Introduction
Hypertrophic cardiomyopathy (HCM) occurs at a
frequency of at least 1 in 500 in the general population, making it
one of the most common inherited heart diseases (1–3). HCM is
defined by the presence of increased left ventricular (LV) wall
thickness that is not solely explained by abnormal loading
conditions (4). The pathology is
characterized by asymmetric or concentric myocardial hypertrophy
associated with myocardial fiber disarray and fibrosis, leading to
global and regional variability, and heterogeneity of systolic and
diastolic deformation (5). At least
1/3 of patients with HCM have the non-obstructive form of the
disease, with few to no outflow gradients (<30 mm Hg) at rest or
with exercise (6).
However, the non-obstructive form of HCM has been
less well studied; in particular, data on cardiac function and
pathophysiology are ambiguous or inconclusive. Previous studies
have demonstrated that patients with HCM with the non-obstructive
form of the disease have exertional dyspnea (with preserved
systolic function), largely as a result of diastolic dysfunction
(6). Furthermore, previous studies
have reported that LV diastolic dysfunction is a hallmark of HCM
that occurs in the majority of patients (7,8).
However, MacIver and Clark (9)
suggested that measures of ‘diastolic dysfunction’ were common in
HCM, although this may not be the dominant abnormality. It was
suggested that the principal abnormality in HCM may be reduced
contractile wall stress, even with a normal or increased ejection
fraction (9). Blood flow dynamics
analysis has emerged as a potential solution, allowing for the
measurement of energy loss (EL) generated from blood viscous
friction by vector flow mapping (VFM) techniques (10), thereby providing a novel way to
assess cardiac function during the early stages of HCM in
patients.
The primary aim of the present study was to
investigate and analyze the EL by VFM in patients with HCM and
control subjects and determine whether the EL may be associated
with cardiac systolic and diastolic function in patients with HCM.
The secondary aim of the present study was to compare classical
echocardiographic parameters and the left atrial (LA) and LV
deformation parameters by 2-D speckle tracking echocardiography
(STE) in patients with HCM and control subjects, and to determine
the impact of global myocardial mass on global longitudinal strain
components.
Materials and methods
Study population
The present cross-sectional study included 52
patients diagnosed with the non-obstructive form of HCM and 40 age-
and sex-matched healthy controls, who were referred to Qilu
Hospital of Shandong University between July 2015 and December
2016. A total of 10 patients were excluded due to hypertension
(n=5), irregular arrhythmias (n=1), LV ejection fraction (LVEF)
<50% (n=2) and poor acoustic windows (n=2). The following
diagnostic criteria for non-obstructive HCM were used, according to
the 2014 ESC guidelines on the diagnosis and management of HCM
(4): LV hypertrophy with LV wall
thickness ≥15 mm for isolated cases and ≥13 mm for familial
screening, with asymmetric distribution associated with a
nondilated and hyperdynamic chamber in the absence of another
cardiac or systemic disease, for example hypertension or aortic
stenosis, associated with a preserved LVEF of >50% assessed by
2D echocardiography; and an instantaneous peak Doppler LV outflow
tract pressure gradient <30 mm Hg at rest, or during
physiological provocation, including the Valsalva maneuver,
standing and exercise. All subjects signed an informed consent
statement and the study protocol was approved by the Medical Ethics
Committee of Qilu Hospital of Shandong University (Jinan,
China).
Standard echocardiography
All subjects underwent comprehensive 2D resting
echocardiography. Echo-Doppler examinations were completed using a
UST-52105 probe (1–5 MHz) on a ProSound F75 ultrasound device
(Hitachi Aloka Medical, Ltd., Tokyo, Japan). Echocardiography was
performed by experienced sonographers. Subsequently, 2D
echocardiographic images of the left ventricle were obtained from
the parasternal long-axis and from the three standard LV apical
views (4-, 2- and 3-chamber). The following parameters were
measured: i) LV end-diastolic diameter (LVEDD; mm) and end-systolic
diameter (mm), LV end-diastolic volume (LVEDV; ml) and end-systolic
volume (LVESV; ml), LVEF (%) using the Simpson's method, wall
thickness, relative wall thickness (RWT), LV mass (LVM) and the LV
mass index (LVMI); ii) LA diameter (LAD; mm), LA volume (LAV; ml),
LA volume index (LAVI), the passive LAEF (%), the total LAEF (%)
and the active LAEF (%); and iii) peak E wave velocity (m/sec),
peak A wave velocity (m/sec), E/A, E wave deceleration time (DT;
msec) and A wave duration time (Adur; msec) of the mitral inflow
wave form measured by pulsed wave Doppler, the mean value of early
diastolic velocities (e'; m/sec) from the septal-lateral mitral
annulus in the apical 4-chamber view using tissue Doppler imaging
and the ratio E/e'.
Speckle tracking imaging study
The offline analysis for speckle tracking was
performed using a DAS-RS1 workstation (Hitachi-Aloka Medical, Ltd.,
Tokyo, Japan). LV global longitudinal systolic peak strain (GLS),
peak atrial longitudinal strain (PALS) and the atrial strain rate
(SR) during systole (SRs), early diastolic (SRe) and atrium
contraction (SRa) were obtained from standard long-axis views (4-,
2- and 3-chamber) and were averaged. The LA stiffness index
(E/e'/PALS) was calculated (11).
Measurements of GLS, PALS and strain rate are presented in Fig. 1.
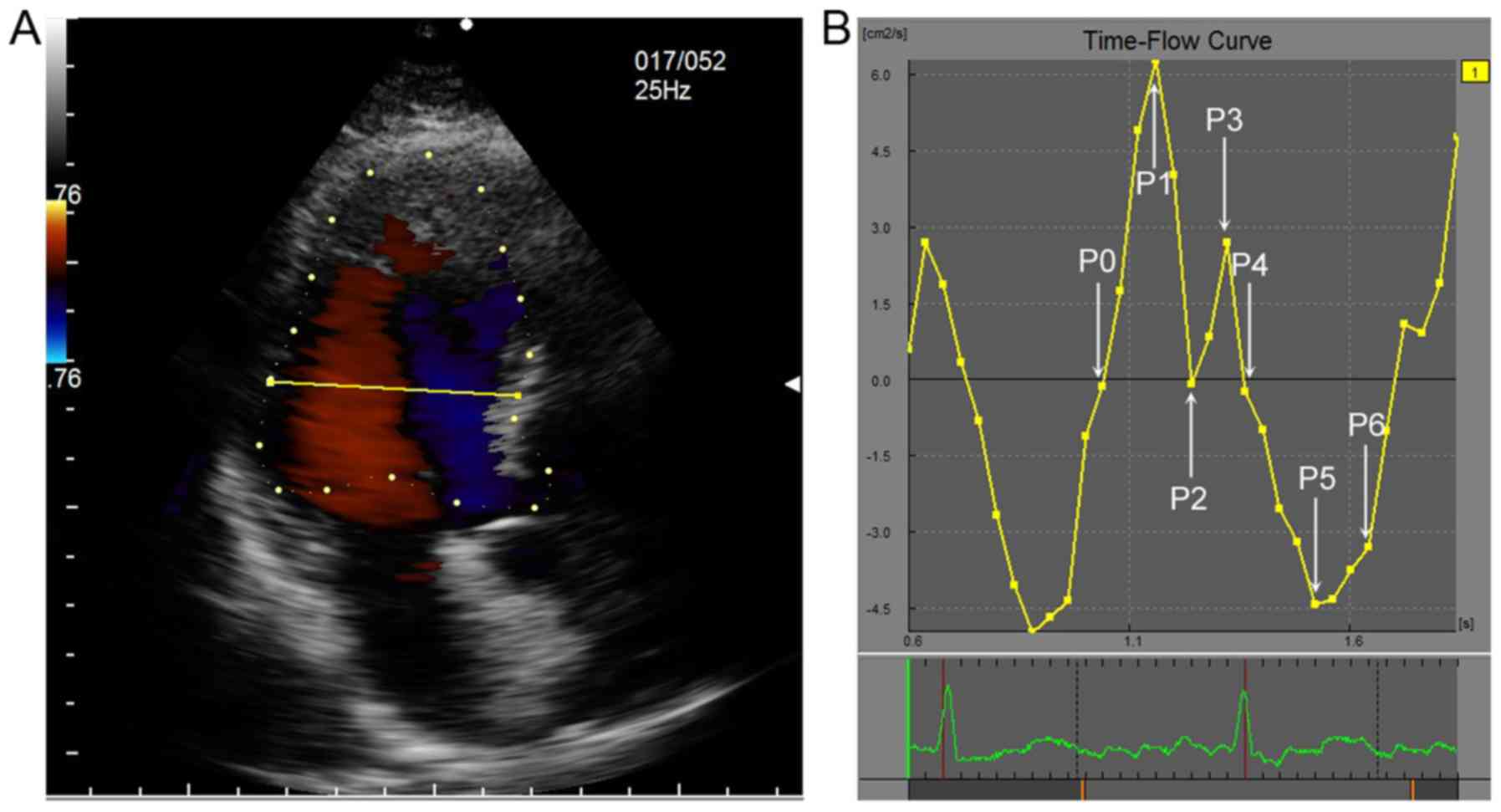
VFM
Intracardiac flow images were recorded in the apical
3-chamber view. Color flow images were transferred into a VFM
workstation (DAS-RS1 5.0; Hitachi-Aloka Medical, Ltd.) for offline
analysis. The frame rates were set to the range of 20–25 frames/sec
for the subsequent VFM analyses. All images were acquired during
three consecutive cardiac cycles. The Nyquist limit for 2D color
Doppler imaging was set high enough to mitigate the aliasing
phenomenon. A cardiac cycle was selected for the analysis by
determining two consecutive QRS complexes as the beginning and
ending points. The phases of one cardiac cycle were determined
according to a time-flow curve and the opening and closing of the
valve with the synchronous ECG. The opening and closing of the
mitral valve were defined as the beginning and ending of the
diastolic phase, respectively. To determine the ventricular cavity,
the endocardial border was manually traced on the first frame. The
phases of the cardiac cycle for LVEL analysis are exhibited in
Fig. 2. The phases of the cardiac
cycle for left atrial energy loss (LAEL) analysis are exhibited in
Fig. 3.
The EL was automatically calculated following the
selection of the region of interest. From the velocity vector
fields of the intra-atrial blood flow, EL was calculated for each
frame of the cine loop image. EL was defined as follows:
EL=∑i,j∫12μ(∂ui∂xj+∂uj∂xi)2dv
where µ indicates the blood viscosity coefficient,
which was set as 0.004 Pa/sec. The total EL and averaged EL were
calculated. The measurements were averaged over three cardiac
cycles and indexed to body surface area (BSA).
Statistical analyses
All continuous variables are presented as the mean ±
standard deviation. For the comparison of data, Student's t-tests
were used to compare continuous data between the HCM and control
groups. χ2 analysis was used to compare categorical
variables between the two groups. One-way analysis of variance was
performed, followed by multiple comparisons using the least
significant difference test or Tamhane's T2 test. To assess the
correlation between parameters, Pearson's or Spearman's correlation
analysis was used. All statistical analyses were performed using
SPSS software 13.0 (SPSS, Inc., Chicago, IL, USA). P<0.05 was
considered to indicate a statistically significant difference.
Results
Baseline clinical characteristics
Baseline clinical characteristics of all the
participants are summarized in Table
I. The results revealed that the body mass index and BSAs of
patients with HCM were significantly increased compared with those
of the control group (25.67±3.96 kg/m2 vs. 23.58±2.94
kg/m2, P=0.026; 1.79±0.18 m2 vs. 1.64±0.15
m2, P=0.002), whereas the age and sex distribution,
heart rate, cholesterol, triglyceride, high-density lipoprotein
cholesterol and low-density lipoprotein cholesterol of the two
groups were similar. The systolic blood pressure of the patients
with HCM was significantly increased compared with the control
group (132±13 mmHg vs. 115±12 mmHg; P=0.02), although approximately
within the normal range according to the HBP diagnostic criteria
(12). The baseline characteristics
of HCM patients were similar to those in the control group.
 | Table I.Clinical parameters in patients with
HCM and control subjects. |
Table I.
Clinical parameters in patients with
HCM and control subjects.
| Parameters | HCM (n=42) | Control (n=40) | P-value |
|---|
| Age (years) |
53.74±12.98 |
50.56±12.93 | 0.319 |
| Sex (M/F) | 20/11 | 16/20 | 0.081 |
| Heart rate |
68.52±10.49 |
68.52±10.49 | 0.198 |
| BMI
(kg/m2) | 25.67±3.96 | 23.58±2.94 | 0.026 |
| BSA
(m2) |
1.79±0.18 |
1.64±0.15 | 0.002 |
| SBP (mmHg) | 132±13 | 115±12 | 0.028 |
| DBP (mmHg) |
87±10 | 74±9 | 0.051 |
| Cho (mmol/l) |
4.227±1.132 |
4.650±0.878 | 0.163 |
| TG (mmol/l) |
1.402±0.654 |
1.459±0.416 | 0.7154 |
| LDL-C (mmol/l) |
2.685±1.063 |
2.683±0.914 | 0.993 |
| HDL-C (mmol/l) |
1.127±0.203 |
1.301±0.379 | 0.124 |
The 2D classical and STE echocardiographic
parameters of the left ventricle are summarized in Table II. In general, patients with HCM had
a greater LV wall thickness including left ventricular posterior
wall, interventricular septum and RWT, and a higher ventricular
mass (LVM and LVMI). No significant differences were observed in
the LVEDD and LVEF in the patients with HCM compared with the
control group. However, LVEDV and LVESV were significantly reduced
compared with the control group (65.07±19.87 vs. 78.78±15.08 and
21.28±8.78 vs. 27.06±5.57, respectively; both P=0.002). The E/e'
and EDT were significantly higher in the HCM group compared with
the controls (10.71±3.88 vs. 6.59±1.46; P<0.001 and
221.57±105.11 vs. 169.5±27.92; P=0.011, respectively), whereas E,
A, the E/A ratio and Adur were not significantly different between
the HCM and control groups. Notably, the GLS was significantly
lower in the HCM group compared with the control group (−11.06±0.41
vs. −15.69±0.42; P<0.001). These results suggest that patients
with HCM had hypertrophic ventricular walls and smaller cardiac
cavities, whereas impaired systolic function (GLS) and diastolic
function (EDT) had already occurred when the traditional systolic
function indicator LVEF and diastolic function indicator E/e' were
still within normal range.
| Table II.Two-dimensional classical and speckle
tracking echocardiography echocardiographic parameters of the left
ventricle in control subjects and patients with HCM. |
Table II.
Two-dimensional classical and speckle
tracking echocardiography echocardiographic parameters of the left
ventricle in control subjects and patients with HCM.
| Parameters | HCM (n=42) | Control (n=40) | P-value |
|---|
| RWT | 0.48±0.15 | 0.33±0.04 | <0.001 |
| LVM (g) | 293.97±101.55 | 119.15±24.90 | <0.001 |
| LVMI
(g/m2) | 156.46±61.43 | 71.53±12.36 | <0.001 |
| LVPW (mm) | 10.74±3.02 | 7.42±0.91 | <0.001 |
| IVS (mm) | 19.21±4.07 | 8.94±1.58 | <0.001 |
| LVEDD (mm) | 46.18±5.81 | 45.11±3.24 | 0.371 |
| LVEDV (ml) | 65.07±19.87 | 78.78±15.08 | 0.002 |
| LVESV (ml) | 21.28±8.78 | 27.06±5.57 | 0.002 |
| LVEF | 0.63±0.18 | 0.65±0.04 | 0.458 |
| E (cm/sec) | 72.44±17.16 | 77.89±14.69 | 0.165 |
| A (cm/sec) | 66.28±27.91 | 72.19±18.74 | 0.321 |
| E/A | 1.27±0.59 | 1.14±0.36 | 0.291 |
| E/e' | 10.71±3.883 | 6.586±1.462 | <0.001 |
| EDT (msec) | 221.57±105.11 | 169.5±27.92 | 0.011 |
| Adur (msec) | 168.13±30.44 | 153±40.84 | 0.373 |
| GLS (%) | −11.06±0.406 | −15.69±0.424 | <0.001 |
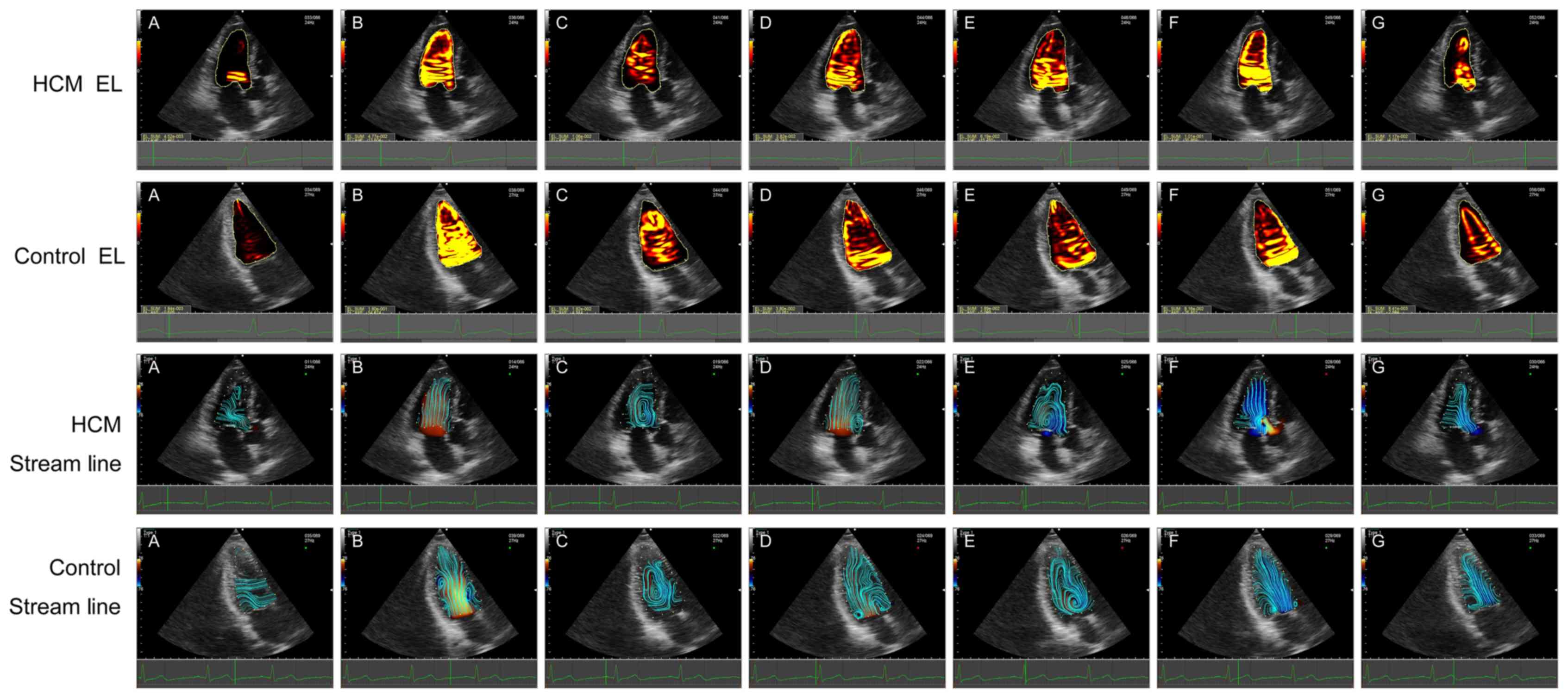
Alterations in dissipative EL values were noted
between the HCM and the control group, as summarized in Figs. 4 and 5. Importantly, the streamline of the left
ventricle in the control group was more intensive and regular
compared with the HCM group (Fig. 3B, F
and G), and the vortex size was smaller in patients with HCM
(Fig. 3C-E). Secondly, EL in all
phases gradually decreased from the base to the middle and apex in
the HCM and control groups. The EL-total of P1 (rapid filling time)
and P5 (rapid ejection time) were higher compared with the other
phases. Thirdly, compared with the controls, the EL-total was
significantly decreased in patients with HCM during the diastolic
phase (P1, P2 and P3; all P<0.05). However, a tendency for
increased systolic EL-total values referring to P4, P5 and P6 in
patients with HCM compared with controls was observed (P>0.05).
The EL-base during P1 and P2 were significantly decreased in
patients with HCM (both P<0.05). Significant differences were
observed in the EL-mid between the two groups. Compared with the
controls, the EL-mid values of patients with HCM were significantly
lower during the diastolic phases (P0, P1, P2 and P3; all
P<0.05). However, the EL-mid values of patients with HCM were
significantly higher compared with those of the controls during
systolic P5 (P<0.05). The EL-apex was significantly decreased in
patients with HCM during diastole phase including P0, P2 and P3
(all P<0.05). These results suggest that in patients with HCM,
the change of diastolic EL was more significant than that of
systolic EL, and therefore myocardial diastolic function may be
more vulnerable in patients with HCM.
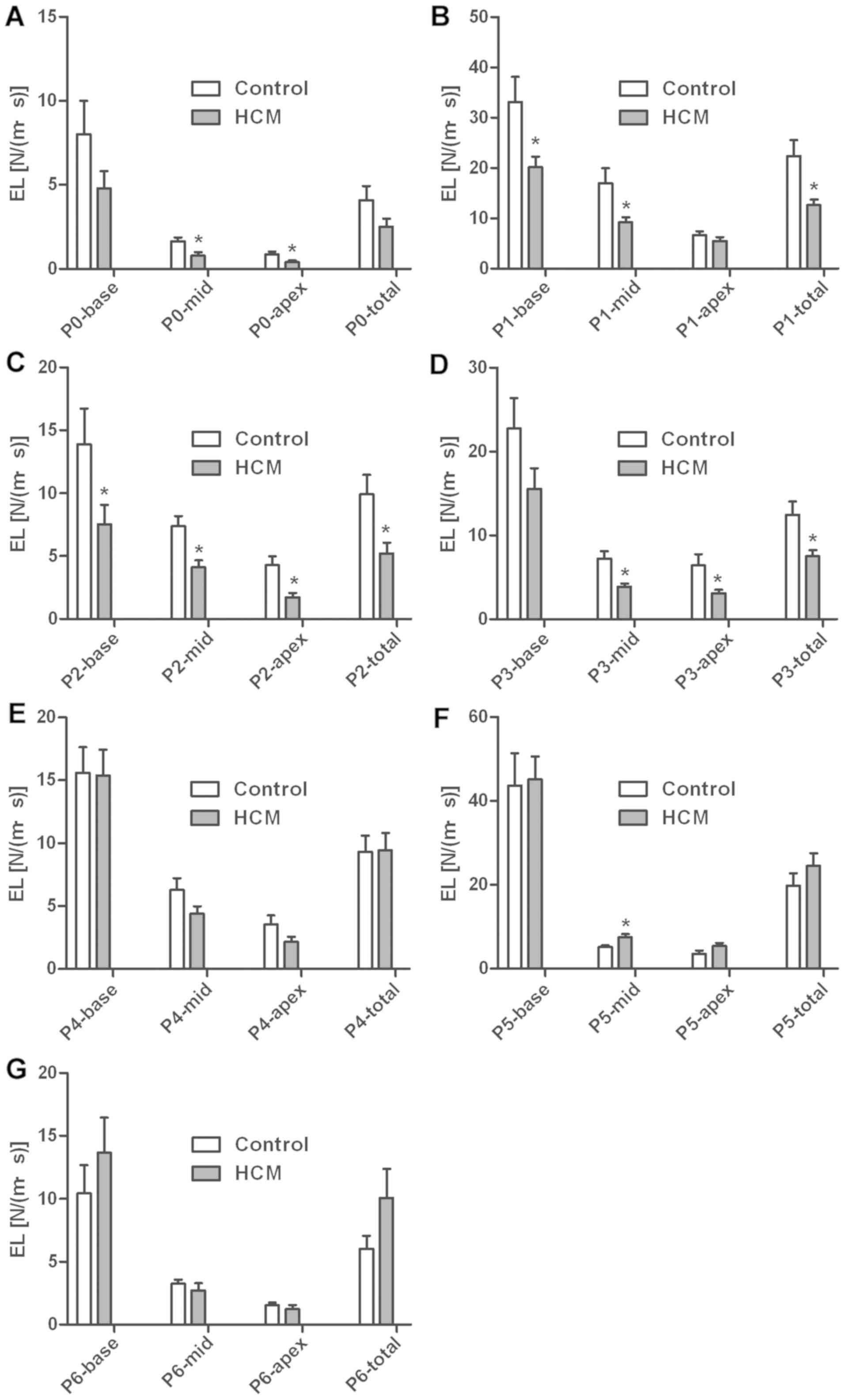 | Figure 4.Comparison of LVEL of different
timing between HCM and control. (A) P0 indicated the IVR time; (B)
P1 indicated the rapid filling time; (C) P2 indicated the slow
filling phase; (D) P3 indicated the atrial contraction time of late
diastole; (E) P4 indicated the IVC time; (F) P5 indicated rapid
ejection time; and (G) P6 indicated the slow ejection time.
Compared with controls, EL-total was significantly decreased in
patients with HCM during the diastolic phase (P1, P2 and P3; all
P<0.05). The systolic EL-total in patients with HCM tended to be
larger compared with the control (P>0.05). EL-base was decreased
in patients with HCM during P1 and P2 (slow filling time). Compared
with the controls, the EL-mid of patients with HCM were lower
during the diastolic phases (P0, P1, P2 and P3; all P<0.05).
However, the EL-mid of patients with HCM was higher than that of
the controls during systolic P5 (P<0.05). EL-apex was decreased
in patients with HCM during P0, P2 and P3. *P<0.05 vs. control.
LVEL, energy loss of left ventricle; EL, energy loss; HCM,
hypertrophic cardiomyopathy; LVEL, energy loss of left ventricle;
IVR, isovolumic relaxation; IVC, isovolumic contraction; N/(m·s),
Newton/(meter·second). |
Echocardiographic parameters of the
left atrium
The 2D classical and STE echocardiographic
parameters of the left atrium are summarized in Table III. Briefly, there were significant
differences in LA diameter and volume (P<0.001). The LAD, LAV
and LAVI were significantly higher in patients with HCM, whereas
the PALS, measured at the end of the reservoir phase, was
significantly decreased in the patients with HCM compared with the
controls (P<0.001). The absolute values of mean strain rate
(mSR) at systolic (mSRs), early diastolic (mSRe) and at atrial
contraction (mSRa) were all significantly decreased in patients
with HCM (P<0.001).
| Table III.Two-dimensional classical and speckle
tracking echocardiography echocardiographic parameters of LA in
control subjects and patients with HCM. |
Table III.
Two-dimensional classical and speckle
tracking echocardiography echocardiographic parameters of LA in
control subjects and patients with HCM.
| Parameters | HCM (n=42) | Control (n=40) | P-value |
|---|
| LAD (mm) | 40.16±5.66 | 30.47±5.03 | <0.001 |
| LAV (ml) | 63.93±25.44 | 40.86±11.57 | <0.001 |
| LAVI
(ml/m2) | 35.31±13.50 | 24.64±6.86 | <0.001 |
| LAPEF | 0.3152±0.1463 | 0.3440±0.0978 | 0.321 |
| LAAEF | 0.3493±0.1098 | 0.3240±0.0842 | 0.282 |
| LATEF | 56.52±7.61 | 55.00±6.83 | 0.412 |
| PALS (%) | 22.22±1.411 | 37.47±1.840 |
<0.001 |
| mSRs
(s−1) | 1.212±0.08 | 1.78±0.07 |
<0.001 |
| mSRe
(s−1) | −0.9772±0.066 | −2.095±0.176 |
<0.001 |
| mSRa
(s−1) | −1.009±0.093 | −1.946±0.117 | <0.001 |
| Stiffness
index | 0.5609±0.317 | 0.2706±0.090 | <0.001 |
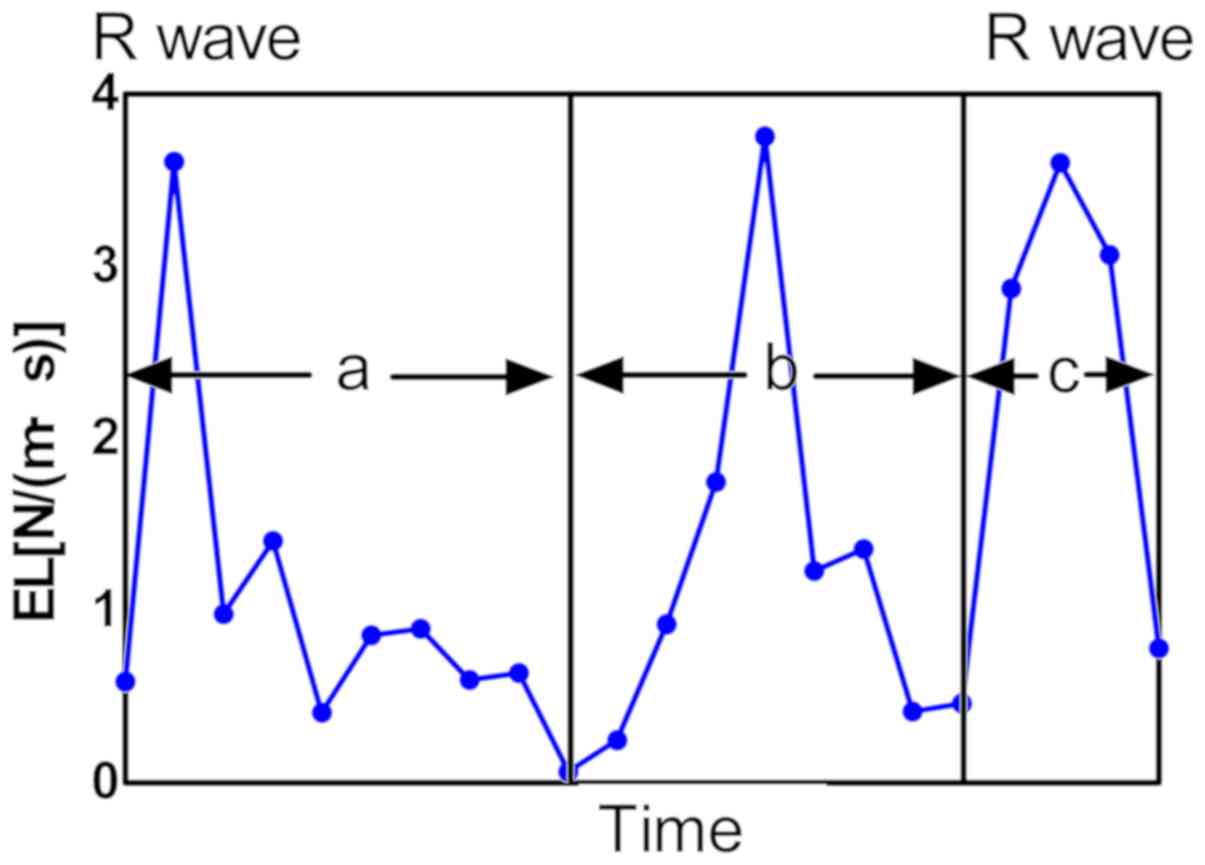
LA physiology during every cardiac cycle consists of
three different phases that modulate LV filling, termed the
reservoir phase, the conduit phase and the atrial systolic phase
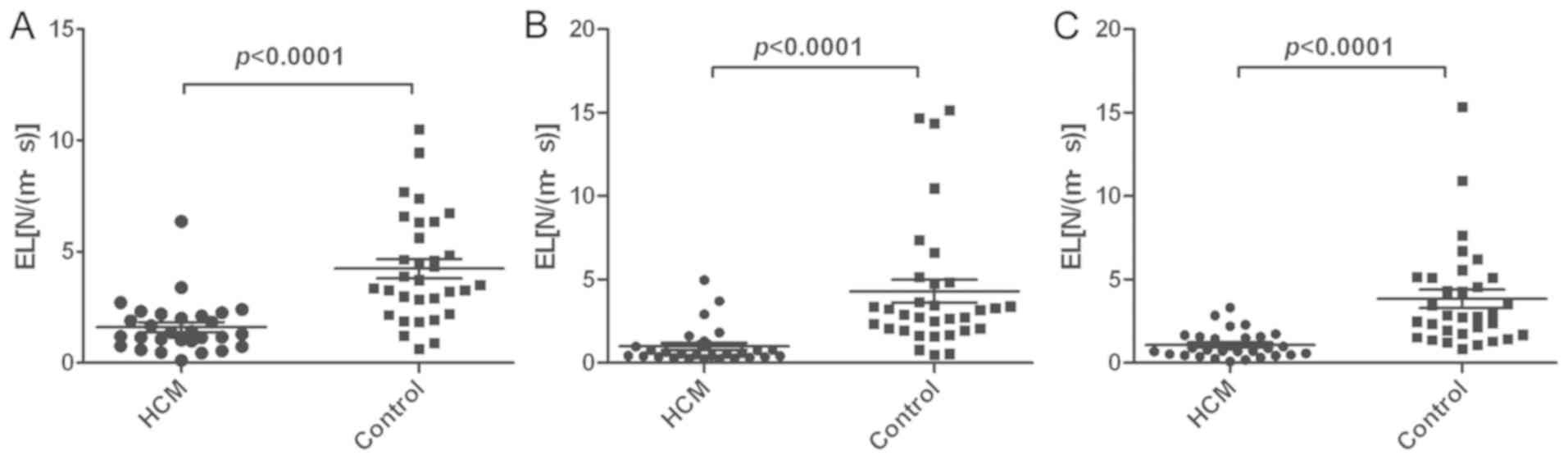
(13,14). To analyze LA function, the
measurements of LAEL were divided into these three phases. LAEL
reached its peak values during LV systole, early diastole and
atrial contraction (Fig. 2).
Compared with the controls, the LAEL of all three phases in
patients with HCM were significantly decreased (P<0.0001;
Fig. 5). In patients with HCM, the
LA function during the reservoir, conduit and atrial systolic
phases was all impaired.
Analysis of correlation
Correlation analysis between specific parameters
measured in the current study was examined (data not shown).
Notably, the GLS did not correlate with LVEF, E/e', LA stiffness
index and LVEL, although it did exhibit a significant correlation
with the PALS (r=−0.373; P=0.011) and the LAEL of the early
diastolic phase (r=−0.348; P=0.032). The diastolic LVEL during P1
phase correlated with E/e' (r=0.682; P<0.001) and the LA
stiffness index (r=0.474; P=0.002). The systolic LVEL during P5 and
P6 phase correlated with the PALS (r=0.430, P=0.004; r=0.387
P=0.009, respectively). The LAEL during LV systole and atrial
contraction phase exhibited a significant correlation with the PALS
(r=0.367, P=0.025; r=0.503, P=0.003, respectively) and LA stiffness
index (r=−0.439, P=0.009; r=−0.317, P=0.047, respectively). These
results indicated that the diastolic and systolic LVEL, as well as
LAEL, were in accordance with traditional echocardiographic
parameters in reflecting diastolic and systolic dysfunction.
Discussion
The present study investigated phasic alterations in
the strength of EL in patients with HCM as a novel method of
quantification of LV and LA function. For patients with early-stage
HCM, radial contractile function (EF or fractional shortening) is
typically normal or increased (15).
The results of the present study demonstrated that during the early
stages of HCM, the LV diastolic EL and the LV GLS were reduced,
while E/e', although increased compared with the control group,
remained <14. However, there was no significant alteration in
LVEF. This suggested that LV systolic and diastolic dysfunction had
already occurred during the early stages, while LVEF and E/e' were
in the normal range. The present results also indicated that during
the whole cardiac cycle, including the LV ejection, early diastolic
and late diastolic stages, LAEL and LA systolic peak strain were
reduced, indicating that atrial mechanical functioning was
impaired.
Clinically, hypertrophy and disarray of the
myocardial fibers are the principal deformities in patients with
HCM, and these may result in impaired kinetic characteristics
(16). Early detection and
interventions for LV dysfunction are essential for patients with
HCM. Color Doppler flow imaging and tissue doppler imaging (TDI)
have been widely used to assess subclinical LV dysfunction in
patients with HCM (17,18). Speckle-tracking strain is a more
advanced method compared with TDI, since it is angle-independent
and more sensitive in its capturing of myocardial damage (19,20). The
newly-developed VFM, based on color Doppler imaging, with the use
of a continuity equation and STE, has been demonstrated to be
useful in the detection of subclinical LV dysfunction in patients
with infarctions, end-stage renal diseases and aortic regurgitation
diseases (21). The dissipative EL
is derived from the velocity vector field of intraventricular blood
flow and is considered to reflect the efficiency of blood flow, and
thus may be an indicator of LV function (10).
Early detection and interventions for LV dysfunction
are essential for patients with HCM. In the present study, patients
with HCM were observed to have thicker ventricular walls and larger
ventricular masses, despite a smaller ventricular cavity. The GLS
was significantly reduced in patients with HCM, despite normal LV
systolic function, as assessed with LVEF, suggesting the presence
of a global subclinical systolic dysfunction. Similar results have
been observed in a number of studies (4,5,22,23). The
present findings revealed that the diastolic EL was significantly
decreased in patients with HCM compared with controls. The
significantly decreased diastolic EL suggested that myocardial
diastolic function appeared to be more vulnerable in patients with
HCM, which was in accordance with previous studies (24–26).
Furthermore, the positive correlation between diastolic LVEL and
the traditional diastolic parameter E/e' suggested a connection
between diastolic LVEL and diastolic function. Although only EL-mid
at systolic P5 in HCM was significantly higher compared with the
control, a tendency towards increased systolic EL was observed in
patients with HCM. In the present study, blood flow velocity
decreased from base to apex, thus EL decreased from base to
apex.
Blood flow dynamics in the left ventricle feature
the formation of vortices, which are associated with the smooth
redirection of flow from the inlet to the outflow tract (27,28). A
recent study indicated that vortex-ring formation reflects
diastolic function and overall cardiac health (29). The vortex of the blood flow is formed
during early diastole, is sustained throughout the diastolic phase
and the blood stream is subsequently directed to the outflow tract
in a laminar flow during the systolic phase (27,30,31). The
instability of the vortex also readily leads to a loss of
coherence, turbulence and the breaking up of the flow into small,
irregular vortex structures (27).
Stugaard et al (21) reported
that diastolic EL increased in aortic regurgitation (AR),
proportional to its severity. A group from China observed that
systolic and diastolic EL were increased in patients with diabetes
mellitus with normal LVEF, and that uncontrolled blood glucose
levels may lead to increased systolic and diastolic EL in the left
ventricle (10). The present study
suggested that LVEL is sensitive in terms of the subclinical LV
dysfunction of patients with HCM, including systolic and diastolic
function. As patients with HCM had smaller ventricular cavities,
stiffer ventricular walls and elevated filling pressures, the
diastolic filling flow from atrium to ventricle has a slower
velocity, a smaller vortex and a decreased EL (32). During the systolic phase, the
decreased longitudinal deformation with compensation of increased
radial deformation maintains a normal or supernormal LVEF (4,8,33), which results in increased systolic EL
in the ventricle.
To the best of our knowledge, the LA physiology
during every cardiac cycle consists of three different phases that
modulate LV filling: The reservoir phase, the conduit phase and the
atrial systolic phase (13,14). When the mitral valve opens, the LA
cavity is in direct contact with the LV cavity; therefore, any
alterations in LA structure, function and hemodynamics may
represent the average LV filling pressure history.
The present study found that LA size and volume were
significantly increased in patients with HCM. Previous studies have
suggested that the E/e' ratio is an instant measurement of LV
filling pressure, and the LA volume index reflects the cumulative
effect of the filling pressures over time (20). The reduced PALS, mSRs, mSRe and mSRa
measured by STE were also similar to previous studies (14,20,34,35). In
the present study, LA reservoir function (PALS and mSRs) and
conduit function (mSRe) were impaired in patients with HCM, without
an increase in LA pump function (mSRa), which is an important
compensatory mechanism that facilitates LA filling during aging
(36). The LA stiffness index was
elevated in patients with HCM, although not in the control group,
which indicated that atrial fibrosis and stiffness may be present
in patients with HCM with existing diastolic dysfunction of the LV,
as heart failure, arterial hypertension and atrial fibrillation was
observed (20,37). LA function progressively decreases in
patients with HCM, and LA longitudinal strain has been recognized
as a useful parameter to predict LA dysfunction and elevated LV
filling pressure (20,35).
The current study revealed that the EL in the
reservoir, conduit and atrial systolic phases was decreased in HCM
compared with the controls. The extent of active, passive and
conduit filling by the atrium is significantly influenced by the
compliance of the left ventricle (14). Structural atrial remodeling
represents an additional morpho-functional correlation with LA
strain, and a close correlation exists between PALS and left atrium
myocardial fibrosis (14). The
present study revealed that the LAEL positively correlated with the
PALS and negatively correlated with the stiffness index. It was
observed that decreased PALS indicated LA pressure rose to maintain
adequate LV filling in response to increased LV stiffness or
non-compliance, as previously observed in patients with HCM
(38) and increased LA pressure
causes elevated atrial wall tension, which leads to chamber
dilatation and stretching of the atrial myocardium (39). LA wall stiffness and fibrosis, as
evaluated by PALS, may lead to LA dysfunction and a reduction in EL
throughout the reservoir, conduit and atrial systolic phases. A
negative impact of diabetes on LA function was previously
demonstrated via assessment of phasic LAEL by VFM, and even in the
presence of a normal left atrium size, the EL during the reservoir
and conduit phases decreased, but increased in the atrial systolic
phase (40). In patients with
various degrees of chronic AR, diastolic EL increases with the
severity of AR. In this situation, EL produced by inefficient
turbulent flow may be a burden to the heart (21).
Of note, there are a number of limitations to the
present cross-sectional study. The principal limitation of the
study is the relatively small sample size. Future studies with
larger sample sizes and increased long-term follow-up times are
required to confirm the prognostic value of EL in HCM. Furthermore,
the current software (DAS-RS1 5.0 workstation) was used for LV
analysis to study LA strain and strain rate. A certain degree of
inaccuracy may have arisen due to technical reasons.
The present study demonstrated the functional and
structural alterations, in addition to hemodynamic alterations, in
patients with the non-obstructive form of HCM with preserved EF.
The results suggested that, although EF and E/e' may be normal,
patients with HCM may have systolic and diastolic dysfunction.
Furthermore, the present findings revealed that VFM combined with
2D STE may be a useful tool for the detection of LA and LV
subclinical dysfunction in patients with HCM. VFM and the derived
dissipative EL may provide a promising novel method to quantify
heart function. However, prospective studies are required to
confirm the present findings and evaluate the usefulness of EL as a
prognostic marker of HCM.
Acknowledgements
Not applicable.
Funding
The present study was supported by research grants
from the Natural Science Foundation of Shandong Province (grant no.
ZR2014HQ037), the National Natural Science Foundation of China
(grant nos. 81600633, 81570400, 81470560, 81670411, 81471036,
81400285 and 81702194), the Key Research and Development Program of
Shandong Province (grant no. 2017GSF18156), the Medicine and Health
Science Technology Development Program of Shandong province (grant
no. 2016WS0091), the Shandong Provincial Natural Science Foundation
of China (grant no. ZR2015CL012) and the Research Program of Qilu
Hospital of Shandong University (grant no. 2017QLQN37).
Availability of data and materials
The datasets used and/or analyzed during the current
study are available from the corresponding author on reasonable
request.
Authors' contributions
YC, WZ and YS drafted the manuscript. MiZ, LL, MeZ
and GJ collected and analyzed the data. ML, YZ and XS statistically
analyzed the data. All authors read and approved the final
manuscript.
Ethics approval and consent to
participate
The current study was approved by the Ethics
Committee of Qilu Hospital of Shandong University (Jinan, China).
Written informed consent was obtained from each patient.
Patient consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing
interests.
References
|
1
|
Ingles J, Burns C, Bagnall RD, Lam L,
Yeates L, Sarina T, Puranik R, Briffa T, Atherton JJ, Driscoll T
and Semsarian C: Nonfamilial hypertrophic cardiomyopathy:
Prevalence, natural history, and clinical implications. Circ
Cardiovasc Genet. 10(pii): e0016202017.PubMed/NCBI
|
|
2
|
Jacoby DL, DePasquale EC and McKenna WJ:
Hypertrophic cardiomyopathy: Diagnosis, risk stratification and
treatment. CMAJ. 185:127–134. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
3
|
Houston BA and Stevens GR: Hypertrophic
cardiomyopathy: A review. Clin Med Insights Cardiol. 8 (Suppl
1):S53–S65. 2015.
|
|
4
|
Authors/Task Force members, ; Elliott PM,
Anastasakis A, Borger MA, Borggrefe M, Cecchi F, Charron P, Hagege
AA, Lafont A, Limongelli G, et al: 2014 ESC Guidelines on diagnosis
and management of hypertrophic cardiomyopathy: The Task Force for
the diagnosis and management of hypertrophic cardiomyopathy of the
European society of cardiology (ESC). Eur Heart J. 35:2733–2779.
2014. View Article : Google Scholar : PubMed/NCBI
|
|
5
|
Voilliot D, Huttin O, Hammache N,
Filippetti L, Vaugrenard T, Aliot E, Sadoul N, Juillière Y and
Selton-Suty C: Impact of Global and segmental hypertrophy on
two-dimensional strain derived from three-dimensional
echocardiography in hypertrophic cardiomyopathy: Comparison with
healthy subjects. J Am Soc Echocardiogr. 28:1093–1102. 2015.
View Article : Google Scholar : PubMed/NCBI
|
|
6
|
Maron BJ and Maron MS: Hypertrophic
cardiomyopathy. Lancet (London, England). 381:242–255. 2013.
View Article : Google Scholar : PubMed/NCBI
|
|
7
|
Kalra A, Harris KM, Maron BA, Maron MS,
Garberich RF, Haas TS, Lesser JR and Maron BJ: Relation of Doppler
tissue imaging parameters with heart failure progression in
hypertrophic cardiomyopathy. Am J Cardiol. 117:1808–1814. 2016.
View Article : Google Scholar : PubMed/NCBI
|
|
8
|
Saccheri MC, Cianciulli TF, Lax JA, Guerra
JE, Redruello HJ, Weich Glogier FL, Gagliardi JA, Dorelle AN,
Prezioso HA and Vidal LA: Impaired myocardial function in
hypertrophic cardiomyopathy. Echocardiography. 26:657–664. 2009.
View Article : Google Scholar : PubMed/NCBI
|
|
9
|
MacIver DH and Clark AL: Contractile
dysfunction in sarcomeric hypertrophic cardiomyopathy. J Card Fail.
22:731–737. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
10
|
Hayashi T, Itatani K, Inuzuka R, Shimizu
N, Shindo T, Hirata Y and Miyaji K: Dissipative energy loss within
the left ventricle detected by vector flow mapping in children:
Normal values and effects of age and heart rate. J Cardiol.
66:403–410. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
11
|
Kurt M, Wang J, Torre-Amione G and Nagueh
SF: Left atrial function in diastolic heart failure. Circ
Cardiovasc Imaging. 2:10–15. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
12
|
Mancia G, Fagard R, Narkiewicz K, Redon J,
Zanchetti A, Böhm M, Christiaens T, Cifkova R, De Backer G,
Dominiczak A, et al: 2013 ESH/ESC guidelines for the management of
arterial hypertension: The Task force for the management of
arterial hypertension of the European society of hypertension (ESH)
and of the European society of cardiology (ESC). Eur Heart J.
34:2159–2219. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
13
|
Cameli M, Mandoli GE and Mondillo S: Left
atrium: The last bulwark before overt heart failure. Heart Fail
Rev. 22:123–131. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
14
|
Cameli M, Ciccone MM, Maiello M, Modesti
PA, Muiesan ML, Scicchitano P, Novo S, Palmiero P, Saba PS and
Pedrinelli R; Gruppo di Studio Ipertensione, Prevenzione e
Riabilitazione, Società Italiana di Cardiologia, : Speckle tracking
analysis: A new tool for left atrial function analysis in systemic
hypertension: An overview. J Cardiovasc Med (Hagerstown).
17:339–343. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
15
|
Xu HY, Chen J, Yang ZG, Li R, Shi K, Zhang
Q, Liu X, Xie LJ, Jiang L and Guo YK: Early marker of regional left
ventricular deformation in patients with hypertrophic
cardiomyopathy evaluated by MRI tissue tracking: The effects of
myocardial hypertrophy and fibrosis. J Magn Reson Imaging.
46:1368–1376. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
16
|
Ozawa K, Funabashi N, Takaoka H, Kamata T,
Kanaeda A, Saito M, Nomura F and Kobayashi Y: Characteristic
myocardial strain identified in hypertrophic cardiomyopathy
subjects with preserved left ventricular ejection fraction using a
novel multi-layer transthoracic echocardiography technique. Int J
Cardiol. 184:237–243. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
17
|
Kato TS, Noda A, Izawa H, Yamada A, Obata
K, Nagata K, Iwase M, Murohara T and Yokota M: Discrimination of
nonobstructive hypertrophic cardiomyopathy from hypertensive left
ventricular hypertrophy on the basis of strain rate imaging by
tissue Doppler ultrasonography. Circulation. 110:3808–3814. 2004.
View Article : Google Scholar : PubMed/NCBI
|
|
18
|
Oki T, Mishiro Y, Yamada H, Onose Y,
Matsuoka M, Wakatsuki T, Tabata T and Ito S: Detection of left
ventricular regional relaxation abnormalities and asynchrony in
patients with hypertrophic cardiomyopathy with the use of tissue
Doppler imaging. Am Heart J. 139:497–502. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
19
|
Amundsen BH, Helle-Valle T, Edvardsen T,
Torp H, Crosby J, Lyseggen E, Støylen A, Ihlen H, Lima JA, Smiseth
OA and Slørdahl SA: Noninvasive myocardial strain measurement by
speckle tracking echocardiography: Validation against
sonomicrometry and tagged magnetic resonance imaging. J Am Coll
Cardiol. 47:789–793. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
20
|
Cameli M, Mandoli GE, Loiacono F, Dini FL,
Henein M and Mondillo S: Left atrial strain: A new parameter for
assessment of left ventricular filling pressure. Heart Fail Rev.
21:65–76. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
21
|
Stugaard M, Koriyama H, Katsuki K, Masuda
K, Asanuma T, Takeda Y, Sakata Y, Itatani K and Nakatani S: Energy
loss in the left ventricle obtained by vector flow mapping as a new
quantitative measure of severity of aortic regurgitation: A
combined experimental and clinical study. Eur Heart J Cardiovasc
Imaging. 16:723–730. 2015. View Article : Google Scholar : PubMed/NCBI
|
|
22
|
Serri K, Reant P, Lafitte M, Berhouet M,
Le Bouffos V, Roudaut R and Lafitte S: Global and regional
myocardial function quantification by two-dimensional strain:
Application in hypertrophic cardiomyopathy. J Am Coll Cardiol.
47:1175–1181. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
23
|
Urbano-Moral JA, Rowin EJ, Maron MS, Crean
A and Pandian NG: Investigation of global and regional myocardial
mechanics with 3-dimensional speckle tracking echocardiography and
relations to hypertrophy and fibrosis in hypertrophic
cardiomyopathy. Circ Cardiovasc Imaging. 7:11–19. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
24
|
Maron BJ, Spirito P, Green KJ, Wesley YE,
Bonow RO and Arce J: Noninvasive assessment of left ventricular
diastolic function by pulsed Doppler echocardiography in patients
with hypertrophic cardiomyopathy. J Am Coll Cardiol. 10:733–742.
1987. View Article : Google Scholar : PubMed/NCBI
|
|
25
|
Liu W, Sun D and Yang J: Diastolic
dysfunction of hypertrophic cardiomyopathy genotype-positive
subjects without hypertrophy is detected by tissue Doppler imaging:
A systematic review and Meta-analysis. J Ultrasound Med.
36:2093–2103. 2017. View Article : Google Scholar : PubMed/NCBI
|
|
26
|
Ho CY: Hypertrophic cardiomyopathy:
Preclinical and early phenotype. J Cardiovasc Transl Res.
2:462–470. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
27
|
Pedrizzetti G, La Canna G, Alfieri O and
Tonti G: The vortex-an early predictor of cardiovascular outcome?
Nat Rev Cardiol. 11:545–553. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
28
|
Kilner PJ, Yang GZ, Wilkes AJ, Mohiaddin
RH, Firmin DN and Yacoub MH: Asymmetric redirection of flow through
the heart. Nature. 404:759–761. 2000. View Article : Google Scholar : PubMed/NCBI
|
|
29
|
Gharib M, Rambod E, Kheradvar A, Sahn DJ
and Dabiri JO: Optimal vortex formation as an index of cardiac
health. Proc Natl Acad Sci USA. 103:6305–6308. 2006. View Article : Google Scholar : PubMed/NCBI
|
|
30
|
Borazjani I, Westerdale J, McMahon EM,
Rajaraman PK, Heys JJ and Belohlavek M: Left ventricular flow
analysis: Recent advances in numerical methods and applications in
cardiac ultrasound. Comput Math Methods Med. 2013:3950812013.
View Article : Google Scholar : PubMed/NCBI
|
|
31
|
Abe H, Caracciolo G, Kheradvar A,
Pedrizzetti G, Khandheria BK, Narula J and Sengupta PP: Contrast
echocardiography for assessing left ventricular vortex strength in
heart failure: A prospective cohort study. Eur Heart J Cardiovasc
Imaging. 14:1049–1060. 2013. View Article : Google Scholar : PubMed/NCBI
|
|
32
|
Maron BJ: Hypertrophic cardiomyopathy: A
systematic review. JAMA. 287:1308–1320. 2002. View Article : Google Scholar : PubMed/NCBI
|
|
33
|
Butz T, van Buuren F, Mellwig KP, Langer
C, Plehn G, Meissner A, Trappe HJ, Horstkotte D and Faber L:
Two-dimensional strain analysis of the global and regional
myocardial function for the differentiation of pathologic and
physiologic left ventricular hypertrophy: A study in athletes and
in patients with hypertrophic cardiomyopathy. Int J Cardiovasc
Imaging. 27:91–100. 2011. View Article : Google Scholar : PubMed/NCBI
|
|
34
|
Aly MF, Brouwer WP, Kleijn SA, van Rossum
AC and Kamp O: Three-dimensional speckle tracking echocardiography
for the preclinical diagnosis of hypertrophic cardiomyopathy. Int J
Cardiovasc Imaging. 30:523–533. 2014. View Article : Google Scholar : PubMed/NCBI
|
|
35
|
Cameli M, Sparla S, Losito M, Righini FM,
Menci D, Lisi M, D'Ascenzi F, Focardi M, Favilli R, Pierli C, et
al: Correlation of left atrial strain and Doppler measurements with
invasive measurement of left ventricular End-diastolic pressure in
patients stratified for different values of ejection fraction.
Echocardiography. 33:398–405. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
36
|
Lakatta EG and Levy D: Arterial and
cardiac aging: Major shareholders in cardiovascular disease
enterprises: Part II: The aging heart in health: links to heart
disease. Circulation. 107:346–354. 2003. View Article : Google Scholar : PubMed/NCBI
|
|
37
|
Cameli M, Mandoli GE, Loiacono F, Sparla
S, Iardino E and Mondillo S: Left atrial strain: A useful index in
atrial fibrillation. Int J Cardiol. 220:208–213. 2016. View Article : Google Scholar : PubMed/NCBI
|
|
38
|
Paraskevaidis IA, Panou F, Papadopoulos C,
Farmakis D, Parissis J, Ikonomidis I, Rigopoulos A, Iliodromitis EK
and Th Kremastinos D: Evaluation of left atrial longitudinal
function in patients with hypertrophic cardiomyopathy: A tissue
Doppler imaging and two-dimensional strain study. Heart.
95:483–489. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
39
|
Pavlopoulos H and Nihoyannopoulos P: Left
atrial size: A structural expression of abnormal left ventricular
segmental relaxation evaluated by strain echocardiography. Eur J
Echocardiogr. 10:865–871. 2009. View Article : Google Scholar : PubMed/NCBI
|
|
40
|
Wang Y, Hou D, Ma R, Ding G, Yin L and
Zhang M: Early detection of left atrial energy loss and mechanics
abnormalities in diabetic patients with normal left atrial size: A
study combining vector flow mapping and tissue tracking
echocardiography. Med Sci Monit. 22:958–968. 2016. View Article : Google Scholar : PubMed/NCBI
|