Introduction
Fusarium is a genus of filamentous fungi
spread in cereals, fruits and vegetables, water and air, and even
in the soil in temperate climates. It affects human health when
infested foods or water are consumed (1). Almost all Fusarium species are
harmless, although some species (Fusarium solani, Fusarium
oxysporum, Fusarium chlamydosporum and Fusarium
moniliforme) produce mycotoxins, such as fumonisins and
trichothecenes, causing opportunistic infections in healthy humans
or hematogenic spreading to immunocompromised individuals, with
very poor prognosis (2).
Contamination with Fusarium saprophytic
species can cause infections in humans that are localized or
disseminated throughout the body (2,3). The
most common clinical aspects of Fusarium infection in
immunocompetent patients may occur in nails (onychomycosis), in
skin, caused particularly by trauma or burns (subcutaneous tender
nodules such as nodous erythema, ecthyma-like lesions and
cellulitis), or in viscera (cornea, lungs, heart or joints)
(4).
Disseminated Fusarium infections cause
significant morbidity and mortality in immunocompromised patients,
being the second most frequent fungal infection after aspergillosis
(1). Infection is characterized by
cutaneous nodules, positive fungemia in 40% of cases and visceral
involvement, particularly in lungs and sinuses, with a high rate of
mortality (5). Studies have shown
that among patients who have received a hematopoietic stem cell
transplant (HSCT) the frequency of fusariosis ranges between
4.21–5.0 cases per 1,000 in human leukocyte antigen (HLA)-matched
related transplant recipients to 20.19 cases per 1,000 in
HLA-mismatched transplant recipients (1,3).
There are few cases presented in the literature of
disseminated fusariosis infection in patients who have received an
allogeneic stem cell transplant (4).
The present report describes a rare clinical case of a female who
developed graft-vs.-host disease (GVHD) following an allogeneic
stem cell transplant for Hodgkin disease and succumbed after
contracting disseminated Fusarium infection. Another
particularity of this case was that the patient did not present
clinical onychomycosis.
Case report
In February 2009, a 24-year old women received an
allogeneic stem cell transplant from a sibling donor for Hodgkin's
disease (chemosensitive relapse following autologous stem cell
transplant). The patient achieved a complete remission, with
negative positron emission tomography-computed tomography (PET-CT)
findings at 100 days after transplant, with full donor chimerism.
On day 220 after transplant the patient developed moderate GVHD
(skin 2, mouth 1, eye 1) (6) with
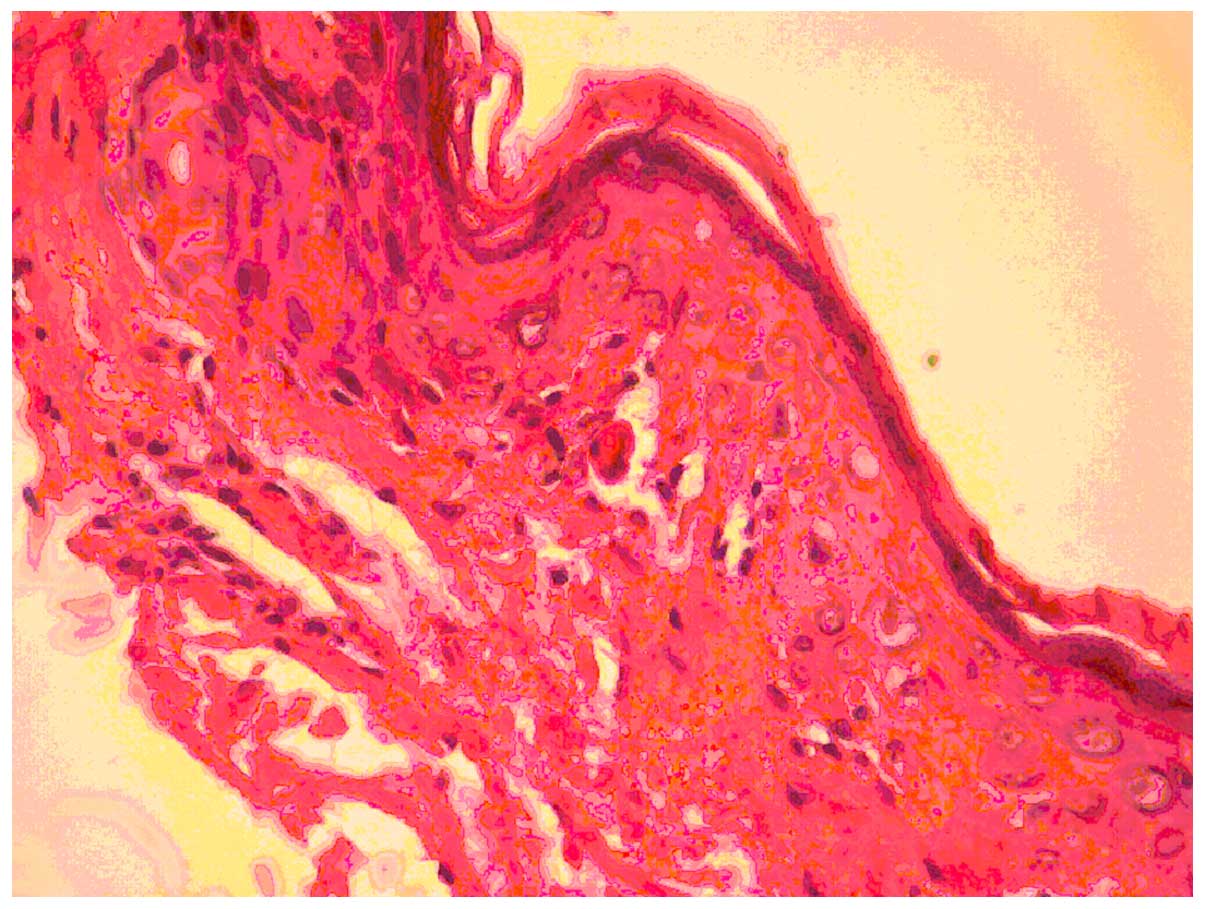
atrophic and sclerodermic skin on the thighs. Cutaneous
histological examination revealed atrophic epidermis, intense
collagenous sclerosis in the papillary dermis, basal cell
vacuolization and apoptotic keratinocytes that confirmed the GVHD
diagnosis (Fig. 1).
Immunosuppressive treatment was initiated with 1 mg/kg/day
methylprednisolone, and prophylactic treatment with 400 mg/day
fluconasol and 1,000 mg/day acyclovir. Despite this treatment,
sclerodermic features of the skin spread, involving progressively
the lower abdomen, thighs and forearms. This was considered as
progressive GVHD and the immunosuppressive therapy was increased,
initially with 2 mg/day tacrolimus, and then with 2 g/day
mycofenolate mofetil.
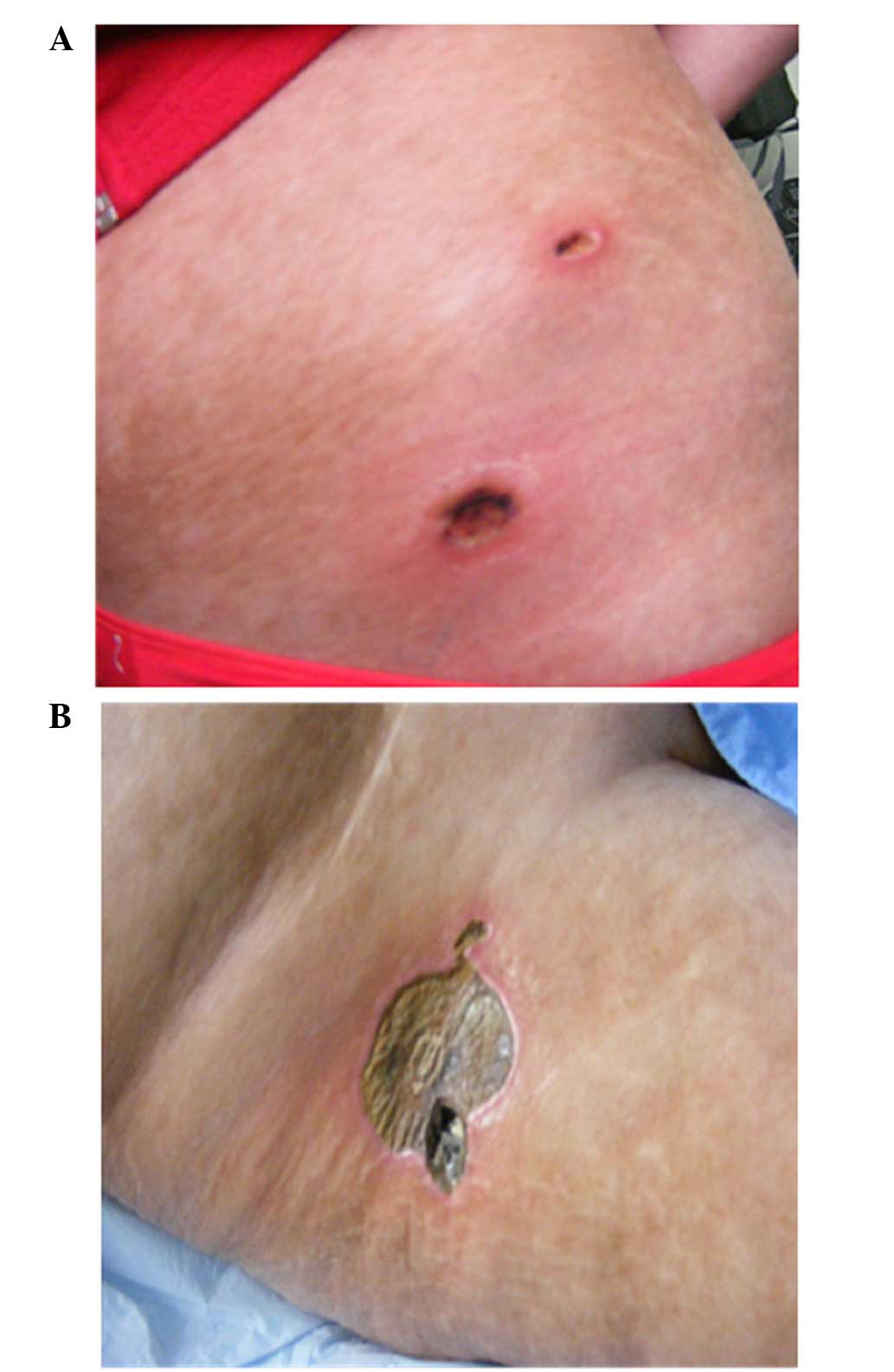
On day 330 after transplant the patient presented
with fever and several painful subcutaneous, tender, red nodules
that quickly became ulcerative, in addition to necrotic features on
the pelvic region and right leg localized on atrophic and
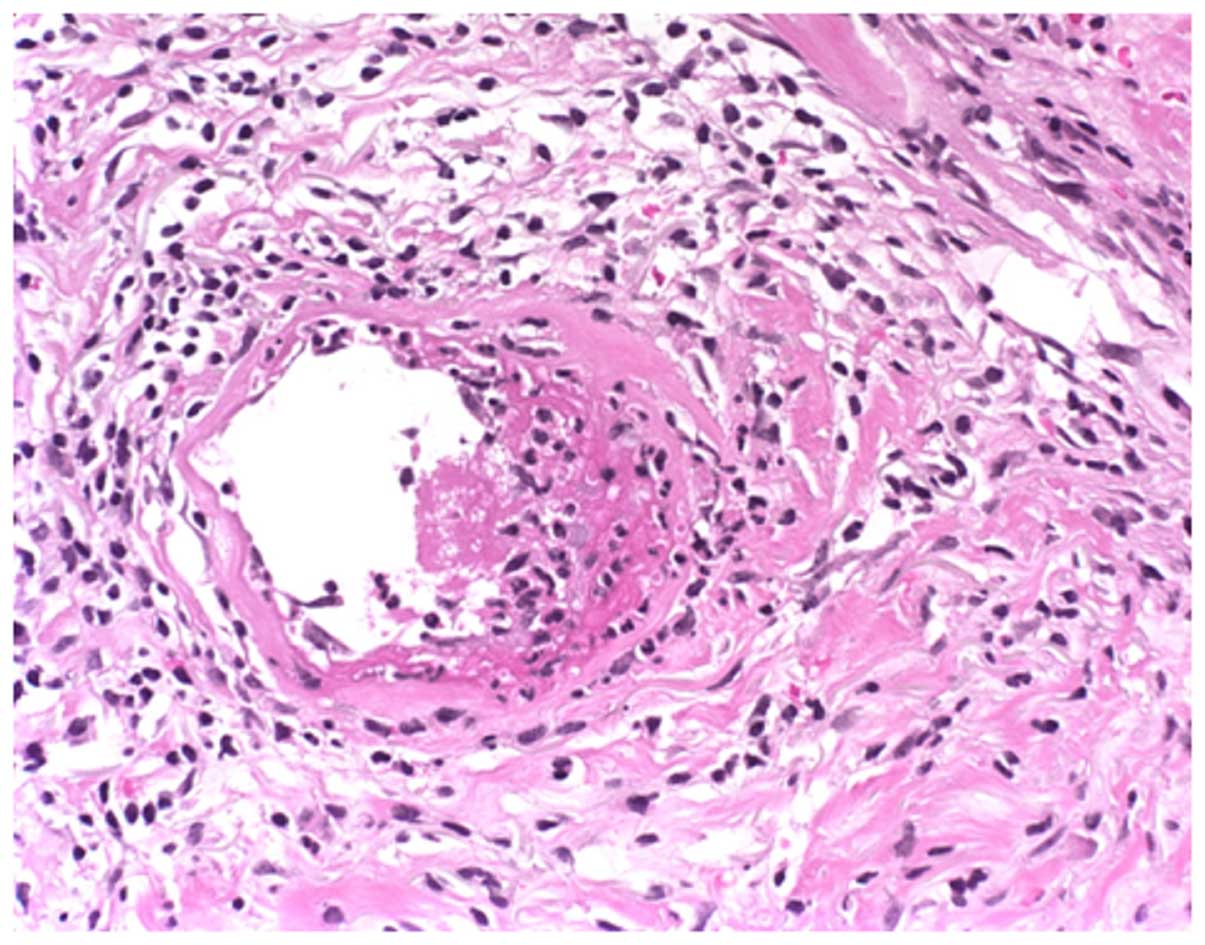
sclerodermic skin (Fig. 2). The skin
biopsy from one of these lesions at the level of reticular dermis
revealed intravascular embolus containing fungal hyphae elements
stained periodic acid-Schiff positive and lymphocytic infiltrate
around the vessel wall (Fig. 3).
When wide spectrum antibiotic treatments were
administered, the patient's condition was aggravated, with severe
acute respiratory and kidney insufficiency that required
ventilatory assistance and peritoneal dialysis (single sessions at
2–3-day intervals).
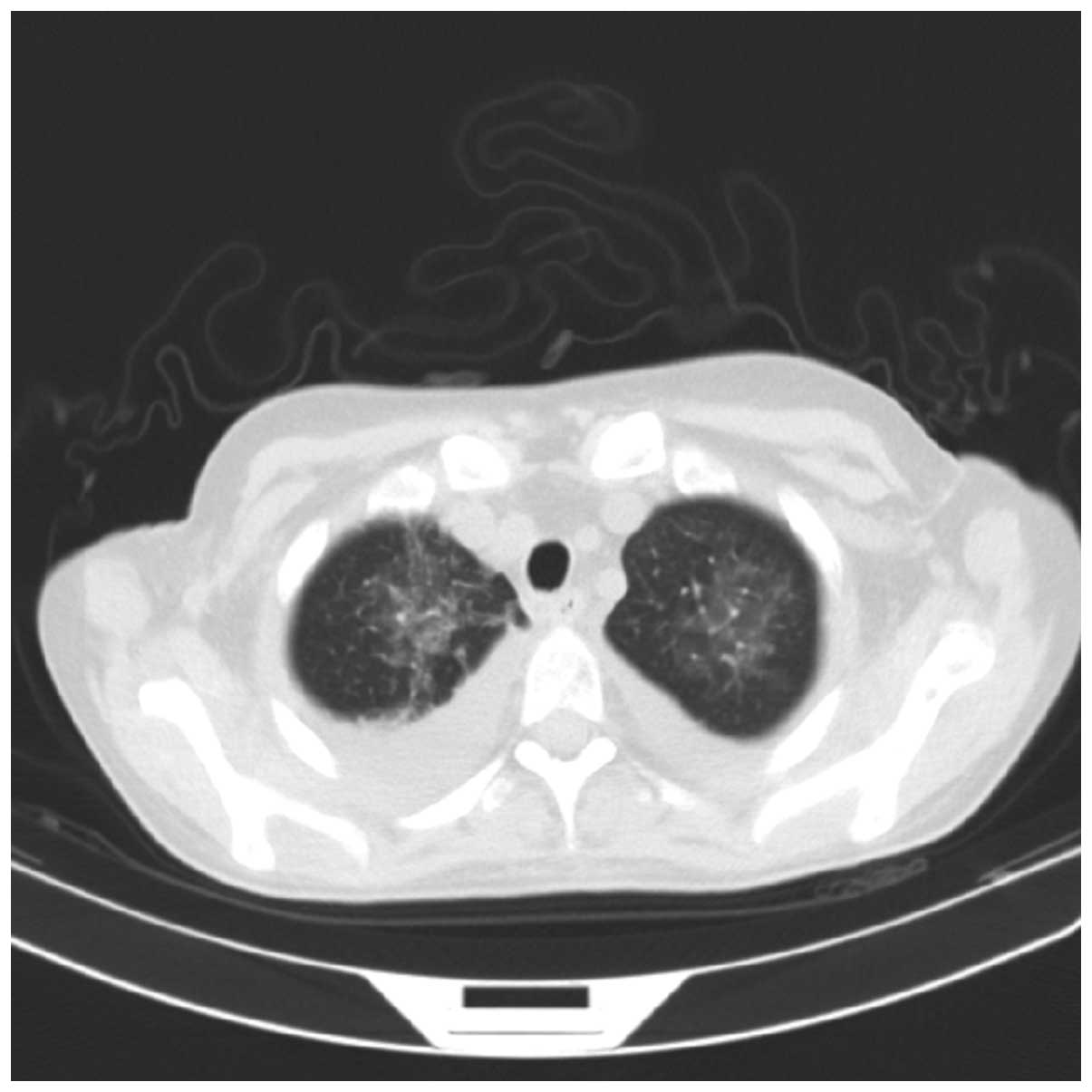
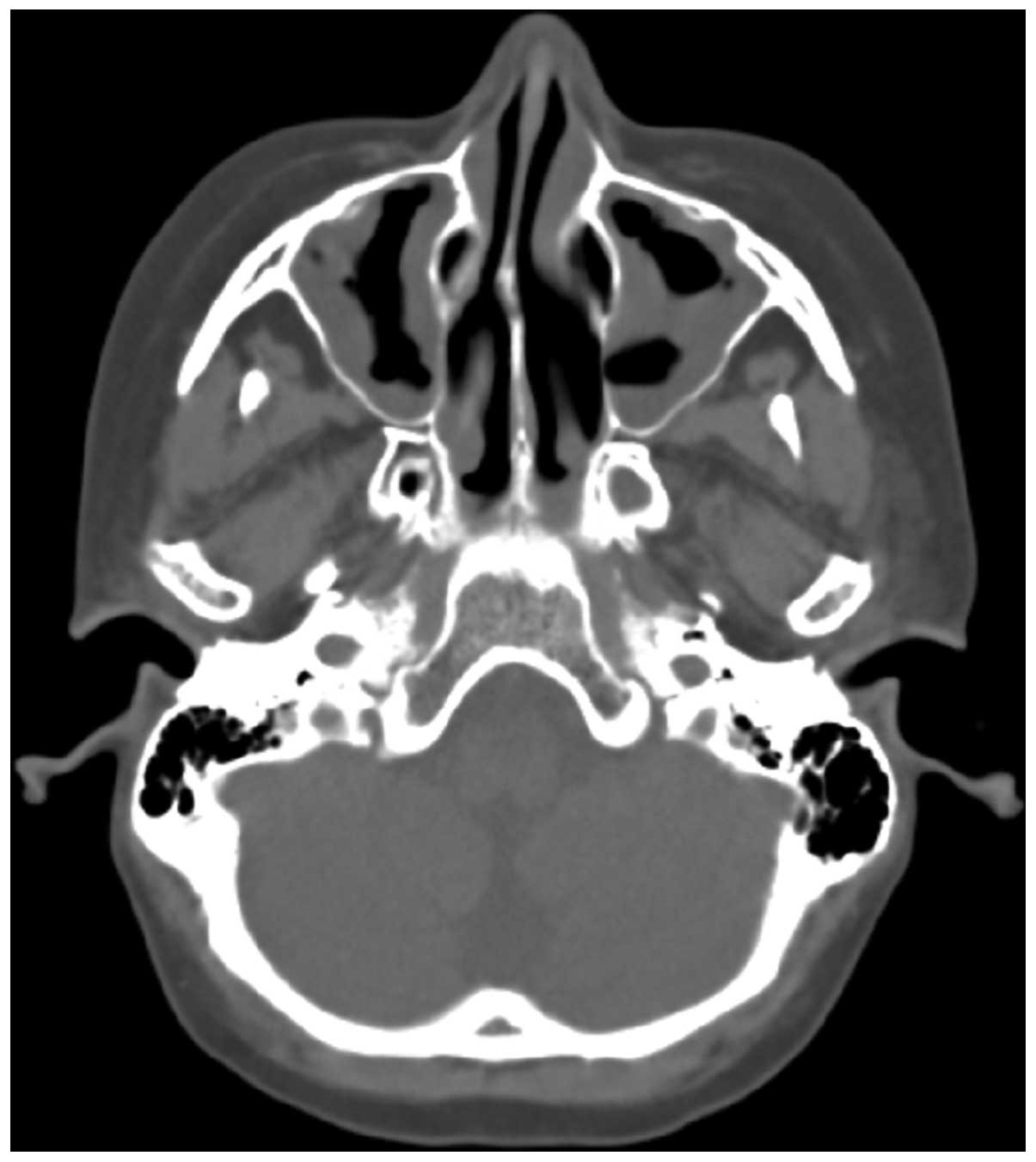
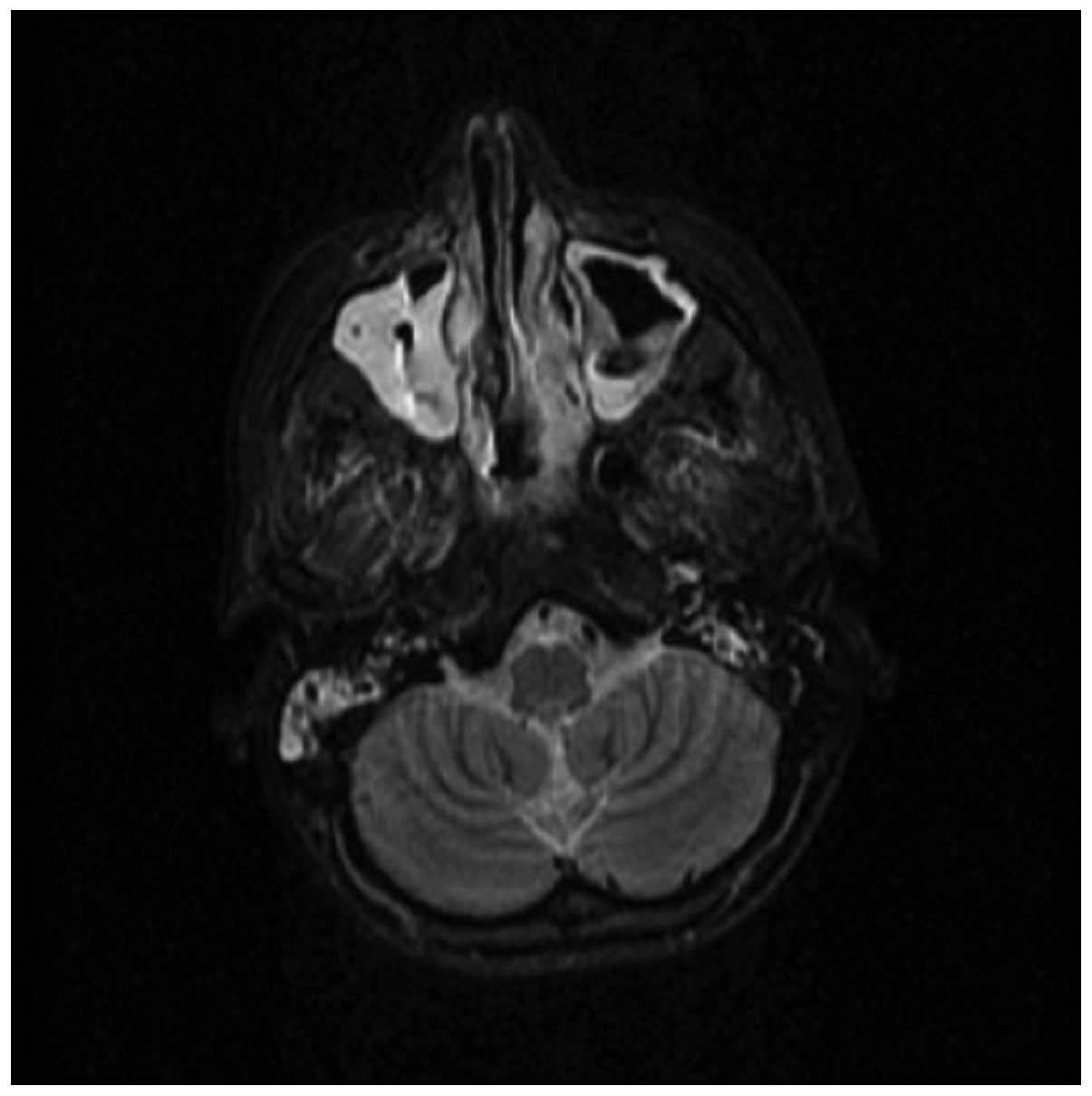
CT scanning of the lungs revealed extensive glass
infiltrative lesions (Fig. 4) and CT
scanning and magnetic resonance imaging of the facial sinuses
showed pansinusitis (Figs. 5 and
6).
Two swabs from skin lesions were performed and
cultured on Sabouraud dextrose agar, sheep blood agar and cystine
lactose electrolyte deficient agar. After 48 h, rapidly growing
fluffy colonies were observed, with a distinct rose-like surface
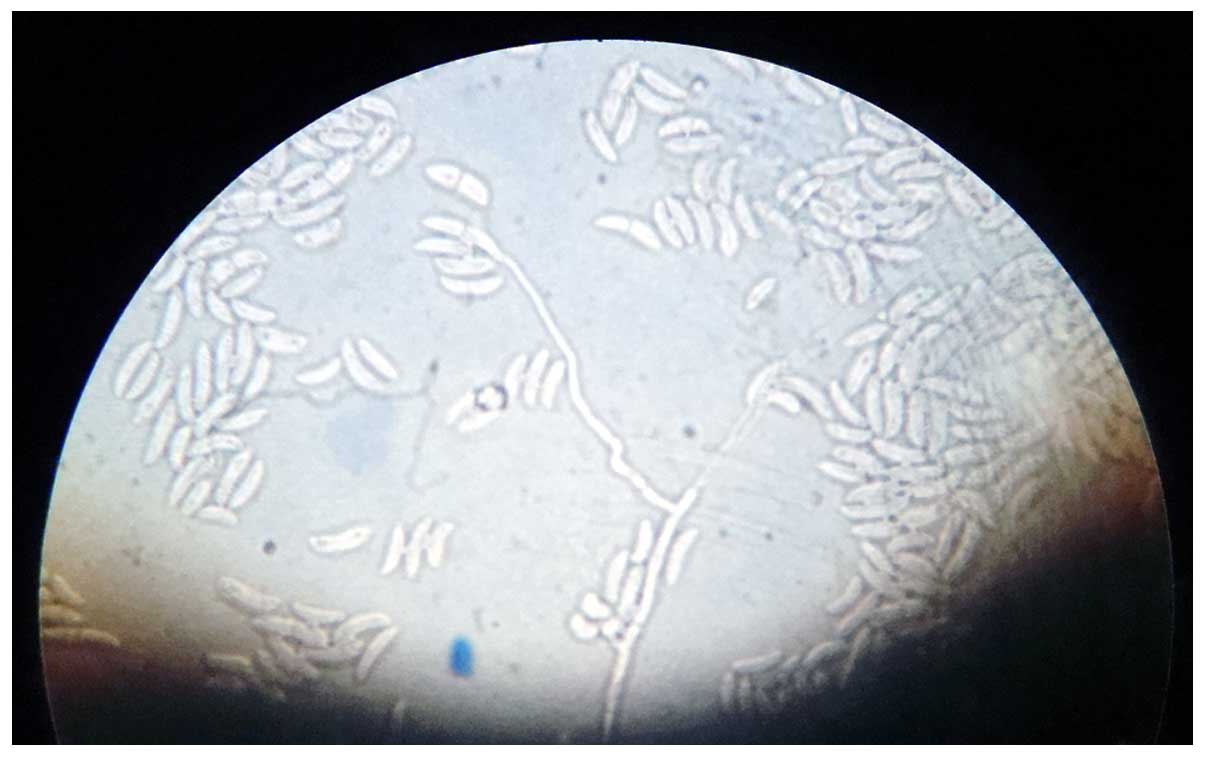
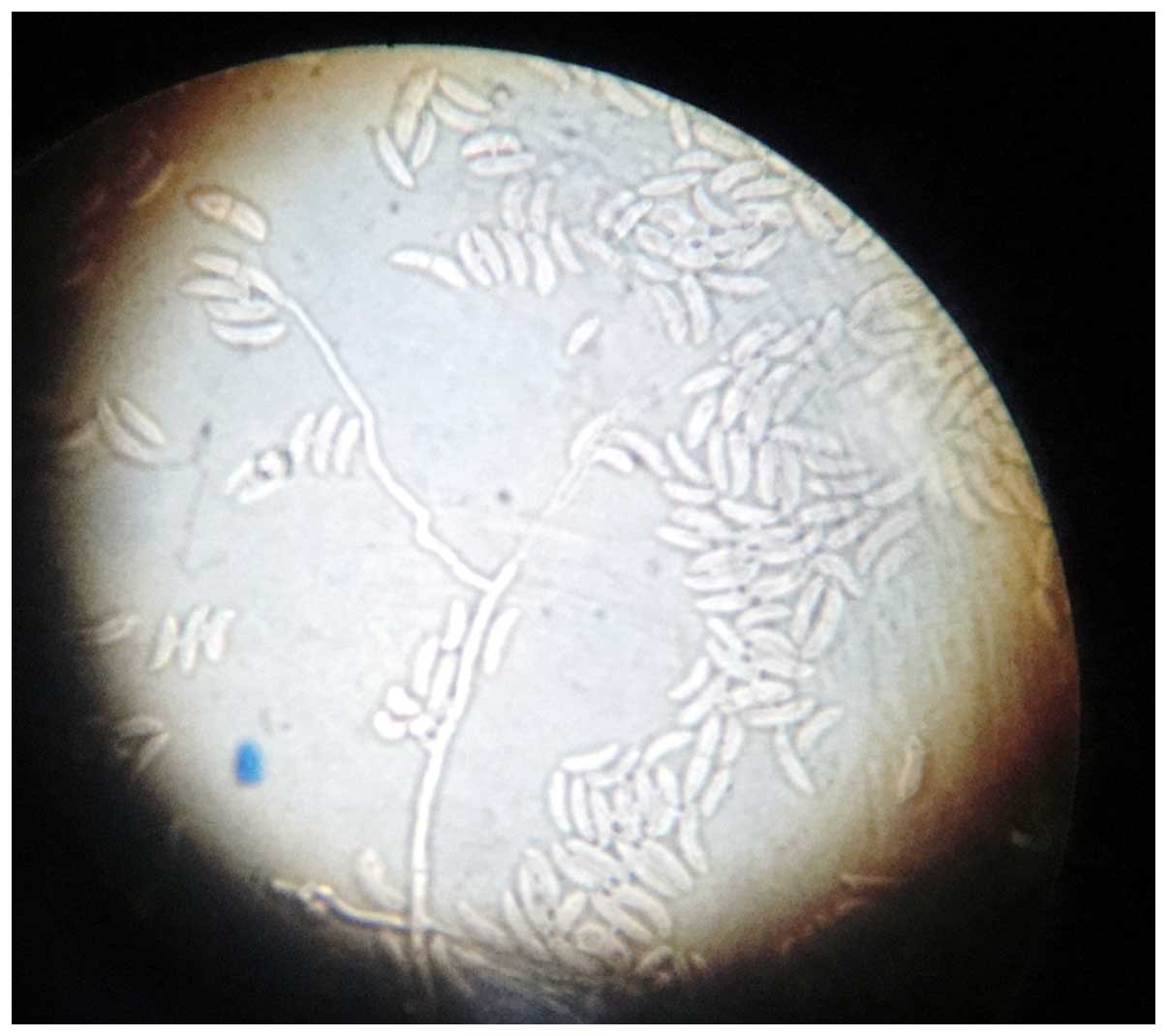
and reverse-side pigmentation (4–6 days; Fig. 7). Microscopic examination performed
by culture, with adhesive tape (lactophenol smear), revealed
hyaline filamentous moulds, producing conidia (microconidia and
macroconidia) in clusters. Of the hyaline filamentous molds,
Fusarium spp. is unique in producing microconidia and
macroconidia (7). The key to the
identification of Fusarium spp. was the observation of long,
sickle-form, multicellular macroconidia, separated by transverse
septa. These macroconidia may be described as ‘canoes’ or ‘boats’
(Fig. 8). Following the examination
of the culture and smear, it was concluded that the hyaline molds
were medically significant, producing conidia in clusters, and
comprised a Fusarium species.
Laboratory findings were as follows: Hemoglobin
level, 8,9 g/dl; leucopenia (3,000/mm3); mild neutropenia
(1,400/mm3); creatinine, 1.3 mg/dl; urea, 47 mg/dl; alkaline
phosphatase, 101 U/l; lactate dehydrogenase, 293 U/l; C-reactive
protein, 92 mg/l.
Repeated hemocultures were performed during fever
outbreaks without fungus identification. Correlating the
investigations with clinical aspects the diagnosis of
Fusarium species infection was established in this patient
with GHVD following allogeneic transplant.
Under these conditions, voriconazole therapy was
initiated while the GHVD immunosuppression therapy was
progressively reduced. While the treatment with intravenous
voriconazole was ongoing, which comprised a 6-mg/kg loading dose
every 12 h for the first 24 h, and a 4-mg/kg maintenance dose every
12 h thereafter, the cutaneous lesions initially improved, but the
patient's clinical condition deteriorated continuously. Despite
continued treatment with voriconazole, the patient succumbed with
respiratory insufficiency due to the overwhelming infection 400
days after receiving the transplant.
Written informed consent was obtained from the
patient's family prior to publication of the present study.
Discussion
There is a very high risk of contamination with
Fusarium species for patients who have received an
allogeneic bone marrow transplant, either early after transplant
(when engraftment is delayed), or later, due to deep
immunosuppression secondary to prolonged treatment with cortisone
for acute or chronic GVHD (2–4,8). Fusarium infections in
solid-organ transplant recipients have a localized character and a
better prognosis compared with those developed after hematologic
malignancies and bone marrow transplant (4).
Current studies have shown an increase in the
frequency of fungal infections caused by unusual opportunistic
fungi such as Fusarium species (9). The notable increase in organ-transplant
procedures and newer aggressive approaches to immunosuppression are
largely responsible for this shift.
It is known that >90% of cases of invasive
fusariosis are linked to immunosuppression and this appears
particularly in patients with hematologic malignancies and
neutropenia (2,4). Fusariosis occurs mostly in patients who
have received a mismatched or unrelated transplant (8). Nucci et al observed a tri-modal
distribution for invasive fusariosis in patients who received an
allogeneic HSCT, with a maximum incidence prior to engraftment, and
at ~62 days and 11 years after transplantation (1). Persistent neutropenia represents the
most important prognostic variable. In the management of
Fusarium infections, neutrophils play an important role.
Once Fusarium species enter the body, neutrophils attach to
the Fusarium hyphae and destroy them extracellularly through
oxidative cytotoxic mechanisms (10,11).
This mechanism is supported by the fact that patients with profound
and prolonged neutropenia and associated fusariosis show 100%
mortality even under substantial antifungal therapy (12). There are two factors involved in the
pathogenesis of fusariosis: one is the Fusarium strain's
virulence, and the other is the host's immune status where
immunosuppression plays an overwhelming role in the disease. The
aggressiveness of Fusarium species is caused by several
mycotoxins that they produce (13,14).
Some of these mycotoxins can cause leukopenia that prolongs
chemotherapy-induced bone marrow suppression (15). Fusarium species have
angiotropic and angioinvasive effects and can produce hemorrhagic
infarction, followed by decreased tissue perfusion and tissue
necrosis similar to that observed with Aspergillus species
and Zygomycetes species (4,8,10).
Patients who have received a transplant from a
matched unrelated donor or missmatch related donor and/or are
receiving therapy for extensive chronic GVHD may develop severe
T-cell-mediated immunodeficiency, which is a potential risk for
Fusarium infections (2,12). This
population of patients develops very late fusariosis. Patients with
hematologic cancer under glucocorticoids therapy showed 70%
mortality for fusariosis compared with 33% for those not receiving
glucocorticoids (11).
Histopathological diagnosis of fusariosis is made by
identifying fungi with septate hyphae and acute angle-branching.
These histological changes are difficult to distinguish from those
induced by the common fungus Aspergillus or of those
produced by the less common, relatively harmless fungus
Pseudallescheria boydii (16). For a more precise identification of
Fusarium species, blood or tissue cultures should be
performed. The results of these cultures can indicate a diagnosis
of proven or probable fusariosis. A diagnosis of probable
fusariosis is made for patients with clinical manifestations if the
Fusarium species are isolated and identified in respiratory
tract secretions in the absence of other pathogens or if there is a
positive culture from skin lesions but hyphae are not
histopathologically identified. A diagnosis of proven fusariosis
can be made if Fusarium species are identified in blood
cultures or in cultures obtained from sterile sites taken from
patients with clinical signs of fungal infection or if hyphae and
the Fusarium species are identified together in the same
tissue (17).
Pathogenic fungi can be differentiated using new
molecular techniques such as in situ hybridization against
ribosomal RNA sequences (18) and
polymerase chain reactions (19–21). The
disadvantages of these techniques are their high cost and low
availability. However, certain studies have shown that these two
molecular techniques have promising results (18,21). In
the case of histologically identical fungi, it is very important to
correctly identify them as Fusarium and
Pseudallescheria are more resistant to antifungal
pharmacotherapy than is Aspergillus (22).
In cases of severe fusariosis, the therapeutic
alternatives are reduced. Once it is diagnosed, invasive fusariosis
requires immediate therapy because of its rapidly evolvement and
high mortality rate. An effective treatment for invasive fusariosis
has not yet been identified, but good results have been achieved
with high doses of amphotericin B, particularly in lipid
formulation and with antifungals from the triazole class such as
posaconazole and voriconazole. Voriconazole is indicated as the
first line therapy for fusariosis (23–25).
In the management of Fusarium infections,
preventive measures are more important than antifungal therapy,
firstly because the latter has a low rate of success in HSCT
recipients and secondly because Fusarium species are usually
resistant to this therapy. In this regard, the clinician must
carefully examine skin and tissue lesions, particularly
onychomycoses, as these are important sites of contamination with
Fusarium species (26,27). The
objectives in future therapies for fusariosis are suggested to be
reduction of the duration of neutropenia, reduction of
immunosuppressive therapy and the administration of novel
antifungal agents such as posaconazole and voriconazole (28,29).
In conclusion, it is important to underline that a
patient receiving an allogeneic stem cell transplant can be at risk
for invasive fusariosis and overlapping GVHD lesions with
Fusarium skin lesions may delay diagnosis and treatment.
Acknowledgements
This study was partially supported by the Sectoral
Operational Programme ‘Human Resources Development’, financed from
the European Social Fund and by the Romanian Government under the
contract number POSDRU/89/1.5/S/64109.
References
|
1
|
Nucci M, Marr KA, QueirozTelles F, Martins
CA, Trabasso P, Costa S, Voltarelli JC, Colombo AL, Imhof A,
Pasquini R, et al: Fusarium infection in hematopoietic stem cell
transplant recipients. Clin Infect Dis. 38:1237–1242. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Marr KA, Carter RA, Crippa F, Wald A and
Corey L: Epidemiology and outcome of mould infections in
hematopoietic stem cell transplant recipients. Clin Infect Dis.
34:909–917. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
3
|
Galimberti R, Torre AC, Baztán MC and
Rodriguez-Chiappetta F: Emerging systemic fungal infections. Clin
Dermatol. 30:633–650. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Campo M, Lewis RE and Kontoyiannis DP:
Invasive fusariosis in patients with hematologic malignancies at a
cancer center: 1998-2009. J Infect. 60:331–337. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Stanzani M, Tumietto F, Vianelli N and
Baccarani M: Update on the treatment of disseminated fusariosis:
Focus on voriconazole. Ther Clin Risk Manag. 3:1165–1173.
2007.PubMed/NCBI
|
|
6
|
Filipovich AH, Weisdorf D, Pavletic S,
Socie G, Wingard JR, Lee SJ, Martin P, Chien J, Przepiorka D,
Couriel D, et al: National Institutes of Health consensus
development project on criteria for clinical trials in chronic
graft-versus-host disease: I. Diagnosis and staging working group
report. Biol Blood Marrow Transplant. 11:945–956. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Girmenia C, Pagano L, Corvatta L, Mele L,
del Favero A and Martino P: The epidemiology of fusariosis in
patients with haematological diseases. Gimema Infection Programme.
Br J Haematol. 111:272–276. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Minor RL Jr, Pfaller MA, Gingrich RD and
Burns LJ: Disseminated Fusarium infections in patients following
bone marrow transplantation. Bone Marrow Transplant. 4:653–658.
1989.PubMed/NCBI
|
|
9
|
Jain A, Jain S and Rawat S: Emerging
fungal infections among children: A review on its clinical
manifestations, diagnosis, and prevention. J Pharm Bioallied Sci.
2:314–320. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Clemons KV, Calich VL, Burger E, Filler
SG, Grazziutti M, Murphy J, Roilides E, Campa A, Dias MR, Edwards
JE Jr, et al: Pathogenesis I: Interactions of host cells and fungi.
Med Mycol. 38(Suppl 1): S99–S111. 2000. View Article : Google Scholar
|
|
11
|
Kontoyiannis DP, Bodey GP, Hanna H, Hachem
R, Boktour M, Girgaway E, Mardani M and Raad II: Outcome
determinants of fusariosis in a tertiary care cancer center: The
impact of neutrophil recovery. Leuk Lymphoma. 45:139–141. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Nucci M, Anaissie EJ, QueirozTelles F,
Martins CA, Trabasso P, Solza C, Mangini C, Simões BP, Colombo AL,
Vaz J, et al: Outcome predictors of 84 patients with hematologic
malignancies and Fusarium infection. Cancer. 98:315–319. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Short DP, O'Donnell K, Zhang N, Juba JH
and Geiser DM: Widespread occurrence of diverse human pathogenic
types of the fungus Fusarium detected in plumbing drains. J Clin
Microbiol. 49:4264–4272. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Pitt JI: Toxigenic fungi: Which are
important? Med Mycol. 38(Suppl 1): S17–S22. 2000. View Article : Google Scholar
|
|
15
|
Perfect JR: The impact of the host on
fungal infections. Am J Med. 125(Suppl): S39–S51. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Muhammed M, Coleman JJ, Carneiro HA and
Mylonakis E: The challenge of managing fusariosis. Virulence.
2:91–96. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
DePauw B, Walsh TJ, Donnelly JP, Stevens
DA, Edwards JE, Calandra T, Pappas PG, Maertens J, Lortholary O,
Kauffman CA, et al: European Organization for Research and
Treatment of Cancer/Invasive Fungal Infections Cooperative Group;
National Institute of Allergy and Infectious Diseases Mycoses Study
Group (EORTC/MSG) Consensus Group: Revised definitions of invasive
fungal disease from the European Organization for Research and
Treatment of Cancer/Invasive Fungal Infections Cooperative group
and the National Institute of Allergy and Infectious Diseases
Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis.
46:1813–1821. 2008. View
Article : Google Scholar : PubMed/NCBI
|
|
18
|
Hayden RT, Isotalo PA, Parrett T, Wolk DM,
Qian X, Roberts GD and Lloyd RV: In situ hybridization for the
differentiation of Aspergillus, Fusarium, and Pseudallescheria
species in tissue section. Diagn Mo Pathol. 12:21–26. 2003.
View Article : Google Scholar
|
|
19
|
Leal SM Jr, Vareechon C, Cowden S, Cobb
BA, Latgé JP, Momany M and Pearlman E: Fungal antioxidant pathways
promote survival against neutrophils during infection. J Clin
Invest. 122:2482–2498. 2012. View
Article : Google Scholar : PubMed/NCBI
|
|
20
|
Walsh TJ, Francesconi A, Kasai M and
Chanock SJ: PCR and single-strand conformational polymorphism for
recognition of medically important opportunistic fungi. J Clin
Microbiol. 33:3216–3220. 1995.PubMed/NCBI
|
|
21
|
Hennequin C, Abachin E, Symoens F, Lavarde
V, Reboux G, Nolard N and Berche P: Identification of Fusarium
species involved in human infections by 28S rRNA gene sequencing. J
Clin Microbiol. 37:3586–3589. 1999.PubMed/NCBI
|
|
22
|
Pfaller MA, Messer SA, Hollis RJ and Jones
RN: SENTRY Participants Group: Antifungal activities of
posaconazole, ravuconazole, and voriconazole compared to those of
itraconazole and amphotericin B tested against 239 clinical
isolates of Aspergillus spp. and other filamentous fungi: Report
from the SENTRY antimicrobial surveillance program, 2000.
Antimicrob Agents Chemother. 46:1032–1037. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Nucci M and Anaissie E: Cutaneous
infection by Fusarium species in healthy and immunocompromised
hosts: Implications for diagnosis and management. Clin Infect Dis.
35:909–920. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
24
|
Bodey GP, Boktour M, Mays S, Duvic M,
Kontoyiannis D, Hachem R and Raad I: Skin lesions associated with
Fusarium infection. J Am Acad Dermatol. 47:659–666. 2002.
View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Segal BH, Almyroudis NG, Battiwalla M,
Herbrecht R, Perfect JR, Walsh TJ and Wingard JR: Prevention and
early treatment of invasive fungal infection in patients with
cancer and neutropenia and in stem cell transplant recipients in
the era of newer broad-spectrum antifungal agents and diagnostics
adjuncts. Clin Infect Dis. 44:402–409. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Anaissie EJ, Kuchar RT, Rex JH,
Francesconi A, Kasai M, Müller FM, Lozano-Chiu M, Summerbell RC,
Dignani MC, Chanock SJ and Walsh TJ: Fusariosis associated with
pathogenic Fusarium species colonization of a hospital water
system: A new paradigm for the epidemiology of opportunistic mold
infections. Clin Infect Dis. 33:1871–1878. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Raad I, Tarrand J, Hanna H, Albitar M,
Janssen E, Boktour M, Bodey G, Mardani M, Hachem R, Kontoyiannis D,
et al: Epidemiology, molecular mycology, and environmental sources
of Fusarium infection in patients with cancer. Infect Control Hosp
Epidemiol. 23:532–537. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
28
|
Dannaoui E, DesnosOllivier M,
GarciaHermoso D, Grenouillet F, Cassaing S, Baixench MT, Bretagne
S, Dromer F and Lortholary O: French Mycoses Study Group: Candida
spp. with acquired echinocandin resistance, France, 2004-2010.
Emerg Infect Dis. 18:86–90. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Ho DY, Lee JD, Rosso F and Montoya JG:
Treating disseminated fusariosis: Amphotericin B, voriconazole or
both? Mycoses. 50:227–231. 2007. View Article : Google Scholar : PubMed/NCBI
|