Introduction
As a common complication in patients with chronic
hepatitis B, thrombocytopenia (platelet count
<100×109/l) occurs in 76% of these patients (1). Effects of mild to moderate
thrombocytopenia on chronic hepatitis B treatment is generally
light without causing spontaneous bleeding, but severe
thrombocytopenia can significantly increase the risk of spontaneous
bleeding in clinical practice, such as cerebral hemorrhage or
gastrointestinal bleeding (2). The
incidence of thrombocytopenia is affected by a variety of factors,
including inhibition of the production of platelets by bone marrow
and decreased activity of thrombopoietin (TPO) (3). In addition, increased intracarotid
platelet damage, autoantibodies produced in spleen and blood
dilution can also cause thrombocytopenia (4,5).
Autoimmunity is a major immunological factor leading
to thrombocytopenia, and studies have reported that T-cell immunity
plays an important role in autoimmunity (6). As CD4+ and CD25+
T cells, regulatory T (Treg) cells can inhibit T cell proliferation
and effector function (7,8). Treg can inhibit antigen presenting
cells to present antigens to T cells by secreting IL-10, which in
turn inhibit T cell immune response (9). Treg can also secrete TGF-β to inhibit
the function of T cells and the production of interferon γ (IFN-γ),
thus maintaining a chronic persistent infection of hepatitis B
virus (10–12). IL-6 and TGF-β can induce the
production of Th17 cells, which can promote the development of
inflammatory responses by secreting IL-17, IL-21 and IL-22, so as
to promote the development of inflammatory responses (13). Percentage of Th17 cells and serum
IL-17 levels were significantly elevated in patients with
autoimmune diseases such as rheumatoid arthritis, asthma, and
systemic lupus erythematosus (14).
This study showed that Treg cells were closely
related to the differentiation process of Th17 cells, and these
factors antagonize each other in immune response. Thus, the balance
of Treg/Th17 is the key in maintaining immune homeostasis, and the
imbalance of Treg/Th17 is associated with a variety of autoimmune
diseases (15–17). TGF-β is the most important cytokine
that affects the differentiation of Treg cells and Th17 cells. Low
levels of TGF-β and IL-10 can induce the expression of
transcription factor RORγ, so as to induce the differentiation of T
cells to Th17, and high levels of expression of TGF-β and IL-10 can
induce expression of transcription factor Foxp3, which in turn
induce the differentiation of T cells to Treg (18). Previous studies have reported
abnormalities in T cell function in patients with thrombocytopenia
(3,4), suggesting that Treg/Th17 cell imbalance
may be involved in the pathogenesis of thrombocytopenia. To this
end, we investigated the relative levels of Treg cells and Th17
cells in the blood of patients with chronic hepatitis B with
thrombocytopenia before and after treatment. In addition, serum
levels of Treg cell function related factors IL-10, TGF-β, and Th17
cell function related factors IL-17, IL-21 and IL-22 were also
measured to test whether treatment can restore the balance of
Treg/Th17 and provide a reference for evaluating the therapeutic
effect.
Patients and methods
General information
In this study, 45 patients with chronic hepatitis B
combined with thrombocytopenia (26 males and 19 females, mean age
44.1±13.5 years, mean duration of chronic hepatitis B 12.7±8.3
years, all HBsAg+, total bilirubin >17.1 µmol/l, HBV
DNA 4.8-12.1×107 copies/ml) were selected in
Heilongjiang Provincial Hospital (Harbin, China) from June 2015 to
December 2016. This study was approved by the Ethics Committee of
Heilongjiang Provincial Hospital. Signed informed consents were
obtained from all participants before the study. All patients were
treated with prednisone acetate tablets (SFDA approval no.
H12020689; Tianjin Tianyao Pharmaceuticals Co., Ltd., Tianjin,
China) and intravenous injection of immunoglobulin (SFDA approval
no. S19994004; Shanxi Kangbao Biological Products Co., Ltd.,
Changzhi, China) for 60 days.
Sample collection
Fasting venous blood (5 ml) was extracted from each
patient before and after treatment. The non-anticoagulated blood
was kept at 4°C until coagulation. Centrifugation at 8,000 × g for
15 min was performed to collect serum to detect cytokines. In
addition, heparin anticoagulant blood (5 ml) was also collected and
gradient centrifugation was performed to isolate peripheral blood
mononuclear cells (PBMC). Cell density was adjusted to
2×106/ml for the detection of Treg and Th17 cells.
Routine blood examination and liver
function tests
Fasting peripheral venous blood was extracted from
each patient on the day of admission for routine blood examination
and liver function tests including alanine aminotransferase (ALT),
aspartate aminotransferase (AST) and prothrombin activity (PTA).
After treatment, platelet count returned to normal levels
(100-300×109/l) was defined as complete response.
Platelet count lower than normal level was defined as
non-response.
Detection of Treg cell ratio in
peripheral blood
Anticoagulant blood (0.1 ml) was transferred to
centrifuge tube, and Ficoll lymphocyte separation solution was used
to separate lymphocytes. Mouse anti-human CD4-FITC and CD25-PE
antibodies (1:1,000; cat. nos. sc-1176 and sc-19628; Santa Cruz
Biotechnology, Inc., Dallas, TX, USA) were added, followed by
incubation at room temperature for 30 min. After washing with 0.05%
PBST 3 times, 0.1 ml of 0.1% Triton X-100 was added and incubated
for 15 min. Then mouse anti-human Foxp3-PEcy5 monoclonal antibody
(1:800; cat. no. sc-53876; Santa Cruz Biotechnology) was added and
incubated at room temperature for 30 min. PEcy5-IgG1 was used as
control. The percentage of CD4+, CD25+ and
Foxp3+ cells in CD4+ cells was detected by
flow cytometry (BD FACSCanto II; BD Biosciences, San Jose, CA,
USA). FlowJo 7.0 software was used to analyze flow cytometry
data.
Detection of Th17 cell ratio in
peripheral blood
Anticoagulant blood (0.1 ml) was transferred to
centrifuge tube, and then Ficoll lymphocyte separation solution was
added to separate lymphocytes. Mouse anti-human CD4-FITC antibody
was added, followed by incubation at room temperature for 30 min.
After washing with 0.05% PBST 3 times, 0.1 ml of 0.1% Triton X-100
was added and incubated for 15 min. Then mouse anti-human IL17-PE
antibody (1:900; cat. no. sc-376374; Santa Cruz Biotechnology) was
added and incubated at room temperature for 30 min. PE-IgG1 was
used as control. The percentage of CD4+ and
IL-17+ cells in CD4+ cells was detected by
flow cytometry (BD FACSCanto II; BD Biosciences). FlowJo 7.0
software was used to analyze flow cytometry data.
Detection of cytokines
Levels of IL-10 (pg/ml), TGF-β (pg/ml), IL-17
(pg/ml), IL-21 (pg/ml) and IL-22 (pg/ml) in serum of patients were
measured before and after treatment using a kit (Invitrogen; Thermo
Fisher Scientific, Inc., Waltham, MA, USA). Double antibody
sandwich ELISA was used. ELISA plate was coated with corresponding
mouse anti-human IL-10, TGF-β, IL-17, IL-21 and IL-22 IgG
monoclonal antibodies and mouse IgGl (1:500; cat. nos. sc-365858,
sc-65378, sc-53937, sc-137120, sc-134366 and sc-2025; Santa Cruz
Biotechnology) was used as a control. A total of 0.1 ml serum was
added and incubated at room temperature for 30 min. After washing
with 0.05% PBST 3 times, horse anti-mouse secondary polyclonal
antibody IgG-HRP (1:1,000; cat. no. 7076; Cell Signaling
Technology, Inc., Danvers, MA, USA) was added and incubated at room
temperature for 30 min. After washing with 0.05% PBST 3 times,
enzyme reaction substrate TMB (0.1 ml) was added and incubated for
10 min. Duplicate wells were set for each sample. OD value at 490
nm was measured by a microplate reader (Multiskan FC; Thermo Fisher
Scientific, Inc.) and results were expressed as the mean values of
two duplicate wells.
Statistical analysis
Statistical analysis was performed using SPSS 19.0
software (IBM Corp., Armonk, NY, USA). The measurement data were
expressed as mean ± standard deviation, and comparisons between
different time-points in the same group were performed using paired
t-test, and comparison between groups were performed using
Student's t-test. ANOVA was used for comparison between multiple
groups and the post hoc test was SNK test. P<0.05 was considered
to indicate a statistically significant difference.
Results
Results of routine blood examination
and liver function tests
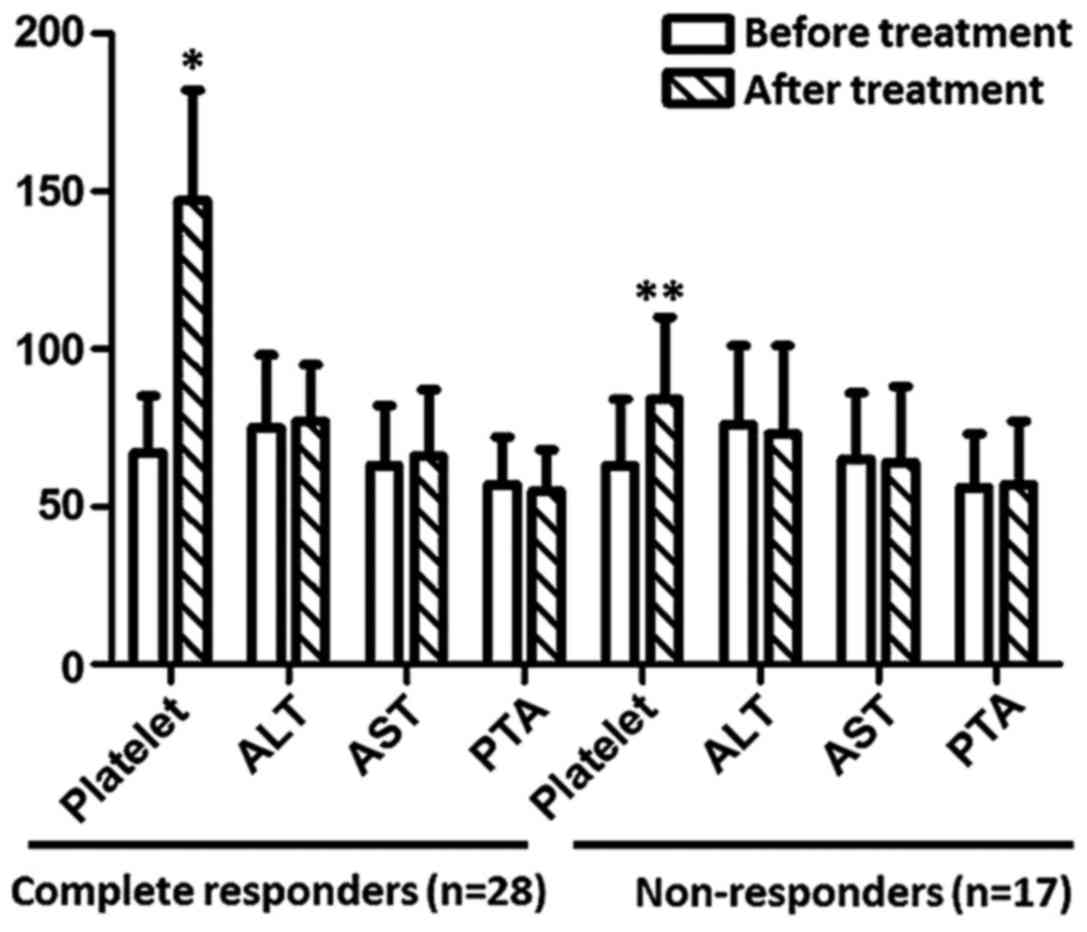
As shown in Fig. 1,
after treatment, platelet count returned to normal level in
complete responders (n=28). Although platelet count was
significantly increased in non-responders (n=17) (P<0.05), the
level is still lower than normal level (100×109/l).
After treatment, no significant changes in ALT, AST and PTA were
observed in complete responders or non-responders (P>0.05).
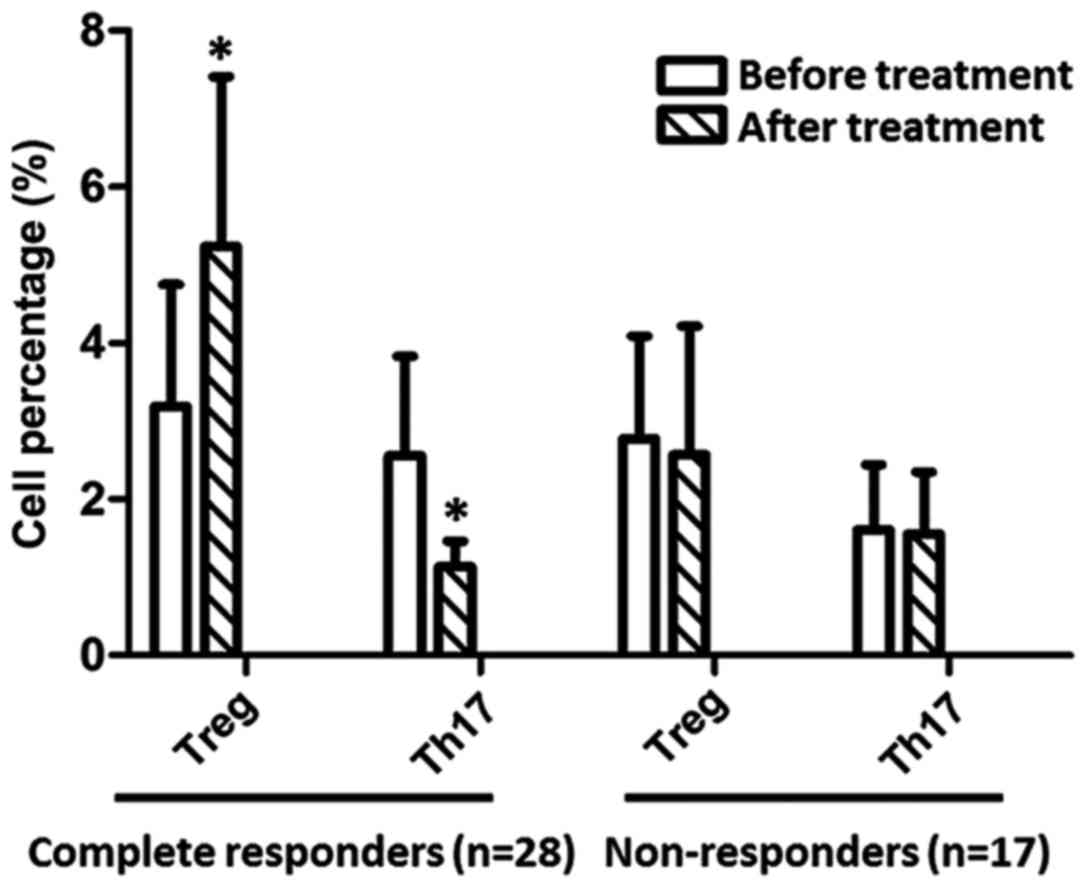
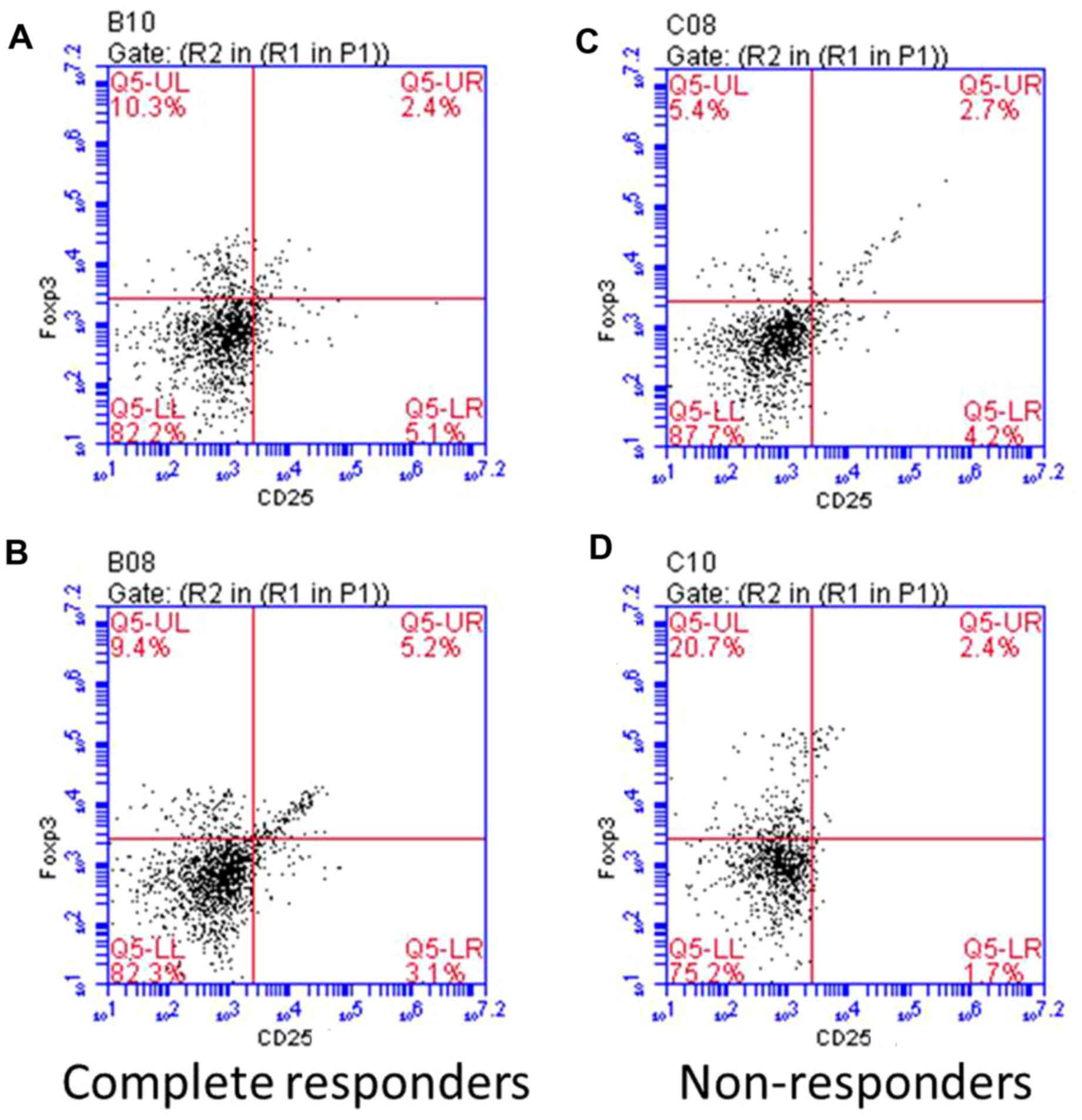
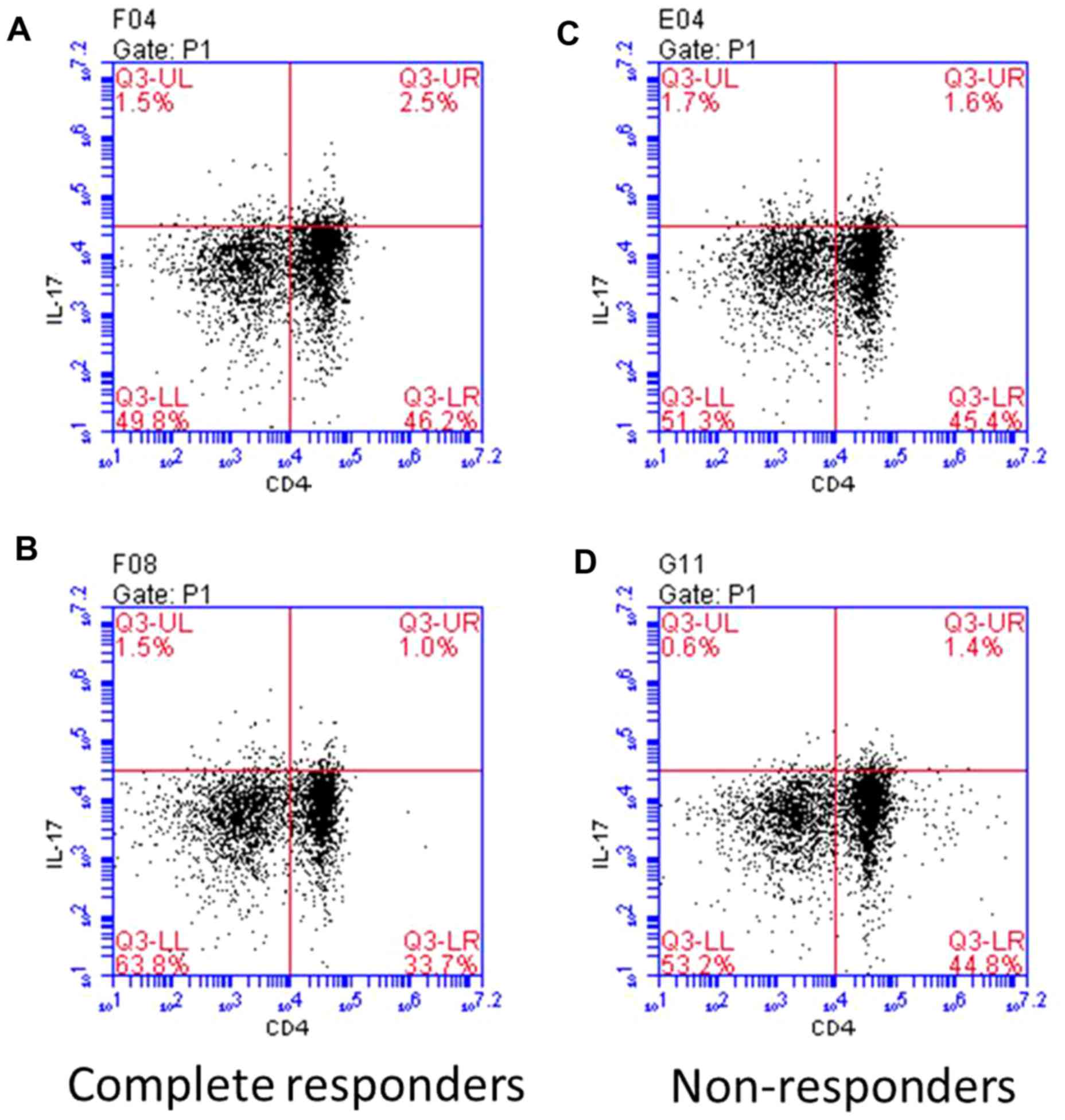
Percentages of Treg and Th17 cells in
CD4+ T cells. As shown in Fig. 2, before treatment, the percentage of
Treg cells was higher in complete responders than that in
non-responders, but the difference was not significant, but the
percentage of Treg cells was significantly higher in complete
responders than that in non-responders (P<0.05). After
treatment, the percentage of Treg cells was significantly increased
and the percentage of Th17 cells was significantly decreased in
complete responders (P<0.01). No significant changes in the
percentage of Treg cells and Th17 cells were found in
non-responders after treatment (P>0.05). Compared with
non-responders, the percentage of Treg cells was significantly
increased and percentage of Th17 cells was significantly decreased
in complete responders after treatment (P<0.01). Repsresentative
flow cytomerty is shown in Figs. 3
and 4.
Serum levels of cytokines in patients before and
after treatment. As shown in Fig. 5,
before treatment, levels of IL-10 and TGF-β were significantly
lower, and levels of IL-17, IL-21 and IL-22 were significantly
higher in complete responders than those in non-responders
(P<0.05). After treatment, levels of IL-10 and TGF-β were
significantly increased, and levels of IL-17, IL-21 and IL-22 were
significantly decreased in complete responders (P<0.05). No
significant differences in levels of IL-10, TGF-β, IL-17, IL-21 and
IL-22 were found in non-responders after treatment. Thus, after
treatment, levels of IL-10 and TGF-β were significantly higher, and
levels of IL-17, IL-21 and IL-22 were significantly lower in
complete responders than those in non-responders (P<0.05).
Discussion
Treg cells can maintain the tolerance of autoimmune
and anti-inflammatory response. On the contrary, Th17 can mediate
autoimmune diseases and inflammatory response. The balance between
these two factors can maintain the steady state of immune response,
and the imbalance will lead to the occurrence of autoimmune
disease. Treg/Th17 cell imbalance is an important mechanism leading
to persistent viral infection in patients with chronic hepatitis B.
Increase in number of Tregs and decrease in the number of Th17 can
lead to inhibition of T cell immunity in patients, and cellular
immune response against hepatitis B virus will be inhibited
(19,20). Studies have shown that
platelet-related antibodies are one of the major causes of
thrombocytopenia (21), suggesting
that Treg/Th17 cell imbalance may be involved in the production of
autoimmune platelet-associated antibodies (22).
This study showed that the percentage of Treg cells
was increased, and percentage of Th17 cells was decreased, and
platelet count returned to normal levels in patients with complete
response. Correspondingly, levels of IL-10 and TGF-β were
significantly increased, and levels of IL-17, IL-21 and IL-22 were
significantly decreased after treatment, which reflects that Treg
cells can inhibit inflammatory response and reduce the number of
Th17, which in turn improves thrombocytopenia. No significant
changes in Treg, Th17 and related cytokines were observed after
treatment, indicating that treatment failed to reverse the
imbalance of Treg/Th17. Therefore, Treg, Th17 and related cytokines
can be used to predict prognosis. It is noteworthy that before
treatment, numbers of both Treg cells and Th17 cells were higher in
complete responders than those in non-responders, suggesting that
the higher percentage of two cells may indicate good treatment
outcomes.
Consistent with previous studies (19,23,24),
this study showed that recovery of Treg/Th17 cell balance is
beneficial for the improvement of thrombocytopenia in patients with
chronic hepatitis B. Our study provides a theoretical basis for
clinical treatment of thrombocytopenia in patients with hepatitis
B.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YW and LW collected and analyzed the general
information of patients. WG collected the blood and tissue samples.
XC performed ELISA. YS helped with flow cytometry. All authors read
and approved the final manuscript.
Ethics approval and consent to
participate
This study was approved by the Ethics Committee of
Heilongjiang Provincial Hospital (Harbin, China). Signed informed
consents were obtained from all participants before the study.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Peck-Radosavljevic M: Thrombocytopenia in
liver disease. Can J Gastroenterol. 14:60D–66D. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Thomopoulos KC, Labropoulou-Karatza C,
Mimidis KP, Katsakoulis EC, Iconomou G and Nikolopoulou VN:
Non-invasive predictors of the presence of large oesophageal
varices in patients with cirrhosis. Dig Liver Dis. 35:473–478.
2003. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Aref S, Mabed M, Selim T, Goda T and
Khafagy N: Thrombopoietin (TPO) levels in hepatic patients with
thrombocytopenia. Hematology. 9:351–356. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Afdhal N, McHutchison J, Brown R, Jacobson
I, Manns M, Poordad F, Weksler B and Esteban R: Thrombocytopenia
associated with chronic liver disease. J Hepatol. 48:1000–1007.
2008. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Stornaiuolo G, Amato A and Gaeta GB:
Adefovir dipivoxil-associated thrombocytopenia in a patient with
chronic hepatitis B. Dig Liver Dis. 38:211–212. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Rodeghiero F, Stasi R, Gernsheimer T,
Michel M, Provan D, Arnold DM, Bussel JB, Cines DB, Chong BH,
Cooper N, et al: Standardization of terminology, definitions and
outcome criteria in immune thrombocytopenic purpura of adults and
children: Report from an international working group. Blood.
113:pp. 2386–2393. 2009, View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Shevach EM: Mechanisms of
foxp3+ T regulatory cell-mediated suppression. Immunity.
30:636–645. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Wing K, Onishi Y, Prieto-Martin P,
Yamaguchi T, Miyara M, Fehervari Z, Nomura T and Sakaguchi S:
CTLA-4 control over Foxp3+ regulatory T cell function.
Science. 322:271–275. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Mittal SK and Roche PA: Suppression of
antigen presentation by IL-10. Curr Opin Immunol. 34:22–27. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Keswani T, Sarkar S, Sengupta A and
Bhattacharyya A: Role of TGF-β and IL-6 in dendritic cells, Treg
and Th17 mediated immune response during experimental cerebral
malaria. Cytokine. 88:154–166. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Liu J, Hong X, Lin D, Luo X, Zhu M and Mo
H: Artesunate influences Th17/Treg lymphocyte balance by modulating
Treg apoptosis and Th17 proliferation in a murine model of
rheumatoid arthritis. Exp Ther Med. 13:2267–2273. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Shrivastava S, TrehanPati N, Patra S,
Kottilil S, Pande C, Trivedi SS and Sarin SK: Increased regulatory
T cells and impaired functions of circulating CD8 T lymphocytes is
associated with viral persistence in Hepatitis B virus-positive
newborns. J Viral Hepat. 20:582–591. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Feng S, Chen XM, Wang JF and Xu XQ: Th17
cells associated cytokines and cancer. Eur Rev Med Pharmacol Sci.
20:4032–4040. 2016.PubMed/NCBI
|
|
14
|
Harrington LE, Hatton RD, Mangan PR,
Turner H, Murphy TL, Murphy KM and Weaver CT: Interleukin
17-producing CD4+ effector T cells develop via a lineage
distinct from the T helper type 1 and 2 lineages. Nat Immunol.
6:1123–1132. 2005. View
Article : Google Scholar : PubMed/NCBI
|
|
15
|
Li J, Lai X, Liao W, He Y, Liu Y and Gong
J: The dynamic changes of Th17/Treg cytokines in rat liver
transplant rejection and tolerance. Int Immunopharmacol.
11:962–967. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ni K, Zhao L, Wu J, Chen W, Hongya Yang
and Li X: Th17/Treg balance in children with obstructive sleep
apnea syndrome and the relationship with allergic rhinitis. Int J
Pediatr Otorhinolaryngol. 79:1448–1454. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Zheng Y, Wang Z, Deng L, Zhang G, Yuan X,
Huang L, Xu W and Shen L: Modulation of STAT3 and STAT5 activity
rectifies the imbalance of Th17 and Treg cells in patients with
acute coronary syndrome. Clin Immunol. 157:65–77. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Kleinewietfeld M and Hafler DA: The
plasticity of human Treg and Th17 cells and its role in
autoimmunity. Semin Immunol. 25:305–312. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Su ZJ, Yu XP, Guo RY, Ming DS, Huang LY,
Su ML, Deng Y and Lin ZZ: Changes in the balance between Treg and
Th17 cells in patients with chronic hepatitis B. Diagn Microbiol
Infect Dis. 76:437–444. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Li K, Liu H and Guo T: Th17/Treg imbalance
is an indicator of liver cirrhosis process and a risk factor for
HCC occurrence in HBV patients. Clin Res Hepatol Gastroenterol.
41:399–407. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Gilli SC, de Souza Medina S, de Castro V,
Fernandes LG and Saad ST: Platelet associated IgG may be related
with thrombocytopenia in patients with myelodysplastic syndromes.
Leuk Res. 36:554–559. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Aboul-Fotoh L-M, Abdel Raheem MM, El-Deen
MA and Osman AM: Role of CD4+CD25+ T cells in
children with idiopathic thrombocytopenic purpura. J Pediatr
Hematol Oncol. 33:81–85. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Liu B, Gao W, Zhang L, Wang J, Chen M,
Peng M, Ren H and Hu P: Th17/Treg imbalance and increased
interleukin-21 are associated with liver injury in patients with
chronic severe hepatitis B. Int Immunopharmacol. 46:48–55. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Cao J, Chen C, Zeng L, Li L, Li X, Li Z
and Xu K: Elevated plasma IL-22 levels correlated with Th1 and Th22
cells in patients with immune thrombocytopenia. Clin Immunol.
141:121–123. 2011. View Article : Google Scholar : PubMed/NCBI
|