Introduction
Premature ejaculation (PE) is a common type of
sexual dysfunction that affects approximately 20–30% of all men
ranging from 18 to 55 years of age (1,2). PE is
detrimental to self-confidence and the relationship with a partner
(3,4). Lifelong PE is that which occurs from
the first sexual experience and remains a problem throughout life.
Ejaculation occurs too rapidly, either prior to vaginal penetration
or <2 min afterwards (3,4). Currently, pharmacotherapy is the
primary treatment for lifelong PE; however, PE is an off-label
indication for all medical treatments (with the exception of
dapoxetine in some countries) (3).
Chronic selective serotonin reuptake inhibitors (SSRIs) and
on-demand topical anaesthetic agents are the only drugs to have
consistently shown efficacy in PE (3). Although there is some evidence of good
efficacy in PE, all drugs have shown several adverse effects, such
as fatigue, drowsiness, yawning, nausea, vomiting, dry mouth,
diarrhoea and perspiration that, in the majority of cases, cause a
high rate of patient drop-out (3,5). In this
sense, the therapeutic armamentarium for PE treatment is not highly
satisfactory.
Phytotherapeutics are an interesting treatment
option because of their generally low incidence of side effects and
high acceptance by patients. The present authors have focused
attention on certain compounds that may be useful for the treatment
of PE. Rhodiola rosea is a noteworthy phytotherapeutic
compound; it has been used for centuries in traditional medicine to
stimulate the nervous system, enhance physical and mental
performance and treat fatigue (6).
The administration of Rhodiola rosea extract has been shown
to elicit antidepressant activity (7). This effect is likely due to its
activity on the serotoninergic pathway (7). Moreover, it has been reported that
folic acid plays important roles in the synthesis of serotonin,
also known as 5-hydroxytryptamine (5-HT) (8). Therefore, it may be hypothesised that
folic acid supplementation could cure premature ejaculation via the
same mechanism, that is, by interacting with monoamine
neurotransmitters in the brain, as an alternative to SSRIs
(8). Moreover, biotin and folic acid
contribute to normal psychological function and this effect should
be useful in the management of patients with PE (8,9).
Finally, the healthy human prostate accumulates a higher level of
zinc than any other soft tissue in the body, and several prostate
diseases arise from changes in zinc metabolism (10). The present study aimed to evaluate
the tolerability and efficacy of a combination of Rhodiola
rosea, folic acid, biotin and zinc (EndEP®) in the
treatment of patients affected by lifelong PE. To the best of our
knowledge, this is the first study to assess the efficacy of a
phytotherapeutic compound on PE in a phase I–II trial.
Materials and methods
Study design
All patients with a clinical and instrumental
diagnosis of lifelong PE according to the European Association of
Urology (EAU) guidelines and the International Society for Sexual
Medicine (ISSM) recommendations (3,4),
attending three Italian tertiary Urological Institutions
(Department of Urology of Santa Chiara Regional Hospital, Trento;
University of Naples Federico II, Naples; University of Foggia,
Foggia) from July to December 2014 were enrolled in this
prospective, multicentre, phase I–II study. All patients underwent
clinical and instrumental examinations and International Prostatic
Symptom Score (IPSS), International Index of Erectile Function
(IIEF-15), Premature Ejaculation Diagnostic Tool (PEDT) and Short
Form (SF)-36 questionnaires were administered. Moreover, a
stop-watch estimation of intravaginal ejaculation latency time
(IELT) and all patient-reported outcomes (PROs) were collected. In
addition, urine examination and urine culture were performed.
Following enrolment, all patients received oral tablets of
EndEP® (one tablet/day) for 90 days.
Inclusion and exclusion criteria
PE was defined in accordance to the ISSM as follows:
‘A male sexual dysfunction characterised by ejaculation which
always or nearly always occurs before or within about 1 min of
vaginal penetration, and the inability to delay ejaculation on all
or nearly all vaginal penetrations, and negative personal
consequences, such as stress, bother, frustration and/or the
avoidance of sexual intimacy’ (4).
Patients were eligible for inclusion if they met all the following
criteria: Aged between 18 and 45 years; in a stable relationship
with a partner for ≥6 months and engaging in sexual intercourse
once a week or more often; and affected by life-long PE (with a
baseline IELT ≤60s) (4). All
enrolled patients were naive to any therapy for PE. All patients
affected by major concomitant diseases such as diabetes, liver
and/or renal failure; with known anatomical abnormalities or
malignancy of the urinary tract or bladder, upper tract stones,
diverticula, foreign bodies, prostatitis, active urinary tract
infection, chronic retention or polycystic kidney disease were
excluded. All patients with concomitant pharmacological therapy for
erectile dysfunction, with clinical suspicion of secondary PE and
all patients in chronic therapy for depression (SSRIs) were also
excluded. In cases of clinical suspicion of secondary PE due to
urinary tract infections or sexually transmitted disease, such as
Chlamydia trachomatis, Ureaplasma urealyticum or
Neisseria gonorrhoeae, a Meares-Stamey test and urethral
swab were performed, in line with Cai et al (11). All patients with positive
microbiological culture were excluded. Moreover, all patients with
an allergy to one or more of the components of EndEP®
were also excluded.
Study and treatment schedule
On arrival at each Centre, all eligible individuals
signed a standard informed consent form for off-label therapy and
new drugs under investigation, underwent a baseline questionnaire
and urological examination with anamnestic interview, in accordance
with the procedure described in EAU guidelines (3). All patients who met the inclusion
criteria underwent oral therapy with EndEP® (one
tablet/day) for 90 days. All patients were contacted by telephone
on day 30 of the therapy to ensure the dosing and timing of
treatment was correct. Each subject was scheduled for follow-up
examination at 90 days from starting therapy, with a urological
visit, and IPSS, IIEF-15, PEDT and SF-36 questionnaires. Moreover,
all PROs were collected. No placebo arm was included. The possible
biases caused by the lack of placebo arm were considered in the
analysis of the results. Figure 1
shows a flow-chart of the study protocol. Clinical failure was
defined as the persistence of symptoms following the treatment, or
the suspension of therapy for significant reported adverse effects.
In addition, spontaneously reported adverse events, or those noted
by the investigator, were recorded during the whole study period.
All subjects gave written informed consent before entering the
study. The study was conducted in line with Good Clinical Practice
guidelines, with the ethical principles laid down in the latest
version of the Declaration of Helsinki. Ethical approval was not
required due to the fact that the compound is registered in the
Italian Pharmacopeia for clinical use as a nutraceutical.
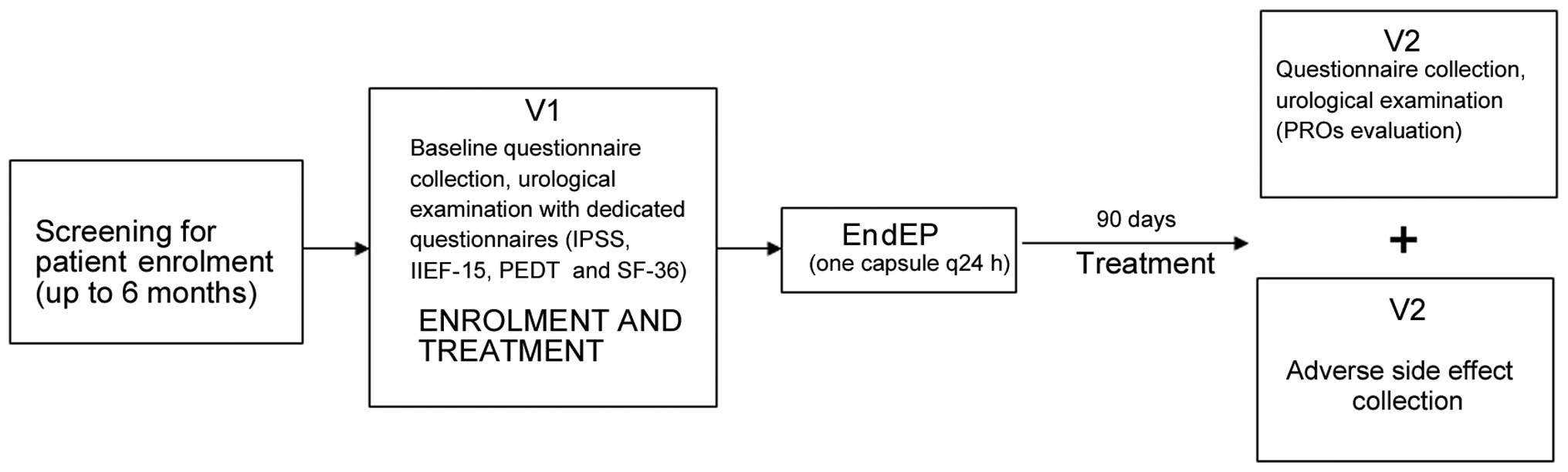 | Figure 1.Study flow-chart in accordance with
consolidated standards of reporting trials criteria. IPSS,
international prostatic symptom score; IIEF, international index of
erectile function; PEDT, premature ejaculation diagnostic tool; SF,
short form; PROs, patient reported outcomes; q24 h, once every 24
h, V1, Visit 1, at the time of enrolment; V2, Visit 2, at the
follow-up, 90 days after the start of treatment. |
Questionnaires and urological
examinations
The validated Italian versions of the IPSS (12), IIEF-15 (13) and PEDT (14) were administered to each patient. In
line with Jannini et al, a careful urological visit with
disease history collection was performed at arrival at each Centre
(15). Moreover, patient quality of
life (QoL) was measured using an Italian version of the SF-36
Health Survey, a test particularly suitable for chronic conditions
(16). The questionnaire was offered
to each patient on arrival at the Centre. All questionnaires were
also used when determining the efficacy of clinical therapy. The
patients and their partners were interviewed individually and each
was requested to give an independent estimation of IELT.
Pre-treatment IELT was measured during a 4-week baseline period;
the patients were provided with a stop watch and instructions on
how to measure IELT, and were requested to experience coitus at
least four times, as reported by Pastore et al (17). Couples were instructed not to use
condoms or any topical anaesthetic cream, and not to pause during
intercourse or have interrupted intromission. Furthermore, the
patients were instructed that if intercourse took place more than
once in a single session, only the first intercourse was to be
measured (17).
Composition and characterisation of
the extracts used
All patients were orally administered
EndEP® once daily, as a tablet in the morning
immediately after breakfast. Each EndEP® tablet (450 mg)
contained 200 mg Rhodiola rosea, 10 mg zinc, 200 µg folic
acid and 50 µg biotin. All compound analyses were carried out
according to the methods described by Fiamegos et al
(18).
Statistical analysis
Normal distribution of the variables was assessed
using the Kolmogorov-Smirnov test, histograms, and P-P plots. If
necessary, the data were log (ln) transformed to achieve a normal
distribution. Data were analysed based on the intention-to-treat
approach. General characteristics of the study participants were
expressed using descriptive statistics (means, standard deviation
and ranges). For each dependent variable, changes from baseline
were calculated by subtracting the baseline value from the
end-of-trial value. Analysis of variance was used for comparing
means, and the Bonferroni adjustment test was used at the second
stage of the analysis of variance. The sample size was calculated
prospectively under the following conditions: Difference between
the groups=10% (reduction in PEDT questionnaire score), α error
level=0.05 two-sided, statistical power = 80% and anticipated
effect size (Cohen's d=0.5). The calculation yielded 72
individuals. Assuming a dropout rate of approximately 20%, 86
patients should be enrolled into the study. The main outcome
measure was the difference from baseline in PEDT questionnaire,
mean IELT and PROs at the end of the follow-up period. P<0.05
was considered to indicate a statistically significant difference.
SPSS software, version 11.0 (SPSS Inc., Chicago, IL, USA) was used
to conduct the statistical analyses.
Results
Study population
From a total population of 95 enrolled patients, 3
patients were excluded for lack of information and 1 patient was
lost during follow-up; thus, 91 patients (mean age, 33.6±9.4 years)
were finally analysed. Anamnestic and clinical data at enrolment
are presented in Table I.
 | Table I.Patient sociodemographic, anamnestic
and clinical characteristics at the time of enrolment. |
Table I.
Patient sociodemographic, anamnestic
and clinical characteristics at the time of enrolment.
| Characteristic | Values |
|---|
| Total no. of
patients | 91 |
| Age, median ± SD | 33.6±9.4 |
| Educational level, n
(%) |
|
| Primary
school | – |
| Secondary
school | 53 (58.2) |
|
Post-secondary education | 38 (41.8) |
|
Sexually active in the past
month, n (%) | 91 (100) |
| BMI in
kg/m2, mean ± SD | 25.9±5.2 |
|
Smoking, n (%) | 30 (32.9) |
| Alcohol
use, n (%) | 11 (12.0) |
| No. of partners, n
(%) |
|
| 1 | 88 (96.7) |
| ≥1 | 3 (3.3) |
| Symptom scores at
baseline, mean ± SD |
|
|
IPSS |
1.1±1.6 |
|
IIEF-15 |
26.1±2.9 |
|
PEDT |
15.3±3.4 |
|
SF-36 |
98.2±0.5 |
| IELT at
baseline, sec | 73.6±46.9 |
Compliance with treatment schedule and
adverse effects
Compliance was observed in 91 patients (95.8%).
Accordingly, compliance to the study protocol was high. The
EndEP® formulation was well tolerated in all patients
analysed and there were no significant drug-related side effects.
Four of the 91 patients (4.4%) had mild adverse effects that did
not require the treatment to be suspended. The most common adverse
effects were mild nausea and mild headache.
Clinical and questionnaire results at
follow up
At the follow-up examination (90 days after
treatment initiation), statistically significant differences were
identified between mean IELT time at enrolment and following
treatment (73.6±46.9 vs. 102.3±60.0s; P<0.001), PEDT score
(15.3±3.4 vs. 12.2±3.2; P<0.001) and SF-36 questionnaire score
(98.2±0.5 vs. 99.4±0.1; P<0.001). Moreover, 55 out of 91
patients reported improvement in control of ejaculation (PRO
evaluation; 60.4%). At the follow-up examination (3 months after
treatment), no statistically significant differences were found in
terms of IPSS or IIEF-15 scores (P=0.19 and P=0.64, respectively).
Table II shows all questionnaire
results at enrolment and at the follow-up visit.
| Table II.Questionnaire results at enrolment
and at the follow-up visit. |
Table II.
Questionnaire results at enrolment
and at the follow-up visit.
|
| Values (mean ±
SD) |
|
|---|
|
|
|
|
|---|
| Symptom | Enrolment | Follow-up
visit | P-value |
|---|
| Symptom scores |
|
|
|
| IPSS |
1.1±1.6 |
1.4±1.5 | 0.19 |
| IIEF-15 | 26.1±2.9 | 26.3±3.1 | 0.64 |
| PEDT | 15.3±3.4 | 12.2±3.2 | <0.001 |
| SF-36 | 98.2±0.5 | 99.4±0.1 | <0.001 |
| IELT, sec |
73.6±46.9 | 102.3±60.0 | <0.001 |
Discussion
Despite PE being among the most common types of
sexual dysfunction in male patients and regardless of the
increasing interest in PE in the field of sexual medicine, highly
satisfactory treatments in terms of efficacy and safety are lacking
(19). Moreover, although dapoxetine
as an on-demand SSRI, several daily SSRIs and local anaesthetics
have been introduced for the treatment of PE, numerous patients
continue to suffer from PE due to a lack of definite treatment
(19). This is probably due to i)
high dropout rates from the treatment and ii) the high prevalence
of adverse events (5). A previous
study reported that 12.6% of patients (6/48) dropped out from a
6-week daily SSRI trial due to side effects (20). The reported side effects were
fatigue, drowsiness, nausea and vomiting, dry mouth, decreased
libido and erectile dysfunction (5,20).
Another important aspect to highlight is that even if the preferred
management of PE is on-demand dapoxetine or daily SSRIs, many
urologists had used other treatment options in 35% of the initial
treatment cases and 50% of the second-line treatment cases
(21). This demonstrates that there
is a deficiency in the management of PE patients. The results of
the present study show that the use of a combination of Rhodiola
rosea, folic acid, biotin and zinc (EndEP®) is able
to improve a patient's ejaculatory control, with a higher IELT and
higher level QoL. Moreover, a high level of treatment compliance
has been reported, probably due to the low frequency of adverse
events and the efficacy of the treatment in terms of ejaculatory
control improvement.
Ejaculation is controlled by a complex reflex arc
that involves the central and peripheral nervous systems, with an
important role of a single neurotransmitter, 5-HT (22). Chen et al previously
demonstrated that Rhodiola rosea extract is able to improve
the level of 5-HT in the hippocampus in an animal model (7), highlighting the role of this extract in
the modulation of the level of serotonin. Moreover, Hung et
al in a systematic review concluded that Rhodiola rosea
might have beneficial effects on physical performance, mental
performance and certain mental health conditions (23). Even if no specific study had been
performed on patients affected by PE, it could be hypothesised that
Rhodiola rosea would effect an improvement of ejaculatory
control and thereby improve QoL and sexual satisfaction. An
important aspect to highlight is the low prevalence of adverse
events; of the 446 subjects examined in the 11 clinical trials
included in another review, five adverse events were mentioned in
only three studies (24). Moreover,
folic acid has been shown to influence the metabolism of 5-HT
(25). An animal study confirmed
that folic acid relieves depression, possibly through the 5-HT
receptor (25). Recently, Yan et
al investigated the role of serum folic acid levels in patients
with erectile dysfunction and/or PE (26). The authors concluded that there were
positive correlations between serum folic acid concentrations and
questionnaire results on sexual function (26). These findings demonstrated a strong
association between serum folic acid levels and sexual dysfunction,
possibly due to an effect of folic acid on the metabolism of nitric
oxide and 5-HT (26). Moreover, the
impact of several ions on male sexual function has been
investigated (27). In particular,
zinc ion has been demonstrated to have an important role in
prostate health and in ejaculatory reflex health (28). Finally, biotin contributes to normal
psychological and sexual function and this effect should be useful
in the management of patients with PE (29).
The present study shows some strengths of the
treatment. Firstly, the use of phytotherapy for the treatment of PE
was well accepted by the patients (95.7% compliance to the
protocol). Moreover, the very low prevalence of adverse events
contributed to the high compliance with the protocol. Furthermore,
the exclusion of all patients with concomitant therapy for PE is a
very important aspect to highlight, as it enabled the present study
to demonstrate the effects of EndEP® alone. However,
even if the results are encouraging, this study has several
limitations. Firstly, it lacks a placebo arm; however, this study
was planned without a placebo arm as we consider it unethical to
not treat patients with PE when it impacts their QoL. Moreover, the
short follow-up period did not allow the possible long-term adverse
side effects to be evaluated.
In conclusion, the present study found that
EndEP® significantly improved the ejaculatory control
and quality of sexual life of patients affected by lifelong PE,
with a very low rate of short- and mid-term adverse events. This is
the first study to address the tolerability and efficacy of a
phythotherapeutic compound in the management of lifelong PE in a
phase I–II trial.
Acknowledgements
The authors are grateful to Professor John Denton
from the University of Florence for manuscript language
revision.
Glossary
Abbreviations
Abbreviations:
|
PE
|
premature ejaculation
|
|
5-HT
|
5-hydroxytryptamine
|
|
IPSS
|
international prostatic symptom
score
|
|
IIEF
|
international index of erectile
function
|
|
PEDT
|
premature ejaculation diagnostic
tool
|
|
IELT
|
intravaginal ejaculation latency
time
|
|
QoL
|
quality of life
|
|
PROs
|
patient-reported outcomes
|
References
|
1
|
Laumann EO, Nicolosi A, Glasser DB, Paik
A, Gingell C, Moreira E and Wang T: GSSAB Investigators' Group:
Sexual problems among women and men aged 40–80 y: Prevalence and
correlates identified in the global study of sexual attitudes and
behaviors. Int J Impot Res. 17:39–57. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Porst H, Montorsi F, Rosen RC, Gaynor L,
Grupe S and Alexander J: The Premature ejaculation prevalence and
attitudes (PEPA) survey: Prevalence, comorbidities and professional
help-seeking. Eur Urol. 51:816–823. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Hatzimouratidis K, Amar E, Eardley I,
Giuliano F, Hatzichristou D, Montorsi F, Vardi Y and Wespes E:
European Association of Urology: Guidelines on male sexual
dysfunction: Erectile dysfunction and premature ejaculation. Eur
Urol. 57:804–814. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Serefoglu EC, McMahon CG, Waldinger MD,
Althof SE, Shindel A, Adaikan G, Becher EF, Dean J, Giuliano F,
Hellstrom WJ, et al: An evidence-based unified definition of
lifelong and acquired premature ejaculation: Report of the second
international society for sexual medicine Ad Hoc committee for the
definition of premature ejaculation. J Sex Med. 11:1423–1441. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Mondaini N, Fusco F, Cai T, Benemei S,
Mirone V and Bartoletti R: Dapoxetine treatment in patients with
lifelong premature ejaculation: The reasons of a ‘Waterloo’.
Urology. 82:620–624. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Mannucci C, Navarra M, Calzavara E, Caputi
AP and Calapai G: Serotonin involvement in Rhodiola rosea
attenuation of nicotine withdrawal signs in rats. Phytomedicine.
19:1117–1124. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Chen QG, Zeng YS, Qu ZQ, Tang JY, Qin YJ,
Chung P, Wong R and Hägg U: The effects of Rhodiola rosea extract
on 5-HT level, cell proliferation and quantity of neurons at
cerebral hippocampus of depressive rats. Phytomedicine. 16:830–838.
2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Yin TL, Yang J, Zhang B, Yan WJ, Xu WM, Li
W, Yu L, Li SJ and Wu GX: Folic acid supplementation as adjunctive
treatment premature ejaculation. Med Hypotheses. 76:414–416. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Denisow B and Denisow-Pietrzyk M:
Biological and therapeutic properties of bee pollen. A review. J
Sci Food Agric. Mar 25–2016.(Epub ahead of print). View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Kolenko V, Teper E, Kutikov A and Uzzo R:
Zinc and zinc transporters in prostate carcinogenesis. Nat Rev
Urol. 10:219–226. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Cai T, Pisano F, Magri V, Verze P,
Mondaini N, D'Elia C, Malossini G, Mazzoli S, Perletti G, Gontero
P, et al: Chlamydia trachomatis infection is related to premature
ejaculation in chronic prostatitis patients: Results from a
cross-sectional study. J Sex Med. 11:3085–3092. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Badia X, Garcia-Losa M and Dal-Re R:
Ten-language translation and harmonization of the International
Prostate Symptom Score: Developing a methodology for multinational
clinical trials. Eur Urol. 31:129–140. 1997.PubMed/NCBI
|
|
13
|
Cappelleri JC, Rosen RC, Smith MD, Mishra
A and Osterloh IH: Diagnostic evaluation of the erectile function
domain of the international index of erectile function. Urology.
54:346–351. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Symonds T, Perelman MA, Althof S, Giuliano
F, Martin M, May K, Abraham L, Crossland A and Morris M:
Development and validation of a premature ejaculation diagnostic
tool. Eur Urol. 52:565–573. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Jannini EA, Maggi M and Lenzi A:
Evaluation of premature ejaculation. J Sex Med. 8(Suppl 4):
328–334. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Apolone G and Mosconi P: The italian SF-36
health survey: Translation, validation and norming. J Clin
Epidemiol. 51:1025–1036. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Pastore AL, Palleschi G, Fuschi A,
Maggioni C, Rago R, Zucchi A, Costantini E and Carbone A: Pelvic
floor muscle rehabilitation for patients with lifelong premature
ejaculation: A novel therapeutic approach. Ther Adv Urol. 6:83–88.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fiamegos YC, Nanos CG, Vervoort J and
Stalikas CD: Analytical procedure for the in-vial
derivatization-extraction of phenolic acids and flavonoids in
methanolic and aqueous plant extracts followed by gas
chromatography with mass-selective detection. J Chromatogr A.
1041:11–18. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Yang DY, Ko K, Lee WK, Park HJ, Lee SW,
Moon KH, Kim SW, Kim SW, Cho KS, Moon du G, et al: Urologist's
practice patterns including surgical treatment in the management of
premature ejaculation: A korean nationwide survey. World J Mens
Health. 31:226–231. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Waldinger MD, Hengeveld MW, Zwinderman AH
and Olivier B: Effect of SSRI antidepressants on ejaculation: A
double-blind, randomized, placebo-controlled study with fluoxetine,
fluvoxamine, paroxetine and sertraline. J Clin Psychopharmacol.
18:274–281. 1998. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Shindel A, Nelson C and Brandes S:
Urologist practice patterns in the management of premature
ejaculation: A nationwide survey. J Sex Med. 5:199–205. 2008.
View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Allard J, Truitt WA, McKenna KE and Coolen
LM: Spinal cord control of ejaculation. World J Urol. 23:119–126.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Hung SK, Perry R and Ernst E: The
effectiveness and efficacy of Rhodiola rosea L.: A systematic
review of randomized clinical trials. Phytomedicine. 18:235–244.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Ishaque S, Shamseer L, Bukutu C and Vohra
S: Rhodiola rosea for physical and mental fatigue: A systematic
review. BMC Complement Altern Med. 12:702012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Brocardo PS, Budni J, Kaster MP, Santos AR
and Rodrigues AL: Folic acid administration produces an
antidepressant-like effect in mice: Evidence for the involvement of
the serotonergic and noradrenergic systems. Neuropharmacology.
54:464–473. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Yan WJ, Yu N, Yin TL, Zou YJ and Yang J: A
new potential risk factor in patients with erectile dysfunction and
premature ejaculation: Folate deficiency. Asian J Androl.
16:902–906. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Omu AE, Al-Bader AA, Dashti H and Oriowo
MA: Magnesium in human semen: Possible role in premature
ejaculation. Arch Androl. 46:59–66. 2001. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kelleher SL, McCormick NH, Velasquez V and
Lopez V: Zinc in specialized secretory tissues: Roles in the
pancreas, prostate and mammary gland. Adv Nutr. 2:101–111. 2011.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Delost P and Terroine T: On the origin of
male sexual disorders due to a biotin deficiency. Hormone and
vitamin treatments. Arch Sci Physiol (Paris). 23:243–268. 1969.(In
French). PubMed/NCBI
|














