Introduction
Herpes simplex encephalitis (HSE) is associated with
high mortality and morbidity rates (1). Relapses and new infections at
anatomically different sites, including the eye, may occur due to
reactivation and neuronal translocation of the causative agent,
herpes simplex virus (HSV) (2). HSE
may be a risk factor for the development of acute retinal necrosis
(ARN), a rapidly progressing and potentially blinding eye disease
induced by HSV (2). ARN was
initially described as a rapidly progressive unilateral necrotizing
retinitis in 1971 by Urayama et al (3). The prevalence of the disease is equal
in both sexes and it typically occurs between the fifth and seventh
decades of life (4). To prevent a
poor outcome, ARN requires aggressive management (5). Although several case reports have
described the occurrence of ARN after herpetic encephalitis
(6), ARN following HSE is rare
(7). In the present case report, the
case of a healthy woman with bilateral ARN that occurred in
combination with HSE following treatment with intravenous acyclovir
is described.
Case report
A 47-year-old woman was admitted to the First
Teaching Hospital of Jilin University (Changchun, China) in October
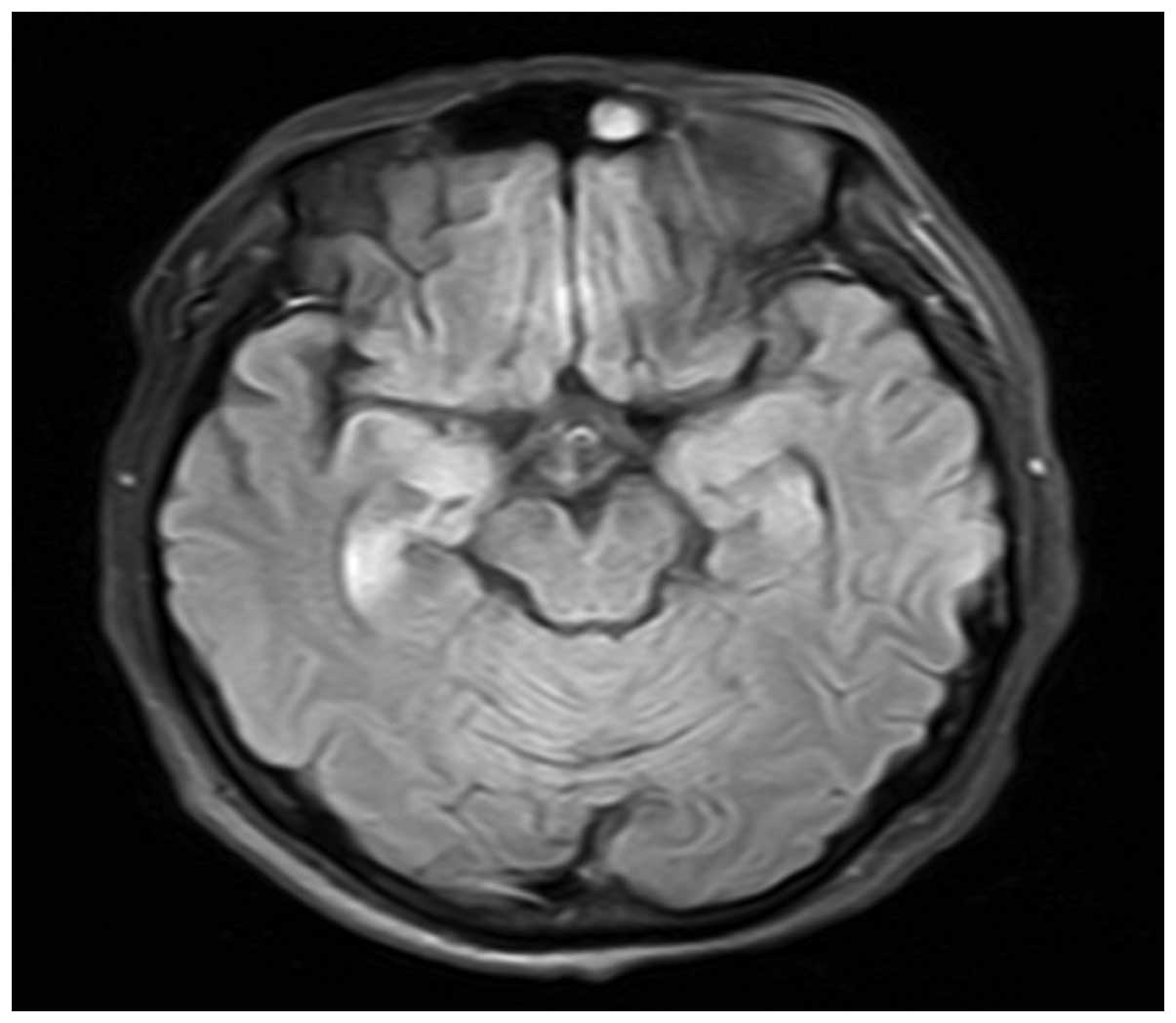
2013 with persistent high fever and somnolence for 5 days. Magnetic
resonance imaging (MRI) showed abnormal signals in the right medial
temporal lobes (Fig. 1). The history
of the patient included frequent oral herpes lesions and infection
of the upper respiratory tract. Therefore, viral encephalitis was
suspected and treatment with intravenous acyclovir (10 mg/kg) was
initiated and continued every 8 h. HSV-1 was identified in the
patient's serum and cerebrospinal fluid by polymerase chain
reaction (PCR), which was performed in our clinical laboratory.
Examination of the cerebrospinal fluid also showed that the
patient's glucose levels remained at a normal level (2.7 mmol/l;
normal range, 2.5–4.4 mmol/l), while the monocyte count was
elevated (2.7×107/l; normal range,
0–5×106/l). An electroencephalogram revealed
intermittent rhythmic slowing in the bilateral hemispheres.
Five days after admission, the patient's
consciousness was slightly improved, but she suddenly developed
blurred vision and visual pain bilaterally. Dexamethasone (15
mg/day; Jilin Aodong Pharmaceutical Group Co., Ltd., Jilin, China)
was administered intravenously for 15 days as an anti-inflammatory
adjunct to intravenous acyclovir therapy. A further 4 days later,
only light perception remained in both eyes. Examination of the
left eye revealed extensive vitritis and retinal thickening with
advanced retinal necrosis in the peripheral and central retina. The
optic disc was swollen along with an inferior retinal detachment,
extending to the macula. Extensive retinal vasculitis and
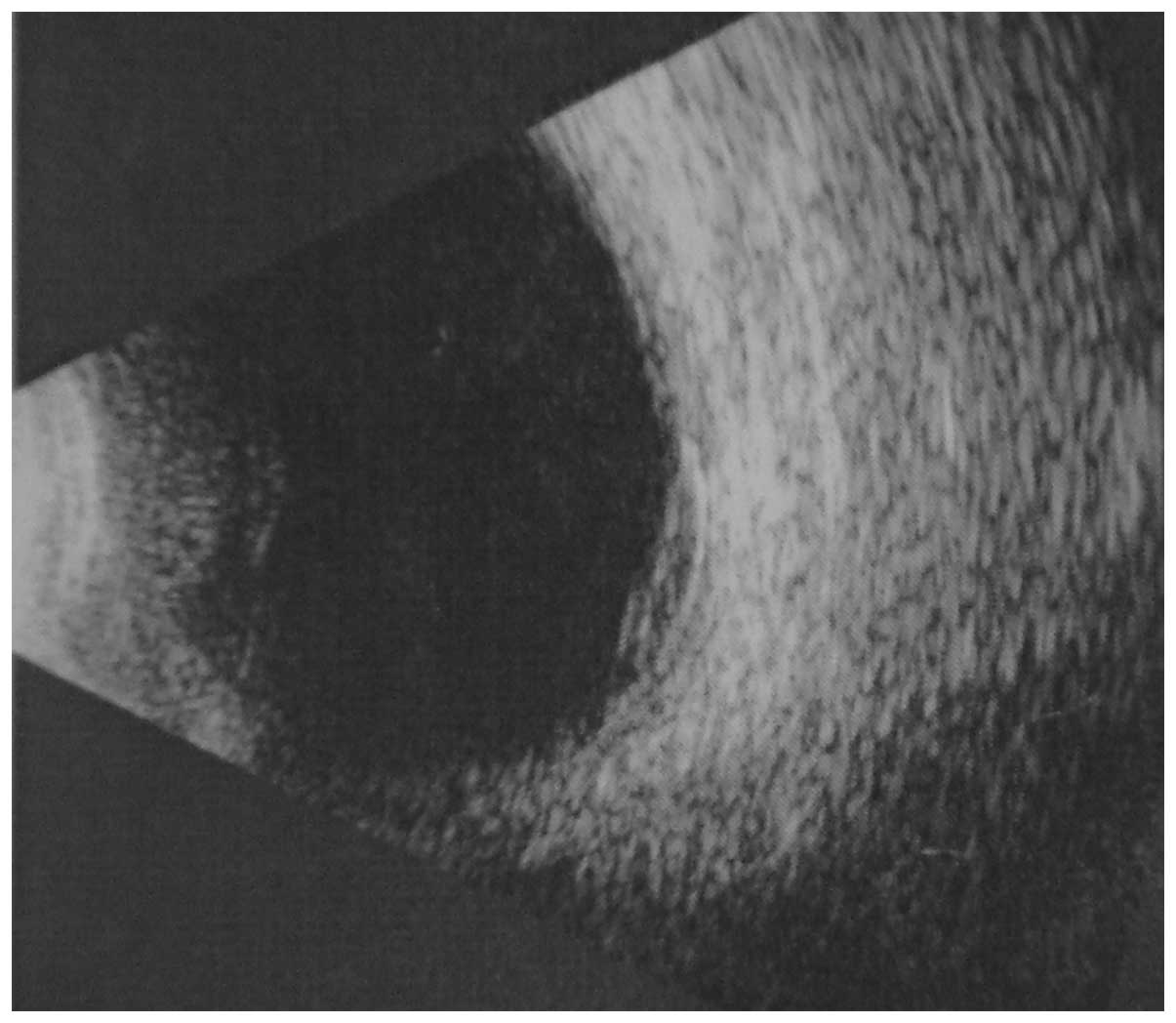
hemorrhage were observed. Ultrasound examination showed a thickened
temporal wall in the right eye (Fig.
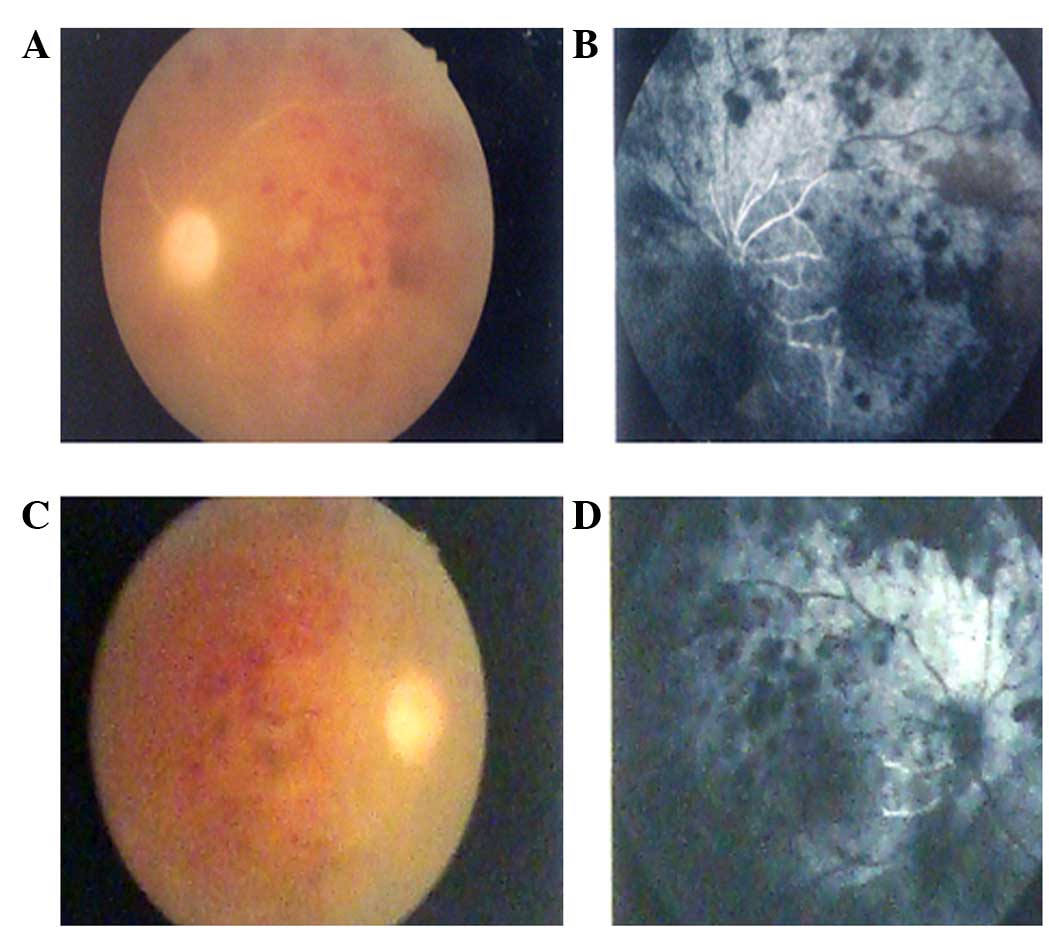
2). Fundus fluorescence angiography (FFA) was conducted in the
hospital ophthalmology department, and revealed bilateral vessel
obstruction and a large amount of low fluorescence, with a flaky
appearance, in the background (Fig.
3). HSE complicated with ARN was considered clinically, marked
by weak light perception. HSV-1 was also detected through vitreous
tap with PCR analysis and this confirmed the diagnosis. Following
diagnosis, the patient was treated with intravenously administered
acyclovir and dexamethasone, and mere light perception remained in
each eye.
Informed consent was obtained from the patient for
the publication of the present case study.
Discussion
The characteristics of ARN syndrome are anterior
segment inflammation, along with periorbital pain, and a loss of
vision due to vitreous opacification, necrotizing retinitis and,
occasionally, optic neuropathy (8).
In the past, ARN was only diagnosed clinically. However, as
understanding of the pathophysiology of ARN advanced, adjunct
laboratory tests were developed. According to the standard clinical
criteria of the American Uveitis Society (9), the diagnosis of ARN can be made on the
basis of focal, well-demarcated areas of retinal necrosis within
the peripheral retina; rapid, circumferential progression of
necrosis; and occlusive vasculopathy. PCR is a valuable diagnostic
tool for the diagnosis of ARN (10).
The patient described in the present case study manifested a
classic case of fulminant bilateral ARN. In contrast to recovery
from impaired light perception in reported cases of ARN syndrome
(11,12), the present patient responded poorly
to antiviral and steroidal treatments. The poor visual outcome of
this patient may be associated with impairment of the optic nerve
in addition to extensive retinal detachment and her possible poor
immune status.
HSV is the most common cause of acute viral
encephalitis (13). The majority of
infections in adults involve HSV-1, and few cases are attributed to
HSV-2 (14). HSE typically affects
the fronto-temporal lobe (1). The
results of MRI and electroencephalography support the diagnosis of
HSE in the present patient. The diagnosis of HSE complicated with
ARN was supported by clinical findings and analysis of the
cerebrospinal fluid and vitreous tap using PCR. The patient's
cerebrospinal fluid and vitreous tap tested positive for HSV-1.
Furthermore, the patient had a history of oral lesions. Although
the majority of cases of HSV-related retinitis are established
clinically, the patient's cerebrospinal fluid and vitreous tap
tested positive for HSV-1. Several reports have described a
retinitis that is consistent with ARN syndrome (6,7,15). However, to the best of our knowledge
there have not been any previous reports of fulminant HSE with ARN
syndrome in which the visual ability was reduced to mere light
perception within 4 days.
The potential of HSV to latently infect neurons
within the central nervous system is well established. HSV is
reactivated and spread via intra-axonal, trans-synaptic and
extracellular mechanisms, resulting in damaging effects on remote
and local tissue. The ability of HSV to migrate has been
demonstrated in an animal model, where recombinant HSV was injected
into the anterior chamber of one eye and retinitis subsequently
occurred in the other eye, due to viral migration along the
hypothalamus and contralateral optic nerve. It was hypothesized
that the virus may have migrated from the suprachiasmatic nucleus
to the retina by retrograde axonal transport along the optic nerve
(16). Vandercam et al
(17) described a case with an
overall interval of 5 weeks (from 14 days to 2 months) between
encephalitis and ARN. In the present patient, encephalitis occurred
~1 week prior to the symptoms of retinal disease. It is
hypothesized that activated virus in the medial temporal lobes may
have been transported to the retina axonally via the optic nerve,
resulting in ARN.
Acknowledgements
The authors thank Dr. He for his excellent
assistance in ophthalmology in the present study.
References
|
1
|
Whitley RJ: Herpes simplex virus
infections of the central nervous system: A review. Am J Med.
85:61–67. 1988.PubMed/NCBI
|
|
2
|
Ganatra JB, Chandler D, Santos C,
Kuppermann B and Margolis TP: Viral causes of the acute retinal
necrosis syndrome. Am J Ophthalmol. 129:166–172. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Urayama A, Yamad N, Sasaki T, et al:
Unilateral acute uveitis with retinal periretinal arteritis and
detachment. Jpn J clin Ophthalmol. 25:607–619. 1971.
|
|
4
|
Bodaghi B, Rozenberg F, Cassoux N, Fardeau
C and LeHoang P: Nonnecrotizing herpetic retinopathies masquerading
as severe posterior uveitis. Ophthalmology. 110:1737–1743. 2003.
View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Palay DA, Sternberg P Jr, Davis J, Lewis
H, Holland GN, Mieler WF, Jabs DA and Drews C: Decrease in the risk
of bilateral acute retinal necrosis by acyclovir therapy. Am J
Ophthalmol. 112:250–255. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gain P, Chiquet C, Thuret G, Drouet E and
Antoine JC: Herpes simplex virus type 1 encephalitis associated
with acute retinal necrosis syndrome in an immunocompetent patient.
Acta Ophthalmol Scand. 80:546–549. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Tada Y, Negoro K, Morimatsu M, Makino H
and Nishida T: Findings in a patient with herpes simplex viral
meningitis associated with acute retinal necrosis syndrome. AJNR Am
J Neuroradiol. 22:1300–1302. 2001.PubMed/NCBI
|
|
8
|
Sergott RC, Belmont JB, Savino PJ, Fischer
DH, Bosley TM and Schatz NJ: Optic nerve involvement in the acute
retinal necrosis syndrome. Arch Ophthalmol. 103:1160–1162. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Holland GN: Executive Committee of the
American Uveitis Society: Standard diagnostic criteria for the
acute retinal necrosis syndrome. Am J Ophthalmol. 117:663–667.
1994. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Tran TH, Rozenberg F, Cassoux N, Rao NA,
LeHoang P and Bodaghi B: Polymerase chain reaction analysis of
aqueous humour samples in necrotizing retinitis. Br J Ophthalmol.
87:79–83. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kianersi F, Masjedi A and Ghanbari H:
Acute retinal necrosis after herpetic encephalitis. Case Rep
Ophthalmol. 1:85–89. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hirota K, Akimoto M and Katsura T:
Bilateral acute retinal necrosis after herpetic meningitis. Clin
Ophthalmol. 6:551–553. 2012.PubMed/NCBI
|
|
13
|
Burk J and Miller JR: Infections of the
nervous systemMerritt's Textbook of Neurology. Rowland LP: Williams
and Wilkins; Baltimore, MD: pp. 1546–159. 1995
|
|
14
|
Whitley RJ: Herpes simples virusFields
Virology. Fields BN, Knipe DM and Howley PM: 3rd. Lippincott-Raven
Publishers; Philadelphia: pp. 2323–2330. 1996
|
|
15
|
Pepose JS, Kreiger AE, Tomiyasu U,
Cancilla PA and Foos RY: Immunocytologic localization of herpes
simplex type 1 viral antigens in herpetic retinitis and
encephalitis in an adult. Ophthalmology. 92:160–166. 1985.
View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Vann VR and Atherton SS: Neural spread of
herpes simplex virus after anterior chamber inoculation. Invest
Ophthalmol Vis Sci. 32:2462–2472. 1991.PubMed/NCBI
|
|
17
|
Vandercam T, Hintzen RQ, de Boer JH and
Van der Lelij A: Herpetic encephalitis is a risk factor for acute
retinal necrosis. Neurology. 71:1268–1274. 2008. View Article : Google Scholar : PubMed/NCBI
|