Introduction
Chyme refeeding therapy (CRT) redirects effluent
chyme from the proximal stoma into the distal intestine. Hence, by
utilizing the downstream bowel, it facilitates enteral nutrient
absorption and physiological stimulation of the intestine, and also
reduces dependence on parenteral nutrition (PN). In addition, CRT
restores the enterohepatic circulation of bile salts, thereby
limiting bile salt hypersecretion and potentially mitigating
intestinal failure-associated liver disease (IFALD) (1). Despite these potential benefits,
however, CRT remains underutilized, particularly in children from
developing countries.
According to the European Society for Clinical
Nutrition and Metabolism (ESPEN), intestinal failure is defined as
a reduction in gut function below the minimum necessary for the
absorption of macronutrients and/or water and electrolytes, such
that intravenous supplementation is required to maintain health and
growth (2). By contrast, a
reduction in intestinal absorptive capacity that does not require
intravenous supplementation is defined as intestinal insufficiency.
ESPEN further classifies intestinal failure into three types, of
which type II intestinal failure (prolonged acute condition, often
in metabolically unstable patients, which requires complex
multi-disciplinary care and intravenous supplementation over
periods of weeks or months) is typically observed in patients with
high-output enterostomy (3). In
this context, CRT may play a role in partially or completely
restoring intestinal function, thereby contributing to the
resolution of intestinal failure.
In recent years, interest in CRT for the treatment
of pediatric populations with prolonged enterostomy has increased.
The study by Wong et al (4)
has shown that CRT is safe among children, can prevent disuse
atrophy in the distal loop, promote weight gain and reduce
dependence on PN. Other more recent research from Lau et al
(5) and Lim et al (6) has shown similar results. However,
there remains a paucity of data from low and middle-income
countries, where the burden of enterostomy-related malnutrition is
substantial and access to PN, as well as novel CRT devices is
limited or unaffordable. Moreover, there are minimal details
available regarding its use among children outside of the neonatal
period.
The practice of CRT in children at Vietnam National
Children's Hospital (VNCH; Hanoi, Vietnam), a selected tertiary
center with a multidisciplinary team dedicated to caring for
children with nutritional complications following gastrointestinal
surgery, has been applied since 2021. The present study aimed to
describe the characteristics, methodology and nutritional outcomes
of CRT in 20 pediatric patients (both neonates and older children)
who had undergone double enterostomies treated at VNCH. By
presenting this clinical experience, the authors hope to contribute
to the growing body of evidence supporting CRT as an effective
strategy for improving nutritional status and reducing PN
dependence in children who have undergong a double enterostomy.
Patients and methods
Ethics approval and study design
The present study was approved by the Ethics
Committee of VNCH (approval no. 3697/BVNTW-HDDD; dated November 26,
2024) prior to data collection and analysis. For the prospective
cohort, written informed consent was obtained from the parents or
legal guardians of the patients after they were informed of the
study. All data were anonymized and participant information was
kept strictly confidential.
The present combined retrospective-prospective
cohort study was conducted at the Clinical Nutrition Department of
VNCH. The department is a leading center in Northern Vietnam
specializing in managing children with nutritional complications
following gastrointestinal surgery. The retrospective cohort
included patients who had completed treatment and follow-up between
January 1, 2021 and November 26, 2024 (the date of ethics
approval). Data for the retrospective cohort were extracted from
medical records between November 27, 2024 and June 30, 2025. The
prospective cohort comprised patients who began CRT on or after
November 27, 2024 (after ethics approval) and completed follow-up
before June 30, 2025.
Study population
Eligible participants were patients aged <18
years who had undergone a double enterostomy and subsequently
received CRT for any indication between January 1, 2021 and June
30, 2025. Patients who received all CRT methods (bolus or
continuous, manual or automated) were eligible for inclusion.
Patients who succumbed prior to enterostomy closure (intestinal
anastomosis) or those who received CRT for ≤1 day in total were
excluded from the study. Due to the rarity of CRT among Vietnamese
children, the present study employed convenience sampling and did
not perform a formal sample size calculation. A total of 20
patients met the inclusion criteria, comprising 13 children in the
retrospective cohort and 7 children in the prospective cohort.
Study process
For the retrospective cohort, patients were
identified through the systematic screening of databases at VNCH,
including the surgical logs and records from the Clinical Nutrition
Department. All pediatric patients who underwent double enterostomy
during the study period were initially screened. Among these,
patients who received CRT prior to enterostomy closure were
selected. These cases were then assessed against predefined
inclusion and exclusion criteria to determine eligibility for
inclusion in the present study. Data for the retrospective cohort
were extracted from medical records between November 27, 2024 and
June 30, 2025.
A standardized CRT protocol had been established and
routinely applied in the Clinical Nutrition Department prior to the
study period. For patients receiving bolus CRT, chyme was manually
collected from the proximal stoma bag and refed into the distal
stoma using either a gastric tube or a Foley catheter, as
determined by the attending gastrointestinal surgeon. A small
opening was created in the stoma bag to allow the insertion of the
tube, which was then secured with medical tape. The collected chyme
was refed as a bolus over a period of 15-20 min, either manually or
using an electronic syringe. To minimize the risk of contamination,
refeeding was performed within 1 h of chyme collection. The
frequency of refeeding was initially set at twice daily and
subsequently increased based on patient tolerance and clinical
judgment. For patients receiving continuous CRT, two gastric tubes
or Foley catheters were inserted into the proximal and distal
stomas and connected via a three-way connector, allowing chyme to
pass continuously from the proximal to the distal bowel.
For the retrospective cohort, the clinical
management was reviewed to ensure that CRT was performed according
to this protocol. For the prospective cohort, the same protocol was
applied prospectively without modification. During the entire study
period, no major changes were made to the core principles of CRT
indication, refeeding techniques or nutritional management.
Surgical management followed the standard pediatric surgical
practices at VNCH and did not differ between study phases.
Data were collected using a standardized data
collection form. The collected baseline demographic and clinical
variables included the indication for a double enterostomy, stoma
site and ileocecal-valve preservation status. Each patient was
monitored from the time of surgery until enterostomy closure. For
the retrospective cohort, these variables were retrieved from the
existing records; for the prospective cohort, data were collected
prospectively following the same protocol. Data were obtained at
three predefined time points: Admission to the Clinical Nutrition
Department (T0), the initiation of CRT (T1) and the final day of
CRT prior to enterostomy closure (T2).
Characteristics of the CRT data
The interval from stoma formation to the initiation
of CRT was measured in weeks, from the date of stoma creation to
T1. The duration of CRT was defined as the period (weeks) from T1
to T2. The CRT method was classified as either bolus or continuous.
The number of CRT episodes per day referred to the number of chyme
refeeding sessions delivered to the distal stoma per day, as
indicated by clinicians. Time to stool passage was measured in days
from T1 to the first time stool passed via the anatomical anus and
rounded to the nearest day (for example, ≤24 h=1 day). The
proportion of patients who underwent temporary cessation of CRT was
calculated, with documented reasons for each case.
Clinical outcomes of patients
receiving CRT
Weight and length/height were routinely measured and
recorded by trained nurses or physicians following standardized
anthropometric procedures. Body weight was measured using a
calibrated mechanical pediatric scale with a precision of 0.1 kg.
Recumbent length (for patients <2 years) or standing height (for
patients ≥2 years) was measured to the nearest 0.1 cm using a
length board or stadiometer, respectively. Body mass index (BMI)
was calculated as weight (kg) divided by height squared
(m2). Weight-for-height Z-scores (WHZs) were calculated
for children aged <59 months and BMI-for-age Z-scores (BMIZs)
were calculated for children aged ≥60 months. Z-score calculations
were performed using AnthroCalc (version 3.1.6), a growth
assessment application developed and supplied by Daniel L. Metzger,
which applies World Health Organization (WHO) growth reference
algorithms to compute standardized anthropometric indices. The
nutritional status was classified as wasting when the WHZ or BMIZ
was ≤-2 SD relative to the WHO 2007 growth reference standards
(7). To account for variability in
the baseline weight and duration of CRT, the weight-gain velocity
before vs. after CRT (g/kg/week) was compared using the following
formula: Weight-gain velocity before CRT=[(W1-W0) x1,000]/[W0 x
(T0-T1)] and weight-gain velocity after CRT=[(W2-W1) x1,000]/[W1 x
(T1-T2)], where W0, W1 and W2 denote the weight (kg) measured at
the T0, T1 and T2 time points, respectively, and (T0-T1) and
(T1-T2) denote the corresponding time intervals in weeks.
PN was defined as the administration of intravenous
amino acids or lipids alone or any combination of at least two
macronutrient components, excluding glucose-only infusions
(8). A total of 17 patients
required complete or partial PN at time point T1. Changes in PN
requirement were classified as follows: Cessation (no PN required
at T2), reduction (any measurable decrease in PN requirement from
T1 to T2) or no change. The interval from CRT initiation to PN
cessation was recorded in weeks. The number of patients analyzed
before and after CRT were exactly the same.
Data processing and statistical
analysis
Statistical analyses were conducted using SPSS
Statistics v27 (IBM Corp.). Continuous variables were tested for
normality using the Shapiro-Wilk test. Non-normally distributed
data are summarized as the median [interquartile range (IQR)] or
median (range) and were compared using the Wilcoxon signed-rank
test. A two-sided P-value <0.05 was considered to indicate a
statistically significant difference. Given the small sample size,
results were interpreted descriptively and no multivariable
modeling was attempted.
Results
The present study included 20 pediatric patients
with a median age of 0.1 years (range, 0.0-12.9 years). The
majority of the patients were male, with a male-to-female ratio of
1.5:1. The most common indication for double enterostomy was
intestinal atresia (30.0%), followed closely by necrotizing
enterocolitis, intestinal obstruction and intestinal volvulus. A
total of 18 patients (90.0%) underwent either jejunostomy or
ileostomy, whereas 2 underwent duodenostomy. At baseline, 85.0% of
the cohort suffered from wasting malnutrition with a median WHZ or
BMIZ of -2.9 SD (Table I).
 | Table IPatient demographics and clinical
characteristics. |
Table I
Patient demographics and clinical
characteristics.
| Characteristic | Value |
|---|
| Sex, n (%) | |
|
Male | 12(60) |
|
Female | 8(40) |
| Age, years; median
(IQR) | 0.1 (0.0-12.9) |
| Indications of
double-enterostomy, n (%) | |
|
Intestinal
atresia | 6(30) |
|
Necrotizing
enterocolitis | 5(25) |
|
Intestinal
obstruction | 4(20) |
|
Intestinal
volvulus | 4(20) |
|
Intestinal
perforation | 1 (5%) |
| Site of ostomy, n
(%) | |
|
Duodenostomy | 2(10) |
|
Jejunostomy | 8(40) |
|
Ileostomy | 10(50) |
| ICV preserved, n
(%) | 19(95) |
| WHZ or BMIZ before
CRT, median (IQR) | -2.9; (-3.8-2.1) |
| Wasting malnutrition
at admission, n (%) | 17(85) |
CRT was initiated at a median of 7 weeks following
stoma formation and was maintained for a median duration of 5 weeks
(range, 2-16 weeks). In total, 18 patients (90.0%) received CRT via
the bolus method, whereas the remaining 2 were managed with
continuous infusion. The median number of chyme refeeding sessions
was 4 per day and stool passage via the anatomical anus occurred
within a median of 1 day (Table
II).
| Table IICharacteristics of chyme refeeding
therapy. |
Table II
Characteristics of chyme refeeding
therapy.
| Characteristics | Value |
|---|
| Duration from stoma
formation to CRT initiation, weeks; median (IQR) | 7 (4.3-10.8) |
| Duration of CRT,
weeks; median (range) | 5 (2.0-16.0) |
| CRT method, n
(%) | |
|
Bolus | 18(90) |
|
Continuous | 2(20) |
| CRT episodes per day;
median (range) | 4 (1-8) |
| Time to stool
passage, days; median (range) | 1 (1-3) |
Among the 17 patients who required PN prior to CRT
initiation, 9 (52.9%) were able to discontinue PN following the
procedure following a median duration of 2 weeks; 3 patients
(17.6%) exhibited a reduction in PN requirement, whereas 5 (29.4%)
patients exhibited no change (Table
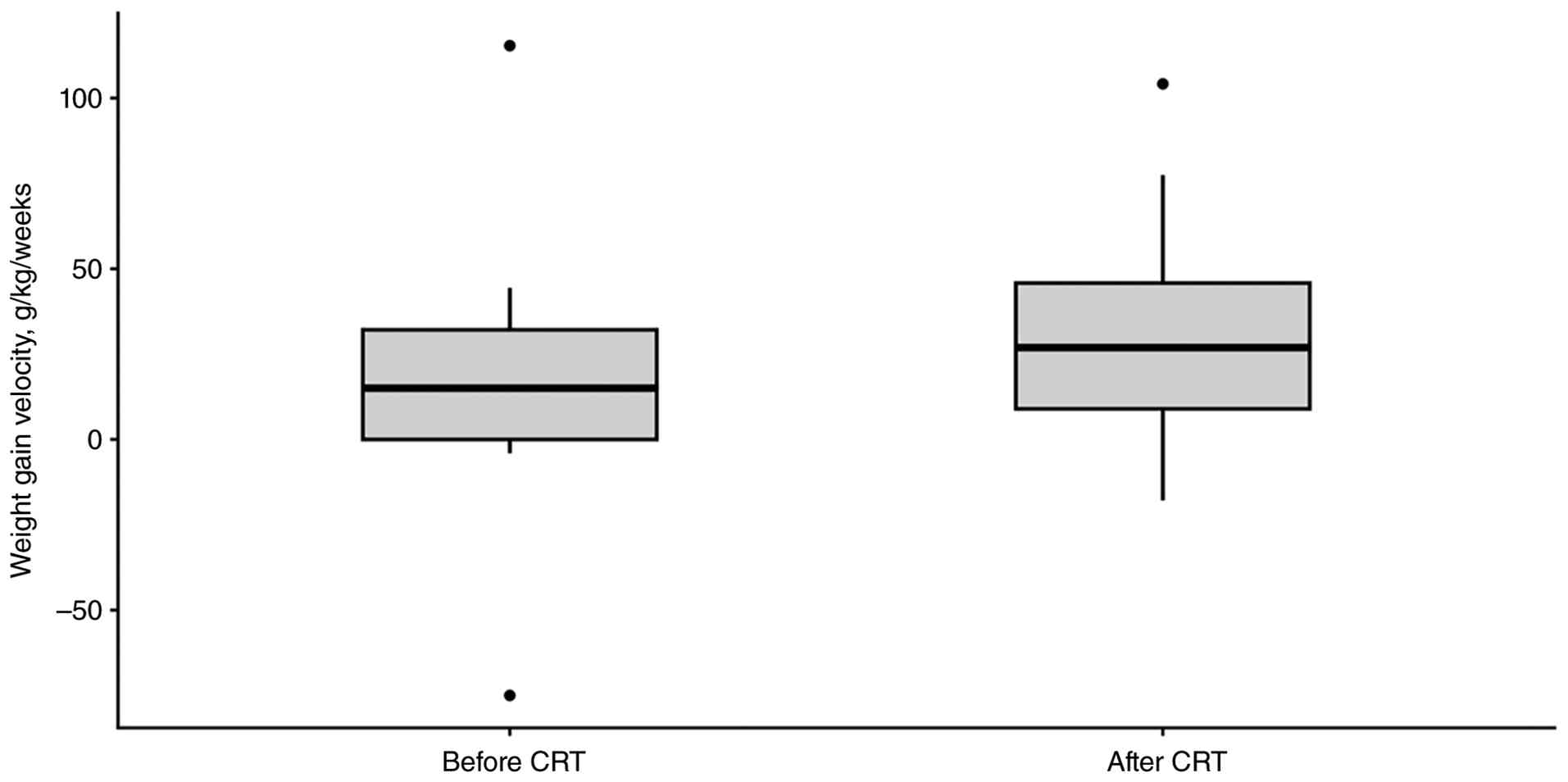
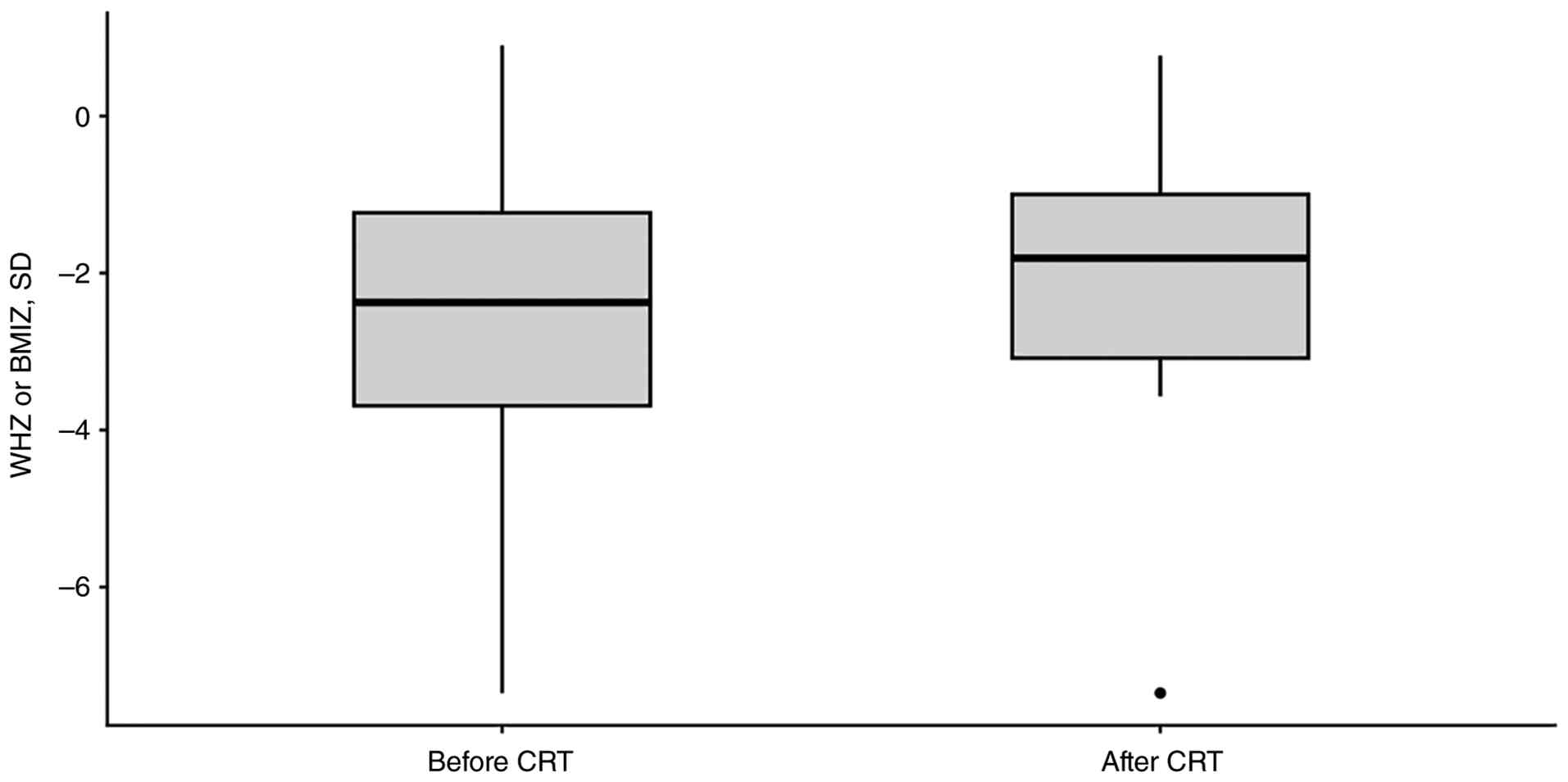
III). The weight-gain velocity per week improved significantly
from a median of 15 g/kg/week before CRT to 26.9 g/kg/week after
CRT (P=0.04; Fig 1). Similarly,
the WHZ/BMIZ increased from -2.4 to -1.8 following CRT, a
difference that was statistically significant (P=0.02; Fig. 2). The temporary cessation of CRT
occurred in 40.0% of cases, which was primarily due to infection
(Table IV). Of note, 1 patient
had pneumonia, and 6 patients were diagnosed with infection of
unknown origin; 1 patient had to discontinue CRT due to distal gut
prolapse.
| Table IIIChange in parenteral nutrition
dependence after chyme refeeding therapy. |
Table III
Change in parenteral nutrition
dependence after chyme refeeding therapy.
| Outcomes | Value |
|---|
| PN required prior to
CRT initiation, n (%) (n=20) | 17(85) |
| Change in PN
requirement, n (%) (n=17) | |
|
Cessation | 9 (52.9) |
|
Reduction | 3 (17.6) |
|
No
change | 5 (29.4) |
| Time to PN cessation
after CRT initiation (weeks), median (IQR) (n=9) | 2 (1.0-4.0) |
| Table IVComplications during CRT. |
Table IV
Complications during CRT.
| Parameter | Value |
|---|
| Rate of complications
(n=20) | n (%) |
|
Infection | 7(35) |
|
Stoma
prolapse | 1(5) |
|
Intestinal
bleeding | 0 (0) |
| CRT cessation rate
due to complications (n=20) | 8(40) |
Discussion
To the best of our knowledge, the present study is
the first to describe CRT in a pediatric population that is not
limited to the neonatal period and is in a low-to-middle income
country setting. The present study included 20 patients and aimed
to describe the characteristics and outcomes of children treated
with CRT.
Double enterostomy is performed in children with
gastrointestinal conditions, such as intestinal atresia or
necrotizing enterocolitis, when primary anastomosis is not feasible
due to inflammation, poor tissue perfusion or a high risk of
anastomosis leakage. However, this procedure may lead to a
substantial loss of fluids, electrolytes and nutrients through the
proximal stoma, placing patients at risk of developing
post-operative malnutrition. In the present study cohort, 85% of
the pediatric patients presented with wasting or acute malnutrition
at admission, with a median WHZ/BMIZ of -2.9 SD. Since the present
study included children of various ages assessed at the acute stage
following stoma formation, it was considered that examining the WHZ
or BMIZ would be more appropriate than the weight-for-age Z-score.
Nonetheless, malnutrition following enterostomy has also been
reported in another study. The study by Chong et al
(9) on 74 infants demonstrated
that 42% of the infants developed severe underweight malnutrition
at the time of stoma closure, with a median weight-to-age Z-score
of -2.8 SD.
Several strategies can improve the nutritional
status of patients who have undergone a double enterostomy. Enteral
nutrition can facilitate intestinal adaptation; however, increasing
the feeding volume is limited by the reduced absorption surface
area and increased stoma losses, particularly in patients with
high-output enterostomy (defined as a stoma output ≥20 ml/kg/day
for 2 consecutive days) (10).
When enteral nutrition is insufficient or not tolerated, PN is
required; however, PN is associated with complications, such as
central line infection, thrombosis or liver injury (11,12).
To overcome these limitations, CRT is a complementary nutritional
intervention that is expected to restore intraluminal stimulation,
improve nutrient and fluid reabsorption, as well as reduce reliance
on PN by redirecting chyme from the proximal to the distal
stoma.
The present study observed a significant improvement
in both weight-gain velocity and WHZ/BMIZ following CRT initiation.
These findings are consistent with those of the prior study by
Ludlow et al (13), in
which a positive weight gain from a mean of 68.8±37.4 to 197±25.0
g/week after CRT (P=0.024) was reported. Although weight-gain
velocity expressed as g/kg/day has not been previously applied in
pediatric CRT research, it was previously used in a study on
children with acute malnutrition to evaluate nutritional status
improvement after medical interventions (14). Thus, the present study expressed
weight change as g/kg/week, which was considered more appropriate
than absolute g/day or g/week, since the majority of the cohort
suffered from wasting malnutrition and had varying ages, initial
weights and CRT durations compared with the majority of other
research, which has been limited to infants (4-6,12,15).
The ‘per week’ unit was selected instead of ‘per day’ as CRT is
typically maintained for several weeks until enterostomy reversal
(at least 2 weeks in the present study). The improvement in weight
gain observed in the present study may partly reflect recovery from
acute illness or regression toward the mean. However, in the
present cohort, CRT was initiated relatively late (median of 7
weeks after stoma formation) compared with other studies, a time
point at which a number of patients had generally passed the acute
post-operative phase and had already received other forms of
nutritional support with limited weight gain (5,6). The
subsequent improvement in weight-gain velocity following CRT
initiation may indicate a possible contribution from CRT to these
changes.
In the present study, CRT also facilitated PN
weaning as over half of the cohort discontinued PN after a median
of 2 weeks following CRT, while an additional 17.6% experienced a
reduction in PN. This cessation rate is comparable to that reported
by in the study by Elliott and Walton (15), in which 48% of cases were able to
withdraw from PN. CRT utilizes the chyme from the proximal stoma,
thereby enhancing nutritional status, reducing PN requirement and
stimulating the release of several gut hormones, particularly
glucagon-like peptide 2, which accelerates enteral mucosal growth
and intestinal adaptation (16).
Reducing PN dependence is essential due to the risks associated
with long-term PN use (11,12).
CRT may also decrease hospitalization duration and healthcare
costs, particularly in settings where home PN is not available,
such as Vietnam.
In the present study, CRT was initiated at a median
of 7 weeks (IQR, 4.3-10.8 weeks) following stoma formation, which
is later than the median of 28.7 days (range, 15.0-140.0 days)
reported by Lau et al (5)
and 17 days (range, 13.0-27.5 days) reported by Lim et al
(6). This delay may reflect the
limited clinical awareness and familiarity with CRT among
Vietnamese pediatricians, as a number of patients were only
referred to the Clinical Nutrition Department when they developed
severe malnutrition, failed to discontinue PN or exhibited signs of
IFALD. In the present study, the median CRT duration was 5 weeks,
which is longer than that reported by Lim et al (6), who reported a median of 19 days
(6), but shorter than the mean of
76.5 days described by Lau et al (5). Since CRT is maintained until
enterostomy closure, these variations may reflect a lack of
consensus regarding the optimal timing of re-anastomosis surgery. A
previous systematic review indicated that there was no significant
difference in complications between early and late closure and that
decisions can vary by center as well as multidisciplinary
assessment (17). At VNCH, closure
is largely based on the preference of the surgeon and is typically
deferred until at least 12 weeks after stoma formation and the
patient has reached a minimum weight of 2 kg if they were born
preterm. In the present study, the majority of patients (90%)
received CRT via the bolus method due to limited technical
resources and staffing constraints.
Despite its benefits, CRT is not without challenges.
In the present study, 8 patients (40%) had to cease CRT temporarily
due to complications. Infection was the leading cause of this,
followed by 1 case of distal stoma prolapse; however, no patients
experienced intestinal bleeding or intestinal perforation. The
infection rate (35%) was comparable to that reported by Lim et
al (6), which was 44%. In the
present study, among the 7 cases of infection observed following
CRT initiation, 1 patient was diagnosed with pneumonia based on
clinical and radiological findings. The remaining 6 patients had
episodes of fever accompanied by elevated inflammatory markers
(leukocytosis and increased C-reactive protein) occurring 1 week to
1 month after initiation of CRT. Microbiological investigations,
including blood and/or stool cultures, were negative in all of
these cases and no definitive infectious source could be
identified. These episodes were managed conservatively and none
resulted in intensive care admission or mortality. Additionally, 1
patient with distal gut prolapse after CRT initiation had to stop
CRT definitively after 2 weeks and subsequently underwent stoma
closure.
The present study has several limitations that
should be acknowledged. First, the sample size was small (n=20),
which limits the generalizability of the findings. Although this
sample size reflects the rarity of CRT in pediatric populations and
its early implementation at VNCH, the results should be interpreted
cautiously as preliminary observational evidence rather than
definitive evidence of efficacy. Second, the combined
retrospective-prospective design is subject to incomplete
documentation and potential selection bias among the retrospective
cohort; however, the routine anthropometric measurements performed
by trained medical staff at VNCH likely mitigated measurement
error. Moreover, as the Clinical Nutrition Department is currently
the only unit implementing CRT at VNCH, the present study cohort
may represent a subset of children with who had undergoen double
enterostomy who had more severe nutritional impairment or greater
clinical complexity than those managed in other departments, such
as the Surgery or Gastroenterology departments. Such a referral
pattern may have influenced both the baseline characteristics and
observed outcomes in the present study and should therefore be
considered when interpreting the results. Third, since the present
cohort was inherently predisposed to infection due to malnutrition
and the use of a central venous line, the association between
infection and CRT should be interpreted with caution. The high
baseline risk of infection makes it difficult to determine whether
infections were related to CRT or to pre-existing vulnerabilities.
Fourth, subgroup analysis was not performed as we considered it
substantially underpowered and likely to yield unreliable or
potentially misleading results. In particular, several subgroups
were very small, including patients with duodenostomy (n=2) and
those receiving continuous CRT (n=2), which would limit meaningful
interpretation and increase the risk of spurious findings. Fifth,
although the observed weight gain may plausibly be attributable to
CRT rather than recovery alone in our cohort, the independent
effect of CRT cannot be definitively established and residual
confounding cannot be completely excluded given the observational
design of the present study. Finally, liver function and stoma
discrepancy following CRT were not assessed in the present study
due to limited data availability. Despite these limitations, the
findings of the present study are consistent with those of previous
reports, suggesting that CRT may serve as a beneficial adjunctive
therapy, with potential improvements in nutritional outcomes and
facilitation of PN weaning in children following a double
enterostomy (4-6,12,15).
However, larger and well-designed prospective studies are required
to confirm these observations and evaluate the long-term outcomes
of CRT.
In conclusion, CRT may be an effective treatment
strategy in pediatric patients who have undergone a double
enterostomy, as demonstrated by the improved weight gain and
reduced PN dependence observed in the present study. While the
observed results are encouraging, they should be interpreted with
caution. Broader clinical adoption of CRT and further research are
required to establish the effectiveness and optimal implementation
of CRT.
Acknowledgements
Not applicable.
Funding
Funding: No funding was received.
Availability of data and materials
The data generated in the present study may be
requested from the corresponding author.
Authors' contributions
All authors (HTTN, NTH, NTKB, DTT, HMV, DQL, LTTN
and TTML) contributed to the conception and design of the present
study. The patient data collection was performed by NTH. The first
draft of the manuscript was written by NTH, HTTN and TTML, and all
authors commented on previous versions of the manuscript. HTTN, NTH
and TTML confirm the authenticity of all the raw data. All authors
have read and approved the final version of the manuscript.
Ethics approval and consent to
participate
The present study was approved by the Ethics
Committee of Vietnam National Children's Hospital (approval no.
3697/BVNTW-HDDD; dated November 26, 2024). The parents or guardians
of the pediatric patients were informed of the purpose of the
present study and signed the consent forms for participation in the
study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Koelfat KVK, Picot D, Chang X,
Desille-Dugast M, van Eijk HM, van Kuijk SMJ, Lenicek M, Layec S,
Carsin M, Dussaulx L, et al: Chyme reinfusion restores the
regulatory bile salt-FGF19 axis in patients with intestinal
failure. Hepatology. 74:2670–2683. 2021.PubMed/NCBI View Article : Google Scholar
|
|
2
|
Pironi L, Arends J, Baxter J, Bozzetti F,
Peláez RB, Cuerda C, Forbes A, Gabe S, Gillanders L, Holst M, et
al: ESPEN endorsed recommendations. Definition and classification
of intestinal failure in adults. Clin Nutr. 34:171–180.
2015.PubMed/NCBI View Article : Google Scholar
|
|
3
|
Adaba F, Vaizey CJ and Warusavitarne J:
Management of intestinal failure: The high-output enterostomy and
enterocutaneous fistula. Clin Colon Rectal Surg. 30:215–222.
2017.PubMed/NCBI View Article : Google Scholar
|
|
4
|
Wong KK, Lan LC, Lin SC, Chan AW and Tam
PK: Mucous fistula refeeding in premature neonates with
enterostomies. J Pediatr Gastroenterol Nutr. 39:43–45.
2004.PubMed/NCBI View Article : Google Scholar
|
|
5
|
Lau EC, Fung AC, Wong KK and Tam PK:
Beneficial effects of mucous fistula refeeding in necrotizing
enterocolitis neonates with enterostomies. J Pediatr Surg.
51:1914–1916. 2016.PubMed/NCBI View Article : Google Scholar
|
|
6
|
Lim AH, Tinawi G, Harrington T, Ludlow E,
Evans H, Bissett I and Keane C: Chyme reinfusion practices in the
neonatal population. Pediatr Surg Int. 41(7)2024.PubMed/NCBI View Article : Google Scholar
|
|
7
|
WHO Multicentre Growth Reference Study
Group. WHO Child Growth Standards based on length/height, weight
and age. Acta Paediatr Suppl. 450:76–85. 2006.PubMed/NCBI View Article : Google Scholar
|
|
8
|
Reintam Blaser A, Cotoia A, Berger MM,
Padar M, Arabi YM, Casaer MP, Gunst J, Kouw IWK, Malbrain MLNG,
Schaller SJ, et al: How to define parenteral nutrition. Crit Care.
28(372)2024.PubMed/NCBI View Article : Google Scholar
|
|
9
|
Chong C, van Druten J, Briars G, Eaton S,
Clarke P, Tsang T and Yardley I: Neonates living with enterostomy
following necrotising enterocolitis are at high risk of becoming
severely underweight. Eur J Pediatr. 178:1875–1881. 2019.PubMed/NCBI View Article : Google Scholar
|
|
10
|
Awouters M, Vanuytsel T, Huysentruyt K, De
Bruyne P, Van Hoeve K and Hoffman I: Nutritional management of
high-output ileostomies in paediatric patients is vital and more
evidence-based guidelines are needed. Acta Paediatr. 113:861–870.
2024.PubMed/NCBI View Article : Google Scholar
|
|
11
|
Fonseca G, Burgermaster M, Larson E and
Seres DS: The relationship between parenteral nutrition and central
line-associated bloodstream infections: 2009-2014. JPEN J Parenter
Enteral Nutr. 42:171–175. 2018.PubMed/NCBI View Article : Google Scholar
|
|
12
|
Di Dato F, Iorio R and Spagnuolo MI: IFALD
in children: What's new? A narrative review. Front Nutr.
9(928371)2022.PubMed/NCBI View Article : Google Scholar
|
|
13
|
Ludlow E, Harrington T, Davidson R,
Davidson J, Aikins K, O'Grady G and Bissett I: Evaluating the
efficacy and safety of neonatal chyme reinfusion therapy: A
feasibility study using a novel medical device. Clin Nutr.
43:2253–2260. 2024.PubMed/NCBI View Article : Google Scholar
|
|
14
|
Kamugisha JGK, Lanyero B,
Nabukeera-Barungi N, Nambuya-Lakor H, Ritz C, Mølgaard C,
Michaelsen KF, Briend A, Mupere E, Friis H and Grenov B: Weight and
mid-upper arm circumference gain velocities during treatment of
young children with severe acute malnutrition, a prospective study
in Uganda. BMC Nutr. 7(26)2021.PubMed/NCBI View Article : Google Scholar
|
|
15
|
Elliott T and Walton JM: Safety of mucous
fistula refeeding in neonates with functional short bowel syndrome:
A retrospective review. J Pediatr Surg. 54:989–992. 2019.PubMed/NCBI View Article : Google Scholar
|
|
16
|
Vegge A, Thymann T, Lund P, Stoll B,
Bering SB, Hartmann B, Jelsing J, Qvist N, Burrin DG, Jeppesen PB,
et al: Glucagon-like peptide-2 induces rapid digestive adaptation
following intestinal resection in preterm neonates. Am J Physiol
Gastrointest Liver Physiol. 305:G277–G285. 2013.PubMed/NCBI View Article : Google Scholar
|
|
17
|
Struijs MC, Sloots CE, Hop WC, Tibboel D
and Wijnen RM: The timing of ostomy closure in infants with
necrotizing enterocolitis: A systematic review. Pediatr Surg Int.
28:667–672. 2012.PubMed/NCBI View Article : Google Scholar
|