Moyamoya disease (MMD) is a type of chronic
occlusive cerebrovascular disease. The pathogenetic mechanisms
remain to be fully elucidated. Its major characteristic is a
steno-occlusive change at the end of the internal carotid artery
(ICA), middle cerebral artery (MCA) and/or proximal anterior
cerebral artery (ACA), which is accompanied by the formation of
smoke-like abnormal blood vessels in the base of the skull in
digital subtraction angiography (DSA). In 1957, Takeuchi and
Shimizu described the pathological manifestation of MMD for the
first time for bilateral hypoplasia of the ICA (1). Cerebral angiography in such patients
reveals smog-like blood vessels in the skull base, which was
officially named MMD by Suzuki and Takaku (2) in 1969. The incidence of MMD is high in
East Asian populations but low in European and North American
populations (3). The clinical signs
of MMD mainly include two types: Cerebral ischemia and cerebral
hemorrhage. These two types of symptom differ in their distribution
between pediatric and adult patients. Most of the pediatric
patients present with progressive cerebral ischemia, including
transient cerebral ischemic attacks and cerebral infarctions.
Mental decline or seizures may be the first symptom in children. In
half of the cases in adults, intracranial hemorrhage is the first
symptom, while ischemic symptoms first occur in the other half
(3). In recent years, large amounts
of research on the diagnosis and treatment of MMD have been
performed in China, Japan and South Korea. The present article
provides a review of the relevant domestic and international
literature for the following aspects of MMD: Diagnosis, clinical
symptoms, epidemiology, genetics, radiographic evaluation,
pathology and treatment methods.
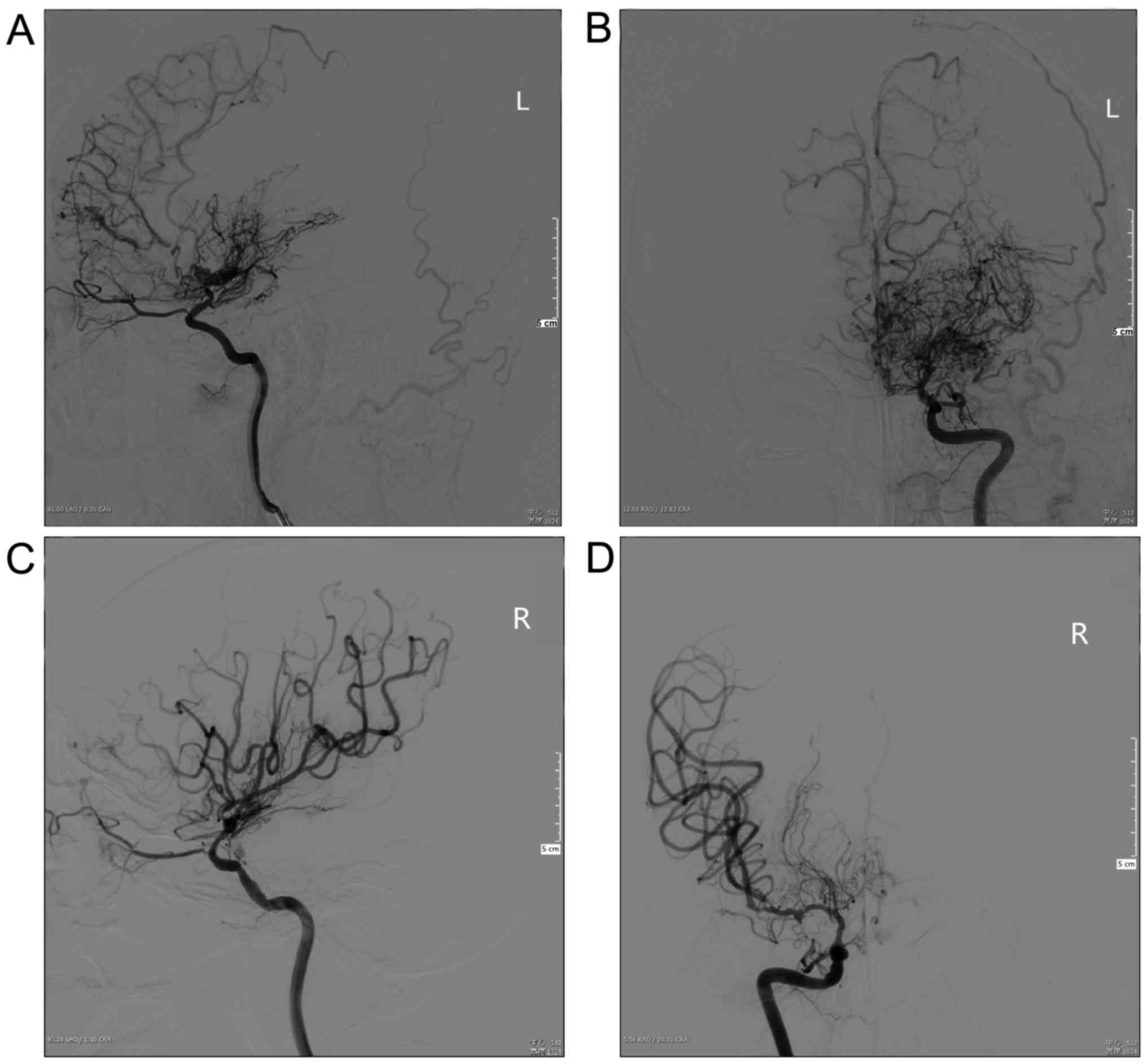
In 1996, Japan issued a guide for the diagnosis and
treatment of the spontaneous occlusion of the circle of Willis
(‘Moyamoya’ disease, MMD) (4), which
suggests the following manifestations on cerebral angiography i)
Stenosis or occlusion at the end of the carotid artery, the
proximal ACA and/or MCA; ii) an abnormal vascular network in the
vicinity of stenotic occlusion lesions in the arterial phase; and
iii) the above manifestations are bilateral (Fig. 1). In 2012, the latest guidelines for
the pathology and treatment of MMD on the basis of the 1997
guidelines were published in Japan; the 1997 diagnostic criteria
were revised in these novel guidelines (5). In the 2012 guidelines, cerebral
angiography remains the gold standard for the diagnosis of MMD with
the staging performed according to angiographic findings (Table I). The novel guidelines added a
staging based on scores of magnetic resonance (MR) angiography
(MRA) and the diagnostic criteria are as follows: i) Stenosis or
occlusion at the end of ICA and/or the initial segment of the ACA
and/or MCA. ii) At least two obvious shadows of the blood flow are
displayed on the same scan level at the basal ganglia region,
suggesting the existence of an abnormal vascular network. iii) The
above manifestations are bilateral, but bilateral lesions may be
staged differently (Table II). In
the evaluation system, the MRA results are simply scored and
totaled. A total score of 0–1 represents stage 1, which indicates
DSA I and II; a score of 2–4 represents stage 2, which indicates
DSA III; a score of 5–7 represents stage 3, which indicates DSA IV;
and a score of 8–10 represents stage 4, which indicates DSA V and
VI.
According to the new guidelines, differential
diagnoses of MMD, which should be excluded, are the following
underlying cerebrovascular diseases: Atherosclerosis, autoimmune
diseases, meningitis, brain tumors, Down syndrome, Recklinghausen's
disease, head injury and cerebrovascular damage after head
irradiation. Recently, a Chinese experts' consensus on the
diagnosis and treatment of MMD and MM syndrome (MMS) was published
(6), which argues that the
identification of MMD and MMS lacks molecular markers or other
characteristic objective indicators. Instead, the identification of
MMS and MMD diagnoses mainly depends on morphological
characteristics and the exclusion of other diseases in which one of
the main symptoms is the presents of smoke-like abnormal blood
vessels, which is not feasible to perform in the clinic. In most
cases, there is no significant difference in principles of
treatment between MMD and MMS. For the diagnosis and treatment
options for patients with suspected MMS, it is possible to refer to
the guidelines for MMD.
The clinical symptoms of MMD include transient
ischemic attacks, ischemic stroke, hemorrhagic stroke, epilepsy,
headache and cognitive dysfunction, with the incidence of each
symptom varying depending on the age of the patient (5). MMD has two major symptoms: Cerebral
ischemia and cerebral hemorrhage. Most pediatric patients with MMD
are characterized by progressive cerebral ischemic symptoms,
including transient ischemic attack and cerebral infarction, mental
decline, seizures and involuntary movements. About half of all
adult patients present with intracranial hemorrhage, and the other
half with ischemic symptoms (3). In
adult patients aged >40 years, the hemorrhagic type is more
common than the ischemic type. The most common symptom for patients
with ischemic MMD is dyskinesia, and an impaired consciousness is
the most common symptom for those with hemorrhagic MMD (7). For each of the two types of MMD,
cerebral ischemia or cerebral hemorrhage is often recurrent, but
these two signs rarely occur in the same type of patient with MMD.
Cerebral ischemia and transient ischemic attack are common in North
American and European patients, while Asian patients often suffer
from intracranial hemorrhage as the first symptom (5,8–11). However, according to certain experts,
MMD is mainly ischemic in China (12).
Among pediatric patients (under 14 years old) with
MMD, ~20% suffer from headache. Seol et al (13) reported that 44 of 204 (21.6%)
pediatric patients with MMD complained of headaches. At present, it
is thought that headache may occur due to the reduction of cerebral
blood flow or cerebral blood flow reserve and diffusive cortical
inhibition. Headache symptoms may be relieved by improving cerebral
vascular perfusion (14).
The incidence of MMD exhibits significant regional
differences, with a high incidence in East Asia and a low incidence
in other regions. According to previous studies, the prevalence of
MMD is 10.5/100,000 individuals and the incidence rate is
0.94/100,000 individuals in Japan (15); in South Korea, the prevalence rate is
16.1/100,000 and the incidence rate is 2.3/100,000 individuals
(16). The incidence of MMD was as
low as 0.09/100,000 individuals in other regions, including North
America, but it has exhibited an upward trend in the US (17). In Nanjing (China), the prevalence of
MMD in the time frame of 2000–2007 was 3.92/100,000 (18). According to the most recent study,
2,430 cases of MMD have been reported in China since 1976 (12).
Worldwide, the age of onset of MMD is significantly
bimodal in distribution, with a bimodal peak consisting of a major
peak in the first decade of life and a moderate peak in the late 20
to 30s (4–6,12,15–19).
Of note, geographic differences in sex distribution have been
observed. In foreign populations, the incidence of MMD in females
was reported to be higher than that in males with the
male-to-female ratio ranging from 1:1.8 to 1:2.2 (5,15–17);
however, the sex ratio is 1:1 in China (12,18,19).
MMD has been reported to have an increased
prevalence in certain ethnicities and pedigrees (20), suggesting that genetic factors may be
involved. Numerous studies have indicated that genetic factors have
an important role in the pathogenesis of MMD (21–23). In
2011, a whole genome-wide association study (GWAS) on 72 patients
with MMD by Kamada et al (24) identified a novel susceptibility gene,
Ringin Protein 213 (RNF213), and indicated that this gene is highly
associated with familial MMD. In the same year, Liu et al
(25) also demonstrated the genetic
susceptibility of RNF213 in patients with MMD in a GWAS on 8 MMD
families. Subsequent studies have indicated that the presence of a
low-frequency variation of RNF213 (c.14576G>A, p.R4810K)
significantly increases the risk of MMD in Asian populations
(26–28). RND213 p.R4810K mutations are divided
into homozygous and heterozygous mutations; MMD patients with a
homozygous mutation are characterized by an earlier onset, more
severe symptoms and a worse prognosis. A study by Kim et al
(29) on a Korean population
revealed that in MMD patients with a RNF213 p.R4810K homozygous
mutation, the age was <5 years, the disease mainly manifested as
cerebral infarction and patients exhibited cognitive dysfunction.
To date, RNF213 p.R4810K mutations have not been detected in
European patients with MMD, but certain rare variants of RNF213
have been identified (28,30,31).
According to the most recent study, RNF213 mutations other than
p.R4810K have an important role in Caucasians with MMD (32).
Domestic genetic studies on MMD have been performed
in succession. In a study by Li et al (33) from 2010, 208 cases of Han Chinese
subjects with MMD and 224 control subjects were assessed, revealing
that a polymorphism of the 1,171 locus of the matrix
metalloproteinase-3 gene was closely associated with MMD. In 2012,
Wu et al (26) reported that
in a population of 170 Han Chinese patients with MMD and 507
control subjects, a single-nucleotide polymorphism of the R4810K
locus of the RNF213 gene was associated with a significantly
increased risk of MMD, while that in another locus, A4399T, may be
associated with hemorrhagic MMD.
Cerebral angiography is the gold standard for
diagnosing MMD and assessing its progression. The system most
widely used for its evaluation is the Suzuki staging system
(2), in which the cerebral
angiographic findings of MMD patients are divided into 6 stages
(Table I). This staging system is
based on the progression degree of smog-like blood vessels
(34), and suggests that, in cases
of stenotic-occlusive changes in the carotid artery system of MMD
patients, a compensation of the intra-cranial cycle exists in the
extracranial arterial system (35).
In 2002, Mugikura et al (36)
proposed a new staging system, which is a revised version of the
Suzuki staging system, where re-staging is performed according to
the severity of stenosis or occlusion in the MCA and the proximal
ACA on cerebral angiography and the angiographic extent of their
branches (Table III). The Suzuki
staging system and the improved version by Mugikura et al
(36) are used for staging of MMD
according to the performance of the internal carotid artery. The
same group has also proposed a classification involving the
vertebral basilar artery in childhood MMD (37).
Brain MR imaging (MRI) is able to display the brain
parenchymal lesions associated with MMD, and MRA is able to reveal
abnormalities consistent with cerebral angiography. In 2005, Houkin
et al (38) established a
scoring system based on the degree of lesions of the ICA, ACA, MCA
and posterior cerebral artery on MRA and claimed that this system
was as suitable as the Suzuki staging system. This MRA scoring
system was added to the 2012 Guidelines for the Diagnosis and
Treatment of MMD in Japan (5). Ryoo
et al (39) reported that
high-resolution nuclear MRI is able to effectively distinguish
between MMD and atherosclerosis based on differences in cerebral
blood vessels.
Assessment of cerebral hemodynamics and the brain
metabolism level is also an important part of the imaging
assessment of patients with MMD. This assessment provides a more
objective and realistic indicator for the selection and efficacy
assessment of surgery regimens for MMD. In the current assessment
of brain metabolism, positron emission tomography (PET) and
single-photon emission computed tomography may be employed for
detection. For the assessment of cerebral hemodynamics, computed
tomography perfusion imaging and MR perfusion-weighted imaging may
be applied (40–45).
The basic pathology of MMD mainly includes intimal
fibrous hyperplasia of the intracranial arterial stenosis,
irregular proliferation of the inner elastic layer, thinning of the
middle layer of the vessel wall and reduction of the outer diameter
of the blood vessel (3,46). A high-resolution MRI cohort study
indicated that most patients with MMD had a contractile remodeling
at the distal end of the ICA and a long concentric enhancement
(39). This result is consistent
with the thickening of the arterial intima and the thinning of the
tunica media detected by vascular pathology (47).
Growing evidence supports the notion that MMD is
essentially a vascular intimal hyperplastic disease.
Histopathological analysis of the distal carotid artery indicated
that the hyperplasia occurs in arterial wall smooth muscle cells
and endothelial cells (48), and
that the endometrial thickening caused by fibrous cell hyperplasia
of the arterial intima is the cause of arterial stenosis and
occlusion (3). Guo et al
(49) reported that arterial
stenosis and occlusion of familial MMD may be due to smooth muscle
tissue hyperplasia associated with a mutation in the actin, α2,
smooth muscle, aorta gene. Endothelial progenitor cells (EPCs) have
an important role in maintaining blood flow in the infarct region
of patients with ischemic stroke (50). Kim et al (51) reported that the angiogenic function
of EPCs in patients with MMD is defective, which may be the cause
of abnormal angiogenesis in patients with MMD. Lee et al
(52) indicated that the expression
of retinaldehyde dehydrogenase 2 was epigenetically inhibited in
endothelial colony-forming cells (ECFCs) from patients with MMD,
which may have a key role in the functional impairment of
ECFCs.
Increased levels of multiple autoimmune antibodies
in patients with MMD suggest that the immune response may be
involved in the pathogenesis of MMD. Kim et al (53) identified that the levels of thyroid
auto-antibodies were elevated in numerous patients with MMD. Sigdel
et al (54) used protein chip
technology to assess patients with MMD and identified a variety of
auto-antibodies associated with MMD. In addition, numerous studies
have indicated that multiple cytokines, including vascular
endothelial growth factor, basic fibroblast growth factor,
hepatocyte growth factor, cellular retinoic acid binding protein 1
and granulocyte-colony-stimulating factor, were present in the
plasma, cerebrospinal fluid, dura mater, as well as arachnoid and
superficial temporal artery of patients with MMD (46,55–58).
Furthermore, chronic arterial inflammation caused by immune
responses has been recognized as an important driver of the
progression of MMD (54). However,
the molecular mechanisms underlying the involvement of the immune
response in MMD have remained to be fully elucidated.
At present, no evidence suggesting that drug
treatment is able to delay or even reverse the progression of MMD
is available. The current drug treatment for in MMD only targets
its clinical symptoms, including ischemia and hemorrhage, by
exerting anti-coagulant or hemostatic effects. The Japanese
guidelines from 2012 recommend the use of anti-platelet aggregation
drugs for the treatment of ischemic MMD (5), but the risk of bleeding remains.
Regarding the occurrence of ischemic stroke in
patients with ischemic MMD, the preventive effect of surgical
revascularization treatment has been clinically demonstrated
(35,59–62).
However, intra- and extra-cranial revascularization for the
prevention of recurrence of bleeding in patients with hemorrhagic
MMD is controversial. Duan et al (19) performed a review of patients with MMD
and noted that the probability of recurrence of cerebral ischemia
or cerebral hemorrhage in patients subjected to surgical
re-vascularization was significantly lower than that in patients
who received conservative treatment. A study on Japanese adults
with MMD from 2010 defined the primary and secondary end points as
all adverse events and rebleeding attacks, respectively. It was
reported that for patients with hemorrhagic MMD, the difference
between the surgical and non-surgical group was statistically
significant, and a Kaplan-Meier analysis suggested that the
collateral circulation provided by the surgery was able to prevent
recurrent bleeding (63). Further
studies have provided similar results (64,65).
Therefore, the prevailing opinion is that patients with ischemic or
hemorrhagic MMD should receive surgical treatment (66).
Surgical revascularization of MMD includes 3 types:
Direct revascularization, indirect revascularization and combined
revascularization. In the direct revascularization surgery, the
most common method is superficial temporal artery-MCA anastomosis.
When ischemic hypoperfusion occurs in the blood supply area of the
ACA or posterior cerebral artery, the superficial temporal
artery-ACA or occipital artery-posterior cerebral artery
anastomosis may be adopted (67,68).
Indirect revascularization is a surgery based on a variety of
tissues used as a source of blood supply, mainly including
encephalomyosynangiosis, encephaloduroarteriosynangiosis, multiple
burr hole surgery, encephaloduromyoarteriosynangiosis,
encephaloduromyoarteriopericranial synangiosis and omental
transplantation (69–74). Combined revascularization refers to
the combined use of the former two revascularization techniques. A
recent meta-analysis revealed that direct or combined
revascularization surgery is better for unstable adult patients
with MMD characterized by symptomatic or hemodynamic instability
(75).
During the peri-operative period, it is necessary to
actively prevent the occurrence of ischemic complications,
particularly in pediatric patients with MMD (76). Most patients undergoing direct
vascular bypass surgery in the acute phase may suffer from
transient neurological dysfunction due to changes in hemodynamics.
The brain tissue hypoperfusion caused by changes in hemodynamics is
mainly caused by the competition between the blood flow from the
superficial temporal artery bridge blood vessels and the blood flow
from the existing collateral circulation, due to damage to the
cerebrovascular auto-regulation function (77). Studies have indicated that ~1/4 of
patients with direct bypass may suffer from high perfusion
symptoms, and there was a high risk of high perfusion in adult
patients with MMD and patients with hemorrhagic MMD (78). A PET study indicated that cerebral
blood flow and cerebral blood volume (CBV) increased, while the
oxygen extraction fraction (OEF) decreased under high perfusion
(71). In terms of hemodynamics, the
increase in pre-operative CBV or OEF is a risk factor for
post-operative high perfusion (79,80). It
is necessary to closely monitor the blood pressure fluctuations in
patients during the peri-operative period, in order to prevent the
occurrence of low or excessive perfusion.
The pathogenesis of MMD still remains to be fully
elucidated. The worldwide incidence of MMD is low, but it has a
higher incidence in Asian countries. MMD is an important cause of
cerebral stroke in pediatric and adult patients. In order to avoid
the occurrence of severe neurological symptoms, a definitive
diagnosis of MMD must be made as soon as possible, so that
treatment may be rapidly performed and a relatively good mid- and
long-term prognosis may be achieved. Surgery remains an important
treatment for MMD, but an individualized clinical treatment
strategy should be selected according to the condition of each
patient. With the increasing number of genetic studies, novel
treatment approaches for MMD at the genetic level may be developed
in the future.
Not applicable.
No funding was received.
Not applicable.
HZ was a major contributor in writing the
manuscript. LZ collected data for the current review. LF designed
and revised this review.
Not applicable.
Not applicable.
The authors declare that they have no competing
interests.
|
1
|
Takeuchi K and Shimizu K: Hypoplasia of
the bilateral internal carotid arteries. Brain Nerve. 9:37–43.
1957.
|
|
2
|
Suzuki J and Takaku A: Cerebrovascular
‘moyamoya’ disease. Disease showing abnormal net-like vessels in
base of brain. Arch Neurol. 20:288–299. 1969. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Kuroda S and Houkin K: Moyamoya disease:
Current concepts and future perspectives. Lancet Neurol.
7:1056–1066. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
4
|
Fukui M: Guidelines for the diagnosis and
treatment of spontaneous occlusion of the circle of Willis
(moyamoya' disease). Research committee on spontaneous occlusion of
the circle of Willis (moyamoya disease) of the ministry of health
and welfare, Japan. Clin Neurol Neurosurg. 99 (Suppl 2):S238–S240.
1997. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Research Committee on the Pathology and
Treatment of Spontaneous Occlusion of the Circle of Willis; Health
Labour Sciences Research Grant for Research on Measures for
Infractable Diseases: Guidelines for diagnosis and treatment of
moyamoya disease (spontaneous occlusion of the circle of Willis).
Neurol Med Chir (Tokyo). 52:245–266. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Syndrome Cecgodatomdam and Committee
TNCoHS PatoissecoS: Chinese expert consensus on diagnosis and
treatment of moyamoya disease and moyamoya syndrome (2017). Chin J
Neurosurg. 6:541–547. 2017.(In Chinese).
|
|
7
|
Research on intractable diseases of the
Ministry of Health Labour and Welfare, Japan: Recommendations for
the management of moyamoya disease: A statement from research
committee on spontaneous occlusion of the circle of Willis
(moyamoya disease). Surgery for Cerebral Stroke. 37:321–337. 2009.
View Article : Google Scholar
|
|
8
|
Piao J, Wu W, Yang Z and Yu J: Research
progress of moyamoya disease in children. Int J Med Sci.
12:566–575. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
9
|
Smith ER and Scott RM: Spontaneous
occlusion of the circle of Willis in children: Pediatric moyamoya
summary with proposed evidence-based practice guidelines. A review.
J Neurosurg Pediatr. 9:353–360. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Khan N, Achrol AS, Guzman R, Burns TC,
Dodd R, Bell-Stephens T and Steinberg GK: Sex differences in
clinical presentation and treatment outcomes in Moyamoya disease.
Neurosurgery. 71:587–593. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kim T, Lee H, Bang JS, Kwon OK, Hwang G
and Oh CW: Epidemiology of moyamoya disease in Korea: Based on
national health insurance service data. J Korean Neurosurg Soc.
57:390–395. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Zhou XW, Wang JZ and Ma Y: Literature
review and current situation of domestic moyamoya disease. Chin J
Pract Nerv Dis. 20:1–4. 2017.
|
|
13
|
Seol HJ, Wang KC, Kim SK, Hwang YS, Kim KJ
and Cho BK: Headache in pediatric moyamoya disease: Review of 204
consecutive cases. J Neurosurg. 103 Suppl 5:S439–S442. 2005.
|
|
14
|
Okada Y, Kawamata T, Kawashima A,
Yamaguchi K, Ono Y and Hori T: The efficacy of superficial temporal
artery-middle cerebral artery anastomosis in patients with moyamoya
disease complaining of severe headache. J Neurosurg. 116:672–679.
2012. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Baba T, Houkin K and Kuroda S: Novel
epidemiological features of moyamoya disease. J Neurol Neurosurg
Psychiatry. 79:900–904. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ahn IM, Park DH, Hann HJ, Kim KH, Kim HJ
and Ahn HS: Incidence, prevalence, and survival of moyamoya disease
in Korea: A nationwide, population-based study. Stroke.
45:1090–1095. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kainth D, Chaudhry SA, Kainth H, Suri FK
and Qureshi AI: Epidemiological and clinical features of moyamoya
disease in the USA. Neuroepidemiology. 40:282–287. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Miao W, Zhao PL, Zhang YS, Liu HY, Chang
Y, Ma J, Huang QJ and Lou ZX: Epidemiological and clinical features
of Moyamoya disease in Nanjing, China. Clin Neurol Neurosurg.
112:199–203. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Duan L, Bao XY, Yang WZ, Shi WC, Li DS,
Zhang ZS, Zong R, Han C, Zhao F and Feng J: Moyamoya disease in
China: Its clinical features and outcomes. Stroke. 43:56–60. 2012.
View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Mineharu Y, Takenaka K, Yamakawa H, Inoue
K, Ikeda H, Kikuta KI, Takagi Y, Nozaki K, Hashimoto N and Koizumi
A: Inheritance pattern of familial moyamoya disease: Autosomal
dominant mode and genomic imprinting. J Neurol Neurosurg
Psychiatry. 77:1025–1029. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Ikeda H, Sasaki T, Yoshimoto T, Fukui M
and Arinami T: Mapping of a familial moyamoya disease gene to
chromosome 3p24.2-p26. Am J Hum Genet. 64:533–537. 1999. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Yamauchi T, Tada M, Houkin K, Tanaka T,
Nakamura Y, Kuroda S, Abe H, Inoue T, Ikezaki K, Matsushima T and
Fukui M: Linkage of familial moyamoya disease (spontaneous
occlusion of the circle of Willis) to chromosome 17q25. Stroke.
31:930–935. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Sakurai K, Horiuchi Y, Ikeda H, Ikezaki K,
Yoshimoto T, Fukui M and Arinami T: A novel susceptibility locus
for moyamoya disease on chromosome 8q23. J Hum Genet. 49:278–281.
2004. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Kamada F, Aoki Y, Narisawa A, Abe Y,
Komatsuzaki S, Kikuchi A, Kanno J, Niihori T, Ono M, Ishii N, et
al: A genome-wide association study identifies RNF213 as the first
Moyamoya disease gene. J Hum Genet. 56:34–40. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu W, Morito D, Takashima S, Mineharu Y,
Kobayashi H, Hitomi T, Hashikata H, Matsuura N, Yamazaki S, Toyoda
A, et al: Identification of RNF213 as a susceptibility gene for
moyamoya disease and its possible role in vascular development.
PLoS One. 6:e225422011. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Wu Z, Jiang H, Zhang L, Xu X, Zhang X,
Kang Z, Song D, Zhang J, Guan M and Gu Y: Molecular analysis of
RNF213 gene for moyamoya disease in the Chinese Han population.
PLoS One. 7:e481792012. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Miyatake S, Miyake N, Touho H,
Nishimura-Tadaki A, Kondo Y, Okada I, Tsurusaki Y, Doi H, Sakai H,
Saitsu H, et al: Homozygous c.14576G>A variant of RNF213
predicts early-onset and severe form of moyamoya disease.
Neurology. 78:803–810. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Cecchi AC, Guo D, Ren Z, Flynn K,
Santos-Cortez RL, Leal SM, Wang GT, Regalado ES, Steinberg GK,
Shendure J, et al: RNF213 rare variants in an ethnically diverse
population with Moyamoya disease. Stroke. 45:3200–3207. 2014.
View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Kim EH, Yum MS, Ra YS, Park JB, Ahn JS,
Kim GH, Goo HW, Ko TS and Yoo HW: Importance of RNF213 polymorphism
on clinical features and long-term outcome in moyamoya disease. J
Neurosurg. 124:1221–1227. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Kobayashi H, Brozman M, Kyselová K,
Viszlayová D, Morimoto T, Roubec M, Školoudík D, Petrovičová A,
Juskanič D, Strauss J, et al: RNF213 rare variants in slovakian and
czech moyamoya disease patients. PLoS One. 11:e01647592016.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Raso A, Biassoni R, Mascelli S, Nozza P,
Ugolotti E, DI Marco E, DE Marco P, Merello E, Cama A, Pavanello M
and Capra V: Moyamoya vasculopathy shows a genetic mutational
gradient decreasing from East to West. J Neurosurg Sci.
2016.PubMed/NCBI
|
|
32
|
Guey S, Kraemer M, Hervé D, Ludwig T,
Kossorotoff M, Bergametti F, Schwitalla JC, Choi S, Broseus L,
Callebaut I, et al: Rare RNF213 variants in the C-terminal region
encompassing the RING-finger domain are associated with moyamoya
angiopathy in Caucasians. Eur J Hum Genet. 25:995–1003. 2017.
View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Li H, Zhang ZS, Liu W, Yang WZ, Dong ZN,
Ma MJ, Han C, Yang H, Cao WC and Duan L: Association of a
functional polymorphism in the MMP-3 gene with Moyamoya disease in
the Chinese Han population. Cerebrovasc Dis. 30:618–625. 2010.
View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Hishikawa T, Tokunaga K, Sugiu K and Date
I: Assessment of the difference in posterior circulation
involvement between pediatric and adult patients with moyamoya
disease. J Neurosurg. 119:961–965. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Fujimura M and Tominaga T: Lessons learned
from moyamoya disease: Outcome of direct/indirect revascularization
surgery for 150 affected hemispheres. Neurol Med Chir (Tokyo).
52:327–332. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Mugikura S, Takahashi S, Higano S, Shirane
R, Sakurai Y and Yamada S: Predominant involvement of ipsilateral
anterior and posterior circulations in moyamoya disease. Stroke.
33:1497–1500. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Mugikura S, Takahashi S, Higano S, Shirane
R, Kurihara N, Furuta S, Ezura M and Takahashi A: The relationship
between cerebral infarction and angiographic characteristics in
childhood moyamoya disease. AJNR Am J Neuroradiol. 20:336–343.
1999.PubMed/NCBI
|
|
38
|
Houkin K, Nakayama N, Kuroda S, Nonaka T,
Shonai T and Yoshimoto T: Novel magnetic resonance angiography
stage grading for moyamoya disease. Cerebrovasc Dis. 20:347–354.
2005. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Ryoo S, Cha J, Kim SJ, Choi JW, Ki CS, Kim
KH, Jeon P, Kim JS, Hong SC and Bang OY: High-resolution magnetic
resonance wall imaging findings of Moyamoya disease. Stroke.
45:2457–2460. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
So Y, Lee HY, Kim SK, Lee JS, Wang KC, Cho
BK, Kang E and Lee DS: Prediction of the clinical outcome of
pediatric moyamoya disease with postoperative basal/acetazolamide
stress brain perfusion SPECT after revascularization surgery.
Stroke. 36:1485–1489. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
41
|
Tanaka Y, Nariai T, Nagaoka T, Akimoto H,
Ishiwata K, Ishii K, Matsushima Y and Ohno K: Quantitative
evaluation of cerebral hemodynamics in patients with moyamoya
disease by dynamic susceptibility contrast magnetic resonance
imaging-comparison with positron emission tomography. J Cereb Blood
Flow Metab. 26:291–300. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
42
|
Federau C, Christensen S, Zun Z, Park SW,
Ni W, Moseley M and Zaharchuk G: Cerebral blood flow, transit time,
and apparent diffusion coefficient in moyamoya disease before and
after acetazolamide. Neuroradiology. 59:5–12. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
43
|
Chen JC, Liu B, Li ZW, Yu JS, He Y and
Chen RD: Using CT perfusion imaging to evaluate the effect of
STA-MCA bypass on hemorrhagic moyamoya disease. Chin J Neurosurg.
25:537–540. 2009.
|
|
44
|
Wang B, Zhou Q, Yao ZW, Li ZY and He GW:
CTP and PWI in assessment of the effect of cerebral
revascularization for moyamoya disease. Chin Comput Med imag.
21:64–68. 2015.
|
|
45
|
Nakagawara J: Reconsideration of
hemodynamic cerebral ischemia using recent PET/SPECT studies.
Trends in Cerebrovascular Surgery (Springer). 99–108. 2016.
View Article : Google Scholar
|
|
46
|
Takagi Y, Kikuta K, Nozaki K, Fujimoto M,
Hayashi J, Imamura H and Hashimoto N: Expression of
hypoxia-inducing factor-1 alpha and endoglin in intimal hyperplasia
of the middle cerebral artery of patients with Moyamoya disease.
Neurosurgery. 60:338–345. 2007. View Article : Google Scholar : PubMed/NCBI
|
|
47
|
Takagi Y, Kikuta K, Nozaki K and Hashimoto
N: Histological features of middle cerebral arteries from patients
treated for Moyamoya disease. Neurol Med Chir (Tokyo). 47:1–4.
2007. View Article : Google Scholar : PubMed/NCBI
|
|
48
|
Chmelova J, Kolar Z, Prochazka V, Curik R,
Dvorackova J, Sirucek P, Kraft O and Hrbac T: Moyamoya disease is
associated with endothelial activity detected by anti-nestin
antibody. Biomed Pap Med Fac Univ Palacky Olomouc Czech Repub.
154:159–162. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
49
|
Guo DC, Papke CL, Tran-Fadulu V, Regalado
ES, Avidan N, Johnson RJ, Kim DH, Pannu H, Willing MC, Sparks E, et
al: Mutations in smooth muscle alpha-actin (ACTA2) cause coronary
artery disease, stroke, and Moyamoya disease, along with thoracic
aortic disease. Am J Hum Genet. 84:617–627. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
50
|
Kumar AH and Caplice NM: Clinical
potential of adult vascular progenitor cells. Arterioscler Thromb
Vasc Biol. 30:1080–1087. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
51
|
Kim JH, Jung JH, Phi JH, Kang HS, Kim JE,
Chae JH, Kim SJ, Kim YH, Kim YY, Cho BK, et al: Decreased level and
defective function of circulating endothelial progenitor cells in
children with moyamoya disease. J Neurosci Res. 88:510–518.
2010.PubMed/NCBI
|
|
52
|
Lee JY, Moon YJ, Lee HO, Park AK, Choi SA,
Wang KC, Han JW, Joung JG, Kang HS, Kim JE, et al: Deregulation of
retinaldehyde dehydrogenase 2 leads to defective angiogenic
function of endothelial colony-forming cells in pediatric moyamoya
disease. Arterioscler Thromb Vasc Biol. 35:1670–1677. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
53
|
Kim SJ, Heo KG, Shin HY, Bang OY, Kim GM,
Chung CS, Kim KH, Jeon P, Kim JS, Hong SC and Lee KH: Association
of thyroid autoantibodies with moyamoya-type cerebrovascular
disease: A prospective study. Stroke. 41:173–176. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
54
|
Sigdel TK, Shoemaker LD, Chen R, Li L,
Butte AJ, Sarwal MM and Steinberg GK: Immune response profiling
identifies autoantibodies specific to Moyamoya patients. Orphanet J
Rare Dis. 8:452013. View Article : Google Scholar : PubMed/NCBI
|
|
55
|
Sakamoto S, Kiura Y, Yamasaki F, Shibukawa
M, Ohba S, Shrestha P, Sugiyama K and Kurisu K: Expression of
vascular endothelial growth factor in dura mater of patients with
moyamoya disease. Neurosurg Rev. 31:77–81. 2008. View Article : Google Scholar : PubMed/NCBI
|
|
56
|
Furuno A, Watari K, Nakamura M, Fukunaga
Y, Jung JH and Ono M: A natural anti-inflammatory enone fatty acid
inhibits angiogenesis by attenuating nuclear factor-κB signaling in
vascular endothelial cells. Int J Oncol. 38:493–501.
2011.PubMed/NCBI
|
|
57
|
Kang HS, Kim JH, Phi JH, Kim YY, Kim JE,
Wang KC, Cho BK and Kim SK: Plasma matrix metalloproteinases,
cytokines and angiogenic factors in moyamoya disease. J Neurol
Neurosurg Psychiatry. 81:673–678. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
58
|
Jeon JS, Ahn JH, Moon YJ, Cho WS, Son YJ,
Kim SK, Wang KC, Bang JS, Kang HS, Kim JE and Oh CW: Expression of
cellular retinoic acid-binding protein-I (CRABP-I) in the
cerebrospinal fluid of adult onset moyamoya disease and its
association with clinical presentation and postoperative
haemodynamic change. J Neurol Neurosurg Psychiatry. 85:726–731.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
59
|
Fung LW, Thompson D and Ganesan V:
Revascularisation surgery for paediatric moyamoya: A review of the
literature. Childs Nerv Syst. 21:358–364. 2005. View Article : Google Scholar : PubMed/NCBI
|
|
60
|
Guzman R, Lee M, Achrol A, Bell-Stephens
T, Kelly M, Do HM, Marks MP and Steinberg GK: Clinical outcome
after 450 revascularization procedures for moyamoya disease.
Clinical article. J Neurosurg. 111:927–935. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
61
|
Hallemeier CL, Rich KM, Grubb RL Jr,
Chicoine MR, Moran CJ, Cross DT III, Zipfel GJ, Dacey RG Jr and
Derdeyn CP: Clinical features and outcome in North American adults
with moyamoya phenomenon. Stroke. 37:1490–1496. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
62
|
Scott RM, Smith JL, Robertson RL, Madsen
JR, Soriano SG and Rockoff MA: Long-term outcome in children with
moyamoya syndrome after cranial revascularization by pial
synangiosis. J Neurosurg. 100 (2 Suppl Pediatrics):S142–S149.
2004.
|
|
63
|
Miyamoto S, Yoshimoto T, Hashimoto N,
Okada Y, Tsuji I, Tominaga T, Nakagawara J and Takahashi JC; JAM
Trial Investigators, : Effects of extracranial-intracranial bypass
for patients with hemorrhagic moyamoya disease: Results of the
Japan Adult Moyamoya Trial. Stroke. 45:1415–1421. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
64
|
Wan M and Duan L: Recent progress in
hemorrhagic moyamoya disease. Br J Neurosurg. 29:189–191. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
65
|
Huang Z, Ding X, Men W, Zhang D, Zhao Y,
Wang R, Wang S and Zhao J: Clinical features and outcomes in 154
patients with haemorrhagic moyamoya disease: Comparison of
conservative treatment and surgical revascularization. Neurol Res.
37:886–892. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
66
|
Lee SU, Oh CW, Kwon OK, Bang JS, Ban SP,
Byoun HS and Kim T: Surgical treatment of adult moyamoya disease.
Curr Treat Options Neurol. 20:222018. View Article : Google Scholar : PubMed/NCBI
|
|
67
|
Kawashima A, Kawamata T, Yamaguchi K, Hori
T and Okada Y: Successful superficial temporal artery-anterior
cerebral artery direct bypass using a long graft for moyamoya
disease. Neurosurgery. 67 (3 Suppl Operative):ons145–ons149.
2010.PubMed/NCBI
|
|
68
|
Hayashi T, Shirane R and Tominaga T:
Additional surgery for postoperative ischemic symptoms in patients
with moyamoya disease: The effectiveness of occipital
artery-posterior cerebral artery bypass with an indirect procedure:
Technical case report. Neurosurgery. 64:E195–E196. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
69
|
Karasawa J, Kikuchi H, Furuse S, Sakaki T
and Yoshida Y: A surgical treatment of ‘moyamoya’ disease
‘encephalo-myo synangiosis’. Neurol Med Chir (Tokyo). 17:29–37.
1977. View Article : Google Scholar : PubMed/NCBI
|
|
70
|
Matsushima Y, Aoyagi M, Koumo Y, Takasato
Y, Yamaguchi T, Masaoka H, Suzuki R and Ohno K: Effects of
encephalo-duro-arterio-synangiosis on childhood Moyamoya patients.
Neurol Med Chir (Tokyo). 31:708–714. 1991. View Article : Google Scholar : PubMed/NCBI
|
|
71
|
Endo M, Kawano N, Miyaska Y and Yada K:
Cranial burr hole for revascularization in moyamoya disease. J
Neurosurg. 71:180–185. 1989. View Article : Google Scholar : PubMed/NCBI
|
|
72
|
Kinugasa K, Mandai S, Tokunaga K, Kamata
I, Sugiu K, Handa A and Ohmoto T: Ribbon
enchephalo-duro-arterio-myo-synangiosis for moyamoya disease. Surg
Neurol. 41:455–461. 1994. View Article : Google Scholar : PubMed/NCBI
|
|
73
|
Kuroda S, Houkin K, Ishikawa T, Nakayama N
and Iwasaki Y: Novel bypass surgery for moyamoya disease using
pericranial flap: Its impacts on cerebral hemodynamics and
long-term outcome. Neurosurgery. 66:1093–1101. 2010. View Article : Google Scholar : PubMed/NCBI
|
|
74
|
Karasawa J, Kikuchi H, Kawamura J and
Sakai T: Intracranial transplantation of the omentum for
cerebrovascular moyamoya disease: A two-year follow-up study. Surg
Neurol. 14:444–449. 1980.PubMed/NCBI
|
|
75
|
Kim H, Jang DK, Han YM, Sung JH, Park IS,
Lee KS, Yang JH, Huh PW, Park YS, Kim DS and Han KD: Direct bypass
versus indirect bypass in adult moyamoya angiopathy with symptoms
or hemodynamic instability: A meta-analysis of comparative studies.
World Neurosurg. 94:273–284. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
76
|
Iwama T, Hashimoto N and Yonekawa Y: The
relevance of hemodynamic factors to perioperative ischemic
complications in childhood moyamoya disease. Neurosurgery.
38:1120–1126. 1996. View Article : Google Scholar : PubMed/NCBI
|
|
77
|
Mukerji N, Cook DJ and Steinberg GK: Is
local hypoperfusion the reason for transient neurological deficits
after STA-MCA bypass for moyamoya disease? J Neurosurg. 122:90–94.
2015. View Article : Google Scholar : PubMed/NCBI
|
|
78
|
Fujimura M, Mugikura S, Kaneta T, Shimizu
H and Tominaga T: Incidence and risk factors for symptomatic
cerebral hyperperfusion after superficial temporal artery-middle
cerebral artery anastomosis in patients with moyamoya disease. Surg
Neurol. 71:442–447. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
79
|
Kaku Y, Iihara K, Nakajima N, Kataoka H,
Fukuda K, Masuoka J, Fukushima K, Iida H and Hashimoto N: Cerebral
blood flow and metabolism of hyperperfusion after cerebral
revascularization in patients with moyamoya disease. J Cereb Blood
Flow Metab. 32:2066–2075. 2012. View Article : Google Scholar : PubMed/NCBI
|
|
80
|
Uchino H, Kuroda S, Hirata K, Shiga T,
Houkin K and Tamaki N: Predictors and clinical features of
postoperative hyperperfusion after surgical revascularization for
moyamoya disease: A serial single photon emission CT/positron
emission tomography study. Stroke. 43:2610–2616. 2012. View Article : Google Scholar : PubMed/NCBI
|