophys Res Commun. 361:79–84. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
91
|
Peng F, Xu Z, Wang J, Chen Y, Li Q, Zuo Y,
Chen J, Hu X, Zhou Q, Wang Y, et al: Recombinant human endostatin
normalizes tumor vasculature and enhances radiation response in
xenografted human nasopharyngeal carcinoma models. PLoS One.
7:e346462012. View Article : Google Scholar : PubMed/NCBI
|
|
92
|
Jain RK: Normalization of tumor
vasculature: An emerging concept in antiangiogenic therapy.
Science. 307:58–62. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
93
|
Jin T, Li B and Chen XZ: A phase II trial
of Endostar combined with gemcitabine and cisplatin chemotherapy in
patients with metastatic nasopharyngeal carcinoma (NCT01612286).
Oncol Res. 21:317–323. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
94
|
Li Y, Tian Y, Jin F, Wu W, Long J, Ouyang
J and Zhou Y: A phase II multicenter randomized controlled trial to
compare standard chemoradiation with or without recombinant human
endostatin injection (Endostar) therapy for the treatment of
locally advanced nasopharyngeal carcinoma: Long-term outcomes
update. Curr Probl Cancer. 44:1004922020. View Article : Google Scholar : PubMed/NCBI
|
|
95
|
Xu L, Li D, Ji J, Chen Z, Tang X, Chen D,
Li X, Bao D, Yan F, Pang Y, et al: Recombinant human endostatin
injection (Endostar) combined with PF chemotherapy and sequential
intensity-modulated radiotherapy is tolerable and improves
prognosis of locally advanced nasopharyngeal carcinoma: A
randomized, open, multicenter phase II clinical study. Am J Cancer
Res. 12:4622–4636. 2022.PubMed/NCBI
|
|
96
|
Zhang Y, Zou Q, Zhao B, Su N, Li Z, Wang
X, Liu P, Tian X, Fang X, Cai J, et al: Toripalimab plus anlotinib
in patients with recurrent or metastatic nasopharyngeal carcinoma:
A multicenter, single-arm phase 2 trial (TORAL). Cell Rep Med.
5:1018332024. View Article : Google Scholar : PubMed/NCBI
|
|
97
|
Yuan L, Jia GD, Lv XF, Xie SY, Guo SS, Lin
DF, Liu LT, Luo DH, Li YF, Deng SW, et al: Camrelizumab combined
with apatinib in patients with first-line platinum-resistant or
PD-1 inhibitor resistant recurrent/metastatic nasopharyngeal
carcinoma: A single-arm, phase 2 trial. Nat Commun. 14:48932023.
View Article : Google Scholar : PubMed/NCBI
|
|
98
|
Mo Y, Pan Y, Zhang B, Zhang J, Su Y, Liu
Z, Luo M, Qin G, Kong X, Zhang R, et al: Apatinib combined with
camrelizumab in the treatment of recurrent/metastatic
nasopharyngeal carcinoma: A prospective multicenter phase II study.
Front Immunol. 14:12984182024. View Article : Google Scholar
|
|
99
|
Liang H, Jiang YF, Liu GY, Wang L, Wang
JW, Lu N, Xia WX, Ke LR, Ye YF, Duan JL, et al: Camrelizumab and
apatinib plus induction chemotherapy and concurrent
chemoradiotherapy in stage N3 nasopharyngeal carcinoma: A phase 2
clinical trial. Nat Commun. 15:10292024. View Article : Google Scholar : PubMed/NCBI
|
|
100
|
Chong WQ, Low JL, Tay JK, Le TBU, Goh GSQ,
Sooi K, Teo HL, Cheo SW, Wong RTX, Samol J, et al: Pembrolizumab
with or without bevacizumab in platinum-resistant recurrent or
metastatic nasopharyngeal carcinoma: A randomised, open-label,
phase 2 trial. Lancet Oncol. 26:175–186. 2025. View Article : Google Scholar
|
|
101
|
Tang LQ, Liu SL, Yang MH, Wang HC, Zhou
YJ, Yang KY, Li Q, Hui M, Chen XZ, Leu YS, et al: GFH018 and
toripalimab combination therapy for previously treated recurrent or
metastatic nasopharyngeal carcinoma: Results from a phase Ib/II
study. Clin Cancer Res. 31:3424–3432. 2025. View Article : Google Scholar : PubMed/NCBI
|














