Introduction
Acute myocardial infarction (MI), with ST-segment
elevation, leads to chronic heart failure and death and results
from the sudden blockage of an epicardial coronary artery, thereby
causing the supplied myocardium to become ischemic, culminating in
permanent damage and scar tissue formation if circulation is not
restored. Scar tissue thus formed, lacks the contractile function
of the myocardium, and contributes to global left ventricular (LV)
dysfunction and finally to failure of the heart (1). Having recognized that it is a blood
clot that leads to ST-segment elevated MI, the timely restoration
of circulation to the affected myocardium was found to limit the
infarct size and also improve myocardial function (2). However, several lines of experimental
and clinical evidences showed that reperfusion of the ischemic
myocardium causes further damage and this is known as
ischemia-reperfusion injury (3).
Myocardial ischemia-reperfusion injury refers to myocardial damage
that occurs as a result of the interaction between substances that
accumulate during ischemia and those that are delivered on the
subsequent restoration of blood flow. Although the institution of
reperfusion following MI led to a marked reduction in mortality due
to MI-related heart failure, there is a significant increase in
surviving patients with chronic cardiac dysfunction that resulted
from ischemia-reperfusion injury (4,5). Indeed,
prolonged ischemia may account for up to 50% of the final MI size
(6) and causes multiple cellular
metabolic and ultra-structural changes and in fact, the size of the
infarct is a major determinant of the treatment outcomes and thus
the primary aim of MI treatment approaches is to reduce the infarct
size. The ischemia-reperfusion injury induces inflammatory
response, which is initially localized but eventually becomes
systemic and induces multi-organ dysfunction and accounts for
30–40% of intensive care unit mortality. Since reperfusion itself
has reduced the MI-related mortality, there has been a paradigm
shift in the treatment focus more towards the prevention or
amelioration of damage caused by reperfusion. However, it is
important to understand the mechanisms of myocardial
ischemia-reperfusion injury in order to develop therapies targeting
both ischemic and reperfusion damage, to reduce the infarct size,
considering that smaller infarct size can lead to better cardiac
function, over long-term. Despite a significant amount of research
as well as encouraging preclinical results with multiple agents,
most of the clinical trials to prevent reperfusion injury have been
disappointing (7) and thus it is
important to identify and develop therapies that potentially reduce
infarct size. In this review we briefly address the mechanisms
underlying the myocardial ischemia-reperfusion injury and the
currently available therapies.
Mechanism of myocardial ischemia-reperfusion
injury
The hypoperfused myocardial zone during MI due to
the coronary artery blockade is an area of myocardium that is under
perfused and this is known as ‘the area at risk (AAR)’, which
rapidly becomes necrotic if reperfusion is not established rapidly.
The salvaged myocardium, after reperfusion displays contraction
bands, karyolysis, abnormalities of mitochondria such as swelling,
and cardiomyocyte membrane disruption in association with
inflammation, interstitial hemorrhage and damaged microvasculature
(8). Myocardial ischemia-reperfusion
injury is a complex process, which involves several interrelated
factors, including a decrease in cellular adenosine triphosphate
(ATP) levels, accumulation of hydrogen ions, calcium overload, and
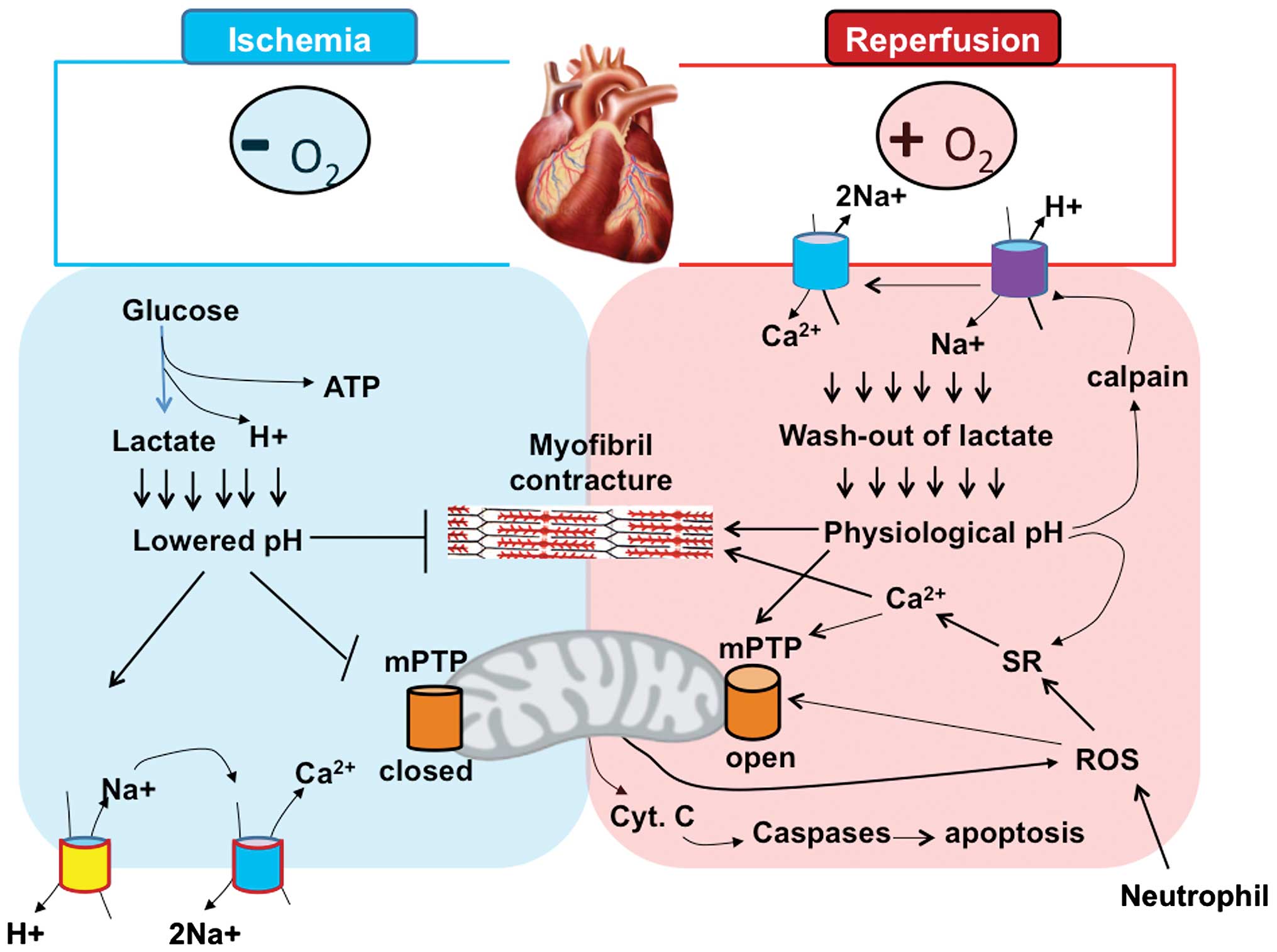
production of reactive oxygen species (ROS). These factors
collectively promote cellular injury and subsequent cardiomyocyte
death (Fig. 1).
Initially, ischemia causes mitochondrial oxidative
phosphorylation arrest due to a lack of sufficient oxygen, leading
to a reduction in ATP production. In order to compensate for this,
the affected cardiomyocytes conduct anaerobic glycolysis for ATP
production, which leads to the accumulation of protons and lactate,
resulting in intracellular acidosis. The elevated intracellular
H+ activates the plasma membrane
Na+/H+ exchanger, which expels the
H+ from the cell in exchange for Na+, leading
to an increase in intracellular Na+. Reduced activity of
Na+/K+-ATPase due to acid and insufficient
ATP, also contributes to the increase in intracellular
Na+, which leads to the activation of sarcolemmal
Na+/Ca2+ exchanger (9) and a build up of intracellular
Ca2+.
Following reperfusion, respiratory activity,
mitochondrial potential, and ATP synthesis are restored and
intracellular pH is restored rapidly to normal level, which causes
activation of Ca2+ dependent protease, calpain, which
degrades the cytoskeleton and the sarcolemma (10). The increased availability of ATP upon
reperfusion in the presence of increased Ca2+ activates
sarcoplasmic reticulum (SR) uptake of Ca2+, exceeding
the threshold of ryanodine channels, which release Ca2+
into the cytosol. Cyclic repetition of this process leads to
Ca2+ oscillations that lead to uncontrolled myofibrillar
hypercontraction (11) and also
promote opening of the mitochondrial permeability transition pore
(mPTP) (12). Opening of mPTP
results in mitochondrial matrix swelling, which triggers the
rupture of mitochondrial outer membrane and release of
mitochondrial intermembrane space contents such as cytochrome c, in
to cytosol. Cytochrome c sets the course of promoting the
programmed cell death by activating the caspase cascade. The
increased Ca2+ oscillations also enhance the activity of
xanthine oxidases, promoting the production of ROS, which further
exacerbate membrane damage by directly promoting opening of the
mPTP (13), and thus contribute to
cell death during reperfusion (14).
ROS is mostly produced by the different types of cells in the
ischemic zone, including the injured myocytes, endothelial cells
and neutrophils. Neutrophils entering the ischemic zone further
aggravate the cellular damage by releasing inflammatory mediators,
causing microvascular obstruction and local and eventually systemic
inflammation (15).
Non-pharmacological protective
approaches
The complexities of events that underlie the
ischemia-reperfusion injury have rendered it difficult to develop
satisfactory treatment approaches for this health problem. Various
studies have shown that damage caused by myocardial
ischemia-reperfusion can be prevented or limited by
non-pharmacological strategies such as ischemic pre-conditioning,
ischemic post-conditioning, and remote ischemic conditioning, as
well as hyperthermia (15).
Ischemic pre-conditioning
The phenomenon of ischemic pre-conditioning refers
to a therapeutic approach whereby repeated short episodes of
ischemia protect the myocardium against a subsequent total
occlusion of the coronary artery. This approach has been recognized
as the strongest form of in vivo protection against
myocardial ischemic injury, since it is most consistent and the
magnitude of protection achieved is larger than that from any other
intervention. It has been suggested that such pre-conditioning has
significant application prior to cardiac surgery. A brief period of
ischemia protects the heart from more prolonged episodes of
ischemia, and reduce not only the infarct size but also its
incidence, and also minimize severity of reperfusion-induced
arrhythmias, preventing endothelial cell dysfunction (16).
The mechanism underlying ischemic pre-conditioning
is very complex and is probably associated with the activation of
certain G-protein-coupled receptors (GPCR). There is also evidence
indicating the transactivation of receptor tyrosine kinase
activity, and the PI3K/Akt signaling pathway. As briefly
illustrated in Fig. 2, activation of
GPCR and PI3K/Akt leads to elevated activity of nitric oxide
synthase (NOS) and nitric oxide (NO) formation, as well as
guanylate cyclase and protein kinase G (PKG). Substrates for PKG
include the SR regulatory protein phospholamban, which promotes SR
Ca2+ uptake, and thus reduces cytosolic Ca2+
overload and inhibition of mPTP. Activation of Akt also inhibits
GSK-3β and pro-apoptosis members of the Bcl-2 protein family such
as Bad and Bim, thereby inhibiting mPTP opening.
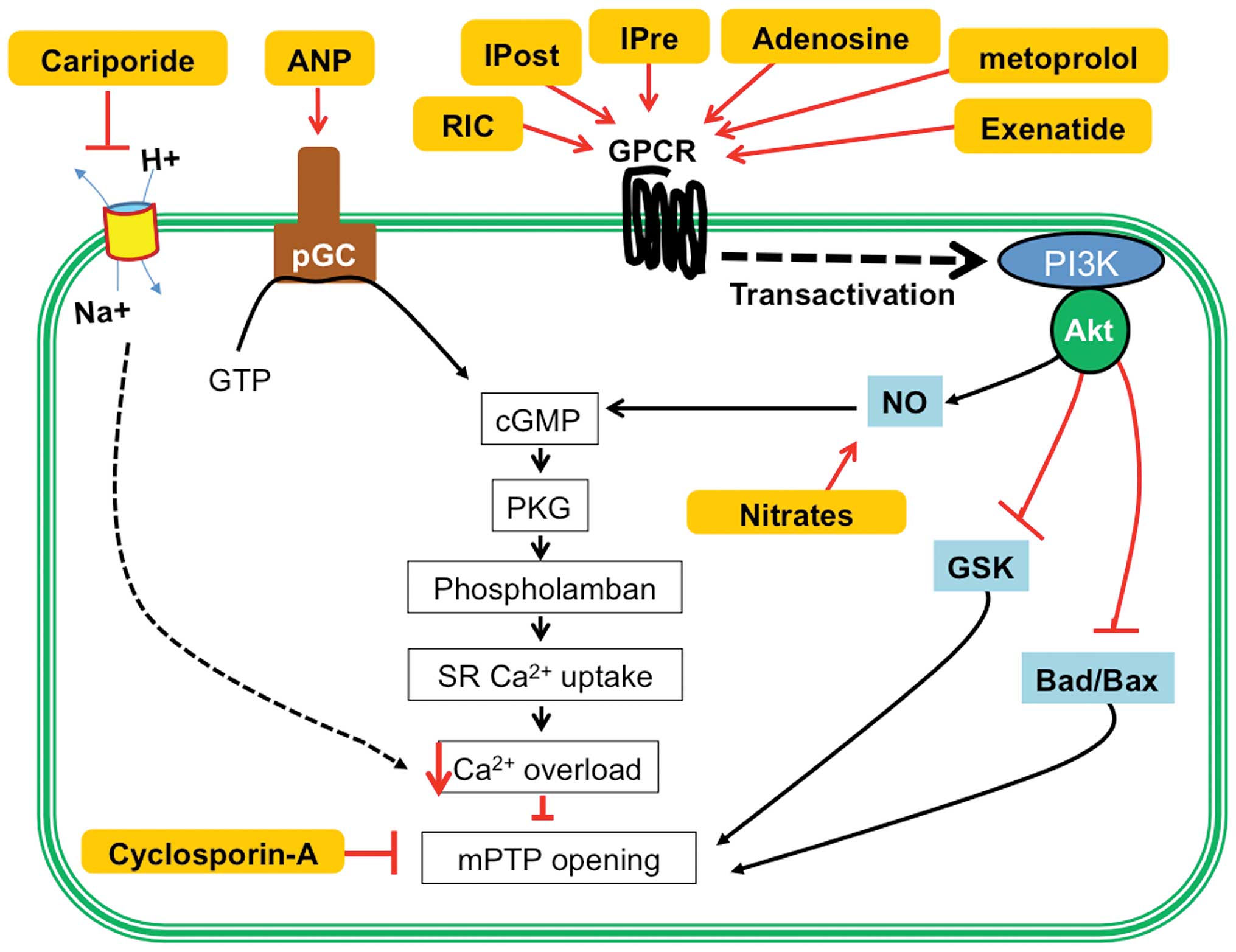 | Figure 2.The more promising strategies for
combating myocardial ischemia-reperfusion injury. ANP, atrial
natriuretic peptide; cGMP, cyclic guanylate monophosphate; GTP,
guanosine triphosphate; IPre, ischemic preconditioning; IPost,
ischemic postconditioning; NO, nitric oxide; pGC, particular
guanylate cyclase; PKG, protein kinase G; RIC, remote ischemic
conditioning; mPTP, mitochondrial permeability transition pore. |
Ischemic post-conditioning
The phenomenon of ischemic post-conditioning
encompasses introduction of brief cycles of ischemia/reflow soon
after the damaging prolonged ischemia followed by reperfusion
(17). Ischemic post-conditioning
has been shown to reduce infarct size, in some cases, equivalent to
that observed with ischemic pre-conditioning. In general, the
protection afforded by ischemic post-conditioning is weak or absent
after brief ischemic episodes that cause small infarcts (18). However, unlike ischemic
pre-conditioning, which delays the development of infarction,
post-conditioning reduces reperfusion injury. Although no standard
operating procedures have been defined, the post-conditioning
intervention must be done within the first few minutes following
reperfusion after ischemia. The mechanism by which
post-conditioning reduces reperfusion injury is less understood.
Several autacoids and kinases appear to share common roles in
classic pre- and post-conditioning (Fig.
2). Post-conditioning probably provides the protective effect
mainly by its ability to delay the normalization of intracellular
pH for few minutes, by slowing metabolite washout, secondary to
flow interruptions. These flow interruptions also reduce oxidative
damage and preserve the NO-cGMP-PKG signaling pathway and inhibit
Na+/H+ exchange and thus Ca2+
overload (19,20).
Remote ischemic conditioning
The phenomenon of remote ischemic conditioning
refers to the protection of the heart against acute
ischemia-reperfusion injury by applying brief episodes of
non-lethal ischemia and reperfusion to another organ or tissue. In
this approach, the therapeutic intervention is applied away from
the heart, to another organ or tissue, thereby facilitating its
clinical application (21). The
procedure is non-invasive and can be applied before and during
sustained ischemia and the onset of reperfusion. In fact, remote
ischemic conditioning can be achieved simply by inflating and
deflating a blood pressure cuff placed around the upper arm and
inducing three 5-min cycles of ischemia and reflow (21). Such therapeutic intervention has been
reported to be beneficial in patients undergoing cardiac surgery
(22). The infarct-size-limiting
effects of remote conditioning have been shown to be comparable to
the effects of ischemic post-conditioning (23). Although the mechanism by which remote
ischemic conditioning approach exerts cardiac protection is not
clear, two major hypotheses have been proposed: i) The neural
hypothesis, which states that autocoids released from the remote
ischemic organ affect the local afferent neural pathway, which in
turn, activates the efferent neural pathways to trigger end organ
protection; and ii) the humoral hypothesis, which states that
autocoids released from the ischemic remote organ are transported
to the end organ, the heart, resulting in the activation of kinase
signaling pathways, such as PI3K/Akt (24).
Rapid cooling
Therapeutic hypothermia, from mild hypothermia
(32–35°C), to moderate (28–32°C), severe (20–28°C), and profound
(<20°C) hypothermia is shown to be beneficial against myocardial
reperfusion injury in animal studies (25,26).
These studies have revealed that lowering myocardial temperature
during ischemia can limit infarct size via reductions in metabolic
demand, inflammatory response, platelet aggregation, and by
increasing myocardial efficiency. However, translation of these
beneficial effects to humans in clinical trials met with limited
success and this is mostly attributed to the cooling devices used,
such as endovascular heat exchange devices, which take considerable
time to induce reduction in core temperatures. Consequently, in
clinical studies employing such devices, only a minority of
patients were able to reach the target temperature of <35°C
before reperfusion. In a pilot study described by Götberg et
al (27) patients were randomly
exposed to hypothermia induced by intravenous infusion of cold
saline before reperfusion and all patients could attain a core body
temperature of <35°C before reperfusion and had reduction in
infarct size (27). In addition, no
increase in adverse events was seen. This pilot study demonstrated
that attaining a core body temperature of <35°C rapidly may be
effective in reducing myocardial infarct size and can be quickly
and safety induced without a significant delay in reperfusion.
Pharmacological cardioprotective
approaches
Elucidation of the mechanistic basis for myocardial
ischemia-reperfusion injury in various studies has resulted in the
identification of various pharmacological agents to protect the
heart. Some of the most promising cardioprotective strategies are
shown in Fig. 2.
Na+/H+ exchange
inhibitors
The build up of intracellular calcium resulting from
the inhibition of Na+/K+-ATPase and by the
hyperactivation of Na+/H+ exchanger in
cardiomyocytes during ischemia and reperfusion, is the rationale
for the use of Na+/H+ exchange inhibitors, to
protect the heart from ischemia-reperfusion injury. Cariporide has
been extensively studied and it demonstrated an attenuation of
reperfusion injury characterized by improved LV function (28). SM-20550, another
Na+/H+ exchange inhibitor, was compared with
nicorandil, a K-channel opener with nitrate-like activity. Both
reduced infarct size in a dose-dependent manner when given
pre-ischemia but only SM-20550 was beneficial when given
post-ischemia (29). Besides the
cardioprotective effects, several lines of evidence indicates that
Na+/H+ exchange inhibition is also effective
to minimize myocardial remodelling (30).
Atrial natriuretic peptide (ANP) and
phosphodiesterase 5 (PDE5) inhibitors
Animal studies have demonstrated that inclusion of
ANP during reperfusion reduces infarct size through the activation
of cGMP/PKG signaling pathway (31),
PKG, when activated by cGMP, phosphorylates several intracellular
target proteins that are involved in the regulation of vascular
tone, vasorelaxation in vascular smooth muscle and also endothelial
permeability, and cell differentiation and proliferation. Targeting
this pro-survival signaling pathway of cGMP/PKG for the prevention
of myocardial reperfusion injury also has evidence from studies
using inhibitors of (PDE enzymes, in particular PDE5, which blocks
the hydrolysis of cGMP. Thus PDE5 inhibitors such as sildenafil,
vardenafil, and tadalafil have been shown to be protective against
myocardial ischemia/reperfusion injury, by inducing the expression
of NOS, and activation of PKG-dependent hydrogen sulfide
generation. There have been several clinical studies indicating the
beneficial effects of PDE5 inhibitors, which appear to act
similarly to cardiac pre-conditioning (32). In studies on pigs, reduction in the
infarct size and improvement in ventricular function has been shown
by intravenous ANP administration at the time of reperfusion
following myocardial ischemia (33).
Glucose-insulin-potassium (GIK)
Insulin administration also acts through the
cGMP/PKG signaling pathway, as well as by increasing glucose use
(34). Experimental animal studies
have shown that promoting anabolic utilization of glucose by
myocardium, using insulin during acute myocardial ischemia is
beneficial for the heart (35). A
large number of clinical trials have investigated the effect of
this therapeutic approach using GIK. Despite mixed results, it
appears that GIK therapy may be more effective to reduce infarct
size as well as serious electrical complications when administered
in the ambulance to patients with MI that will receive primary
angioplasty (36).
Glucagon-like peptide-1(GLP-1)
The insulinotropic incretin, GLP-1 and its analogue
exenatide have been shown to offer protection during
ischemia-reperfusion (37,38). This therapeutic approach has
successfully been translated into the clinical setting, employing
exenatide during reperfusion (39).
Adenosine receptor agonists
Adenosine and other adenosine receptor agonists have
been studied in numerous experimental models and some, but not all,
showed cardioprotective effects. A variety of mechanisms of action
of a cardioprotective effect for adenosine has been suggested,
including a potent vasodilatory action, among others. In addition
to its effects on the vasculature and leukocytes, adenosine
increases NO availability via activation of Akt/cGMP/PKG signaling
pathway. This autocoid has been evaluated intravenously in several
trials (40) without conclusive
results, although evidence was obtained for cardiac protection at
high dose of adenosine, in patients with previous infarctions
(41). However, a subsequent
double-blind study with 200 patients revealed that even though not
all patients benefit from adenosine to limit infarct size, this
goal could be achieved in patients receiving primary angioplasty
within the first 3 h after the onset of pain (42). These patients also showed an
improvement in LV ejection fraction during the first 6 months after
the infarction. Since intracoronary adenosine is a safe and
inexpensive treatment, its early use in reperfused patients could
be easily adopted if later studies confirm the benefits.
mPTP inhibitors
Cyclosporine-A is the first pharmacologic agent that
has been shown to limit infarct size by inhibiting the opening of
the mPTP. Although other indirect mPTP inhibitors, including sodium
nitrite, bendavia, and TRO40303 have been described, cyclosporine-A
remains the most promising intervention. In a first pilot study,
cyclosporine-A limited infarct size in 58 patients with MI
undergoing primary angioplasty (43). Even though another study with similar
number of patients found no benefit in clinical outcomes (44), the current concern is to know whether
this therapeutic approach can reduce death, hospitalization for
heart failure, and LV remodeling. Also the negative results from a
recent multi center study on the ability of cyclosporine to contain
the reperfusion injury and infarct size were questioned by the
possible differences in the vehicle used for cyclosporine
administration (45).
β-blockers
The beneficial effect of β-blockers on LV
remodeling, reinfarction, life-threatening arrhythmias, and most
importantly, mortality are well documented. However, their effect
on infarct size is somewhat more controversial, and preclinical
evidence on the use of β-blockers for reducing infarct size is
mixed. From the 1970s to 1980s, different β-blockers were tested
with no definite conclusion on their cardioprotective effect. These
trials were performed before reperfusion became established
practice. Preclinical data from the pig model of MI demonstrated
that intravenous injection of metoprolol significantly reduced
infarct size when administered before reperfusion (46). The mechanism responsible for this
infarct-limiting effect is proposed to be related to the effect of
metoprolol on circulating cells such as neutrophils and platelets,
rather than cardiomyocytes (47).
This pre-clinical evidence led to a clinical study aimed to
determine the effect of intravenous metropolol, administered
immediately before primary angioplasty, on infarct size determined
with magnetic resonance imaging and the results showed protection
via an increase in myocardial salvage without complications
(48). Although there is excitement
about the cardioprotective potential of new β-blockers such as
nebivolol (49), sufficient
pre-clinical investigation, including reproducible results in
multiple animal models, should be completed before large-scale
clinical testing. Majority of the earlier clinical trials that
looked at the efficacy of β-blockers in MI were carried out in the
pre-thrombolytic era, and the consensus from these studies was that
β-blockers might reduce infarct size when given very early after
the onset of symptoms.
Glycoprotein IIb/IIIa inhibitors
Glycoprotein IIb/IIIa inhibitors were developed for
the reduction of thrombotic events due to their potent effect on
platelets and platelet-leukocyte aggregates implicated in
ischemia-reperfusion injury. Most of the clinical trials employed
abciximab, the potent glycoprotein IIb/IIIa inhibitor, and it was
suggested that abciximab could reduce myocardial infarct size and
lead to improved clinical outcomes when administered early to
patients with myocardial infarct (50) or when given via an intracoronary
route compared with intravenous route (51). This benefit may be related to
reduction in platelet aggregation, thus keeping the infarct-related
coronary artery patent. However, it has been noted that certain
antiplatelet agents, such as clopidogrel and cangrelor, reduce
myocardial infarct size and prevent myocardial reperfusion injury
when administrated at the time of myocardial reperfusion in
ischemia-reperfusion models that do not primarily involve in
formation of thrombus as the cause of the coronary occlusion but
induce ischemia mechanically (52).
Therefore, antiplatelet therapy given to MI patients undergoing
percutaneous coronary intervention may be cardioprotective through
some pleitropic mechanisms. Currently, the standard of care for MI
patients includes potent oral antiplatelet agents primarily and
glycoprotein IIb/IIIa inhibitors are prescribed for a selected MI
population. Comparison of two different glycoprotein IIb/IIIa
inhibitors, abciximab and eptifibatide, has revealed that abciximab
was superior to eptifibatide in improving angiographic and
electrocardiographic assessment of coronary perfusion, as well as
in reducing infarct size (53).
Nitrates and nitroglycerin
Although early clinical trial in the
pre-thrombolytic era of the 1970s and 1980s suggested that nitrates
could reduce mortality in the setting of MI, large clinical trials
failed to confirm this benefit (54). Nevertheless, there is renewed
interest in nitrates as a cardioprotectant in recent years because
new clinical and animal model studies have shown promising results.
Several recent clinical studies have shown the potential of
nitrates to limit myocardial infarct size. A retrospective analysis
of the Global Registry of Acute Coronary Syndromes data set aiming
to determine if antecedent nitrate therapy led to less myocardial
necrosis during the ischemic event, has revealed that 18% of
chronic nitrate users were diagnosed with MI compared with 41% of
nitrate-naive patients (55).
Similarly, 82% of nitrate users presented with non-MI compared with
59% of patients who were nitrate naive. Moreover, nitroglycerin
used as nitrate, was associated with lower tropin levels,
regardless of acute coronary syndrome type. Nitroglycerin has also
been shown to have pre-conditioning mimetic action in several
clinical circumstances. In patients with stable angina,
pre-treatment with nitroglycerin 24 h before an exercise tolerance
test improved functional capacity and electrocardiographic
manifestations of ischemia. Patients who received nitroglycerin had
improvement in ST-segment shifts, regional wall motion
abnormalities, and chest pain score after balloon inflation
compared with patients who received saline (56).
Conclusion
Myocardial ischemia-reperfusion injury is a complex
event with many interlinked processes. Approaches to combat this
phenomenon are not adequately developed. Indeed, an agent that aids
in the reduction of myocardial ischemia-reperfusion injury might
only address one aspect of the pathological condition. In addition,
therapeutic attempts to minimize the damage by targeting individual
players of the process have shown promise in the laboratory, but
have been less encouraging in clinical application. It is important
that a potential course of treatment involves a variety of
intervening mechanisms that are appropriately timed to ensure a
complete protection from ischemia-reperfusion injury.
References
|
1
|
Callender T, Woodward M, Roth G, Farzadfar
F, Lemarie JC, Gicquel S, Atherton J, Rahimzadeh S, Ghaziani M,
Shaikh M, et al: Heart failure care in low- and middle-income
countries: A systematic review and meta-analysis. PLoS Med.
11:e10016992014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Ibáñez B, Heusch G, Ovize M and Van de
Werf F: Evolving therapies for myocardial ischemia/reperfusion
injury. J Am Coll Cardiol. 65:1454–1471. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Yellon DM and Hausenloy DJ: Myocardial
reperfusion injury. N Engl J Med. 357:1121–1135. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Eapen ZJ, Tang WH, Felker GM, Hernandez
AF, Mahaffey KW, Lincoff AM and Roe MT: Defining heart failure end
points in ST-segment elevation myocardial infarction trials:
Integrating past experiences to chart a path forward. Circ
Cardiovasc Qual Outcomes. 5:594–600. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Reeve JL, Duffy AM, O'Brien T and Samali
A: Don't lose heart - therapeutic value of apoptosis prevention in
the treatment of cardiovascular disease. J Cell Mol Med. 9:609–622.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Piper HM, García-Dorado D and Ovize M: A
fresh look at reperfusion injury. Cardiovasc Res. 38:291–300. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Cannon RO III: Mechanisms, management and
future directions for reperfusion injury after acute myocardial
infarction. Nat Clin Pract Cardiovasc Med. 2:88–94. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Reimer KA, Jennings RB and Tatum AH:
Pathobiology of acute myocardial ischemia: Metabolic, functional
and ultrastructural studies. Am J Cardiol. 52:72A–81A. 1983.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Ladilov YV, Siegmund B and Piper HM:
Protection of reoxygenated cardiomyocytes against hypercontracture
by inhibition of Na+/H+ exchange. Am J
Physiol. 268:H1531–H1539. 1995.PubMed/NCBI
|
|
10
|
Inserte J, Hernando V and Garcia-Dorado D:
Contribution of calpains to myocardial ischaemia/reperfusion
injury. Cardiovasc Res. 96:23–31. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Ruiz-Meana M, García-Dorado D, González
MA, Barrabés JA and Soler-Soler J: Effect of osmotic stress on
sarcolemmal integrity of isolated cardiomyocytes following
transient metabolic inhibition. Cardiovasc Res. 30:64–69. 1995.
View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Barrabés JA, Garcia-Dorado D, Ruiz-Meana
M, Piper HM, Solares J, González MA, Oliveras J, Herrejón MP and
Soler J Soler: Myocardial segment shrinkage during coronary
reperfusion in situ. Relation to hypercontracture and myocardial
necrosis. Pflugers Arch. 431:519–526. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Halestrap AP, Clarke SJ and Javadov SA:
Mitochondrial permeability transition pore opening during
myocardial reperfusion - a target for cardioprotection. Cardiovasc
Res. 61:372–385. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Ruiz-Meana M, Inserte J, Fernandez-Sanz C,
Hernando V, Miro-Casas E, Barba I and Garcia-Dorado D: The role of
mitochondrial permeability transition in reperfusion-induced
cardiomyocyte death depends on the duration of ischemia. Basic Res
Cardiol. 106:1259–1268. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Buja LM: Myocardial ischemia and
reperfusion injury. Cardiovasc Pathol. 14:170–175. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Heusch G: Cardioprotection: Chances and
challenges of its translation to the clinic. Lancet. 381:166–175.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zhao ZQ, Corvera JS, Halkos ME, Kerendi F,
Wang NP, Guyton RA and Vinten-Johansen J: Inhibition of myocardial
injury by ischemic postconditioning during reperfusion: Comparison
with ischemic preconditioning. Am J Physiol Heart Circ Physiol.
285:H579–H588. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Rodríguez-Sinovas A, Cabestrero A, del
Blanco García B, Inserte J, García A and García-Dorado D:
Intracoronary acid infusion as an alternative to ischemic
postconditioning in pigs. Basic Res Cardiol. 104:761–771. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Inserte J, Ruiz-Meana M, Rodríguez-Sinovas
A, Barba I and Garcia-Dorado D: Contribution of delayed
intracellular pH recovery to ischemic postconditioning protection.
Antioxid Redox Signal. 14:923–939. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Inserte J, Barba I, Poncelas-Nozal M,
Hernando V, Agulló L, Ruiz-Meana M and Garcia-Dorado D: cGMP/PKG
pathway mediates myocardial postconditioning protection in rat
hearts by delaying normalization of intracellular acidosis during
reperfusion. J Mol Cell Cardiol. 50:903–909. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Hausenloy DJ and Yellon DM: Remote
ischaemic preconditioning: Underlying mechanisms and clinical
application. Cardiovasc Res. 79:377–386. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Thielmann M, Wendt D, Tsagakis K, Price V,
Dohle DS, Pasa S and Kottenberg E: Remote ischemic preconditioning:
The surgeon's perspective. J Cardiovasc Med (Hagerstown).
14:187–192. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Gritsopoulos G, Iliodromitis EK, Zoga A,
Farmakis D, Demerouti E, Papalois A, Paraskevaidis IA and
Kremastinos DT: Remote postconditioning is more potent than classic
postconditioning in reducing the infarct size in anesthetized
rabbits. Cardiovasc Drugs Ther. 23:193–198. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Hausenloy DJ, Iliodromitis EK, Andreadou
I, Papalois A, Gritsopoulos G, Anastasiou-Nana M, Kremastinos DT
and Yellon DM: Investigating the signal transduction pathways
underlying remote ischemic conditioning in the porcine heart.
Cardiovasc Drugs Ther. 26:87–93. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Tissier R, Chenoune M, Ghaleh B, Cohen MV,
Downey JM and Berdeaux A: The small chill: Mild hypothermia for
cardioprotection? Cardiovasc Res. 88:406–414. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Hale SL and Kloner RA: Mild hypothermia as
a cardioprotective approach for acute myocardial infarction:
Laboratory to clinical application. J Cardiovasc Pharmacol Ther.
16:131–139. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Götberg M, Olivecrona GK, Koul S, Carlsson
M, Engblom H, Ugander M, van der Pals J, Algotsson L, Arheden H and
Erlinge D: A pilot study of rapid cooling by cold saline and
endovascular cooling before reperfusion in patients with
ST-elevation myocardial infarction. Circ Cardiovasc Interv.
3:400–407. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Rupprecht HJ, vom Dahl J, Terres W,
Seyfarth KM, Richardt G, Schultheibeta HP, Buerke M, Sheehan FH and
Drexler H: Cardioprotective effects of the Na(+)/H(+) exchange
inhibitor cariporide in patients with acute anterior myocardial
infarction undergoing direct PTCA. Circulation. 101:2902–2908.
2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Yamada K, Matsui K, Satoh K, Kitano M,
Yamamoto S and Ohashi N: Reduction of myocardial infarct size by
SM-20550, a novel Na(+)/H(+) exchange inhibitor, in rabbits. Eur J
Pharmacol. 404:201–212. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Karmazyn M: NHE-1: Still a viable
therapeutic target. J Mol Cell Cardiol. 61:77–82. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Yang XM, Philipp S, Downey JM and Cohen
MV: Atrial natriuretic peptide administered just prior to
reperfusion limits infarction in rabbit hearts. Basic Res Cardiol.
101:311–318. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Das A, Durrant D, Salloum FN, Xi L and
Kukreja RC: PDE5 inhibitors as therapeutics for heart disease,
diabetes and cancer. Pharmacol Ther. 147:12–21. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Padilla F, Garcia-Dorado D, Agulló L,
Barrabés JA, Inserte J, Escalona N, Meyer M, Mirabet M, Pina P and
Soler-Soler J: Intravenous administration of the natriuretic
peptide urodilatin at low doses during coronary reperfusion limits
infarct size in anesthetized pigs. Cardiovasc Res. 51:592–600.
2001. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Gao F, Gao E, Yue TL, Ohlstein EH, Lopez
BL, Christopher TA and Ma XL: Nitric oxide mediates the
antiapoptotic effect of insulin in myocardial ischemia-reperfusion:
The roles of PI3-kinase, Akt, and endothelial nitric oxide synthase
phosphorylation. Circulation. 105:1497–1502. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Suranadi IW, Demaison L, Chaté V, Peltier
S, Richardson M and Leverve X: An increase in the redox state
during reperfusion contributes to the cardioprotective effect of
GIK solution. J Appl Physiol (1985). 113:775–784. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Selker HP, Beshansky JR, Sheehan PR,
Massaro JM, Griffith JL, D'Agostino RB, Ruthazer R, Atkins JM,
Sayah AJ, Levy MK, et al: Out-of-hospital administration of
intravenous glucose-insulin-potassium in patients with suspected
acute coronary syndromes: The IMMEDIATE randomized controlled
trial. JAMA. 307:1925–1933. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Ban K, Noyan-Ashraf MH, Hoefer J, Bolz SS,
Drucker DJ and Husain M: Cardioprotective and vasodilatory actions
of glucagon-like peptide 1 receptor are mediated through both
glucagon-like peptide 1 receptor-dependent and -independent
pathways. Circulation. 117:2340–2350. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Timmers L, Henriques JP, de Kleijn DP,
Devries JH, Kemperman H, Steendijk P, Verlaan CW, Kerver M, Piek
JJ, Doevendans PA, et al: Exenatide reduces infarct size and
improves cardiac function in a porcine model of ischemia and
reperfusion injury. J Am Coll Cardiol. 53:501–510. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Lønborg J, Vejlstrup N, Kelbæk H, Bøtker
HE, Kim WY, Mathiasen AB, Jørgensen E, Helqvist S, Saunamäki K,
Clemmensen P, et al: Exenatide reduces reperfusion injury in
patients with ST-segment elevation myocardial infarction. Eur Heart
J. 33:1491–1499. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Mahaffey KW, Puma JA, Barbagelata NA,
DiCarli MF, Leesar MA, Browne KF, Eisenberg PR, Bolli R, Casas AC,
Molina-Viamonte V, et al: Adenosine as an adjunct to thrombolytic
therapy for acute myocardial infarction: results of a multicenter,
randomized, placebo-controlled trial: the Acute Myocardial
Infarction STudy of ADenosine (AMISTAD) trial. J Am Coll Cardiol.
34:1711–1720. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Ross AM, Gibbons RJ, Stone GW, Kloner RA
and Alexander RW: AMISTAD-II Investigators: A randomized,
double-blinded, placebo-controlled multicenter trial of adenosine
as an adjunct to reperfusion in the treatment of acute myocardial
infarction (AMISTAD-II). J Am Coll Cardiol. 45:1775–1780. 2005.
View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Garcia-Dorado D, García-del-Blanco B,
Otaegui I, Rodríguez-Palomares J, Pineda V, Gimeno F, Ruiz-Salmerón
R, Elizaga J, Evangelista A, Fernandez-Avilés F, et al:
Intracoronary injection of adenosine before reperfusion in patients
with ST-segment elevation myocardial infarction: A randomized
controlled clinical trial. Int J Cardiol. 177:935–941. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Piot C, Croisille P, Staat P, Thibault H,
Rioufol G, Mewton N, Elbelghiti R, Cung TT, Bonnefoy E, Angoulvant
D, et al: Effect of cyclosporine on reperfusion injury in acute
myocardial infarction. N Engl J Med. 359:473–481. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
44
|
Ghaffari S, Kazemi B, Toluey M and
Sepehrvand N: The effect of prethrombolytic cyclosporine-A
injection on clinical outcome of acute anterior ST-elevation
myocardial infarction. Cardiovasc Ther. 31:e34–e39. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
45
|
Hausenloy DJ and Yellon DM: Targeting
myocardial reperfusion injury - the search continues. N Engl J Med.
373:1073–1075. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
46
|
Ibanez B, Cimmino G, Prat-González S,
Vilahur G, Hutter R, García MJ, Fuster V, Sanz J, Badimon L and
Badimon JJ: The cardioprotection granted by metoprolol is
restricted to its administration prior to coronary reperfusion. Int
J Cardiol. 147:428–432. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
García-Prieto J, García-Ruiz JM, Sanz-Rosa
D, Pun A, García-Alvarez A, Davidson SM, Fernández-Friera L,
Nuno-Ayala M, Fernández-Jiménez R, Bernal JA, et al: β3 adrenergic
receptor selective stimulation during ischemia/reperfusion improves
cardiac function in translational models through inhibition of mPTP
opening in cardiomyocytes. Basic Res Cardiol. 109:4222014.
View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Ibanez B, Macaya C, Sánchez-Brunete V,
Pizarro G, Fernández-Friera L, Mateos A, Fernández-Ortiz A,
García-Ruiz JM, García-Álvarez A, Iñiguez A, et al: Effect of early
metoprolol on infarct size in ST-segment-elevation myocardial
infarction patients undergoing primary percutaneous coronary
intervention: The Effect of Metoprolol in Cardioprotection During
an Acute Myocardial Infarction (METOCARD-CNIC) trial. Circulation.
128:1495–1503. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Sorrentino SA, Doerries C, Manes C, Speer
T, Dessy C, Lobysheva I, Mohmand W, Akbar R, Bahlmann F, Besler C,
et al: Nebivolol exerts beneficial effects on endothelial function,
early endothelial progenitor cells, myocardial neovascularization,
and left ventricular dysfunction early after myocardial infarction
beyond conventional β1-blockade. J Am Coll Cardiol. 57:601–611.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Rakowski T, Zalewski J, Legutko J, Bartus
S, Rzeszutko L, Dziewierz A, Sorysz D, Bryniarski L, Zmudka K,
Kaluza GL, et al: Early abciximab administration before primary
percutaneous coronary intervention improves infarct-related artery
patency and left ventricular function in high-risk patients with
anterior wall myocardial infarction: A randomized study. Am Heart
J. 153:360–365. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Thiele H, Schindler K, Friedenberger J,
Eitel I, Fürnau G, Grebe E, Erbs S, Linke A, Möbius-Winkler S,
Kivelitz D, et al: Intracoronary compared with intravenous bolus
abciximab application in patients with ST-elevation myocardial
infarction undergoing primary percutaneous coronary intervention:
The randomized Leipzig immediate percutaneous coronary intervention
abciximab IV versus IC in ST-elevation myocardial infarction trial.
Circulation. 118:49–57. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
52
|
Yang XM, Liu Y, Cui L, Yang X, Liu Y,
Tandon N, Kambayashi J, Downey JM and Cohen MV: Platelet P2Y(1)(2)
blockers confer direct postconditioning-like protection in
reperfused rabbit hearts. J Cardiovasc Pharmacol Ther. 18:251–262.
2013. View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Bajaj RR, Mohammad A, Hong T, Irfan A,
Sharieff W, Bagnall A, Christie JA, Kutryk MJ, Chisholm RJ and
Cheema AN: Comparison of abciximab and eptifibatide on angiographic
and clinical outcomes in rescue percutaneous coronary intervention
for failed fibrinolytic therapy. J Invasive Cardiol. 22:347–352.
2010.PubMed/NCBI
|
|
54
|
No authors listed, . ISIS-4: a randomised
factorial trial assessing early oral captopril, oral mononitrate,
and intravenous magnesium sulphate in 58,050 patients with
suspected acute myocardial infarction. ISIS-4 (Fourth International
Study of Infarct Survival) Collaborative Group. Lancet.
345:669–685. 1995. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Ambrosio G, Del Pinto M, Tritto I, Agnelli
G, Bentivoglio M, Zuchi C, Anderson FA, Gore JM, López-Sendón J,
Wyman A, et al: GRACE Investigators: Chronic nitrate therapy is
associated with different presentation and evolution of acute
coronary syndromes: Insights from 52,693 patients in the Global
Registry of Acute Coronary Events. Eur Heart J. 31:430–438. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Leesar MA, Stoddard MF, Dawn B, Jasti VG,
Masden R and Bolli R: Delayed preconditioning-mimetic action of
nitroglycerin in patients undergoing coronary angioplasty.
Circulation. 103:2935–2941. 2001. View Article : Google Scholar : PubMed/NCBI
|