Introduction
Paraquat (PQ), as an electron acceptor, induces a
large number of reactive oxygen species (ROS) upon entry into the
mitochondria, thus resulting in damage to tissue cells (1,2). After
oral administration of PQ, PQ is quickly absorbed by the blood and
actively transported into cells by inverse chemical gradients of
type I and II lung cells, leading to a significant increase in the
concentration in the lung, which is 6–10 times as high as that of
the plasma concentration. Even though the plasma PQ concentration
significantly declines, it can still be maintained at a high
concentration within the lung, so the lung is its main target
organ. In addition, PQ triggers the alveolar interstitial
infiltration of a large number of inflammatory cells, which causes
acute lung injury in the early stage and results in lung fibrosis
in the advanced stage, so it is the main cause of death of
patients. Liver and kidney damage in patients can jointly lead to
multiple organ failure (3). PQ in
the blood is mainly excreted through the kidney as a prototype. The
direct toxic effects of PQ on the renal tubules can cause acute
kidney function impairment and delayed excretion of PQ (4). Maintaining the kidney function is very
important for reducing the PQ concentration in the plasma, which
can also reduce the accumulation of PQ in lung cells (5).
The lethal dose of orally administered PQ is ~20 ml,
and the mortality rate is positively related to PQ intake. The
mortality rate of patients with high-dose poisoning reaches 60–90%,
and the survival rate of patients taking >60 ml PQ is <1%.
Besides, survivors are also often companied by severe lung
fibrosis, thus seriously affecting the respiratory function of
patients (5).
The current treatment regimens for PQ are mainly
early gastric lavage, oral administration of cathartic agents, oral
administration of activated carbon and increased infusion quantity,
excretion of PQ accelerated by diuretics, early hemoperfusion, and
the applications of immunosuppressive agents and conventional
antioxidants (5–7). However, according to the actual
observation in Xiangyang First People's Hospital, Hubei University
of Medicine (Xiangyang, China) and the literature reports, the
mortality rate of patients with severe PQ poisoning is high
(5,6). At present, there is no recognized
specific treatment for high-dose PQ poisoning, including the
treatment with conventional antioxidants (5).
The mass production of ROS is the main mechanism of
PQ poisoning (1,3,8), and a
large number of cell and animal experiments have confirmed the
effectiveness of antioxidative therapy (9), but only two clinical reports have
suggested that antioxidant therapy is effective (10,11).
Observation in clinical practice and the literature analysis have
indicated that conventional antioxidant therapy does not
effectively improve the survival rate of patients. Therefore, there
is currently no consensus on the application of antioxidants as the
primary treatment method (5,6).
For a long time, the core issue ignored in the
clinical treatment for PQ poisoning is whether ROS can be
effectively cleared, which is the key to determining the success of
treatment in patients with high-dose PQ poisoning. Considering that
PQ induces ROS generation in a dose-dependent manner (12), and that antioxidants inhibit ROS in a
dose-dependent manner (12,13), antioxidants at the conventional dose
cannot effectively increase the survival rate. Therefore, it was
proposed for the first time to employ high-dose long-term
antioxidants for treating patients with severe PQ poisoning, so as
to observe changes in the patient's survival rate, lung fibrosis
and function.
Materials and methods
General data of patients
Group 1: a total of 23 hospitalized patients with PQ
poisoning in the hospital from January 2011 to May 2013 were
selected after patients with the oral dose of <20 ml were
excluded.
Group 2: a total of 6 hospitalized patients in the
hospital from June 2013 to March 2017 were selected after patients
with the oral dose of <20 ml were excluded.
The study was approved by the Ethics Committee of
Xiangyang First People's Hospital, Hubei University of Medicine.
The patients who participated in this research, signed an informed
consent and had complete clinical data.
Treatment regimens
Group 1: all patients underwent conventional
hemoperfusion, followed by continuous venovenous hemofiltration
(CVVH) and glucocorticoid treatment (methylprednisolone, 40–80
mg/day), and they received intravenously vitamin C (2 g/day) and
orally took activated carbon, so as to maintain the electrolyte
balance. Antibiotic therapy and other therapies were conducted when
patients were complicated with infection, and they received
ventilator-assisted respiration when respiratory failure occurred.
Following the acute lung injury phase, patients were given 40 mg
prednisone daily with weekly reduction of 5 mg after discharge, and
the administration was kept for 1 month after the dose was reduced
to 5 mg daily, followed by discontinuation.
Group 2: after the approval was gained from patients
and their family members, the dose of vitamin C was changed to 3 g
q.8 h (intravenous drip) on the basis of the conventional therapy,
and that of glutathione (GSH) was changed to 2.4 g q.12 h
(intravenous drip). Seven days later, the dose of vitamin C was
changed to 3 g q.12 h, and that of GSH was changed to 2.4 g q.d,
with hospital stays of 10–14 days. After discharge, patients were
orally administered with 0.6 g acetyl cysteine tablets twice a day
for a total of 3 months. Besides, 40 mg prednisone tablets were
given to patients daily, with weekly reduction of 5 mg, and the
administration was kept for 1 month after the dose was reduced to 5
mg daily, followed by discontinuation.
Before treatment, oral PQ dose, time interval from
administration to treatment, white blood cell (WBC), creatinine
(Cr), alanine aminotransferase (ALT), partial pressure of oxygen
(PaO2) and partial pressure of carbon dioxide
(PaCO2) of patients in each group were collected.
The survival rate evaluation after the end of
treatment: patients were regarded as survived if they were alive
for 6 months or longer from the date of hospitalization. The
highest Cr and ALT values of patients were taken as indicators for
liver and kidney damage. The lowest PaO2 value of
patients was seen as the indicator for acute respiratory function
impairment. Lung fibrosis was evaluated according to the chest
X-ray examination results of patients. Moreover, the lung
dysfunction of the survived patients was determined based on the
existence of chest tightness and dyspnea after physical
activities.
Statistical analysis
Statistical Product and Service Solutions (SPSS)
22.0 was applied for statistical analysis. Enumeration data are
expressed as case (n) and percentage. As the total number of
samples was <40, Fisher's exact test was used to analyze
intergroup differences. Measurement data were presented as mean ±
standard deviation, and intergroup differences were analyzed via
the independent samples t-test. P<0.05 indicates that the
difference is statistically significant.
Results
There was no significant difference in the basic
data between the two groups of patients (p>0.05) (Table I).
 | Table I.Characteristics of the two groups of
patients with PQ poisoning. |
Table I.
Characteristics of the two groups of
patients with PQ poisoning.
| Variables | Group 1 (n=23) | Group 2 (n=6) | P-value |
|---|
| Age (years) | 33.70±10.50 | 35.50±12.86 | 0.723 |
| Male | 12 (52.2%) | 2 (33.3%) | 0.651 |
| Amount of
ingested |
| PQ (ml) | 42.17±14.13 | 48.33±38.17 | 0.713 |
| Time interval
(h) | 5.26±2.14 | 5.83±2.48 | 0.576 |
The independent samples t-test was conducted for the
two groups of patients before treatment, which revealed that there
were no significant differences in WBC, PaO2,
PaCO2, ALT and Cr (p>0.05), suggesting that there are
no obvious differences in the infection index, lung, liver and
kidney function between the two groups of patients before admission
(Table II).
| Table II.Various detection indicators of the
two groups of patients before admission. |
Table II.
Various detection indicators of the
two groups of patients before admission.
| Variables | Group 1 (n=23) | Group 2 (n=6) | P-value |
|---|
| WBC
(109/l) | 10.05±2.35 | 9.55±2.60 | 0.651 |
| PaO2
(mmHg) | 95.57±5.35 | 96.33±6.25 | 0.764 |
| PaCO2
(mmHg) | 39.09±3.09 | 38.83±2.64 | 0.856 |
| ALT (U/l) | 37.04±4.43 | 37.50±2.81 | 0.813 |
| Cr (mg/dl) | 1.10±0.20 | 1.06±0.20 | 0.608 |
Fisher's exact test demonstrated that the survival
rate of group 1 was lower than that of group 2, and the difference
was statistically significant (p<0.05), indicating that the
high-dose long-term antioxidant therapy significantly improves the
patient's survival rate (Table
III).
| Table III.Analysis of the mortality rate of the
two groups of patients. |
Table III.
Analysis of the mortality rate of the
two groups of patients.
| Groups | Death (n, %) | Survival (n,
%) | P-value |
|---|
| Group 1 | 17 (73.9) | 6 (26.1) | 0.002 |
| Group 2 | 0 (0.0) | 6 (100.0) |
|
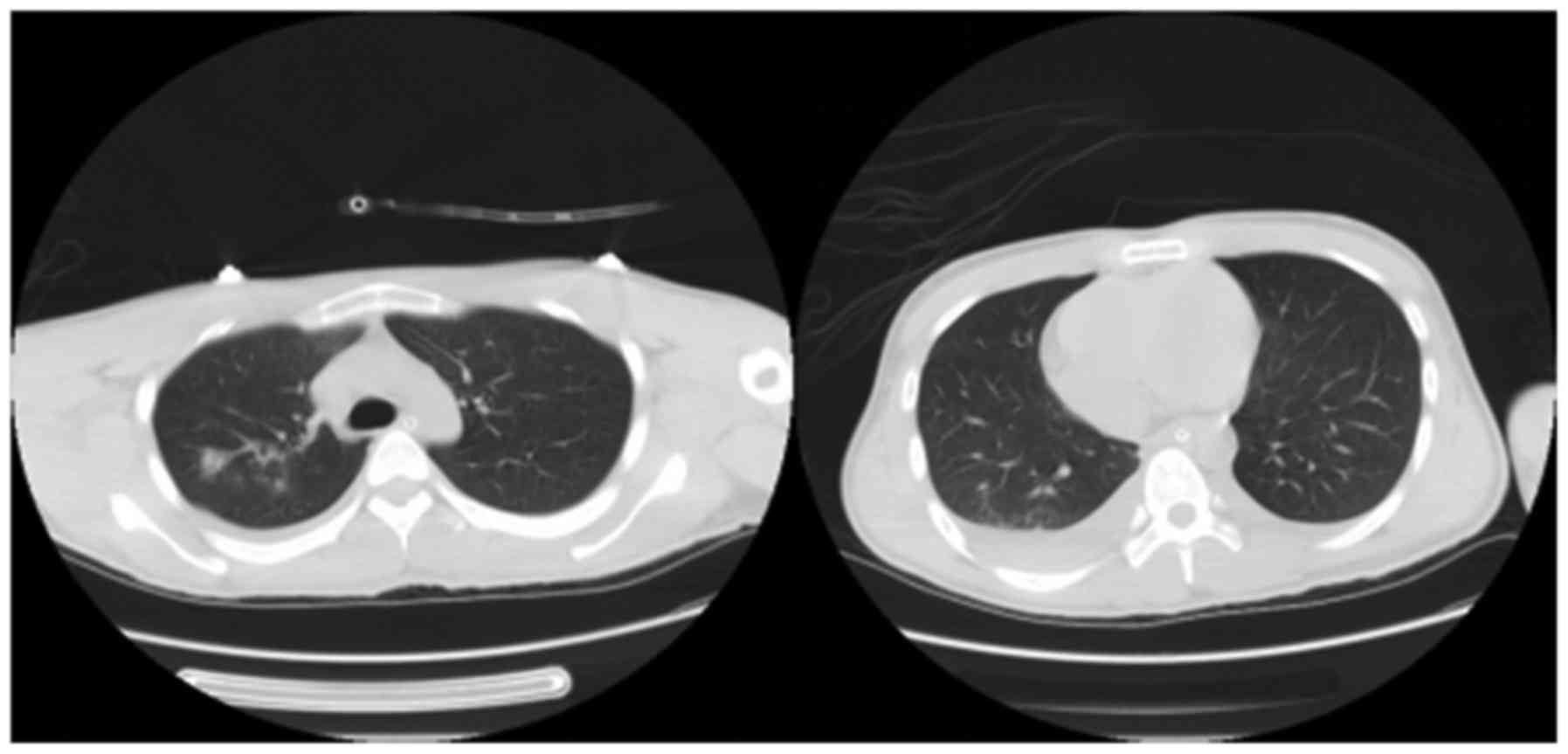
According to Fisher's exact test, there was no
significant difference in the incidence rate of lung fibrosis among
the survivors in either group (p>0.05). However, 6 patients in
group 1 died of respiratory failure due to severe lung fibrosis
while there was no patient with severe lung fibrosis in group 2,
suggesting that high-dose long-term antioxidants effectively reduce
lung fibrosis in patients (Table
IV, Figs. 1 and 2).
| Table IV.Analysis of the difference in the
incidence rate of lung fibrosis between the two groups of
patients. |
Table IV.
Analysis of the difference in the
incidence rate of lung fibrosis between the two groups of
patients.
|
| Lung fibrosis (n,
%) |
|
|---|
|
|
|
|
|---|
| Groups | No | Yes | P-value |
|---|
| Group 1 | 0 (0.0) | 6 (100.0) | 0.182 |
| Group 2 | 3 (50.0) | 3 (50.0) |
|
The results manifested that after the independent
samples t-test, there was no statistically significant difference
in the highest Cr value between the two groups of patients before
and after treatment (p>0.05). The paired sample t-test
illustrated that in group 1, Cr value after treatment was higher
than that before treatment, and the difference was statistically
significant (p<0.05), suggesting that severe PQ poisoning
remarkably impairs kidney function of patients, but not revealing
that long-term high-dose antioxidant therapy can protect the
patient's kidney function (Table
V).
| Table V.Analyses of Cr value of the two
groups of patients before and after treatment. |
Table V.
Analyses of Cr value of the two
groups of patients before and after treatment.
| Variables | Cr value before
treatment (mg/dl) | Cr value after
treatment (mg/dl) | P-value |
|---|
| Group 1 | 1.10±0.20 | 2.95±1.85 | <0.001 |
| Group 2 | 1.06±0.20 | 1.86±0.75 | 0.061 |
| P-value | 0.608 | 0.173 |
|
Based on the results, the independent samples t-test
demonstrated that there was no significant difference in
preoperative ALT between the two groups (p>0.05). After
treatment, ALT in group 1 was higher than that in group 2, with
statistically significant difference (p<0.05). The paired sample
t-test manifested that in group 1, ALT after treatment was higher
than that before treatment, showing a statistically significant
difference (p<0.05), which suggested that severe PQ poisoning
obviously damages liver function of patients, and the high-dose
long-term antioxidant therapy can protect liver function of
patients (Table VI).
| Table VI.Analyses of ALT of the two groups of
patients before and after treatment. |
Table VI.
Analyses of ALT of the two groups of
patients before and after treatment.
| Variables | ALT before
treatment (U/l) | ALT after treatment
(U/l) | P-value |
|---|
| Group 1 | 37.04±4.43 | 216.74±126.23 | <0.001 |
| Group 2 | 37.50±2.81 | 52.50±24.83 | 0.189 |
| P-value | 0.813 | <0.001 |
|
On the basis of the results, the independent samples
t-test showed that there was no statistically significant
difference in PaO2 between the two groups before
treatment (p>0.05). After treatment, PaO2 in group 1
was lower than that in group 2, with a statistically significant
difference (p<0.05). The paired sample t-test illustrated that
in group 1, PaO2 after treatment was lower than that
before treatment, and the difference was statistically significant
(p<0.05), manifesting that severe PQ poisoning significantly
impairs lung function of patients, and the high-dose long-term
antioxidant therapy can protect lung function of patients in the
acute phase (Table VII).
| Table VII.Analyses of PaO2 of the
two groups of patients during hospitalization before and after
treatment. |
Table VII.
Analyses of PaO2 of the
two groups of patients during hospitalization before and after
treatment.
| Variables | PaO2
before treatment (mmHg) | PaO2
after treatment (mmHg) | P-value |
|---|
| Group 1 | 95.57±5.35 | 70.26±16.38 | <0.001 |
| Group 2 | 96.33±6.25 | 91.17±3.43 | 0.230 |
| P-value | 0.764 | <0.001 |
|
Fisher's exact test revealed that the incidence rate
of lung dysfunction in group 1 was higher than that in group 2, and
the difference was statistically significant (p<0.05),
indicating that the high-dose long-term antioxidant therapy can
prevent lung dysfunction in survivors (Table VIII).
| Table VIII.Analysis of the difference in the
incidence rate of lung dysfunction between the two groups of
patients. |
Table VIII.
Analysis of the difference in the
incidence rate of lung dysfunction between the two groups of
patients.
| Groups | No incidence of
lung dysfunction (n, %) | Incidence of lung
dysfunction (n, %) | P-value |
|---|
| Group 1 | 1 (16.7) | 5 (83.3) | 0.015 |
| Group 2 | 6 (100.0) | 0 (0.0) |
|
Discussion
The mortality rate of patients with severe PQ
poisoning is extremely high, and there is currently no specific
treatment for it. Clinical treatments mainly include
immunosuppressive agents and early hemoperfusion, and the lung
transplantation in the later period can increase the survival rate
of patients to a limited degree (6,7).
Efficient clearance of ROS is the core of the
treatment for high-dose PQ poisoning, but few clinical papers
discuss how to effectively clear ROS. In this study, high-dose
long-term antioxidants successfully saved the life of all patients
in group 2, and effectively relieved the patient's lung fibrosis
and dysfunction in the advanced stage, in which its maximum oral
dose reached 120 ml.
Main mechanism of PQ poisoning
PQ induces ROS mass production through
mitochondria
PQ produces only a small amount of ROS if not
ingested by mitochondria, whereas ROS produced by PQ ingested by
mitochondria is significantly increased (2). After PQ enters mitochondria,
PQ2+ gains electrons [originated from nicotinamide
adenine dinucleotide phosphate oxidase (NADPH)] from the complex I
at the electron transport chain (ETC), and then PQ2+ is
reduced to a monovalent PQ+, which transfers electrons
to O2 to form ROS, and is oxidized to PQ2+,
thus forming a redox cycle that produces large amounts of ROS [such
as superoxide radicals (O2−), hydrogen
peroxide (H2O2), and hydroxyl radicals
(−OH)] (1). However,
literature has also revealed that complex III is the site of
PQ2+ producing mass ROS (2). Therefore, regardless of the site of
production, PQ2+ largely plucks electrons from the ETC
through the redox cycle and delivers it to oxygen to form ROS,
which is the primary mechanism of PQ poisoning.
PQ destroys mitochondrial
deoxyribonucleic acid (mtDNA) and ETC, resulting in secondary ROS
increase
ROS can destroy cell proteins, DNA, cell membranes
and other macromolecular substances, leading to cell death
(9,14). ETC in mitochondria is very sensitive
to ROS and is easily damaged by ROS (15). PQ can lead to a significant reduction
of mitochondrial respiratory chain complex in the lung, liver,
kidney and brain tissues (15). A
large number of basic studies have shown that the ETC injury,
especially the complex I injury, will lead to a large number of
electronic leaks to form ROS (16).
PQ induces mtDNA and nuclear DNA (nDNA) oxidative damage (17). mtDNA encodes 13 of the 113 subunits
of ETC, and oxidative damage to mtDNA leads to insufficient
secondary synthesis of ETC (18).
8-Oxoguanine glycosylase 1 (OGG1) is a DNA repair enzyme that
maintains the integrity of mtDNA and reduces ROS generation.
However, OGG1 knockdown results in a significant increase in ROS,
suggesting that mtDNA injury will further increase ROS generation
(19).
ROS induces the production of
inflammatory cytokines in large quantities
Another notable feature of PQ poisoning is the large
increases of inflammatory cytokines and cells in the lung (3,6). ROS is
the most important signal molecule inducing inflammation. ROS
induces nuclear factor of κ light polypeptide gene enhancer in B
cell inhibitor α (IκB-α) phosphorylation, so as to lead to
dissociation of nuclear factor κ-light-chain-enhancer of activated
B cell-IκB-α (NF-κB-IκB-α) complex. Then, NF-κB translocates into
the nucleus and binds to κB transcription factor, thus inducing the
expression of various inflammatory cytokines [such as tumor
necrosis factor-α (TNF-α), interleukin-6 (IL-6), IL-8, and
transforming growth factor-β (TGF-β)] (3,20–22), and
the inflammatory cytokine TNF can also promote the destruction of
alveolar epithelial mitochondrial I, resulting in the production of
ROS and the formation of a vicious circle (23). At the same time, ROS destroys the
vascular epithelial cells and leads to the destruction of the
intercellular junctions. Inflammatory cytokines induce inflammatory
cells to enter the lung through the gap between the two vascular
endothelia.
In summary, PQ induces a large number of
inflammatory cytokines by inducing ROS generation, thus leading to
apoptosis or necrosis of the lung epithelial cells in patients
(9,14), resulting in acute lung injury with
multiple organ damage to such as the liver and kidney (17,24), and
triggering lung fibrosis in the later period, which is the main
mechanism of PQ poisoning (3).
The role of antioxidants and confusion in clinical
applications. Antioxidants directly combat ROS-induced cellular
damage. A large number of cell and animal experiments have shown
that antioxidants can reduce PQ-induced ROS generation, reduce cell
death and protect the lung, liver and kidney function of patients
(11,17). The mortality rate of patients is
mainly positively related to the patient's oral dose, and those who
take >60 ml PQ almost never survive (5). The most important reason is that PQ
induces ROS generation in a dose-dependent manner (12), and similarly, the effect of
antioxidants is dose-dependent. High-dose antioxidants can
effectively inhibit ROS generation (13).
Antioxidants restore the function of
mtDNA, ETC and mitochondria
Loss of mtDNA and damage to ETC are important
sources of ROS generation (16).
Mitochondrial GSH level is an important factor for maintaining the
integrity of mtDNA. Antioxidants can reduce the formation of
8-hydroxy-2′-deoxyguanosine (8-OHdG), a DNA oxidative product, and
restore the integrity of mtDNA (17). In addition, N-acetylcysteine
(NAC) can restore the integrity of ETC with oxidative damage
(25), thereby reducing ROS
regeneration.
Antioxidants reduce the formation of
inflammatory cytokines, inhibit the destruction of inflammatory
cytokines to cells, and play an anti-lung fibrosis role
ROS, as an intracellular signaling molecule, induces
the mass production of inflammatory cytokines, in which the mass
production of TGF-β is the main pathogenesis of lung fibrosis
(20,22). Inflammatory cytokines, such as TNF-α,
induce cell death primarily through the induction of intracellular
ROS generation, whereas antioxidants reduce TNF-α-induced cell
death (26). Antioxidants can
remarkably reduce the generation of various inflammatory cytokines,
while reducing that of TGF-β (20).
Therefore, in theory, antioxidative therapy is the
core of the treatment for the disease, but the current
antioxidative therapy is not regarded as the main treatment, and
the patient's mortality rate is high (5,6,27). There are few clinical reports on
high-dose vitamin C treatment for PQ poisoning, but it can
effectively protect kidney function and reduce the mortality rate
(10,11). Therefore, it is hypothesized that
antioxidants at the conventional dosage cannot clear all ROS, which
is the major cause of high mortality rate of patients.
Test results suggest that the high-dose long-term
antioxidant therapy brings a good clinical effect. High-dose
vitamin C (maximum dose of 3 g, 3 times daily) and GSH (50 mg/kg,
once daily) can effectively reduce the oxidant level in the body
(11,28) and increase the patient's survival
rate (10). Therefore, the aim of
high-dose long-term antioxidant lies in effectively preventing the
damaging effect of ROS on tissues, thereby increasing the patient's
survival rate.
In the past, it was believed that the removal of
large amounts of ROS was difficult to be achieved, so there is no
report on the application of high-dose long-term antioxidants in
the treatment of severe PQ poisoning (5).
The experimental results suggested that the
high-dose long-term antioxidant therapy can effectively improve the
patient's survival rate and reverse liver function impairment
(24).
After patients get through the acute lung injury
phase, another important issue is lung fibrosis (3,20).
Recent studies have shown that the increase of TGF-β triggered by
abnormal ROS in the lung is still the main factor for lung fibrosis
(20,21). mtDNA damage is an important molecular
change of lung fibrosis (29). Early
application of NAC can prevent the formation of lung fibrosis
(30). Moreover, high-dose long-term
antioxidant therapy can obviously reduce lung fibrosis in patients
and improve lung function, suggesting that this therapy can
effectively reduce the generation of the inflammatory cytokine
TGF-β in the lung, which is the most important factor for
preventing lung fibrosis and enhancing lung function.
Conventional glucocorticoids resistant to lung
fibrosis are considered as the main treatment option, but its
actual effect is not good. High-dose glucocorticoids or cytotoxic
drugs can also effectively improve the patient's survival rate and
prevent lung fibrosis, but they cause serious side-effects such as
increased infection, bone marrow suppression and osteoporosis that
limit their clinical application (27).
In conclusion, the main pathogenesis of PQ poisoning
is the induction of ROS and the mass production of inflammatory
cytokines. Acute lung injury in patients and lung fibrosis in the
later period are the main causes of death of patients. To the best
of our knowledge, it is proposed in this study for the first time
that the high-dose long-term antioxidant therapy is a specific
treatment for serious PQ poisoning. The results evidenced that this
therapy significantly improved the patient's survival rate,
prevented lung fibrosis in the advanced stage, and improved lung
and liver function of patients. It is hoped that more clinical
studies will continue to validate the clinical efficacy of this
therapy.
Acknowledgements
Not applicable.
Funding
No funding was received.
Availability of data and materials
The datasets used and/or analyzed during the present
study are available from the corresponding author on reasonable
request.
Authors' contributions
SH and CQ conceived and designed the experiments.
SH, JZ, ML and JY performed the experiments. JZ, HM and JW analyzed
the data. SH, JZ, CQ, ZY, ML, JY, HM and JW contributed to
providing reagents, materials and analysis tools. SH, ML and SX
wrote the manuscript. CQ and ZY revised and finalized the
manuscript. ZY and SX were also involved in the conception and
design of the study. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The study was approved by the Ethics Committee of
Xiangyang First People's Hospital, Hubei University of Medicine
(Xiangyang, China). The patients who participated in this research,
signed an informed consent and had complete clinical data.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Cochemé HM and Murphy MP: Complex I is the
major site of mitochondrial superoxide production by paraquat. J
Biol Chem. 283:1786–1798. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
2
|
Castello PR, Drechsel DA and Patel M:
Mitochondria are a major source of paraquat-induced reactive oxygen
species production in the brain. J Biol Chem. 282:14186–14193.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Dinis-Oliveira RJ, Duarte JA,
Sánchez-Navarro A, Remião F, Bastos ML and Carvalho F: Paraquat
poisonings: Mechanisms of lung toxicity, clinical features, and
treatment. Crit Rev Toxicol. 38:13–71. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Weng CH, Chen HH, Hu CC, Huang WH, Hsu CW,
Fu JF, Lin WR, Wang IK and Yen TH: Predictors of acute kidney
injury after paraquat intoxication. Oncotarget. 8:51345–51354.
2017. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Gil HW, Hong JR, Jang SH and Hong SY:
Diagnostic and therapeutic approach for acute paraquat
intoxication. J Korean Med Sci. 29:1441–1449. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Gawarammana IB and Buckley NA: Medical
management of paraquat ingestion. Br J Clin Pharmacol. 72:745–757.
2011. View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Hsu CW, Lin JL, Lin-Tan DT, Chen KH, Yen
TH, Wu MS and Lin SC: Early hemoperfusion may improve survival of
severely paraquat-poisoned patients. PLoS One. 7:e483972012.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Bonilla E, Medina-Leendertz S, Villalobos
V, Molero L and Bohórquez A: Paraquat-induced oxidative stress in
drosophila melanogaster Effects of melatonin, glutathione,
serotonin, minocycline, lipoic acid and ascorbic acid. Neurochem
Res. 31:1425–1432. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Cappelletti G, Maggioni MG and Maci R:
Apoptosis in human lung epithelial cells: Triggering by paraquat
and modulation by antioxidants. Cell Biol Int. 22:671–678. 1998.
View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Moon JM and Chun BJ: The efficacy of high
doses of vitamin C in patients with paraquat poisoning. Hum Exp
Toxicol. 30:844–850. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Hong SY, Hwang KY, Lee EY, Eun SW, Cho SR,
Han CS, Park YH and Chang SK: Effect of vitamin C on plasma total
antioxidant status in patients with paraquat intoxication. Toxicol
Lett. 126:51–59. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Hong SY, Yang JO, Lee EY and Lee ZW:
Effects of N-acetyl-L-cysteine and glutathione on antioxidant
status of human serum and 3T3 fibroblasts. J Korean Med Sci.
18:649–654. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Hong SY, Gil HW, Yang JO, Lee EY, Kim HK,
Kim SH, Chung YH, Hwang SK and Lee ZW: Pharmacokinetics of
glutathione and its metabolites in normal subjects. J Korean Med
Sci. 20:721–726. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Jang YJ, Won JH, Back MJ, Fu Z, Jang JM,
Ha HC, Hong S, Chang M and Kim DK: Paraquat induces apoptosis
through a mitochondria-dependent pathway in RAW264.7 cells. Biomol
Ther (Seoul). 23:407–413. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Musatov A and Robinson NC: Susceptibility
of mitochondrial electron-transport complexes to oxidative damage.
Focus on cytochrome c oxidase. Free Radic Res. 46:1313–1326.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Indo HP, Davidson M, Yen HC, Suenaga S,
Tomita K, Nishii T, Higuchi M, Koga Y, Ozawa T and Majima HJ:
Evidence of ROS generation by mitochondria in cells with impaired
electron transport chain and mitochondrial DNA damage.
Mitochondrion. 7:106–118. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Ortiz MS, Forti KM, Suárez Martinez EB,
Muñoz LG, Husain K and Muñiz WH: Effects of antioxidant
N-acetylcysteine against paraquat-induced oxidative stress
in vital tissues of mice. Int J Sci Basic Appl Res. 26:26–46.
2016.PubMed/NCBI
|
|
18
|
Płoszaj T, Robaszkiewicz A and Witas H:
Oxidative damage of mitochondrial DNA: The result or consequence of
enhanced generation of reactive oxygen species. Postepy Biochem.
56:139–146. 2010.(In Polish). PubMed/NCBI
|
|
19
|
Bacsi A, Chodaczek G, Hazra TK, Konkel D
and Boldogh I: Increased ROS generation in subsets of OGG1 knockout
fibroblast cells. Mech Ageing Dev. 128:637–649. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Liu RM and Gaston Pravia KA: Oxidative
stress and glutathione in TGF-beta-mediated fibrogenesis. Free
Radic Biol Med. 48:1–15. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Cheresh P, Kim SJ, Tulasiram S and Kamp
DW: Oxidative stress and pulmonary fibrosis. Biochim Biophys Acta.
1832:1028–1040. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Mittal M, Siddiqui MR, Tran K, Reddy SP
and Malik AB: Reactive oxygen species in inflammation and tissue
injury. Antioxid Redox Signal. 20:1126–1167. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Mariappan N, Elks CM, Fink B and Francis
J: TNF-induced mitochondrial damage: A link between mitochondrial
complex I activity and left ventricular dysfunction. Free Radic
Biol Med. 46:462–470. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Awadalla EA: Efficacy of vitamin C against
liver and kidney damage induced by paraquat toxicity. Exp Toxicol
Pathol. 64:431–434. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Boer LA, Panatto JP, Fagundes DA, Bassani
C, Jeremias IC, Daufenbach JF, Rezin GT, Constantino L, Dal-Pizzol
F and Streck EL: Inhibition of mitochondrial respiratory chain in
the brain of rats after hepatic failure induced by carbon
tetrachloride is reversed by antioxidants. Brain Res Bull.
80:75–78. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Kamata H, Honda S, Maeda S, Chang L,
Hirata H and Karin M: Reactive oxygen species promote
TNFalpha-induced death and sustained JNK activation by inhibiting
MAP kinase phosphatases. Cell. 120:649–661. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
He F, Xu P, Zhang J, Zhang Q, Gu S, Liu Y
and Wang J: Efficacy and safety of pulse immunosuppressive therapy
with glucocorticoid and cyclophosphamide in patients with paraquat
poisoning: A meta-analysis. Int Immunopharmacol. 27:1–7. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kim JH, Gil HW, Yang JO, Lee EY and Hong
SY: Effect of glutathione administration on serum levels of
reactive oxygen metabolites in patients with paraquat intoxication:
A pilot study. Korean J Intern Med (Korean Assoc Intern Med).
25:282–287. 2010.
|
|
29
|
Kim SJ, Cheresh P, Jablonski RP, Williams
DB and Kamp DW: The role of mitochondrial DNA in mediating alveolar
epithelial cell apoptosis and pulmonary fibrosis. Int J Mol Sci.
16:21486–21519. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Yu WC, Tian LY and Cheng W: Efficacy study
of edaravone and acetylcysteine towards bleomycin-induced rat
pulmonary fibrosis. Int J Clin Exp Med. 8:8730–8739.
2015.PubMed/NCBI
|