Introduction
Pneumonia due to Candida infection is rare
and frequently associated with a fatal outcome, with a mortality
rate up to 70% (1–3). It occurs predominantly in
immunocompromised patients, or patients receiving broad-spectrum
antibiotic therapy (4). Haron et
al (5) revealed an incidence of
0.4% among 7,725 patients (1), which
is similar to Masur's observations several years before (0.23%).
Candida pneumonia was first described by Nils Rosén von
Rosenstein in 1984 (6), and later
reported by Castellani in 1927 (7).
However, only a limited number of cases have since been reported in
the English literature (8). In
search of the PubMed database (http://www.ncbi.nlm.nih.gov/pubmed accessed 14 May,
2009), 91 cases of Candida pneumonia confirmed by
histopathology (1–3,8–10) were identified. In particular,
Candida krusei (C. krusei) infection is less
frequently encountered in clinical mycology compared with other
species of Candida pathogens, with the first case of C.
krusei infection reported in 2002 (3,11).
The diagnosis of Candida pneumonia is one of
the most challenging of all Candida infections to diagnose
(12), not only because of its rare
occurrence, but also its non-specific clinical manifestation, with
fever and tachypnea being the most common symptoms and cough,
expectoration of purulent secretions, hemoptysis, and chest pain
only present occasionally (13).
Making a convincing diagnosis of Candida pneumonia is only truly
possible on the basis of a histopathological examination of samples
(14,15). MERS, a viral respiratory infection
caused by the novel MERS-CoV pathogen, also had common symptoms
with Candida pneumonia, including fever, cough and shortness
of breath (16).
The present study reported a case of C.
krusei pneumonia in a 64-year-old male patient, who was
initially suspected with Middle East respiratory syndrome
(MERS).
Case report
A 64-year-old Saudi Arabian male patient was
admitted to Tiantai County People's Hospital (Taizhou, China) in
December 2014 with complaints of cough and dyspnea that had
persisted for 6 days. Written informed consent was obtained from
the patient. The patient initially presented abrupt onset of
paroxysmal cough without evident inducements, accompanied by chest
tightness, tachypnea and slight fever; however, no expectoration,
chest pain, hemoptysis or oliguresis were reported, and the patient
did not receive regular therapy. Within the 6 days after the onset
of symptoms, cough and chest tightness became progressively worse,
and the edema of both lower limbs appeared. The patient's medical
history indicated that the patient suffered from diabetes within
the past 20 years, which was treated with insulin, coronary heart
disease performed 10 years before presentation to our hospital and
chronic diabetic kidney insufficiency over the last 4 years. In
addition, the patient reported that chest tightness and tachypnea
had occurred soon after walking for ~100 steps within the past 10
years. Family history was unremarkable.
On admission, the patient was found to have fever
(oral temperature of 38.5°C; normal 36.3–37.3°C) and slight
tachypnea (25 respirations/min; normal 12–20 respirations/min),
with a heart rate (HR) of 60 beats/min (normal 60–100 beats/min), a
pulse of 60/min (normal 60–100/min) and blood pressure (BP) of
180/90 mmHg (normal 90/60 mmHg-120/80 mmHg). The patient had an
oxygen saturation of 90% (normal 98–100%) on air and presented
cyanosis in the lips. Cardiovascular examinations Laboratory
examinations revealed an irregular heart rhythm, however, no
evident pathological murmur was observed at the auscultatory valve
areas and no distension of the jugular vein was observed at a
semireclining position. Crude breath sounds of bilateral lung were
heard on chest auscultation, without marked dry and moist rales.
Other physical examinations included the abdominal bulge in the
absence of tenderness and rebound, unsatisfactory palpation of
liver and spleen, borborygmus at a rate of 4/min with negative
shifting dullness, as well as mild edema of the lower limbs.
Neurogenic examination showed no abnormalities. The admitting
diagnosis was severe pneumonia due to suspected MERS, respiratory
and heart failure, acid base imbalance and electrolyte
disturbances, diabetes, chronic kidney insufficiency and
hypertension.
Laboratory examinations by a Sysmex XE-2100
hematology analyzer (Sysmex Corporation, Kobe, Japan) revealed the
following levels: Hemoglobin, 96 g/l (depressed; normal, 130–175
g/l); white blood cells, 10.2×109/l [(77.6% neutrophils,
13.7% lymphocytes and 8.7% monocytes); elevated; normal, 3.5–9.5 ×
109/l (40.0–75.0% neutrophils)]; and C-reactive protein,
>200 mg/dl (elevated; normal, 0–80 mg/dl). In addition, blood
gas examination by an SC-501 automated blood gas analyzer
(Radiometer, Copenhagen, Denmark) demonstrated the following
results: pH 7.42 (normal 7.35–7.45); partial pressure of oxygen,
65.8 mmHg (depressed; normal 80–100 mmHg); partial pressure of
carbon dioxide, 30.8 mmHg (depressed; normal 35–45 mmHg); BE, 4
mmol/l (elevated; normal −3-+3 mmol/l); bicarbonate level, 19.8
mmol/l (depressed normal 22–27 mmol/l); and lactic acid level, 2.10
mmol/l (elevated; normal 0.44–1.78 mmol/l). Furthermore,
biochemical analyses by a fully automatic biochemical analyzer
(Architect c16000; Abbott Diagnostics, Lake Forest, IL, USA) showed
the following results: Aspartate aminotransferase, 85 U/l
(elevated; normal 9–50 U/l); lactate dehydrogenase, 369 U/l
(elevated; normal 0–200 U/l); blood potassium, 5.01 mmol/l (normal,
3.50–5.50 mmol/l); blood sodium, 128 mmol/l (depressed; normal
137–147 mmol/l); blood glucose, 16.89 mmol/l (elevated; normal
3.60–6.10 mmol/l); creatinine, 224 µmol/l (elevated; normal 15–110
µmol/l); blood urea nitrogen, 20.62 mmol/l (elevated normal
1.10–8.30 mmol/l). Besides, troponin was assessed as weakly
positive (normal negative) by a troponin analyzer (Zhe Jiang Ikon
Biotechnology Co., Ltd, Zhejiang, China), and the brain natriuretic
peptide was detected 4,567 pg/ml (elevated; normal 0.00–125 pg/ml)
by a Cobas 6000 biochemistry analyzer (Roche, Berlin, Germany).
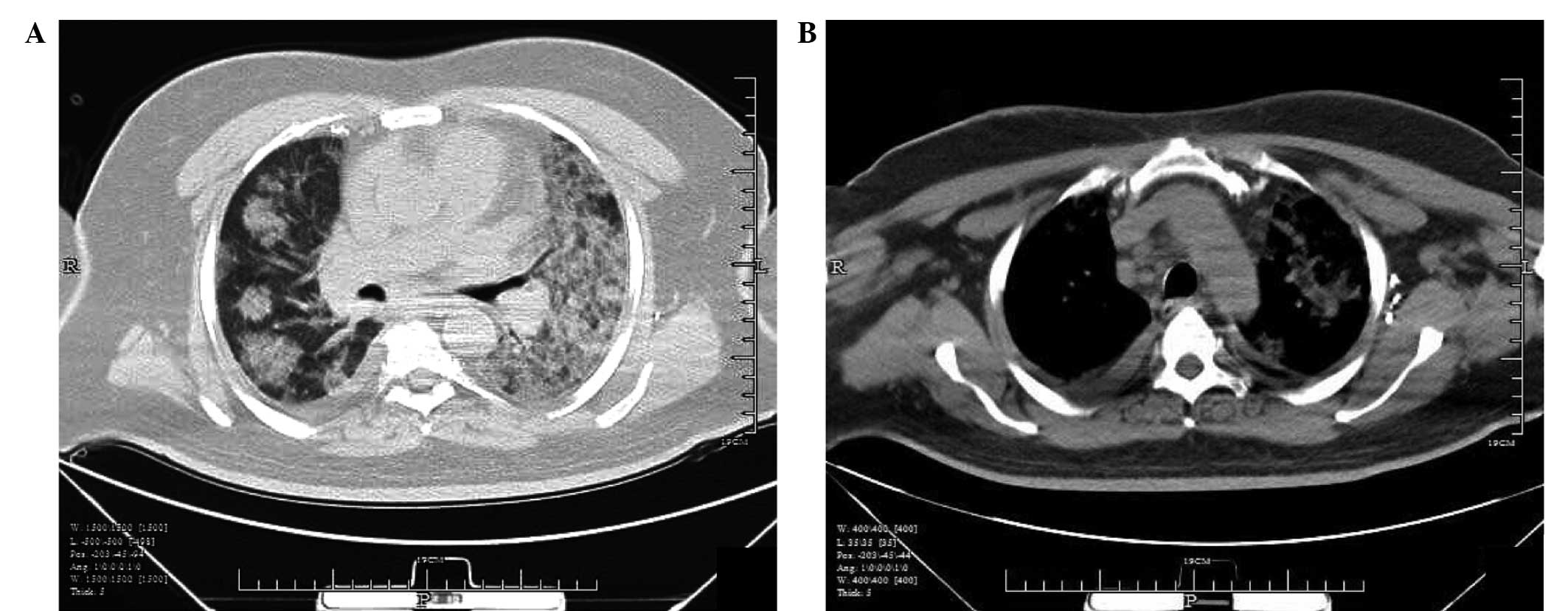
Computerized tomography (CT) of the chest at
lung-window setting demonstrated unclear lung fields associated
with diffuse pathological changes in the two lungs and signs of
severe pulmonary infection (Fig.
1A). In addition, pleural effusion and multiple
lymphadenectasis in retrocaval and para-aortic arch area were
observed at mediastinal-window setting (Fig. 1B). Blood samples were obtained for
the detection of procalcitonin (PCT), and syphilis or human
immunodeficiency virus (HIV) infection. Blood, sputum and pharynx
swab samples were also collected and sent to the Provincial Center
for Disease Control (Hangzhou, Zhejiang, China) in order to detect
viruses or bacteria. Antibodies to syphilis and HIV in the blood
were found to be negative at day 2 after admission. In addition,
the serum PCT concentration of the patient was 4.73 µg/l at day 2
after admission and 7.23 µg/l (normal <0.06 µg/l) at day 3 after
admission. All repeat blood culture sets did not yield any growth.
Diagnosis of numerous viruses by nucleic acid detection was also
negative at 2 days after admission, including absence of infection
with MERS-coronavirus (MERS-CoV), flu viruses of type A and B
(including the H1N1 and H7N9 subtypes of influenza A),
Mycoplasma pneumoniae, Chlamydia pneumoniae,
respiratory adenovirus, respiratory syncytial viruses and various
parainfluenza viruses (types I, II and III). In addition,
galactomannan (GM) detection in the blood was negative. A sputum
smear showed a preliminary result of fungal infection, and the
culture was repeated three times, indicating a positive result for
C. krusei infection 4 days after admission. Therefore, the
diagnosis of C. krusei pneumonia was established, but
specific treatment for C. krusei was not administered due to
the patient succumbing to the disease 2 days after admission.
Initially, the patient was isolated and received
95–98% oxygen at atmospheric pressure at a rate of 6 l/min through
a nasal catheter for 24 h after admission to the hospital. Due to
the history of diabetes, a poor therapeutic effect for community
infection, an auxiliary and radiological examination, the patient
was administered sulbactam sodium/cefoperazone sodium (1:1) by
injection (3.0 g/time, which is the total dose used for injection;
Pfizer Pharmaceuticals Ltd., Liaoning, China) every 12 h for
antibacterial infection treatment before the definite diagnosis.
Oral administration of oseltamivir capsules (75 mg/time; Roche,
Bale, Switzerland) was performed twice a day for antiviral
infection treatment. Intravenous administration of medaron (Pfizer
Manufacturing Belgium NV, Puurs, Belgium) at a dose of 80 mg/time
was also started empirically for anti-inflammatory treatment, as
well as 750 ml fluid infusion. However, no significant improvement
was noted, and the condition of the patient deteriorated, with
cardiac and respiratory arrest occurring one day after admission.
Cardiopulmonary resuscitation was immediately performed, and the
patient recovered weak respiration with an assisted respirator. The
BP of the patient at this time was 70/50 mmHg, which was raised and
stabilized at 110/80 mmHg after adjusting the speed of fluid
infusion, monitoring central venous pressure, and minipump infusion
(4–20 ml/h, adjusted according to the BP) of vasoactive agents,
including noradrenaline (10 mg) and normal saline (50 ml).
Furthermore, a low HR of 30–40 beats/min was recorded and thus
cardiotonic therapy was administered, which consisted of adrenalin
injection (10 mg) and normal saline (50 ml) at a minipump
maintenance dose of 4–20 ml/h (adjusted according to the BP and
HR). Furthermore, the renal function of the patient was aggravated,
with the appearance of oliguria and anuresis. In spite of
continuing renal replacement therapy, the patient succumbed to the
infection 2 days after admission.
Discussion
C. krusei is an opportunistic pathogen of
normal human microbial flora localized in the skin, mucous
membranes and digestive tract, and it may cause life-threatening
invasive infections (17). Despite
not being the most frequently isolated species of Candida in
infected patients, C. krusei is an invasive infection with
growing incidence (18).
Candida pneumonia, a rare infection associated with high
mortality, should always be considered in patients presenting
cough, expectoration of purulent secretions, occasional hemoptysis
and invariably hypoxemia (8).
In the present study, the patient developed
paroxysmal cough, accompanied by chest tightness, tachypnea and
slight fever. However, pulmonary infection due to C. krusei
in the current patient was difficult to diagnose, and initially
MERS was suspected. MERS is caused by the novel MERS-CoV pathogen,
a viral respiratory infection first reported in the Saudi Arabian
peninsula in 2012 (16). This
infection is characterized by acute respiratory infection, and
develops into respiratory failure, acute respiratory distress
syndrome and multiple organ failure, particularly renal failure
(19). The common symptoms of MERS
also include fever, cough and shortness of breath. In addition, the
majority of MERS patients present underlying comorbid medical
disorders, including diabetes, hypertension, chronic cardiac
disease and chronic renal disease (20). The patient of the current study
presented similar symptoms to the aforementioned MERS symptoms;
however, MERS was excluded by negative detection of the virus
through the nucleic acid detection method.
Histopathological examination of tissue specimens
obtained by invasive procedures is considered as the gold standard
for diagnosis of Candida pneumonia (21). Considering the difficulty in
performing biopsy, repeat blood and sputum cultures are typically
conducted (4), and the patient and
his family disallowed for invasive operation because of their
belief. Isolation of C. krusei from the sputum is almost
always considered to represent colonization of the respiratory
tract. However, this diagnostic method presents great hysteresis.
Currently, PCT and GM tests are used as auxiliary examination
methods for the diagnosis of fungal infection (22,23).
Serum PCT levels are 0.1 µg/l in healthy individuals, and increased
secretion is observed under bacterial infection (24,25). In
the present case, the repeatedly high PCT concentrations supported
a diagnosis of C. krusei infection, although a
false-negative result was obtained in the GM test, which was not
considered to be inaccurate since it was not conducted
successionally and repeatedly.
Candida invasive infection usually affects
immunocompromised patients or those receiving broad-spectrum
antibiotic therapy. As reported in previous studies, solid organ
transplant (3,26), hematological malignancies (27), esophageal perforation (28) and diabetes (29) appear to facilitate C. krusei
pneumonia and empyema (11).
Similarly, the patient of the current study presented a long-term
medical history of diabetes, coronary heart disease and chronic
diabetic kidney insufficiency, but did not receive administration
of hormone therapy and antibiotics. The pathogenetic condition
progressed severely and fast, which is inconsistent with common
fungal pneumonia, and thus resulted in misdiagnosis.
In conclusion, the present case provides several
learning points on Candida pneumonia. The diagnosis of
Candida pneumonia should be strongly considered in the
presence of growth of Candida pathogens from a sputum
culture and a suggestive CT image. In addition, tumescent
diaphragmatic lymph nodes may be an important symptom of
Candida pneumonia. Finally, treatment should be initiated
immediately in order to improve tissue oxygenation, restore
cardiovascular function and improve other organ functions. This
study, to a certain extent, would provide guidance or some
experiences to the physician in diagnosing Candida pneumonia in the
clinic.
Acknowledgements
The authors would like to thank the Zhejiang
Provincial Center for Disease Control and Prevention Clinical
Laboratory, and the Zhejiang First Hospital Infection Department
Laboratory that conducted comprehensive etiology detection for the
current patient.
References
|
1
|
Haron E, Vartivarian S, Anaissie E,
Dekmezian R and Bodey GP: Primary Candida pneumonia: Experience at
a large cancer center and review of the literature. Medicine
(Baltimore). 72:137–142. 1993. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Von Eiff M, Roos N, Fegeler W, Von Eiff C,
Schulten R, Hesse M, Zühlsdorf M and Van de Loo J: Hospital -
acquired candida and aspergillus pneumonia - diagnostic approaches
and clinical findings. J Hosp Infect. 32:17–28. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Petrocheilou-Paschou V, Georgilis K,
Kontoyannis D, Nanas J, Prifti H, Costopoulos H and Stamatelopoulos
S: Pneumonia due to Candida krusei. Clin Microbiol Infect.
8:806–809. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Carvajal C, Rello J and Lipman J: Candida
pneumonia in patients with hematological neoplasiaPulmonary
Involvement in Patients with Hematological Malignancies. Azoulay E:
Springer; Berlin: pp. 349–356. 2011, View Article : Google Scholar
|
|
5
|
Masur H, Rosen PP and Armstrong D:
Pulmonary disease caused by Candida species. Am J Med. 63:914–925.
1977. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
von Rosenstein NR: The diseases of
children and their remedies. The Classics of Medicine Library,
Wenneberg and Nordstrom; Stockholm: 1984
|
|
7
|
Castellani A: Notes on certain
bronchomycoses which may simulate pulmonary tuberculosis. Am Rev
Tuberc. 16:1927–1928. 1927.
|
|
8
|
Mohsenifar Z, Chopra SK, Johnson BL and
Simmons DH: Candida pneumonia: Experience with 20 patients. West J
Med. 131:196–200. 1979.PubMed/NCBI
|
|
9
|
Schröter GP, Hoelscher M, Putnam CW,
Porter KA and Starzl TE: Fungus infections after liver
transplantation. Ann Surg. 186:115–122. 1977. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Buff SJ, McLelland R, Gallis HA, Matthay R
and Putman CE: Candida albicans pneumonia: radiographic appearance.
Am J Roentgenol. 138:645–648. 1982. View Article : Google Scholar
|
|
11
|
Imtiaz T, Thomson F, Innes A, du Toit FC
and Bal AM: Candida krusei bronchopneumonia with nodular
infiltrates in a patient with chronic renal failure on
haemodialysis - case report and review of literature. Mycoses.
54:e611–e614. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Meersseman W, Lagrou K, Spriet I, Maertens
J, Verbeken E, Peetermans W and Van Wijngaerden E: Significance of
the isolation of Candida species from airway samples in critically
ill patients: a prospective, autopsy study. Intens Care Med.
35:1526–1531. 2009. View Article : Google Scholar
|
|
13
|
Gogia P: Pulmonary fungal infections.
Current Medicine Research and Practice. 5:221–227. 2015. View Article : Google Scholar
|
|
14
|
Kontoyiannis D, Reddy B, Torres H, Luna M,
Lewis R, Tarrand J, Bodey G and Raad I: Pulmonary candidiasis in
patients with cancer: an autopsy study. Clin Infect Dis.
34:400–403. 2002. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Rodriguez L, Anaissie E and Rex J:
Pneumonia due to Candida speciesSarosi GA and Davies SF: Fungal
disease of the lung. 3rd. Lippincott Williams & Wilkins;
Philadelphia: pp. 115–122. 2000
|
|
16
|
Zaki AM, Van Boheemen S, Bestebroer TM,
Osterhaus AD and Fouchier RA: Isolation of a novel coronavirus from
a man with pneumonia in Saudi Arabia. N Engl J Med. 367:1814–1820.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Galván B and Mariscal F: Epidemiology of
candidemia in ICU. Rev Iberoam Micol. 23:12–15. 2006.(In Spanish).
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Fidan I, Yesilyurt E, Kalkanci A, Aslan
SO, Sahin N, Ogan MC and Dizbay M: Immunomodulatory effects of
voriconazole and caspofungin on human peripheral blood mononuclear
cells stimulated by Candida albicans and Candida krusei. Am J Med
Sci. 348:219–223. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
WHO MERS-CoV Research Group, . State of
knowledge and data gaps of Middle East respiratory syndrome
coronavirus (MERS-CoV) in humans. PLoS Curr. 5:2013.
|
|
20
|
Assiri A, Al-Tawfiq JA, Al-Rabeeah AA,
Al-Rabiah FA, Al-Hajjar S, Al-Barrak A, Flemban H, Al-Nassir WN,
Balkhy HH, Al-Hakeem RF, et al: Epidemiological, demographic, and
clinical characteristics of 47 cases of Middle East respiratory
syndrome coronavirus disease from Saudi Arabia: A descriptive
study. Lancet Infect Dis. 13:752–761. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Vélez L, Correa LT, Maya MA, Mejía P,
Ortega J, Bedoya V and Ortega H: Diagnostic accuracy of
bronchoalveolar lavage samples in immunosuppressed patients with
suspected pneumonia: Analysis of a protocol. Respir Med.
101:2160–2167. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Musher B, Fredricks D, Leisenring W,
Balajee SA, Smith C and Marr KA: Aspergillus galactomannan enzyme
immunoassay and quantitative PCR for diagnosis of invasive
aspergillosis with bronchoalveolar lavage fluid. Journal of
clinical microbiology. 42:5517–5522. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Charles PE, Castro C, Ruiz-Santana S, León
C, Saavedra P and Martín E: Serum procalcitonin levels in
critically ill patients colonized with Candida spp: new clues for
the early recognition of invasive candidiasis? Intensive care
medicine. 35:2146–2150. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Groselj-Grenc M, Ihan A, Pavcnik-Arnol M,
Kopitar AN, Gmeiner-Stopar T and Derganc M: Neutrophil and monocyte
CD64 indexes, lipopolysaccharide-binding protein, procalcitonin and
C-reactive protein in sepsis of critically ill neonates and
children. Intensive Care Med. 35:1950–1958. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Christ-Crain M, Jaccard-Stolz D, Bingisser
R, Gencay MM, Huber PR, Tamm M and Müller B: Effect of
procalcitonin-guided treatment on antibiotic use and outcome in
lower respiratory tract infections: Cluster-randomised,
single-blinded intervention trial. Lancet. 363:600–607. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Bonatti H, Stelzmueller I, Berger N,
Lechner M, Grif K, Geltner C, Margreiter R and Lass-Flörl C:
Infections caused by Candida krusei in five transplant and two
surgical patients. Surg Infect. 10:265–271. 2009. View Article : Google Scholar
|
|
27
|
Speletas M, Vyzantiadis T-A, Kalala F,
Plastiras D, Kokoviadou K, Antoniadis A and Korantzis I: Pneumonia
caused by Candida krusei and Candida glabrata in a patient with
chronic myeloid leukemia receiving imatinib mesylate treatment. Med
Mycol. 46:259–263. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cascio A, Barone M, Micali V, Iaria C,
Delfino D, David A, Monaco M and Monaco F: On a fatal case of
Candida krusei pleural empyema in a pregnant woman with spontaneous
esophagus perforation. Mycopathologia. 169:451–455. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kofteridis DP, Mantadakis E, Karatzanis
AD, Bourolias CA, Papazoglou G, Velegrakis GA and Samonis G:
Non-Candida albicans Candida mediastinitis of odontogenic origin in
a diabetic patient. Med Mycol. 46:345–348. 2008. View Article : Google Scholar : PubMed/NCBI
|