Introduction
The consequences of myocardial infarction (MI)
mainly comprise myocardial hypertrophy and myocardial remodeling.
The mechanisms of myocardial remodeling following MI are complex,
and in recent years, studies have demonstrated that except for
mechanical stimulation and neuroendocrine activation, post-MI
myocardial remodeling is also associated with the overexpression of
inflammatory cytokines. Seropian et al (1) reported that the expression of
myocardial interleukin 1β (IL-1β) and tumor necrosis factor α
(TNF-α) in rats was still significantly increased at 20 weeks after
MI. Shioi et al (2) found
that in hypertrophic left ventricles, the expression of myocardial
IL-1β mRNA was increased by 3.9-fold of that in normal ones, which
was also correlated with the left ventricular mass index.
Zarrouk-Mahjoub et al (3)
investigated the roles of inflammatory cytokines in myocardial
remodeling and identified that after MI, the excessive and
persistent presence of cytokines in post-MI myocardial cells
gradually induces their morphological changes and activation of
matrix metalloproteinase (MMP), thus further inducing the
remodeling process.
The nuclear factor-κB (NF-κB) activation pathway
exists in cardiac cells, smooth muscle cells and endothelial cells
(4). The transcriptional process of
inflammatory cytokines is mainly regulated by NF-κB, which has an
important role in the process of myocardial remodeling. Sun et
al (5) used the NF-κB inhibitor
IMD-0534 to reduce myocardial remodeling and improve cardiac
function in MI rats. NF-κB is a transcription factor with the
ability to regulate multidirectional gene transcription. It usually
forms a dimer with p65/p50 and binds to the inhibitor of NF-κB
(I-κB) to thereby form an inactive trimer that then prevails in the
cytoplasm (6). The activation of
NF-κB is controlled by ubiquitin-proteasome system, and the
specific activation process is as follows: First, the Ser32 and 36
residues of I-κB are phosphorylated by certain protein kinases and
then ubiquitinated through combining with ubiquitin; when the above
complex is degraded by the 26S proteasome, I-κB and NF-κB then
dissociate, and NF-κB enters the nucleus so as to initiate the
relevant gene transcription (7).
When cells are stimulated by ischemia and hypoxia, the activity of
the proteasome increases, leading to the degradation of I-κB, the
dissociation of NF-κB and I-κB, and the penetration of the
activated p65 into the nucleus, followed by upregulation of
inflammatory cytokines, including TNF-α, IL-6 and IL-1β. Although
NF-κB activates inflammatory cytokines at the transcriptional
level, these factors also contribute to the activation of NF-κB,
thus initiating inflammatory self-amplification (8). Studies have indicated that
ubiquitin-proteasome inhibitors block the activation of NF-κB,
which were therefore recommended as novel anti-inflammatory drugs
used in diseases including asthma and rheumatoid arthritis
(9). Santos et al (10) reported that the proteasome inhibitor
MLN519 inhibits the activation of NF-κB, thus reducing the
expression of inflammatory cytokines TNF-α, IL-1β and IL-6 and
reducing myocardial ischemia-reperfusion injury. Chen et al
(11) obtained similar results with
carbobenzoxy-Leu-Leu-leucinal (MG-132). However, to the best of our
knowledge, no previous study has reported on the application of
proteasome inhibitors toward post-MI myocardial remodeling.
Previous studies by our group have demonstrated that MG-132
improves myocardial remodeling in MI rats (12), but the underlying mechanisms have
remained elusive. In the present study, it was hypothesized that
MG-132 may have an important role in post-MI myocardial remodeling
by inhibiting the activation of NF-κB and downregulating
inflammatory cytokines such as IL-1β; furthermore, the process of
remodeling was histologically examined.
Materials and methods
Generation of animal model and
specimen collection
A total of 68 Sprague Dawley rats (8 weeks old,
male-to-female ratio, 1:1; body weight, 200-250 g) were purchased
from the Experimental Animal Center of Chongqing Medical University
(Chongqing, China) and used to prepare the MI model. All rats were
housed under standard conditions (temperature, 20±1°C; humidity,
60±10%; 12-h light/dark cycle) and had free access to standard
rodent chow and water. The experimental processes strictly abided
the requirements of the animal experimental guidelines issued by
the International Association for the Study of Pain (13,14). The
18 rats in which modeling was successful and who survived for
>24 h were randomly divided into the MI group, the MG group and
the pyrrolidine dithiocarbamic acid (PDTC) group, with 6 rats in
each group. Another 6 rats were set as the sham operation group
(SH). The operation procedures in the SH group were identical to
those for the MI rats, with the exception that the rats were only
threaded but not ligated. The intervention measures in the
different groups were as follows: Animals in the MG group were
intraperitoneally injected daily with 0.1 mg/kg/day MG-132
(Calbiochem, Shanghai, China) on the second day as described
previously (15) until the 28th day;
in the PDTC group, animals were intraperitoneally injected with 80
mg/kg/day PDTC (Shanghai Zhen Zhen Biological Science and
Technology Co., Ltd., Shanghai, China) on the second day as
described previously (16) until the
28th day; in the MI and SH group, animals were intraperitoneally
injected the same volume of saline. On day 28, the rats were
weighed and then inhaled a lethal concentration of isoflurane
(3-5%) in a chamber. The heart was then sampled out before it
stopped beating, washed with normal saline and divided into 3 parts
along the long axis of the left ventricle. The cardiac base and
cardiac apex (non-infarct areas) were frozen in liquid nitrogen at
−70°C for reverse-transcription quantitative polymerase chain
reaction (RT-qPCR) and western blot analysis. The middle part was
cut into 3-mm pieces, fixed in 4% formaldehyde solution for 24 h,
embedded in paraffin and cut into 5-µm slices. This study was
performed in strict accordance with the recommendations in the
Guide for the Care and Use of Laboratory Animals of the National
Institutes of Health. The experimental animal protocol was reviewed
and approved by the Institutional Animal Care and Use Committee of
Dali University (Dali, China) since the experiment was conducted at
Dali University.
Volume fraction of collagens
Five non-overlapping microscopic fields were
randomly selected from the non-MI zone of the picrosirius
red-stained slices (17) to
determine the ratio of collagen (red) vs. the whole area by a
biomedical image analysis system (CM2000B, Beijing University of
Aeronautics and Astronautics, Beijing, China), and the mean value
was used as the total collagen content. Furthermore, the non-MI
zone was imaged under a polarized light microscope to calculate the
volume fractions of type I collagen (red) and type III collagen
(green), as well as to calculate the ratio of type I/III
collagen.
Morphological parameters
For each specimen, two hematoxylin and eosin-stained
slices were selected to determine various morphometric parameters
of cardiomyocytes using the CM-2000B biomedical imaging system
(Beijing University of Aeronautics and Astronautics) as described
previously (17). From each slice,
five fields of view were selected and a computer was used to
calculate the morphometric parameters of cardiomyocytes in the
field center, including the myocardial cell area, perimeter and
mean diameter.
RT-qPCR
The total RNA of rat cardiomyocytes was isolated
with TRIzol (Thermo Fisher Scientific, Inc., Waltham, MA, USA). The
primers were synthesized by Shanghai Biosune Biotech Co., Ltd.
(Shanghai, China) and their sequences are listed in Table I. The RT-qPCR reaction system had a
volume of 50 µl, and the two-step process was performed according
to the kit instructions (FSQ-101; Toyobo, Tokyo, Japan) and
reagents listed in Table II. A
cycle for 5 min at 94°C, followed by 31 cycles of 30 sec at 94°C,
30 sec at 50-56°C, 45 sec at 72°C and a final cycle for 5 min at
72°C.
 | Table I.Primer sequences used for polymerase
chain reaction. |
Table I.
Primer sequences used for polymerase
chain reaction.
| Gene | Primer sequence
(5′-3′) | Product length
(bp) |
|---|
| NF-κB p65 |
|
|
|
Forward |
CAGCACATCCAGACAGACACCA | 480 |
|
Reverse |
GCTGCTAAAAGAATCCTCAAAACC |
|
| IL-1β |
|
|
|
Forward |
CACCTTCTTTTCCTTCATCTTTG | 381 |
|
Reverse |
AAGACAAACCGCTTTTCCATC |
|
| MMP-2 |
|
|
|
Forward |
CTACACCAAGAACTTCCGACTATC | 305 |
|
Reverse |
CCTCGTACACGGCATCAATC |
|
| β-actin |
|
|
|
Forward |
CAGCTTCTTCTAGTGCCGTTCC | 219 |
|
Reverse |
GGAGTCAGGTGTTTCTGGTGGAG |
|
| Table II.Two-step reverse transcription
quantitative polymerase chain reaction components. |
Table II.
Two-step reverse transcription
quantitative polymerase chain reaction components.
| Agents | Volume (µl) |
|---|
| ReverTra
Ace® | 50 |
| RNase lnhibitor | 50 |
| 5X RT Buffer (25 mM
MgCI2) | 200 |
| 10 mM dNTPs | 150 |
| RNase Free
H2O | 600 |
| Oligo(dT) 20 (10
pmol/µl) | 250 |
| Random Primer (25
pmol/µl) | 50 |
| Control Primer F (10
pmol/µl) | 50 |
| Control Primer R (10
pmol/µl) | 25 |
| Positive Control RNA
(105 copies/µl) | 25 |
| KOD | 50 |
| 10X PCR Buffer for
ReverTra | 250 |
| 25 mM
MgSO4 | 250 |
The relative production of NF-κB p65, IL-1β and
MMP-2 was calculated by QuantityOne 4.6 Image Analysis software
(Bio-Rad Laboratories, Inc., Hercules, CA, USA). The following
thermocycling conditions were used: The integral ratio of the
absorbance areas was used to express the DNA content, and the mRNA
expression levels were evaluated by the integral ratios of the
absorbance areas of the amplified NF-κB p65, IL-1β, MMP-2 and
β-actin bands (18).
Western blot analysis
The total myocardial protein was extracted from the
rat myocardium using radioimmunoprecipitation assay buffer,
followed by determination of the protein content via the
bicinchoninic acid method. The protein (40 µg per lane) was then
separated by 10% SDS-PAGE and transferred onto a polyvinylidene
fluoride membrane (Thermo Fisher Scientific, Inc.). Following
blocking in 5% non-fat milk for 1 h, the membrane was incubated
with rabbit anti-mouse NF-κB, IL-1β, MMP-2 and β-actin antibodies
(1:750, 1:400, 1:500 and 1:400 dilution; Santa Cruz Biotechnology,
Inc., Dallas, TX, USA) at room temperature for 2 h. The membrane
was then incubated with secondary antibody (goat anti-rabbit
immunoglobulin G, SA00001-2; ProteinTech Group, Inc., Chicago, IL,
USA) at room temperature for 1 h, followed by visualization using a
chemoluminescent reagent (Jiangsu Biyuntian Biotechnology Research
Institute, Jiangsu, China). Images were captured using a gel
imaging system (Bio-Rad Laboratories, Inc.), and then scanned and
analyzed.
Immunohistochemistry
Sample preparation was performed according to the
instructions of the Goat anti-rabbit SP immunohistochemical kit S
(P-0023; Shanghai Dingjie Biotechnology Co., Ltd., Shanghai, China)
and NF-κB p65 expression was then observed under high-power vision
(magnification, ×400). Samples were embedded, sliced and dewaxed,
then xylene I and II were added for 20 min each at room
temperature. Subsequently, samples were subjected to rehydration in
a gradient alcohol series and were washed with PBS three times for
5 min each time. Samples, were submerged in 3%
H2O2 20 µl for 5 min to eliminate the
activity of endogenous peroxidase and washed with PBS three times
for 5 min each time. Samples were incubated with NF-κB p65
rabbit-anti-mouse IgG (sc-8008, dilution 1:100; Santa Cruz
Biotechnology, Inc.) and incubated overnight at 4°C, washed with
PBS three times for 5 min each and incubated with secondary
antibody labeled with biotin at 37°C for 15 min. Following this,
samples were washed with PBS three times for 5 min and incubated
with horseradish peroxidase 37°C for 15 min, washed with PBS three
times for 5 min, incubated with 3,3′-diaminobenzidine for 3-5 min
and counterstained with hematoxylin for 3-5 min at room
temperature. Sections were observed using a light microscope
(magnification, ×400).
Semi-quantitative analysis was performed according
to the method by Wang et al (4), with positive staining appearing as
brown granules in the myocardial nuclei. The positive index (PI)
was then calculated as PI=number of positive cells/total number of
cells in the field ×100%. Five non-overlapping high-power fields
were randomly selected from each slice to calculate the average.
The observation of IL-1β and MMP-2 followed the same steps; the
antibody concentration was 1:100, and positive staining was defined
as brown granules appearing in the myocardial cytoplasm or nuclei.
Medical image analysis software Image Pro Plus 6.0 (Media
Cybernetics, Inc., Rockville, MD, USA) was used to calculate the
integral optical density value.
Statistical analysis
All the data were analyzed using the SPSS12.0
statistical package (SPSS, Inc., Chicago, IL, USA). Values are
expressed as the mean ± standard deviation. Comparison between two
groups was performed using the Student's t-test. Multigroup
comparisons were performed using one-way analysis of variance
followed by Student-Newman-Keuls post hoc test. P<0.05 was
considered to indicate a statistically significant difference.
Results
Volume fraction of collagens by sirius
red staining
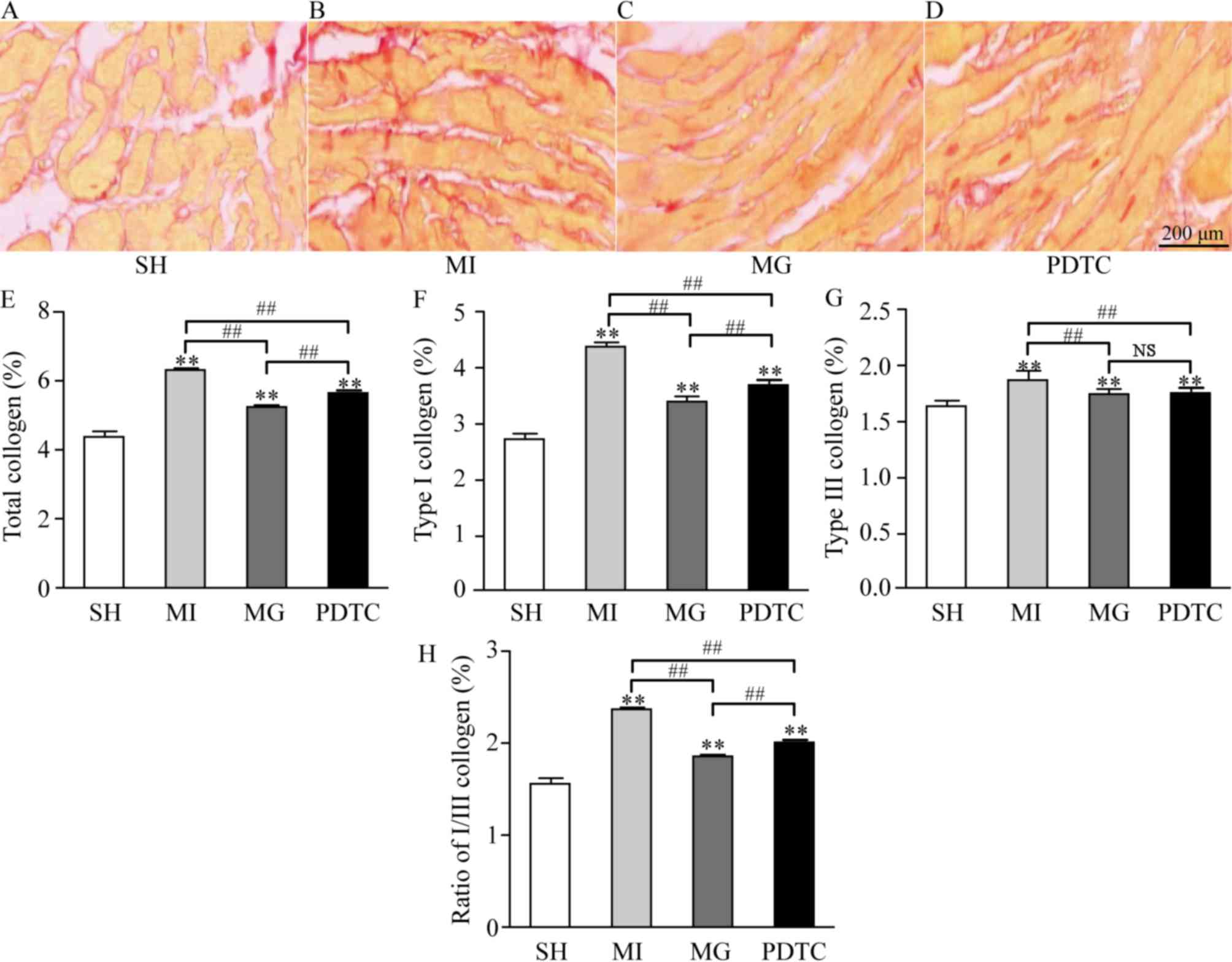
As indicated in Fig.
1, collagen was deposited differently in the different groups.
In the sham group, only a small amount of collagen was deposited in
the non-infarct area, while the amount of collagen deposited in the
MI group was large. In comparison with that in the MI group, the
volume of collagen deposition in the MG group was decreased after
treatment with MG-132, and there were significant differences
between the PDTC group and the MI group. Compared with the SH
group, total collagen, type I collagen, type III collagen and the
ratio of I/III collagen in the MI, MG and PDTC groups were
significantly increased (P<0.01). This was more notable in the
MI group; however, the above indexes in the MG group and the PDTC
group were significantly lower compared with those in MI group
(P<0.01), suggesting that MG-132 and PDTC improved the collagen
remodeling in non-infarcted area after myocardial infarction in
rats. In comparison with that in the PDTC group, total collagen,
type I collagen and the ratio of I/III were significantly decreased
in the MG group (P<0.01). However, there was no significant
difference between the MG and PDTC groups with regard to type III
collagen.
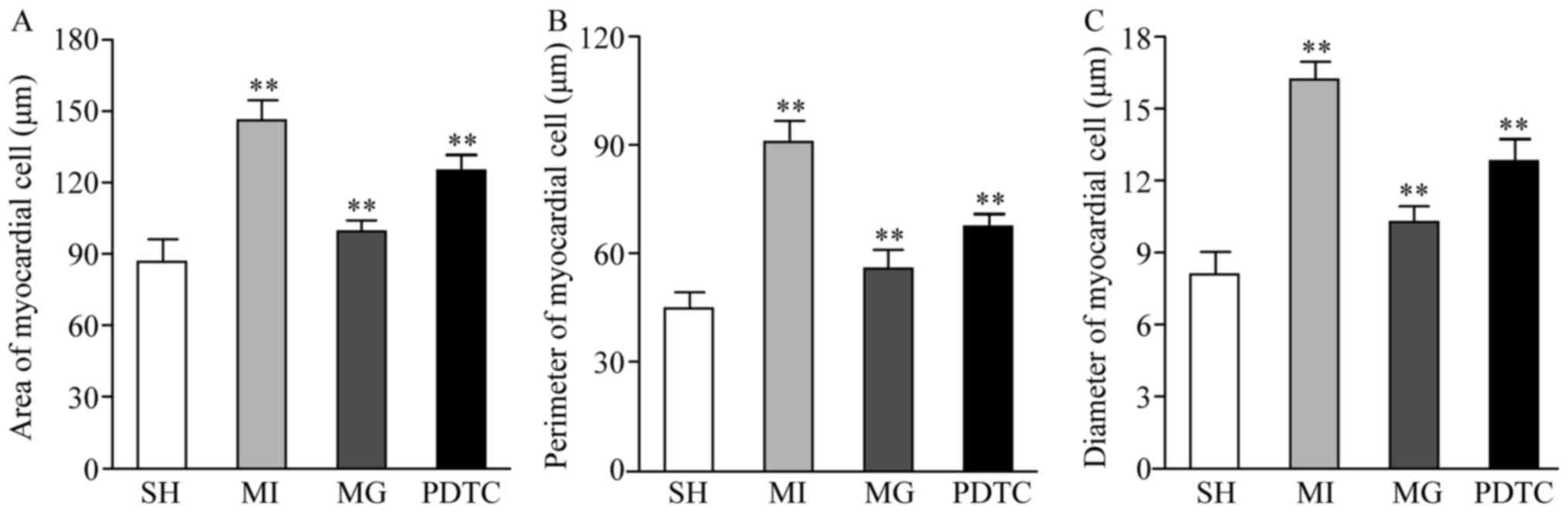
Morphological parameters
The cell surface area, perimeter and diameter in the
non-infraction zone were significantly increased in the MI group
compared with those in the SH group, while they were reduced in the
PDTC group and further decreased in the MG group compared with
those in the MI group. Significant differences were determined
between each pair of groups (P<0.01; Fig. 2).
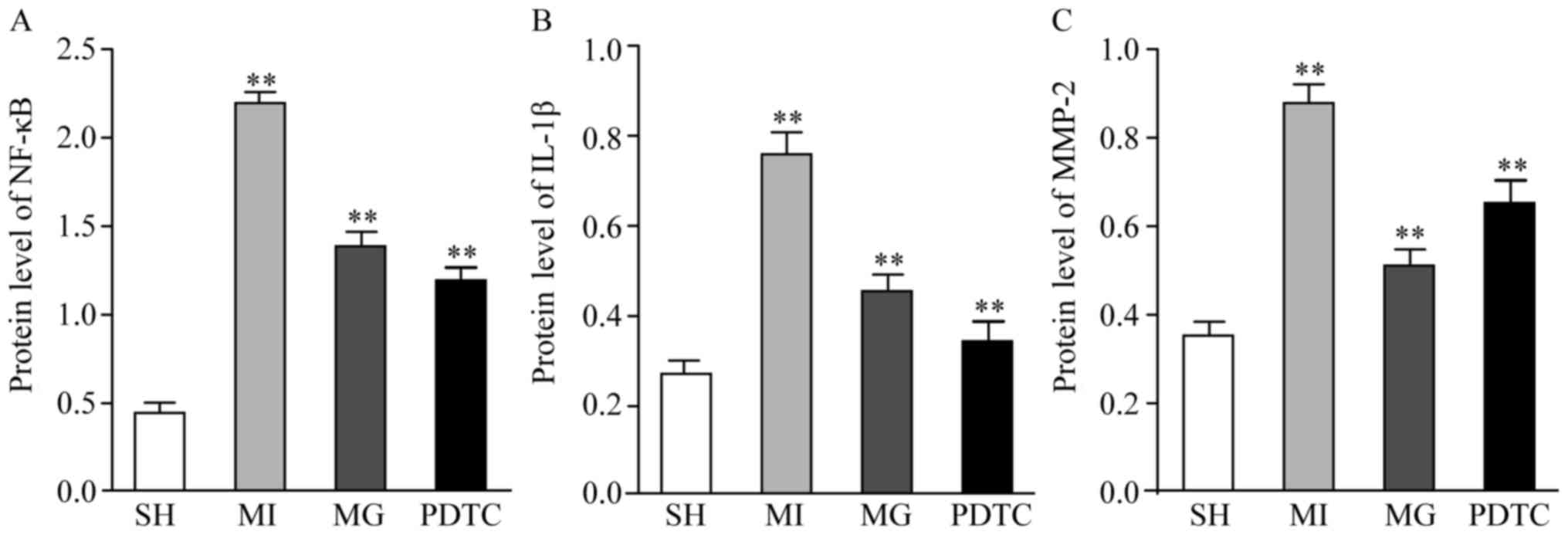
Effects of MG-132 and PDTC on NF-κB,
IL-1β and MMP-2 after MI
The mRNA and protein levels of NF-κB, IL-1β and
MMP-2 were determined by RT-qPCR (Fig.
3) and western blot analysis (Fig.
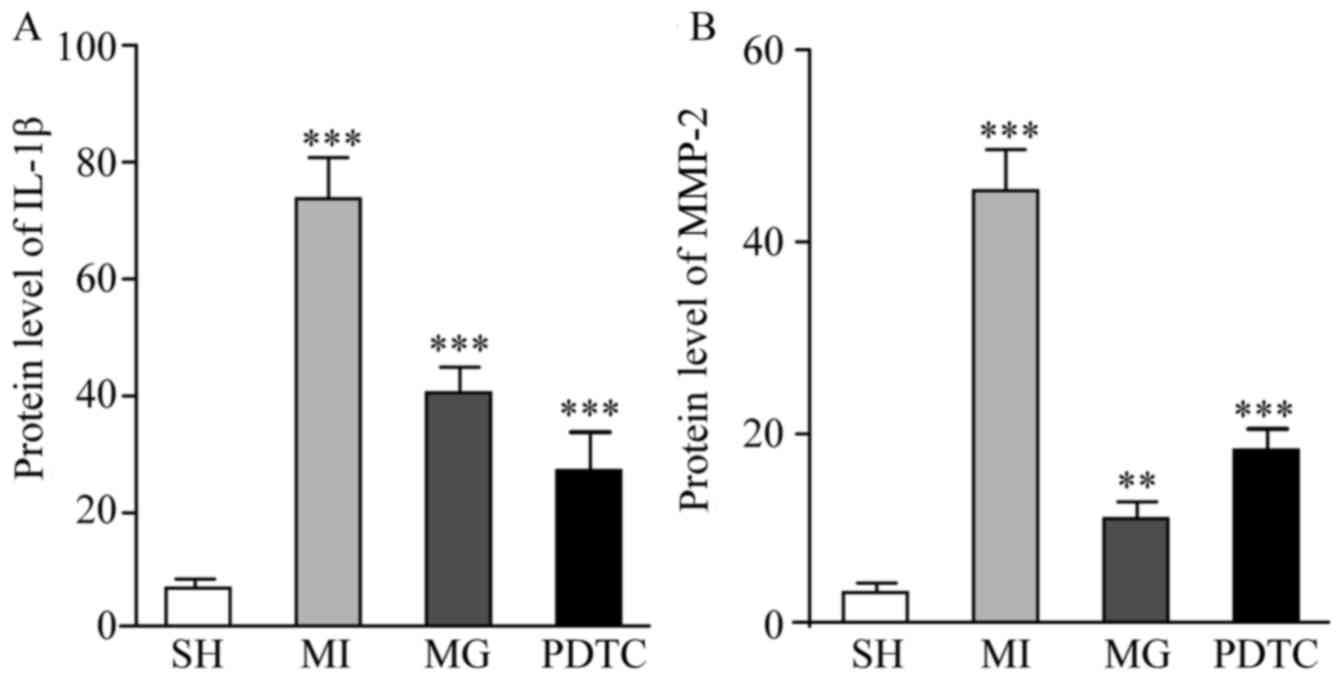
4). Furthermore, immunohistochemistry was performed to indicate
these effects (Figs. 5 and 6; data not shown for NF-κB). The results
indicated that NF-κB, IL-1β and MMP-2 displayed the greatest
increase in the MI group compared with that in the SH group, while
these increases were significantly blunted by treatment with PDTC
or MG-132. Treatment with PDTC caused the greatest decrease in
NF-κB and IL-1β and MG-132 caused the greatest decrease in MMP-2.
Immunohistochemistry indicated that NF-κB was expressed in the
nuclei (data not shown), IL-1β was expressed in the cytoplasm and
MMP-2 was expressed in the nuclei as well as the cytoplasm. The
results of the semi-quantitative analysis of the
immunohistochemical images were in accordance with the western blot
results (Fig. 6).
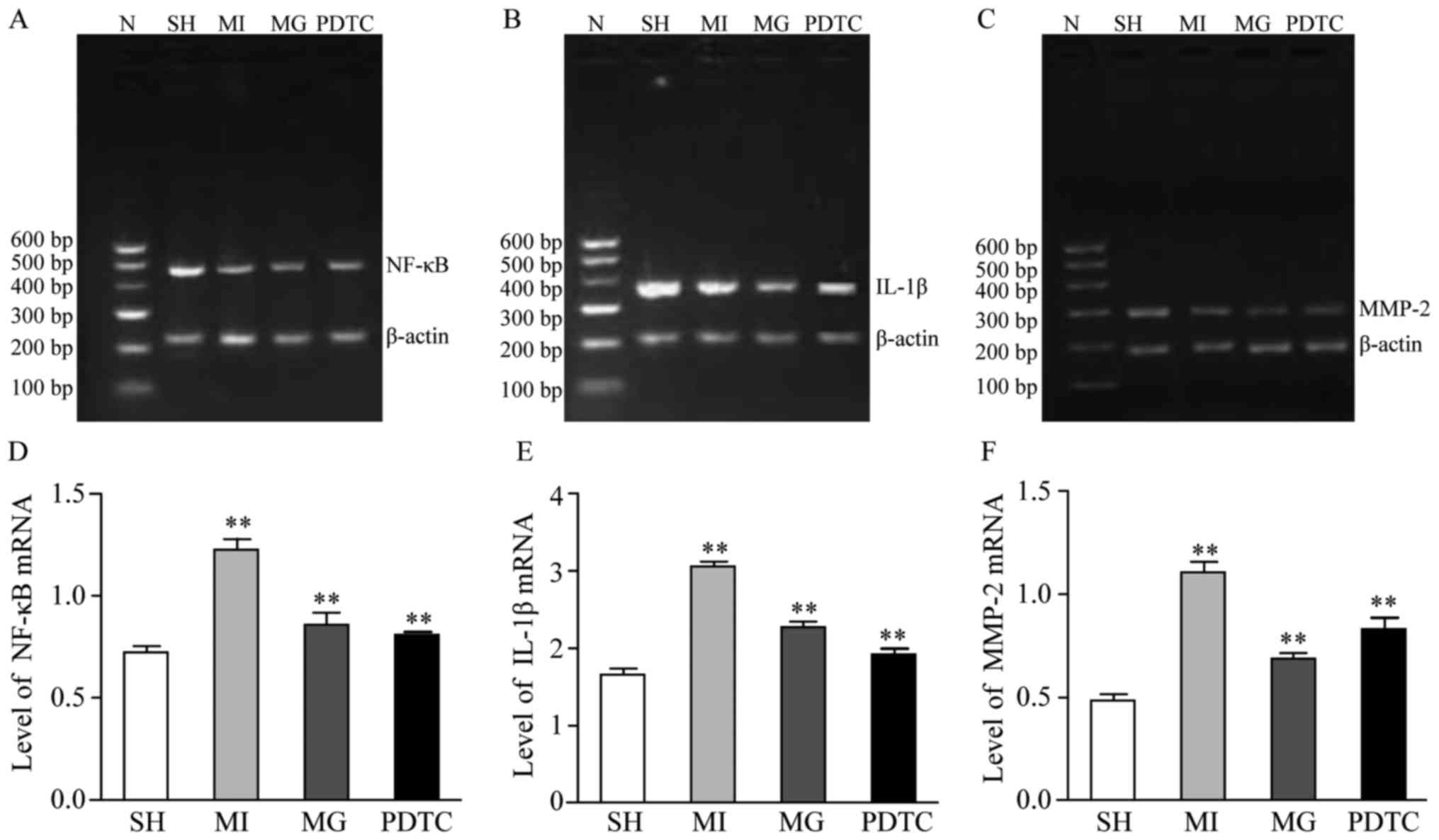 | Figure 3.mRNA expression of NF-κB, IL-1β and
MMP-2 in non-infarction zone in different groups. (A-C)
Representative gels of the amplimers of (A) NF-κB, (B) IL-1β and
(C) MMP-2. (D-F) Quantified expression levels of (D) NF-κB, (E)
IL-1β and (F) MMP-2. **P<0.01 for comparison between either two
groups. Groups: MI, myocardial infarction model group treated with
saline for 28 days; SH, sham; MG, model group treated with MG-132
for 28 days; PDTC, model group treated with pyrrolidine
dithiocarbamic acid for 28 days; N, marker; IL, interleukin; MMP,
matrix metalloproteinase; NF, nuclear factor. |
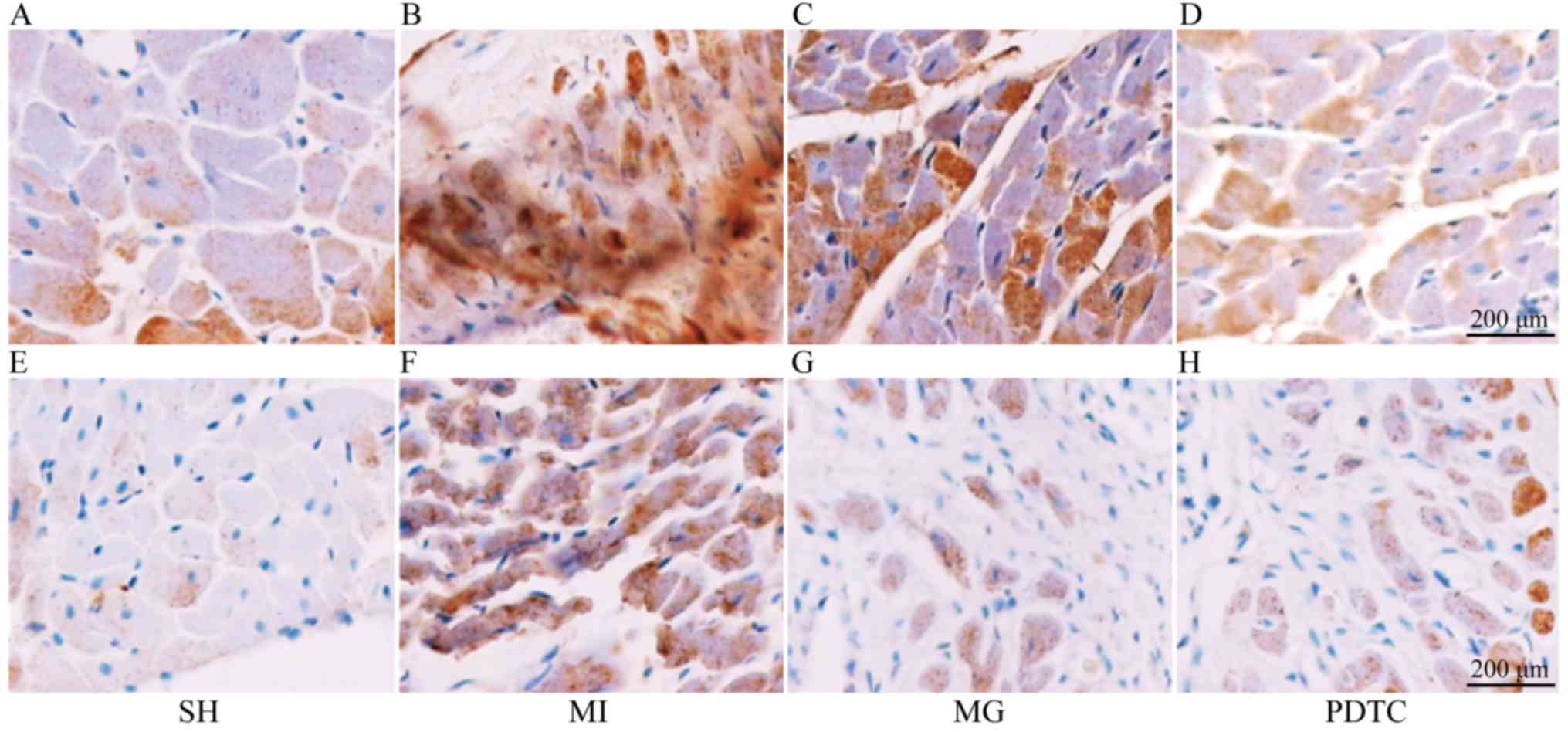 | Figure 5.Immunohistochemical staining for IL-1β
and MMP-2. (A-D) Staining for IL-1β in the (A) SH, (B) MI, (C) MG
and (D) PDTC groups. (E-H) Staining for MMP-2 in the (E) SH, (F)
MI, (G) MG and (H) PDTC groups (scale bar, 200 µm). Groups: MI,
myocardial infarction model group treated with saline for 28 days;
SH, sham; MG, model group treated with MG-132 for 28 days; PDTC,
model group treated with pyrrolidine dithiocarbamic acid for 28
days; IL, interleukin; MMP, matrix metalloproteinase; NF, nuclear
factor. |
Discussion
Post-MI myocardial remodeling is associated with the
upregulation of inflammatory cytokines, while intervention with
ubiquitin proteasome inhibitors blocks the activation of NF-κB and
leads to downregulation of the inflammatory cytokines. It has been
reported that short- and long-term treatment with MG-132
significantly attenuated hypertension-induced cardiac remodeling
and dysfunction, which may be mediated by the NF-κB/transforming
growth factor β1 signaling pathway (16). The present study investigated the
effects of MG-132 on myocardial remodeling in comparison with the
MI, SH and PDTC groups. Morphological changes and collagen
remodeling of myocardial cells were observed at 28 days after MI,
and the mRNA and protein expression of NF-κB, IL-1β and MMP-2 were
also determined.
The present study demonstrated that on day 28 after
MI, the surface area, perimeter and diameter of non-infarcted
cardiomyocytes in the MI group were increased compared with those
in the SH group, indicating that myocardial hypertrophy occurred in
the non-infarcted zone after MI. The application of MG-132 reduced
the surface area, perimeter and diameter of cardiomyocytes,
indicating that MG-132 reduced the degree of myocardial hypertrophy
in the non-MI zone. Studies using a model of myocardial hypertrophy
revealed that the proteasome inhibitors MG-132 and MG-262 reduce
the size of hypertrophic cardiomyocytes by 2-fold and reduce the
expression of myocardial hypertrophy-associated α-myosin heavy
chain, myosin light chain 2 and α-actin (19). The present study demonstrated that
in vivo application of MG-132 inhibited post-MI myocardial
remodeling, thus improving post-MI myocardial hypertrophy in the
non-MI zone.
Post-MI myocardial remodeling includes myocardial
parenchymal and interstitial remodeling, while the former appears
as myocardial hypertrophy and the latter is mainly caused by
myocardial interstitial fibrosis through increased collagen
deposition; changes of myocardial collagens are the driving factor
of interstitial remodeling. The present study used picrosirius red
staining and microscopically observed the deposition of total
collagen, type I collagen and type III collagen in the non-MI zone.
The results demonstrated that the MI group exhibited a significant
increase in collagen deposition as well as the quantified content
of total collagen, type I collagen and type III collagen.
Furthermore, the ratio of type I/III collagen was also increased,
indicating that collagen remodeling occurs after MI. The deposition
of total collagen, type I collagen and type I/III collagen in the
MG group was significantly decreased compared with that in the MI
group, and the ratio of type I vs. III collagen was decreased,
consistent with the results of Meiners et al (20), who used a rat model of spontaneous
hypertensive to demonstrate that MG-132 improves myocardial
collagen remodeling in the MI model.
In order to confirm whether MG-132 exerted its
effect of improving post-MI myocardial remodeling through
inhibiting the activation of NF-κB and downregulating the
expression of inflammatory cytokines, the present study detected
the expression of NF-κB, IL-1β and MMP-2 in cardiomyocytes at the
mRNA and protein level. The immunohistochemical results indicated
that NF-κB in the MI group was mainly expressed in the nuclei (data
not shown), indicating that NF-κB was continuously activated after
MI, consistent with the results of Wang et al (21). Furthermore, the RT-qPCR results of
the present study demonstrated that the mRNA expression of NF-κB
was increased after MI, and the protein expression of NF-κB p65 was
also confirmed to be increased by western blot analysis. Activation
of NF-κB increases the expression of inflammatory cytokines, which
then participate in cardiomyocyte hypertrophy and collagen
remodeling through a series of signaling pathways. In the present
study, the gene and protein levels of IL-1β in the MI group were
upregulated, indicating that inflammatory cytokines are upregulated
in the process of post-MI myocardial remodeling, consistent with
the results of a previous study (19). IL-1β may initiate the
c-Jun-N-terminal kinase/stress activated protein kinase pathway and
activate mitogen-activated protein kinase signaling, thus leading
to myocardial hypertrophy (20).
IL-1β also inhibits collagen synthesis by myocardial fibroblasts,
increases the activity of MMPs and promotes interstitial collagen
remodeling (20). After application
of MG-132, NF-κB and its downstream inflammatory cytokines (such as
IL-1β) were decreased, and the trend in the expression of IL-1β was
consistent with that of NF-κB, thus further confirming that MG-132
inhibited the activation of NF-κB and decreased the expression of
inflammatory cytokines. In parallel with the decrease in IL-1β,
myocardial hypertrophy in the non-MI zone was improved, consistent
with the results of previous studies (17). The present study also demonstrated
that after MG-132 was applied, the expression of MMP-2 reduced in
parallel with the decrease of NF-κB, IL-1β and the deposition of
total collagen, type I collagen and type I/III collagen in the
non-MI zone was significantly reduced, indicating that this pathway
improves collagen remodeling in the non-MI zone. While previous
studies reported that MG-132 attenuated myocardial hypertrophy and
collagen remodeling by decreasing the expression of IL-1β, no
direct evidence regarding inhibition of NF-κB was ever provided
(4,11). In the present study, by measuring the
gene and protein expression of NF-κB and its downstream products
IL-1β and MMP-2 and analyzing their association with myocardial
remodeling in the non-MI zone, it was confirmed that the mechanisms
by which MG-132 inhibited post-MI myocardial remodeling included
the reduction of NF-κB activation and the downregulation of
inflammatory factors. MG-132 may inhibit NF-κB through blocking the
activity of the 20 s proteasome (21,22), so
that the degradation of I-κB is reduced, the combination of NF-κB
with I-κB is increased, and the nuclear translocation of NF-κB is
blocked to thereby inhibit the activation of NF-κB.
The effects of MG-132 in improving post-MI
myocardial remodeling may proceed via additional mechanisms. The
present study compared MG-132 with PDTC, a specific inhibitor of
NF-κB. The results indicated that the expression of NF-κB, IL-1β
and MMP-2 in the PDTC group were decreased at the mRNA and protein
level, and morphological parameters including the cell surface
area, perimeter, diameter, and collagen deposition were improved,
which further confirmed that inhibiting the activation of NF-κB
improves post-MI myocardial remodeling. However, the comparison
between MG-132 and PDTC revealed that although PDTC exhibited
stronger effects in inhibiting the activation of NF-κB and
downregulating IL-1 than MG-132, its effects in myocardial
morphological changes, improving collagen deposition and
downregulating MMP-2 were less pronounced than those of MG-132.
This difference may be due to the dosage of MG-132 and PDTC, which
requires further study. However, in addition to inhibiting the
activation of NF-κB and downregulating the expression of
inflammatory proteins, MG-132 may have further mechanisms of
action, including dopaminergic neurons (23), nuclear factor erythroid 2-related
factor 2 (24) and it also could
induce apoptosis (25). Since MG-132
has not been introduced for clinical use, additional experiments
and clinical research are needed in the future.
Acknowledgements
Not applicable.
Funding
This work was funded by the Doctoral Research
Foundation of Dali University (grant no. KYBS201212).
Availability of data and materials
All data generated or analyzed during this study are
included in this published article.
Authors' contributions
XW, ZC and KL collaborated to design the study. HL
and SK were responsible for data analysis. YY performed RT-qPCR
experiments. ZC and YD performed western blot analysis and
immunohistochemistry analysis. All authors collaborated to
interpret results and develop the manuscript.
Ethics approval and consent to
participate
The experimental animal protocol was reviewed and
approved by the Institutional Animal Care and Use Committee of Dali
University (Dali, China).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Seropian IM, Toldo S, Van Tassell BW and
Abbate A: Anti-inflammatory strategies for ventricular remodeling
following ST-segment elevation acute myocardial infarction. J Am
Coll Cardiol. 63:1593–1603. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Shioi T, Matsumori A, Kihara Y, Inoko M,
Ono K, Iwanaga Y, Yamada T, Iwasaki A, Matsushima K and Sasayama S:
Increased expression of interleukin-1 beta and monocyte chemotactic
and activating factor/monocyte chemoattractant protein-1 in the
hypertrophied and failing heart with pressure overload. Circ Res.
81:664–671. 1997. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Zarrouk-Mahjoub S, Zaghdoudi M, Amira Z,
Chebi H, Khabouchi N, Finsterer J, Mechmeche R and Ghazouani E:
Pro- and anti-inflammatory cytokines in post-infarction left
ventricular remodeling. Int J Cardiol. 221:632–636. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Wang S, Kotamraju S, Konorev E, Kalivendi
S, Joseph J and Kalyanaraman B: Activation of nuclear factor-kappaB
during doxorubicin-induced apoptosis in endothelial cells and
myocytes is pro-apoptotic: The role of hydrogen peroxide. Biochem
J. 367:729–740. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Sun B, Xia Q and Gao Z: Total flavones of
choerospondias axillaris attenuate cardiac dysfunction and
myocardial interstitial fibrosis by modulating NF-kB signaling
pathway. Cardiovasc Toxicol. 15:283–289. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Xiao C and Ghosh S: NF-kappaB, an
evolutionarily conserved mediator of immune and inflammatory
responses. Adv Exp Med Biol. 560:41–45. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Zandi E and Karin M: Bridging the gap:
Composition, regulation, and physiological function of the IkappaB
kinase complex. Mol Cell Biol. 19:4547–4551. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Tanner H, Mohacsi P, Fuller-Bicer GA,
Rieben R, Meier B, Hess O and Hullin R: Cytokine activation and
disease progression in patients with stable moderate chronic heart
failure. J Heart Lung Transplant. 26:622–629. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Elliott PJ, Zollner TM and Boehncke WH:
Proteasome inhibition: A new anti-inflammatory strategy. J Mol Med
(Berl). 81:235–245. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Santos DG, Resende MF, Mill JG, Mansur AJ,
Krieger JE and Pereira AC: Nuclear Factor (NF) kappaB polymorphism
is associated with heart function in patients with heart failure.
BMC Med Genet. 11:892010. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Chen FT, Yang CM and Yang CH: The
protective effects of the proteasome inhibitor bortezomib (velcade)
on ischemia-reperfusion injury in the rat retina. PLoS One.
8:e642622013. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Ma Y, Chen B, Liu D, Yang Y, Xiong Z, Zeng
J and Dong Y: MG132 treatment attenuates cardiac remodeling and
dysfunction following aortic banding in rats via the NF-κB/TGFβ1
pathway. Biochem Pharmacol. 81:1228–1236. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Zimmermann M: Ethical guidelines for
investigations of experimental pain in conscious animals. Pain.
16:109–110. 1983. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jin JL, Lv RG, Guo J, Liu XH, Liang YW,
Wei JR and Wang L: Improvement of left ventricular remodelling by
inhibition of NF-κB in a rat model of myocardial infarction. Heart
Lung Circ. 25:1007–1012. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Chen ZR, Wu XH, Luo KL, He Q and Xiang YL:
Proteasome inhibitor MG-132 improves myocadial hypertrophy after
myocardial infarction in rats. Basic Clin Med. 32:1326–1331.
2012.(In Chinese).
|
|
16
|
Snyder JG, Prewitt R, Campsen J and Britt
LD: PDTC and Mg132, inhibitors of NF-kappaB, block endotoxin
induced vasodilation of isolated rat skeletal muscle arterioles.
Shock. 17:304–307. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Lattouf R, Younes R, Lutomski D, Naaman N,
Godeau G, Senni K and Changotade S: Picrosirius red staining: A
useful tool to appraise collagen networks in normal and
pathological tissues. J Histochem Cytochem. 62:751–758. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Livak KJ and Schmittgen TD: Analysis of
relative gene expression data using real-time quantitative PCR and
the 2(-Delta Delta C(T)) method. Methods. 25:402–408. 2001.
View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Huang W, Li SN, Huang S and Xu B:
Inhibitor of ubiquitin proteasome system suppress
Calcineurin-dependent cardiomyocyte hypertrophy. Chin J
Arteriosclerosis. 22:774–778. 2014.(In Chinese).
|
|
20
|
Meiners S, Hocher B, Weller A, Laule M,
Stangl V, Guenther C, Godes M, Mrozikiewicz A, Baumann G and Stangl
K: Downregulation of matrix metalloproteinases and collagens and
suppression of cardiac fibrosis by inhibition of the proteasome.
Hypertension. 44:471–477. 2004. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Wang Y, Suo F, Liu J, Hu H, Xue M, Cheng
W, Xuan Y and Yan S: Myocardial infarction induces sympathetic
hyperinnervation via a nuclear factor-κB-dependent pathway in
rabbit hearts. Neurosci Lett. 535:128–133. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Li B, Liao YH, Cheng X, Ge H, Guo H and
Wang M: Effects of carvedilol on cardiac cytokines expression and
remodeling in rat with acute myocardial infarction. Int J Cardiol.
111:247–255. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Wójcik S, Spodnik JH, Spodnik E,
Dziewiątkowski J and Moryś J: Nigrostriatal pathway degeneration in
rats after intraperitoneal administration of proteasome inhibitor
MG-132. Folia Neuropathol. 52:41–55. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Wang Y, Sun W, Du B, Miao X, Bai Y, Xin Y,
Tan Y, Cui W, Liu B, Cui T, et al: Therapeutic effect of MG-132 on
diabetic cardiomyopathy is associated with its suppression of
proteasomal activities: Roles of Nrf2 and NF-κB. Am J Physiol Heart
Circ Physiol. 304:H567–H578. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Chen SF, Chen HY, Liu XB, Zhang YX, Liu W,
Wang WH, Zhang B and Wang LX: Apoptotic effect of MG-132 on human
tongue squamous cell carcinoma. Biomed Pharmacother. 65:322–327.
2011. View Article : Google Scholar : PubMed/NCBI
|